Embed Size (px)
Citation preview

1
Choosing an inhaler for COPD
made simple
Dr Simon Hart
Castle Hill Hospital

Declaration of interests
I have received speaker fees, sponsorship to attend conferences, and funding for research from companies that make COPD treatments



£29.32
£29.32
£27.80
£59.48
£40.92
£38.00
£29.97
£45.56
£33.50
£33.50 £28.60
£32.19
£27.50
£27.50 £32.50
£32.50
£32.50 £32.50
£26.35 £1.50 £5.56

What is COPD? • characterized by persistent airfow limitation (reduced FEV1 and
FEV1/FVC ratio) that is usually progressive
• a leading cause of morbidity and mortality worldwide and results in an economic and social burden that is both substantial and increasing.
Chronic bronchitis Emphysema


Hyperinflation in COPD


Treating airflow obstruction
bronchodilators

Bronchodilators: relax airway smooth muscle

• Bronchodilators increase the radius of the small airways and so reduce the resistance of the airflow during breathing
r r
Air flow resistance ∝ 1/r4
A small change makes a big difference
Bronchodilation Bronchoconstriction
• Airflow is inversely proportional to the radius of the small airway to the power of four 1
1) Chang DW. Clinical Application of Mechanical Ventilation 2nd Edition. 2005
The impact of effective bronchodilation

β2 agonist
Muscarinic antagonist

LAMA/LABA combination inhalers
Long acting
muscarinic
antagonist
(LAMA)
Long acting beta
agonist (LABA)
Daily dosing
Anoro Umeclidinium
55 mcg
Vilanterol
22 mcg
One dose
Once daily
Ultibro Glycopyrronium
50 mcg
Indacaterol
110 mcg
One dose
Once daily
Duaklir Aclidinium
340 mcg
Formoterol
12 mcg
One dose
Twice daily
Spiolto Tiotropium
2.5 mcg
Olodaterol
2.5 mcg
Two doses
Once daily

Summary effects of LABA/LAMA combination versus comparators on changes in trough FEV1 at 3 months, 6 months and 12 months.
Yuji Oba et al. Thorax 2016;71:15-25
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.

Summary effects of LABA/LAMA combination versus comparators on changes in (A) St. George’s Respiratory Questionnaire and (B) Transition Dyspnoea Index at 3 months and 6 months.
Yuji Oba et al. Thorax 2016;71:15-25
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.

Summary effects of LABA/LAMA combination versus comparators on proportion of SGRQ and TDI responders at 6 months.
Yuji Oba et al. Thorax 2016;71:15-25
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.

Summary effects of LABA/LAMA combination versus comparators on COPD exacerbations.
Yuji Oba et al. Thorax 2016;71:15-25
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.

£32.50
£32.50
£32.50
£32.50
LAMA/LABA combination
£33.50
£33.50
LAMA alone
How much do they cost?

Treating airflow obstruction
bronchodilators
Use a LAMA/LABA combination inhaler

Treating airways inflammation
Inhaled steroids


TORCH 2007: exacerbations Placebo Salmeterol Fluticasone Salm/Flut
mod/severe 1.13 0.97* 0.93* 0.85*
requiring steroids
0.8 0.64* 0.52* 0.46*
hospitalised 0.19 0.16* 0.17 0.16*
pneumonia 3 year rate
12.3% 13.3% 18.3%* 19.6%*
ISOLDE 2000
Exacerbation rate
1.32/yr on placebo
vs
0.99/yr on fluticasone
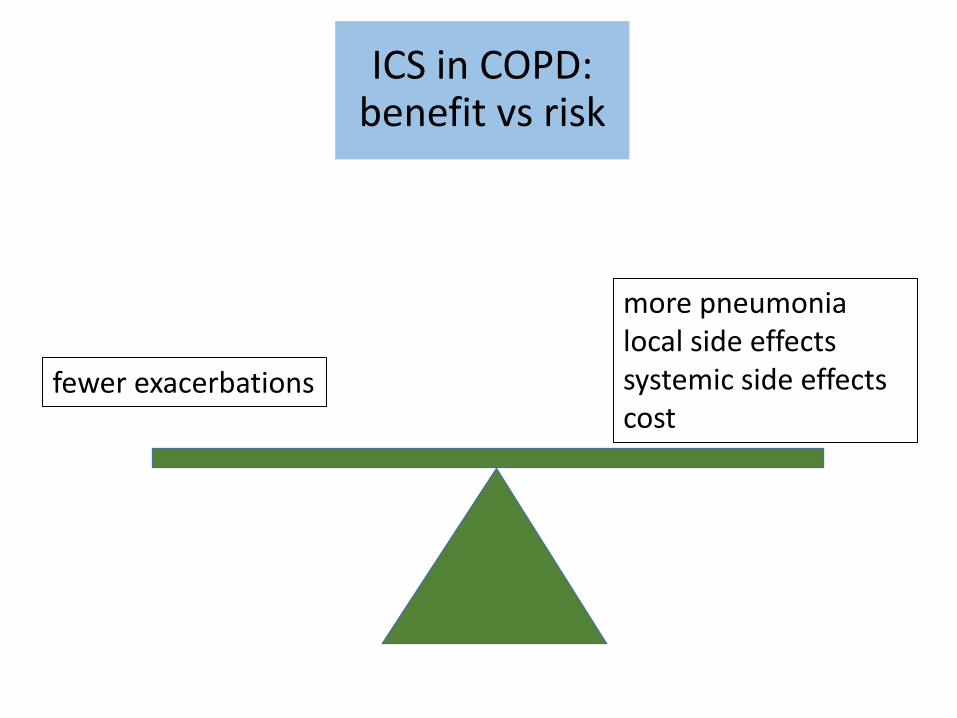
ICS in COPD: benefit vs risk
fewer exacerbations
more pneumonia local side effects systemic side effects cost

Dose–response curves for the rate ratio (solid lines) and 95% CIs (dashed lines) of
pneumonia as a function of inhaled fluticasone (blue lines) and budesonide (red lines) dose in
μg (measured in fluticasone equivalents) estimated by cubic splines model fit by conditional
logistic regression.
Suissa S et al. Thorax 2013;68:1029-1036
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.
fluticasone
budesonide

Steroid molecule beginning with F
Seretide fluticasone propionate
+ salmeterol
Relvar fluticasone furoate
+ vilanterol
Options?
Fostair fine particle beclometasone
+ formoterol
Duoresp Spiromax Symbicort budesonide + formoterol

Targeted steroid therapy

J. bras. pneumol. vol.32 no.3 São Paulo May/June 2006

Percentage reduction in moderate/severe exacerbation rates with fluticasone propionate (FP)/salmeterol (SAL) and monocomponents for treatment
comparisons of interest in ≥1-year studies by percentage baseline blood eosinophil level in (A) INSPIRE, (B) TRISTAN and (C) SCO30002.
Ian D Pavord et al. Thorax 2016;71:118-125
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.

Patient 1, aged 72 yrs, COPD
eosinophil reference range 0.04-0.4 x 109/L
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
04/09/2015 04/10/2015 04/11/2015 04/12/2015
eosinophil count
eosinophil count
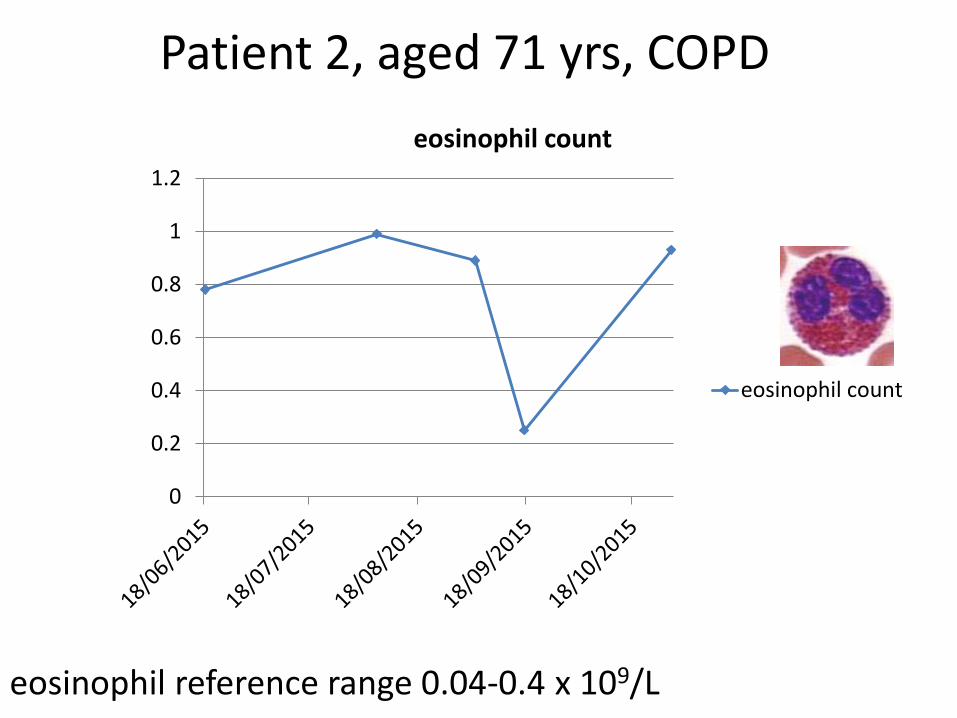
Patient 2, aged 71 yrs, COPD
eosinophil reference range 0.04-0.4 x 109/L
0
0.2
0.4
0.6
0.8
1
1.2
eosinophil count
eosinophil count

Conclusions
Treatable traits
Airflow obstruction
LAMA/LABA combination inhaler
Eosinophilic airway inflammation
inhaled corticosteroid

£57.92
£37.66
+
ICS/LABA LAMA
1.
2.
LAMA/LABA cheap ICS
+
Cost saving 35%


Targeted oral steroid therapy for acute exacerbations of COPD

Bafadhel, M, et al Am J Respir Crit Care Med 2012, 186, 48-55.
Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic
obstructive pulmonary disease: a randomized placebo-controlled trial

Bafadhel, M, et al Am J Respir Crit Care Med 2012, 186, 48-55.
Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic
obstructive pulmonary disease: a randomized placebo-controlled trial

Consort figure for all analysed data taken from the three randomised control trials
Mona Bafadhel et al. Eur Respir J 2014;44:789-791 ©2014 by European Respiratory Society
Blood
eosinophils
Intervention placebo prednisolone placebo prednisolone
Treatment
failure
(retreatment,
hospitalisation
or death
within 90 days
of
randomisation)
16/80
20%
22/84
26%
18/27
66%
12/109
11%
<2% ≥2%

Learning point
Blood eosinophils ≥2% (≈0.15 x 109/L)
identify risk and likely steroid responsiveness