Embed Size (px)
DESCRIPTION
A Journal for Physicians
Citation preview
A JOURNAL FOR PHYSICIANS
TREATMENT PROTOCOLS
P. 4
PEDIATRIC CT SCANS
P. 8
MRSA CAUSES, TREATMENTS
P. 10
EZ-IO DEVICE
P. 12
NEURODEVELOPMENTAL FOLLOW-UP
P. 14
EOSINOPHILIC ESOPHAGITIS
P. 16
ISSUE 1, 2009
Proudly serving children since 1948, Children’s Hospital & Medical Center is the only full-service, pediatric health care center in Nebraska. Located in Omaha, it provides expertise in more than 30 pediatric specialty services to children and families across a five-state region and beyond. The 144-bed, nonprofit hospital houses the only dedicated pediatric emergency department in the region and offers 24-hour, in-house services by pediatric critical care specialists. Children’s Hospital & Medical Center has achieved the Magnet designation for nursing excellence and is an InfoWorld 100 award winner for innovation in information technology. A pediatric affiliation established between Children’s Hospital & Medical Center and the University of Nebraska Medical Center College of Medicine supports enhancements in pediatric education, research and clinical care. Children’s is also the primary teaching site for the family practice and joint pediatric residency programs at Creighton University and UNMC. For more information on Children’s Hospital & Medical Center go to ChildrensOmaha.org.
TREATMENT PROTOCOLS
P. 4
As part of the Children’s Oncology Group, Minnie Abromowitch, M.D. helps develop protocols that spell out standard treatments to improve outcomes for pediatric patients regardless of where in the world they are.
PEDIATRIC CT SCANS
P. 8
Pediatric radiologists at Children’s tailor radiation to the pediatric patient during CT scans while still obtaining the desired images.
MRSA CAUSES, TREATMENTS
P. 10
Clinical research is underway at Children’s to study causes and treatments of CA MRSA infections.
EZ-IO DEVICE
P. 12
Children’s has added the EZ-IO intraosseous infusion system to its arsenal of life-saving tools.
NEURODEVELOPMENTAL FOLLOW-UP
P. 14
TIPS, a comprehensive neurodevelopmental follow-up program, tracks the progress of children who have spent time in the NICU.
EOSINOPHILIC ESOPHAGITIS
P. 16
Based on research being conducted in the Food Hypersensitivity Clinic at Children’s, Eosinophilic Esophagitis (EE) is now identified as a fifth major allergic disease.
CONTENTS
BRIEFLY NOTED
P. 7
NEW PHYSICIANS
P. 18
NEW PEDIATRIC RESOURCE DIRECTORY
P. 18
QUICK REFERENCE DIRECTORY
P. 19
ALSO:
CHILDREN’S CONNECTION ADVISORY COUNCIL
SHAHAB F. ABDESSALAM, M.D.DAVID M. CHRISTENSEN, M.D.BRADY A. KERR, M.D.JOHN D. KUGLER, M.D.JOSEPH T. (JAY) SNOW, M.D.JAYESH C. THAKKER, M.D.PEGGY HOGAN, R.N., PHYSICIAN LIAISON
TREATMENT PROTOCOLS BENEFIT CANCER PATIENTS WORLDWIDE
TREATMENT PROTOCOLS
P. 4

From her desk in the Hematology/Oncology Clinic offices at Children’s Hospital & Medical Center, pediatric oncologist Minnie Abromowitch, M.D., helps develop and administer treatment protocols that impact the care – and the lives – of young cancer patients around the world.
The first protocol she developed as part of the Children’s Oncology Group for the treatment of pediatric lymphoblastic lymphoma was published in the October 2008 issue of the British Journal of
Haematology. The report detailed the results of a pilot study to estimate the feasibility, toxicity and efficacy of a 12-month aggressive multi-agent chemotherapy regimen in children and adolescents with advanced lymphoblastic lymphoma (LL).
Dr. Abromowitch presented the second protocol at the American Society of Hematology in December.
“The second protocol incorporates the results of a five-year study based on a treatment developed in Germany and has become the mainstay for treatment around the world,” she says. “About 85 percent of children and adolescents with lymphoblastic lymphoma are cured with this treatment.
“The next protocol we are working on,” she says, “will incorporate information we have learned about the importance of rate of response and highly sophisticated techniques of measuring minimal residual disease to further improve outcomes.”
The Children’s Oncology Group (COG) is the world’s largest cooperative cancer research organization. Its mission is “to cure and prevent childhood and adolescent cancer through scientific discovery and compassionate care.” COG draws together experts in pediatric cancer from around the world. Children’s Hospital & Medical Center is a member.
“Treatment protocols allow patients to be treated in the same fashion no matter where
they are,” Dr. Abromowitch says. “They are written by experts in the field, and while the treatments are usually variations of standard treatments, there is considerable time, effort and resources put into their refinement. That’s reflected in the results.”
Dr. Abromowitch, who earned her medical degree from the University of Manitoba, has spent half her life conducting research and treating childhood leukemias and lymphomas.
She completed her pediatric residency at the Hospital for Sick Children in Toronto and was chief resident at Winnipeg Children’s Hospital. She served fellowships in pediatric hematology/oncology in Winnipeg, and in hematology/oncology at St. Jude Children’s Research Hospital in Memphis, Tenn.
Dr. Abromowitch is board certified in pediatrics and in pediatric hematology/oncology. She moved to Nebraska in 1991.
In addition to her duties as medical director of the Hematology/Oncology Clinic at Children’s, she is an associate professor in the Section
ABOUT 85 PERCENT OF CHILDREN AND ADOLESCENTS WITH LYMPHOBLASTIC LYMPHOMA ARE CURED WITH THIS TREATMENT.
MINNIE ABROMOWITCH, M.D.MEDICAL DIRECTORHEMATOLOGY/ONCOLOGY CLINICCHILDREN’S HOSPITAL & MEDICAL CENTER
P. 5
PHYSICIAN’S PRIORITY HOTLINE 1.888.592.7955

of Hematology/Oncology at the University of Nebraska Medical Center and a member of the pediatric bone marrow transplant team at The Nebraska Medical Center. She has served as chair in several clinical research studies.
“And I do it all out of this office,” she says.
Indeed, the intense nature of Dr. Abromowitch’s practice at Children’s – coupled with the pressure of continuing research – requires significant personal commitment and dedication.
“This is obviously something I’m passionate about,” she says. “My motivation has been a devotion to changing the lives of these children. The majority of children diagnosed
with cancer will be cured and grow up to be healthy adults.
“It hasn’t always been that way. The paradigm is not comparing it to adult cancer. It’s very different.”
She says that when she began her fellowship in 1980, the cure rate for childhood leukemia was 50 percent. “It’s 85 percent today. And with Burkitt’s Lymphoma, it’s gone from 20 percent up to 90 percent.”
Improvements come from finding not only the right drugs but the right combination of drugs that display the greatest success targeting particular varieties of cancers.
“We’re always asking questions,” she says, “and we’re making progress.”
“We are fortunate to have several nationally known experts here,” she says, “involved in national and international research ventures. They are instrumental in developing therapies used everywhere.”
The dedication of the entire clinic staff pays off.
“In general, if we took the next 100 kids who walked into this clinic,” she says, “we could
look forward to 80 percent being cured. That’s where we are today.”
Two of Dr. Abromowitch’s patients, brothers 10-year-old Connor and 6-year-old Caden Ballard, were diagnosed with acute lymphoblastic leukemia. After undergoing intensive chemotherapy, Dr. Abromowitch expects both boys to live normal, healthy lives. The boys were recently featured in a series of advertisements for Children’s with the title, “They beat cancer, two to nothing.”
And while not all outcomes are as successful as with the Ballard brothers, Dr. Abromowitch says the rewards outweigh the losses.
“It has given me a lot of satisfaction,” she says. “At the end of the day, I feel like I’ve done something worthwhile. This is one of the few areas in pediatrics where you can measure and document major, major gains.
“Others manage disease. We cure patients.”
“IN GENERAL, IF WE TOOK THE NEXT
100 KIDS WHO WALKED INTO THIS
CLINIC, WE COULD LOOK FORWARD
TO 80 PERCENT BEING CURED.”
MINNIE ABROMOWITCH, M.D.MEDICAL DIRECTORHEMATOLOGY/ONCOLOGY CLINICCHILDREN’S HOSPITAL & MEDICAL CENTER
CURE RATES
➜ Child Leukemia
1980 2009 1980 2009
➜ Burkitt’s Lymphoma
50%
85%
20%
90%
P. 6
BRIEFLY NOTED
WEST VILLAGE POINTE SPECIALTY PEDIATRIC CENTER
COMPUTERIZED ORDER ENTRY IMPROVES SAFETY
Children’s Hospital & Medical Center opened a satellite campus at West Village Pointe in April. The office address is 110 N. 175th St., at 175th & Burke Streets, just south of West Dodge Road. The Indian Hills Children’s Physicians office relocated to this location in March, and the Eagle Run Urgent Care Clinic relocated in April.
Children’s Rehab Services opened a second location at West Village Pointe in May, followed by laboratory specimen collection and Radiology. Additional clinical services are being evaluated for the West Village Pointe location.
Construction of the Specialty Pediatric Center remains on track, with a goal of occupancy in spring 2010. The parking deck is near completion and the steel for the structure will begin to be put in place later this month. Employee-led process redesign teams are developing plans to make the move as smooth as possible. Planning for the Scott Pavilion redesign will begin soon, with the actual renovation of the Scott Pavilion to begin in the summer of 2010.
Visit ChildrensOmaha.org for construction updates.
Children’s now requires the use of Computerized Provider Order Entry (CPOE) for all high-risk medications and TPN. Led by Chief Medical Informatics Officer George Reynolds, M.D., this initiative will further ensure the safety of patients at Children’s Hospital & Medical Center. The voluntary use of CPOE has been steadily rising over the past 12 months and is now just shy of 80 percent of all orders. Since Children’s implemented CPOE, there has been a decrease in medication errors from prescribing and transcription. The list of high-risk medications for which CPOE is required includes chemotherapy agents, vasoactive drips, IV digoxin, concentrated IV potassium and calcium salts, insulin, heparin and LMWH for anticoagulation, neuromuscular blocking agents and all controlled substances.
P. 7
PHYSICIAN’S PRIORITY HOTLINE 1.888.592.7955
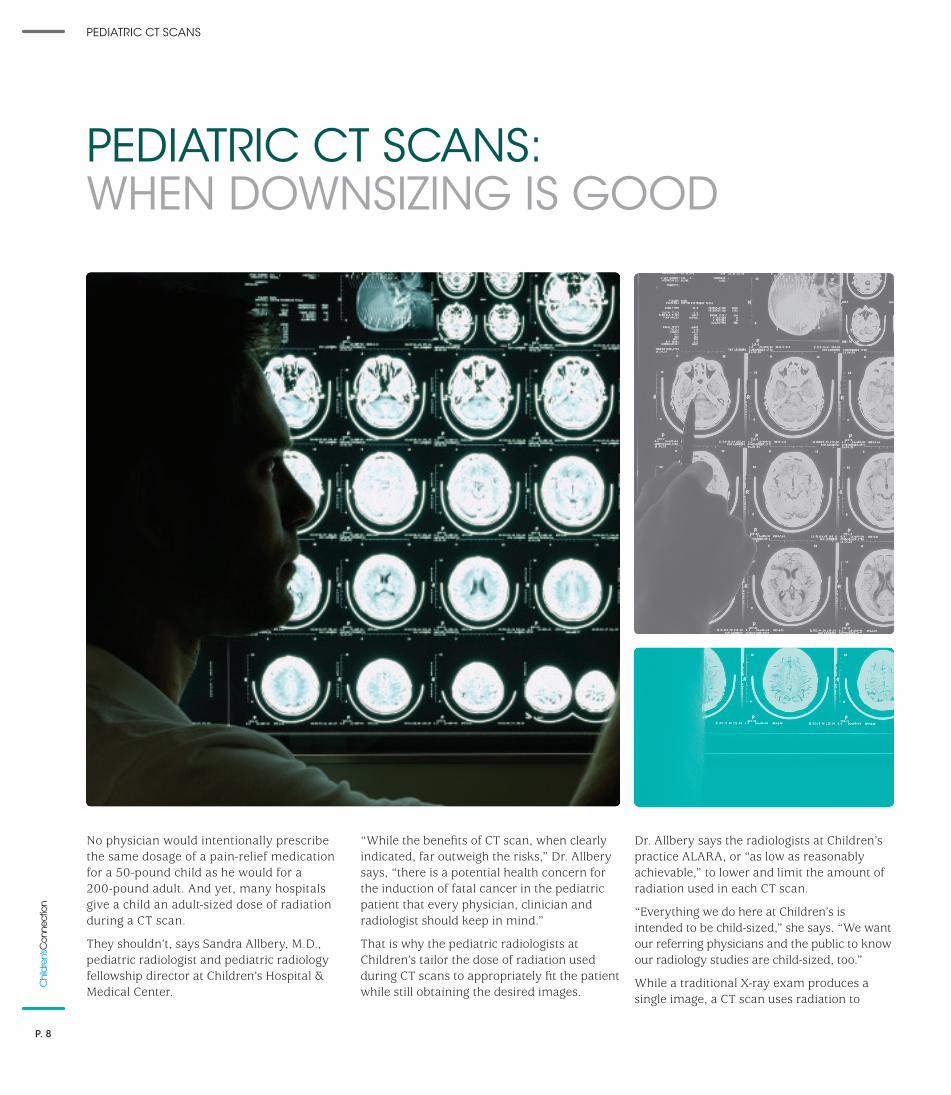
No physician would intentionally prescribe the same dosage of a pain-relief medication for a 50-pound child as he would for a 200-pound adult. And yet, many hospitals give a child an adult-sized dose of radiation during a CT scan.
They shouldn’t, says Sandra Allbery, M.D., pediatric radiologist and pediatric radiology fellowship director at Children’s Hospital & Medical Center.
“While the benefits of CT scan, when clearly indicated, far outweigh the risks,” Dr. Allbery says, “there is a potential health concern for the induction of fatal cancer in the pediatric patient that every physician, clinician and radiologist should keep in mind.”
That is why the pediatric radiologists at Children’s tailor the dose of radiation used during CT scans to appropriately fit the patient while still obtaining the desired images.
Dr. Allbery says the radiologists at Children’s practice ALARA, or “as low as reasonably achievable,” to lower and limit the amount of radiation used in each CT scan.
“Everything we do here at Children’s is intended to be child-sized,” she says. “We want our referring physicians and the public to know our radiology studies are child-sized, too.”
While a traditional X-ray exam produces a single image, a CT scan uses radiation to
PEDIATRIC CT SCANS: WHEN DOWNSIZING IS GOOD
PEDIATRIC CT SCANS
P. 8

produce a series of images of internal organs and structures in cross section, resulting in greater detail.
The brief, targeted exposure to ionizing radiation that occurs in a CT scan is higher than the amount of radiation in a traditional X-ray. It’s estimated that it would take 250 traditional chest X-rays to equal the amount of radiation exposure in one CT scan, Dr. Allbery says. And, the average adult CT scan is “two to three times” the exposure necessary in a pediatric CT scan, she says.
Dr. Allbery subscribes to the “Image Gently” campaign, an educational effort of the Alliance for Radiation Safety in Pediatric Imaging. The
campaign seeks to have all hospital radiology departments pledge to adopt pediatric CT protocol and adjust their CT doses to fit their pediatric patients.
“Approximately 80 percent of all pediatric imaging is not done at pediatric hospitals,” Dr. Allbery says. “That’s why educational efforts such as the Image Gently campaign are so important.”
Of additional concern for pediatric patients is the occurrence of repeat scans, especially if the radiation dose is not adjusted to fit the patient. The Image Gently Web site (www.imagegently.org) offers downloadable information packets for parents and pediatricians that include a “medical imaging record” in which parents can keep track of the date, type of exam and place where the exam was performed.
“The risks of repeated scans should always be weighed,” Dr. Allbery says. “There are valuable alternatives, such as ultrasound and MRI (magnetic
resonance imaging), which utilize no radiation at all.
“If referring physicians have any questions, they are always welcome to contact us and we can help them decide what the appropriate study should be.”
The radiologists at Children’s can minimize the exposure in a pediatric CT scan to conform to the referring physician or clinician’s diagnosis.
“We try to make certain that we know what we’re looking for,” she says. “If there is an indicated area they want to look at, we scan just that area – not the whole body, top to bottom.
“We also make every attempt to get a good picture in just one run. If we do need to make a second run, then we make every attempt to limit it to the area needed, because a second run obviously subjects the patient to a second dose.”
Dr. Allbery says choosing the appropriate imaging tool requires looking beyond a single symptom, especially if the resulting diagnosis would not alter the treatment.
“For example, if we have a child in the Emergency Department who we think has a renal stone, we can start with an ultrasound to determine if there is blockage of the kidney,” she says. “If there’s no blockage, there’s really no recommended intervention other than hydration initially.
“By using ultrasound rather than a CT scan, we’ve achieved the desired outcome and yet exposed the child to zero radiation.”
She says Children’s Hospital & Medical Center has invested in state-of-the-art equipment that includes dose-monitoring capability. Radiologists are able to employ “pulsed” fluoroscopy that limits the radiation exposure to a series of “bursts” that produce the desired images.
“With pulsed fluoroscopy, because you’re not giving X-rays constantly, you can quarter the dose of radiation exposure,” she says.
Image degradation in pulsed fluoroscopy is minor, she says. “With adults, the emphasis in a CT scan is often to give a strong dose to get the ‘prettiest’ picture possible. With our pediatric patients, I want the dose to be only enough to show me what we need to see.”
While the overall effects of exposure to radiation in X-rays and CT scans and the resulting lifetime cancer risk remain the subject of continuing research, it is clear that any risk should be considered by parents and physicians when deciding upon the appropriate form of imaging.
“If a CT scan is indicated, we do our very best at Children’s to make sure it’s appropriate for the patient,” Dr. Allbery says.
Because, as the “Image Gently” campaign points out, when it comes to radiation imaging, one size does not fit all.
“EVERYTHING WE DO HERE AT CHILDREN’S IS
INTENDED TO BE CHILD-SIZED. WE WANT OUR
REFERRING PHYSICIANS AND THE PUBLIC TO KNOW
OUR RADIOLOGY STUDIES ARE CHILD-SIZED, TOO.”
SANDRA ALLBERY, M.D.PEDIATRIC RADIOLOGIST AND PEDIATRIC RADIOLOGY FELLOWSHIP DIRECTORCHILDREN’S HOSPITAL & MEDICAL CENTER
P. 9
PHYSICIAN’S PRIORITY HOTLINE 1.888.592.7955

The attention given to a recently published medical study underscores the pressing need for clinical research already underway at Children’s Hospital & Medical Center.
A report in January’s Archives of Otolaryngology made national newspaper headlines when it outlined a significant increase in methicillin-resistant Staphylococcus aureus (MRSA) infections in pediatric patients.
The study quoted said that from 2001 through 2006, more than 21,000 reported pediatric head and neck infections were caused by staph germs, and of those infections, the percentage caused by MRSA bacteria more than doubled (from 12 percent to 28 percent) during that five-year period. An author of the report declared that increase to be “alarming.”
The study determined nearly 60 percent of the MRSA infections were “community acquired” (CA)
rather than “health care acquired” (HCA). An expert in Chicago said the report should serve as an alert to agencies that fund U.S. research that the rise in MRSA infections constitutes “a major public health problem.”
At the time the report was published, clinical research was already taking place at Children’s Hospital & Medical Center on two new antibiotics that could one day be used to fight CA MRSA infections in children.
Kari Simonsen, M.D., assistant professor in the Department of Pediatrics at the University of Nebraska Medical Center, Section of Pediatric Infectious Diseases, is conducting the antibiotic studies at Children’s.
Dr. Simonsen says CA MRSA “is one of the most common outpatient referrals” specialists see in the Infectious Diseases Clinic at Children’s – and the rate of occurrence is increasing.
MRSA is a strain of Staphylococcus aureus that is resistant to a large group of traditional anti-staphylococcal antibiotics called beta-lactams, which include penicillins and cephalosporins such as cephalexin. CA MRSA is susceptible to other antibiotics, including sulfa drugs, and sometimes tetracyclines and clindamycin.
CA MRSA strains were first reported in the late 1990s and defined by a lack of exposure to the health care setting in infected persons. Eventually, it became clear that CA MRSA infections were caused by strains of MRSA that differed from the older and better studied health care-acquired strains, says Dr. Simonsen.
MRSA emerges as small red bumps that resemble pimples, spider bites or boils that may be accompanied by fever and rashes. Within a few days, the bumps become larger, painful and eventually open into deep, pus-filled boils.
RESEARCHERS EXAMINE COMMUNITY ACQUIRED MRSA CAUSES, TREATMENTS
MRSA CAUSES, TREATMENTS
P. 10

CA MRSA strains have rapidly spread in the United States to become a common cause of cultured skin infections. They can also cause more serious infections, including pneumonia, skeletal and bloodstream infections.
In addition to a rise in outpatient cases of CA MRSA, “we also are seeing more and more outpatients with recurrent soft tissue infections,” Dr. Simonsen says. “Once they acquire them, some kids get them over and over again.”
Ongoing clinical research at Children’s involves two new antibiotics: daptomycin, which has been approved by the FDA for use by adults, and dalbavancin, which is currently under study nationally in both adults and children.
Daptomycin is being studied for use in treating pediatric soft tissue and skin infections caused by Gram positive bacteria, Dr. Simonsen says. Currently, three patients have been enrolled in the study, “and we hope to enroll 10,” she says.
Children’s is one of several medical centers nationally taking part in the trial.
Dr. Simonsen says it is too early to draw any conclusions regarding the drug’s effectiveness. “It appears to be safe and well-tolerated in the patients we’ve seen, and it does have a good track record in adults,” she says.
Other research has been conducted at Children’s regarding MRSA infections.
Archana Chatterjee, M.D., Ph.D., professor of pediatrics at Creighton University School of Medicine, hospital epidemiologist at Children’s and chief of the Division of Pediatric Infectious Diseases at the Creighton School of Medicine, is one author of a study which examined MRSA infections at Children’s between 1989 and 2004.
When examining the charts of the 150 known patients with MRSA infections during that period, researchers found a significant increase in community-acquired MRSA infections. In 1989, for example, there were no CA MRSA cases reported at the hospital, while in 2004 there were 10 cases.
Dr. Chatterjee says one difficulty the researchers noted was the lack of standardized definition of what constitutes a community acquired infection. This can lead to problems determining if the MRSA infection was truly community acquired and simply not diagnosed until the patient was in a health care environment.
“The numbers for HCA MRSA are fairly stable, but we have seen a rapid increase in CA MRSA,” she says. “We really do not know why.”
She says the “molecular fingerprints” of the infections do not indicate that HCA MRSA has spread into the community. “It’s more like the CA MRSA we’ve seen is a first cousin to HCA MRSA.”
While daycare environments have long been suspected of being sources for CA MRSA, a local study currently underway indicates that is not the case. Dr. Chatterjee says that of 70 children tested in a sampling of daycare centers throughout Omaha, none was positive for MRSA.
She says it is important for clinical research such as hers regarding the sources of MRSA to continue. “Much of the epidemiology tends to be regional and local. That’s why we need local data upon which we can base treatment.”
Although the majority of CA MRSA infections are localized to skin and soft tissue and often can be treated effectively, some CA MRSA strains have been reported to spread more rapidly and cause illness more severe than traditional HCA MRSA infections, affecting vital organs and leading to widespread infection.
These severe infections can be difficult to manage, Dr. Simonsen says. “It’s important to
have a specialist involved in any invasive MRSA infection.” Specialists such as those at the Infectious Disease Clinic at Children’s Hospital & Medical Center.
“IT’S IMPORTANT TO HAVE A SPECIALIST INVOLVED IN ANY INVASIVE MRSA INFECTION.”
KARI SIMONSEN, M.D.INFECTIOUS DISEASE EXPERTCHILDREN’S HOSPITAL & MEDICAL CENTER
A STUDY DETERMINED NEARLY 60 PERCENT OF THE MRSA INFECTIONS WERE “COMMUNITY ACQUIRED” RATHER THAN “HEALTH CARE ACQUIRED.”
P. 11
PHYSICIAN’S PRIORITY HOTLINE 1.888.592.7955
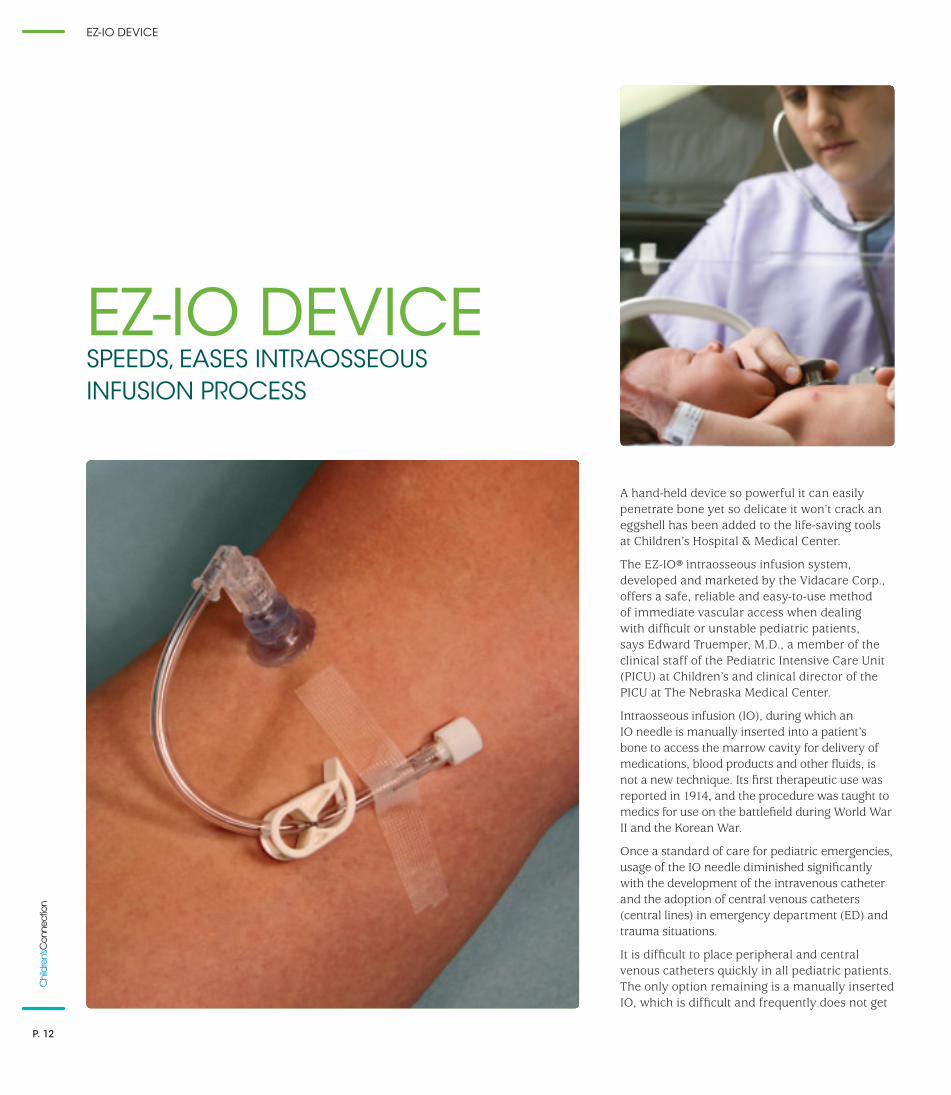
A hand-held device so powerful it can easily penetrate bone yet so delicate it won’t crack an eggshell has been added to the life-saving tools at Children’s Hospital & Medical Center.
The EZ-IO® intraosseous infusion system, developed and marketed by the Vidacare Corp., offers a safe, reliable and easy-to-use method of immediate vascular access when dealing with difficult or unstable pediatric patients, says Edward Truemper, M.D., a member of the clinical staff of the Pediatric Intensive Care Unit (PICU) at Children’s and clinical director of the PICU at The Nebraska Medical Center.
Intraosseous infusion (IO), during which an IO needle is manually inserted into a patient’s bone to access the marrow cavity for delivery of medications, blood products and other fluids, is not a new technique. Its first therapeutic use was reported in 1914, and the procedure was taught to medics for use on the battlefield during World War II and the Korean War.
Once a standard of care for pediatric emergencies, usage of the IO needle diminished significantly with the development of the intravenous catheter and the adoption of central venous catheters (central lines) in emergency department (ED) and trauma situations.
It is difficult to place peripheral and central venous catheters quickly in all pediatric patients. The only option remaining is a manually inserted IO, which is difficult and frequently does not get
EZ-IO DEVICE SPEEDS, EASES INTRAOSSEOUS INFUSION PROCESS
EZ-IO DEVICE
P. 12

placed successfully. Thus, life-sustaining fluids and medications cannot be given.
“Prior to the development of the EZ-IO, if every attempt failed to start a peripheral IV, a central line or manual insertion of an IO line – you were out of options,” Dr. Truemper says. “If that happened, and if the dehydration has led to severe shock, then the patient is going to die.”
There are methods available for assisting physicians in locating veins in pediatric patients, such as the VeinViewer® Imaging System by Luminetx, or through the use of ultrasound.
“These devices can help find a vein, but they are slow when placing an IV quickly which is critical to successful resuscitation when the child is deteriorating rapidly,” Dr. Truemper says. “Also, even more problematic is that a sick kid’s veins tend to collapse, which makes it even harder to insert the catheter.”
In some cases, the only viable option was manual IO insertion. Dr. Truemper estimates he has placed approximately 30 IO needles via manual insertion.
“You push the needle into the bone until the needle tip reaches the marrow cavity which connects to the surrounding veins,” he says. “It takes skill and brute force.”
In researching for a better method, Dr. Truemper came across the EZ-IO. Resembling a hot glue gun, the EZ-IO is a battery-powered drill that provides intraosseous access in all care environments. Dr. Truemper says it is easy to teach, easy to learn and easy to use.
“I can teach the drill technique in less than 10 minutes,” he says. “To mimic infant bones, we use chicken eggs. The drill is so
sensitive it can penetrate the egg without cracking the shell.
“The whole process of insertion can take less than 10 seconds. And the drill bit is the actual IO needle with a cutting edge, which greatly reduces the time between insertion and the delivery of fluids.”
EZ-IO affords drug delivery equivalent to a central line, even in CPR patients; relatively painless insertion; and very low complication rate, especially when compared to the risk of bloodstream infections from the placement of a central line.
In the first two months of having the EZ-IO device at Children’s, more than 150 people were trained in its use. “We are the first children’s hospital in the U.S. to stock every resuscitation cart with this device.”
Dr. Truemper, who has given presentations about EZ-IO and other medical innovations, also teaches with other trainers how to use the device as part of his pediatric advanced life support class.
Since its first use at Children’s in February 2006, the EZ-IO has been employed approximately 60 times in 48 different pediatric patients with a successful insertion rate “well over 90 percent,” he says. “It has also been used in at least four resuscitations where it provided the only initial IV access.”
In one case, a pediatric patient destabilized in the hours prior to surgery for a cardiac condition.
“We tried peripheral lines but he was going into shock. He needed more fluid and an anti-coagulant to keep his cardiac condition from shutting off the blood supply to his lungs, and he needed it immediately.”
Using the EZ-IO device, doctors drilled two IO lines into the child’s leg bones in less than 40 seconds.
“We got him out of shock, his oxygen level up and stabilized so he could be taken to the operating room and have his cardiac condition corrected. After that, the surgeon and anesthesiologist were finally able to place an IV line. Up to that point, his sole IV access was the two IO lines in his legs.
“That boy recovered and left the hospital one month later.”
The EZ-IO, which costs approximately $300 and comes with a battery guaranteed for 15 years, is being investigated for use in bone marrow examinations and other diagnostic procedures, Dr. Truemper says.
“It is by no means a complete answer,” he says, “but it is a significant leap for IV access where the need outweighs the time you would spend trying to get access from other routes.
“I believe it should be a part of every emergency department. Until then, referring physicians need to know it’s available and being put to good use here at Children’s.”
“PRIOR TO THE DEVELOPMENT OF THE EZ-IO, IF EVERY
ATTEMPT FAILED TO START A PERIPHERAL IV, A CENTRAL
LINE OR MANUAL INSERTION OF AN IO LINE – YOU WERE
OUT OF OPTIONS.”
EDWARD TRUEMPER, M.D.PEDIATRIC CRITICAL CARE PHYSICIANCHILDREN’S HOSPITAL & MEDICAL CENTER
P. 13
PHYSICIAN’S PRIORITY HOTLINE 1.888.592.7955
Howard Needelman, M.D., doesn’t have a crystal ball. He has something better – the data-rich Developmental TIPS program.
A neonatologist and developmental specialist at Children’s Hospital & Medical Center, Dr. Needelman is medical director of the Developmental TIPS (Tracking Infant Progress Statewide) program with administrative offices at the University of Nebraska Medical Center’s Munroe-Meyer Institute in Omaha.
Developmental TIPS is a comprehensive neurodevelopmental follow-up program that tracks the progress of children who have spent more than 96 hours in any of the neonatal intensive care units (NICUs) in Nebraska.
Since its inception more than 10 years ago, Developmental TIPS has compiled into a single database a wealth of information about the more than 8,000 children who have been enrolled.
Originally a research program, Developmental TIPS has evolved into an ongoing patient service program funded by the Nebraska Department of Education and Department of Health and Human Services, and supported by every hospital in Nebraska that has a NICU. It is the largest standardized developmental follow-up program of its kind in the nation.
Dr. Needelman, one of less than a dozen physicians in the United States who is sub-board certified in both neonatology and developmental behavioral pediatrics, heads the program’s developmental assessment team.
After children are registered by the reporting NICU, they are examined at 6 months corrected age, 16 months and 2 years. The team spends 90 minutes conducting a complete developmental assessment of the child to determine any developmental issues and make certain that steps are taken to provide the child access to any necessary services.
“A lot of these children have both major and minor disabilities,” Dr. Needelman says. “And yet, many health care providers in the region are unaware of the risks these children have for developmental delays.
“By conducting a thorough assessment and continuing follow-up assessments, we make every attempt to be sure these children get all the services they need to optimize their development.”
The children’s risk is dependent upon factors such as the extent of their prematurity, the complexity of their medical history and the results of preliminary hearing and vision screenings. The children are followed through age 3.
Through the Developmental TIPS database and by examining national data, Dr. Needelman can provide physicians and parents of premature children information regarding possible developmental risks and
NEURODEVELOPMENTAL FOLLOW-UP IDENTIFIES RISKS, SPECIAL NEEDS
NEURODEVELOPMENTAL FOLLOW-UP
P. 14

outcomes. “We have the local, regional and national data to be able to tell you how your child may do.”
The program has become “well-accepted by the people who care for neonatal and premature children as the source for developmental assessments and the beginning of the coordination of developmental care for this population of kids,” Dr. Needelman says, “so they don’t slip through the cracks.”
The commitment of Children’s Hospital & Medical Center to the program “has been nothing short of phenomenal. Our success in capturing data regarding the population at Children’s compared to other busy nurseries in the state has been very, very good.”
Data amassed by the program has served to support or refine other previously published data descriptive of certain populations, Dr. Needelman says.
“Like the published national outcomes for the extremely premature and traditionally most at-risk children, it is still a relatively unusual event to have a significant disability, such as cerebral palsy or blindness,” he says. “That is very heartening news.
“What we find, as we look less at these major morbidities, is a fairly high, perhaps 25 percent to 30 percent, rate of more minor sequelae, like language delays at 2 years, in kids whom we would have thought 10 years ago were a minimal risk.”
Because the data indicates those less medically at-risk children have a significant risk for minor delays like speech and
language, “they end up needing special education at a much greater rate when they get into school,” Dr. Needelman says.
Supplying current information about this segment of the population enables school districts, educational service units and other education providers to better anticipate special education needs and funding.
“Through this program, we’re helping the Department of Education plan its budget. We’re able to say, ‘you’ve got this many kids in the pipeline and this is what they’re likely to need.’”
The early intervention triggered by the assessments also affords at-risk children a better opportunity for success. “Our job is to identify those children showing developmental delays and make sure they can take advantage of the services available.”
Family physicians and pediatricians should be aware of the program and make certain enrollment is made available to parents if their child has been hospitalized in a NICU more than 96 hours. There is no cost.
Dr. Needelman says that through the Developmental TIPS program, the collaboration and funding from state agencies, and the participation of the NICUs in the state, “we’ve created a very good working relationship between the medical and educational communities – sharing information and helping kids.”
“BY CONDUCTING A THOROUGH ASSESSMENT AND CONTINUING FOLLOW-UP
ASSESSMENTS, WE MAKE EVERY ATTEMPT TO ENSURE THESE CHILDREN GET
ALL THE SERVICES THEY NEED TO OPTIMIZE THEIR DEVELOPMENT.”
HOWARD NEEDELMAN, M.D.NEONATOLOGIST AND DEVELOPMENTALISTCHILDREN’S HOSPITAL & MEDICAL CENTER
MEDICAL
EDUCATIONAL
P. 15
PHYSICIAN’S PRIORITY HOTLINE 1.888.592.7955
Research is being conducted in the Food Hypersensitivity Clinic at Children’s Hospital & Medical Center that could lead to the application of a new treatment in the fight against pediatric eosinophilic esophagitis.
“This is a unique and pivotal proof of concept study,” says Russell Hopp, D.O., medical director of the Allergy and Asthma Clinic and Food Hypersensitivity Clinic at Children’s.
There are four major allergic diseases which have been recognized for at least 100 years: asthma, allergic rhinitis (hay fever), eczema and food allergies. “Eosinophilic esophagitis can be considered as the fifth allergic disease,” says Dr. Hopp, “but we didn’t know it existed before 1978.”
Eosinophilic esophagitis (EE) is an allergic inflammatory reaction of the esophagus, the muscular tube that carries food from
the throat to the stomach. It is found in approximately one of every 1,500 children, Dr. Hopp says, and though it is most often associated with another existing allergy, it can exist independently.
The symptoms of EE are similar to gastro-esophageal reflux disease (GERD). To distinguish between the two, a biopsy of the esophagus and GERD studies are performed. In EE, high levels of eosinophils are detected in the esophagus but not other parts of the digestive tract. Eosinophils are a type of white blood cell that are not normally found in the esophagus.
The presence of eosinophils in the esophagus causes inflammation that can make swallowing difficult and digestion painful. Other symptoms include vomiting, abdominal pain, chest pain, choking, cramping, nausea, weight loss and failure to thrive.
“We knew about the presence of eosinophils in the rest of the gastrointestinal tract prior to 1978, but not about having an allergic disease in the esophagus itself,” Dr. Hopp says. “While it still is not commonly diagnosed, EE has been increasing in recognition, and possibly in prevalence, in the last decade.”
EE can occur in any age but is most often seen in children older than 6 months up to teenagers. It is much less common in adults.
“Most of the time, when teenagers are diagnosed as having EE it’s because they’ve gotten a pill or some food temporarily stuck in their esophagus. By that age, either the condition is relatively new or has been under recognized in their earlier years.”
To help diagnose EE, Dr. Hopp queries everyone who comes into the allergy clinic about their esophagus.
PRODUCTION OF EOSINOPHILS TARGETED IN ALLERGY RESEARCH
EOSINOPHILIC ESOPHAGITIS
P. 16
“Because allergic diseases tend to come in multiples, those with EE often have asthma or hay fever or food allergies,” he says. “Anyone who comes into my clinic with an allergic disease coupled with recurrent heartburn also gets referred to GI to get scoped.”
Dr. Hopp estimates that between 80 percent and 90 percent of the patients seen at the Food Hypersensitivity Clinic at Children’s have EE.
An endoscopy can reveal either a normal esophagus or one that is constricted or exhibiting the rings and white bumps associated with elevated levels of eosinophils.
“The pathologist reads the slides to determine the number of eosinophils, and how well the patient responds to therapy may depend on the numbers,” Dr. Hopp says.
Therapy begins with anti-reflux medicines and often is coupled with food avoidance and the prescription of a swallowed corticosteroid. “Because some refer to EE as ‘asthma of the esophagus,’ we have seen a good response to asthma medications.”
The Food Hypersensitivity Clinic team at Children’s, which includes gastroenterologist Fernando Zapata, M.D., nurse coordinator Kristie Schwab, R.N., and a registered dietician, is studying the application of an anti-interleukin (IL) drug given intravenously.
Cytokine is an immunoregulatory protein. The cytokine IL-5 is involved in the maturation, proliferation and regulation of eosinophils. The anti-IL-5 drug under study at Children’s serves as a cytokine blocker.
“By giving the patient anti-IL-5, we turn off production of eosinophils in the bone marrow,” Dr. Hopp explains. “Once production of the eosinophils is stopped, their movement to the target organ in an allergic disease is also stopped.”
He says that while eosinophils serve to kill parasites in the bloodstream and tissue, there is no adverse reaction to stopping their production, as long as the patient is not traveling to a country where such parasites are common.
To participate in the study, a patient must have moderate to severe symptoms of EE, agree to a four-month IV study, and not have begun other forms of treatment that would prevent researchers from obtaining a clear response to the drug.
“The study is about nine months old, and we are still actively enrolling patients,” Dr. Hopp says. “Children’s Hospital & Medical Center is one of about 30 medical centers taking part nationally.”
If approved, anti-IL-5 is not expected to be a first-line therapy against EE, he says. “More than likely, it will be used for extreme and severe cases.”
“WHILE IT IS STILL NOT COMMONLY DIAGNOSED, EOSINOPHILIC ESOPHAGITIS HAS BEEN INCREASING IN RECOGNITION, AND POSSIBLY IN PREVALENCE, IN THE LAST DECADE.” RUSSELL HOPP, D.O.MEDICAL DIRECTORALLERGY AND ASTHMA CLINICFOOD HYPERSENSITIVITY CLINICCHILDREN’S HOSPITAL & MEDICAL CENTER
FERNANDO ZAPATA, M.D.GASTROENTEROLOGISTCHILDREN’S HOSPITAL & MEDICAL CENTER
1.888.592.7955PHYSICIANS’ PRIORITY LINE
Your 24-hour link to pediatric specialists for physician-to-physician consults, referrals, admissions and neonatal transport service.
P. 17
PHYSICIAN’S PRIORITY HOTLINE 1.888.592.7955

NEW PEDIATRICIANS
NEONATOLOGYLYNN O’HANLON, M.D.Dr. O’Hanlon received her medical degree from the University of Nebraska Medical Center in 1996. She completed her pediatrics residency at Children’s Mercy Hospital in Kansas City, Mo., in 1999, and her neonatology fellowship in 2008, also at Children’s Mercy Hospital. She serves as a neonatologist at Children’s Hospital & Medical Center’s Newborn Intensive Care Unit.
HOSPITALIST SERVICELISA M. SIECZKOWSKI, M.D., F.A.A.P.Dr. Sieczkowski received her medical degree from the University of Nebraska Medical Center in 2000. She completed her pediatrics residency at Phoenix Children’s Hospital and Maricopa Medical Center in Phoenix, Ariz., in 2003. She is currently serving as a hospitalist at Children’s Hospital & Medical Center.
ANESTHESIAD. ALAN TINGLEY, M.D., M.B.A.Dr. Tingley serves as an anesthesiologist at Children’s Hospital & Medical Center. He received his medical degree from the University of Texas Southwestern Medical School in Dallas, Texas, in 1986, and a master’s degree in business administration from Capital University in Columbus, Ohio. Dr. Tingley completed his general surgery internship at the Medical College of Ohio in Toledo, Ohio, in 1987. He also completed anesthesiology residencies at the University of Kansas, in Kansas City, Kan., in 1989, and at the University of Louisville in Louisville, Ky., in 1990.
PATHOLOGYJIRI B. BEDRNICEK, M.D.Dr. Bedrnicek received his medical degree from Charles University in Prague, Czech Republic, in 2000. He completed his anatomic and clinical pathology residency at the University of Arizona in Tucson, Ariz., in 2008. He will complete his fellowship in pediatric pathology at Nationwide Children’s Hospital & Ohio State University in Columbus, Ohio, in June 2009. Dr. Bedrnicek is a pathologist at Children’s Pathology Center.
NEW PHYSICIANS
PEDIATRIC RESOURCE DIRECTORY
Children’s Hospital & Medical Center has created a new pediatric resource directory available in printed form and downloadable at www.ChildrensOmaha.org/PediatricResourceDirectory.
If you would like a printed copy, please call 402.955.6957.
The directory highlights various specialty services available to health care providers across the region. It is a quick reference tool, but is not intended to serve as a
complete medical staff directory. A more comprehensive listing is available online 24/7 at www.ChildrensOmaha.org.
Please note the following updates to phone numbers in the Pediatric Specialty Services Section of the directory: ENDOCRINOLOGY 402.955.3871
RESPIRATORY MEDICINE 402.955.5570
COMMUNITY PEDIATRIC ORTHOPAEDIC PHYSICIANS 402.778.6800
P. 18
Physicians’ Priority Line (physician-to-physician consult and referral line)1.888.592.7955
Transport (Physicians’ Priority Line) 1.888.592.7955
Hospitalist Service 402.955.5400 or 1.888.592.7955
PICU 402.955.4200
NICU 402.955.6230
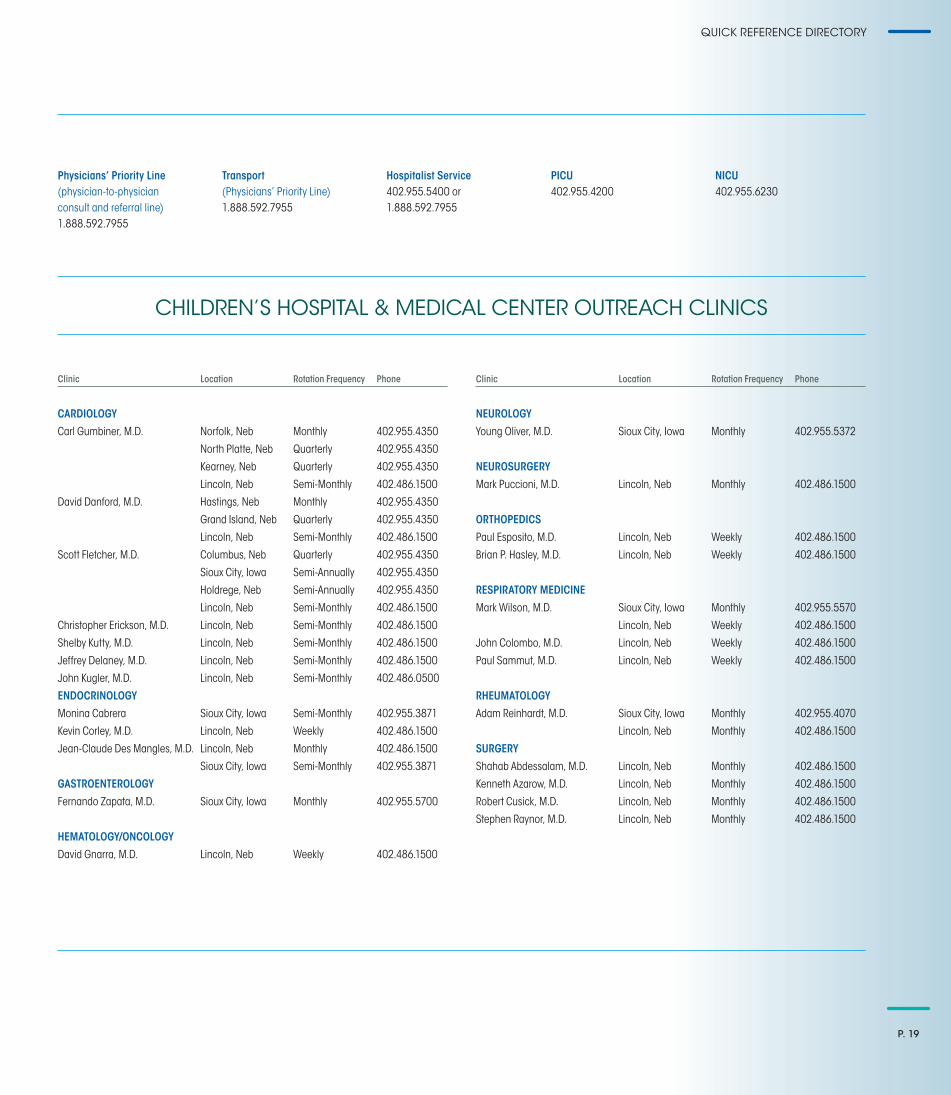
CHILDREN’S HOSPITAL & MEDICAL CENTER OUTREACH CLINICS
QUICK REFERENCE DIRECTORY
Clinic Location Rotation Frequency Phone
CARDIOLOGY
Carl Gumbiner, M.D. Norfolk, Neb Monthly 402.955.4350
North Platte, Neb Quarterly 402.955.4350
Kearney, Neb Quarterly 402.955.4350
Lincoln, Neb Semi-Monthly 402.486.1500
David Danford, M.D. Hastings, Neb Monthly 402.955.4350
Grand Island, Neb Quarterly 402.955.4350
Lincoln, Neb Semi-Monthly 402.486.1500
Scott Fletcher, M.D. Columbus, Neb Quarterly 402.955.4350
Sioux City, Iowa Semi-Annually 402.955.4350
Holdrege, Neb Semi-Annually 402.955.4350
Lincoln, Neb Semi-Monthly 402.486.1500
Christopher Erickson, M.D. Lincoln, Neb Semi-Monthly 402.486.1500
Shelby Kutty, M.D. Lincoln, Neb Semi-Monthly 402.486.1500
Jeffrey Delaney, M.D. Lincoln, Neb Semi-Monthly 402.486.1500
John Kugler, M.D. Lincoln, Neb Semi-Monthly 402.486.0500
ENDOCRINOLOGY
Monina Cabrera Sioux City, Iowa Semi-Monthly 402.955.3871
Kevin Corley, M.D. Lincoln, Neb Weekly 402.486.1500
Jean-Claude Des Mangles, M.D. Lincoln, Neb Monthly 402.486.1500
Sioux City, Iowa Semi-Monthly 402.955.3871
GASTROENTEROLOGY
Fernando Zapata, M.D. Sioux City, Iowa Monthly 402.955.5700
HEMATOLOGY/ONCOLOGY
David Gnarra, M.D. Lincoln, Neb Weekly 402.486.1500
Clinic Location Rotation Frequency Phone
NEUROLOGY
Young Oliver, M.D. Sioux City, Iowa Monthly 402.955.5372
NEUROSURGERY
Mark Puccioni, M.D. Lincoln, Neb Monthly 402.486.1500
ORTHOPEDICS
Paul Esposito, M.D. Lincoln, Neb Weekly 402.486.1500
Brian P. Hasley, M.D. Lincoln, Neb Weekly 402.486.1500
RESPIRATORY MEDICINE
Mark Wilson, M.D. Sioux City, Iowa Monthly 402.955.5570
Lincoln, Neb Weekly 402.486.1500
John Colombo, M.D. Lincoln, Neb Weekly 402.486.1500
Paul Sammut, M.D. Lincoln, Neb Weekly 402.486.1500
RHEUMATOLOGY
Adam Reinhardt, M.D. Sioux City, Iowa Monthly 402.955.4070
Lincoln, Neb Monthly 402.486.1500
SURGERY
Shahab Abdessalam, M.D. Lincoln, Neb Monthly 402.486.1500
Kenneth Azarow, M.D. Lincoln, Neb Monthly 402.486.1500
Robert Cusick, M.D. Lincoln, Neb Monthly 402.486.1500
Stephen Raynor, M.D. Lincoln, Neb Monthly 402.486.1500
P. 19
ChildrensOmaha.org
1.888.592.7955PHYSICIANS’ PRIORITY LINE
Your 24-hour link to pediatric specialists for physician-to-physician consults, referrals, admissions and neonatal transport service.
“WHEN I CALL, I ALWAYS SPEAK TO AN ATTENDING PHYSICIAN WHO CAN ASSIST ME WITH MY HOSPITALIZED PATIENTS. I ESPECIALLY APPRECIATE HOW PROMPTLY I AM CONNECTED TO ONE OF THE INTENSIVISTS OR THE HOSPITALIST. CHILDREN’S PHYSICIANS’ PRIORITY LINE IS AN EFFICIENT AND VALUABLE SERVICE.”
ANN REHAN, M.D., PEDIATRICIANPRAIRIE PEDIATRICS & ADOLESCENT CLINIC P.C.SIOUX CITY, IOWA





























