Embed Size (px)
Citation preview

CHINA’S POOR AND POOR POLICIES: THE CASE OF RURAL HEALTH INSURANCE
Yuanli Liu* William C. Hsiao
Program in Health Care Financing Harvard School of Public Health
To be presented at the Conference on
Financial Sector Reform in China September 11-13, 2001
* Corresponding author. 124 Mount Auburn Street, Fourth Floor South, Harvard School of Public Health, Cambridge, MA 02138; Phone: 617-496-8841; Fax: 617-496-8833; Email: [email protected]

China’s Poor and Poor Policies: The Case of Rural Health Insurance
(abstract)
Thanks to continued economic growth and increasing income, the overall poverty rate has
been on decline in China. However, due to medical cost escalation and lack of insurance
coverage, catastrophic medical spending constitutes an increasingly important cause for poverty
in rural areas. In 1993, the insurance coverage for the rural residents was already low (12.8%).
By 1998, only 9.5% of the rural populations were insured. Ever since collapse of the once
successful Cooperative Medical System (CMS) in the early 1980s when China transformed its
system of collective agricultural production to private production, many rural communities,
especially the poor, faced several major problems. User charges and high direct costs effectively
block access for many rural residents who lack adequate income to purchase basic healthcare
when it is needed. Using the 1998 National Health Services Survey data, we estimated impact of
medical expenditure on the poverty headcount for different rural regions. Based on the reported
income statistics alone, the headcount for the whole rural sample is 7.22%. Out-of-pocket
spending on healthcare has raised the headcount by more than 3 percentage points. In other
words, medical spending raised the number of rural households living below poverty line by
44.3%. Why has there been no vigorous development of a rural health insurance system in
China? This paper provides a systematic review of the underlying factors affecting the initiation
and sustainability of China’s rural health insurance system, and discusses inadequacies of current
policies.
2

1. Introduction*
During its two decades of economic system reform, China has achieved remarkable
agricultural and industrial growth. Since 1978 aggregate gross domestic product (GDP) has
grown at an average annual rate of 10 percent; agricultural GDP, at 5.2 percent; and rural
industrial output, at 31 percent (The World Bank, 2000). The world community is also deeply
impressed by China’s achievements in reducing absolute poverty. Government’s estimates of the
incidence of absolute poverty demonstrate a significant drop from 270 million people in 1978 to
about 60 million in 1997. The number of rural poor declined from around 1/3 of the total rural
population in 1978 to roughly 1/20 at the end of 1998 (MOA, 2000). However, China’s growth
pattern has led to a rising income disparities between the resource poor inteior and western
regions on the one hand, and the more affluent and rapidly growing coastal areas on the other
(World Bank, 1997). In 1994, China launched a far-reaching poverty reduction strategy under the
8-7 Plan, which targets 592 nationally designated poverty counties. It’s objective is to raise per
capita incomes to 500 yuan (in constant 1990 prices) for about 80 million poor living in absolute
poverty, within 7 years. The impact of the 8-7 Plan has been significant. Since it’s adoption,
poverty has fallen markedly according to China’s own estimates. Not withstanding the progress
to-date, China faces a great challenge to lift the remaining poor out of poverty. It is well known
to the policy-makers and public at large in China that an increasing share of the remaining poor
are now concentrated in China’s western provinces, and mostly within resource deficient areas.
That is why the latest poverty reduction and economic development programs have focused on
3
* This paper draws, in part, on a research report TOWARDS ESTABLISHING A HEALTH PROTECTION SYSTEM FOR RURAL CHINA, presented by Liu, Y. et al at the Conference on China’s Rural Social Security, held by the ADB and the China State Development and Planning Commission in Beijing on July 9-10, 2001.

developing China’s western regions. Less well known, however, is the increasing importance of
transient poverty, which cannot be adequately addressed by the past and current strategies.
Some of the poverty observed at one date is temporary due to a short-lived drop in the
individual levels of living, and thus termed “transient poverty”. For other poor households,
poverty arises from low long-term welfare (“chronic poverty”). Therefore, different policies may
well be called for dealing with these two types of poverty. Longer term investment in the poor,
such as increasing their physical and human capital, are likely to be more appropriate for
reducing chronic poverty. On the other hand, insurance and income-stabilizing schemes, which
protect households against idiosyncratic economic shocks, may be needed to address the
transient poverty problems (Jalan and Ravallion, 1997). Using panel data from 4 provinces,
Ravillion (1998) estimated that about half of the average severity of poverty was directly
attributed to inter-temporal variability in consumption, and the exposure to income risk in this
setting is also significant. So, transient poverty would appear to be a serious concern in China.
However, China’s anti-poverty strategy has given more emphasis to fighting chronic poverty
than transient poverty. For example, most of the poverty reduction programs focus on reducing
poverty by promoting income-generating investments in local agriculture and rural development,
rather than providing short-term insurance or state-contingent transfers. An illustrative case in
point is the lack of rural health insurance, a problem that has persisted ever since the inception of
agricultural reforms in the early 1980s.
To understand China’s rural health insurance system, one has to understand the role and
function of “The Rural Cooperative Medical System” (RCMS). Unlike other transitional
economies with a legacy of providing universal access to publicly funded and provided health
services, financing of healthcare for the rural populations in China has been left to the local
communities. Under the old command economy, RCMS was developed as a community-based
4

prepaymen system. The RCMS was an integrated part of the overall collective system for
agricultural production and social services. Under RCMS, the financing of health care relied on
a pre-payment plan. Most villages funded their RCMS with three sources: (1) premiums—
depending on the plan’s benefit structure and the local community’s economic status, 0.5 to 2
percent of a peasant family’s annual income (4-8 yuan) was paid to the Fund; (2) collective
welfare fund—according to State guidelines, each village contributed a certain portion of its
income from collective agricultural production or rural enterprises into a welfare fund; (3)
subsidies from upper-level governments. In most cases, this subsidy was used to compensate
health workers and purchase medical equipment. During the peak period of the RCMS’s tenure
(1970s), 90% of the rural populations were covered under this prepayment schemes. However,
after the agricultural reform in the early 1980’s, this community financing system collapsed in most
of the rural areas (Gu et al, 1997; Liu et al 1995). There have been efforts to revitalize RCMS since
then. In 1996, the Central Party Committee and the State Council held China’s first national health
policy conference, and announced that voluntary RCMS schemes should be established and
improved as a major strategy to provide rural health insurance coverage (MOH, 1997). But very
little progress has been made to date.
This paper focuses on rural health insurance in the context of poverty reduction for several
reasons. First, a health insurance system functions as an income-protection mechanism when the
need arises for medical treatment that requires large expenses. Second, insurance buys access to
health care services for the low-income people, who otherwise may not be able to afford them.
Since health is an important dimension of human capital in poverty reduction and healthcare has
important role to play in saving lives and improving health, providing health insurance coverage
would appear to serve the purposes of income-protection and human capital-enhancing. Third, no
matter what definitions are used, majority of the Chinese populations live in rural areas. While
5

urban insurance system is being established as one of the government’s top policy priorities, very
little progress has been made with regard to rural health insurance system. Currently, more than
80% of the rural populations are still uninsured. They have to pay for healthcare services totally
out-of-pocket. High medical charges effectively block access to care for many poor households,
and cause financial hardships for others. Is lack of rural health insurance really that serious a
problem? Why has the governments or society have not taken effective actions to remedy the
problem? In the following sections, this paper will first provide statistical evidence on the
problems associated with lack of rural health insurance, especially the poverty impact. Then, it
discusses major factors that hinder development of China’s rural health insurance system. Only
when these factors are clearly understood, effective strategies can be developed to help solve the
problems.
2. Problems Associated With Lack of Rural Health Insurance
2.1 Medical cost increase and lack of insurance
Table 2 summarized the levels and sources of total health spending in China. While total
health spending as percentage of GDP increased from 3.17 percent in 1980 to 4.82 percent in
1998, the government share of the total spending, rather against international trend, decreased
from 36.4 percent in 1980 to 15.5 percent in 1998. Over the same period of time, the private
share of the total spending increased from 23.2% to 57.8%. An international comparison of
growth of economy in relation to out of pocket expenditures on health as a share of total health
expenditure shows China to be in stark contrast to most comparable economies (Table 2). The
table shows that as countries develop and their economies grow, the governments assume a
larger share of health spending, thus resulting in lower out of pocket health expenditures. Among
6

the listed countries, many of which with smaller economies and per capita incomes, China's
private share of total health expenditures are highest.
Table 1: Health Care Spending in China ( 1980 - 1998)
1980 1990 1991 1992 1993 1994 1995 1996 1997 1998
% of GDP spent on health 3.17 4.01 4.11 4.09 3.96 3.78 3.86 4.2 4.55 4.82
Total Health Expenditure (Billion Yuan) 45.1 138.4 155.1 176.5 193.6 208.5 235.2 280.9 330.3 377.6
% of Total Health Expenditure by Government 36.4 25 22.8 20.8 19.7 19.2 17 16.1 15.4 15.5
% of Total Health Expenditure by Individuals (out of pocket) 23.2 37.1 38.8 41.1 43.4 45.6 50.3 54.4 56.8 57.8
% of Government Health Spending on Public Health 76.1 75.1 74.3 71.6 72.8 70.6 70.5 69.4 69.9
Source: HEI, 1990 - 1998 National Health Accounts
Table 2. International Comparison of Per Capita GDP and Out of Pocket Expenditures on Health
Per Capita GDP (PPP US$) 2
Total Expenditure on health as % of GDP 1
Out of Pocket Exp as % of total health expenditure 1
United States 30041.07 13.7 16.6 Japan 25372.77 7.1 19.9 Germany 22678.15 10.5 11.3 Sweden 21209.77 9.2 22.0 United Kingdom 20998.15 5.8 3.1 Korea 15306.59 6.7 43.0 Malaysia 8556.40 2.4 42.4 Russian Federation 7190.76 5.4 23.2 Thailand 6575.07 5.7 65.4 Philippines 3869.93 3.4 49.1 Indonesia 3217.83 1.7 47.4 China 3152.87 2.7 75.1 Sri Lanka 3035.29 3.0 51.8 Zimbabwe 2812.20 6.2 38.2 Bangladesh 1381.50 4.9 54.0
Despite escalating medical costs, insurance coverage in China is miniscule. According to
China’s two national health services surveys conducted by the Ministry of Health, percentage of
population with any health insurance decreased from 30.2% in 1993 to 23.6% in 1998 (MOH,
1994; MOH, 1999). The problem is particularly pronounced for the rural population. In 1993, the
7

insurance coverage for the rural residents was already low (12.8%). By 1998, only 9.5% of the
rural populations were insured (Table 3). That means, currently majority of the rural residents
have to pay out-of-pocket for any health service they need. Rapid medical cost escalation has
made health care unaffordable for many people.
Table 3: Medical Costs and Insurance coverage
1990 1995 1999 % Change (1990 - 1999)
Medical Costs * Per visit 10.9 39.9 79 625%
Per admission 473.3 1668 2891.1 511% Insurance Coverage**
Urban 53.73 42.09 -22% Rural 12.83 9.58 -25%
Data Source: * Ministry of Health, 2000 National Health Statistics ** Ministry of Health, 1993 & 1998 National Health Services Survey
Ever since the 1980’s, China's annual health expenditure has increased at a rate consistently
higher than economic growth rate. China’s total health expenditure could rise from the current
4.8 percent of GDP to more than 10 percent of GDP by the year 2020, due to the aging of the
population, lifestyle changes, medical price inflation, and environmental pollution (Rao et al,
2000). This, combined with the problem of lack of insurance coverage, has caused health care
utilization in China to fall, despite the increasing supply of health care facilities. Large medical
expenses can also cause financial catastrophe. Numerous community surveys indicated that
medical expenses have become the number one poverty generators (Yuan and Wang, 1998; The
State Council Research Office, 1994).
8

2.2 Poverty impact of medical expenditures
Different proportions of income spent on healthcare for different income groups reflect
redistributive effect: namely, indicating how income inequality is affected by out-of-pocket
payments for healthcare. It does not indicate whether these payments push households into
poverty. Ever since collapse of the once successful Cooperative Medical System (CMS) in the
early 1980s when China transformed its system of collective agricultural production to private
production, many rural communities, especially the poor, faced several major problems.
Currently 90 percent of the rural population are uninsured, and they pay out-of-pocket for any
health service they receive. User charges and high direct costs effectively block access for many
rural residents who lack adequate income to purchase basic healthcare when it is needed. Lost
workdays and bed-ridden days in poor rural areas are twice as high as the national rural average.
Moreover, Medical expenses can cause financial catastrophe. According to a survey study on
China's rural poor (Liu and Hu et al., 1996), about 18 percent of the rural households that used
health services incurred health expenditures that exceeded their total household income. Of the
11,353 rural households interviewed, 24.3 percent borrowed or became indebted for health
expenses. Another 5.5 percent sold their meager assets in order to pay for health care. Forty-
seven percent of the medically indebted households reported having suffered from hunger for
extended period of time. When households have large debts, their investment in agricultural
production and subsequent living standards decline, which adversely affects the health status of
the household members. This interaction between income and health sets off a vicious cycle of
illness that produces poverty, which, in turn, causes more illness.
There have been numerous surveys conducted in China trying to measure the extent of
“illness-induced impoverishment”, namely addressing the question of how many of the poor
9
households have become poor due to illnesses (Yuan & Wang, 1998; The State Council
Research Office, 1994). Most of the locally administered surveys indicated that illness is the
number one poverty generator. However, results of these surveys cannot be generalized for the
whole country, because they are not based on representative samples of the nation. The 1998
National Health Services Survey is the first national survey, which asked questions about the
major reasons for impoverishment (MOH, 1999). Among the 40,210 rural households surveyed,
2,036 households (5.06%) are identified as households living under poverty by the local
government agencies. These poor households are then asked to list the major reason for their
impoverishment, and they are given a multiple choice of five reasons: lack of labor, poor
ecological conditions, natural disaster such as draught, social reasons, and diseases or injuries.
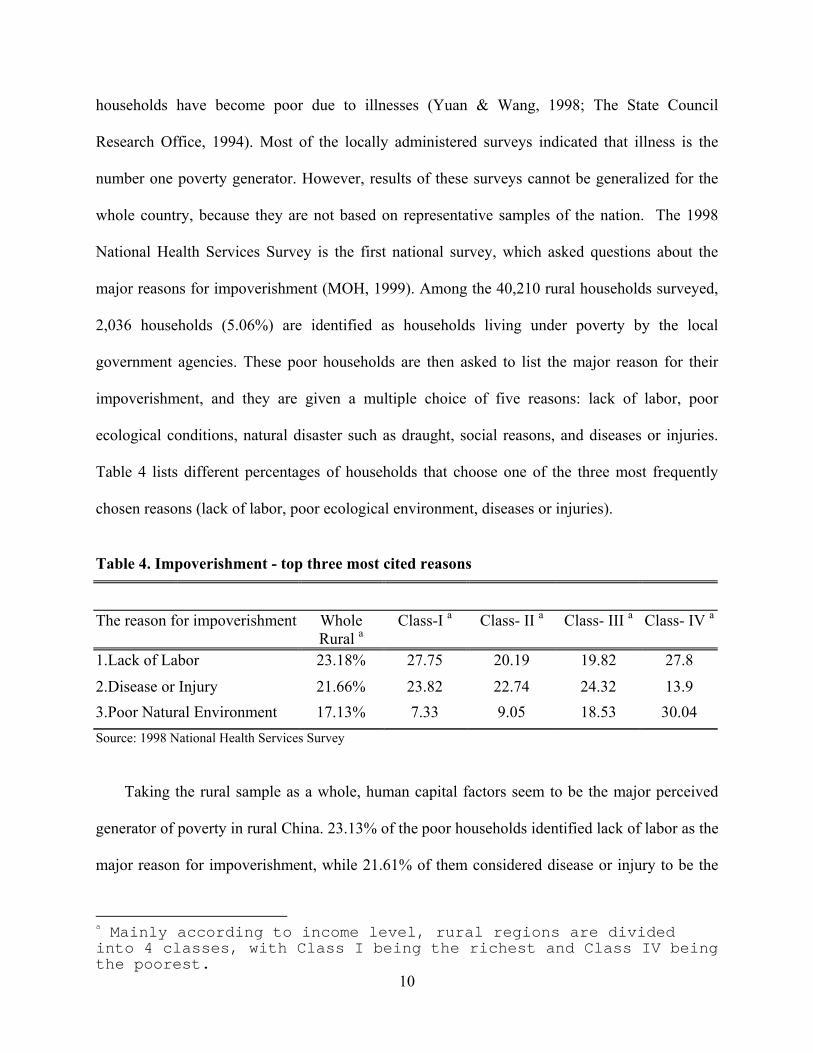
Table 4 lists different percentages of households that choose one of the three most frequently
chosen reasons (lack of labor, poor ecological environment, diseases or injuries).
Table 4. Impoverishment - top three most cited reasons
The reason for impoverishment Whole Rural a
Class-I a Class- II a Class- III a Class- IV a
1.Lack of Labor 23.18% 27.75 20.19 19.82 27.8
2.Disease or Injury 21.66% 23.82 22.74 24.32 13.9 3.Poor Natural Environment 17.13% 7.33 9.05 18.53 30.04 Source: 1998 National Health Services Survey
Taking the rural sample as a whole, human capital factors seem to be the major perceived
generator of poverty in rural China. 23.13% of the poor households identified lack of labor as the
major reason for impoverishment, while 21.61% of them considered disease or injury to be the
10
a Mainly according to income level, rural regions are divided into 4 classes, with Class I being the richest and Class IV being the poorest.

major poverty generator. Only 16.94% of the poor households blamed the poor natural
environment for their lot. Even though we cannot conclude from the 1998 survey, that diseases
or injuries is the number one poverty generator from the rural population’s point of view, there
are two strong reasons for us to be concerned about the major poverty impact of illnesses. First,
the most frequently cited reason for poverty is lack of labor. If the bread-earners suffer from
illness (especially during the planting and harvesting seasons) or the families should lose their
bread-earners due to illnesses, the economic consequences are dire. As depicted by Figure 1
workdays lost per thousand increased for all the rural regions over the period of 1993-1998. This
gives an alarming indication of the increasing economic burden of diseases via impairing the
rural labor. Second, while for the whole rural population, diseases or injuries ranked number two
for poverty generation, the number one poverty generator perceived by the poor households in
middle-income regions (class II and class III) are diseases or injuries. Majority of the rural
population in China lives in class II and class III regions.
Figure 1: Work Days lost due to Illness per 1000 working adults ( 2-week period)
050
100150200250300350400450
Urban Rural (avg) Rural- I Rural -II Rural-III Rural-IV
Source: Ministry of Health, China National Health Services Survey, 1993 & 1998
19931998
11

Answers provided by poor households regarding their perceived poverty generators, no
matter how informative they are on the poverty impact of ill-health, do not distinguish the
poverty impact through labor-impairment effect from that through catastrophic medical
spending. Due to data limitations, we cannot ascertain the poverty impact of ill health through
the pathway of labor performance. We can, however, examine the poverty impact of medical
expenditures, based on further analysis of the household survey data from the 1998 National
Health Services Survey. Figure 2, adopted from Wagstaff (2000), provides a simple framework
for examining the impact of the out-of-pocket payments on the two basic measures of poverty –
the headcount and the poverty gap. The head count measures the number of individuals or
households living below the poverty line as a percentage of the total population/ households. The
poverty gap measures the total amount of income transfer that is needed to lift all the poor
households out of poverty. The chart is a variant of Pen’s parade, named after the Dutch
economist Pen who invented it. Pen’s parades plot household income (before and after medical
payments) along the y-axis against households ranked by prepayment income along the x-axis.
Reading off the parade at the poverty line gives the number of households living below poverty-
the headcount. The area below the poverty line above the parade gives the poverty gap (the total
shortfall from the poverty line).
12

Income A C B Poverty line
Postpayment
Prepayment
H0 H1 Cumul % smpl Figure 2. Pen's parade showing the impact of the out-of-pocket payments on the two basic measures of poverty – the headcount and the poverty gap. In the case of the prepayment parade the headcount is H0 and the poverty gap is equal to the
area A. In the post-payment parade, assuming the poverty line is held constant, the headcount is
H1 and the poverty gap is equal to the area A+B+C. Area B represents the deepening poverty
experienced by households who were poor before medical payments. Area C corresponds to the
addition to the poverty gap caused by households who were not poor before payments but are
poor after their out-of-pocket payments. Figure 3 shows the estimated impact of medical
expenditure on the headcount for different rural regions. The headcount for the whole rural
sample is 7.22%. Out-of-pocket spending on healthcare has raised the headcount by more than 3
percentage points. In another word, medical spending raised the number of rural households
living below poverty line by 44.3%. Not surprisingly, the biggest percentage point increase
(4.21%) of headcount due to medical spending occurred for households living in the poorest
regions, driving up the total headcount to about 30%.
13
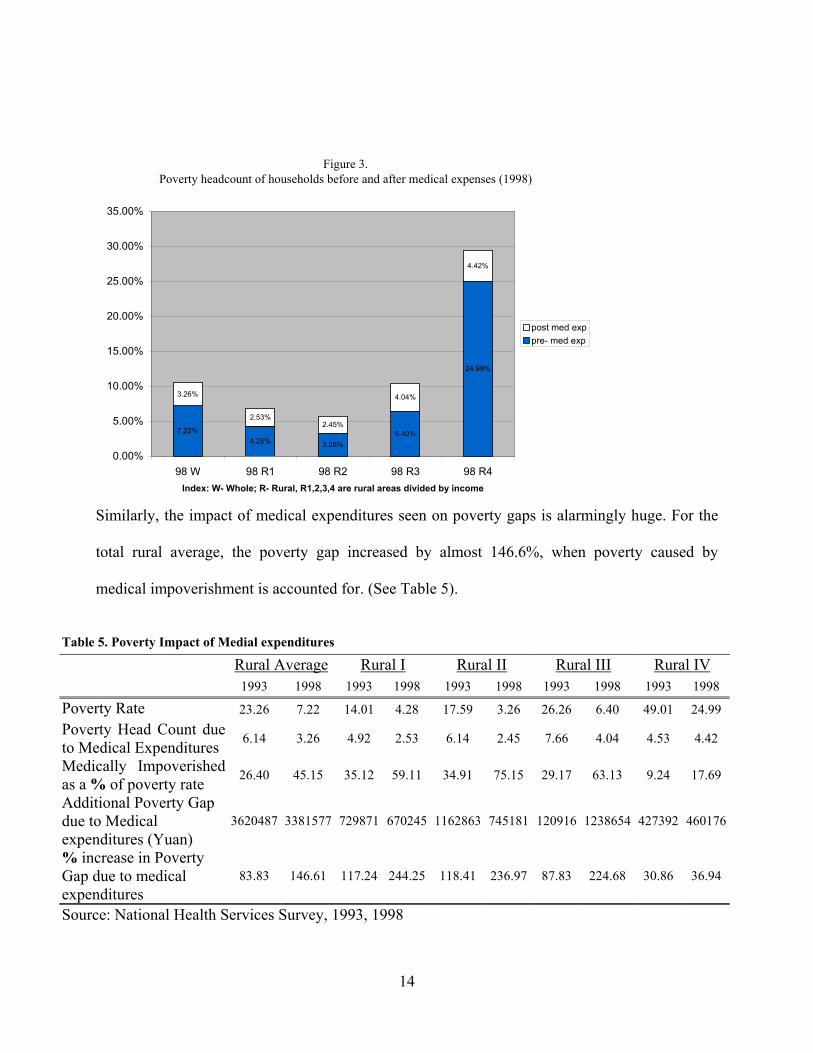
Figure 3. Poverty headcount of households before and after medical expenses (1998)
7.22%4.28% 3.26%
6.40%
24.99%
3.26%
2.53%2.45%
4.04%
4.42%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
98 W 98 R1 98 R2 98 R3 98 R4Index: W- Whole; R- Rural, R1,2,3,4 are rural areas divided by income
post med exppre- med exp
Similarly, the impact of medical expenditures seen on poverty gaps is alarmingly huge. For the
total rural average, the poverty gap increased by almost 146.6%, when poverty caused by
medical impoverishment is accounted for. (See Table 5).
Table 5. Poverty Impact of Medial expenditures
Rural Average Rural I Rural II Rural III Rural IV 1993 1998 1993 1998 1993 1998 1993 1998 1993 1998
Poverty Rate 23.26 7.22 14.01 4.28 17.59 3.26 26.26 6.40 49.01 24.99 Poverty Head Count due to Medical Expenditures 6.14 3.26 4.92 2.53 6.14 2.45 7.66 4.04 4.53 4.42
Medically Impoverished as a % of poverty rate 26.40 45.15 35.12 59.11 34.91 75.15 29.17 63.13 9.24 17.69
Additional Poverty Gap due to Medical expenditures (Yuan)
3620487 3381577 729871 670245 1162863 745181 120916 1238654 427392 460176
% increase in Poverty Gap due to medical expenditures
83.83 146.61 117.24 244.25 118.41 236.97 87.83 224.68 30.86 36.94
Source: National Health Services Survey, 1993, 1998
14
The gap increased by over 200% in rural area 1,2 and 3 in 1998. Even though the poverty rate as
well as poverty head count due to medical expenses decreased from 1993 to 1999, reflecting
increases in income, the relative poverty impact of medical expenses increased. For example, in
1993, the number of households who were medically impoverished as a percentage of the total
number of households living under poverty was 26.4%. By 1998, it had gone up to 45.1%.
3. Major Factors Affecting Development of Rural Health Insurance
If the need for a rural health insurance system is real and serious, as indicated in the above
discussions, a question naturally arises: why there has been no vigorous development of such a
system in China? Given China’s vast rural population and very much decentralized economic
and fiscal system, it is inconceivable that China will develop an one-size-fits-all nationalized
system of health insurance for all the rural population any time soon. China’s current policy is to
build on the RCMS models, and gradually increase the coverage of China’s rural population
under the RCMS. However, RCMS as a community-based risk-sharing scheme is subject to
variations in socioeconomic development across communities. Ever since the economic system
reforms in the early 1980s, no remarkable progress has been made in RCMS development.
Therefore, a thorough understanding of the factors affecting RCMS development in China helps
us understand major issues underlying development of China’s rural health insurance systems.
Economic theory posits, if an insurance market is to be developed, as assumed by the current
policy of pursuing voluntary community prepayment schemes, then there has to be effective
demand and adequate supply (Phelps, ). In studying external socioeconomic and internal
organizational factors pertaining to CMS, we have identified four major conditions for setting up
and sustaining China’s rural health insurance systems. These conditions include the levels of
economic development, people’s willingness to participate in the system, proper ways of
15

organization and management, and government support. Elsewhere (Liu et al., 2001) we have
analyzed extensively issues related to demand for RCMS. Here we focus on supply-side issues.
We will argue that given it’s social, economic, and political context, China’s current policy of
relying on voluntary community actions to develop rural health insurance is inadequate, and
moreover, irresponsible.
3.1 Variations Across Rural Communities
International experiences have shown that both individual and collective spending on health
increase with economic development, thus demand for health protection is also increasing
(World Bank 1993; WHO, 2000). This trend is further accompanied by enhanced capabilities to
organize health protection systems, as economy improves. Therefore, it is not surprising to find
that the percentage of China’s rural population either insured by social insurance and private
insurance schemes or covered by the CMS schemes vary across regions with different levels of
economic development (Table 6). For example, 26 % of the residents living in high-income
regions had health insurance coverage in 1998, whereas only 18 % of the poor rural residents had
any insurance coverage in 1998. The differences in the insurance coverage are found to be
associated with inter-regional differences in individuals’ ability to pay (e.g. per capita income),
potentials for organized financing (e.g. village collective fund and township government
revenue), and healthcare supply conditions (e.g. drug supply at the village health posts) (see
Table 6). In the following section we discuss different patterns of rural health protection systems
in high-income, middle-income, and low-income regions in China.
16

Table 6. Rural Health Protection system and correlates in different regions
Factors Rural Average Rural I Rural II Rural III Rural IV 1993 1998 1993 1998 1993 1998 1993 1998 1993 1998
% of Residents Insured 15.8% 12.6% 35.8% 26.6% 11.9% 7.6% 4.6% 5.2% 16.9% 18.5%
% of Residents covered under CMS
9.8% 6.5% 28.7% 20.8% 9.1% 3.7% 0.7% 1.6% 1.0% 1.8%
Village Industry Output Value (10,000 Yuan)
163 524 396 1161 91 621 54 116 4 7
Income per capita (Yuan) 684 1759 920 2591 667 2085 488 1257 361 884
Town Government Revenue (10,000 Yuan)
247 465 325 1050 246 318 244 262 87 136
Drug supplies at village post (kinds)
119 139 136 150 120 138 117 149 65 92
Source: National Health Services Survey, 1993, 1998
3.1.1 Health insurance systems in high-income rural regions
The income spectrum in China coincides with the three broad geographic regions – the
eastern coastal regions (especially the Yangzi delta region), the central region, and the western
region – a scheme of regionalization adopted in the Seventh Five Year Plan (1986-1990) and
commonly employed by students of China’s regional development ever since. Rural health
protection systems in China’s high-income region are characterized by their strong collective and
government support, comprehensive coverage with emphasis on hospital insurance, and
modeling after the urban health protection system reforms.
The levels of private contributions to the rural protection system are higher in the high-
income regions, compared to their counterparts in middle- and low-income regions. Also
remarkable are supports from the local industries and governments. One of the most successful
cases in rural health protection system development can be found in Suzhou City1. Ever since the
collapse of the CMS schemes after the agricultural reforms, governments in Suzhou at the city,
17
1 Description of the Suzhou experiences in rural health protection system draws on Liu and Rao’s meetings with and documents from the local officials during a field trip on April 19-20, 2001.

county, and township levels realized the problems of lack of rural health protection systems, and
put revitalizing and strengthening CMS schemes high on their policy agenda. Governments
provided leadership in mobilizing contributions from the individuals and local industries by
matching funds. On average, farm families contributed 15-20 yuan per capita annually to the
township-managed CMS funds. Almost equal amounts of contributions were made by the
township industries and township governments. On top of these, the county and city
governments provided 2-10 yuan per CMS members, mainly to finance catastrophic medical
expenses by the CMS members. Half of the funds are earmarked as hospital insurance fund used
to cover catastrophic medical expenses. The risk-pool for small expenses (e.g. outpatient
expenses) is at the township level, while the risk-pool for large medical expenses (e.g. hospital
expenditures exceeding certain threshold) is managed at the county/city level. For the past five
years, the enrollment rate of the rural population in the rural health protection system in Suzhou
has been kept at more than 70%. In 1999, the membership was as high as 313, 000. As an
illustration for Suzhou’s financing patterns, Table 15 depicts developments in Qunshan City for
the period of 1997-1999.
Table 7. CMS in Qunshan City
Funding Source (%)
Per Capita
Income
Rural
Residents
Enrollment
Rate City Town Collective Household
1997 4786 420367 72% 4.9 4.2 18.5 73.2
1998 5031 409685 75% 4.5 3.9 19.7 71.9
1999 5175 397361 73% 5.3 5 21.2 68.5
Another trend in high-income regions is gradual merge of the urban and rural health
protection systems. Even though we have yet to find a completely integrated urban-rural system, 18
operations of urban and rural health protection system have been increasingly inter-related. First,
the organizations for operating the two systems are no longer totally separate. For example,
commercial insurance carriers such as The People’s Insurance Company, which have been
selling hospital insurance policies to the urban dwellers, began to penetrate the rural market.
Consequently, as seen in the 1993 and 1998 surveys, the percentage of rural residents obtaining
private insurance coverage, though still a small proportion of the total population, increased over
the years. Since 1996, Shuide city government in Guangdong Province has been operating a
hospital insurance scheme, with compulsory participation by the industrial workers and
voluntary participation of the rural farmers. Depending on their levels of premium contributions
(instead of official “urban” or “rural” status), people got different benefit packages. Second,
some schemes exercised cross-subsidization policies (e.g. transferring benefits from the
industrial workers to rural farmers as in the case of Qunshan). Third, the urban social insurance
model of combining Individual Medical Savings Account (IMSA) and social risk pooling is
introduced in the rural health protection systems. Setting up a revised MSA – Family Medical
Savings Account (FMSA) as part of the reformed rural health protection systems in some
communities in Suzhou (e.g. Qunshan) and Shanghai (e.g. Nanhui County) is aimed at further
promoting a multi-tiered rural health protection system by targeting those households who are
able to make the prepayment but have a low willingness to share financial risks with non-family
members of the larger community.
3.1.2 Rural health insurance systems in middle-income regions.
The middle-income (per capita income of about $713) regions cover large parts of China –
central region provinces and provinces in the northeastern regions. These regions vary a great
deal in rural agricultural and industrial development. So the individual as well as collective
funding capabilities also vary. This indicates greater need as well as potential for spreading the
19
financial risks among different population groups. These regions also have the largest cultural
varieties such as mix of the ethnic groups. These cultural diversities, if effectively taped as social
resources, can turn out to be advantages in developing rural health protection system. More
detailed discussion on this aspect will come later. Unlike their counterparts in high-income
regions with a large industrial base and in low-income regions with significant transfer payment
by upper level governments, the government revenue (thus the budget for social spending) is
very limited in these regions. As a result, funding and management models of rural health
protection systems in middle-income regions vary from community to community. Most of the
funding, however, comes from the household contributions. Compared to the health protection
systems in high-income regions, most of the risk pools are much smaller, often operating at the
village levels. CMS schemes in Jianyang and Meishan of Sichuan Province represent one of the
earliest efforts to revitalize CMS in rural areas in the post-reform era. With technical assistance
provided by the RAND Corporation and the Chinese Ministry of Health, the Jianyang-Meishan
project aimed to provide operational experiences in organizing rural healthcare financing under a
market economy and basing medical cost prediction and thus benefit design on a more sound
actuarial foundation. Initial experiences indicated that the CMS schemes found wide support
among the rural farmers (Jiang et al, 2000). However, the schemes were interrupted twice in
1993 and 1998, because the State Council forcefully carried out the tax-relief policies for the
farmers, and thus rendered local CMS schemes illegal. Another example of the vulnerability of
CMS schemes in these regions can be found in Henan Province. In 1996, the National Work
Meeting on Rural CMS was held in Kaifeng and Linxian, where the percentage of villages under
CMS was as high as 90%. In 1997, however, the Ministry of Agriculture issued a policy
document regulating what items can be taxed locally and what not. This document included fund
collection for CMS schemes in it’s “black list” of items, for which local taxes were not allowed.
20

This prompted disband of many CMS schemes, which were considered as models for other rural
regions to follow merely a year ago.
3.1.3 Rural health insurance systems in low-income regions
Despite of their greatest need, low-income regions in China face the most difficult situations
in the process of developing rural health protection systems. On the one hand, low-income
communities have the least capabilities (among the three types of regions in China) to initiate
and sustain rural health protection systems on their own, due to limited financial and
organizational resources. On the other hand, the same of amount of government support may
have the biggest marginal impact in these regions than in other regions. This is not only because
the expectations for the rural health protection system are generally low to begin with. This is
also because low income regions are less mobile and thus socially more cohesive than other
regions, making people in those communities more responsive in terms of reciprocating with
their own contributions to the system, if outside support is provided and individual contributions
are set at an affordable level. Two cases below help illustrate these two points.
The 10 Poverty County Intervention Study
Since 1993, the UNICEF has been supporting an applied study on Financing and Provision
of Health Care for China's Rural Poor (Liu, 2000). Under the leadership of the Ministry of
Health and supported by hundreds of local officials and health workers, this project was carried
out by the China Network for Training and Research in Health Care Financing and Economics in
collaboration with Harvard School of Public Health (Technical Teams). The project has two
phases: phase 1 (1993-1996) involved survey studies on 114 poverty counties to make a
comprehensive diagnosis on major problems and opportunities, and phase 2 (1997-2000) focused
on CMS interventions in 10 poverty counties in 8 provinces. The interventions on the grounds
involved a process of many interactive activities, including selecting intervention sites in 1996
21

(2-3 intervention townships and a control township were selected in each of the 10 counties),
conducting baseline surveys on 3,103 households in 1997, detailed design of the CMS benefit
and management structure, social marketing campaigns and fund collection, regular site visits (2-
3 times a year) for monitoring purposes and technical assistance by the Technical Teams, and the
evaluation survey in July 2000.
0
20
40
60
80
100
Enrollment
1997 1998 1999Year
Fig. 4 Enrollment Max Mean Mi n
Figure 4 summarized the average level and range of overall enrollment rate in 1997, 1998, and
1999. Both the enrollment rate and premium levels declined over the intervention period. Even
though all the project counties managed to establish CMS in the intervention townships, the
operation of the CMS schemes in the past three years have been very unstable. Except for two
townships (Huang Yang Shan of Gulang county in Gansu province and Hung Jia Wuan of Zhen An
county in Shanxi province), which steadily increased their rate of CMS enrollment, more than half
of the intervention townships experienced a rate decrease. Some townships (such as Long Jiang of
Longlin County in Yunan province) even experienced over 50% drop in CMS membership during
the course of the intervention study. Townships in Yunan and Guizhou provinces were never able to
22

enroll more than 40% of the farm families into CMS. What are the major factors underlying the
process? Following factors are found to be important: people’s ability and willingness to pay,
organization and management issues, and government support and policy constraints. Many of the
families (20%) in our intervention sites are poor. The per capita income of the surveyed households
in our sample in 1999 was 1,651 yuan, which was about 20% lower than the 1998 per capita
income in rural China. About 12% of the families reported negative cash flow. Lack of income
certainly limited people's financial capacity to contribute to the CMS fund. Without exception, all
the townships that have experienced disastrous weather changes (flood or drought) also experienced
significant drop of enrollment rate. Therefore, without external financial assistance, CMS in poor
rural areas is bound to have two characteristics: it is either very difficult to establish a CMS scheme
with very limited benefit package, or the established scheme is financially vulnerable.
The CMS in Tibet. With direct support and subsidies from the central government, residents in
Tibet Autonomous Region (TAR) had been receiving healthcare services from the publicly owned
and operated facilities free of charge until 1997. The “free care” system suffered from under-
funding, under-supply, and inefficiency problems. To correct for these system deficiencies, the
TAR government initiated health-financing reforms since 1997. The TAR government used the
subsidies from the central government, which used to be allocated directly to the healthcare
providers, to set up the township CMS funds. On average, the contributions by the governments to
the funds amounted to 15-30 yuan per capita. The households are also required to prepay into these
CMS funds, and they pay on average 10-20 yuan per capita (representing 1.5-3%of their annul per
capita income). For those poor households who cannot afford to pay the CMS premiums, county,
township governments, and village collectives will share the premium payments according to a
specified formula (50% of the premium costs are paid for by the county governments, 30% by the
township governments, and 20% by the village collective funds). By 1999, CMS schemes were
23

established in 66 counties and 455 townships covering 54.8% of the population in TAR. Initial
evaluation studies indicated that establishment of CMS schemes improved people’s access to
primary as well as tertiary care services, and enhanced funding and quality of healthcare provision
in Tibet (Cheng and Fan, 2000). Experiences from Tibet clearly indicated that with strong
government support matched by contributions from the households and local communities, rural
health protection systems can be established in poor rural areas.
3.2 Government Policies and Rural Health Insurance System
China’s own experiences clearly indicate that strong government support is necessary for
establishing and sustaining wide coverage of rural health protection systems. Some policy makers,
especially those in support of a “voluntary” community-based rural health protection system, hoped
that with economic growth people’s demand for health protection will increase, and this increasing
demand will automatically lead to community initiatives to address the health protection issues.
This has not yet happened. Despite of steady economic growth since 1980s and the announced
policy directions on rural health protection in 1996, majority of the rural population remain
uninsured today. Discussions above indicate that all the successful CMS schemes that exist today
did it with strong government backing. We have yet to find one single example in China, whereby
government support is not needed and the scheme is totally initiated and operated on a sustainable
basis by a non-government organization (NGO). There are several reasons for the need of
government support. First, increasing inter-regional inequalities in economic and social
development, brought about by the economic system reforms, imply that some communities will
certainly be left behind, if developing rural health protection system is totally subject to the
discretions by the local communities. There always are communities, where the stock of financial
and social capital is too low for any meaningful health protection system to shape up. Governments
have a responsibility to help the helpless. Second, establishing rural health protection system in
24

China, where the market for health insurance is yet to be developed, requires that people trust the
institutions in charge of the system and that the institutions have sufficient authority and skills for
fund collection and risk-transfer. Except for coastal regions or those regions with well developed
township and village enterprises (TVEs), many rural communities lack alternatives to government
organizations for handling the complicated process of problem identification, benefit design, social
marketing, fund collection, contracting and management etc. This is especially true in poor rural
areas.
By virtue of high poverty rate, China's poor rural areas do not have abundant supply of
financial and human capital. Many people need health insurance protection, but with a meager
income they cannot afford to pay the premium. Government simply must provide financial
assistance to the poor for them to be able to join the CMS. Meanwhile, local governments (township
and county governments) often have faced problems of budget shortfall. Sometimes government
officials working in the poverty regions cannot even receive their salaries on time. It is obvious that
local resources alone cannot finance a comprehensive package of CMS benefits. Moreover, many
young and educated people went out to find jobs in the cities or worked in the government. There
are very few social organizations existing in the poverty regions. In light of lack of alternative
organizations that can take on the role of CMS organizers, CMS schemes would have to be initiated
by the local governments in many cases. Ever since the fiscal decentralization reform in the mid-
1980s, local governments have been given increasing responsibilities for developing local economy
and social infrastructure. Therefore, local governments have the discretionary power to decide
whether a CMS scheme is to be established, continued or disbanded. In light of their increasing
budgetary obligations and pressures to raise extra-budgetary funds to meet those obligations, local
governments in middle-income and low-income regions do not have strong incentive nor sufficient
resources for promoting RCMS schemes (Oi, 1999). A common experience by the students of
25

China’s CMS is that whether or not the party chief of a county or township government is really
committed to the course of CMS matters a great deal. The interruption of CMS operations in several
townships was often found to be a result of changing township government heads in the 10 County
Study. Due to lack of control by the local people in CMS's operations and the vertical political
structure that still governs China's political system, county government can intervene in the
township level schemes on behalf of the people. In sum, for foreseeable future, government has an
important role to play in developing rural health protection systems both as an enabler and as a
supervisor.
So far, however, the role played by the governments, especially by the central government, in
developing China’s rural health protection system has been miniscule. Recent years have seen
increasing policy attention paid to social security issues, because without an effective social security
system, China's deeper and wider economic reform programs cannot go forward. However, social
security reforms including health insurance system reforms have limited to the urban sector. The
Ministry of Labor and Social Security, which was established in 1998 to take charge of social
security, is only responsible for health care financing for the urban workers. The administrative
responsibility for financing health care for the 800 million rural populations, especially for the rural
poor, remained undefined. Why has there been lack of government support for rural health
protection systems? Ideology shift, institutional constraints, and misunderstanding of some key
issues may explain the observed government inaction.
Ever since the inception of economic system reforms, the dominant ideology guiding public
policies gradually shifted from the fixation on an equalitarian society under Mao to Deng
Xiaoping’s “hard truth” (“Ying Dao Li”) of economic development at the expense of reduced
equity. Therefore, governments' top priority has been and continues to be economic growth. Social
sector development including health care has been low on the public policy agenda. Social sector
26

development is often valued by it’s contribution to the economic growth. For example, investment
in education is aimed to develop “human capital”, fundamental for economic growth. Thus,
strengthening education has become part of the development strategies for developing China’s vast
western regions (“Kai Fa Da Xi Bei”). However, due to lack of understanding of the role of health
in economic development, health investment is not included in the new development strategies. This
report tried to use some empirical evidence from China’s own data to shed some light on the
economic impact (e.g. poverty impact) of health. Further studies in this area would help inform the
policy-making process in a more comprehensive way.
Economic system reforms in China have created a new set of institutional context for the
governments to fulfilling their roles in the society. The reforms introduced since 1978 can be seen
as actions to rectify some of the irrationalities and inefficiencies that had developed under a highly
centralized planning system. Investment and spending decisions have been decentralized both to the
provinces and to the individual enterprises. Within provinces social spending for the rural
population, including health spending, are largely decentralized to the county and township
governments. A system of fiscal responsibility was introduced in the early 1980s and lasted until
1994. Each province signed a contract with the central government, stipulating the amount of funds
that had to be forwarded to the center annually. Revenues generated over and above this stipulated
sum could be retained in whole or in part for the provincial usage. Under this system, the provinces
have more resources at their disposition. By the late 1980s, however, the shortcomings of the
contract responsibility system, especially in terms of inhibiting the center’s ability to redistribute
resources had become apparent. The center has since tried to rectify the situation by launching a
series of reforms. In 1994, a “tax sharing” system, which formally delineates local and center taxes,
was introduced to replace the contract responsibility system. The main aim was to strengthen the
center’s financial position and sever the direct link between the revenues of the local government
27

and those of the enterprises located within their respective geographical jurisdictions. As the central
and provincial governments have been in the process of sorting out their respective responsibilities
in tax and spending, it is not surprising that there has been a lack of clear division of responsibilities
within the governments in the area of health protection for the 800 million rural populations.
However, now given the much improved revenue position of the central government and the
constant declarations of the party and government top policy agenda on rural agricultural
development, solving problems faced by the rural regions and rural populations (the so-called
“Three Rural Problems”), one would expect the central government to have taken a more active role
in developing China’s rural health protection systems. What has gotten in their way?
There are three major concerns for the central government regarding rural health protection
system development: budget implications, effectiveness of reforming the existing resource
allocation processes, and unbearable tax burden for the rural farmers. First, having experienced
many difficulties and challenges in developing the urban social insurance system, the government
hesitates to take on the seemingly larger challenge to be responsible for establishing health
protection systems for the 800 million rural residents. Urban health protection system development
experiences, though informative in certain respects, need not totally apply to the rural sector.
To begin with, no one, certainly not the rural farmers, expects the government to give the same
kind of financial support to the rural health protection system as that to the urban system. Unlike
other former socialist countries such as Russia that provided a nationalized system of welfare, with
access to public funded healthcare for all the citizens., China’s health systems for the urban and
rural populations had been separate. The two systems differed not only in benefit packages, but also
in funding sources. Under the old planning system, urban workers received low wages and part of
their deferred compensation took the form of entitlement to a set of benefits in kind, including
housing and health insurance. That’s why governments felt obligated to honor the social contract by
28

taking care of the urban pensioners and unemployed workers of the State Owned Enterprises
(SOEs), when the SOEs underwent reforms or simply went under. Large enough number of the
SOE workers not receiving their pay check or reimbursement for their medical bills could often lead
to social unrest. By contrast, majority of the rural residents had never received any benefits from
the governments in terms of entitlements. CMS was a community-based risk-sharing system, and
largely funded by the farmers’ own financial contributions. Therefore, there has been never a formal
nor implicit social contract between the rural people and the governments on a guaranteed health
protection benefits. That’s why we have not seen any social unrest as a result of 600 million rural
residents becoming uninsured, when CMS collapsed. Furthermore, socioeconomic conditions are
different across rural areas, and thus the needs for government support are different. While rich rural
areas may not need financial support as much as need policy and regulatory support from the
governments, middle- and low-income regions need financial assistance. So, the governments need
not and should not being concerned about financing healthcare for the whole rural population.
Instead, the governments need and should be helping the most needy and vulnerable.
Some government officials, including those who are committed to provide support to the rural
population, are content with the existing supply-side-centered resource allocation policies. In their
view, the major problem with the rural health system is not health protection on the demand-side,
but inadequacies of the supply-side. Therefore government funds should be used to help upgrade the
rural health facilities, especially for the poverty regions. This policy addresses one of the health
system problems, but not the most critical one. It is true that many rural regions suffer acute
problems of inadequate supply. Many more areas, however, suffer from chronic under-utilization
due to low effective demand. Many surveys found that many rural health facilities, including those
with updated new medical technologies, are running idle (Liu et al., 1998). As indicated by
discussions in part two of this report, it is time for the government to critically re-examine it’s old
29

policy of supporting or subsidizing the supply-side. Using part of the existing funds, which would
have gone directly to the providers previously, to support an adequate rural health protection system
would help both the demand-side and the supply-side at the same time.
Given the size and need of China’s rural population relative to the government budget2,
significant portion of the funding for the rural health protection system still needs to come from the
household contributions. However, central government is concerned that collecting household
contributions for rural health protection system would further increase the already high tax burden
for the rural farmers. China’s tax system is still a very centralized one. All tax laws are enacted by
the Central government. Even legislation governing local taxes is generally promulgated by the
Central government for local implementation. Local governments virtually have no fiscal autonomy
and no taxing power. In the meantime, local governments are required to pay for various
expenditures. To raise revenue to cover the expenditures, local governments have adopted
numerous “non-taxation” “extra-budgetary” measures. In that process, local taxes in the name of
various “cost-sharing” and “fees” had been increasing thus the financial burden for the farmers. One
of the major objectives for the latest rural tax reform since 2000, on a pilot basis in Anhui Province
right now, is to reduce the tax burden faced by the rural farm families. Under the new system, ear-
marked contributions to the rural health protection system can only be collected at the village level,
when the contributions are totally voluntary and establishing a risk-pool at the village is approved
by the villagers. This new tax policy, if enacted, would pose the greatest difficulty for establishing
China’s rural health protection systems, because the local governments (e.g. township government)
would have no power to collect contributions for rural health protection purposes. Even if a rural
30
2 Studies have been conducted in China on feasibilities and potentials of raising cigarette tax to finance rural health protection systems (Mao et al, 1997; Liu et al., 1997).

health protection system is established at the village level, the small risk-pool would render the
scheme unstable.
To illustrate how inadequate and irresponsible China’s current policies are, or lack thereof, on
the rural health protection system, Table 8 compares government policies on the urban health
protection system to those on the rural system. A particularly disturbing finding from the table is
that the government has applied a “double standards” in dealing with some known issues of
developing health protection systems.
For example, to avoid tax evasion and adverse selection, the urban health protection system is
made a compulsory social insurance scheme. By contrast, current policies dictate that rural health
protection system can only be developed on a voluntary basis. On one hand, realizing the “law of
large numbers” in stabilizing insurance fund, governments required that the risk-pool for urban
health protection system should not be smaller than the prefecture or city. On the other hand, the
only legitimate collective body that is allowed to collect contributions for rural health protection
system (thus share risks among the community members) is village - the smallest unit of all the rural
organizations beside family.
Table 8. Government Policies on Health Protection Systems in China
Dimension Urban Sector Rural Sector
System Nature Social Insurance Community Financing Enrollment Requirement Mandatory Voluntary Premium Contribution 25% by members 80% by members Risk pool requirement City wide No specification
Organizational Guidelines Comprehensive, based on organized pilots No specification
Central Administration Ministry of Labor and Social Security Undefined
The Ministry of Labor and Social Security, which was established in 1998 to take charge of
social security, is only responsible for health care financing for the urban workers through social 31

health insurance schemes. The administrative responsibility for financing health care for the 800
million rural populations, especially for the rural poor, remained undefined. To fill the void,
many of the CMS schemes are initiated by local health administration and managed by health
care providers. Neither the health care provision side nor the local governments have the
legitimacy as well as strong incentive to organize CMS schemes. Local governments, being pre-
occupied with income generation (not with social spending) and perceiving people's ability and
willingness to participate in CMS to be low, often consider CMS as a difficult course with little
payoff. Lack of legal status for rural health protection systems appeared to be the number one
concern among the various local government officials (Liu et., 2000). Enforcers of the tax relief
policy – the party office for tax reduction and the Ministry of Agriculture – often posed serious
threat to disrupt operations of existing CMS schemes.
4. Conclusion
Today, majority of China’s rural populations do not have any health insurance. This paper
highlighted medical impoverishment as an important cause for poverty due to lack of rural health
insurance in China. According to the 1998 National Health Services Survey, the poverty
headcount for the whole rural sample is 7.22%. Out-of-pocket spending on healthcare has raised
the headcount by more than 3 percentage points. In another word, medical spending raised the
number of rural households living below poverty line by 44.3%. Comparing the results from the
1993 and 1998 national survey data, the problem of medical impoverishment appeared to have
become more pronounced over time in China’s rural areas. Therefore, providing rural health
insurance coverage would seem to be not only an important health protection measure, but also
an important poverty reduction strategy.
However, China does not yet have a supportive policy and regulatory framework for rural
health insurance development in general and for government's role in particular. There have been
32

serious inconsistencies in government policies and regulatory framework, which affect operation
and sustainability of RCMS schemes. For a long time since the economic system reforms,
governments have ignored the issues of rural health care financing. While there has been a
general relative reduction of public resources that are allocated to rural health sector, government
intervention in rural health sector has been limited to provision side - capital investment,
medical education and training etc. Financing of health care has been largely left private and
unorganized. That is why we found that many uninsured rural families have suffered from lack
of financial access to the health services they need and medical impoverishment. To be sure, the
1997 Central Party Committee and State Council Decisions on Health Sector Reform and
Development did recognize the potential of RCMS and included a provision , specifying the
voluntary nature of the scheme and urging government organizations to provide financial
assistance to RCMS schemes. But that document has left roles and responsibilities of the
governments unspecified. Worse yet, uncoordinated policies from different ministries
constrained RCMS development. For example, according to the State Council policy of reducing
farmers' tax burden, it is illegal to collect RCMS contributions.
Economic policies and social policies (including health policy) need to be coordinated to
provide an enabling environment for rural health insurance development. At present, inconsistent
and uncoordinated policies directly affecting RCMS schemes include poverty alleviation (how
much of the poverty alleviation fund should be used to support health care and RCMS), taxes
(can contributions by the farmers to RCMS be collected as part of the local taxes), financial
market regulation (how should part of the RCMS funds be invested?), political system and
institutional reforms (should MOLSS or Civil Service Administration take on the responsibility
of public financing agent for China's poor rural population and 800 million rural population in
general?). Each of the above policy areas represents both challenges and opportunities for rural
33

health insurance development. Since many of the above policies were initially made without
consideration of their impact on rural health insurance, a thorough and systematic review of
relevant policies would help guide necessary adjustments to make those policies more RCMS-
friendly without compromising their original economic and social objectives.
34

Reference Bennett S, Creese A, Roeland M (1998) Health Insurance Schemes for People outside Formal Sector Employment; Current Concerns ARA Paper Number 16. World Health Organization Chen H. (2000) Current Situation and Prospect of the Urban Social Security System in China. Paper prepared for the Workshop on China's Long-term Economic Prospects and Challenge, Manila, June 2, 2000. Chen CC. (1989) Medicine in Rural China: A Personal Account. Berkeley: University of California Press.
Chen, HF and Zhu, C. ed. (1984) Modern Chinese Medicine, Vol. 3: Chinese Health Care. Lancaster: MTP Press Ltd.
Cheng, X. and Fan, W. (2000). CMS in Tibet Autonomous Region. Paper presented at the International Seminar on Rural Health Care Financing, held by the UNICEF and Chinese Ministry of Health in Beijing on December 11-13, 2000. China Health Economics Institute (2000). Studies on China’s National Health Account. Paper presented at the Conference on China Rural Health Reform and Development, held by CHEI and IDS in Beijing on November 7-9, 2000. Du J, Sun Z. (1999) The Handbook on The Reforms of Employee Health Insurance. Beijing: Economics Press.
Fu, W. et al. (1997). Different models of community financing schemes in the 30 counties. In: Health Care Financing and Organization in Poor Rural Areas of China Project Group eds. Policy reports on 30 poverty counties. Beijing: the People’s Publishing House. Hartland-Thunberg P. (1989) A Decade of China's Economic Reform: Challenges for the Future. Washington, D.C.: Center for Strategic and International Studies. Hinman, AR, Parker RL, Gu XQ, Gu XY, and Huang DY, eds. (1982) “Health services in Shanghai county,” In American Journal of Public Health, 72: 1224-1225. Hsiao WC, Roberts MJ, Berman PA, Reich MR (2001) Getting Health Reform Right. Mimeo. Harvard University. Hsiao (1995) "The Chinese health care system: lessons for other nations", In Social Science & Medicine 8:1047-1055. Hsiao WC, Liu YL. (1996) “Economic reform and health--lessons from China.” In New England Journal of Medicine 335: 430-432. Hsiao WC. (1984) “Transformation of health care in China.” In New England Journal of Medicine, 310:932-936.
35

Hu S. (1995) “The health impact of economic development and reform.” In Chinese Health Economics 14(1): 58-63. Hu, S. et al. (2000). The 10 County Intervention Studies. Paper presented at the International Seminar on Rural Health Care Financing, held by the UNICEF and Chinese Ministry of Health in Beijing on December 11-13, 2000. Jacobs, P. (1996). The economics of health and medical care. Gaithersburg: Aspen Publishers, Inc. Jalan, J and Ravallion, M. (1997). Determinants of transient and chronic poverty: evidence from rural China. Washington, D.C.: The World Bank Policy Research Working Paper Series 1936. Jamison DT et al. (1984) China: The Health Sector. Washington, D.C.: The World Bank. Jiang, J. et al. (2000). Report on the investigation of CMS in Maishan and Jianyang of Sichuan Province. Paper presented at the International Seminar on Rural Health Care Financing, held by the UNICEF and Chinese Ministry of Health in Beijing on December 11-13, 2000. Liu X, Liu Y, Chen N. (2000) “The Chinese experience of hospital price regulation,” in Health policy and Planning 15(2):157-163. Liu, Y. (2000). Understanding and setting up the process for health equity. Bulletin of the World Health Organization 78(1): 82-83. Liu Y, Hu S et al.(1996) “Is Community Financing Necessary and Feasible for Rural China?” In Social Science & Medicine 49:1349-1356. Liu Y, Hsiao WC, et al. (1995) “Transformation of China's rural health care financing,” In Social Science & Medicine 8:1085-1093. Liu, Y. et al. (1997). Efficiency in rural healthcare: a stochastic frontier model. In: Health Care Financing and Organization in Poor Rural Areas of China Project Group eds. Policy reports on 30 poverty counties. Beijing: the People’s Publishing House. Liu, Y. (2000). Reforming China’s Urban Health Insurance System. Mimeo. Asian Development Bank. Liu, Y. et al. (2000). Major factors affecting the CMS operations: experience from the 10 county study. Paper presented at the International Seminar on Rural Health Care Financing, held by the UNICEF and Chinese Ministry of Health in Beijing on December 11-13, 2000.
Liu, Y., Rao, K., Hu, S. (2001) Towards establishing a health protection system for rural China. Paper presented at the International Conference on China’s Rural Social Security, held by the Asian Development Bank and the China State Development and Planning Commission in Beijing on July 9-10, 2001.
36

Ma, J. and Wang, L. (2000). An investigation report on CMS in Keshi of Xinjiang Autonomous Region. Paper presented at the International Seminar on Rural Health Care Financing, held by the UNICEF and Chinese Ministry of Health in Beijing on December 11-13, 2000. Ministry of Agriculture, PRC. (2000). China agricultural development report 2000. Beijing: The Agricultural Press. Ministry of Health, PRC. (1988) Health Statistics in China Beijing: Ministry of Health. Ministry of Health, PRC. (1992) Data From Mortality Monitoring Sites. Beijing: Ministry of Health. Ministry of Health, PRC. (1993) National Health Service Survey Beijing: Ministry of Health. Ministry of Health, PRC. (1994) Research on National Health Services-An Analysis Report of the National Health Services Survey in 1993 Beijing: Ministry of Health, PRC. Ministry of Health, PRC. (1995) Health Statistics in China for 1995 Beijing: Ministry of Health. Ministry of Health, PRC (1997). Proceedings of the 1996 National Health Conference. Beijing: The People’s Publishing House. Ministry of Health, PRC. (1998) National Health Service Survey Beijing: Ministry of Health. Ministry of Health, PRC. (1999) Reports on the 1998 National Health Services Survey Results Beijing: the Ministry of Health, Center for Health Statistics and Information. Ministry of Health, PRC. (2000). National Health Statistics. Beijing: MOH. Oi, J. (1999). Rural China takes off: institutional foundations of economic reform. Berkeley: University of California Press. Rao et al 2000. Economic burden of ill health in China Paper presented at the Senior Policy Seminar on Health Sector Reform and Development in China in the 21Century. The Chinese Ministry of Health and others, Guangzhou Hotel, Beijing, June 21-23, 2000. Reform Committee of the State Council et al. (1996) The Reform in Employee Health Insurance Systems Beijing: Reforms Press. Research Group on China's health expenditure (1997), Study on Health Expenditure of China, Beijing, the National Health Economics Institute of the Ministry of Health Sidel, VW. (1972) “The barefoot doctors of the People’s Republic of China,” In New England Journal of Medicine, 286:1292-1299.
37

Sidel, R, Sidel, VW. (1982) The Health of China: Current Conflicts in Medical and Human Services for One Billion People. Boston: Beacon Press. Sidel, VW. (1993) “New lessons from China: equity and economics in rural health care,” In American Journal of Public Health, 83:1665-1666. State Statistics Bureau, PRC. (1995) Social Statistic Information on China. Beijing, PRC: State Statistics Bureau. The State Council Research Office (1994). Rural Cooperative Medical Systems. Beijing: The State Council Research Office. The State Council (1998) Decisions on Establishing the Basic Medical Insurance System for the Urban Workers. Beijing: The State Council. The State Council (2000) Guidelines for Reforming the Urban Health and Pharmaceutical Sectors. Beijing: The State Council. The State Council (2001). Guidelines for Reforming the Rural Healthcare Systems. Beijing: The State Council. UNDP (1998) China: Human Development Report. UNICEF/Beijing (2000). Major health problems in rural China. Paper presented at the International Seminar on Rural Health Care Financing, held by the UNICEF and Chinese Ministry of Health in Beijing on December 11-13, 2000. Wagstaff A, Doorslaer EV. (1993) “Equity in the finance and delivery of health care: concepts and definitions,” In Doorslaer EV et al, eds., Equity in the Finance and Delivery of Health Care An International Perspective. Oxford: Oxford University Press. The World Bank. (1992) China - Strategies for Reducing Poverty in the 1990’s. Washington, D.C.: The World Bank. The World Bank. (1996) World Development Report 1996: From Plan to Market. New York: Oxford University Press. The World Bank. (1997) Financing Health Care: Issues and Options for China. Washington, D.C.: The World Bank. The World Bank (1999) World Development Indicators 1999 Washington, D.C.: The World Bank. The World Bank (2000) World Development Report 2000: Attacking Poverty New York: Oxford University Press.
38

WHO (2000). The World Health Report 2000: Health Systems: Improving Performance. Geneva. WHO Williams, A. (2001). Science or marketing at WHO? A commentary on “World Health 2000”. Health Economics 10(2): 93-100. Yuan M and Chen M. (1994) “The Chinese rural health care reform,” In The People's Daily, July 2, 1994. Zhang X. (1999) Correctly Understanding the Relationship Between Need and Feasibility of Health Insurance Reforms. Shanghai: Shanghai Social Insurance Bureau.
Zhang Z. (1992) “Review of the early period of the Cooperative Medical System,” In Chinese Health Economics, 6:54-62.
39





























