Childhood ADHD: Recent Updates and Treatment Review. Rushiraj C. Laiwala. Attention-Deficit/Hyperactivity Disorder. The most common childhood behavioral disorder diagnosed in outpatient setting in United States. - PowerPoint PPT Presentation
ADHD: Recent Updates and Treatment Review
Childhood ADHD: Recent Updates and Treatment ReviewRushiraj C.
LaiwalaAttention-Deficit/Hyperactivity DisorderThe most common
childhood behavioral disorder diagnosed in outpatient setting in
United States. ADHD has been the focus of a great deal scientific-
clinical research and controversy. Overall, ADHD is one of the best
researched disorders in medicine and overall data on its validity
are far more compelling than many other medical conditions-
American Medical Associations Council on Scientific Affairs (
Goldman et al., 1998)History1902 George Still wrote about children
with restless, impulsive and inattentive, intense affective
responses and conduct problems. 1919 & 1920- Influenza pandemic
and encephalitis lethargica epidemic- Children who survived the flu
developed similar behavioral symptoms-Hypothesis of brain damage-
Minimal Brain Damage Syndrome1937- C.Bradley- d,l- amphetamine
reduced restlessness and improved concentration in children with
behavioral problems in residential treatment center. 30 years later
Keith Conners and Leon Isenberg evaluated efficacy of
dextroamphetamine for children with learning disability and
behavioral problems. HistoryEarly 1960s- Minimal Brain Dysfunction
Late 1960s- ICD-9 & DSM- II adopted- Hyperkinetic Syndrome of
Childhood.1970- Further research suggested that the main
disability- impaired attention and impulsivity- gross motor
overactivity was secondary. 1980- DSM III- Attention-Deficit
Disorder ADD. With HyperactivityWithout HyperactivityResidual Type.
DSM IV- ADHDDefinition: (DSM-IV)ADHD is a behavioral and
neurocognitive condition characterized by developmentally
inappropriate and impairing levels of gross motor overactivity,
inattention, and impulsivity.There are five main diagnostic
criteria: (1) an onset before age 7 years (2) duration greater than
6 months (3) an 18-item symptom list of which 6 of 9 inattention or
6 of 9 hyperactive/impulsive symptoms have persisted for at least 6
months to a degree that is maladaptive and inconsistent with
developmental level; (4) some impairment in two or more settings
(5) symptoms that do not occur exclusively during the course of a
pervasive developmental disorder, schizophrenia, or other psychotic
disorder and are not better accounted for by another mental
disorder, such as depression.
Definition: (DSM-IV)ADHD, Predominately Inattentive Type - 6 of
9 symptoms of inattention,
ADHD, Predominately Hyperactive-Impulsive Type-6 of 9 symptoms
of hyperactivity/impulsivity
ADHD, Combined Type- 6 of 9 symptoms in both areas.
Proposed Revision for DSM V
http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=383#Comparative
NosologyICD-10 DSM-IV-TRHyperkinetic Disorder (HD)ADHDMinimum
criteria: 6 of 9 Inattentive and 3 of 5 Hyperactivity and 1 of 4
impulsiveCriteria: 6 of 9 Inattentive or 6 of 9
Hyperactivity/impulsive or Both. Can not diagnose HD if criteria
for emotional disorder are met (Depression or Anxiety) Can diagnose
ADHD even if criteria for emotional disorder metCases not meeting
HD criteria- Must be managed psychologically before medication can
be started. Out of 579 children with DSM-IV ADHD, Combined Subtype,
from Multimodal Treatment Study (MTA trial), only 25% met the
diagnostic criteria for HD. EPIDEMIOLOGYPolanczyk and colleagues
estimated worldwide prevalence to be 5.2 percent. (meta-analysis
that included hundreds of articles and more than 100,000 patients).
Significant geographical variability and local variability among
studies. Prevalence in N. America is higher than Africa, Europe and
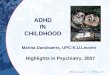
Middle East. According to CDC data,Approximately 9.5% or 5.4
million children 4-17 years of age have ever been diagnosed with
ADHD (2007) The percentage of children with a parent-reported ADHD
diagnosis increased by 22% between 2003 and 2007.Boys (13.2%) were
more likely than girls (5.6%) to have ever been diagnosed with
ADHDPrevalence of parent-reported ADHD diagnosis varied
substantially by state State-based Prevalence Data of ADHD
Diagnosis20032007
Stimulant Use - Steady Rise. National Institutes of Health (NIH)
and the Agency for Healthcare Research and Quality (AHRQ): Use of
Stimulant Medication, 1987- 0.6 % 1997- 2.7 % 2008- 3.5 % Use among
6-12-year-olds was highest, going from 4.2 percent in 1996 to 5.1
percent in 2008. Fastest growth of use among 13-18-year-olds, going
from 2.3 percent in 1996 to 4.9 percent in 2008.
What Causes ADHD?Exact cause unknownMeta-analysis of 83 studies
with more than 6,000 subjects showed that patients with ADHD have
impairments in the executive functioning domains of response
inhibition, vigilance, working memory, and some measures of
planning (Willcutt et al., 2005). A growing consensus that the
condition involves functional and anatomical dysfunction in the
brain's frontal cortex and basal ganglia segments of the
cortico-basal ganglia-thalamo-cortical circuitry.So what causes
this dysfunction- Genetics Neuroanatomical Neurotransmitter
Environment Brain Injuries
Genetics Twin, sibling, adoption, and family studies, have all
suggested that genetic factors play an important role in
ADHD.Thyroid Receptor B GeneDopamine Type D2 Receptor GeneDopamine
Transporter GeneDopamine 4 Receptor GeneDopamine -hydroxylase
(DBH)LPHN3 gene (Arcos-Burgos M, et al.)(ADHD cases where LPHN3
gene (9%) is present are particularly responsive to stimulant
medication.)Neurotransmitters in ADHDDopamine SystemMolecular
genetic studies have targeted genes involved in Dopamine
Regulation. Stimulant drugs bind strongly to dopamine transporter
to prevent reuptake of dopamine back into the presynaptic axon for
metabolism. Noradrenergic SystemDysfunction in norepinephrine
systems can explain- inattention and higher levels of gross motor
activity. TCAs and Atomoxetine (potent norepinephrine reuptake
inhibitors) have shown clinical improvement. Neuroanatomical
(Neuroimaging Research)Children with ADHD have reduced cortical
white and gray matter volume. Volume deficits are more pronounced
in treatment-naive children (Castellanos et al., 2002).Decreased
frontal and temporal lobe volume in children with ADHD relative to
controls (Sowell et al. 2003).NIMH intramural researchers found
that cortex is thinner in children with ADHD and remains thin in
those with less improvement. In teens who showed improvement, the
cortex thickened on the right side( Drs. Philip Shaw and Judith
Rapoport, NIMH Child Psychiatry Branch, and colleagues )
Neuroimaging ResearchBrain matures in a normal pattern but is
delayed three years in some regions, on average, compared to
control. (Philip Shaw, M.D., NIMH Child Psychiatry Branch) Frontal
and temporal lobe showed the greatest maturational delay in youth
with ADHD. The motor cortex emerged as the only area that matured
faster than normal in the youth with ADHD, in contrast to the
late-maturing frontal cortex areas that direct it. This mismatch
might account for the restlessness and fidgety symptoms. The
delayed pattern of maturation observed in ADHD is the opposite of
that seen in other developmental brain disorders like autism, in
which the volume of brain structures peak at a much
earlier-than-normal age. Neuroimaging Research
Environmental Factors.Studies suggest a potential link between
cigarette smoking and alcohol use during pregnancy and ADHD in
children.Preschoolers who are exposed to high levels of lead, may
have a higher risk of developing ADHD.Sugar: The idea that refined
sugar causes ADHD or makes symptoms worse is popular, but more
research discounts this theory than supports it.Food additives:
Recent British research indicates a possible link between
consumption of certain food additives like artificial colors or
preservatives, and an increase in activity. Research is under way
to confirm the findings and to learn more about how food additives
may affect hyperactivity.
Brain injuriesChildren suffering a severe head injury may
develop symptoms of ADHD, usually of the inattentive subtype.
However, only a small percentage of children with ADHD have
suffered a traumatic brain injury.
Encephalopathies can cause inattention but generally produce
other neurological symptoms (language or motor impairment) in
addition to inattention.
ComorbiditiesOppositional defiant disorder (ODD)- 50% Some of
these patients will develop conduct disorder. Anxiety Disorder-
30-35 % Learning Disorder and Language Problem- 25-35 % Substance
Abuse- 15-19 % Mood Disorder- contentious issue- with various
studies indicating 0-33%
Screening: In any mental health assessment, ask questions
regarding major symptoms ( inattention, impulsivity and
hyperactivity) regardless of chief complaint.
Rating scales and specific questionnaires can be included during
office/clinic registration or before the interview.
If a parent reports that the patient suffers from any symptoms
of ADHD that induce impairment or if the patient scores in the
clinical range for ADHD symptoms on a rating scale, then a full
evaluation for ADHD should be done. EvaluationThree Major
Components: Interview with the parents. Interview with the
child/adolescent.Investigation & psychological testing.
Interview with the parents A detail interview about each 18
symptoms. For each symptomsAge of Onset ( Childhood ) Duration (
Chronic ) Frequency ( More days than not ) Impairment ( Do not
confuse with symptom) Interview parent regarding common psychiatric
disorders ( ODD, CD, Depression, Anxiety, tic disorder, Substance
Abuse, Psychosis) Family history: psychiatric illness. ( ADHD,
Anxiety, Tic, CD) Social history: Structured Vs
DisorganizedPerinatal history, development history, milestones,
medical history and mental health history. Interview with the
parentsParent should complete one of many standardized behavior
rating scales. Request release of information- obtain similar
rating scale from school teacher. Common rating scales: Academic
Performance Rating Scale (APRS)ADHD Rating Scale-IVChild Behavior
Checklist (CBCL)Conners Parent Rating Scale RevisedConners Teacher
Rating Scale-Revised Conners Wells Adolescent Self-Report
ScaleVanderbilt ADHD Diagnostic Parent and Teacher Scales and
others These scales also provide information about other
psychiatric symptoms which could be comorbid with ADHD or would
suggest alternative diagnosis.
Interview with the child or adolescentPreschool or young
school-age child (5-8 years old), interview may be done
concurrently with the parent interview.Older children and
adolescents should be interviewed separately from parents, as they
may not reveal significant symptoms (depression, suicidal
ideations, drug or alcohol abuse) in the presence of a parent. The
interview with the child or adolescent is not to confirm or rule
out the diagnosis of ADHD. ( Young child may not be aware of
symptoms and teenage may under report symptoms) Specific emphasis
to objective features to assess vocabulary, thought processes, and
content of thought. Investigation & Psychological Testing For
unremarkable medical history- no investigation required.
Psychological Testing: Not mandatory To differentiate between ADHD
and learning disorder. Academic impairment can be from ADHD or
learning disorder or both. 1:1 Supervision- if child can perform at
grade level or above- likely from ADHD- first treat ADHDChild
engages in leisure activity that require a skill but would avoid
reading a book for examination, first treat ADHDPresence of
symptoms not from ADHD like impairment in expressive receptive
language, poor phonological processing, poor motor co-ordination,
difficulty grasping fundamental mathematics.
TreatmentSeveral interventions are effective in treating
children with ADHD, including medications and behavior therapy.To
examine how intensive treatment with medications compares with
intensive behavior therapy, or with the combination of the two,
NIMH sponsoredthe Multimodal Treatment of ADHD (MTA) study.The
study included nearly 579 children, ages 7-9, who were randomly
assigned to one of four treatment modes:Intensive medication
management alone;Intensive behavioral treatment alone;A combination
of both; orRoutine community care (the control group).
Multimodal Treatment of ADHD (MTA) studyAt the end of the 14
months, all groups showed improvement. The medication management
and combined treatment groups showed significantly greater
reduction in core ADHD symptoms and impairment.Combined treatment,
but not medication management, was superior to community care and
intensive behavioral treatment for oppositional and aggressive
symptoms, internalizing symptoms, teacher-rated social skills,
parentchild relationships, and reading achievement.
Multimodal Treatment of ADHD (MTA) studyMTA treatment lasted for
14 months only, after which the children were referred back to
their community providers.All participants, were invited to return
to the MTA clinics every one to two years for an assessment of
their ADHD symptoms and level of functioning.At the end of three
year follow up, Sustained improvement after three years. Initial
advantages of medication management alone or in combination with
behavioral treatment over purely behavioral or routine community
care started to wane.Ratings from families and teachers favored the
combination treatment, which allowed for lower medication doses.
The careful management of medication by MTA physicians produced
better outcomes than medication provided through usual community
care sources.Multimodal Treatment of ADHD (MTA) study8 year
follow-up, The eight-year follow-up revealed no differences in
symptoms or functioning among the youths assigned to the different
treatment groups as children. Youths with ADHD still had
significantly more academic and social problems compared with peers
who did not have ADHD. Youths who had responded well to treatment
and maintained their gains for two more years after the end of the
trial tended to be functioning the best at eight years.
Multimodal Treatment of ADHD (MTA) study8 year follow-up (
Continued) A majority (61.5 percent) of the children who were
medicated at the end of the 14-month trial had stopped taking
medication by the eight-year follow-up, suggesting that medication
treatment may lose appeal with families over time. The reasons for
this decline are under investigation, but they nevertheless signal
the need for alternative treatments.Children who were no longer
taking medication at the eight-year follow-up were generally
functioning as well as children who were still medicated, raising
questions about whether medication treatment beyond two years
continues to be beneficial or needed by all.
Treatment Begins with psychoeducationInvolves educating the
parent and child about ADHD and its various treatment options
(medication and behavior therapy), linkage with community supports
and additional school resources. Take into account the most recent
evidence concerning effective therapies as well as family
preferences and concerns.Use books, articles, videos, and some
noncommercial web sites on ADHD to educate parents and patients.
http://www.adhdawarenessweek.org/,http://www.nimh.nih.govhttp://www.cdc.gov
and many more.
Medication (Stimulants) The short-term efficacy of
psychopharmacological intervention for ADHD is well established.
Methylphenidate (MPH) or amphetamine the two are equally
efficacious. Long-acting formulations (Offers convenience and
confidentiality) are equally efficacious as the immediate-release
forms in both adolescents as well as children. (Spencer et al.,
2006; Wilens et al., 2006) Medication (Stimulants)Careful titration
Teacher and parent rating scales at end of one week of increase in
dose Equal response to both MPH and Amphetamine - 41 % Preferential
response to MPH or Amphetamine - 44 %Initial response rate- 85% if
both stimulants are tried (65% -75% response when only one
stimulant is tried). Regular monitoring. Look for side effects,
Most common: appetite decrease, weight loss, insomnia, headache
Less common: tics and emotional lability/irritability Medication-
Monitoring Height and Weight:Serial plotting of on growth charts.
Change in height or weight that shows aberrant growth trajectory-
consider drug holidays or switching medication.
Blood Pressure and Pulse: MTA at 14th Month- higher heart rates
but no tachycardia.10 year follow-up- Did not appear to increase
the risk for abnormal elevations in blood pressure or heart rate.
Epidemiological studies have indicated that even modest elevations
in heart rate may increase a persons lifetime risk for
cardiovascular problems. Persistent effect of continuous stimulant
treatment on heart rate should not be dismissed. Medication-
MonitoringEKG: Cases of sudden death have been reported. MPH:
0.2/100,000 & Amphetamine: 0.2/100,000 (exposure period
January1, 1992 to December 31, 2004) (Villalaba-2006) Package
insert- generally not be used in children and adolescents with
preexisting heart disease or symptoms suggesting significant
cardiovascular disease. No evidence currently indicates a need for
routine cardiac evaluation (i.e., electrocardiography,
echocardiography) before starting any stimulant treatment in
otherwise healthy individuals (Biederman et al., 2006). Adding ECG
to the current standard of care may identify more children at risk
for SCD prior to starting them on stimulants for treating ADHD but
it is borderline cost-effective. (Dr. Peter Denchev, and
colleagues, 2010)The American Heart Association currently
recommends that doctors consider obtaining an ECG prior to
prescribing stimulants if they believe it is warranted.Medication-
MonitoringTics: Stimulant induced tics- less clearChildren with
comorbid ADHD and tic disorders, on average, show a decline in tics
when treated with a stimulant but clinicians have noticed stimulant
induced tics, too. Treatment-emergent tics during a trial- consider
an alternative stimulant or a non stimulant Symptoms respond
adequately only to a stimulant medication that induces tics-
consider clonidine or guanfacine (Tourettes Syndrome Study Group,
2002)Medication- MonitoringAggression and Mood Lability: Aggressive
acts and antisocial behavior may decline with stimulants (Connor et
al., 2002 [rct]). Stimulant induced vs ReboundFor rebound
hyperactivity- small dose of immediate release stimulant in the
late afternoon. Rare cases of aggressive behavior, psychosis and
manic symptoms reported (black box warning)If stimulant induced
agression, mood lability, psychosis are evident- stop stimulant.
Adjunctive therapy with neuroleptics or mood stabilizers is not
recommended. Medication- AtomoxetineNoradrenergic reuptake
inhibitor.Less pronounced effects on appetite and sleep.Relatively
more nausea or sedation.Full therapeutic dose for at least several
weeks to obtain full effect. Indicated for ADHD comorbid with
substance abuse. RCT showed a reduction in ratings of symptoms of
both ADHD and anxiety, when used in patient with ADHD and co-morbid
anxiety. (Sumner et al., 2005 ). Black Box Warnings for suicidality
and not approved for major depression. Treatment Failure with
stimulantIf the patient fails to respond to trials after an
adequate length of time at appropriate doses, Review diagnosis of
ADHD again. Consider behavioral therapy. Consider alternative
medications like bupropion, tricyclic antidepressants (TCAs), and
alpha-agonists. Psychosocial TreatmentIncludes different
modalities, such as psychoeducation, academic organization skill
teaching and remediation, parent training, behavior modification,
cognitivebehavioral therapy (CBT), social skills training, and
individual therapy.Parent training, intensive behavior
modification, and social skills training have shown most efficacy
for children with ADHD in controlled trials.
Intensive Behavioral InterventionsPsychoeducation about the
course, risk factors, and long-term outcomes of ADHDThe parents are
encouraged to attend more carefully to their child's
behaviorParents are trained to use time out effectively.Parents are
instructed how to establish a contingency management or token
economy system at home.Parents learn how to manage noncompliant
behaviors in public settings.Finally, advances in prosocial
behavior in school are supported by use of a daily report card.
Psychosocial TreatmentExamples of social skills training, how to
wait for their turn, share toys, ask for help, or respond to
teasing. Learning to read facial expressions and the tone of voice
in others, and how to respond appropriately can also be part of
social skills training. It is crucial to evaluate the parents and
family for dysfunction related to the child's ADHD. Parental ADHD
may interfere with behavioral modification programs, indicating
that treatment of the affected parent may be necessary before the
child's intervention can be successful.Medications versus
Psychosocial Management If a patient with ADHD has a robust
response to psychopharmacological treatment and subsequently shows
normative functioning in academic, family, and social functioning,
then psychopharmacological treatment of the ADHD alone is
satisfactory. If a patient with ADHD has a less than optimal
response to medication, has a comorbid disorder, or experiences
stressors in family life, then psychosocial treatment in
conjunction with medication treatment is often beneficial. [(A A C
A P) Practice Parameter] [email protected]
Academy of Child and Adolescent Psychiatry (1997), Practice
parameters for the assessment and treatment of children,
adolescents, and adults with attention-deficit/hyperactivity
disorder. American Academy of Child and Adolescent Psychiatry
(2002), Practice parameters for the assessment and treatment of
children, adolescents, and adults with
attention-deficit/hyperactivity disorder. American Academy of Child
and Adolescent Psychiatry (2007), Practice parameters for the
assessment and treatment of children, adolescents, and adults with
attention-deficit/hyperactivity disorder. Arnold LE (2000),
Methylphenidate vs. amphetamine: comparative review. J Atten Disord
3:200211*The MTA Cooperative Group: A 14-month randomized clinical
trial of treatment strategies for attention deficit/ hyperactivity
disorder (ADHD). Arch Gen Psychiatry. 1999;56:1073.Swanson JM,
Kinsbourne M, Nigg J, Lanphear B, Stephanos GA: Etiologic subtypes
of attention-deficit/hyperactivity disorder: Brain imaging,
molecular genetic and environmental factors and the dopamine
hypothesis. Neuropsychol Rev. 2007;17(1):39.Shaw P, Lerch J,
Greenstein D, Sharp W, Clasen L, Evans A, Giedd J, Castellanos FX,
Rapoport J. Longitudinal mapping of cortical thickness and clinical
outcome in children and adolescents with
attention-deficit/hyperactivity disorder. Arch Gen Psychiatry. 2006
May;63(5):540-9.Plessen KJ, Bansal R, Zhu H, Whiteman R, Amat J,
Quackenbush GA, Martin L, Durkin K, Blair C, Royal J, Hugdahl K,
Peterson BS. Hippocampus and Amygdala Morphology in
Attention-Deficit/Hyperactivity Disorder. Arch Gen Psychiatry. 2006
Jul;63(7):795-807. MTA Cooperative Group: National Institute of
Mental Health Multimodal Treatment Study of ADHD follow-up: changes
in effectiveness and growth after the end of treatment. Pediatrics
2004;113:762-769.Swanson JM, Elliott GR, Greenhill LL, Wigal T,
Arnold LE, Vitiello B, Hechtman L, Epstein J, Pelham W, Abikoff HB,
Newcorn J, Molina B, Hinshaw S, Wells K, Hoza B, Severe JB, Jensen
PS, Gibbons R, Hur K, Stehli A, Davies M, March J, Caron M, Volkow
ND, Posner MI, for the MTA Cooperative Group: Effects of stimulant
medication on growth rates across 3 years in the MTA follow-up. J
Am Acad Child Adolesc Psychiatry 2007;46:1014-1026.Molina BSG,
Hinshaw S.P., Swanson J.M., Arnold, L.E., Vitiello B, Jensen PS,
Epstein JN, Hoza B, Hechtman L., Abikoff, H.B., Elliott GR,
Greenhill LL, Newcorn, JH, Wells KC, Wigal TL, Severe JB, Gibbons
RD, Hur K, Houck PR, and the MTA Cooperative Group: The MTA at 8
years: prospective follow-up of children treated for combined type
ADHD in a multisite study. J Am Acad Child Adolesc Psychiatry
2009;48:484-500.Kaplan & Sadock's Comprehensive Textbook of
Psychiatry Zuvekas S and Vitiello B. Stimulant medication use in
children: a 12-year perspective. American Journal of Psychiatry.
Online ahead of print September 28, 2011.Molina BSG, Hinshaw SP,
Swanson JM, Arnold LE, Vitiello B, Jensen PS, Epstein JN, Hoza B,
Hechtman L, Abikoff HB, Elliott GR, Greenhill LL, Newcorn JH, Wells
KC, Wigal T, Severe JB, Gibbons RD, Hur K, Houck PR, and the MTA
Cooperative Group.The MTA at 8 years: Prospective follow-up of
children treated for combined type ADHD in the multisite study.
Journal of the American Academy of Child and Adolescent Psychiatry.
Online ahead of print March 2009.Other MTA references,
http://www.nimh.nih.gov/http://www.cdc.gov/en.wikipedia.org/wiki/Attention_deficit_hyperactivity_disorder
Referenceshttp://www.nimh.nih.gov/http://www.cdc.gov/en.wikipedia.org/wiki/Attention_deficit_hyperactivity_disorderOther
MTA referencesThe MTA Cooperative Group:A 14-Month randomized
clinical trial of treatment strategies for
attention-deficit/hyperactivity disorder (ADHD).Arch Gen
Psychiatry1999;56:1073-1086.The MTA Cooperative Group: Moderators
and mediators of treatment response for children with
attention-deficit/hyperactivity disorder (ADHD).Arch Gen
Psychiatry1999;56:1088-1096.Swanson JM, Kraemer HC, Hinshaw SP,
Arnold LE, Conners CK, Abikoff HB, Clevenger W, Davies M, Elliott
GR, Greenhill LL, Hechtman L, Hoza, B, Jensen PS, March JS, Newcorn
JH, Owens EB, Pelham WE, Schiller E, Severe JB, Simpson S, Vitiello
B, Wells K, Wigal T, Wu M: Clinical relevance of the primary
findings of the MTA: success rate based on severity of ADHD and ODD
symptoms at the end of treatment.J Am Acad Child Adolesc
Psychiatry2001; 40:168-179.Greenhill LL, Swanson JM, Vitiello B,
Davies M, Clevenger W, Wu M, Arnold LE, Abikoff HB, Bukstein OG,
Conners CK, Elliott GR, Hechtman L, Hinshaw SP, Hoza B, Jensen PS,
Kraemer HC, March JS, Newcorn JH, Severe JB, Wells K, WigalT:
Impairment and deportment responses to different methylphenidate
doses in children with ADHD: the MTA titration trial.J Am Acad
Child Adolesc Psychiatry2001; 40:180-187.Vitiello B, Severe JB,
Greenhill LL, Arnold LE, Abikoff HB, Bukstein O, Elliott GR,
Hechtman L, Jensen PS, Hinshaw SP, March JS, Newcorn JH, Swanson
JM, Cantwell DP: Methylphenidate Dosage for Children with ADHD over
Time under Controlled Conditions: Lessons from the MTA.J Am Acad
Child Adolesc Psychiatry2001; 40:188-196.Owens EB, Hinshaw SP,
Kraemer HC, Arnold LE, Abikoff HB, Cantwell DP, Conners CK, Elliot
G, Greenhill LL, Hechtman L, Hoza B, Jensen PS, March JS, Newcorn
JH, Pelham WE, Richters JE, Schiller EP, Severe JB, Swanson JM,
Vereen D, Vitiello B, Wells KC, Wigal T: What treatment for whom
for ADHD: Moderators of treatment response in the MTA.J Consult
Clin Psychol2003;71:540-552.MTA Cooperative Group: National
Institute of Mental Health Multimodal Treatment Study of ADHD
follow-up: 24-month outcomes of treatment strategies for
attention-deficit/hyperactivity
disorder.Pediatrics2004;113:754-761.MTA Cooperative Group: National
Institute of Mental Health Multimodal Treatment Study of ADHD
follow-up: changes in effectiveness and growth after the end of
treatment.Pediatrics2004;113:762-769.Swanson JM, Elliott GR,
Greenhill LL, Wigal T, Arnold LE, Vitiello B, Hechtman L, Epstein
J, Pelham W, Abikoff HB, Newcorn J, Molina B, Hinshaw S, Wells K,
Hoza B, Severe JB, Jensen PS, Gibbons R, Hur K, Stehli A, Davies M,
March J, Caron M, Volkow ND, Posner MI, for the MTA Cooperative
Group: Effects of stimulant medication on growth rates across 3
years in the MTA follow-up.J Am Acad Child Adolesc
Psychiatry2007;46:1014-1026.Molina BSG, Hinshaw S.P., Swanson J.M.,
Arnold, L.E., Vitiello B, Jensen PS, Epstein JN, Hoza B, Hechtman
L., Abikoff, H.B., Elliott GR, Greenhill LL, Newcorn, JH, Wells KC,
Wigal TL, Severe JB, Gibbons RD, Hur K, Houck PR, and the MTA
Cooperative Group: The MTA at 8 years: prospective follow-up of
children treated for combined type ADHD in a multisite study.J Am
Acad Child Adolesc Psychiatry2009;48:484-500.
Thank You and Merry Christmas!!Special Thanks to Dr. Bird, Dr.
McCarley, Dr. Shulruff