Embed Size (px)
Citation preview

CHNB Urinary System
1
URINARY SYSTEM
The urinary system consists of two kidneys, two ureters, the urinary bladder, and the urethra. The formation
of urine is the function of the kidneys, and the rest of the system is responsible for eliminating the urine.
Body cells produce waste products such as urea, creatinine, and ammonia, which must be removed from the
blood before they accumulate to toxic levels. As the kidneys form urine to excrete these waste products, they
also accomplish several other important functions:
1. Regulation of the volume of blood by excretion or conservation of water
2. Regulation of concentration of electrolytes (Na+, K+, HCO3 – and other ions) in the plasma and the pH
of plasma by controlling the loss hydrogen ions and bicarbonate ions in urine.
3. Regulation of all of the above in tissue fluid.
4. Conserving valuable nutrients, by preventing their loss in urine while removing organic wastes—
especially nitrogenous wastes such as urea and uric acid.
5. Gluconeogenesis during prolonged fasting.
6. Producing the hormones renin and erythropoietin. Renin acts as an enzyme to help regulate blood
pressure and kidney function. Erythropoietin stimulates red blood cell production.
7. Metabolizing vitamin D to its active form.
These activities are carefully regulated to keep the composition of blood within acceptable limits. A
disruption of any one of them has immediate consequences and can be fatal.
Kidney:
The two kidneys are located in the upper abdominal cavity on either side of the vertebral column. The upper
portions of the kidneys rest on the lower surface of the diaphragm and are enclosed and protected by the lower
rib cage. Kidneys are reddish, bean shaped organs situated posteriorly, below the diaphragm in the lower
thoracic and lumbar vertebrae (T12-L3). The right kidney is crowded by the liver and lies slightly lower than
the left. An adult’s kidney has a mass of about 150 g and its average dimensions are 12 cm long, 6 cm wide,
and 3 cm thick—about the size of owner’s fist. The lateral surface is convex and the medial surface is
concave. The hilum, a prominent medial indentation, is the point of entry for the renal artery and renal
nerves. The hilum is also the point of exit for the renal vein and the ureter.

CHNB Urinary System
2
Internal Anatomy
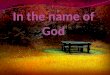
A frontal section of a kidney reveals three distinct regions: cortex, medulla, and pelvis. The most superficial
region, the renal cortex, is light in color and has a granular appearance. Deep to the cortex is the darker,
reddish-brown renal medulla, which exhibits cone-shaped tissue masses called medullary or renal pyramids.
The pyramids appear striped because they are formed almost entirely of parallel bundles of microscopic urine-
collecting tubules and capillaries. Minor calyces are funnel-shaped chambers into which the renal papillae
extend. The minor calyces of several pyramids merge to form larger funnels, the major calyces. Each kidney
contains 8–20 minor calyces and 2 or 3 major calyces. The major calyces converge to form an enlarged
chamber called the renal pelvis, which is surrounded by the renal sinus. The renal pelvis narrows into a small
diameter tube, the ureter, which exits the kidney at the hilum and connects to the urinary bladder. The walls
of the calyces, pelvis, and ureter contain smooth muscle that contracts rhythmically to propel urine along its
course by peristalsis.
Kidneys are highly vascularized organs since they are concerned with the purification of blood and also help
in maintaining its composition. About 25% of the total blood (i.e., 1200ml/min) passes through the kidneys
each minute. Kidneys account for only 1% of body weight but consume 20–25% of all oxygen used by the
body at rest. The blood supply occurs via the left and right renal arteries. Each renal artery after entering the
kidney, gives off branches termed as segmental arteries, which supply blood to various segments of the
kidney. Within the kidney, there is repeated branching of the artery, with the branches becoming smaller and
smaller. These branches pass along the sides and bases of the renal pyramids, project into the cortex, and give
rise to afferent arterioles supplying the glomerular capillaries inside the Bowman capsule. Efferent
arterioles arise from the glomerular capillaries and carry blood away from the glomeruli.

CHNB Urinary System
3
After each efferent arteriole exits the glomerulus, it gives rise to a plexus of capillaries, called the peritubular
capillaries, around the proximal and distal convoluted tubules. The vasa recta are specialized portions of the
peritubular capillaries that extend deep into the medulla of the kidney and surround the loops of Henle and
collecting ducts. The peritubular capillaries, which include the vasa recta, join small veins. These veins form
larger veins that run parallel to the arteries.
Nephron- The Functional unit:
The functional unit of the kidney is the nephron, and there are approximately 1.3 million of them in each
kidney. Each nephron consists of a renal corpuscle; a proximal convoluted tubule, a loop of Henle and a
distal convoluted tubule. The renal corpuscle consists of a Bowman capsule and a glomerulus. The Bowman
capsule is the enlarged end of the nephron surrounding the glomerulus, which is a network of capillaries.
Fluid from the blood in the glomerulus enters the Bowman capsule and then flows into the proximal
convoluted tubule. From there, it flows into the loop of Henle. Each loop of Henle has a descending limb,
which extends toward the renal sinus, and an ascending limb, which extends back toward the cortex.
The fluid flows through the ascending limb of the loop of Henle to the distal convoluted tubule. Many distal
convoluted tubules empty into a collecting duct, which carries the fluid from the cortex, through the medulla.
Many collecting ducts empty into a papillary duct and the papillary ducts empty their contents into a minor
calyx.

CHNB Urinary System
4
Physiology of Urine Formation:
Of the approximately 1200 ml of blood that passes through the glomeruli each minute, some 650 ml is
plasma, and about one-fifth of this (120–125 ml) is forced into the renal tubules. This is equivalent to filtering
out entire plasma volume more than 60 times each day.
Filtrate and urine are quite different. Filtrate contains everything found in blood plasma except proteins, but
by the time filtrate flows into the collecting ducts, it has lost most of its water, nutrients, and ions. What
remains, now called urine, contains mostly metabolic wastes and unneeded substances. The kidneys process
about 180 L of blood-derived fluid daily. Of this amount, less than 1% (1.5 L) typically leaves the body as
urine; the rest returns to the circulation. Urine formation and the adjustment of blood composition involve
three major processes:

CHNB Urinary System
5
Glomerular filtration by the glomeruli,
Tubular reabsorption and
Tubular secretion in the renal tubules.
Step 1: Glomerular Filtration:
Glomerular filtration is a passive process in which hydrostatic pressure forces fluids and solutes through a
membrane. The glomerulus is a much more efficient filter than are other capillary beds because:
1. Its filtration membrane has a large surface area and is thousands of times more permeable to water and
solutes, and
2. Glomerular blood pressure is much higher than that in other capillary beds (approximately 55 mm Hg
as opposed to 18 mm Hg or less), resulting in a much higher net filtration pressure.
As a result of these differences, the kidneys produce about 180 L of filtrate daily, in contrast to the 3 to 4 L
formed daily by all other capillary beds of the body combined.
Molecules smaller than 3 nm in diameter such as water, glucose, amino acids, and nitrogenous wastes pass
freely from the blood into the glomerular capsule. Hence, these substances usually show similar
concentrations in the blood and the glomerular filtrate. Larger molecules pass with greater difficulty, and
those larger than 5 nm are generally barred from entering the tubule. Keeping the plasma proteins in the
capillaries maintains the colloid osmotic pressure of the glomerular blood, preventing the loss of all its water
to the renal tubules. The presence of proteins or blood cells in the urine usually indicates a problem with the
filtration membrane.

CHNB Urinary System
6
The net filtration pressure (NFP), responsible for filtrate formation, involves forces acting at the glomerular
bed. Glomerular hydrostatic pressure (HPg) is the chief force pushing water and solutes out of the blood and
across the filtration membrane. The HPg is opposed by two forces that inhibit fluid loss from glomerular
capillaries. These filtration-opposing forces are (1) colloid osmotic pressure of glomerular blood (OPg) and
(2) capsular hydrostatic pressure (HPc) exerted by fluids in the glomerular capsule. Thus, the NFP
responsible for forming renal filtrate from plasma is 10 mm Hg:
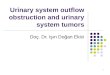
Glomerular Filtration Rate:
The glomerular filtration rate or GFR is
the volume of filtrate formed each minute
by the combined activity of all 2 million
glomeruli of the kidneys. Factors
governing filtration rate at the capillary
beds are:
Total surface area available for filtration,
Filtration membrane permeability, and
NFP.
In adults the normal GFR in both kidneys
is 120–125 ml/min. Because glomerular
capillaries are exceptionally permeable
and have a huge surface area (collectively

CHNB Urinary System
7
equal to the surface area of the skin), huge amounts of filtrate can be produced even with the usual modest
NFP of 10 mm Hg.
Because the GFR is directly proportional to the NFP, any change in any of the pressures acting at the
filtration membrane changes both the NFP and the GFR. In the absence of regulation, an increase in arterial
(and glomerular) blood pressure in the kidneys increases the GFR. As we shall see in the next section
however, GFR is tightly regulated.
Regulation of Glomerular Filtration
GFR is regulated by both intrinsic and extrinsic controls. These two types of controls serve two different (and
sometimes opposing) needs. The kidneys need a relatively constant GFR in order to do their job and maintain
extracellular homeostasis. On the other hand, the body as a whole needs a constant blood pressure, and
therefore a constant blood volume. Intrinsic controls (renal autoregulation) act locally within the kidney to
maintain GFR, while extrinsic controls by the nervous and endocrine systems maintain blood pressure. In
extreme changes of blood pressure (mean arterial pressure less than 80 or greater than 180 mm Hg), extrinsic
controls take precedence over intrinsic controls. Both types of control are examined next.
Intrinsic Controls:
Renal Autoregulation: By adjusting its own resistance to blood flow, a process called renal autoregulation,
the kidney can maintain a nearly constant GFR despite fluctuations in systemic arterial blood pressure. Renal
autoregulation entails two types of controls: (1) a myogenic mechanism and (2) a tubuloglomerular feedback
mechanism.

CHNB Urinary System
8
2. Extrinsic Controls: Neural and Hormonal Mechanisms: The purpose of the extrinsic controls
regulating the GFR is to maintain systemic blood pressure—sometimes to the detriment of the
kidneys.
1. Sympathetic nervous system controls: Norepinephrine released by sympathetic nerve fibers acts
on alpha-adrenergic receptors on vascular smooth muscle, strongly constricting afferent arterioles,
thereby inhibiting filtrate formation. This, in turn, indirectly trips the renin-angiotensin mechanism
by stimulating the macula densa cells. The sympathetic nervous system also directly stimulates the
granular cells to release renin.
2. Renin-angiotensin mechanism
Step 2: Tubular Reabsorption
Our total plasma volume filters into the renal tubules about every 22 minutes, so all our plasma would be
drained away as urine in less than 30 minutes were it not for the fact that most of the tubule contents are
quickly reclaimed and returned to the blood. This process, called tubular reabsorption, the movement of
water and solutes from the filtrate back into the blood, makes this possible. Almost all of the water and useful
solutes are reabsorbed, whereas waste products, excess solutes, and a small amount of water are not. The
reabsorbed substances enter the peritubular capillaries and vasa recta and flow through the renal veins to enter
the general circulation.
Mechanisms of Reabsorption
1. Active transport—the cells of the renal tubule use ATP to transport most of the useful materials from the
filtrate to the blood. These useful materials include glucose, amino acids, vitamins, and positive ions.
For many of these substances, the renal tubules have a threshold level of reabsorption. This means that there
is a limit to how much the tubules can remove from the filtrate. For example, if the filtrate level of glucose is
normal (reflecting a normal blood glucose level), the tubules will reabsorb all of the glucose, and none will be
found in the urine.

CHNB Urinary System
9
What happens is this: The number of glucose transporter molecules in the membranes of the tubule cells is
sufficient to take in the number of glucose molecules passing by in the filtrate. If, however, the blood glucose
level is above normal, the amount of glucose in the filtrate will also be above normal and will exceed the
threshold level of reabsorption. The number of glucose molecules to be reabsorbed is more than the number of
the transporter molecules available to do so. In this situation, therefore, some glucose will remain in the
filtrate and be present in urine.
The reabsorption of Ca+2 ions is increased by parathyroid hormone (PTH). The parathyroid glands secrete
PTH when the blood calcium level decreases. The reabsorption of Ca+2 ions by the kidneys is one of the
mechanisms by which the blood calcium level is raised back to normal.
The hormone aldosterone, secreted by the adrenal cortex, increases the reabsorption of Na+ ions and the
excretion of K+ ions. Besides regulating the blood levels of sodium and potassium, aldosterone also affects the
volume of blood.
2. Passive transport—many of the negative ions that are returned to the blood are reabsorbed following the
reabsorption of positive ions, because unlike charges attract.
3. Osmosis—the reabsorption of water follows the reabsorption of minerals, especially sodium ions. The
hormones that affect reabsorption of water are discussed in the next section.
4. Pinocytosis—small proteins are too large to be reabsorbed by active transport. They become adsorbed to
the membranes of the cells of the proximal convoluted tubules. The cell membrane then sinks inward and
folds around the protein to take it in. Normally all proteins in the filtrate are reabsorbed; none is found in
urine.
Step-3: Tubular Secretion
This mechanism also changes the composition of urine. In tubular secretion, substances are actively secreted
from the blood in the peritubular capillaries into the filtrate in the renal tubules. Waste products, such as
ammonia and some creatinine, penicillin and the metabolic products of medications may be secreted into the
filtrate to be eliminated in urine. Hydrogen ions may be secreted by the tubule cells to help maintain the
normal pH of blood.
In the end, urine contains (1) substances that have undergone glomerular filtration but have not been
reabsorbed, and (2) substances that have undergone tubular secretion.
Hormones That Influence Reabsorption of Water
Aldosterone is secreted by the adrenal cortex in response to a high blood potassium level, to a low blood
sodium level, or to a decrease in blood pressure. When aldosterone stimulates the reabsorption of Na+ ions,
water follows from the filtrate back to the blood. This helps maintain normal blood volume and blood
pressure.
You may recall that the antagonist to aldosterone is atrial natriuretic peptide (ANP), which is secreted by
the atria of the heart when the atrial walls are stretched by high blood pressure or greater blood volume. ANP

CHNB Urinary System
10
decreases the reabsorption of Na+ ions by the kidneys; these remain in the filtrate, as does water, and are
excreted. By increasing the elimination of sodium and water, ANP lowers blood volume and blood pressure.
Antidiuretic Hormone (ADH) is released by the posterior pituitary gland when the amount of water in the
body decreases. Under the influence of ADH, the distal convoluted tubules and collecting tubules are able to
reabsorb more water from the renal filtrate. This helps maintain normal blood volume and blood pressure, and
also permits the kidneys to produce urine that is more concentrated than body fluids. Producing concentrated
urine is essential to prevent excessive water loss while still excreting all the substances that must be
eliminated. If the amount of water in the body increases, however, the secretion of ADH diminishes, and the
kidneys will reabsorb less water. Urine then becomes dilute, and water is eliminated until its concentration in
the body returns to normal. This may occur following ingestion of excessive quantities of fluids.
Renal Clearance
The rate at which a particular chemical is removed from the plasma indicates kidney efficiency. This rate is
called renal clearance.
The Ureters
The ureters are a pair of muscular tubes that extend from the kidneys to the urinary bladder—a distance of
about 30 cm. Each ureter begins at the funnel-shaped renal pelvis. The paths taken by the ureters in men and
women are different, due to variations in the nature size, and position of the reproductive organs. The ureters
penetrate the posterior wall of the urinary bladder without entering the peritoneal cavity. They pass through
the bladder wall at an oblique angle.
Histology of the Ureters
The wall of each ureter consists of three layers:
(1) an inner mucosa, made up of a transitional epithelium and the surrounding lamina propria;
(2) a middle muscular layer made up of longitudinal and circular bands of smooth muscle; and
(3) an outer connective tissue layer that is continuous with the fibrous capsule and peritoneum.
About every 30 seconds, a peristaltic contraction begins at the renal pelvis. As it sweeps along the ureter, it
forces urine toward the urinary bladder.
The Urinary Bladder
The urinary bladder is a hollow, muscular organ that serves as a temporary reservoir for urine. The
dimensions of the urinary bladder vary with its state of distension. A full urinary bladder can contain as much
as a liter of urine.
A layer of peritoneum covers the superior surfaces of the urinary bladder.
In sectional view, the mucosa lining the urinary bladder is usually thrown into folds, or rugae, that disappear
as the bladder fills. The triangular area bounded by the openings of the ureters and the entrance to the urethra
makes up a region called the trigone of the urinary bladder. There, the mucosa is smooth and very thick. The
trigone acts as a funnel that channels urine into the urethra when the urinary bladder contracts.

CHNB Urinary System
11
The region surrounding the urethral opening is known as the neck of the urinary bladder. It contains a
muscular internal urethral sphincter. The smooth muscle fibers of this sphincter provide involuntary control
over the discharge of urine from the bladder. The urinary bladder is innervated by postganglionic fibers.
Histology of the Urinary Bladder
The wall of the urinary bladder contains mucosa, submucosa, and muscularis layers. The muscularis layer
consists of inner and outer layers of longitudinal smooth muscle, with a circular layer between the two.
The Urethra
The urethra extends from the neck of the urinary bladder and transports urine to the exterior of the body. The
urethra of males and females differ in length and in function. In males, the urethra extends from the neck of
the urinary bladder to the tip of the penis. This distance may be 18–20 cm. In females, the urethra is very
short. It extends 3–5 cm from the bladder to the vestibule. The external urethral orifice is near the anterior
wall of the vagina.
In both sexes, a circular band of skeletal muscle forms the external urethral sphincter. This muscular band
acts as a valve. The external urethral sphincter is under voluntary control. This sphincter has a resting muscle
tone and must be voluntarily relaxed to permit micturition.