Embed Size (px)
Citation preview
Children’s Health Serviceshealth • care • people
Managing Young People in Youth Detention who suffer from Posttraumatic Stress and associated Mental Health and Substance Misuse Problems
Assoc. Prof. Stephen StathisConsultant Psychiatrist
Ivan DoolanSenior Social Worker – Forensic
On behalf of the Mental Health Alcohol Tobacco and Other Drugs Service (MHATODS)
Children’s Health Serviceshealth • care • people
“Sometimes it is more important to know what sort of person has a disease, than what sort of disease a person has.”
Sir William Osler, M.D
Children’s Health Serviceshealth • care • people
Outline
• Brief description of Mental Health Tobacco and Other Drugs Service (MHATODS)
• Prevalence of Mental Health Problems and Substance Use for YP in detention
• Treatment of Traumatised YP in detention– Specific issues in this population– Management difficulties & dilemmas– Relatively little on medication
Children’s Health Serviceshealth • care • people
Imagine ……..• Almost all your clients had conduct disorder• Almost all your clients had been abused• Up to 90% use drugs or alcohol• Over half were Indigenous• One third were:
– Depressed– Anxious– ADHD– Significant posttraumatic symptoms – Broad range of “other” mental health problems
Children’s Health Serviceshealth • care • people
What is MHATODS?• Mental Health Alcohol Tobacco and Other Drugs
Service
• First time in Qld. that mental health & drug and alcohol treatment for young people has been integrated
• Run in the Brisbane Youth Detention Centre– Males in detention from Rockhampton to NSW border – All females in Qld
Children’s Health Serviceshealth • care • people
The MHATODS Team • Half time Consultant Psychiatrist • 4+ Allied Health Clinicians specialised in C&YMH and
substance misuse. • Team Leader (½ time clinical load)• Administration Officer• Indigenous Health Worker/s• +/- Psychology Masters students• Psychiatric Registrar from January 2009
Children’s Health Serviceshealth • care • people
Aim of MHATODS
• Provide YP in detention with the same services they could expect if they were to attend a Community Mental Health Clinic or Drug and Alcohol Service
• Some modification due to setting – Limited History– Access to Family– Therapeutic Strategies– Rapid “churn-through”
Children’s Health Serviceshealth • care • people
Case Discussion
ZZ; 15 yr. male with 9 yr. Hx of disruptive behaviours. Seen in juvenile detention.
• Stealing• Some fire setting & graffiti/destruction of public
property• Fighting & suspensions• Entered the JJS at age 13; property offences• Lack of remorse.
Children’s Health Serviceshealth • care • people
Case Discussion
Complicated by:• Low-average IQ (V = 66; P = 78; FS = 71)• Learning problems & school-based behavioural problems
– Left school IX grade• Never sit still in class/fidgety• Poor attention & concentration• Always disruptive
• “Weird”; unusual stereotypical behaviours • Poor peer relationships• Poor awareness of social cues
Children’s Health Serviceshealth • care • people
Case Discussion
Well documented history of physical abuse and neglect: • DV - mother• Repetition of M’s own childhood/ few friends, poor
parenting.• Rarely sees father• M’s current partner is physically abusive when
intoxicated• Reported to DChS ++
Children’s Health Serviceshealth • care • people
Case Discussion
Mums main concerns:
• He is always “hyper” … • He acts “crazy without thinking”• It is getting worse in high school. • He was diagnosed with ADD and the medicines helped
him
Children’s Health Serviceshealth • care • people
Case Discussion In talking with ZZ:
• Admits he gets frustrated and “blows up”• Constantly feels sad • Hx DSI ?? Suicide attempts (x3)• People laugh at him because he is “strange”; never can keep friends• Difficulties sleeping: nightmares (trauma related) and some
flashbacks• Alcohol, occasional marijuana. ecstasy & speed:
– Likes the “rush” – Attempt to get rid of “bad memories”
• People call me a schizo & a retard”• Has heard that he can get “dex” from you
Children’s Health Serviceshealth • care • people
Diagnosis ???
Lots of Co-morbidities here:
• ADHD; Combined type• ODD / Childhood Onset Conduct Disorder• Depressive Disorder• PTSD• Polysubstance abuse • “Aspergers Disorder” / PDD-NOS• Learning Disorder• Borderline Mental Retardation/ V:P mismatch
Children’s Health Serviceshealth • care • people
Multiple Paradoxes
• Rapid assessment required of complex cases vs. Short assessment time frame
• Significant co-morbidity vs. Collateral Hx difficult to obtain
• Medication Seeking vs. Lack of therapeutic relationship• Remand vs. Sentence
Children’s Health Serviceshealth • care • people
Multiple Paradoxes (cont)
• High levels of MH and D&A problems– Precontemplative – Difficult to engage
• Marginalised group of YP where trust in authority figures is rare
Children’s Health Serviceshealth • care • people
Patterns of Substance Use at BYDC
Children’s Health Serviceshealth • care • people
Substance Use in Youth Detention
• Lennings & Pritchard (1999) found 90% of young people in detention had some degree of drug/alcohol use.
• 33% of these believed they had a problem. – Of those, 70% thought they should have treatment
• >50% young people in detention met criteria for a substance use disorder (Teplin et al., 2002)
Children’s Health Serviceshealth • care • people
Reported Substance Use Prior to Admission to BYDC
• Chart audit of admissions in the period 1/1/06 – 31/3/06
• 209 admissions• 174 individual young people• 31 females; 143 males• 78 Indigenous; 96 non-Indigenous• Mean age 15.4 years (+/-1.3)
Children’s Health Serviceshealth • care • people
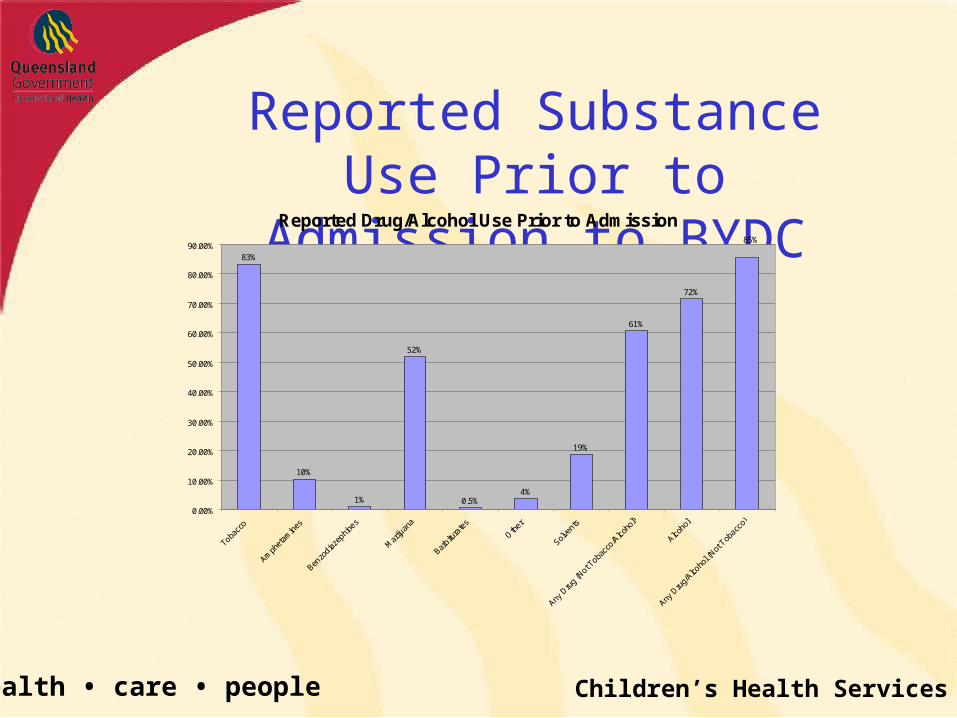
Reported Substance Use Prior to Admission to BYDC
Reported Drug/Alcohol Use Prior to Admission
19%
61%
72%
4%0.5%
52%
1%
10%
83%
85%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
Tobacc
o
Amph
etam
ines
Benzo
diazep
hines
Mar
ijuan
a
Barbitu
rate
s
Oth
er
Solve
nts
Any D
rug
(Not T
obacc
o/Alco
hol)
Alcoho
l
Any D
rug/
Alcoho
l (Not
Tob
acco)
Children’s Health Serviceshealth • care • people
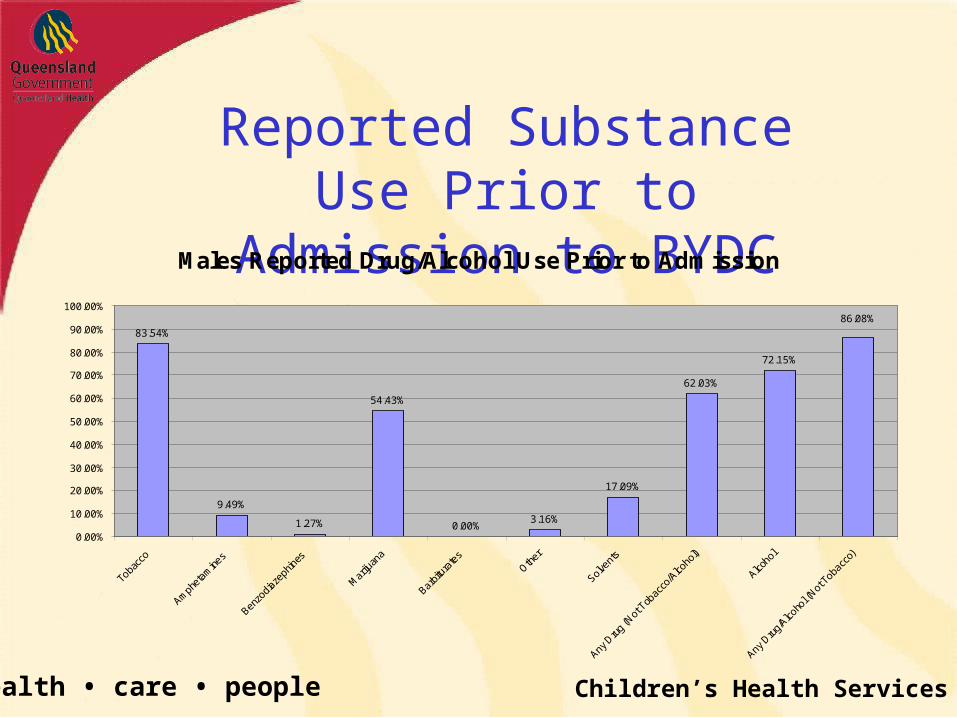
Reported Substance Use Prior to Admission to BYDCMales Reported Drug/Alcohol Use Prior to Admission
83.54%
9.49%
1.27%
54.43%
0.00%3.16%
17.09%
62.03%
72.15%
86.08%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Toba
cco
Amph
etam
ines
Benzo
diaze
phin
es
Mar
ijuan
a
Barbit
urat
esOth
er
Solven
ts
Any D
rug
(Not
Tob
acco
/Alco
hol)
Alcoho
l
Any D
rug/
Alcoho
l (Not
Tob
acco
)
Children’s Health Serviceshealth • care • people
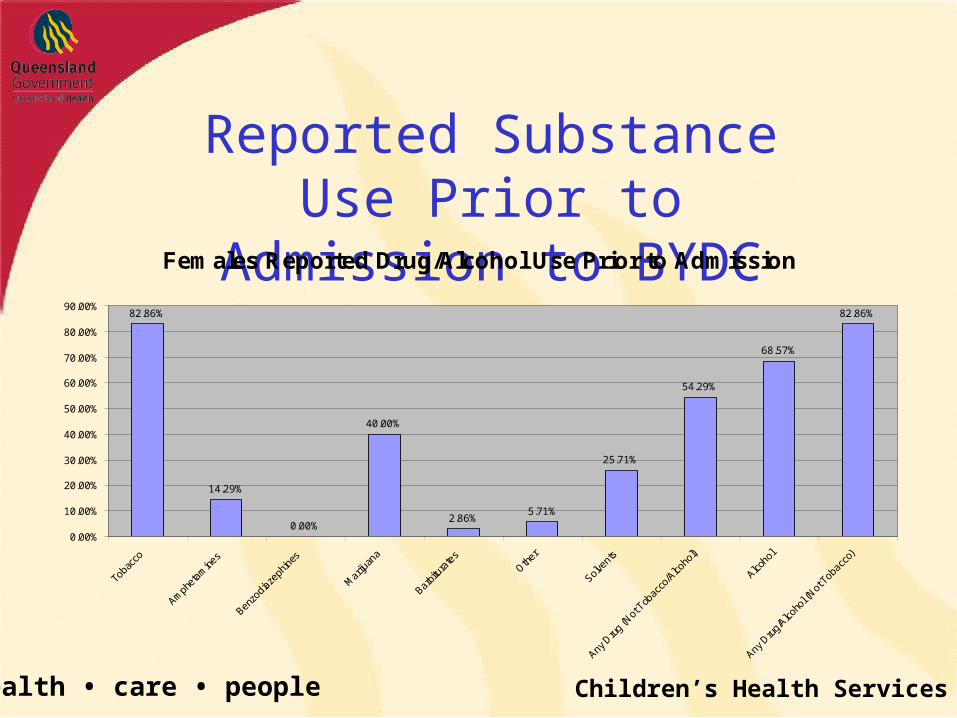
Reported Substance Use Prior to Admission to BYDCFemales Reported Drug/Alcohol Use Prior to Admission
82.86%
14.29%
0.00%
40.00%
2.86%5.71%
25.71%
54.29%
68.57%
82.86%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
Toba
cco
Amph
etam
ines
Benzo
diaze
phin
es
Mar
ijuan
a
Barbit
urat
esOth
er
Solven
ts
Any D
rug
(Not
Tob
acco
/Alco
hol)
Alcoho
l
Any D
rug/
Alcoho
l (Not
Tob
acco
)
Children’s Health Serviceshealth • care • people
Audit Summary
• Males higher rates for marijuana, alcohol• Females higher rates inhalants, amphetamines• Non-Indigenous higher rates alcohol,
amphetamines• Indigenous higher rates inhalants
Children’s Health Serviceshealth • care • people
MHATODS Programs
• Four Session Individual Substance Use Intervention Program
• Voluntary• Individual one-on-one counselling for
anyone• Aim is to understand substance use in
context of life and experience• Can be referred by Caseworker, Nurse or
VMO
Children’s Health Serviceshealth • care • people
MHATODS Programs
• Four Session Group Relapse Prevention Program
• Voluntary• Group counselling for anyone• Aim is to maximise reducing or ceasing
substance use• Can be referred by Caseworker, Nurse or
VMO
Children’s Health Serviceshealth • care • people
Prevalence of Mental Health Problems at BYDC
Children’s Health Serviceshealth • care • people
MH Problems: YP in Detention
• 2/3 of males and 3/4 females in detention centres will have one or more psychiatric disorders (Teplin et al, 2002)– Similar findings in Australia, Canada, UK &
Europe– Comorbidity is the NORM rather than the
EXCEPTION
Children’s Health Serviceshealth • care • people
PTSD in Youth Detention(Abram et al. 2004)
• ~900 young people in juvenile detention• Diagnostic Interview Schedule for Children,
version IV (DISC IV)• 92.5% experienced 1 or more traumas (mean,
14.6 incidents; median, 6 incidents)• Significantly more males (93.2%) than females
(84.0%) reported at least 1 traumatic experience• 11.2% of the sample met criteria for PTSD in the
past year. • > 50% with PTSD reported witnessing violence
as the precipitating trauma.
Children’s Health Serviceshealth • care • people
Massachusetts Youth Screening Instrument (MAYSI-2)
• Screens for 7 scales of mental health or behavioural problems:– Alcohol and Drug– Angry-Irritable– Depressed-Anxious– Somatic Complaints – Suicide Ideation– Thought Disturbance (males only)– Traumatic Experience (gender specific)
Children’s Health Serviceshealth • care • people
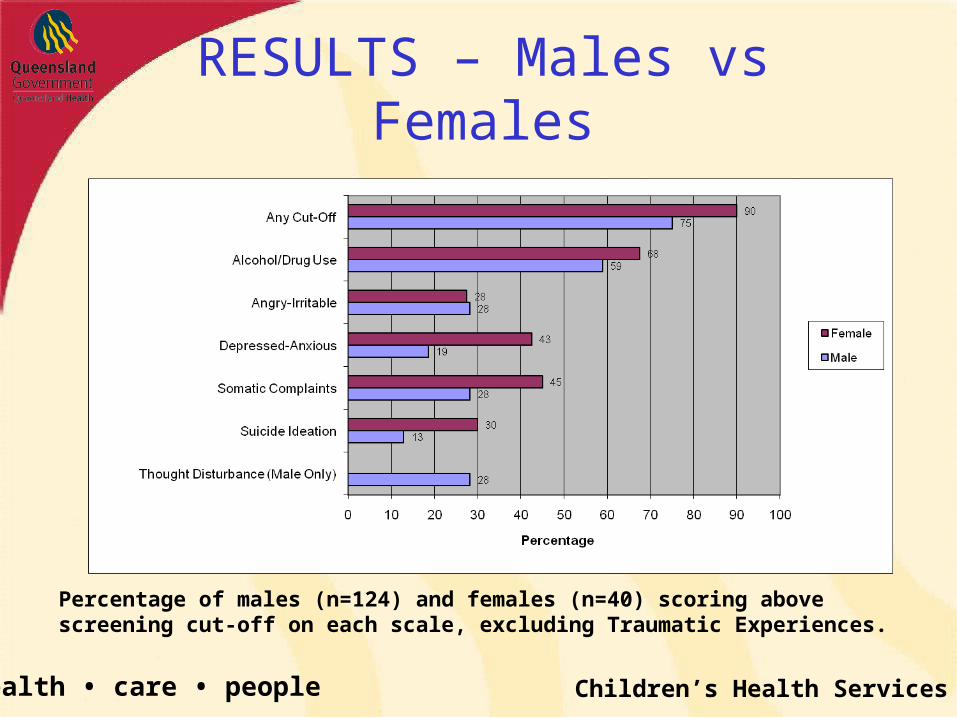
RESULTS – Males vs Females
Percentage of males (n=124) and females (n=40) scoring above screening cut-off on each scale, excluding Traumatic Experiences.
Children’s Health Serviceshealth • care • people
RESULTS
• 75% males and 90% of all females scored above the clinical cut-off on at least one of the scales (excluding Thought Dist. & Traumatic Experiences).
• Females screened for significantly higher mental health problems than males across three scales:– Depressed-Anxious (2 = 9.41; p < 0.01)– Somatic Complaints (2 = 3.89: p < 0.05)– Suicide Ideation (2 = 6.24; p < 0.05)
Children’s Health Serviceshealth • care • people
What About Traumatic Experiences?
Children’s Health Serviceshealth • care • people
TE Subscale- 5 Questions
1. Have you ever in your whole life had something bad or terrifying happen to you?
2. Have you ever been badly hurt or in danger of getting badly hurt or killed?
3. Have you had a lot of bad thoughts or dreams about a bad or scary event that happened to you?
4. Have you ever seen someone severely injured or killed (in person not just on TV)?
5. FEMALE: Have you ever been raped or in danger of being raped?
MALE: Have people talked about you a lot when you’re not there?
Children’s Health Serviceshealth • care • people
RESULTS – TE Subscale
Disturbingly high rates of trauma• 82% females reported at least 1 traumatic
event; Mean 3.4• 67% of males reported at least 1 traumatic
event; Mean 2.2
Children’s Health Serviceshealth • care • people
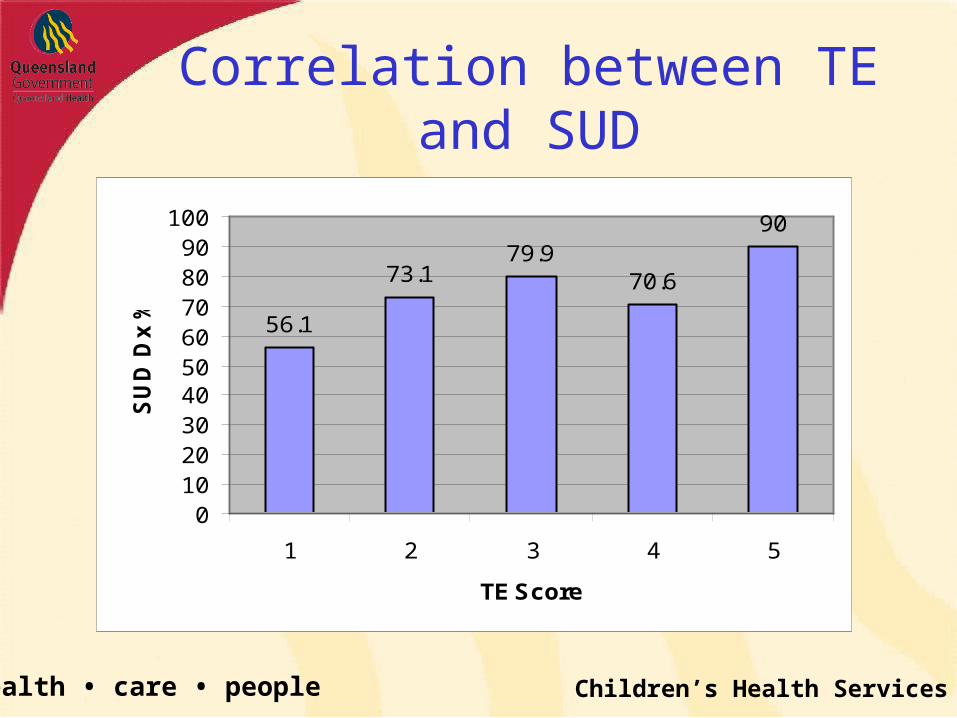
Correlation between TE and SUD
56.1
73.179.9
70.6
90
0102030405060708090
100
1 2 3 4 5
TE Score
SU
D D
x %
Children’s Health Serviceshealth • care • people
Screening: Implications for practice?
• DO NO HARM• We know there is a high burden of D&A and MH problems• We know there are heaps of traumatised young people in
detention• We know that admission into detention precipitates posttraumatic
symptoms (PTS)– Agitated young people historically poorly tolerated!!
• New environment including loss of (limited) supports• Close living quarters• Stress of court process• ?Withdrawal symptoms• Away from country (Indigenous)
• We don’t know evidence-based ways to treat these young people
Children’s Health Serviceshealth • care • people
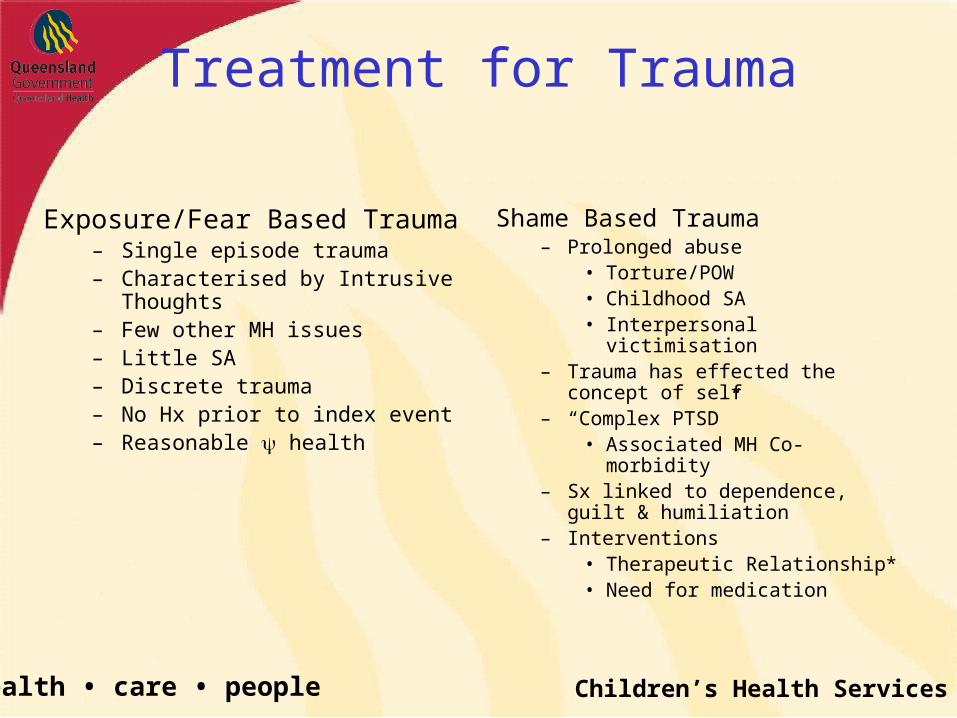
Treatment for Trauma
Exposure/Fear Based Trauma– Single episode trauma– Characterised by Intrusive
Thoughts– Few other MH issues– Little SA– Discrete trauma– No Hx prior to index event– Reasonable health
Shame Based Trauma– Prolonged abuse
• Torture/POW• Childhood SA• Interpersonal victimisation
– Trauma has effected the concept of self
– “Complex PTSD”• Associated MH Co-morbidity
– Sx linked to dependence, guilt & humiliation
– Interventions • Therapeutic Relationship*• Need for medication
Children’s Health Serviceshealth • care • people
Evidence Base - Adolescents
• Surprise, surprise.! Very little• Usually associated with natural disasters or
single assaults (fear-based trauma)• Soon after trauma• Few with the types of traumatised YP we see in
detention• Very few “brief” interventions
– 6, 8, 10, 18 weekly sessions– 1-2 hour/session
Children’s Health Serviceshealth • care • people
Evidence Base - Therapies
• Silverman (2008) reviewed 21 treatment studies for children suffering from PTSD and PTSS– Violence, Abuse, Disasters, MVA
• 8 studies using Traumatic-Focused CBT met “Well Established Criteria” for efficacy– Shared the following:
• Working with children individually• Child exposure tasks via narratives, drawings or
imagination
• Most ~ 12 sessions; up to 20• Most 45-90 minutes duration
Children’s Health Serviceshealth • care • people
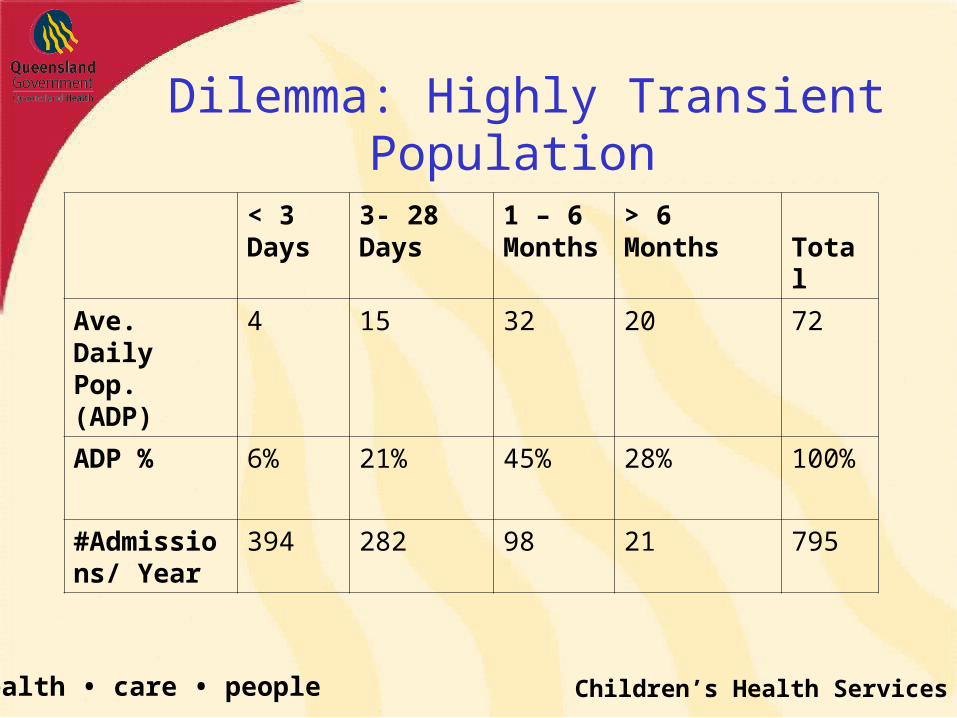
Dilemma: Highly Transient Population
< 3 Days
3- 28 Days 1 – 6 Months
> 6 Months Total
Ave. Daily Pop. (ADP)
4 15 32 20 72
ADP % 6% 21% 45% 28% 100%
#Admissions/ Year
394 282 98 21 795
Children’s Health Serviceshealth • care • people
The Dilemma Continue
• Highly Transient Population in BYDC– Short and frequent admission
• Environment of BYDC– Contain vs Exacerbate– Need for short term symptom control– Confounding bias
• Co-morbidity is the norm– Need to also treat MH and SU problems
Children’s Health Serviceshealth • care • people
The Dilemma (continued)
• Psychologically minded– Precontemplative– Stimulus to change in BYDC only?– External locus of control and medication … “Give me a pill, doc”– Cognitive Scores skewed to left
• Marginalised group of YP – Lack of trust
• Community Toxicity– Longstanding social disadvantage / Maslow’s Hierarchy– Ongoing trauma after release
• Indigenous– Narrative Approach best
Children’s Health Serviceshealth • care • people
The Dilemma (yes, there is more)
• Inappropriate dismantling of complex defenses– “Professional Voyeurism”
• Ability to extract information from a patient which does not assist in management
• What can you do with the history obtained?!
Children’s Health Serviceshealth • care • people
Conclusion: Need to Develop Our Own Program
• Brief (~ 4 sessions within a month)• Narrative• Focused on Acute symptoms reduction
– Solution Focused
• Psychoeducational– Understanding the meaning behind the Sx
• Cognitive Restructuring– Understanding the negative/intrusive thoughts
Children’s Health Serviceshealth • care • people
Brief Intervention for Trauma Symptoms (BITS)
• Narrative strength based approach• Integrate trauma experience symptomatology• Regain mastery of the parts of their lives
affected by their trauma related symptoms
Children’s Health Serviceshealth • care • people
4 Sessions
1. Psychoeducation
2. Trauma Narrative
3. Cognitive Restructuring
4. Symptom Management
Children’s Health Serviceshealth • care • people
Session 1: Psychoeducation• Re-Experiencing Phenomena• Avoidance Symptoms• Arousal• Mood disturbances• Goal is to normalise the response• Normal/recognised experience to an abnormal
event• “I would expect someone who has experienced
what you have to be having (flashbacks etc…)”• Reassurance they are not going …. crazy, womba
etc
Children’s Health Serviceshealth • care • people
Session 2: Trauma Narrative
• Attempt to get a young person to give you an idea of what they have suffered
• Use of the TSCC• A lot of young people have things happen to
them that are difficult to talk about. Has something like that happened to you?
• eg. If sexual abuse evident– “Sometimes adults touch children in a sex way, or make children touch
them in a sexual way. Has this happened to you?– Sometimes children enjoy these things and then feel really guilty and
bad about it. Has that ever happened to you?
Children’s Health Serviceshealth • care • people
Session 3: Cognitive Re-Structuring
• Aim of this session is to enable the YP to move from a position of self-blame and responsibility for the trauma to a position of being able to place the blame and responsibility with the perpetrator
• Many YP blame themselves for being unable to stop the trauma
• Facilitate YP need to gain a realistic view of their experience
Children’s Health Serviceshealth • care • people
Realistic View
1. YP not to blame for what they have experienced
2. They could not have stopped the trauma from occurring
3. Responding to the trauma in a maladaptive way is allowing the perpetrator to win / retain control
Children’s Health Serviceshealth • care • people
Addressing the Blame
• Question the YP in a manner that challenges their thoughts– “If you were talking to an X yr. old child who
experienced what you have, would you blame them?– “What would you say to them?”– “If you were an X yr. old child and the perpetrator was
an adult, who would be to blame?”
Children’s Health Serviceshealth • care • people
Addressing the Blame (cont)
– “Children are brought up to obey adults. If an adult tells you to do something, are you really going to say no?”
• At what age does this change?
– “Children trust adults. Do you think a child is going to question what an adult says or does?”
• At what age does this change?
Children’s Health Serviceshealth • care • people
Addressing the Maladaption
• Reframe the maladaptive coping mechanism– “How have you coped with what has happened?”
• DSH• Substance use• Promiscuity etc
– “Is this helping or hurting you?”– “What other ways might you cope?”– “What would you suggest to other YP?”
Children’s Health Serviceshealth • care • people
Session 4: Symptom Management
• Aim of this session is to identify strengths and resilience YP possess that has allowed them to survive the trauma
• YP often are unable to see any positives about themselves – Self-blame they have developed about the trauma.– Toxic environment, few supports etc
• The goal in this session is assist the young person to identify these positives.
Children’s Health Serviceshealth • care • people
Focus on the Positive
• What do you do when you have …………. (flashbacks, nightmares, intrusive thoughts, etc.)
• What have you found to help the most?• What would you tell other young people to do?• How have you been able to survive all of this
– What does that tell you about yourself?– Did you ever think you possessed those strengths?
• I am amazed at how you have been able to cope. What other coping methods have you used?
Children’s Health Serviceshealth • care • people
Medication
• Emerging evidence of some SSRIs and atypical antipsychotics
• Quetiapine (low dose)– Sedation– Reduction in re-enactment phenomena– Reduced affective lability
• Blinded trial of Quetiapine and Fluvoxamine
Children’s Health Serviceshealth • care • people
Evaluation
• Pilot program• MAYSI as a screening tool• TSCC beginning and end• ?Other instruments
• Watch this space!
Children’s Health Serviceshealth • care • people
Future
• Medication vs. Therapy alone
• Individual vs. Group Therapy – Group therapy is risky in detention– Not a debrief
• Most of what passes as psychological debriefing has essentially been debunked
Children’s Health Serviceshealth • care • people