Embed Size (px)
Citation preview
Childhood Maltreatment, Shame-Proneness andSelf-Criticism in Social Anxiety Disorder: ASequential Mediational Model
Ben Shahar,* Guy Doron and Ohad SzepsenwolInterdisciplinary Center, School of Psychology, Herzliya, Israel
Previous research has shown a robust link between emotional abuse and neglect with social anxietysymptoms. However, the mechanisms through which these links operate are less clear. We hypothe-sized a model in which early experiences of abuse and neglect create aversive shame states, internalizedinto a stable shame-based cognitive–affective schema. Self-criticism is conceptualized as a safetystrategy designed to conceal flaws and prevent further experiences of shame. However, self-criticismmaintains negative self-perceptions and insecurity in social situations. To provide preliminary, cross-sectional support for this model, a nonclinical community sample of 219 adults from Israel (110 females,mean age= 38.7) completed measures of childhood trauma, shame-proneness, self-criticism and socialanxiety symptoms. A sequential mediational model showed that emotional abuse, but not emotionalneglect, predicted shame-proneness, which in turn predicted self-criticism, which in turn predicted so-cial anxiety symptoms. These results provide initial evidence supporting the role of shame and self-criticism in the development and maintenance of social anxiety disorder. The clinical implications ofthese findings are discussed Copyright © 2014 John Wiley & Sons, Ltd.
Key Practitioner Message:• Previous research has shown that histories of emotional abuse and emotional neglect predict social anx-
iety symptoms, but the mechanisms that underlie these associations are not clear.• Using psycho-evolutionary and emotion-focused perspectives, the findings of the current study suggest
that shame and self-criticism play an important role in social anxiety and may mediate the link betweenemotional abuse and symptoms.
• These findings also suggest that therapeutic interventions specifically targeting shame and self-criticismshould be incorporated into treatments for social anxiety, especially with socially anxious patients withabuse histories.
Keywords: Childhood Maltreatment, Emotional Abuse, Self-Criticism, Shame, Shame-Proneness, SocialAnxiety Disorder
An increasing number of studies have been emphasizingthe role of childhood maltreatment in the developmentof social anxiety disorder (SAD; Arrindell, Emmelkamp,Monsma, & Brilman, 1983; Arrindell et al., 1989; Bandelowet al., 2004; Bruce et al., 2012; Knappe et al., 2012; Kuo et al.,2011; Simon et al., 2009). However, the specific cognitiveand affective processes that are triggered as a result ofchildhood maltreatment and contribute to the develop-ment and maintenance of SAD are less clear. Current re-search in SAD has been largely focusing on cognitivemaintenance processes, such as self-focused attention,safety behaviours and distorted beliefs regarding the
probability and cost of negative social events (Clark &Wells, 1995; Hofmann, 2007). The occurrence of these pro-cesses, however, has not been systematically linked withchildhood maltreatment. In this paper, we propose a con-ceptual model that attempts to integrate early experiencesof emotional abuse and neglect with subsequentcognitive–affective processes involved in the developmentand maintenance of SAD.Specifically, it is suggested that early experiences of mal-
treatment contribute to the development of SAD via theinternalization of a shame-based cognitive–affectiveschema, characterized by an overall sense of inadequacy.Feeling inferior and different, individuals with SAD areprimarily concerned that their perceived flaws will be ex-posed (Moscovitch, 2009), which would result in the acti-vation of highly aversive shame-based feelings.Therefore, they develop a self-monitoring, self-critical
*Correspondence to: Ben Shahar, Interdisciplinary Center School ofPsychology P.O. Box 167, Herzliya 46150, Israel.E-mail: [email protected]
Clinical Psychology and PsychotherapyClin. Psychol. Psychother. (2014)Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/cpp.1918
Copyright © 2014 John Wiley & Sons, Ltd.

style as a defensive strategy designed to conceal flaws andprevent shame activation. Thus, consistent with a psycho-evolutionary approach to psychopathology (Gilbert &Trower, 2001; Trower & Gilbert, 1989), self-criticism inSAD functions to minimize damage to social rank. How-ever, self-criticism is in itself shaming, maintains negativeself-views and low self-worth, prevents restructuring ofthe shame-based schema, and leads individuals to be con-stantly vigilant about concealing their (perceived) defi-ciencies. The primary aim of this paper is to delineatethis model in more detail and to provide preliminary datato support it in a nonclinical community sample.
Childhood Maltreatment and Shame
Psychoanalytic theorists have long emphasized the linkbetween certain parental behaviours and shame (Kohut,1971; Morrison, 2011). Social psychologists have also em-phasized the link between certain parental behavioursand the development of children’s negative self-concept(Higgins, 1987; Mikulincer & Shaver, 2004). A large num-ber of empirical studies have corroborated these observa-tions, demonstrating associations between forms ofparental behaviours and internalization of shame(Andrews, 1998; Claesson & Sohlberg, 2002; Gilbert,2000; Gilbert, Allan, & Goss, 1996; Kim, Talbot, &Cicchetti, 2009; Stuewig & McCloskey, 2005). Thus, itseems that early experiences of being shamed, by care-givers or peers, lead to intense shame states, which arethen internalized and lead to the development of a morestable shame-based self-schema.Recent studies showed that shame memories can have
the same characteristics as traumatic memories (e.g., in-volving flashbacks, intrusions and avoidance features;Matos & Pinto-Gouveia, 2010) and can become central inpeoples’ life narratives and identities (Pinto-Gouveia &Matos, 2011), which in turn is associated with currentshame-proneness. Thus, intense shame states in childhoodcan be encoded as strong emotional autobiographicalmemories to form a more stable schematic structure. Thepresence of such a schema is associated with perceivingthe self to be inferior in social rank and deficient com-pared with others, to the perception that one’s social sta-tus can easily be lost or damaged, and to possible socialexclusion (Gilbert & Trower, 2001).
Shame and Social Anxiety
Surprisingly, aside from a handful of correlational studies(Fergus, Valentiner, McGrath, & Jencius, 2010; Gilbert,2000; Matos, Pinto-Gouveia, & Gilbert, 2013; Zimmerman,Morrison, & Heimberg, 2014), the direct association be-tween shame measures and social anxiety has not beensystematically studied. However, given that social anxiety
is strongly connected with a preoccupation with socialrank (Aderka, Weisman, Shahar, & Gilboa-Schechtman,2009; Weisman et al., 2011) and that shame is a self-conscious emotion that regulates social rank (Gilbert,1998; Tangney & Dearing, 2002), the association betweenexperiences of shame and social anxiety symptomsappears to be central. Indeed, several social anxietyresearchers (Weeks, Heimberg, & Heuer, 2011) havenoted that shame-related submissive displays are verysimilar to behaviours displayed by socially anxious indi-viduals. For example, many of the safety behavioursdescribed by Clark and Wells (1995) are behavioursdesigned to hide various aspects of the self, and hidingis the primary action tendency of shame (Tangney &Dearing, 2002). The self-monitoring process (self-focusedattention) described by Clark and Wells is also consistentwith descriptions regarding the phenomenology ofshame (e.g., searching internally to locate potential flawsin order to conceal them).According to Gilbert’s psycho-evolutionary model
(Gilbert, 2000; Gilbert & Trower, 2001), individuals withSAD, as a result of feeling inferior and deficient, are overlyfocused on their social rank and tend to view their socialworld in terms of hierarchies (i.e., constantly evaluatingwho is inferior and who is superior). Feeling inferior in so-cial situations elicits submissive-appeasing behaviours,such as avoiding eye contact, appearing timid, avoidingassertive claims and demands, blushing, or speaking withhesitancy (Keltner & Harker, 1998; see Johnson, Leedom,& Muhtadie, 2012, for a review). From an evolutionaryperspective, these submissive-appeasing behaviours arebuilt-in evolved mechanisms that are automatically acti-vated to de-escalate aggressive conflicts and to signal todominant members that the self poses no challenge. How-ever, in human social groups, where the primary goal is tobe liked, valued and wanted (e.g., prestige hierarchy asopposed to dominance hierarchy; Fessler, 2007), such be-haviours are not attractive, and they prevent individualsfrom engaging in pro-social and engaging behaviours,only perpetuating one’s unattractiveness and low socialrank (Gilbert, 2000).Shame is an important factor in this sequence of pro-
cesses. As described above, individuals with SAD areprone to feel shame due to previous early experiences. Insocial situations, or even while anticipating them, ashame-based cognitive–affective schema, rooted in auto-biographical shame memories, is activated. This schematicstructure includes several components, such as experienc-ing oneself as inferior and inadequate; experiencing othersas ‘better’ (smarter, better looking) and potentially critical,and rejecting; beginning a critical self-monitoring process(e.g., self-consciousness) to detect possible flaws; and en-gaging in submissive-appeasing behaviours (Lewis, 1971;Tangney, Wagner, Hill-Barlow, Marschall, & Gramzow,1996). The evolutionary-based functions of these
B. Shahar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

components are (a) to signal to the self that social rank is atstake and possible exclusion is imminent (e.g., ‘be careful,your flaws are about to be exposed, conceal them, other-wise you will be excluded’), and (b) to signal to others thatthe individual is not a threat to them, elicits empathy(Keltner & Harker, 1998; Stearns & Parrott, 2012) and min-imizes the risk of being shunned.
The Role of Self-Monitoring and Self-Criticism
Although research has clearly established that sociallyanxious individuals are highly self-critical (Cox, Fleet,& Stein, 2004; Cox et al., 2000), a more fine-grained un-derstanding regarding the role of self-criticism in socialanxiety is needed. We hypothesize that because inten-sive shame states from childhood are remembered ashighly aversive, individuals develop a self-monitoringand self-critical style as a safety strategy designed toconceal perceived deficiencies and prevent re-activationof highly aversive shame states. This view is consistentwith Gilbert and Irons (2005) who conceptualized self-criticism and self-blame as a defensive strategy de-signed to prevent subordinates from making assertivemoves that can further escalate conflicts and elicit fur-ther attack from a powerful dominant. In abusive con-texts, shame and self-criticism serve an adaptivefunction of submission and appeasement that elicit rec-onciliation and forgiveness (Keltner & Harker, 1998).Later on, self-criticism protects people from taking so-cial risks and thus prevents re-activation of full-blownshame episodes. For example, one socially anxious pa-tient experienced being ostracized by his peers in Ju-nior High. One of his strongest shame memoriesinvolved sitting in the school cafeteria for lunch andhis friends were leaving the table as a result. He feltshunned, rejected and humiliated. In the context of thisand other highly aversive shame memories, he devel-oped a strong inner critical voice that continued toput him down in order to prevent him from taking so-cial risks (e.g., ‘don’t take of your shirt because every-one will see that you are overweight and will laughat you’ or ‘you must over-prepare for your lecture to-morrow so that your students will not see that you re-ally don’t know what you’re talking about’). Suchinternal critical attacks function in a similar way tosafety behaviours because they prevent full exposurein social situations.Furthermore, socially anxious individuals are often crit-
ical of themselves following a social event. This phenom-ena is termed post-event processing or post-eventrumination by cognitively oriented social anxiety re-searchers (Brozovich & Heimberg, 2008), but a closer ex-amination of the content of post-event repetitivethoughts reveals that these are self-attacking thoughts
(‘why did you say this stupid thing?’). From psycho-evolutionary and emotion-focused perspectives, suchpost-event self-criticism is designed to reprimand the selffor risking exposing one’s flaws and prevent doing so inthe future.
The Current Study
Given this theoretical model, we hypothesized that ret-rospective reports of childhood emotional abuse andneglect will predict current symptoms of social anxietythrough an indirect effect composed of shame-proneness and self-criticism. Specifically, we hypothe-sized a three-path sequential process in whichretrospective reports of childhood emotional abuseand neglect predict current shame-proneness, which inturn predict current self-criticism, which then predictscurrent symptoms of social anxiety. Although a cross-sectional design has many limitations in testing amodel that integrates both developmental and mainte-nance processes that naturally unfold over time, we be-lieve it is a viable first step in this research direction.Previous studies using self-report assessments of vari-
ous forms of childhood maltreatment in SAD (mainlyusing the Childhood Trauma Questionnaire [CTQ]) havefound that emotional abuse and emotional neglect arethe type of maltreatments that tend to be most robust pre-dictors of SAD symptoms (Bruce et al., 2012; Kuo et al.,2011; Simon et al., 2009). Therefore, in the current study,we hypothesized a priory that these two forms of mal-treatment would predict social anxiety symptoms throughshame-proneness and self-criticism. We predicted thatboth emotional abuse and neglect will be associated withshame and self-criticism because both can be experiencedas shaming. Although parental emotional abuse involvesdirect shaming (e.g., parental criticism and insults), emo-tional neglect may be experienced as shaming in a less di-rect manner, as parental withholding of love and affectionmay lead children to experience being unwanted and, inturn, inadequate. In fact, Claesson and Sohlberg (2002)showed that recalling parents as ignoring had larger cor-relations with current shame-proneness compared withrecalling parents as blaming and attacking.
METHOD
Participants and Procedure
The sample consisted of 219 Israeli participants (109 malesand 110 females) from the general populationwhowere re-cruited via Midgam.com, an Israeli online survey platform.Participants were informed of their rights and completedan online informed consent form in accordance with
Shame and Self-Criticism in Social Anxiety
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

university Institutional Review Board standards.Theycompleted the survey in one session (the website allowsone entry per participant) and were reimbursed 20 NIS(around $5) for their time. It took about 15–20min tocomplete all questionnaires. Participants’ mean age was38.7 years (SD=13.1 years), and age ranged from 19 to64 years. Seventy-one (32%) were single, 115 (53%) weremarried, 32 (15%) were divorced and one participant wasa widow. The vast majority (90.4%) had finished at leasthigh school, and 73.1% of the sample had some posthigh-school education. One hundred and five (51.2%) ofthe participants reported having a lower than average in-come, and 100 participants reported having an averageor higher than average income. Fifteen participants (7%)indicated that they are unemployed.
Measures
Childhood MaltreatmentThe CTQ—Short Form (CTQ-SF; Bernstein et al., 2003)
was used to measure various forms of childhood mal-treatment. The CTQ-SF includes 28 items rated on afive-point scale, three of which are validity items, andthe remaining 25 items are grouped into five subscalesrepresenting different forms of maltreatment (sexualabuse, physical abuse, physical neglect, emotionalabuse and emotional neglect). After reversing the direc-tion of some of the items, each of the five individualsubscales can range between 5 and 25, and total scorescan range from 25 to 125 where higher scores indicatemore severe abuse. The CTQ-SF has very good psycho-metric properties in community samples (Bernsteinet al., 2003; Scher et al., 2001).
Shame-PronenessShame-proneness was measured with the shame sub-
scale of the short version of the Test of Self-ConsciousAffect-3 (TOSCA-3; Tangney, Dearing, Wagner, &Gramzow, 2000). The short version of the TOSCA-3 in-cludes 11 negative daily scenarios, and respondents areasked to evaluate the extent to which they might reactwith shame or guilt to each scenario (the originalTOSCA-3 contains additional items reflecting externaliz-ing and detachment that were not administered in thisstudy). Respondents are asked to use a five-point scaleranging from 1 (not likely) to 5 (likely) to indicate theprobability of responding with shame and guilt, such thateach scale can range from 11 to 55, with higher scoresreflecting greater propensity to experience these feelings.Several studies have successfully used the shorter versionof the TOSCA-3 while showing good psychometric prop-erties (Hasson-Ohayon et al., 2012; Rüsch et al., 2007;Woien, Ernst, Patock-Peckham, & Nagoshi, 2003).
Self-CriticismThe Inadequate Self (IS) Subscale from the Forms of Self-
Criticizing/Self-Reassuring Scale (FSCRS; Gilbert et al.,2004) was used to measure self-criticism. The FSCRS in-cludes 22 items measuring the extent to which individualsare either self-critical or self-reassuring when they experi-ence failure. In addition to the self-reassuring subscale,this instrument measures two types of self-criticism. TheIS Subscale measures a moderate level of self-criticismand a sense of inadequacy (‘There is a part of me that putsme down’ or ‘I remember and dwell on my failings’),whereas a second subscale, called ‘Hated-Self’, measuresa more destructive, severe, disgust-based self-criticism (‘Ihave become so angry with myself that I want to hurt orinjure myself’). The self-reassuring subscale measures thecapability to be self-supportive and self-reassuring. Re-spondents are given the following probe: ‘when thingsgo wrong for me…’ followed by 22 items rated on a five-point scale. In the current study, only the IS Scale wasused. It includes nine items, and scores can range from 0to 36, with higher scores indicating greater self-criticism.
Social Anxiety SymptomsThe Social Interaction Anxiety Scale (SIAS; Mattick &
Clarke, 1998) was used to measure severity of social anxi-ety symptoms. The SIAS is a widely used questionnairefocusing on anxiety levels during dyadic and group-basedsocial interactions. It includes 20 items rated on a five-point scale. Scores are summed and can range from 0 to80, with higher scores reflecting greater symptomatic se-verity. The SIAS has excellent psychometric properties(Mattick & Clarke, 1998; Heimberg et al., 1992).
Depressive SymptomsThe Depression Subscale of the Depression Anxiety
Stress Scale—21 item version (DASS-21; Antony et al.,1998; Henry & Crawford, 2005) was used to measure de-pressive symptoms. The DASS-21 is a psychometricallysound self-report assessing depressive, anxiety andstress-related symptoms over the past week. The Depres-sion Subscale measures dysphoric mood with seven itemsscored on a four-point scale (0 = ‘Did not apply to me atall’ to 3 = ‘Applied to me very much, or most of the time’).Scores on this subscale range from 0 to 21, with higherscores reflecting more depressive symptoms.
RESULTS
Approach to Data Analysis
To examine whether childhood emotional abuse andneglect predict social anxiety symptoms throughshame-proneness and self-criticism, we used a three-
B. Shahar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)
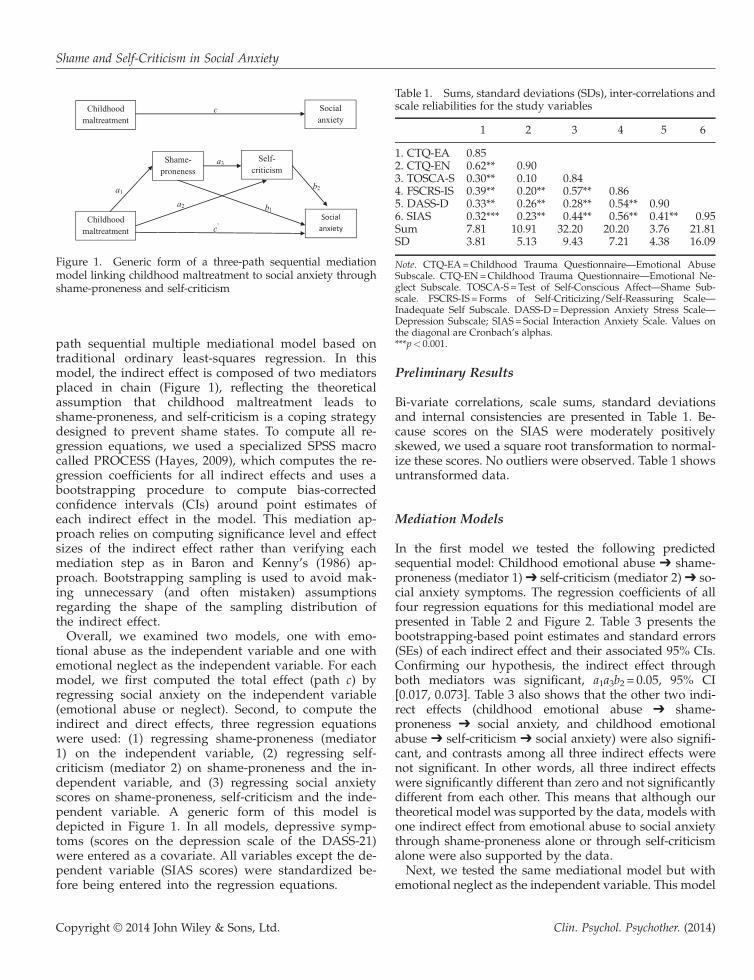
path sequential multiple mediational model based ontraditional ordinary least-squares regression. In thismodel, the indirect effect is composed of two mediatorsplaced in chain (Figure 1), reflecting the theoreticalassumption that childhood maltreatment leads toshame-proneness, and self-criticism is a coping strategydesigned to prevent shame states. To compute all re-gression equations, we used a specialized SPSS macrocalled PROCESS (Hayes, 2009), which computes the re-gression coefficients for all indirect effects and uses abootstrapping procedure to compute bias-correctedconfidence intervals (CIs) around point estimates ofeach indirect effect in the model. This mediation ap-proach relies on computing significance level and effectsizes of the indirect effect rather than verifying eachmediation step as in Baron and Kenny’s (1986) ap-proach. Bootstrapping sampling is used to avoid mak-ing unnecessary (and often mistaken) assumptionsregarding the shape of the sampling distribution ofthe indirect effect.Overall, we examined two models, one with emo-
tional abuse as the independent variable and one withemotional neglect as the independent variable. For eachmodel, we first computed the total effect (path c) byregressing social anxiety on the independent variable(emotional abuse or neglect). Second, to compute theindirect and direct effects, three regression equationswere used: (1) regressing shame-proneness (mediator1) on the independent variable, (2) regressing self-criticism (mediator 2) on shame-proneness and the in-dependent variable, and (3) regressing social anxietyscores on shame-proneness, self-criticism and the inde-pendent variable. A generic form of this model isdepicted in Figure 1. In all models, depressive symp-toms (scores on the depression scale of the DASS-21)were entered as a covariate. All variables except the de-pendent variable (SIAS scores) were standardized be-fore being entered into the regression equations.
Preliminary Results
Bi-variate correlations, scale sums, standard deviationsand internal consistencies are presented in Table 1. Be-cause scores on the SIAS were moderately positivelyskewed, we used a square root transformation to normal-ize these scores. No outliers were observed. Table 1 showsuntransformed data.
Mediation Models
In the first model we tested the following predictedsequential model: Childhood emotional abuse ➔ shame-proneness (mediator 1) ➔ self-criticism (mediator 2) ➔ so-cial anxiety symptoms. The regression coefficients of allfour regression equations for this mediational model arepresented in Table 2 and Figure 2. Table 3 presents thebootstrapping-based point estimates and standard errors(SEs) of each indirect effect and their associated 95% CIs.Confirming our hypothesis, the indirect effect throughboth mediators was significant, a1a3b2 = 0.05, 95% CI[0.017, 0.073]. Table 3 also shows that the other two indi-rect effects (childhood emotional abuse ➔ shame-proneness ➔ social anxiety, and childhood emotionalabuse ➔ self-criticism ➔ social anxiety) were also signifi-cant, and contrasts among all three indirect effects werenot significant. In other words, all three indirect effectswere significantly different than zero and not significantlydifferent from each other. This means that although ourtheoretical model was supported by the data, models withone indirect effect from emotional abuse to social anxietythrough shame-proneness alone or through self-criticismalone were also supported by the data.Next, we tested the same mediational model but with
emotional neglect as the independent variable. This model
Figure 1. Generic form of a three-path sequential mediationmodel linking childhood maltreatment to social anxiety throughshame-proneness and self-criticism
Table 1. Sums, standard deviations (SDs), inter-correlations andscale reliabilities for the study variables
1 2 3 4 5 6
1. CTQ-EA 0.852. CTQ-EN 0.62** 0.903. TOSCA-S 0.30** 0.10 0.844. FSCRS-IS 0.39** 0.20** 0.57** 0.865. DASS-D 0.33** 0.26** 0.28** 0.54** 0.906. SIAS 0.32*** 0.23** 0.44** 0.56** 0.41** 0.95Sum 7.81 10.91 32.20 20.20 3.76 21.81SD 3.81 5.13 9.43 7.21 4.38 16.09
Note. CTQ-EA=Childhood Trauma Questionnaire—Emotional AbuseSubscale. CTQ-EN=Childhood Trauma Questionnaire—Emotional Ne-glect Subscale. TOSCA-S=Test of Self-Conscious Affect—Shame Sub-scale. FSCRS-IS = Forms of Self-Criticizing/Self-Reassuring Scale—Inadequate Self Subscale. DASS-D=Depression Anxiety Stress Scale—Depression Subscale; SIAS= Social Interaction Anxiety Scale. Values onthe diagonal are Cronbach’s alphas.***p< 0.001.
Shame and Self-Criticism in Social Anxiety
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)
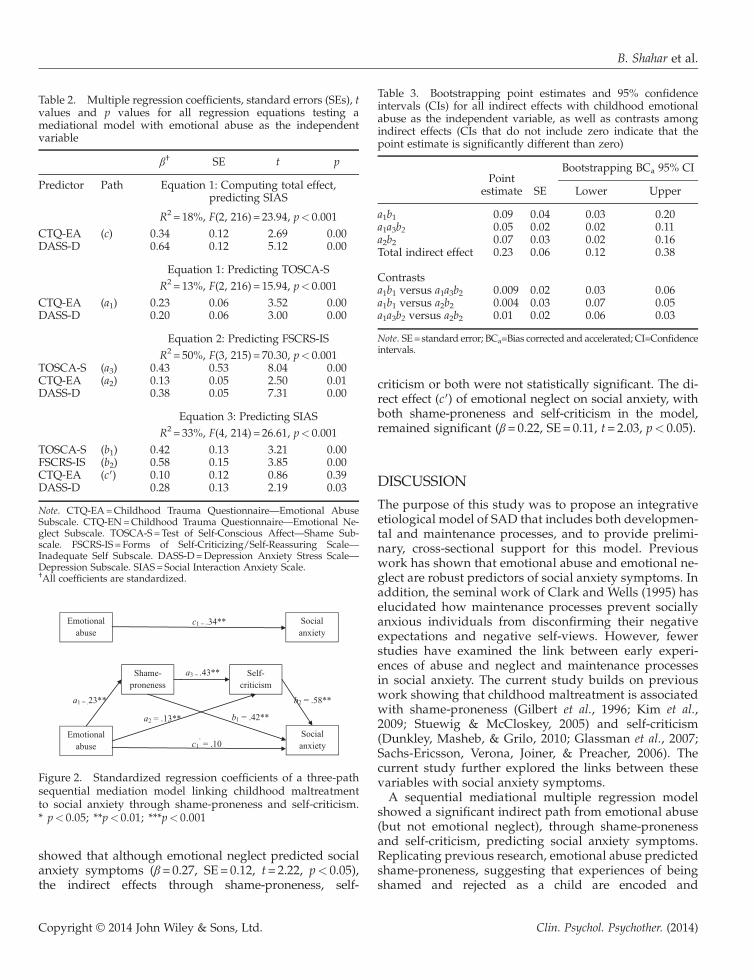
showed that although emotional neglect predicted socialanxiety symptoms (β = 0.27, SE = 0.12, t= 2.22, p< 0.05),the indirect effects through shame-proneness, self-
criticism or both were not statistically significant. The di-rect effect (c′) of emotional neglect on social anxiety, withboth shame-proneness and self-criticism in the model,remained significant (β = 0.22, SE= 0.11, t= 2.03, p< 0.05).
DISCUSSION
The purpose of this study was to propose an integrativeetiological model of SAD that includes both developmen-tal and maintenance processes, and to provide prelimi-nary, cross-sectional support for this model. Previouswork has shown that emotional abuse and emotional ne-glect are robust predictors of social anxiety symptoms. Inaddition, the seminal work of Clark and Wells (1995) haselucidated how maintenance processes prevent sociallyanxious individuals from disconfirming their negativeexpectations and negative self-views. However, fewerstudies have examined the link between early experi-ences of abuse and neglect and maintenance processesin social anxiety. The current study builds on previouswork showing that childhood maltreatment is associatedwith shame-proneness (Gilbert et al., 1996; Kim et al.,2009; Stuewig & McCloskey, 2005) and self-criticism(Dunkley, Masheb, & Grilo, 2010; Glassman et al., 2007;Sachs-Ericsson, Verona, Joiner, & Preacher, 2006). Thecurrent study further explored the links between thesevariables with social anxiety symptoms.A sequential mediational multiple regression model
showed a significant indirect path from emotional abuse(but not emotional neglect), through shame-pronenessand self-criticism, predicting social anxiety symptoms.Replicating previous research, emotional abuse predictedshame-proneness, suggesting that experiences of beingshamed and rejected as a child are encoded and
Figure 2. Standardized regression coefficients of a three-pathsequential mediation model linking childhood maltreatmentto social anxiety through shame-proneness and self-criticism.* p< 0.05; **p< 0.01; ***p< 0.001
Table 2. Multiple regression coefficients, standard errors (SEs), tvalues and p values for all regression equations testing amediational model with emotional abuse as the independentvariable
β† SE t p
Predictor Path Equation 1: Computing total effect,predicting SIAS
R2 = 18%, F(2, 216) = 23.94, p< 0.001CTQ-EA (c) 0.34 0.12 2.69 0.00DASS-D 0.64 0.12 5.12 0.00
Equation 1: Predicting TOSCA-SR2 = 13%, F(2, 216) = 15.94, p< 0.001
CTQ-EA (a1) 0.23 0.06 3.52 0.000.20 0.06 3.00 0.00DASS-D
Equation 2: Predicting FSCRS-ISR2 = 50%, F(3, 215) = 70.30, p< 0.001
TOSCA-S (a3) 0.43 0.53 8.04 0.00CTQ-EA (a2) 0.13 0.05 2.50 0.01DASS-D 0.38 0.05 7.31 0.00
Equation 3: Predicting SIASR2 = 33%, F(4, 214) = 26.61, p< 0.001
TOSCA-S (b1) 0.42 0.13 3.21 0.00FSCRS-IS (b2) 0.58 0.15 3.85 0.00CTQ-EA (c′) 0.10 0.12 0.86 0.39DASS-D 0.28 0.13 2.19 0.03
Note. CTQ-EA=Childhood Trauma Questionnaire—Emotional AbuseSubscale. CTQ-EN=Childhood Trauma Questionnaire—Emotional Ne-glect Subscale. TOSCA-S=Test of Self-Conscious Affect—Shame Sub-scale. FSCRS-IS = Forms of Self-Criticizing/Self-Reassuring Scale—Inadequate Self Subscale. DASS-D=Depression Anxiety Stress Scale—Depression Subscale. SIAS= Social Interaction Anxiety Scale.†All coefficients are standardized.
Table 3. Bootstrapping point estimates and 95% confidenceintervals (CIs) for all indirect effects with childhood emotionalabuse as the independent variable, as well as contrasts amongindirect effects (CIs that do not include zero indicate that thepoint estimate is significantly different than zero)
Pointestimate SE
Bootstrapping BCa 95% CI
Lower Upper
a1b1 0.09 0.04 0.03 0.20a1a3b2 0.05 0.02 0.02 0.11a2b2 0.07 0.03 0.02 0.16Total indirect effect 0.23 0.06 0.12 0.38
Contrastsa1b1 versus a1a3b2 0.009 0.02 �0.03 0.06a1b1 versus a2b2 �0.004 0.03 �0.07 0.05a1a3b2 versus a2b2 �0.01 0.02 �0.06 0.03
Note. SE=standard error; BCa=Bias corrected and accelerated; CI=Confidenceintervals.
B. Shahar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

remembered as strong emotional memories affecting cur-rent self-views (Mikulincer & Shaver, 2004). These resultsfurther corroborate findings showing that shame memo-ries can have the properties of traumatic memories andbecome central in one’s life narrative and identity (Matos& Pinto-Gouveia, 2010; Pinto-Gouveia & Matos, 2011).The path from emotional abuse, through shame-proneness, predicting self-criticism, is consistent withthe theoretical notion that self-criticism functions as aprotective strategy against more painful shame states. In-dividuals with social anxiety are self-critical and often sethigh, perfectionistic standards for themselves (Frost,Glossner, & Maxner, 2010), and this can be understoodas a coping process against the risk of being exposed asflawed. It is important to note that the indirect effect be-tween emotional abuse and SAD through shame-proneness alone and through self-criticism alone was alsosignificant. However, given our priory, theory-driven hy-potheses regarding the importance of both shame and self-criticism, we believe it is important to continue to empha-size and research both processes as maintainingprocesses.Consistent with previous research, retrospective recall
of emotional neglect predicted social anxiety symptoms.Contrary to our prediction, however, emotional neglectdid not predict shame-proneness and self-criticism. Onepossible explanation for this finding is that emotionalabuse, compared with neglect, is more directly related toexperiences of subordination and shame. Emotionalabuse was defined by the developers of the CTQ as ‘ver-bal assaults on a child’s sense of worth or well-being, orany humiliating or demeaning behaviour directed to-wards a child by an adult or older person’ (Bernsteinet al., 2003, p. 175). Emotional abuse, then, refers to re-peated shaming attacks that can directly contribute tothe development of shame-based schemata. Similarly,Rose and Abramson (1992) argued that when parentalabuse is verbal (as in emotional abuse), children are morelikely to develop negative self-schemata because theshaming messages are directly supplied by the parents.In contrast, emotional neglect was defined as ‘the failureof caretakers to meet children’s basic emotional and psy-chological needs, including love, belonging, nurturance,and support’ (p. 175). Emotional neglect may only indi-rectly provoke shame, in cases where children blamethemselves for caretakers’ neglect. Therefore, the associa-tion between emotional neglect and shame and self-criticismmay be less robust andmay not be revealed withexplicit self-reports or in nonclinical samples.
Treatment Implications
The results of this study suggest that shame and self-criticism may be important therapeutic targets in the
treatment for social anxiety. Therapeutic principles ad-dressing these processes may enhance existingcognitive–behavioural therapies or may be used inother treatment development efforts. For example,Shahar et al. (2012) showed that a brief course ofemotion-focused therapy based on the two-chair dia-logue intervention was useful in reducing self-criticism,increasing self-compassion, and reducing anxiety anddepressive symptoms among highly self-critical pa-tients. One of the primary goals in this approach is toaccess, evoke and restructure maladaptive shame-basedschemata that result from earlier abuse experiences.Such therapeutic strategy can be incorporated as amodule in CBT, especially for socially anxious patientswith particularly high levels of self-criticism andperfectionism.Other emotion-focused principles and techniques may
be useful in working with socially anxious individuals.For example, socially anxious individuals with abusehistories usually hold unresolved feelings towards theindividuals who injured them (significant others orpeers). As previously mentioned, shame-based sche-mata have largely developed in the context of suchabuse experiences. Imaginary confrontations withshaming attachment figures or peers using an emptychair dialogue task (Paivio & Pascual-Leone, 2010) canhelp patients access adaptive anger and sadness thathelp to restructure and transform shame (Paivio &Greenberg, 1995).The notion that shame and self-criticism play an im-
portant role in social anxiety should also guidecognitive–behavioural therapists in constructing specifi-cally tailored exposure-based interventions. Consistentwith Moscovitch (2009), we believe that exposure pro-cedures should focus on helping socially anxious pa-tients to gradually reveal their most authentic aspectsof themselves rather than focus on reducing anxiety insocial situations. Although this distinction seemssubtle, we agree with Moscovitch that it is quite impor-tant. If the most feared stimulus in social anxiety is acertain self-aspect that the patient is afraid to reveal,exposure should be specifically focused on revealingthis self-aspect in order to fully activate the most rele-vant fear structure (Foa, Huppert, & Cahill, 2006) orperhaps more relevant in the case of social anxiety,shame structure.
Limitations and Future Directions
The current study contains all the limitations inherentin a cross-sectional design based on self-report ques-tionnaires. These limitations are particularly problem-atic when attempting to examine developmentalhypotheses, as causal and temporal links cannot be
Shame and Self-Criticism in Social Anxiety
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

made. For example, individuals who are shame-proneand self-critical may be biassed towards recalling moreabuse experiences (Widom, Raphael, & DuMont, 2004).Future studies should further examine the propositionsmade in this paper using a variety of research method-ologies. For example, the association we found betweenshame-proneness and self-criticism is not sufficient toclaim that self-criticism serves as a defensive strategyagainst shame experiences. This claim needs to be spe-cifically examined using appropriate experimental de-signs that include shame induction procedures. Suchexperimental studies should be able to show that self-criticism actually reduce the intensity of shame. In ad-dition, it is important to examine whether the findingsof the current study are replicated in a clinical sample.The clinical implications discussed above are relevantonly to the extent to which the model we described inthis paper applies to a clinical population. Finally, fu-ture studies should assess whether the mediationalmodel proposed in the current study is equally relevantin different subtypes of SAD (generalized versus spe-cific) and different social situations (interaction versusperformance). One might assume that this modelwould be more pertinent in the generalized typebecause emotional abuse plays a more significant rolein that subtype.
CONCLUSIONS
In conclusion, shame and self-criticism seem to play animportant role in SAD, especially in the context ofabuse histories. Previous studies showed a robust linkbetween emotional abuse and social anxiety. The resultsof the present study imply that this link is mediatedthrough shame-proneness and self-criticism. Targetingshame and self-criticism in this population mayimprove treatment outcomes.
REFERENCESAderka, I. M., Weisman, O., Shahar, G., & Gilboa-Schechtman,
E. (2009). The roles of the social rank and attachment sys-tems in social anxiety. Personality and Individual Differences,47(4), 284-288. doi:10.1016/j.paid.2009.03.014
Andrews, B. (1998). Shame and childhood abuse. In P. Gilbert&B. Andrews (Ed.), Shame: Interpersonal behavior,psychopathology, and culture. Series in affective science (pp.176–190). New York, NY, US: Oxford University Press.
Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson,R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales inclinical groups and a community sample. PsychologicalAssessment, 10(2), 176–181. doi:10.1037/1040-3590.10.2.176
Arrindell, W. A., Emmelkamp, P. M., Monsma, A., & Brilman,E. (1983). The role of perceived parental rearing practices in
the aetiology of phobic disorders: A controlled study. TheBritish Journal of Psychiatry, 143, 183–187. doi:10.1192/bjp.143.2.183
Arrindell, W. A., Kwee, M. G., Methorst, G. J., Van der Ende,J., & Moritz, B. J. (1989). Perceived parental rearing styles ofagoraphobic and socially phobic in-patients. The BritishJournal of Psychiatry, 155, 526–535. doi:10.1192/bjp.155.4.526
Bandelow, B., Torrente, A. C., Wedekind, D., Broocks, A.,Hajak, G., & Rüther, E. (2004). Early traumatic life events,parental rearing styles, family history of mental disorders, andbirth risk factors in patients with social anxiety disorder.European Archives of Psychiatry and Clinical Neuroscience, 254(6),397–405. doi:10.1007/s00406-004-0521-2
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediatorvariable distinction in social psychological research:Conceptual, strategic, and statistical considerations. Journal ofPersonality and Social Psychology, 51(6), 1173–1182.doi:10.1037/0022-3514.51.6.1173
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge,D., Ahluvalia, T., . . . Zule, W. (2003). Development andvalidation of a brief screening version of the childhood traumaquestionnaire. Child Abuse & Neglect, 27(2), 169–190.doi:10.1016/S0145-2134(02)00541-0
Brozovich, F., & Heimberg, R. G. (2008). An analysis of post-event processing in social anxiety disorder. Clinical PsychologyReview, 28(6), 891–903. doi: 10.1016/j.cpr.2008.01.002
Bruce, L. C., Heimberg, R. G., Blanco, C., Schneier, F. R., &Liebowitz, M. R. (2012). Childhood maltreatment and socialanxiety disorder: Implications for symptom severity and re-sponse to pharmacotherapy. Depression and Anxiety, 29(2),131-138. doi:10.1002/da.20909
Claesson, K., & Sohlberg, S. (2002). Internalized shame and earlyinteractions characterized by indifference, abandonment andrejection: Replicated findings. Clinical Psychology & Psychother-apy, 9(4), 277–284. doi: 10.1002/cpp.331
Clark, D. M. & Wells, A. (1995). A cognitive model of social pho-bia. In R. Heimberg, M. Liebowitz, D. A. Hope & F. R. Schneier(Eds.), Social phobia: Diagnosis, assessment and treatment.(pp. 69–93). New York: Guilford Press.
Cox, B. J., Fleet, C., & Stein, M. B. (2004). Self-criticism andsocial phobia in the US national comorbidity survey. Journalof Affective Disorders, 82(2), 227–234. doi:10.1016/j.jad.2003.12.012
Cox, B. J., Rector, N. A., Bagby, R. M., Swinson, R. P., Levitt,A. J., & Joffe, R. T. (2000). Is self-criticism unique for de-pression? A comparison with social phobia. Journal of Affec-tive Disorders, 57(1-3), 223–228. doi:10.1016/S0165-0327(99)00043-9
Dunkley, D. M., Masheb, R. M., & Grilo, C. M. (2010). Childhoodmaltreatment, depressive symptoms, and body dissatisfactionin patients with binge eating disorder: The mediating role ofself-criticism. International Journal of Eating Disorders, 43(3),274–281.
Fergus, T. A., Valentiner, D. P., McGrath, P. B., & Jencius, S.(2010). Shame- and guilt-proneness: Relationships with anx-iety disorder symptoms in a clinical sample. Journal ofAnxiety Disorders, 24(8), 811–815. doi:10.1016/j.janxdis.2010.06.002
Fessler, D. M. T. (2007). From appeasement to conformity:Evolutionary and cultural perspectives on shame,competition, and cooperation. In J. L. Tracy, R. W. Robins & J.P. Tangney (Eds.), The self-conscious emotions: Theory andresearch (pp. 174–193). New York, NY: Guilford Press.
B. Shahar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)
Foa, E. B., Huppert, J. D., & Cahill, S. P. (2006). Emotional processingtheory: An update. In B. O. Rothbaum (Ed.), Pathological anxiety:Emotional processing in etiology and treatment. (pp. 3-24). NewYork, NY, US: Guilford Press.
Frost, R. O., Glossner, K., & Maxner, S. (2010). Social anxiety dis-order and its relationship to perfectionism. In S. G. Hofmann &P. M. DiBartolo (Eds.), Social anxiety: Clinical, developmental,and social perspectives (2nd ed.) (pp. 119–145). San Diego, CA,US: Elsevier Academic Press. doi:10.1016/B978-0-12-375096-9.00005-5
Gilbert, P. (2000). The relationship of shame, social anxiety anddepression: The role of the evaluation of social rank. ClinicalPsychology & Psychotherapy, 7(3), 174–189. doi:10.1002/1099-0879(200007)7:3<174::AID-CPP236>3.0.CO;2-U
Gilbert, P. (1998). What is shame? Some core issues and contro-versies. In P. Gilbert & B. Andrews (Ed.), Shame: Interper-sonal behavior, psychopathology, and culture. Series inaffective science (pp. 3–38). New York, NY, US: Oxford Uni-versity Press.
Gilbert, P., Allan, S., & Goss, K. (1996). Parental representations,shame, interpersonal problems, and vulnerability topsychopathology. Clinical Psychology & Psychotherapy, 3(1),23–34. doi:10.1002/(SICI)1099-0879(199603)3:1<23::AID-CPP66>3.0.CO;2-O
Gilbert, P., Clarke, M., Hempel, S., Miles, J. N. V., & Irons, C.(2004). Criticizing and reassuring oneself: An exploration offorms, styles and reasons in female students. British Journal ofClinical Psychology, 43(1), 31–50. doi:10.1348/014466504772812959
Gilbert, P., & Irons, C. (2005). Focused therapies and compassion-ate mind training for shame and self-attacking. In P. Gilbert(Ed.), Compassion: Conceptualisations, research and use inpsychotherapy (pp. 263–325). New York, NY, US: Routledge.
Gilbert, P., & Trower, P. (2001). Evolution and process in socialanxiety. In W. R. Crozier & L. E. Alden (Eds.), Internationalhandbook of social anxiety: Concepts, research and interven-tions relating to the self and shyness. (pp. 259–279). New York,NY, US: John Wiley & Sons Ltd.
Glassman, L. H., Weierich, M. R., Hooley, J. M., Deliberto, T. L., &Nock, M. K. (2007). Child maltreatment, non-suicidal self-injury, and the mediating role of self-criticism. Behaviour Re-search and Therapy, 45(10), 2483–2490. doi:10.1016/j.brat.2007.04.002
Hasson-Ohayon, I., Ehrlich-Ben Or, S., Vahab, K., Amiaz, A.,Weiser, M., & Roe, D. (2012). Insight into mental illness andself-stigma: The mediating role of shame proneness. PsychiatryResearch, 200, 802–806.
Hayes, A. F. (2009). Beyond Baron and Kenny: Statistical media-tion analysis in the new millennium. Communication Mono-graphs, 76(4), 408–420. doi:10.1080/03637750903310360
Heimberg, R. G., Mueller, G. P., Holt, C. S., Hope, D. A., &Liebowitz, M. R. (1992). Assessment of anxiety in social inter-action and being observed by others: The social interactionanxiety scale and the social phobia scale. Behavior Therapy, 23(1),53–73. doi:10.1016/S0005-7894(05)80308-9
Henry, J. D., & Crawford, J. R. (2005). The short-form version ofthe Depression Anxiety Stress Scales (DASS-21): Construct va-lidity and normative data in a large non-clinical sample. BritishJournal of Clinical Psychology, 44(2), 227–239. doi:10.1348/014466505X29657
Higgins, E. T. (1987). Self-discrepancy: A theory relating self andaffect. Psychological Review, 94(3), 319–340. doi:10.1037/0033-295X.94.3.319
Hofmann, S. G. (2007). Cognitive factors that maintain social anx-iety disorder: A comprehensive model and its treatment impli-cations. Cognitive Behaviour Therapy, 36(4), 193–209.doi:10.1080/16506070701421313
Johnson, S. L., Leedom, L. J., & Muhtadie, L. (2012). The domi-nance behavioral system and psychopathology: Evidence fromself-report, observational, and biological studies. PsychologicalBulletin, 138(4), 692–743. doi:10.1037/a0027503
Keltner, D., & Harker, L. (1998). The forms and functions of thenonverbal signal of shame. In P. Gilbert, & B. Andrews(Eds.), Shame: Interpersonal behavior, psychopathology, andculture. Series in affective science (pp. 78-98). New York, NY,US: Oxford University Press.
Kim, J., Talbot, N. L., & Cicchetti, D. (2009). Childhood abuseand current interpersonal conflict: The role of shame. ChildAbuse & Neglect, 33(6), 362–371. doi:10.1016/j.chiabu.2008.10.003
Knappe, S., Beesdo-Baum, K., Fehm, L., Lieb, R., & Wittchen, H.(2012). Characterizing the association between parenting andadolescent social phobia. Journal of Anxiety Disorders, 26(5),608-616. doi:10.1016/j.janxdis.2012.02.014
Kohut, H. (1971). The analysis of the self: A systematic approachto the psychoanalytic treatment of narcissistic personality dis-orders. Chicago, IL, US: University of Chicago Press.
Kuo, J. R., Goldin, P. R., Werner, K., Heimberg, R. G., & Gross,J. J. (2011). Childhood trauma and current psychologicalfunctioning in adults with social anxiety disorder. Journal ofAnxiety Disorders, 25(4), 467-473. doi:10.1016/j.janxdis.2010.11.011
Lewis, H. B. (1971). Shame and guilt in neurosis. PsychoanalyticReview, 58(3), 419–438.
Matos, M., & Pinto-Gouveia, J. (2010). Shame as a traumaticmemory. Clinical Psychology & Psychotherapy, 17(4), 299-312.
Matos, M., Pinto-Gouveia, J., & Gilbert, P. (2013). The effect ofshame and shame memories on paranoid ideation and socialanxiety. Clinical Psychology & Psychotherapy, 20(4), 334–349.doi:10.1002/cpp.1766
Mattick, R. P., & Clarke, J. C. (1998). Development and validationof measures of social phobia scrutiny fear and social interac-tion anxiety. Behaviour Research and Therapy, 36(4), 455-470.doi:10.1016/S0005-7967(97)10031-6
Mikulincer, M., & Shaver, P. R. (2004). Security-based self-representations in adulthood: Contents and processes. In W.S. Rholes &J. A. Simpson (Eds.), Adult attachment: Theory, re-search, and clinical implications. (pp. 159–195). New York, NY,US: Guilford Publications.
Morrison, A. P. (2011). The psychodynamics of shame. In R. L.Dearing & J. P. Tangney (Ed.), Shame in therapy hour (pp.23–43). Washington, DC, US: American Psychological Associa-tion. doi:10.1037/12326-001
Moscovitch, D. A. (2009). What is the core fear in social phobia?A new model to facilitate individualized case conceptualiza-tion and treatment. Cognitive and Behavioral Practice, 16(2),123–134. doi:10.1016/j.cbpra.2008.04.002
Paivio, S. C., & Greenberg, L. S. (1995). Resolving “unfinishedbusiness”: Efficacy of experiential therapy using empty-chairdialogue. Journal of Consulting and Clinical Psychology, 63(3),419–425. doi:10.1037/0022-006X.63.3.419
Paivio, S. C., & Pascual-Leone, A. (2010). Emotion-focused therapyfor complex trauma: An integrative approach. Washington, DC,US: American Psychological Association. doi:10.1037/12077-000
Pinto-Gouveia, J., & Matos, M. (2011). Can shame memoriesbecome a key to identity? The centrality of shame memories
Shame and Self-Criticism in Social Anxiety
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

predicts psychopathology. Applied Cognitive Psychology, 25(2),281–290. doi:10.1002/acp.1689
Rose, D. T., & Abramson, L. Y. (1992). Developmental predictorsof depressive cognitive style: Research and theory. In D.Cicchetti & S. L. Toth (Eds.), Developmental perspectives ondepression. Rochester symposium on developmentalpsychopathology, vol. 4. (pp. 323–349). Rochester, NY, US:University of Rochester Press.
Rüsch, N., Corrigan, P. W., Bohus, M., Jacob, G. A., Brueck, R., &Lieb, K. (2007). Measuring shame and guilt by self-report ques-tionnaires: A validation study. Psychiatry Research, 150(3), 313–325. doi:10.1016/j.psychres.2006.04.018
Sachs-Ericsson, N., Verona, E., Joiner, T., & Preacher, K. J. (2006).Parental verbal abuse and the mediating role of self-criticismin adult internalizing disorders. Journal of Affective Disorders,93(1-3), 71–78. doi:10.1016/j.jad.2006.02.014
Scher, C. D., Stein, M. B., Asmundson, G. J. G., McCreary, D. R., &Forde, D. R. (2001). The childhood trauma questionnaire in acommunity sample: Psychometric properties and normativedata. Journal of Traumatic Stress, 14(4), 843–857. doi:10.1023/A:1013058625719
Shahar, B., Carlin, E. R., Engle, D. E., Hegde, J., Szepsenwol,O., & Arkowitz, H. (2012). A pilot investigation of emotion-focused two-chair dialogue intervention for self-criticism.Clinical Psychology & Psychotherapy, 19(6), 496–507.doi:10.1002/cpp.762
Simon, N. M., Herlands, N. N., Marks, E. H., Mancini, C.,Letamendi, A., Li, Z., . . . Stein, M. B. (2009). Childhoodmaltreatment linked to greater severity and poorer qualityof life and function in social anxiety disorder. Depressionand Anxiety, 26(11), 1027–1032. doi:10.1002/da.20604
Stearns, D. C., & Parrott, W. G. (2012). When feeling bad makesyou look good: Guilt, shame, and person perception. Cognitionand Emotion, 26(3), 407–430. doi:10.1080/02699931.2012.675879
Stuewig, J., & McCloskey, L. A. (2005). The relation of childmaltreatment to shame and guilt among adolescents:
Psychological routes to depression and delinquency. ChildMaltreatment, 10(4), 324–336. doi:10.1177/1077559505279308
Tangney, J. P., & Dearing, R. L. (2002). Shame and guilt. NewYork, NY, US: Guilford Press.
Tangney, J. P., Dearing, R., Wagner, P., Gramzow, R. (2000) TheTest of Self-Conscious Affect (TOSCA-3). Fairfax (VA): GeorgeMason University.
Tangney, J. P., Wagner, P. E., Hill-Barlow, D., Marschall, D. E., &Gramzow, R. (1996). Relation of shame and guilt to construc-tive versus destructive responses to anger across the lifespan.Journal of Personality and Social Psychology, 70(4), 797–809.doi:10.1037/0022-3514.70.4.797
Trower, P., & Gilbert, P. (1989). New theoretical conceptions of so-cial anxiety and social phobia. Clinical Psychology Review, 9(1),19–35. doi:10.1016/0272-7358(89)90044-5
Weeks, J. W., Heimberg, R. G., & Heuer, R. (2011). Exploring therole of behavioral submissiveness in social anxiety. Journal ofSocial and Clinical Psychology, 30(3), 217–249. doi:10.1521/jscp.2011.30.3.217
Weisman, O., Aderka, I. M., Marom, S., Hermesh, H., & Gilboa-Schechtman, E. (2011). Social rank and affiliation in social anx-iety disorder. Behaviour Research and Therapy, 49(6-7), 399–405.doi:10.1016/j.brat.2011.03.010
Widom, C. S., Raphael, K. G., & DuMont, K. A. (2004). The casefor prospective longitudinal studies in child maltreatment re-search: Commentary on Dube, Williamson, Thompson, Felitti,and Anda (2004). Child Abuse & Neglect, 28(7), 715–722.doi:10.1016/j.chiabu.2004.03.009
Woien, S. L., Ernst, H. A. H., Patock-Peckham, J., & Nagoshi, C. T.(2003). Validation of the TOSCA to measure shame and guilt.Personality and Individual Differences, 35(2), 313–326.doi:10.1016/S0191-8869(02)00191-5
Zimmerman, J., Morrison, A. S. and Heimberg, R. G. (2014),Social anxiety, submissiveness, and shame in men and women:A moderated mediation analysis. British Journal of ClinicalPsychology. doi: 10.1111/bjc.12057
B. Shahar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)