Embed Size (px)
Citation preview

Building an ethical South Africa Reg. No. 1999/020697/08
CHRIS HANI
BARAGWANATH HOSPITAL
ETHICS AUDIT
Willem A. Landman
Ethics Institute of South Africa
Johann Mouton
Centre for Interdisciplinary Studies, University of Stellenbosch
Khanyisa H. Nevhutalu
Ethics Institute of South Africa
Research Report No. 2
© 2001


i
TABLE OF CONTENTS Page
List of Tables v
List of Figures vii
List of Boxes viii
List of Diagrams ix
ACKNOWLEDGEMENTS x
EXECUTIVE SUMMARY xii
SECTION 1: INTRODUCTION 1
1.1 Background 1
1.2 Research aims 6
1.3 Outline of report 9
SECTION 2: RESEARCH DESIGN AND METHODOLOGY 11
2.1 First phase: Focus groups 11
2.2 Second phase: Design and construction of pilot
questionnaires 12
2.3 Third phase: The ethics survey 12
SECTION 3: SAMPLE PROFILE 15
3.1 Staff profile 15
3.2 Patient profile 16

ii
SECTION 4: THE PHYSICAL PLANT/INFRASTRUCTURE,
MATERIAL RESOURCES, AND SECURITY 19
4.1 The physical plant 19
4.2 Medicine and linen 21
4.3 Cuts to the health-care budget 26
4.4 Quality and maintenance of equipment 27
4.5 Safety and security 27
Salient points 29
4.6 Concluding comments 29
SECTION 5: ORGANISATIONAL CULTURE AND VALUES 31
5.1 Perceptions of staff relations 31
Summary trends 36
5.2 Ratings of organisational values 36
Salient points 37
5.3 Ratings of professional values 38
5.4 Recommendations by respondents 43
5.5 Concluding comments 45
SECTION 6: LEADERSHIP, MANAGEMENT, AND
CHANNELS OF COMMUNICATION 47
6.1 Leadership and management 48
Salient points 48
6.2 Channels of communication 52
Salient points 54
6.3 Concluding comments 55
SECTION 7: HUMAN RESOURCES ISSUES 57
7.1 Job satisfaction 57
7.2 Conditions of service 58
7.3 Staff shortages 59
7.4 Concluding comments 60

iii
SECTION 8: MISCONDUCT AND STANDARDS OF CARE 63
8.1 Rank ordering of instances of misconduct 63
Salient points 65
8.2 Reasons for misconduct 67
Four main findings 68
8.3 Misconduct and the need for an ethics committee 68
8.4 Concluding comments 69
SECTION 9: PROBLEMS AND SOURCES OF STRESS 71
9.1 Most serious problems for the organisation
as a whole 73
9.2 Most serious problems for each category of staff 73
9.2 Most serious problems within each of four
categories of problems 75
9.4 Concluding comments 76
SECTION 10: PATIENT PERSPECTIVES 77
10.1 Relationship with nurses and doctors 77
Discussion 80
10.2 Levels of satisfaction with various aspects of
hospital services 81
Summary 83
10.3 Experience of unethical behaviour by hospital staff 83
10.4 Treatment by student nurses and student doctors 84
Discussion 86
10.5 Various ethical issues 86
Salient points 89
10.6 Concluding comments 89
iv
SECTION 11: CONCLUSIONS AND RECOMMENDATIONS 91
11.1 Conclusions 91
The foundation 92
First pillar: General organisational culture 93
Second pillar: Clinical care culture special to a
hospital as an institution 93
The pinnacle 93
11.2 Recommendations 93
Management and leadership 94
Human resources 96
Material resources 98
Admissions 101
Discipline and ethics 101
Patient care 103
Gauteng Department of Health and the Treasury 104
APPENDICES 105
Appendix 1: Letter accompanying questionnaires,
addressed to respondents 105
Appendix 2: Questionnaire: Management 107
Appendix 3: Questionnaire: Doctors 117
Appendix 4: Questionnaire: Allied Health Professionals 127
Appendix 5: Questionnaire: Nurses 137
Appendix 6: Questionnaire: Support Staff 147
Appendix 7: Questionnaire: Patients 157
Appendix 8: National Patients� Rights Charter
(National Department of Health) 163
Appendix 9: Mission Statement:
Chris Hani Baragwanath Hospital 167

v
LIST OF TABLES
Table 2.1: Comparison of designed and realised samples 13
Table 3.1: Average working experience by employee category 16
Table 3.2: Returning patients (How many times have you
been a patient?) 17
Table 4.1: Do you experience an under-supply of medicine
at CHBH? 21
Table 4.2: Do you experience a general shortage of line
at CHBH? 22
Table 4.3: Reasons for under-supply of medicine 22
Table 4.4: Reasons for linen shortage 24
Table 4.5: Perceptions about safety and security measures 28
Table 5.1: Ratings of organisational values 37
Table 5.2: Rank ordering of values 37
Table 5.3: Ratings of professional values 38
Table 6.1: Leadership, management, and channels of
communication 47
Table 6.2: Perceptions of channels of communication 53
Table 7.1: Perceptions of job satisfaction 57
Table 7.2: Perceptions of conditions of service 58
Table 8.1: Rank ordering of instances of misconduct 63
Table 8.2: Clinical staff�s observations of instances of
misconduct 66
Table 8.3: Reasons for misconduct 67
Table 9.1: Ratings of the main problems 71
Table 9.2: Most serious problems identified by doctors 73
Table 9.3: Most serious problems identified by nurses 74
Table 9.4: Most serious problems identified by allied health
professionals 74
Table 9.5: Most serious problems identified by support staff 75
vi
Table 10.1: Assistance by nurses on day duty 81
Table 10.2: Assistance by nurses on night duty 81
Table 10.3: Quality of medical treatment received 82
Table 10.4: Linen on your bed 82
Table 10.5: Quality of food 82
Table 10.6: The room you are in 82
Table 10.7: Incidents of unethical behaviour experienced
by patients 84
Table 10.8: Do you mind being cared for by student nurses? 85
Table 10.9: Do you mind being examined by student doctors? 85
Table 10.10: Patients who give money to staff at CHBH for
services or treatment act wrongly 87
Table 10.11: Staff at CHBH do not have sufficient time to treat
patients with the necessary compassion and
understanding 87
Table 10.12: Language barriers make it difficult for staff to
convey to patients proper information about their
diagnosis and treatment 87
Table 10.13: I sometimes find it difficult to understand what
doctors tell me about my illness 88
Table 10.14: I am always told what is wrong with me and why
certain medicines are given to me 88
Table 10.15: I usually find it easy to understand what nurses
tell me about my illness 88

vii
LIST OF FIGURES Figure 3.1: Age distribution of sample 15
Figure 3.2: Age distribution of patients 16
Figure 4.1: Physical plant: Clean to dirty ratings (staff and patient rating) 19
Figure 4.2: Physical plant: Safe to unsafe ratings (staff and patient rating) 20
Figure 4.3: Physical plant: Attractive � unattractive ratings (staff and patient rating) 20
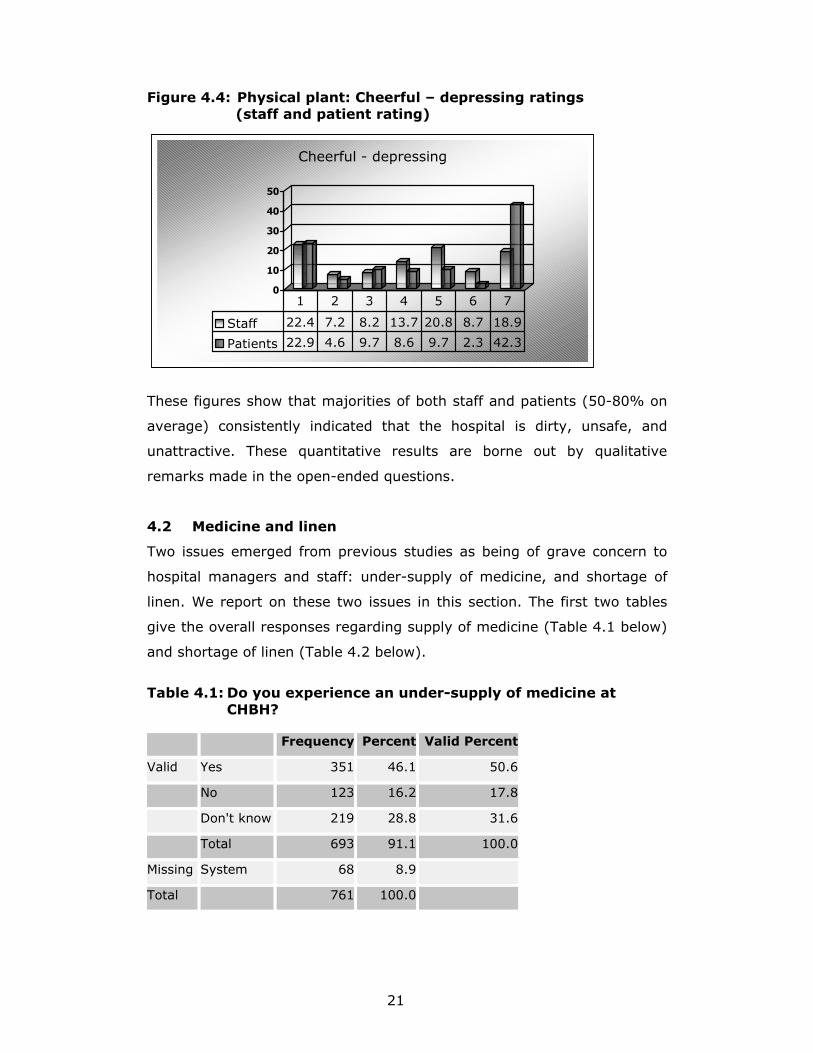
Figure 4.4: Physical plant: Cheerful � depressing ratings (staff and patient rating) 21
Figure 5.1: Honest � dishonest 31
Figure 5.2: Respectful � disrespectful 31
Figure 5.3: Loyal � disloyal 32
Figure 5.4: Trusting � distrusting 33
Figure 5.5: Professional � unprofessional 33
Figure 5.6: Relaxed � tense/stressed 34
Figure 5.7: Ratings of doctors by others 43
Figure 5.8: Ratings of nurses by others 43
Figure 6.1: Management takes suggestions from below
seriously 49
Figure 6.2: There are proper incentives to improve staff
performance 49
Figure 6.3: Staff members have a say in decision making 50
Figure 6.4: Hospital management is clear about employees�
career prospects 50
Figure 6.5: Top management has no secrets from employees 51
Figure 6.6: Management at CHBH is basically powerless 51
Figure 10.1: Nurses and doctors: Respectful � disrespectful 78
Figure 10.2: Nurses and doctors: Professional � unprofessional 78
Figure 10.3: Nurses and doctors: Relaxed � tense 78
Figure 10.4: Nurses and doctors: Caring � uncaring 79
Figure 10.5: Nurses and doctors: Compassionate � cold 79
Figure 10.6: Nurses and doctors: Approachable � unapproachable 79
Figure 10.7: Nurses and doctors: Trusting � distrusting 80

viii
LIST OF BOXES
Box 4.1: Medicine supply and control 23
Box 4.2: Linen shortage 25
Box 4.3: Theft of linen and equipment 25
Box 4.4: Budget 26
Box 4.5: Equipment 27
Box 4.6: Security concerns 28
Box 5.1: Respect for other professionals 32
Box 5.2: Professionalism and professional ethics 33
Box 5.3: Ethical values 34
Box 5.4: Discipline 35
Box 5.5: Staff relationships 35
Box 5.6: General working conditions 36
Box 5.7: Patient care related issues 39
Box 5.8: Problems encountered with patient admission 40
Box 5.9: Problems encountered with patient discharge 41
Box 5.10: Patient care and HIV/AIDS pandemic 41
Box 5.11: In-service and continuing education and training 44
Box 5.12: Need for team building 44
Box 6.1: Involvement of staff in decision making 48
Box 6.2: Management and leadership 52
Box 6.3: Communication 54
Box 7.1: Incentives 58
Box 7.2: Staff shortages 59
Box 8.1: General observations about staff misconduct 64
Box 8.2: Ethics and disciplinary committees 69
Box 10.1: Treatment by student nurses 85
Box 10.2: Treatment by student doctors 86

ix
LIST OF DIAGRAMS
Diagram 1.1: Conceptual framework for data collection
and analysis 8
Diagram 11.1: A hospital as an institution: Foundation,
cultural pillars, and pinnacle 92

x
ACKNOWLEDGEMENTS
The authors wish to commend the Chief Executive Officer (CEO) of Chris
Hani Baragwanath Hospital (CHBH), Reg Broekmann, who had the
courage of his conviction to commission this audit in the same year that
he took charge of the management of what is said to be the world�s
largest hospital. He faces a daunting task, within a public health-care
system under severe strain due to transformational changes, inadequate
budgetary provisions, an HIV/AIDS pandemic of momentous proportions,
and the like.
A number of people contributed significantly to various aspects of this
project. We wish to express our sincere gratitude to all of them. They are:
• Catharine Payze (University of South Africa), for conducting the
focus-group interviews at CHBH, and Marius van Wyngaard (Alpha
Transcriptions), for recording and transcribing them
• Brigitte Smit (University of Pretoria), for processing the data
generated by the focus-group interviews
• Brigitte Smit (University of Pretoria), Lesley Henley (University of
Cape Town), Donna van Bogaert, Percy Mahlati (CEO, South African
Medical Association), Ingrid Lohr (Ethics Resource Center,
Washington, DC, USA), and Catharine Payze (University of South
Africa), for participating in the workshop where we developed the
framework for the six questionnaires
• Joshua Joseph (Ethics Resource Center, Washington, DC, USA),
Lesley Henley (University of Cape Town), and Donna van Bogaert,
for critical comments on the questionnaires
• Jean Johnstone, Phinda Magwaza, Peggy Mohlamme, Claude
Mondzanga, Vis Naidoo, Salome Mothopi, Noxolo Nhose, Alice
Serobatse, and Johanna Sethsedi at CHBH, and Dorah Thekwe (St
Johns Eye Hospital), for assisting with arduous fieldwork at the
hospital
• Marthie van Niekerk (University of Stellenbosch), Dawie van
Niekerk, Maria Mouton (University of Stellenbosch), Charline

xi
Mouton, and Nelius Boshoff (University of Stellenbosch), for the
data capturing
• Nelius Boshoff (University of Stellenbosch), for the data formatting
• Lesley Henley (University of Cape Town) and Donna van Bogaert,
for critical comments on the recommendations
• Annelize Worst (Ethics Institute of South Africa), for preparing the
manuscript for publication
The Ethics Institute of South Africa (EthicSA) wishes to acknowledge the
financial support of The Merck Company Foundation, based in New Jersey
in the United States of America, which funds EthicSA�s infrastructure while
safeguarding its complete independence and integrity. The Merck
Company Foundation is a constituent of Merck and Company, the
multinational pharmaceutical company.
Willem A. Landman
CEO, Ethics Institute of South Africa
Johann Mouton
Director, Centre for Interdisciplinary Studies
University of Stellenbosch
Khanyisa H. Nevhutalu
Operations Director, Ethics Institute of South Africa
Pretoria
South Africa
2 November 2001

xii
EXECUTIVE SUMMARY
1. Background and objectives of the ethics audit
Various studies and surveys during recent years have highlighted that public
hospitals in South Africa are in a precarious state. Staff shortages, deteriorating
infrastructure, increased centralisation, equipment failures and shortages, and
an increased influx of (especially HIV/AIDS) patients, have all been identified as
factors contributing to a progressively worsening public health-care situation. In
the final analysis, such conditions seriously compromise the quality of patient
care.
An in-house survey, done in May 2000, found many of these problems exist at
Chris Hani Baragwanath Hospital (CHBH) as well. In addition, there were
indicators that the ethical fabric of the hospital was seriously problematic.
Towards the end of 2000, and against this background, CHBH approached the
Ethics Institute of South Africa (EthicSA), requesting it to undertake a
comprehensive ethics audit of the hospital. This study reports on the results of
the audit.
The specific objectives of the study were formulated as follows:
1. To identify the key ethical issues and problems that live in the �minds� of
the various �actors� in the hospital.
2. To establish what the general working environment is like at CHBH, and
the possible effects that factors in that environment might have on the
personal and interpersonal conduct of employees.
3. To describe in detail the �ethics culture� at CHBH by identifying the
salient attitudes, beliefs and values employees hold and the way in which
these affect everyday conduct in the hospital.
2. Research design and methodology
With a view to addressing these objectives rigorously and objectively, a design
consisting of three major phases was developed.

xiii
• First phase: Focus groups
In order first to identify the key ethical issues in the hospital (the first objective),
during April 2001 focus-group interviews were conducted with the five main
�categories of health personnel�, namely, central hospital management, doctors,
nurses, allied health professionals, and support staff. A sixth group consisted of
patients. Each group comprised of 8-12 individuals, except for the management
group that consisted of four individuals. The main purpose of the focus-group
interviews was to gather initial information that would reveal trends indicative of
ethical problems in the organisation. The main categories for the questionnaire
were developed on the basis of these discussions.
Second phase: Design and construction of pilot questionnaires
Six questionnaires, one for each of the subgroups, were then developed. Pilot
versions of each questionnaire were distributed in the hospital during July 2001.
The results of this pilot study were captured and analysed statistically. This led to
changes to all versions of the questionnaire. As a final check, the revised
questionnaires were sent to a panel of experts for comments. The final versions
of the six questionnaires were completed early August 2001.
Third phase: The ethics survey
The main component of the study was a sample survey conducted at CHBH. A
stratified multistage sampling design was used. Approximately 1 200
questionnaires were hand distributed with the help of staff and under the
supervision of one of the authors. This took place during the latter part of August
and early September 2001. On the basis of information provided to the research
team by the hospital, we were able to stratify the population into six categories.
3. Sample profile
The analysed dataset consists of 772 members of staff and 205 patients.
Concerning staff, a comparison between the sample categories and the overall
staff complement confirmed the representativeness of the sample. The salient
demographic features of the sample are as follows:
• Respondents were predominantly female (70%), with 30% male.
• When asked to indicate whether they belonged to a labour union, 89% of
respondents answered in the affirmative.
• The average respondent was at the hospital for 14 years, with no
differences between male and female employees.

xiv
Concerning patients, the following describes the main demographics of this
sample:
• In respect of gender, 65% of the 205 patients were female, 35% male.
• The vast majority of patients interviewed (95%) said that they were South
African citizens.
• Slightly more than a third (34%) indicated that they were first-time
patients at CHBH.
4. Physical plant/infrastructure, material resources,
and security
This section covers three aspects of the environment: the physical plant
(buildings), resources (especially medicine and linen), and security arrangements.
• Majorities of staff (on average) rated the buildings as dirty, unsafe, and
unattractive. Ratings by patients were, on the whole, very similar.
• A majority of staff (51%) indicated that there was, in their opinion, an
under-supply of medicine.
• A substantial majority (86%) of staff indicated that there was a general
shortage of linen at CHBH.
• In both cases � under-supply of medicine and linen shortage � cuts to the
health-care budget were cited as the most important reason for these
problems.
• More than two-thirds of staff agreed that the number of security staff was
inadequate (64%), and that they were poorly equipped to do their job
(76%).
• A majority of staff (57%) also believed that screening of visitors was
problematic.
• Nearly three-quarters (73%) were of the opinion that it was government�s
responsibility to ensure a safe environment.
Three summary conclusions can be drawn:
• The overwhelming majority of staff viewed the physical environment as
unacceptable.
• The shortage of linen was regarded as a much bigger problem than the
under-supply of medicine. In both cases staff listed a combination of
contributing factors.
• There is a huge lack of confidence in the capacity and ability of security
staff to ensure a safe environment.

xv
5. Organisational culture and values
Perceptions of staff relations:
• Two out of every five staff members were negative about various aspects
of staff relations, between 15 and 20% were undecided, with the
remaining 30-45% more positive.
• The one exception relates to whether staff relations are relaxed or tense
(stressed), a majority of staff (57%) rating this aspect negatively.
• It is clear from qualitative comments that morale is low and that most staff
members do not think that enough is being done to promote and establish
a healthy working climate in the hospital.
Organisational values:
In response to the question which of a number of values CHBH stands for, the
responses (in descending order of importance) are as follows:
• Serving the greatest number of patients possible (75%)
• Avoiding bad publicity (50%)
• Not having strikes and social unrest (45%)
• Balancing the books (38%)
• Good work ethic (35%)
• Providing the best possible working environment (32%)
These results show that more �administrative values� (number of patients served;
publicity; balancing the books/financial issues; good order) are valued higher than
a good work ethic and having a good working environment.
Professional values:
• Staff is clearly divided about whether doctors and nurses care for patients,
with 50% (on average) saying that doctors and nurses show sufficient
commitment to various aspects of patient care (�care� means compassion
for patients, confidentiality of patient information, and respect for the
dignity and well-being of patients), while the other 50% was split evenly
between 25% undecided and 25% negative about/disagreeing with the
quality of patient care.
• Concerning differences between the ratings of clinical-care provision by
doctors and nurses (as perceived by other staff members), the results
clearly reveal a significant gap, with doctors being rated higher than nurses

xvi
6. Leadership, management and channels of communication
Main points:
• There is little evidence of a participatory management culture, with three-
quarters (76%) of staff indicating they had no say in decision making. An
even higher proportion of doctors - 84% - held this view.
• There is clearly an insufficient degree of transparency in the hospital. This
is evidenced by rumour (the �grapevine�) being an important source of
information, too little communication between management and staff, and
too much secrecy.
• According to respondents, there is not enough commitment on the part of
central hospital management to staff development, incentives are
inadequate, and performance evaluations are insufficient.
• A substantial proportion of staff (45%) did not believe that employees
were allowed to say what they really thought.
• Communication between employees and their supervisors is less than
optimal - 50% of staff said their complaints had not been acted upon, and
nearly two-thirds (65%) said they had not received regular feedback from
their supervisors.
• A clear majority (54%) of staff also did not believe that there was a
system in place for reporting instances of misconduct.
• The fact that 62% of staff said that rumour was a common source of
information in the hospital is yet another indicator that existing channels of
and procedures for communication were regarded as inadequate.
One�s overwhelming impression, having analysed the data on management and
communication, is of an organisation that does not treasure participation and
consultation in decision making, where views of ordinary staff members do not
matter, and where opportunities for constructive communication are limited, if not
non-existent.
7. Human resources issues
Key findings:
• Respondents are generally satisfied with their jobs, and they find their jobs
interesting and even stimulating.
• Two-third of staff (66%) is proud to be associated with CHBH.

xvii
But there are also some less positive results:
• A very large proportion of staff (40%) frequently thought of quitting their
jobs.
• A clear majority (58%) felt as if they were working for a �second-class�
hospital.
• There was general dissatisfaction with salaries (75%) and workloads
(66%).
• Large proportions (over 50%) were dissatisfied with conditions of service
and prospects for promotion.
We believe that these results lead to two major conclusions:
• There is a kind of �split image� at work here. On the one hand, there is the
positive legacy or ideal of CHBH, but, on the other, its quality is declining �
or, rather, that is the perception.
• Although staff is positive about their own jobs and job contents, they are
very negative about staff development (no prospects for promotion; high
workload).
8. Misconduct and standards of care
Our key finding is that the extent of misconduct � as reported by staff � is serious
and points to a situation that is not conducive to professional and responsible
patient care. The following are some of the more salient points to emerge from
this analysis:
• There is widespread (physical and verbal) abuse of staff by patients, as
well as incidents of abuse of patients.
• This result is confirmed by the fact that nearly half of staff said that they
had observed incidents of negligence in patient care, and nearly one-third
indicated having witnessed substandard post-operative care.
• There is strong evidence that patients� rights are being violated - nearly
two out of every five staff members indicated that they had witnessed
incidents where informed consent had not been obtained, and one-third
said they had seen incidents where confidentiality of patient information
had been breached. These results are supported by evidence provided by
patients themselves.
• Although other forms of misconduct, such as bribery and over-ordering of
medicine, do not seem to occur as frequently as the ones listed above, it
must be emphasised that these are nevertheless transgressions of basic
ethical principles and require urgent attention.

xviii
•
• Given reported staff shortage, the fact that such a huge proportion of staff
(37%) seems to be involved in some form of moonlighting, clearly
warrants further investigation.
Responses suggest four clusters of possible reasons for observed instances of
misconduct.
• The reasons having most support among staff concern the lack of punitive
measures - no real or visible disciplining of misconduct occurs (60% of
staff)
• Working conditions - the heavy workload that leads to inadequate attention
to care (60% indicated it as a main reason)
• No consensus about ethical values - there is clearly insufficient agreement
about the meaning of misconduct as evidenced by the fact that substantial
proportions of respondents do not believe �tipping� and �fraud� to be
wrong.
• The demographics of patients, especially the existence of language
barriers, lead to misunderstanding and possibly abuse (about 50%-50%)
9. Problems and sources of stress
What are the main problems and sources of stress experienced and identified by
CHBH staff? We presented staff with 20 possible problems and asked them to
indicate which of these they rated as being the most serious problems.
Key findings:
The six most serious problems for the organisation as a whole are the following:
• Shortage of staff (83.1%)
• Linen shortage (70.9%)
• Substandard care because of large numbers (67%)
• Poor remuneration (65.5%)
• Unhygienic conditions (63.6) and lack of safety (63.4%)
• Poor maintenance of buildings (60.8%)
The five most serious problems for each category of staff are as follows:
• Doctors - general shortage of staff; unsanitary/unhygienic conditions;
poor/outdated equipment; poor remuneration; and long shifts
• Nurses - general staff shortage; linen shortage; substandard care because
of large numbers; poor remuneration; and lack of safety

xix
•
• Allied health professionals - general shortage of staff; poor maintenance of
buildings; poor remuneration; lack of safety; and poor staff communication
• Support staff � general shortage of staff; linen shortage; poor staff
communication; substandard care because of large numbers; and poor
remuneration
Concluding comments:
It is significant that the same basic issues (staff shortages; linen shortages;
substandard care; poor remuneration; lack of safety; and unhygienic conditions)
are recurring problems and sources of stress across all staff categories. This
suggests that these problems are hospital-wide and prevalent across departments
and staff functions, and, therefore, should receive urgent attention.
10. Patient perspectives
The views of patients were integrated into the report where they related to issues
common to all categories of respondents. Our attention here is on patients�
perspectives as they pertain to other issues.
Majorities of patients rated nurses and doctors as respectful, professional, caring,
approachable, and trustworthy. Although these figures, in broad outline, do
present a positive picture and might give cause for complacency, it is still worth
pointing out the following:
• 15% of patients viewed nurses and doctors as being disrespectful
• 22% of patients viewed nurses as being unprofessional
• 20% of patients experienced nurses as being uncaring and cold
• 19% of patients said nurses were unapproachable
• 20% of patients rated nurses as being distrusting
Expressed as numbers of patients, these findings relate to the actual experiences
of hundreds of patients (more than 500) in the hospital at any given time.
In order of satisfaction (combining �very satisfied� and �satisfied�), patients
indicated that they were the most satisfied with the following:
• Assistance received from nurses on day duty (74%)
• The quality of medical treatment received (74%)
• Assistance received from nurses on night duty (65%)
• Their rooms (62%)
• The quality of food (61%)
• The linen on their beds (58%)
xx
•
Salient points:
• The vast majority of patients (70%) agreed that giving money to staff for
treatment was wrong.
• A similar proportion of patients (71%) agreed that hospital staff did not
have sufficient time to treat them properly.
• Language barriers between staff and patients are a serious problem given
that three-quarters of patients said that such barriers posed difficulties for
mutual understanding. A similar proportion of patients (72%) indicated
that they had had problems understanding what doctors had told them
about their illness.
• Nearly two-thirds of patients (64%) claimed that they had not been told or
informed what was wrong with them and why they had received certain
kinds of medication.
• There seems to be better communication between patients and nurses,
with 62% of patients indicating that they found it easy to understand what
nurses told them about their illness. By contrast, almost three-quarters of
patients (72.5%) sometimes found it hard to understand what doctors
tried to communicate to them about their illness.
One�s overarching impression is that most patients are not well informed about
their illness, or the reason for the treatment or medication they receive, which are
basic patients� rights.
Concluding comments:
• Majorities of patients (ranging between 65 and 75%) rated nurses as being
respectful, professional, relaxed, compassionate, and the like. A small
minority of 10-20% of patients rated nurses to be disrespectful,
unprofessional, uncaring, and the like. However, it is interesting � and a
cause for concern � that nurses and doctors consistently received different
ratings for clinical care. These results are in line with earlier findings -
doctors get more positive ratings, within a range of 15�20% higher ratings
on all dimensions.
• Patients are mostly satisfied with the assistance and quality of medical
treatment they received. They are less satisfied with their rooms and the
quality of food, and least satisfied with the linen on their beds.

xxi
• There are unacceptably high levels of verbal abuse, especially by nurses
and support staff, patient information is not always treated in confidence,
and the quality of health care and professionalism leaves much to be
desired. These results are cause for grave concern and require immediate
action by hospital management.
• Relatively small proportions of patients indicated reservations about being
examined by student nurses and student doctors. Common reasons for
such reservations relate to perceived lack of professionalism, inexperience,
and possible lack of quality care.
• Concerning informed consent and general sharing of medical information,
most patients are not well informed about their illness or the reasons for
treatment or medication regimes.

xxii

1
SECTION 1 INTRODUCTION
1.1 Background
Almost on a daily basis, media reports describe the conditions of public
hospitals in South Africa as �appalling�, �shocking�, or, putting it more
strongly, as being in �dire straits�. In addition, numerous accounts of
profoundly unprofessional and unethical conduct often border on the
surreal. Health-care professionals, particularly doctors and nurses, in
public hospitals are reported to work in harsh and often squalid
conditions. In addition, extreme power differentials between nurses and
their poor, often illiterate or semi-literate, patients continue to exist. It is,
therefore, not surprising that nurses have been reported to employ
humiliation, verbal coercion and even physical violence to assert their
authority and control patient behaviour.1
The media regularly reports on alleged misconduct by doctors and other
health-care professionals. In November 2000, five months before the end
of that financial year, hospitals in the Eastern Cape ran out of money for
medicines and food for patients.2 In January 2001, a nursing sister at
Natalspruit Hospital�s paediatric department was reported to have been
haunted by the crying of babies. She and two of her colleagues took care
of more than sixty ill babies, aged between one and 12 months, in two
12-hour shifts a day. Their working conditions are not unique in what
appears to be an emerging trend in many public hospitals, plagued by a
variety of inadequacies, such as ageing buildings, a shortage of
equipment and medicines, understaffed units, and a growing population
of patients.3
Some of the hospitals were built as far back as 1860. Natalspruit Hospital
was constructed in 1973, but some of the buildings are said to be in a
state of disrepair. Over the past two years, the staff complement at
1 Tagwireyi, S. (2001). Public hospitals in dire straits. Mail & Guardian, 2-8 February 2001, 11. 2 Jewkes, R. et al. (1998). Why do nurses abuse patients? Reflections from South African Obstetric Services. Social Science and Medicine, 47(11):1781-1795. 3 Tagwireyi, S. (2001). Public hospitals in dire straits. Mail & Guardian, 2-8 February 2001, 11.

2
Natalspruit has shrunk from 1 093 to 871. Resigned nurses have not been
replaced. The remaining staff has been put under immense pressure by
having to cope with an average of 15 000 patients per month. The
situation is further aggravated by the impact of HIV/AIDS. �Admission is
around 110% and sometimes goes up to 140%�.4 A hospital the size of
Natalspruit needs about R106,5 million a year to function properly;
however, according to matron Khumalo at the hospital, government
allocates only 75% of that amount. 5
According to a media report6, doctors and hospital superintendents in
Gauteng presented a memorandum to the province in November 1998,
warning that �patients will die� if staff and budgetary cutbacks at
hospitals were not halted.7 The memorandum reads as follows:
�We cannot in good conscience accept that financial constraints will
mandate the collapse of health services in Gauteng. We are tired of
being held responsible by patients for dirty wards, long queues, no
beds, unfriendly and inadequate services. It is time for those in
power to stand up and be accountable for this crisis in public
hospitals�.
Hospital superintendents warned that health services were heading
toward �irreversible collapse�. During the same period, four babies at
Chris Hani Baragwanath Hospital (CHBH) died of klebsiella, a condition
resulting from unhygienic conditions. Only four nurses were on duty to
care for 35 babies in intensive care (IC), while the standard of care would
recommend a minimum ratio of one nurse for every two babies.8
An audit9 commissioned by the government in 1996 to investigate the
state of public hospitals nationwide, similarly reflected a bleak picture.
The report indicated that about 30% of hospitals are in a serious crisis,
11% of these need to be replaced, while 19% need major upgrading. The
audit report recommended that in order to remedy the deteriorating
4 Ibid. 5 Ibid. 6 Ibid. 7 Ibid. 8 Ibid. 9 Ibid. Despite numerous efforts by EthicSA, we were unable to obtain a copy of the original audit report from the Gauteng Department of Health.

3
condition of public hospitals, government has to review the state of most
of its 359 hospitals, upgrade some and replace others altogether.
According to Dr T Sibeko, the then Director of Hospitals in the Gauteng
Department of Health (DOH), �hospitals have been neglected over the
past years.�10
According to a 1998 study11, many of the patients interviewed reported
clinical neglect, and verbal and physical abuse by nursing staff, which was
at times reactive and, at others, ritualised in nature. Analysis of the data
revealed a complex interplay of concerns including organisational issues,
professional insecurities, a perceived need to assert �control� over the
environment, sanctioning of the use of coercive and punitive measures to
that end, and an underpinning ideology of patient inferiority. The study
asserts that the use of violence has become commonplace because of a
lack of local accountability for services and a lack of action by managers
and higher levels of the profession against nurses who abuse patients.12
The lack of a powerful competing ideology of professional patient care and
nursing ethics was identified as one of the factors leading to deterioration
in nurse-patient relationships, which became considered as �normal� in
nursing practice.
The national DOH13 emphasised government�s commitment to improve
the quality of care provided in the public health sector as a key challenge
during the next four years. The department highlighted the following as
critical: (1) the role of health-service users in ensuring that their needs
are met, and (2) the quality of care being of acceptable standard. The
DOH asserted that health-care providers also have an important role to
play in improving quality of care in the public health sector.
Worldwide, popular and professional discourses characterise nursing as a
profession of dedicated staff, exhibiting qualities of care, nurturing,
10 Ibid. 11 Jewkes, R. et al. (1998). Why do nurses abuse patients? Reflections from South African Obstetric Services. Social Science and Medicine, 47(11):1781-1795. 12 Ibid. 13 National Department of Health (1999). Health Sector Strategic Framework (1999-2004).

4
comfort and concern, and motivated by the desire to help people.14 The
same convictions and ideals are cherished and valued by the medical and
allied health professions. Nevertheless, the South African public health-
care situation is both intricate and confusing. A survey conducted in April
1999 by the Gauteng provincial government on the state of five public
hospitals in the province � namely, CHBH, Natalspruit Hospital, Pretoria
Academic Hospital, Sebokeng Hospital and Thembisa Hospital - identified
the following problems: poor management, shortage of staff and
medicines, long queues, and poor staff behaviour.15 The survey report
stated that surgical procedures had been compromised by a shortage of
basic supplies and services, and that nurses who had resigned from some
of these hospitals had not been replaced. This resulted in the remaining
staff working under stressful conditions with an average of 15 000
patients per month in some of these hospitals.
Sibeko blamed bad management for the poor state of most of the
province�s hospitals.16 This resulted in misconduct as well as ethically
unacceptable behaviour and attitudes of doctors and nurses.
According to the South African Health Review 200017 issued by the Health
Systems Trust (HST), the combined levels of bed provision in central and
tertiary hospitals in Gauteng and the Western Cape significantly exceed
the affordable norms of the Health Strategy Project (HSP). The HST
recommends that beds in these institutions be reduced in order to shift
funds to the resourcing of beds in feeder facilities. Alternatively, central
and tertiary hospitals should be resourced appropriately for multiple levels
of care. Lack of clarity about the levels of care provided in affected
hospitals impedes national planning. Capital infrastructure and equipment
are deteriorating at levels significantly exceeding existing spending on
rehabilitation, maintenance and replacement. The HST argues that
hospitals in a very poor condition (grade 1-2) would in most cases be
14 Davis, A.J. and Aroskar, M.A. (1983). Ethical dilemmas and nursing practice, 2nd edition. Norwalk: Appleton-Century-Crofts. 15 Tagwireyi, S. (2001). Public hospitals in dire straits. Mail & Guardian, 2-8 February 2001, 11. 16 Ibid. 17 Health Systems Trust. South African Health Review 2000. http://www.hst.org.za/sahr/2000/chapter11.html (Chapter 11: �Hospital restructuring�, authored by Boulle, A., Blecher, M., and Burn, A.)

5
written off. Data on the national pool of medical equipment are poor.
Models by the national DOH suggest serious problems with deterioration
of medical equipment. Models of replacement and maintenance suggest
an annual requirement of R1,02 billion per year. Backlogs of medical
equipment, repairs and maintenance exist in much of the country.
The HST review advises, however, that the key to efficient utilisation of
hospital services is the strengthening of the integrity of the various levels
of care and the referral systems between them, based on a clear
understanding of the differential costs of treating patients at the various
levels in the health-care system. Real increases in funding for hospital
services have on aggregate not translated into increased staffing or
outputs, but are likely to have been spent largely on increased salaries
and benefits.
A wide-ranging survey of the ethics of South African doctors� business
practices, conducted by the Ethics Institute of South Africa (EthicSA) in
2000, yielded strong evidence of widespread unethical business practices
among the country�s doctors (general practitioners and specialists),
including those in the public sector.18, 19
Given this background, EthicSA is convinced that there is a wide range of
issues relating to the (business) ethics of organisational and management
performance, involving public hospitals� organisational relationships with
employees, contractors, the public, and government. A second set of
issues relates to the (clinical) ethics, of relationships between health-care
professionals (doctors, nurses, and others) and patients. These two areas
of ethical concern - business and clinical ethics - are often interrelated,
and both form aspects of the organisational ethics of a hospital as an
institution.
18 Landman, W.A. and Mouton J. (2000). A Profession Under Siege? Medical Practice and Ethics in South Africa. Pretoria: Ethics Institute of South Africa, 4pp (Technical Report No. 1). 19 Landman, W.A. and Mouton J. (2001). A Profession Under Siege? Medical Practice and Ethics. Pretoria: Ethics Institute of South Africa, 93pp. (Research Report No. 1).

6
It is against this background that EthicSA was approached to undertake
an exploratory study of CHBH in order to examine (audit) its ethics
culture, commonly known as an �ethics audit�. We also wished to
ascertain the root causes of the reported appalling conditions at the
hospital, rather than concentrate merely on manifestations or symptoms
of poor performance of CHBH as an institution.
1.2 Research aims
The problems identified by the survey20 of five hospitals in Gauteng in
April 1999, highlighted the need for appropriate remedies. However, an
appropriate remedy requires identifying the nature of the organisation�s
problems by conducting an enquiry into its performance. One forms of
enquiry normally conducted is an ethics audit to assess the values and
beliefs, as well as the specific actions informed by them, of individuals or
personnel employed by an organisation.
The CHBH, situated on the outskirts of Soweto, has been considered
Africa�s largest hospital, and the largest in the southern hemisphere. In
1997, CHBH was entered in the Guinness Book of Records as the largest
hospital in the world, a claim that has, to our knowledge, not been
challenged. It has 3 400 authorised beds, of which 2 888 were occupied at
the time of writing. It caters for more than two million patients/clients per
calendar year, from Soweto and surrounding areas, with a staff
complement of 4 885 (in all categories of workers).
CHBH is a public hospital. The vast majority of South Africans (86%) are
not members of medical schemes, and are consequently completely
dependant on the public tier of our public/private health-care system. And
public hospitals account for 62% of public sector health expenditure.21
20 Tagwireyi, S. (2001). Public hospitals in dire straits. Mail & Guardian, 2-8 February 2001, 11. 21 Health Systems Trust. South African Health Review 2000. http://www.hst.org.za/sahr/2000/chapter11.html (Chapter 11: �Hospital restructuring�, authored by Boulle, A., Blecher, M. and Burn, A.).

7
Currently, CHBH does not have enough doctors or nurses to cope with
demands. Its resources and infrastructure are poor by world standards, as
well as South African standards. CHBH, like any organisation, is located in
� and influenced by - a larger environment, which includes people, other
organisations, social and economic forces, and public-policy and legal
constraints. More specifically, the environment includes markets (clients
or customers), suppliers, government and regulatory bodies, and
technological and special-interest groups.
In May 2000, CHBH conducted an in-house survey22. Areas covered by
the survey included a few questions on ethics, which indicated that a high
degree of mistrust exists amongst staff members - 57% did not think that
staff at CHBH value honesty; a significant proportion of staff found
corrupt ways to enrich themselves; and when pressed, many staff
members would lie to avoid adverse consequences for themselves.23
Following the survey report, CHBH committed itself to addressing the
problem of �weak ethics� over a five-year period. This current ethics audit
by EthicSA is the first major step by the hospital to address the ethical
problems identified by the earlier in-house survey.
Problems at public hospitals, highlighted by various sources in this
literature review, are complex, requiring multiple solutions. The findings
of the different surveys and audits, and their analyses, provide pointers
towards solutions, but considerable further research into the nature of the
problems and possibilities for change is required. Undoubtedly, the first
step for South Africa is to acknowledge that there is a problem and then
to embrace efforts to investigate it further and seek solutions. This ethics
audit of CHBH is only one step in such a process, but we believe it to be
important in the prevailing compromised circumstances.
The preceding literature review assisted us in developing the following
conceptual framework that guided the data collection and analysis in the
22 Chris Hani Baragwanath Hospital (May 2000): Employment Equity Report and Plan in terms of the Employment Equity Act (Act 55 of 1998). Johannesburg. 23 Ibid.

8
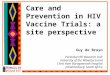
study (see Diagram 1.1 below). The underlying argument of the
framework can be summarised in the following set of premises:
1. Recent studies in South Africa all point to the fact that public hospitals
are under huge and increased pressures in terms of inadequate
funding, deteriorating infrastructure, and insufficient staffing.
2. These conditions in public hospitals put staff under increasing stress
and strain; most health-care professionals work in an �unhealthy�
environment.
3. These factors could - and this becomes the main question of the study
- produce behaviours and practices that are unprofessional and
unethical. It is a commonplace that �normal� patterns of behaviour
become difficult to maintain in �abnormal� circumstances.
Diagram 1.1: Conceptual framework for data collection and analysis
Internal organisational environment of the hospital: policies, procedures, values, culture
The actors:• Management • Doctors • Nurses • Other health
professionals • Support staff • Patients
The health discipline and profession: codes of conduct
The external environment: government, professional bodies, general public
9
1.3 Outline of report
In the next section (Section 2), we present an outline of the research
design and methodology used in this study.
This is followed, in Section 3, by a description of the sample profile.
The remainder of the report is organised as follows around different
categories of the findings:
Section 4: The physical plant/infrastructure, material resources, and
security
Section 5: Organisational culture and values
Section 6: Leadership, management, and channels of communication
Section 7: Human resource issues
Section 8: Misconduct and standards of care
Section 9: Problems and sources of stress
Section 10: Patient perspective
In the final section - Section 11 - we bring together our broad conclusions
in diagrammatic form, and put forward twenty-six recommendations,
based on the data and analysis of this report.

10

11
SECTION 2 RESEARCH DESIGN AND METHODOLOGY
The specific objectives of the study were formulated as follows:
1. To identify the key ethical issues and problems that live in the
�minds� of the various �actors� in the hospital.
2. To establish what the general working environment is like in CHBH,
and the possible effects that factors in the environment might have
on the personal and interpersonal conduct of employees.
3. To describe in detail the �ethics culture� at CHBH by identifying the
salient attitudes, beliefs and values employees hold, as well as the
way in which these affect everyday conduct in the hospital.
In order to address these objectives rigorously and objectively, a design
consisting of three major phases was developed.
2.1 First phase: Focus groups
In order first to identify the key ethical issues in the hospital (the first
objective), during April 2001 focus-group interviews were conducted with
the five main �categories of health personnel�, namely, central hospital
management, doctors, nurses, allied health professionals, and support
staff. A sixth group consisted of patients. Each group comprised 8-12
individuals, except for the management group that consisted of four
individuals. The main purpose of focus-group interviews was to gather
initial information that would reveal trends indicative of ethical problems
in the organisation. The data generated through focus-group interviews
were captured and transcribed and thoroughly discussed during a
workshop of experts held in Pretoria on 24 May 2001. The main
categories for the questionnaire were developed on the basis of these
discussions.

12
2.2 Second phase: Design and construction of
pilot questionnaires
Six questionnaires, one for each of the subgroups, were then developed.
Pilot versions of each questionnaire were distributed in the hospital during
July 2001. The results of this pilot study were captured and analysed
statistically. This led to changes made to all versions of the questionnaire.
As a final check, revised questionnaires were sent to a panel of experts
for comments. The final versions of the six questionnaires (see
Appendices 2-7) were completed early August 2001.
2.3 Third phase: The ethics survey
The main component of the study was a sample survey conducted at
CHBH. A stratified multistage sampling design was used. On the basis of
information provided to the research team by the hospital, we were able
to stratify the population into six categories. Detail on these categories is
as follows:
1. The management group includes the CEO, departmental heads, and
members of the Board of Management, which includes organised
labour unions.
2. The doctors group includes levels of the medical profession across
the board, for example, specialists, general practitioners, and
medical interns.
3. Nurse categories include a range, such as general trained nurses,
midwives, and enrolled nursing assistants.
4. The allied health professions group encompasses a variety of health
professionals, for example, pharmacists, physiotherapists,
occupational health therapists, speech and hearing therapists,
psychologists, social workers, dental therapists, medical scientists,
laboratory technicians, medical technologists, and radiographers.
5. Support staff includes porters, messengers, cleaners, cooks,
drivers, laundry workers, and security officers.
6. Patients are those admitted to any of the wards at CHBH with
chronic, acute, or terminal illnesses. They may also be patients
seen at CHBH�s out-patient departments or special clinics.

13
All questionnaires were hand distributed to participants by the respective
heads of departments or units at CHBH during the latter part of August
and early September 2001. An explanatory letter, addressed to
respondents, accompanied the questionnaires (see Appendix 1). One of
the authors of this report, Ms Nevhutalu, spent more than three weeks in
the hospital ensuring high rates of returns and assisting respondents
where needed. The realised sample is compared with the sample as
designed in Table 2.1 below.
Table 2.1: A comparison of the designed and realised samples
CATEGORY TOTAL
NUMBERSAMPLE
(DESIGNED) SAMPLE
(REALISED)Management 8 8 8Doctors 565 220 124Nurses 2 141 440 421Allied Health Professionals 227 160 88Support staff 1 944 150 131STAFF TOTAL 4 885 978 772Patients (general wards) 100 105Patients (outpatient depts.)
100 100
TOTAL QUESTIONNAIRES
1178 977
All questionnaires were subsequently captured in MS Access 2000. This
enabled us to capture all numeric and textual data. Numeric data were
then exported into SPSS Version 10 for statistical analysis. Cross checks
were made on the data to ensure high quality. A number of statistical
procedures were also run as validation checks.
Of the 1 178 questionnaires distributed in the hospital, a total of 977 were
completed (a sample realisation rate of 84%). In order to ensure
representativeness, the statistical data were subsequently weighted to
correct for any skewness in the sample. The realised sample (977 out of
the population of 4 885) constitutes a sample size of nearly 20%. The
large sample size, together with the stratified design and weighting of
data, have produced a dataset that is representative of the hospital in
every respect.

14

15
SECTION 3 SAMPLE PROFILE
Our design involved drawing two different samples: a representative
sample of staff (see description in previous chapter), and a representative
sample of in-patients and out-patients. We describe the key demographic
features of each sample separately.
3.1 Staff profile
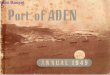
Respondents were predominantly female (70%), with 30% male. The age
distribution of the sample is presented in Figure 3.1 below.
Figure 3.1: Age distribution of sample
When asked to indicate whether they belonged to a labour union, 89% of
respondents answered in the affirmative.
We also asked respondents to indicate how long they had been working at
CHBH. The average respondent was at the hospital for 14 years, with no
differences between male and female employees. There are, however,
significant differences between different employee categories, as is
evident from Table 3.1 below. This Table also includes a column showing
the total years working experience for each category.
0
50
100
150
200
250
Age groups 9 145 246 220 95 13
<21 years
21 - 20
31-40 41-50 51-60 >60

16
Table 3.1: Average working experience by employee category
Employee category N Total years working experience Years working at CHBHManagement 8 24.00 13.50Doctor 117 11.42 7.26Nurse 398 15.68 14.35Allied Health Professional 79 10.51 7.86Support Staff 119 19.75 17.68Total 721 15.19 13.01 3.2 Patient profile
The sample of patients drawn for this study comprises equal proportions
of in-patients and out-patients. Assistance was given to those patients
who could, because of mother tongue preferences or illiteracy, not
complete questionnaires themselves.
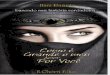
In respect of gender, 65% of the 205 patients were female, 35% male.
The age distribution of the patient sample is presented in Figure 3.2
below.
Figure 3.2: Age distribution of patients
The vast majority of patients interviewed (95%) said that they were South
African citizens. Slightly more than a third (34%) indicated that they were
first-time patients at CHBH. Table 3.2 below shows the pattern of
returning patients.
0
10
20
30
40
50
Age groups 17 39 44 26 28 27
<21 years
21 - 20
31-40 41-50 51-60 >60

17
Table 3.2: Returning patients (How many times have you been a
patient?)
Frequency Percent Valid
PercentCumulative
PercentValid Once before 34 16.6 21.4 21.4
Twice before 40 19.5 25.2 46.5Three times before 21 10.2 13.2 59.7Four or more times before
64 31.2 40.3 100.0
Total 159 77.6 100.0Missing System 46 22.4
Total 205 100.0

18

19
SECTION 4 THE PHYSICAL PLANT/INFRASTRUCTURE, MATERIAL RESOURCES, AND SECURITY
It stands to reason that the environment in which one works and the
material resources (infrastructure, equipment) with which one works are
important factors in determining job satisfaction and overall work
performance. This section looks at three aspects of the environment: the
physical plant (buildings), resources (especially medicine and linen), and
security arrangements.
4.1 The physical plant
Staff and patients were asked to rate various aspects of their physical
environment on a seven-point scale. The results are summarised in
Figures 7.1�7.4 below.
Figure 4.1: Physical plant: Clean to dirty ratings (staff and patient rating)
0
10
20
30
40
50
Clean - dirty
Staff 3.6 1.7 5.1 11.5 25 9.1 44
Patients 24.5 6 7.6 12 9.2 1.6 39.1
1 2 3 4 5 6 7

20
Figure 4.2: Physical plant: Safe to unsafe ratings
(staff and patient rating)
Figure 4.3: Physical plant: Attractive � unattractive ratings (staff and patient rating)
0
10
20
30
40
50
Safe - unsafe
Staff 3.7 3.6 7.5 6.8 18.4 15.1 44.8
Patients 29.4 7.3 7.9 8.5 7.9 2.3 36.7
1 2 3 4 5 6 7
0
10
20
30
40
50
Attractive - unattractive
Staff 4.1 1.7 8.5 10.1 22.3 15.7 37.7
Patients 17.6 4 10.8 9.7 11.9 1.7 44.3
1 2 3 4 5 6 7
21
Figure 4.4: Physical plant: Cheerful � depressing ratings (staff and patient rating)
These figures show that majorities of both staff and patients (50-80% on
average) consistently indicated that the hospital is dirty, unsafe, and
unattractive. These quantitative results are borne out by qualitative
remarks made in the open-ended questions.
4.2 Medicine and linen
Two issues emerged from previous studies as being of grave concern to
hospital managers and staff: under-supply of medicine, and shortage of
linen. We report on these two issues in this section. The first two tables
give the overall responses regarding supply of medicine (Table 4.1 below)
and shortage of linen (Table 4.2 below).
Table 4.1: Do you experience an under-supply of medicine at
CHBH? Frequency Percent Valid Percent
Valid Yes 351 46.1 50.6
No 123 16.2 17.8
Don't know 219 28.8 31.6
Total 693 91.1 100.0
Missing System 68 8.9
Total 761 100.0
0
10
20
30
40
50
Cheerful - depressing
Staff 22.4 7.2 8.2 13.7 20.8 8.7 18.9
Patients 22.9 4.6 9.7 8.6 9.7 2.3 42.3
1 2 3 4 5 6 7

22
Table 4.2: Do you experience a general shortage of linen at
CHBH?
Frequency Percent Valid
Percent
Valid Yes 601 79.0 85.7
No 24 3.1 3.4
Don't know 77 10.1 10.9
Total 702 92.2 100.0
Missing System 59 7.8
Total 761 100.0
As is evident, a majority of staff (51%) indicated that there was, in their
opinion, an under-supply of medicine. A substantial majority (86%) of
staff indicated that there was a general shortage of linen at CHBH.
What are the reasons for the under-supply of medicine? Table 4.3 below
lists the reasons in descending order of importance, whereas Box 4.1
below contains some of the qualitative comments made on this topic.
Table 4.3: Reasons for under-supply of medicine
Very great /
great extent
Moderate extent
Small / No extent
Total
Decreasing health care budget Count 308 42 94 444 % 69.3% 9.5% 21.2% 100.0%HIV/AIDS pandemic Count 281 53 112 446 % 63.0% 11.9% 25.1% 100.0%Influx of non-South African patients
Count 233 67 153 453
% 51.4% 14.8% 33.8% 100.0%Theft of medicines from hospital stocks by staff
Count 195 76 183 453
% 43.0% 16.7% 40.3% 100.0%Over-ordering of medicines by ward sisters
Count 95 82 287 464
% 20.5% 17.7% 61.8% 100.0%

23
To summarise, the main reasons for under-supply of medicine (combining
the first two categories) are:
• Health-care budget decrease (69%)
• HIV/AIDS patients (63%)
• Influx of non-South African patients (51%)
• Theft by staff (43%)
• Over-ordering of medicine (21%)
Box 4.1 Medicine supply and control Zulu speaking female radiographer at Radiology for three years: �Employ more pharmacy workers since there are long queues for medication and to order more; more medication since patients come a long way; some of them do not have money to travel every week because of medication insufficiency.� English speaking female doctor for 18 months at CHBH: �Under-supply of medicine I believe is due mainly to a shortage of funds due to budget cuts.� English speaking female doctor for one year at CHBH: �Proper seating facilities for patients waiting for medication should be provided as there are always long queues.� English and German speaking female doctor for eight years at CHBH: �Pharmacy: no pharmacy assistants � too many mistakes! They don�t bother to phone us with information if something is out of stock � just sent patient home.� Southern Sotho speaking female nurse at the Maternity Section for eight years: �There should be a pharmacist allocated in the special units, e.g. labour ward, who would see to it that adequate medicine is ordered as it is difficult to order for instance once in a week in a quick turnover department.� Zulu speaking female nurse at St Johns Eye Section for ten years: �With regard to medicines, I recommend that the hospital employs other pharmacists and some dispensaries to be open 24 hours and even over weekends and holidays as per needs.� Zulu speaking female nurse at the Medical Section for 13 years: �Supervisors to attend meetings with chief pharmacist regularly and ward pharmacist to visit the ward at least weekly to check the stock.� Northern Sotho speaking male nurse at the Medical Admission Section for one year: �Dispensary to be opened at night (24 hrs); staff given internal accommodation in Bara - like any other hospital; this will help nurses who come on duty early.� Tswana speaking female nurse at Paediatrics for 17 years: �Most outsiders (non-South Africans) are pharmacists. They steal a lot of expensive medicine. They claim that they earn little money � this is a great problem and a great concern for us South Africans.�

24
Box 4.1 (continued) Xhosa speaking female nurse at Psychiatric Department for 15 years: �I think the new government has introduced free medicine to all. Has created a big problem because government is trying for each patient to get medicine by supplying cheap stuff for medicine that makes them to come to hospital every day.� Swazi speaking female nurse at the General Section for 12 years: �Medicine should be given according to the needs of each department and not according to the needs of each pharmacy's preference or representatives� demands. As there is a high death rate related to AIDS, our patient might also attack staff members.�
Concerning linen shortage, Table 4.4 below summarises the main reasons
(organised in descending order of importance).
Table 4.4: Reasons for linen shortage
Very great / great extent
Moderate extent
Some / Very little
extent
Total
Decreasing health care budget
Count 352 76 144 572
% 61.6% 13.3% 25.2% 100.0%Increased patient population related to the HIV/AIDS pandemic
Count 333 88 170 591
% 56.3% 14.9% 28.8% 100.0%Ineffective logistical and practical arrangements
Count 307 137 124 569
% 54.0% 24.2% 21.9% 100.0%Stealing of linen by hospital staff
Count 293 79 230 601
% 48.7% 13.1% 38.2% 100.0%Linen theft committed by patients
Count 132 97 351 580
% 22.8% 16.7% 60.5% 100.0%
Summary of reasons for shortage of linen:
• Health-care budget decrease (62%)
• HIV/AIDS patients (56%)
• Ineffective logistics (54%)
• Theft by staff (49%)
• Theft by patients (23%)

25
We have included two boxes on the issue of linen shortage. The first box
(Box 4.2 below) contains comments about linen shortage in general; the
second (Box 4.3 below) lists remarks that specifically comment on the
theft of linen and other hospital equipment.
Box 4.2 Linen shortage English speaking male therapist at the Rehabilitation Section for 18 months: �Possibly contracting of laundry services to outside/private companies, e.g. for handling of linen.� Tswana speaking female nurse at Ophthalmology for 13 years: �The linen problem is because there is no effective mechanism in place to sort it out. Staff in laundry are not well supervised. Stealing is mainly by them (staff) as they have access to mostly new linen. Patients also contribute to this shortage as they also steal it. Education should be done to community at large to tell them that if they remove linen from the hospital they will be prosecuted. Towels of the hospital are at the taxi rank and no one makes an effort to collect them. Strong disciplinary action should be used to stop stealing, e.g. pay (salary) deduction to buy the stolen goods, or work without pay and, ultimately, dismissal. Southern Sotho speaking female radiographer at Radiology for 21 years: �Each department - stock control of linen. Penalties for shortage - that way a department will make sure linen is counted correctly every time.� Venda speaking female nurse at the Medical Section for 19 years: �Good maintenance and repair of equipment, servicing of laundry machines, since they are mostly not working. Control measures to avoid theft need to be considered when issuing linen since we have AIDS epidemic, to send linen daily and have all linen type packed, not just e.g. trousers without pyjamas.� Zulu speaking female nurse at Psychiatry for five and half year: �Buy more linen and have it washed or delivered two times a week. Have more equipment that is up to date.�
Box 4.3 Theft of linen and equipment English speaking female speech therapist at the Speech Therapy/Audiology Section for ten years: �More staff should be employed to develop and instate systems to improve these areas, also improved stock control (theft by staff).� Southern Sotho female speaking therapist at the Occupational Therapy Section for one year: �Theft - no one is allowed to leave the hospital with any equipment; security should start taking their job seriously and stop accepting bribes from staff and visitors.� Venda speaking female nurse at the Medical Ward for 19 years: �Rooms to be kept locked at all times. Report anyone suspected of stealing, and measures to be taken.� Xhosa speaking female nurse at the Surgical Section for 14 years: �Everybody, regardless of position he or she is holding in the hospital, must be searched to avoid theft.� Zulu speaking female nurse at the Surgical Section for 32 years: �Devise means of controlling theft by placing surveillance cameras around the hospital.�

26
Box 4.3 (continued) Tswana speaking female nurse at Ophthalmology for 13 years: �Stealing is mainly by them (staff) as they have access to mostly new linen � Strong disciplinary action should be used to stop stealing, e.g. pay (salary) deduction to buy the stolen goods, or work without pay, and ultimately, dismissal.� English speaking female doctor at CHBH for four years �Much of the non-medical activities such as porters, linen supply and cleaners need to be outsourced, as these are areas of usage of resource base in a very inefficient manner. It will also allow for the medical staffing and remuneration issues to be dealt with more efficiently.�
4.3 Cuts to the health-care budget
In the cases of both under-supply of medicine and linen shortage, cuts to
the health-care budget were cited as the most important reason for these
problems. Box 4.4 below summarises some of the comments made about
budget cuts.
Box 4.4 Budget Swazi speaking female dietician at Human Nutrition Division for five months: �Increase health-care budget together with logistical and practical arrangements; can help in improving or resolving resource management.� English speaking male doctor at CHBH for six years: �Realistic budget, budget based not on money saving but on real needs of community. Decentralised ordering system.� English speaking female doctor at CHBH for 18 months: �Under-supply of medicine I believe is due mainly to a shortage of funds due to budget cuts - if the pharmacy budget is increased, I believe this problem would be alleviated.� Xhosa speaking female nurse at the Maternity Section for 12 years: �That CHBH should not be declared as an only referral hospital in Gauteng region without enquiring [at] Bara [about] enough budget and staff - because that leads to overcrowding in hospital. That patients must pay for the service they get.� Zulu speaking female nurse at the Maternity Section for 17 years: �I think if there can be control over patients flocking from all over South Africa and outside countries, e.g. from Malawi to Bara, maybe we can manage to have enough because most of our budget finances are wasted by outside people whilst they leave their places where their health monies have been allocated to them.� Zulu speaking female nurse at the Medical Admission Ward for 19 years: �Government should increase budget to hospitals as they say patients should be treated for free. They (government) legalised TOPs [termination of pregnancy patients] free of charge and legalised the influx of non-South Africans to South Africa, hence the high number of patients, hence the shortage. Patients should be referred back to their nearest hospitals unless being referred by a doctor from their nearest hospital for e.g. specialist treatment or therapy.�

27
4.4 Quality and maintenance of equipment
Although not separately probed, the issue of the quality and maintenance
of equipment was mentioned so frequently that we list the qualitative
comments in Box 4.5 below.
Box 4.5 Equipment Xhosa speaking female nurse at Psychiatry for five years: �Equipment must have big and bold wording that will embarrass the person stealing.� Afrikaans speaking female dietician at Human Nutrition Division for five year: �Hospital should be broken down into more manageable units where better control can be exercised over equipment, etc.� Southern Sotho speaking male radiographer at Radiology for 21 years: �Staff must take care of equipment, there must be service contracts with good, reliable and reasonable companies assigned to check on these equipment.� Zulu speaking female nurse at CHBH for 18 years: �People must be taught about the expense and proper usage of items to prevent shortage, e.g. know of cost of a machine; maybe when they handle things they will always be conscious.� Tswana speaking female nurse at the Ophthalmology Division for 13 years: �Management should involve staff that use equipment before ordering. Some equipment is forced on staff; therefore there is a reluctance to use them, e.g. needle incinerators. When staff request equipment that they feel they need, they are told there is no money, e.g. defibrillators or ECG machines, but useless things are bought.� Southern Sotho speaking female nurse at the Maternity Section for 14 years: �Equipment used at CHBH is very old. Though not all, but most of it is old. It must be replaced with new equipment here and there to assist the old equipment, because it malfunctions many a time; send for repairs and within no time it is again out of order, because it is overused due to an overflowing hospital.� Southern Sotho speaking female nurse at the Medical Ward for three years: �There is nothing more frustrating than running around the whole hospital looking for equipment, especially at night.� Xhosa speaking female nurse at the Maternity Section for 28 years: �Equipment - follow up by department, or any department, to various firms that are repairing, to solve the problem immediately. Some of the equipment, they go up to 12 months or more to a supposed servicing company without any report being sent to CHBH informing the hospital as to whether or not the equipment is being condemned or not.�
4.5 Safety and security
A recurring theme during previous studies, as well as during the focus-
groups interviews with different staff categories, is the lack of adequate
safety measures. There are feelings of insecurity and perceptions that
security staff at CHBH are not well-trained and are � in fact � more part of
the problem than the solution. These issues were raised in both the close-

28
ended (see Table 4.5 below) and open-ended questions (see Box 4.6
below).
Table 4.5: Perceptions about safety and security measures
Agree Disagree No opinion
Total
The screening of visitors leaves much to be desired
Count 406 219 89 714
% 56.8% 30.7% 12.5% 100.0%
The unsafe environment at CHBH can be related to the influx of non-South African patients
Count 227 376 111 714
% 31.8% 52.7% 15.5% 100.0%
The number of security staff at CHBH is sufficient to combat crime
Count 187 455 70 713
% 26.3% 63.9% 9.9% 100.0%
Security staff at CHBH is well equipped with the necessary skills and facilities to combat crime
Count 93 543 83 718
% 13.0% 75.5% 11.5% 100.0%
The security screening of applicants for employment leaves much to be desired
Count 265 228 199 692
% 38.3% 32.9% 28.7% 100.0%
It is the responsibility of government to ensure a safe environment at CHBH
Count 527 155 42 724
% 72.8% 21.5% 5.7% 100.0%
Box 4.6 Security concerns Zulu speaking female nurse at the General Section for 16 years: �Proper training of security staff and proper searching of cars and people leaving the hospital. I think the securities, too, should be searched because they also take hospital properties outside.� Zulu, Sotho and Xhosa speaking female nurse at the Medical Section for 22 years: �I think the best suggestions is to exchange securities at the gates because they are being bribed by the people; moreover dispensary people, stores people and kitchen people they eat together and share whatever, and there is this senior security [name edited out], who is treating people very badly. He likes Zulu people in hospital; he still has apartheid; even his colleagues are threatened because of him and his group. Some of group still want medication and they are buying expensive posh cars. You will even wonder where does he get all this money because of the drugs they are stealing. Thank you.�

29
Salient points
• More than two-thirds of staff agreed that the number of security
staff was inadequate (64%), and that they were poorly equipped to
do their job (76%).
• A majority of staff (57%) also believed that the screening of visitors
was poor.
• Nearly three-quarters (73%) were of the opinion that it was
government�s responsibility to ensure a safe environment.
4.6 Concluding comments
There are three summary conclusions:
• Without question the overwhelming majority of staff views the
physical environment as being unacceptable.
• As regards resources, it is significant to note that the shortage of
linen is regarded as a much bigger problem than the under-supply
of medicine. Interestingly, in both cases staff lists a combination of
factors that contribute to this situation.
• There is a huge lack of confidence in the capacity and ability of
security staff to ensure a safe environment.

30

31
0.00%
10.00%
20.00%
30.00%
Honest/Dishonest
15.60%
7.70%
12.90%
21.70%
23.50%
4.00%
14.60%
1 2 3 4 5 6 7
0.00%
10.00%
20.00%
30.00%
Respectful/Disrespectful
15.50%
10.40%
17.30%
15.90%
21.50%
6.20%
13.10%
1 2 3 4 5 6 7
SECTION 5 ORGANISATIONAL CULTURE AND VALUES
Three aspects of the organisational culture were examined:
• Perceptions of staff relations
• Ratings of various organisational values
• Ratings of various professional values
5.1 Perceptions of staff relations
How does staff rate their relations with their colleagues at the hospital?
Six value sets were given to respondents to rate on a seven-point scale,
ranging from very positive (Point 1) to very negative (Point 7). The results
for the hospital as a whole are summarised under each value. (Points 1-3
represent degrees of positive ratings, Point 4 represents the middle
category or �neutral� option, and Points 5-7 represent degrees of negative
ratings.)
Figure 5.1: Honest � dishonest
Similar proportions rated
honesty (36%) and
dishonesty (42%) equally,
with 22% selecting the
middle category (see Figure
5.1).
Figure 5.2: Respectful - disrespectful
The sample was split on its
ratings, with 43% selecting
the �respectful� end of the
spectrum, 16% the
�neutral� option and 41%
the �disrespectful� end of
the scale (see Figure 5.2).
Box 5.1 summarises some of the qualitative comments made with regard
to the issue of respect.

32
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
Loyal/Disloyal 15.00 8.50 18.40 16.30 22.70 7.70 11.30
1 2 3 4 5 6 7
Box 5.1 Respect for other professionals Male radiographer at X-Rays for one year: �All we need is respect. Seniors, juniors and students should respect one another and respect patients. We should be informed of what is going to be done in our department in time so that we can have a say, you know! More staff should be hired to reduce stress.� Female doctor at CHBH for four years: �There is a total lack of respect in all ranks � clerks, cleaners, medical staff, nurses. Unfortunately, individuals don't know their job descriptions, and this would be the first step in rectifying the situation. Employing more staff.� Female nurse at Orthopaedic for 13 years: �Respect goes a long way and personally I feel everyone seems to feel nurses are their punching bags. So, if the multi-disciplinary team can acknowledge that each of us has an important role to play, things will be much better.� Female nurse at Surgical Section for six years: �Respect and professionalism have to exist among staff members. People should respect each other and they should behave professionally.� Female nurse at Medical Ward for 15 years: �Supervisors should respect their subordinates, treat them with dignity, then everything will run smoothly. Supervisors should also be approachable, have listening skills.� Female nurse at Ortho-gynaecology for eleven years: �Our seniors must respect our juniors, e.g. when I am in the middle of something the senior must suggest an appropriate time to see him/her and not demand now. They should also address us in private and not in front of patients.�
Figure 5.3: Loyal - disloyal
The split in responses is
quite even: 43% loyal;
16% middle; and 41%
rating staff relations high
on disloyalty (see Figure
5.3).

33
0.00%
10.00%
20.00%
30.00%
Trusting/Distrusting 14.00 7.10 16.50 22.00 18.30 8.60 13.50
1 2 3 4 5 6 7
0.00%
10.00%
20.00%
30.00%
Professional/Unprofessional
20.90%
11.50%
12.50%
13.80%
21.50%
7.80%
11.90%
1 2 3 4 5 6 7
Figure 5.4: Trusting � distrusting
The sample was split on
its ratings, with 38%
selecting the �trusting�
end of the spectrum, 22%
the �middle� option, and
41% the �distrusting� end
of the scale (see Figure
5.4).
Figure 5.5: Professional � unprofessional
Nearly half of the sample
(45%) rated staff
relations to be
professional, 14% chose
the middle option, and
41% the �unprofessional�
end of the scale (see
Figure 5.5). Some of the
comments made on the issue of professionalism and professional values
are listed in Box 5.2.
Box 5.2 Professionalism and professional ethics Female occupational therapist at Occupational Therapy for one year: �Professionalism should be emphasised in the work place.� Male radiographer at Radiology for seven years: �Patient care has to be the first priority.� Female doctor for four years: �Senior nurses should not be cleaning and feeding patients. These tasks can be performed by competent nursing auxiliaries. We need more staff!� Male person at Management for two years: �Commitment to professional ethics.� Female radiographer for Radiology for 21 years: �Polite communication. Call patient by name. Make him/her feel good or like a human being. Respect [patients�] religion, race, culture, behaviour wishes, fears, etc. Be patient.�

34
0.00%
10.00%
20.00%
30.00%
40.00%
Relaxed/tense 10.70 7.60% 9.00% 15.90 12.40 10.20 34.30
1 2 3 4 5 6 7
Figure 5.6: Relaxed � tense/stressed
A significant majority
(57%) of staff believed the
climate in the hospital to be
tense or stressed, 16%
chose the middle option,
and only 27% rated the
climate as being relaxed
(see Figure 5.6).
Qualitative responses commenting on ethical values in general are listed
in Box 5.3 below.
Box 5.3 Ethical values Female radiographer at Radiology: �Transparency, honesty, trust, no favouritism in allocating work to people. Respect your juniors and remember they are adults.� Female dietician at Human Nutrition for five months: �Staff need to be honest, respectful (etc).� Female doctor at CHBH for one year: �Lack of trust among colleagues is a major problem.� Female nurse at the Operating Theatre for 27 years: �Tolerance, accepting each other, professionalism, professional secrecy, no gossip, avoid people's affairs because they are none of your business. All under the cover of love; love each other.� Female nurse at the Surgical Section for 30 years: �Respect most important, supervisors to stop loving this one and disliking that one, stop receiving �threats� from subordinates. Things must be explained well to both senior and subordinates; any changes tell on how her conduct is. Be professional.� Female nurse at the Maternity Ward for six months: �Staff members should conduct themselves professionally, improve their respect to both fellow workers and patients, and treat them with dignity.� Female doctor at CHBH: �Some ways or means of ensuring that all employees fulfil their work obligations should be put in place. Many patients are on medical aids, or are foreigners who give false local addresses - the hospital loses out on revenue from these patients. Measures should be instituted to detect this.� English speaking male doctor at CHBH for 5 years: �The hospital needs a complete makeover of attitude, management and ethics.� Xhosa speaking female nurse at Paediatrics for 24 years: �The government should allocate people to be their investigators and they should be honest and responsible.�
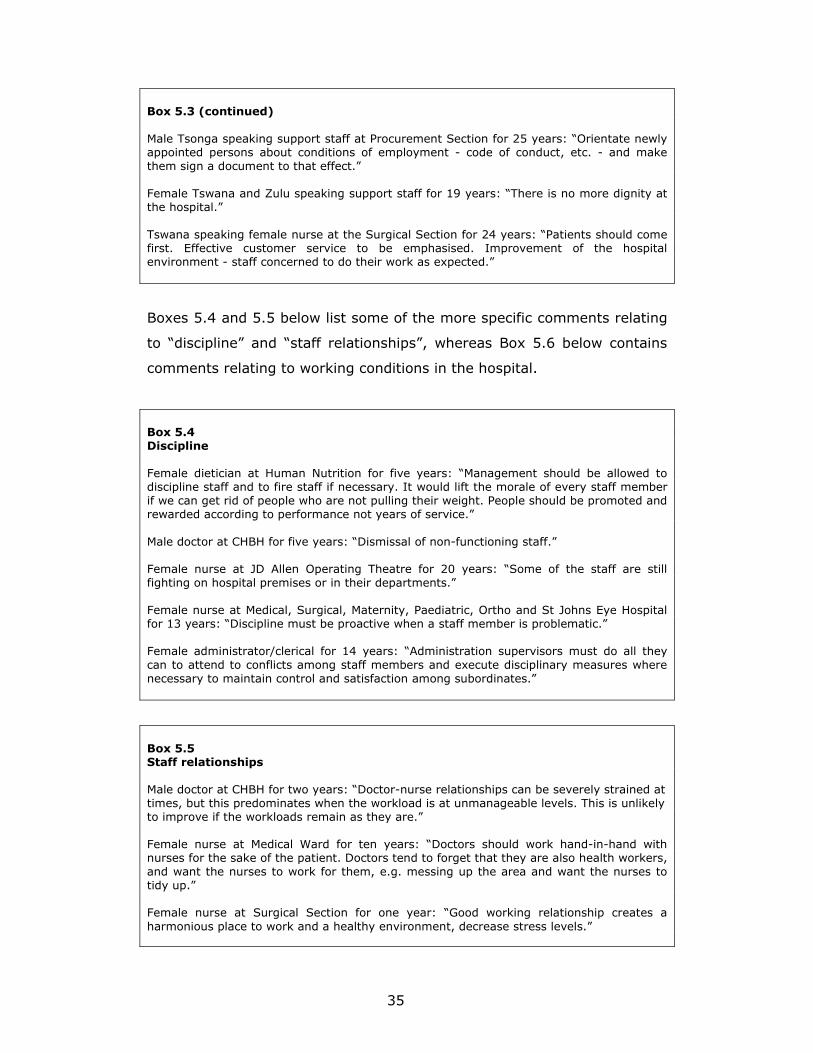
35
Box 5.3 (continued) Male Tsonga speaking support staff at Procurement Section for 25 years: �Orientate newly appointed persons about conditions of employment - code of conduct, etc. - and make them sign a document to that effect.� Female Tswana and Zulu speaking support staff for 19 years: �There is no more dignity at the hospital.� Tswana speaking female nurse at the Surgical Section for 24 years: �Patients should come first. Effective customer service to be emphasised. Improvement of the hospital environment - staff concerned to do their work as expected.�
Boxes 5.4 and 5.5 below list some of the more specific comments relating
to �discipline� and �staff relationships�, whereas Box 5.6 below contains
comments relating to working conditions in the hospital.
Box 5.4 Discipline Female dietician at Human Nutrition for five years: �Management should be allowed to discipline staff and to fire staff if necessary. It would lift the morale of every staff member if we can get rid of people who are not pulling their weight. People should be promoted and rewarded according to performance not years of service.� Male doctor at CHBH for five years: �Dismissal of non-functioning staff.� Female nurse at JD Allen Operating Theatre for 20 years: �Some of the staff are still fighting on hospital premises or in their departments.� Female nurse at Medical, Surgical, Maternity, Paediatric, Ortho and St Johns Eye Hospital for 13 years: �Discipline must be proactive when a staff member is problematic.� Female administrator/clerical for 14 years: �Administration supervisors must do all they can to attend to conflicts among staff members and execute disciplinary measures where necessary to maintain control and satisfaction among subordinates.�
Box 5.5 Staff relationships Male doctor at CHBH for two years: �Doctor-nurse relationships can be severely strained at times, but this predominates when the workload is at unmanageable levels. This is unlikely to improve if the workloads remain as they are.� Female nurse at Medical Ward for ten years: �Doctors should work hand-in-hand with nurses for the sake of the patient. Doctors tend to forget that they are also health workers, and want the nurses to work for them, e.g. messing up the area and want the nurses to tidy up.� Female nurse at Surgical Section for one year: �Good working relationship creates a harmonious place to work and a healthy environment, decrease stress levels.�

36
Box 5.6 General working conditions Female nurse at Medical Ward for 19 years: �Improve staffing and proper personnel utilisation. Decrease the workload; seminars for stress relief; in-service education and on-the-job-training; detect teachable moments for staff to regain job satisfaction. Stop being biased. Do work according to job description.� Female doctor at CHBH: �Everybody is stressed; staff shortages; too many patients; long hours; poor standards of working conditions lead to poor staff relations; patient load; improve working conditions.� Female support staff at Auxiliary Services for 12 years: �Create mechanisms to boost staff morale.� Female nurse at Maternity Ward for eight years: �Minimise stress in all respects; seniors to respect juniors and juniors to respect seniors.�
Summary trends
Two out of every five staff members are negative about various aspects of
staff relations, between 15 and 20% are undecided, with the remaining
30-45% more positive. The one exception relates to the question whether
staff relations are relaxed or tense (stressed), a majority of staff (57%)
rating this aspect negatively.
In addition, it is clear from qualitative comments that morale is low and
that most staff members do not think that enough is being done to
promote and establish a healthy working climate in the hospital.
5.2 Ratings of organisational values
Respondents were also asked to indicate which values CHBH stands for. A
summary of responses is presented in Table 5.1 below, in descending
order according to which values were rated most positively.

37
Table 5.1: Ratings of organisational values
Very great extent
Great extent
Moderate extent
To some extent
Very little extent
Serving the greatest number of patients as possible
N 416 129 85 67 25
% 57.6% 17.9% 11.7% 9.3% 3.4%
Not having strikes and social unrest
N 159 145 158 102 105
% 23.7% 21.7% 23.6% 15.2% 15.7%
Balancing the books N 118 132 222 93 95
% 17.9% 20.0% 33.6% 14.1% 14.4%
Good work ethic N 126 110 192 161 89
% 18.6% 16.3% 28.3% 23.7% 13.1%
Providing the best possible working environment
N 111 105 125 136 213
% 16.2% 15.2% 18.1% 19.7% 30.9%
Avoiding bad publicity
N 138 199 197 85 60
% 20.4% 29.3% 29.0% 12.5% 8.8%
Table 5.2: Rank ordering of values
1 Serving the greatest number of patients as possible
75% 12 13
2 Avoiding bad publicity 50 29 21
3 Not having strikes and social unrest 45 24 31
4 Balancing the books 38 34 28
5 Good work ethic 35 28 37
6 Providing the best possible working environment 32 18 50
Salient points
If one combines the first two and last two categories, the rank ordering
(from more to less important) above (see Table 5.2) is obtained.
Interestingly, more �administrative values� (number of patients served;
publicity; balancing the books/financial issues; good order) are valued
higher than a good work ethic and having a good working environment. If

38
this is a fair reflection of the organisational culture at CHBH, it does not
augur well for staff relations. In fact, this rank ordering is consistent with
results reported earlier.
5.3 Ratings of professional values
The final set of values included in this section refers to the clinical
situation. We wished to establish two things: first, whether staff believes
that doctors and nurses care for patients; and secondly, whether doctors
and nurses are given similar ratings for clinical care by other groups. The
results are summarised in Table 5.3 below.
Concerning the first question about clinical care (whether staff believes
that doctors and nurses care for patients), staff is clearly divided, with
50% (on average) saying that doctors and nurses show sufficient
commitment to various aspects of patient care (�care� means compassion
for patients, confidentiality of patient information, and respect for the
dignity and well-being of patients). However, the other 50% is split evenly
between 25% undecided and 25% being negative about/disagreeing with
the quality of patient care. Qualitative comments pertaining to patient
care are listed in Box 5.7 below.
Table 5.3: Ratings of professional values
Very great extent
Great extent
Moderate extent
To some extent
Very little
extent
Doctors: Compassion for patients
N 188 210 183 71 36
% 27.3% 30.5% 26.6% 10.4% 5.3%
Nurses: Compassion for patients
N 166 180 144 126 58
% 24.6% 26.8% 21.3% 18.8% 8.6%
Doctors: Confidentiality of patient information
N 257 171 126 52 69
% 38.0% 25.3% 18.7% 7.7% 10.3%

39
Nurses: Confidentiality of patient information
N 220 164 154 84 58
% 32.4% 24.0% 22.6% 12.4% 8.6%
Doctors: Respect for dignity of patients
N 180 163 167 84 74
% 27.0% 24.4% 25.1% 12.6% 11.0%
Nurses: Respect for dignity of patients
N 183 140 167 104 81
% 27.2% 20.7% 24.7% 15.5% 11.9%
Doctors: Respect for well-being of patients
N 216 195 146 70 39
% 32.4% 29.2% 21.9% 10.6% 5.9%
Nurses: Respect for well-being of patients
N 205 157 164 97 68
% 29.6% 22.7% 23.7% 14.1% 9.8%
Box 5.7 Patient care related issues Female radiographer at Radiology for four years: �Patients must not be scared to report unsatisfactory treatment. Staff members shouldn�t be scared to voice out if not satisfied. That is, management must be approachable, and responsive.� Female doctor at CHBH for one year: �Disregard / disrespect of certain patients - senior members of clinical staff surely influence how subordinates behave.� Female doctor at CHBH for 26 years: �Clinical performance should be more clearly maintained, and professional people should be answerable for poor patient management.� Male doctor at CHBH for 31 years: �Assaults on patient and staff to be reported and followed up. A small number of nurses and doctors behave unethically and need to be disciplined or dismissed.� Female nurse at General Surgical Section for two years: �Staff should have good conduct towards their co-workers, do their work professionally, know about patient rights, and know about patients� charter.� English speaking male doctor at CHBH for 31 years: �Adequate screens to ensure patients� privacy. Adequate bedpans and urinals. Glasses and water should be provided for bedridden patients, as nurses are often too busy to bring patients water and to supervise feeding.� Tswana speaking female nurse at Paediatrics for 18 years: �Resources need no compromises because of the high influx of patients coming to the hospital, especially patients with conditions related to HIV and AIDS.� Zulu speaking female nurse at the Maternity Ward for 17 years: �I think there can be control over patients flocking from all over South Africa and outside countries, e.g. from Malawi to Bara. Most of our budget finances are wasted by outside people whilst they leave their places where their health monies have been allocated to them.�

40
Box 5.7 (continued) Female nurse at the Surgical Section for six years: Non-South Africans to pay more admission fees. Patients with medical aids to use them.� Southern Sotho speaking female at the Maternity Ward for 14 years: �I would suggest that free health services should come to an end. Patients should be responsible and pay for their health so that the government should buy equipment, linen and medicines. If patients were paying, overcrowding of the hospital wouldn't be there.� Tswana speaking female nurse at the Nursing / Casualty Section for 25 years: �Influx of patients must be controlled. Non-South African patient must be treated in their hospitals by origin. AIDS patients� families must be taught home care. Remuneration for public holidays, weekends to make staff happy.� Southern Sotho speaking female nurse at Paediatrics for ten years: �Non-South African patients should pay for services, free services should be stopped, patients under six and pensioners should pay less unlike not paying at all.� Tswana speaking female nurse at Ophthalmology for 13 years: �Patients also contribute to this shortage as they also steal it [linen]. Education should be done to community at large to tell them that if they remove linen from the hospital they will be prosecuted.� Female Tsonga speaking support staff at Casualty Admission for 20 years: �All patients, including clinics and those who come for TOP [termination of pregnancy], must pay at least a minimum amount.�
In addition to these general comments on patient care (Box 5.7 above),
three more specific issues were frequently raised in the open-ended
questions. These relate to patient admissions (Box 5.8 below), patient
discharge (Box 5.9 below), and patient care directly influenced by the
HIV/AIDS pandemic (Box 5.10 below).
Box 5.8 Problems encountered with patient admission Male radiographer at Radiology for ten years: �Care should be given to emergency clinic patients as most of them lose their lives before seeing a doctor.� Male nurse at Medicine for 20 years: �Long queues. Long wait for admissions.� Male doctor at CHBH for five years: �Admission bottlenecks occur due to sub-standard organisation in casualty - casualty can be markedly improved.� Female nurse at Pediatrics for 18 years: �More admission wards should be created to reduce the work load. There will be fewer patients in a ward, proper treatment will be done, and patients will be discharged sooner.� Female nurse at Medical Section for 19 years: �Patients to be admitted when there is a need and beds for them to sleep on because that is where the problems start because they get lost and are unmanageable and impossible to care for.�

41
Box 5.9 Problems encountered with patient discharge Female radiographer at Radiology for 32 years: �On discharge, staff have to go and collect medicines for patients, like before, thus curbing the long queues at the chemist. Some patients actually collapse whilst in that queue.� Female occupational therapist at Occupational Therapy Department for 18 months: �Transport for patients who get discharged while they are not well enough, because several times one witnesses patients collapsing on the bridge after being discharged.� Female physiotherapist at Physiotherapy for one year: �Patients should not be discharged just because it is intake and they need more beds, without any regard to whether the patient is ready to go home - will the family cope at home?� Female doctor at CHBH for one year: �Patients must not be discharged from Ward 20 on next day unless adequate follow-up is arranged and especially to get speedy TB results one month later in the clinic!! Patients should remain in hospital until TB results back.� Female nurse at General Section for 21 years: �Patients must be discharged really when they are fit for discharge. I met two patients on the highway, collapsed. With the help of public I brought the patient back to the hospital and admitted.�
Box 5.10 Patient care and HIV/AIDS pandemic Female student radiographer at X-Rays for three years: �The patients are discharged without being better in their condition, more especially when the patient is HIV positive; they discharge them because there's this thing that he is going to die so there's no use to keep him in the hospital. Which is wrong.� Female doctor at CHBH for five years: �Home-based AIDS care and hospital are needed to relieve the burden of the hospital coming from terminal patients.� Male doctor at CHBH for two years: �Admission of HIV patients and their treatment needs review and protocol to save resources.� Female nurse at Medical, Surgical, Maternity, Paediatric, Ortho and St Johns Eye Hospital for 13 years: �Community must be taught how to take care of full-blown AIDS patients and very frail patients, to minimise admissions due to shortage of staff, and so that quality care can be rendered. Before discharge, relatives to be informed early and be taught how to take care of the patient at home.�
We conclude our discussion of the first question about patient care
(whether staff believes that doctors and nurses care for patients) with
some quotations on patients� rights. They illustrate quite clearly the
concern expressed about violation of these rights and the absolute need
for re-establishing a culture of respect for patients and their rights.
Significantly, the five most common patients� rights recognised in

42
declarations and the literature24 are the rights to respectful care,
information (regarding the caregiver�s name, diagnosis, treatment
options, and prognosis), informed consent, confidentiality of private
information, and refusal of treatment.
Female radiographer at Radiology for 26 years: �Staff members should respect every patient they handle and treat them like human beings, give them the proper service they are expected to give them. There should be some good communication between staff members and the patient they nurse.� Male radiographer at X-Ray for one year: �Be compassionate to patients. Respect them, e.g. explain to them everything until they understand. Patients who are not harassed won�t harass us.� Male radiographer at Radiology for ten years: �There should be mutual respect and understanding between staff and patients. Staff members should be polite and communicate with patients and should listen to what patients are saying.� Female radiographer at Radiology for 20 years: �Privacy, especially regarding information about patients� illnesses.� Female nurse at Orthopaedic for 13 years: �Staff to learn to respect different cultures and also to treat them with respect, and in turn patients need to be educated that we are not the �enemy� and that they are in good hands.�
The second question about the clinical care concerns differences between
the ratings of doctors and nurses, respectively, by others (whether
doctors and nurses are given similar ratings for clinical care by other
groups). The results clearly reveal a significant gap between the ways in
which doctors� and nurses� respective clinical care was rated by others,
with doctors being rated significantly higher overall. These ratings are
visually displayed in Figures 5.7 and 5.8 below.25
24 See, for example, the following: National Department of Health (November 1999). National Patients� Rights Charter. Pretoria. (see Appendix 8); Wilson Silver, M.H. (1997). Patients� rights in England and the United States of America: The Patients� Charter and the New Jersey Patient Bill of Rights: A Comparison. Journal of Medical Ethics 23:213-220; Neary, I. (1999). Patients� Rights. http://privatewww.essec.ac.uk/inj/HR/patients/pa_general.html 25 Figure 5.7, which contains the ratings of doctors, excludes doctors� own ratings; similarly, nurses ratings of themselves were excluded from Figure 5.8.

43
Figure 5.7: Ratings of doctors by others
Figure 5.8: Ratings of nurses by others
5.4 Recommendations by respondents
Respondents put forward various recommendations, but two major
categories emerged as priority areas: education and training of staff
(Box 5.11 below), and the need for team building (Box 5.12 below).
0
10
20
30
40
50
Compassion for patients 36 32 41
Confidentiality of patientinfo
47 26 27
Respect for dignity ofpatients
36 27 37
Respect for well-being ofpatients
39 29 32
Positive ratings
Neutral rating
Negative rating
0
10
20
30
40
50
60
70
Compassion for patients 60 23 17
Confidentiality of patientinfo
64 17 19
Respect for dignity ofpatients
54 23 23
Respect for well-being ofpatients
63 19 18
Positive ratings
Neutral ratingNegative
rating

44
Box 5.11 In-service and continuing education and training Female radiographer at Radiology for 21 years: �In-service training in departments must be on ongoing basis. Interdepartmental talks or visits by representatives from one to the other just to give a broad view of what takes place, in that particular department. At least every department will know what other departments are doing, in that way we will respect each other and also understand each other better.� Female doctor at CHBH for one year: �Intercultural courses promoting staff relations should be given in the form of in-service or continuing education.� Female person at Management for 36 years: �Workshops should be provided on communication skills and human relations in general.� Female nurse at Maternity Ward for seven years: �Staff to be in-serviced in communications, ethics. �De-stressing� programmes to be put in place for staff problems to be attended individually.� Female nurse at General Surgical Section for two years: �Supervisors to go for some sort of training on interpersonal skills and relationships whereby they will be taught communication skills and how to deal with their subordinates in a more friendly way without being too authoritarian. Channels of communication to be easy for all staff members and to do crisis management course.�
Box 5.12 Need for team building Female occupational therapist at Occupational Therapy Department for 18 months: �Team buildings of staff to be encouraged, which will improve communication of staff. Staff incentives will also boost staff morale. Proper training of supervising staff to be taken seriously as this seems to cause power-struggles.� Female therapist at Speech Therapy/Audiology for ten years: �At present, there is no staff for the programme. Money needs to be allocated and team development and team building, as well as stress management, need to be looked at.� Female therapist at Speech Therapy/Audiology for three and half years: �Team building exercises between departments are pivotal to the effective and smooth running of the hospital.� Female dietician at Human Nutrition for eleven years: �Staff working in the different departments work in isolation from one another. Having tea in the dining halls (or even smaller communal tea rooms) will improve communication. Welcoming/orientation of new staff and farewell of old staff need more attention. Start staff forums. This will keep supervisors in touch with activities on ground level (especially in bigger departments, like kitchens, cleaning department.)� Male doctor at CHBH for 31 years: �Nurses and doctors should work together. At present, we are working separately and nurses are often too busy with routine duties to obey doctors� instructions.�

45
5.5 Concluding comments
This section has been devoted to a discussion of the organisational culture
at CHBH, under three headings: staff relations, organisational values, and
professional values. Concerning perceptions of staff relations, we have
seen that two out of every five staff members are negative about various
aspects of them. These results are confirmed by qualitative comments
which show that staff morale is generally low.
Which organisational values are rated highly? Again, results showed that
most employees believe that more �administrative values�, such as the
number of patients served, avoiding bad publicity, and not having strikes,
are more important (to management?) than a good work ethic and the
best possible working environment.
Finally, with regard to professional values, staff is clearly divided: equal
percentages believe that doctors and nurses show compassion for
patients, treat patient information confidentially, and respect the dignity
and well being of patients. These results also revealed that ratings of
doctors on these aspects are consistently higher than the ratings given to
nurses.
The overall picture that emerged from these analyses is not a positive
one. It unequivocally shows that the organisational culture of the hospital
is not healthy, that staff is not positive about the institution, and that
morale is low.

46
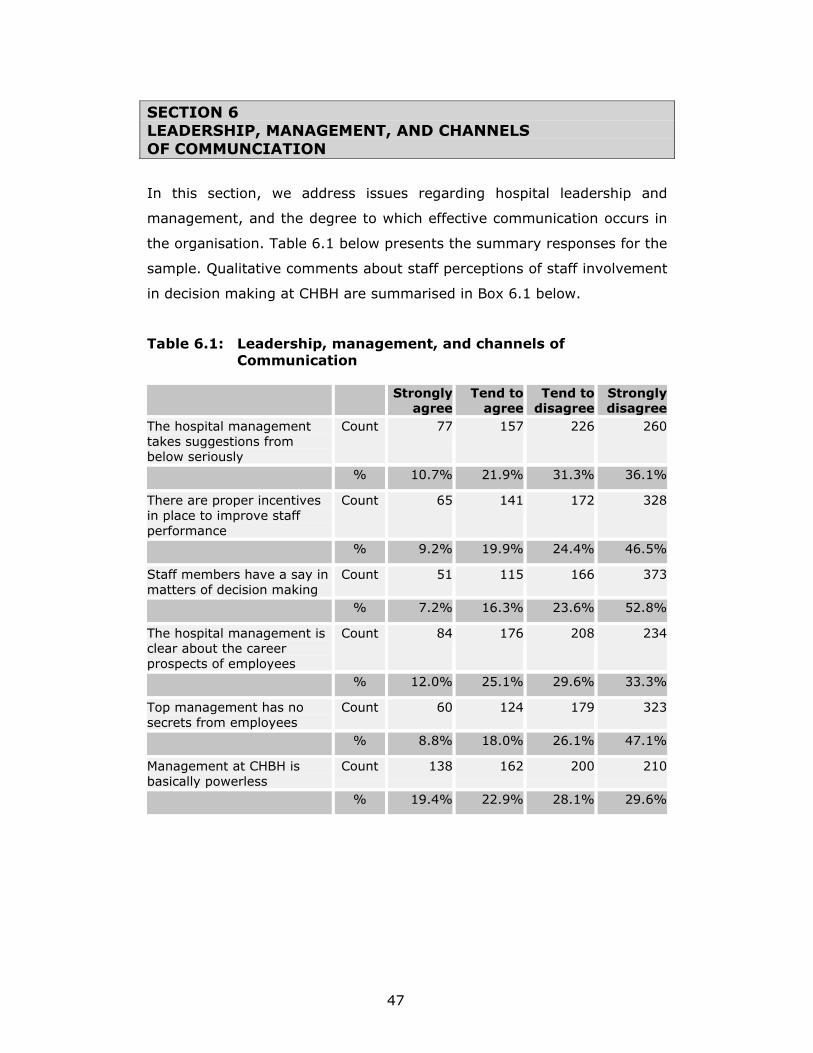
47
SECTION 6 LEADERSHIP, MANAGEMENT, AND CHANNELS OF COMMUNCIATION
In this section, we address issues regarding hospital leadership and
management, and the degree to which effective communication occurs in
the organisation. Table 6.1 below presents the summary responses for the
sample. Qualitative comments about staff perceptions of staff involvement
in decision making at CHBH are summarised in Box 6.1 below.
Table 6.1: Leadership, management, and channels of Communication
Strongly
agreeTend to
agreeTend to
disagree Strongly disagree
The hospital management takes suggestions from below seriously
Count 77 157 226 260
% 10.7% 21.9% 31.3% 36.1%
There are proper incentives in place to improve staff performance
Count 65 141 172 328
% 9.2% 19.9% 24.4% 46.5%
Staff members have a say in matters of decision making
Count 51 115 166 373
% 7.2% 16.3% 23.6% 52.8%
The hospital management is clear about the career prospects of employees
Count 84 176 208 234
% 12.0% 25.1% 29.6% 33.3%
Top management has no secrets from employees
Count 60 124 179 323
% 8.8% 18.0% 26.1% 47.1%
Management at CHBH is basically powerless
Count 138 162 200 210
% 19.4% 22.9% 28.1% 29.6%

48
Box 6.1 Involvement of staff in decision making Female nurse at General Ward for nine years: �Good staff relations can be improved by inviting staff in decision making concerning management of the ward/department, by promoting teaching sessions in the ward. Prevent favouritism, and praise an individual if she has done something good.� Female nurse at Nursing Division for 26 years: �Supervisors should involve staff in decision making for co-operation sake; also the issue of over-emphasising one's position, e.g. director etc., and looking at others as beggars instead of co-operates. The senior personnel should develop staff more than destroying.� Female nurse at Medical Ward for 12 years: �Involve grassroot people in decision making. Cultivate culture of respect for subordinates especially in general category by proper orientation of staff, hierarchy of institution clearly defined, work expectations and procedures, adequate staffing to relieve work load.� Male radiographer at Radiography for seven months: �Open dialogue among staff members and ensure feedbacks and positive response and implementation on resolutions made.� Female nurse at Medicine for 13 years: �Staff members, especially the so-called bosses or supervisors, to come down to our level, not to think of themselves as being high and mighty. Our complaints to be listened to. Let us be involved in decision making and not be told that this is in place without being informed. Let us respect one another, senior or junior.� Female nurse at Ophthalmology for 13 years: �Management does not involve people at grassroot in decision making. Most issues are forced on the working people therefore the negative attitude towards management. Management is also not visible to the people on the ground. They rule in offices. New rules are not in place for what staff has to do when dissatisfied with decisions management makes. Some unions seem to enjoy management support.�
6.1 Leadership and management
Salient points
• There is little evidence of a participatory management culture, with
three-quarters (76%) of staff indicating they had no say in decision
making. An even higher proportion of doctors - 84% - held this
view.
• There is clearly an insufficient degree of transparency in the
hospital. This is evidenced by rumour (the �grapevine�) being an
important source of information, too little communication between
management and staff, and too much secrecy.
• There is also not enough concern for and commitment to staff
development, there are inadequate incentives, and there is
insufficient performance.

49
Further analyses of the subgroups reveal that two of the most professional
groups (doctors and allied health professionals) are even more negative
about leadership and management issues than the rest of staff. In the
following figures, we grouped together doctors, nurses and allied health
professionals (under the heading of �clinical professional group�) and
compared their views on each of these questions with those of
management and support staff. These differences are summarised in
Figures 6.1 to 6.6 below.
Figure 6.1: Management takes suggestions from below seriously
Figure 6.2: There are proper incentives to improve staff performance
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
Management 37.50% 50% 12.50%
Clinical professional 7.60% 20.60% 32.70% 39.10%
Support staff 14.60% 25.20% 29.30% 30.90%
SA A D SD
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
Management 37.50% 37.50% 25.00%
Clinical professional 8.40% 18.70% 24.60% 48.30%
Support staff 9.60% 20.00% 26.10% 44.30%
SA A D SD

50
Figure 6.3: Staff members have a say in decision making
Figure 6.4: Hospital management is clear about employees� career prospects
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Management 12.50% 62.50% 25.00%
Clinical professional 6.80% 14.90% 29.00% 49.30%
Support staff 7.80% 19.00% 15.50% 57.80%
SA A D SD
0
0.1
0.2
0.3
0.4
Management 37.50% 25.00% 37.50%
Clinical professional 9.00% 26.70% 31.60% 32.70%
Support staff 15.50% 22.40% 26.70% 35.30%
SA A D SD

51
Figure 6.5: Top management has no secrets from employees
Figure 6.6: Management at CHBH is basically powerless
In addition to the quantitative ratings presented in the figures below, we
have selected a number of qualitative comments that reflect staff
perceptions about management, leadership style, and practices at the
hospital. They are presented in Box 6.2 below.
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Management 37.50% 12.50% 37.50% 12.50%
Clinical professional 5.20% 18.60% 32.30% 44.00%
Support staff 14.80% 17.40% 16.50% 51.30%
SA A D SD
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Management 25.00% 37.50% 12.50% 25.00%
Clinical professional 17.00% 24.30% 31.60% 27.10%
Support staff 22.70% 21.00% 22.70% 33.60%
SA A D SD

52
Box 6.2 Management and leadership English speaking female doctor at CHBH for four years: �Better overall management at different levels. Management to take responsibility and also to be evaluated. Insight into problem, reasonable solution, application of solution and follow�up. There is lack of insight at almost all levels by higher management: rest of the �steps� cannot be carried out satisfactorily. Zulu speaking male at Management for seven years: �Management needs enough authority to make decisions.� English speaking female at Management for 36 years: �Appoint appropriately qualified personnel to supervise.� Xhosa speaking nurse at the Medical Section for 20 years: �Management should be changed within one year or six months; they must be educated and have better skills.� Tswana speaking female nurse at the General Section for 13 years: �Management must work hand-in-hand with staff and listen to our concerns.� Zulu speaking female nurse at the Medical Section for 15 years: �Management should reach people on the ground to hear their views.� Tswana speaking female nurse at CSSD [Central Sterilising Service Department] General for 24 years: �Management in this hospital doesn't care about nurses.� English speaking nurse at Orthopaedic for 21 years: �Management to be truly changed rather than old-fashioned people. It must provide enough medicines, like the old government.� Female Tswana speaking support staff at Administration for 20 years: �Management should stop using money for buying expensive furniture for their offices; use that money to buy patients� medicine, linen and other equipment which are needed in other wards.� Male Northern Sotho speaking support staff at Security Department for 21 years: �The management of hospital must check departments if they are clean, like before 1992.�
6.2 Channels of communication
Open channels of communication, regular feedback from one�s superiors,
access to official forms of communication, and the freedom to express
oneself without fear of reprisal, are all indicators of a culture of open and
free communication in an organisation. How does staff at CHBH feel about
these and other matters of communication? Responses are summarised in
Table 6.2 below.

53
Table 6.2: Perceptions of channels of communication
Strongly
agree
Tend to
agree
Tend to
disagree
Strongly
disagree
Employees are not allowed to say what they really think
Count 234 169 195 131
% 32.1% 23.2% 26.7% 18.0%
Clear guidelines exist regarding staff members' responsibilities
Count 188 256 182 72
% 26.9% 36.7% 26.1% 10.3%
My supervisor effectively follows up on complaints that I direct via him/her
Count 186 214 153 163
% 26.0% 29.9% 21.4% 22.8%
My supervisor regularly gives me feedback about my performance
Count 117 132 178 275
% 16.7% 18.8% 25.4% 39.1%
I am always last to be informed about decisions that concern my work
Count 162 142 192 207
% 23.0% 20.2% 27.3% 29.5%
There is a system in place that employees can use to report instances of misconduct without being victimized
Count 139 185 158 221
% 19.8% 26.3% 22.5% 31.4%
Rumour (the �grapevine�) is a common source of information at CHBH
Count 258 185 130 137
% 36.3% 26.0% 18.4% 19.3%
One of the issues that appeared very prominently in the qualitative
comments concerns communication. We list some of these in Box 6.3
below.

54
Box 6.3 Communication Female radiographer at Radiology for 26 years: �Good communication between staff- members can make the workplace a stress-free area, and patients will receive a better service. Also, there should be enough staff employed for work to be easy as well as good remunerations to prop them up.� Female radiographer at Radiology for 17 years: �Talk openly about things that affect relations directly.� Male doctor at CHBH for three years: �Better communications between doctors and nurses, and between departments.� Male doctor at CHBH for 25 years: �Improved communication is essential. We need to engineer a caring ethos and provide quality work. Teamwork needs to be stressed. Sufficient nurses need to be employed to restore morale.� Male doctor at CHBH for 23 years: �Better communication between top management and staff, and especially Gauteng Health. Staff need to develop a pride and care for CHBH!!� Male doctor at CHBH for 27 years: �There is no common language (working) at the hospital. English should be made a common working language for the hospital.� Female doctor at CHBH for two years: �Language courses to be encouraged. More communication with people above us.� Female nurse at Maternity Ward for three months: �English must be the medium/language of communication.�
Salient points
• A substantial proportion of staff (45%) did not believe that
employees were allowed to say what they really thought.
• Communication between employees and their supervisors was less
than optimal - 50% of staff said their complaints had not been
acted upon, and nearly two-thirds (65%) said that they had not
received regular feedback from their supervisors.
• A clear majority (54%) of staff also did not believe that there was a
system in place for reporting instances of misconduct.
• The fact that 62% of staff said that rumour was a common source
of information in the hospital was another indicator that existing
channels of and procedures for communication are regarded as
inadequate.

55
6.3 Concluding comments
One�s overwhelming impression, having analysed the data on
management and communication, is of an organisation that does not
treasure participation and consultation in decision making, where the
views of ordinary staff members do not matter, and where opportunities
for constructive communication are limited, if not non-existent.
56

57
SECTION 7 HUMAN RESOURCES ISSUES
This section addresses matters related to perceived job satisfaction,
perceptions of the hospital as a workplace, conditions of service, prospects
for promotion, and other related human-resource matters. Table 7.1
below presents the overall findings on a number of scaled items relating
mostly to job satisfaction.
7.1 Job satisfaction
Table 7.1: Perceptions of job satisfaction
Strongly agree
Tend to agree
Tend to disagree
Strongly disagree
I am often bored with my job Count 108 103 151 320 % 15.8% 15.2% 22.2% 46.9%I am satisfied with my job for the time being
Count 211 203 114 142
% 31.5% 30.3% 17.0% 21.2%Each day of work seems like it will never end
Count 167 135 156 214
% 24.9% 20.1% 23.2% 31.8%I find real enjoyment in my work Count 243 168 141 123 % 36.0% 24.8% 20.9% 18.2%It feels as if I am working in a �second-class� hospital
Count 202 181 136 149
% 30.2% 27.0% 20.4% 22.3%I feel proud to be associated with CHBH
Count 286 177 99 114
% 42.3% 26.1% 14.7% 16.9%My opinion of myself increases when I do my job well
Count 405 180 56 43
% 59.3% 26.3% 8.1% 6.3%I frequently think of quitting my job
Count 151 116 138 273
% 22.2% 17.1% 20.4% 40.2%
Table 7.2 below summarises the ratings on various aspects of conditions
of service in the hospital, whereas Box 7.1 below lists some of the
numerous comments and suggestions regarding the use of incentives in
performance management.
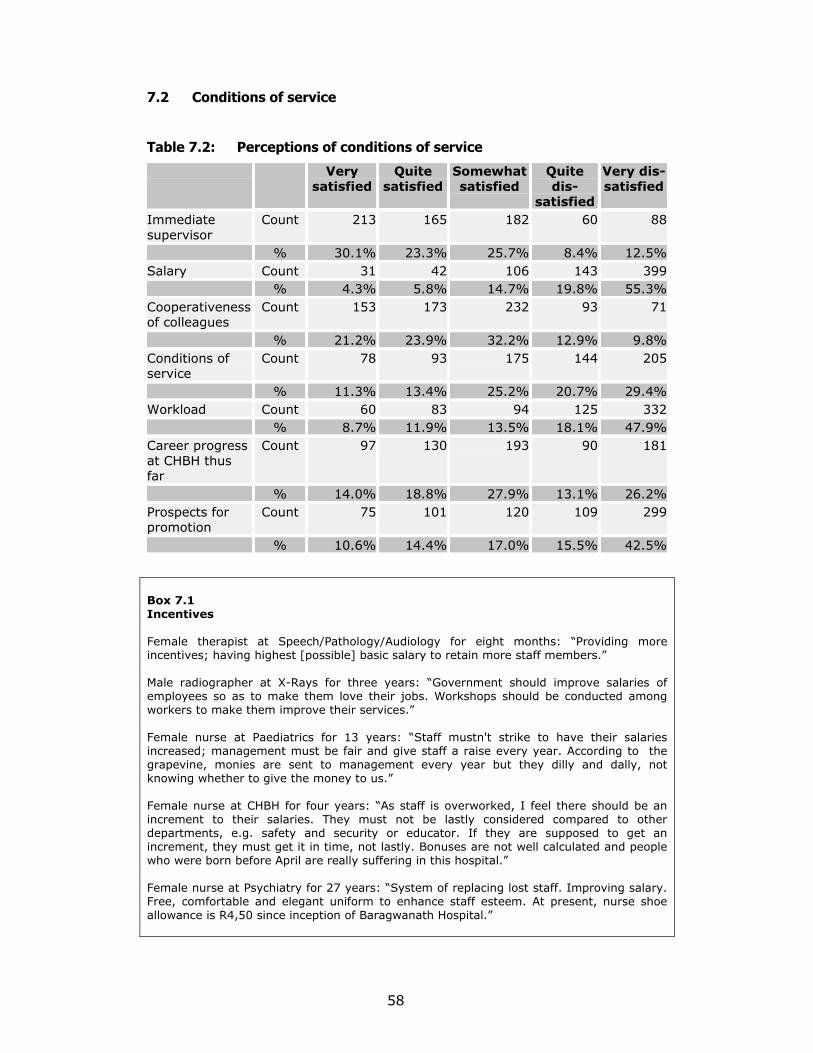
58
7.2 Conditions of service
Table 7.2: Perceptions of conditions of service
Very satisfied
Quite satisfied
Somewhat satisfied
Quite dis-
satisfied
Very dis-satisfied
Immediate supervisor
Count 213 165 182 60 88
% 30.1% 23.3% 25.7% 8.4% 12.5%Salary Count 31 42 106 143 399 % 4.3% 5.8% 14.7% 19.8% 55.3%Cooperativeness of colleagues
Count 153 173 232 93 71
% 21.2% 23.9% 32.2% 12.9% 9.8%Conditions of service
Count 78 93 175 144 205
% 11.3% 13.4% 25.2% 20.7% 29.4%Workload Count 60 83 94 125 332 % 8.7% 11.9% 13.5% 18.1% 47.9%Career progress at CHBH thus far
Count 97 130 193 90 181
% 14.0% 18.8% 27.9% 13.1% 26.2%Prospects for promotion
Count 75 101 120 109 299
% 10.6% 14.4% 17.0% 15.5% 42.5%
Box 7.1 Incentives Female therapist at Speech/Pathology/Audiology for eight months: �Providing more incentives; having highest [possible] basic salary to retain more staff members.� Male radiographer at X-Rays for three years: �Government should improve salaries of employees so as to make them love their jobs. Workshops should be conducted among workers to make them improve their services.� Female nurse at Paediatrics for 13 years: �Staff mustn't strike to have their salaries increased; management must be fair and give staff a raise every year. According to the grapevine, monies are sent to management every year but they dilly and dally, not knowing whether to give the money to us.� Female nurse at CHBH for four years: �As staff is overworked, I feel there should be an increment to their salaries. They must not be lastly considered compared to other departments, e.g. safety and security or educator. If they are supposed to get an increment, they must get it in time, not lastly. Bonuses are not well calculated and people who were born before April are really suffering in this hospital.� Female nurse at Psychiatry for 27 years: �System of replacing lost staff. Improving salary. Free, comfortable and elegant uniform to enhance staff esteem. At present, nurse shoe allowance is R4,50 since inception of Baragwanath Hospital.�

59
Box 7.1 (continued) Female support staff at Casualty Admission for 20 years: �Incentives must be implemented in order to boost the morale of staff. Employees should be promoted or demoted and be merited (a happy worker produces more).�
7.3 Staff shortages
There is no question that the biggest human-resource issue consistently
referred to in the survey � both in the close-ended and open-ended
questions - is the shortage of staff. We selected (from a very long list of
comments) some of the remarks made in this regard for inclusion in Box
7.2 below.
Box 7.2 Staff shortages Female student radiographer at X-Ray Department for three years: �Government must get more employees because really there is a shortage of staff. Patients think that we are not working, but the problem is that we are short staffed.� Female doctor at CHBH for eight and half years: �Most problems related to being short staffed, but there is hope for Bara. Sisters seem not to care for patients and night staff usually sleep at night. Numerous times doing ward calls. Also having to take attitude from radiographers who do not X-ray as ordered having to report to radiographers. If staff not corrected in time.� Female doctor at CHBH for three years: �The shortage of nurses leads to poor relations between nurses and doctors. Wards are ridiculously short staffed and many nurses seem to have stopped caring due to poor working conditions and low salary.� Female dietician at Human Nutrition for five years: �This could be improved by relieving pressure from staff, by employing more staff. Thus enabling staff to spend time with patients.� Female physiotherapist at Physiotherapy for nine years: �Number of staff - doctors, nurses, paramedics - must be increased; enforce discipline when patients� rights are violated, and enforce an atmosphere of �compassion� and high standards! - perhaps incentives?� Male nurse at Cardiology for three and half years: �If more nursing and auxiliary staff is employed, relations would improve.�

60
Box 7.2 (continued) Male doctor at CHBH for four years: �Increased number of staff will increase level of care at the hospital.� Female person at management for 36 years: �Increase the number of medical and nursing staff to allow better communication.� Female nurse at General Ward for 16 years: �More staff will reduce some of the problems, e.g. long stays in hospital. To have enough and modernised equipment, enough medicines. Encourage staff to attend in-service.� Female nurse at Maternity Ward for 14 years: �Due to staff shortage there is no time for staff to have good relations with our patients. At least one nurse for two or three patients will give a chance to know patients.� Female nurse at Maternity Ward for six years: �If staff is enough there will be time to attend to patients and nurse them in totality, thus improving nurse-patient relationship.� Female nurse at Surgical Section for 32 years: �Address the problem of human-resources shortage. How can one nurse look after 40 patients and be expected to be OK (well) at the end of the shift? Revise nursing activities - facing one individual, then pushing the person to the edge?� Female nurse at the Theatre for 20 years: �More nurses should be employed to improve the nursing standard. To relieve overstretching from nurses. We work without meals because of pressure of work. Staff is prone to illness. We get added responsibility by transfers (patients) from other hospitals.� Female nurse at Maternity Ward for 14 years: �For good relations to improve, the government should employ more staff for coverage of workload. The work overload doesn't help people to relate well because they are always under stress. Everyone thinks she works more than the other one.�
7.4 Concluding comments
A number of positive findings emerge from this section of the survey.
• Respondents are generally satisfied with their jobs, and they find
their jobs interesting and even stimulating.
• Two-thirds of staff (66%) was proud to be associated with CHBH.
But there are also some less positive results:
• A very large proportion of staff (40%) frequently thought of quitting
their jobs
• A clear majority (58%) felt as if they were working for a �second-
class� hospital
• There was general dissatisfaction with salaries (75%) and
workloads (66%)
• Large proportions (over 50%) were dissatisfied with conditions of
service and prospects for promotion

61
We believe that these results lead to two major conclusions:
• There is a kind of �split image� at work here. On the one hand,
there is the positive legacy or ideal of CHBH, but, on the other, its
quality is declining � or, rather, that is the perception.
• Although staff is positive about their own jobs and job contents,
they are very negative about staff development (no prospects for
promotion; high workload).

62

63
SECTION 8 MISCONDUCT AND STANDARDS OF CARE Two of the main objectives of our ethics audit were to establish the
existence and degree of instances of ethical misconduct, and the reasons
offered for such misconduct.
8.1 Rank ordering of instances of misconduct
In respect of the first objective (occurrence and weighting of instances of
ethical misconduct), staff was asked to indicate how often they had
witnessed various forms of misconduct. Table 8.1 below lists responses in
descending order � from instances that recorded the highest response
rate to the lowest.
Table 8.1: Rank ordering of instances of misconduct
Once or more
Never No opinion
Total
Patients verbally abusing staff Count 457 98 112 667 % 68.6% 14.7% 16.7% 100.0%Professional negligence in patient care
Count 342 201 156 699
% 48.9% 28.7% 22.4% 100.0%Lack of compassion for patients Count 313 167 165 646 % 48.5% 25.9% 25.6% 100.0%Staff verbally abusing patients Count 333 203 162 699 % 47.7% 29.1% 23.2% 100.0%Patients physically abusing staff Count 318 226 140 684 % 46.6% 33.0% 20.5% 100.0%Special groups of patients getting different levels of care (TOP, AIDS, Aliens, Pregnant women, TB)
Count 284 140 265 688
% 41.2% 20.3% 38.5% 100.0%Lack of informed consent Count 257 183 244 684 % 37.5% 26.8% 35.7% 100.0%Moonlighting by staff Count 259 205 234 697 % 37.1% 29.4% 33.5% 100.0%Breach of confidentiality of patient information
Count 224 229 210 663
% 33.7% 34.6% 31.7% 100.0%Substandard post-operative care Count 217 189 271 677 % 32.1% 27.9% 40.1% 100.0%Staff physically abusing patients Count 198 315 167 680 % 29.1% 46.4% 24.5% 100.0%Over-ordering of medicine Count 182 147 363 691 % 26.3% 21.2% 52.5% 100.0%Patients/visitors bribing staff Count 127 328 240 695 % 18.2% 47.2% 34.6% 100.0%

64
The rank ordering of instances (from highest to lowest) where staff
observed different kinds of misconduct at least once is as follows:
• Patients verbally abusing staff (68.6%)
• Professional negligence in patient care (48.9%)
• Lack of compassion for patients (48.5%)
• Staff verbally abusing patients (47.7%)
• Patients physically abusing staff (46.6%)
• Special groups of patients getting different levels of care (41.2%)
• Lack of informed consent (37.5%)
• Moonlighting by staff (37.1%)
• Breach of confidentiality of patient information (33.7%)
• Substandard post-operative care (32.1%)
• Staff physically abusing patients (29.1%)
• Over-ordering of medicine (26.3%)
• Patients/visitors bribing staff (18.2%)
Box 8.1 below lists some of the qualitative comments made with regard to
misconduct.
Box 8.1 General observations about staff misconduct Female doctor at CHBH for one year: �Doctors are often very superficial, discharge patients prematurely without adequate explanation or follow-up. Interns check blood results the following day so don't act on acute emergencies. Very little effort is made to explain proceedings; doctors shout at patients, throw specimen bottles at them, patients are not seen for days on end and found a week later either dead or much sicker. A patient in Ward 15 was not seen by any other officer except the consulted service for 20 days!! Social workers are useless for ward patients. They almost never see them in the ward and uncommonly actually help. Nurses drag patients along the passage by the pajama collar (Ward 16). Nurses tell patients to go home and die; nurses drink tea and chat instead of attending to their duties.� Female doctor at CHBH for eight years: �Peer pressure - work by example to junior staff. Consultants shouldn't be leaving by 10am - what example to junior staff? Those doing limited private practice - should be limited! Treatment modalities neglected at Bara - the same teams would have treated patient immediately if they were in private practice � ICU [Intensive Care Unit]/orthopaedics. One should treat as one would like and expect to be treated. Two different sets of medical ethics, or is it all money?� Male doctor at CHBH for five years: �Clinical misconduct only surfaces when a medical-legal problem arises. There is no routine review of clinical performance - or very little.�

65
Box 8.1 (continued) Female nurse at Pediatrics for 15 years: �General workers, especially cleaners, are not properly supervised because they work whenever they like to, they go off as early as 10:00 in the morning.� Female nurse at the Theatre for 20 years: �General assistants are not cooperative in the workplace. Most of the time they are not there. They also add stress in the set-up.� Female nurse at Comprehensive Sections for four years: �General workers must stop abusing patients, as it implicates on the nursing staff as if they are the ones who are treating ill patients. They must allow to be disciplined, not ignore junior sisters as they are now.� Female nurse at Ortho-gynaecology for eleven years: �There are still those people who are untouchable because they are so-and-so - and if so-and-so cannot be touched, even having misconduct herself, so I am also going to develop a strategy of don't touch.� Female nurse at Maternity Ward for ten years: �People found drunk on duty must be suspended because they can be dangerous to patients.� Female nurse at Paediatrics for four months: �Stealing of medication can be controlled by counting them always when giving medication; and talk to the staff in the ward. Ask them how they feel about shortage of medication and do they know that they can go to jail for stealing.� Female nurse at Medical Ward for 18 years: �Staff to behave in an appropriate way, come on duty on time. Patients to be given medication, meals at the correct times.� Female nurse for 28 years: �Unsober behaviour, sleeping on duty - instant dismissal.�
Salient points
The following are some of the more salient points to emerge from this
analysis:
• The widespread (physical and verbal) abuse of staff by patients,
together with the fact that nearly 50% of staff also witnessed
incidents of abuse of patients, is clear evidence that there is a
serious lack of a culture of respect and care between staff and
patients.
• This result is confirmed by the fact that nearly half of staff said that
they had observed incidents of negligence in patient care, and
nearly one-third indicated having witnessed substandard post-
operative care.
• There is strong evidence that patients� rights are being violated -
nearly two out of every five staff members indicated that they had
witnessed incidents where informed consent had not been obtained,
and one-third said they had observed incidents where

66
confidentiality of patient information had been breached. These
results are supported by evidence provided by patients themselves
(see Section 10 below).
• Although other forms of misconduct, such as bribery and over-
ordering of medicine, do not seem to occur as frequently as the
ones listed above, it should be emphasised that these are
nevertheless transgressions of basic ethical principles and require
urgent attention.
• Given reported staff shortage, the fact that such a huge proportion
of staff (37%) seems to be involved in some form of moonlighting,
clearly warrants further investigation.
In an attempt to get a clearer picture of the experiences of clinical staff at
CHBH (doctors, nurses, and allied health professionals), we analysed
separately this combined (clinical) group�s responses to the questions on
observed misconduct. Although the ranking does not change radically, it is
interesting to note that some of the percentages have changed
considerably. Table 8.2 below contains the rank ordering of the top seven
categories of misconduct observed by clinical staff.
Table 8.2: Clinical staff�s observations of instances of misconduct
Once or more
Never No opinion
Patients verbally abusing staff Count 328 52 40 % 78.1% 12.4% 9.5%Staff verbally abusing patients Count 229 120 84 % 52.9% 27.8% 19.3%Lack of compassion for patients Count 200 112 87 % 50.1% 28.1% 21.9%Patients physically abusing staff Count 208 159 59 % 48.8% 37.3% 13.9%Professional negligence in patient care Count 206 141 85 % 47.7% 32.6% 19.7%Moonlighting by staff Count 199 136 95 % 46.3% 31.6% 22.2%Lack of informed consent Count 178 151 95 % 42.0% 35.6% 22.4%

67
These results reveal even better to what extent the relationship between
staff and patients is characterised by abuse and negligence, rather than
respect and care. This is perhaps the most serious finding of the study
since it concerns the basic rationale of an institution devoted to the care
and healing of human beings. The fact that such a large proportion of staff
reports instances of abuse of patients, and by patients, is an indication of
seriously deteriorated relationships. Unless a culture of mutual respect is
(re)instated, it is impossible for staff at CHBH to do their job in a
professional and responsible manner.
8.2 Reasons for misconduct
What are the reasons for this state of affairs? We asked respondents to
indicate the extent of their agreement or disagreement with a list of
possible reasons. Table 8.3 below summarises the results.
Table 8.3: Reasons for misconduct
Agree Disagree No opinion
Total
Misconduct at CHBH relates mainly to lack of discipline
Count 435 215 72 722
% 60.2% 29.8% 10.0% 100.0%
Disciplinary measures at CHBH are not �visible�
Count 403 212 65 680
% 59.3% 31.1% 9.6% 100.0%
Health professionals at CHBH do not have sufficient time to treat patients with the necessary compassion and understanding
Count 421 200 90 711
% 59.2% 28.1% 12.7% 100.0%
Employees who engage in threatening or violent behaviour on the job are seldom subjected to immediate disciplinary action
Count 362 225 126 713
% 50.8% 31.5% 17.7% 100.0%
Language barriers make it difficult for health care professionals to convey to patients proper information about their diagnosis and treatment
Count 300 328 84 711
% 42.1% 46.0% 11.8% 100.0%

68
Payment to employees at CHBH by patients or their family for services or treatment given is fraud
Count 270 276 184 730
% 37.0% 37.8% 25.2% 100.0%
Because of the heavy workload at CHBH it is fair for employees to ask for small incentives ("tips") for services
Count 163 452 100 715
% 22.8% 63.2% 14.0% 100.0%
Four main findings
Responses suggest four clusters of possible reasons for observed
instances of misconduct.
• The reasons having the most support among staff concern the lack
of punitive measures - no real or visible disciplining of misconduct
occurs (60% of staff)
• Working conditions - the heavy workload that leads to inadequate
attention to clinical care (60% indicate it as a main reason)
• No consensus about ethical values - there is clearly insufficient
agreement about the meaning of misconduct as evidenced by the
fact that substantial proportions of respondents do not believe
�tipping� and �fraud� to be wrong.
• The demographics of patients, especially the existence of language
barriers, lead to misunderstanding and possibly abuse (about 50%-
50%)
8.3 Misconduct and the need for an ethics committee
In response to the question whether a hospital ethics committee would
assist in guiding professional conduct, more than two-thirds of staff (69%)
answered positively. Box 8.2 below lists some of the remarks and
suggestions about such a committee.

69
Box 8.2 Ethics and disciplinary committees Female nurse at Medical Section for 12 years: �Proper code of conduct [should] be in place and copies given to staff members. Disciplinary code clearly defined. Grievance procedure clearly defined to all staff members.� Female doctor at CHBH: �Managing committee to deal with misconduct without alienating the complainant.� Female doctor at CHBH for four years: �Disciplinary committee - comprising management staff, doctors, and nurses.� Female nurse at Surgical Section for 20 years: �There should be a disciplinary committee available for every employee category.�
8.4 Concluding comments
This section vividly illustrates the severity of problems at CHBH. The
extent of misconduct � as reported by staff � is serious and points to a
situation not conducive to professional and responsible patient care. It is
imperative that hospital management addresses these issues as a matter
of priority. And, as suggested by the quotations below, a starting point
should be issues related to the current lack of discipline in the hospital.
Female speech therapist at Audiology for ten years: �Systems
need to be in place and offenders immediately punished - CEO
needs to have delegated authority.�
Male doctor at CHBH for one year: �Need policing body to police
the general running of the clinical disciplines, i.e. not bureaucratic,
[but] a medical body to review the running of the disciplines.�
Male doctor at CHBH for 27 years: �The following mechanisms
must be put in place urgently: senior supervision - daily ward
rounds by consultants; regular mortality and morbidity meetings;
regular meetings for nursing staff; and limitation of excess work.�

70
Female nurse at General Surgical Section for 13 years: �Clear
guidelines and lines of communication to be spelled out so that if
personnel have a problem they should know where to go.�
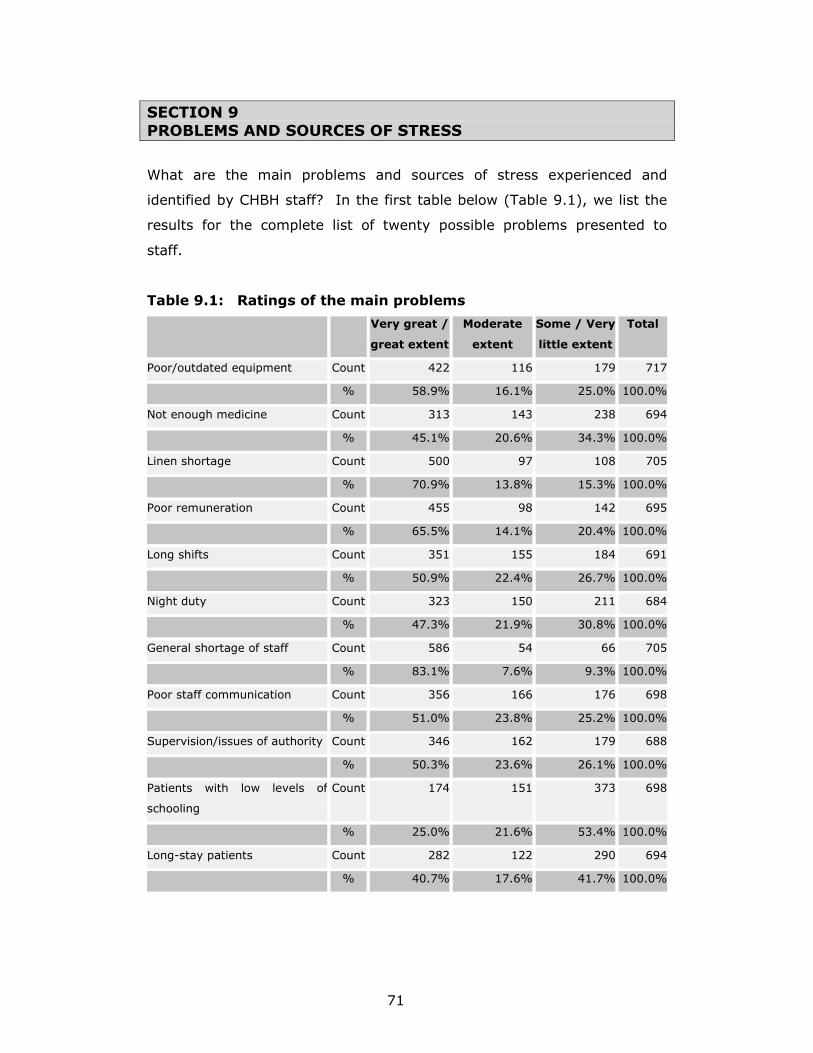
71
SECTION 9 PROBLEMS AND SOURCES OF STRESS
What are the main problems and sources of stress experienced and
identified by CHBH staff? In the first table below (Table 9.1), we list the
results for the complete list of twenty possible problems presented to
staff.
Table 9.1: Ratings of the main problems
Very great /
great extent
Moderate
extent
Some / Very
little extent
Total
Poor/outdated equipment Count 422 116 179 717
% 58.9% 16.1% 25.0% 100.0%
Not enough medicine Count 313 143 238 694
% 45.1% 20.6% 34.3% 100.0%
Linen shortage Count 500 97 108 705
% 70.9% 13.8% 15.3% 100.0%
Poor remuneration Count 455 98 142 695
% 65.5% 14.1% 20.4% 100.0%
Long shifts Count 351 155 184 691
% 50.9% 22.4% 26.7% 100.0%
Night duty Count 323 150 211 684
% 47.3% 21.9% 30.8% 100.0%
General shortage of staff Count 586 54 66 705
% 83.1% 7.6% 9.3% 100.0%
Poor staff communication Count 356 166 176 698
% 51.0% 23.8% 25.2% 100.0%
Supervision/issues of authority Count 346 162 179 688
% 50.3% 23.6% 26.1% 100.0%
Patients with low levels of
schooling
Count 174 151 373 698
% 25.0% 21.6% 53.4% 100.0%
Long-stay patients Count 282 122 290 694
% 40.7% 17.6% 41.7% 100.0%

72
Impossible/demanding patients Count 302 152 238 692
% 43.7% 22.0% 34.4% 100.0%
Substandard care because of
large numbers
Count 463 91 137 690
% 67.0% 13.1% 19.8% 100.0%
Language difficulties in dealing
with patients
Count 203 171 321 695
% 29.2% 24.6% 46.1% 100.0%
AIDS patients Count 315 117 258 690
% 45.7% 17.0% 37.3% 100.0%
Influx of non-South African
patients
Count 248 107 222 577
% 43.0% 18.6% 38.5% 100.0%
Unsanitary/unhygienic
conditions
Count 454 93 167 713
% 63.6% 13.0% 23.4% 100.0%
Poor maintenance of buildings Count 427 107 169 703
% 60.8% 15.2% 24.0% 100.0%
Lack of safety Count 456 113 149 718
% 63.4% 15.8% 20.8% 100.0%
Vandalism Count 342 124 226 692
% 49.4% 18.0% 32.6% 100.0%
In the remainder of this section, these results are organised in three
forms:
• The six most serious problems for the organisation as a whole
• The five most serious problems for each category of staff
• The two most serious problems within each of four categories of
problems

73
9.1 Most serious problems for the organisation as a whole
For all staff at CHBH, these are the six most serious problems in order of
importance:
• Shortage of staff (83.1%)
• Linen shortage (70.9%)
• Substandard care because of large numbers (67%)
• Poor remuneration (65.5%)
• Unhygienic conditions (63.6) and lack of safety (63.4%)
• Poor maintenance of buildings (60.8%)
9.2 Most serious problems for each category of staff
The five most serious problems identified by each of the different
categories of staff are summarised in Tables 9.2 to 9.5 below:
Table 9.2: Most serious problems identified by doctors
Count Col % General shortage of staff Very great / great extent 80 94.2% Moderate extent 4 4.1% Some / Very little extent 1 1.7%Unsanitary/unhygienic conditions Very great / great extent 69 79.7% Moderate extent 15 17.1% Some / Very little extent 3 3.3%Poor/outdated equipment Very great / great extent 64 74.6% Moderate extent 15 17.2% Some / Very little extent 7 8.2%Poor remuneration Very great / great extent 62 74.2% Moderate extent 17 20.0% Some / Very little extent 5 5.8%Long shifts Very great / great extent 61 73.1% Moderate extent 18 21.8% Some / Very little extent 4 5.0%

74
Table 9.3: Most serious problems identified by nurses
Count Col %General shortage of staff Very great / great extent 282 86.5% Moderate extent 11 3.4% Some / Very little extent 33 10.0%Linen shortage Very great / great extent 261 80.1% Moderate extent 21 6.4% Some / Very little extent 44 13.5%Substandard care because of large numbers
Very great / great extent 229 71.9%
Moderate extent 37 11.6% Some / Very little extent 53 16.6%Poor remuneration Very great / great extent 200 64.4% Moderate extent 58 18.6% Some / Very little extent 53 17.0%Lack of safety Very great / great extent 222 68.6% Moderate extent 48 14.9% Some / Very little extent 54 16.6% Table 9.4: Most serious problems identified by allied health
professionals Count Col %General shortage of staff Very great / great extent 30 89.2% Moderate extent 2 6.0% Some / Very little extent 2 4.8%Poor maintenance of buildings Very great / great extent 24 69.4% Moderate extent 8 22.4% Some / Very little extent 3 8.2%Poor remuneration Very great / great extent 27 81.7% Moderate extent 3 8.5% Some / Very little extent 3 9.8%Lack of safety Very great / great extent 26 75.3% Moderate extent 5 14.1% Some / Very little extent 4 10.6%Poor staff communication Very great / great extent 22 66.3% Moderate extent 7 21.7% Some / Very little extent 4 12.0%

75
Table 9.5: Most serious problems identified by support staff
Count Col % General shortage of staff Very great / great extent 193 74.3% Moderate extent 37 14.2% Some / Very little extent 30 11.5% Linen shortage Very great / great extent 170 64.3% Moderate extent 48 18.3% Some / Very little extent 46 17.4% Poor staff communication Very great / great extent 133 50.9% Moderate extent 55 21.1% Some / Very little extent 74 28.1% Substandard care because of large numbers
Very great / great extent 147 57.7%
Moderate extent 35 13.5% Some / Very little extent 74 28.8% Poor remuneration Very great / great extent 166 62.1% Moderate extent 21 7.8% Some / Very little extent 80 30.2%
9.3 Most serious problems within each of four categories of
problems
If one divides problems into different categories � namely, those related
to resources, staff, patients, and the environment � the following were
identified as the two most important problems in each of these four
categories of problems.
Resource related problems
• Linen shortage (70.9%)
• Poor/outdated equipment (58.9%)
Staff related problems
• General shortage of staff (83.1%)
• Poor remuneration (65.5%)
Patient related problems
• Substandard care because of large numbers (67.0%)
• HIV/AIDS patients (45.7%)
Environment related problems
• Unsanitary/unhygienic conditions (63.6%)
• Lack of safety (63.4%)

76
9.4 Concluding comments
It is significant that the same basic problems (staff shortages, linen
shortages, substandard care, poor remuneration, lack of safety, and
unhygienic conditions) are recurring problems and sources of stress across
all staff categories. This suggests that these problems are hospital-wide
problems and prevalent across departments and staff functions and
should, therefore, receive urgent attention.

77
SECTION 10 PATIENT PERSPECTIVES
�� I will come for the benefit of the sick,
remaining free of all intentional injustice ��
- The Hippocratic Oath, 5th Century BC
Hospitals exist to produce quality health care for their patients. In the final
analysis, all members of the hospital staff should dedicate themselves to
the pursuit of the well-being and health of all patients. Whereas our
concern thus far in the report has been to convey and analyse the beliefs,
values, and practices of different categories of staff, we now shift our
focus to the patient. In the preceding sections, patients� views were
integrated into the report where they related to issues common to all
categories of respondents. In this section, we focus on patients�
perspectives as they pertain to other issues.
Results are presented under the following headings:
• Relationship with nurses and doctors
• Levels of satisfaction with various aspects of the hospital service
• Experience of unethical behaviour by hospital staff
• Treatment by student nurses and student doctors
• Various ethical issues
10.1 Relationship with nurses and doctors
How do patients experience their relationship with nurses and doctors? Do
they view nurses and doctors differently in respect of seven sets of
categories presented to them? The answers to these questions �
comparing patients� experiences of nurses and doctors � are presented in
Figures 10.1 to 10.7 below.

78
0
50
100
Respectful - disrespectul
Nurses 52.1 5.7 8.8 18 5.7 0.5 9.3
Doctors 75 2.1 4.7 4.2 2.1 1.6 10.4
1 2 3 4 5 6 7
0
50
100
Professional - unprofessional
Nurses 48.2 9.9 11 9.9 6.3 4.2 10.5
Doctors 77.4 5.8 1.6 5.8 2.1 1.6 5.8
1 2 3 4 5 6 7
0
50
100
Relaxed - tense
Nurses 48.1 8.1 13 16.2 5.4 1.1 8.1
Doctors 69.7 4.3 7.4 6.9 5.3 1.1 5.3
1 2 3 4 5 6 7
Figure 10.1: Nurses and doctors: Respectful � disrespectful
Figure 10.2: Nurses and doctors: Professional � unprofessional
Figure 10.3: Nurses and doctors: Relaxed - tense

79
0
50
100
Caring - Uncaring
Nurses 48.4 10.5 9.5 10.5 6.8 3.2 11.1
Doctors 74.1 5.8 4.8 3.2 1.6 2.6 7.9
1 2 3 4 5 6 7
0
50
100
Compassionate - Cold
Nurses 48.1 9.2 10.3 11.4 7 2.7 11.4
Doctors 64.8 5.6 7.8 3.9 2.8 2.8 12.3
1 2 3 4 5 6 7
0
50
100
Approachable - unapproachable
Nurses 48.7 9.4 9.4 13.6 4.2 2.1 12.6
Doctors 74.7 3.7 3.7 4.2 2.6 1.1 10
1 2 3 4 5 6 7
Figure 10.4: Nurses and doctors: Caring - uncaring
Figure 10.5: Nurses and doctors: Compassionate - cold
Figure 10.6: Nurses and doctors: Approachable - unapproachable

80
0
50
100
Trusting - distrusting
Nurses 54.2 7.8 7.8 10.4 7.3 3.1 9.4
Doctors 77.2 3.6 1.6 5.7 3.1 2.1 6.7
1 2 3 4 5 6 7
Figure 10.7: Nurses and doctors: Trusting - distrusting
Discussion
Two trends emerge from these figures. First, the overall pattern of
patients� responses with regard to nurses and doctors is very consistent
across all dimensions. If one collapses the three extreme categories at
both ends of the spectrum, one finds that patients rate various aspects of
care by nurses and doctors very similarly across these dimensions. In all
of these cases, 65-75% of patients rated nurses as being respectful,
professional, relaxed, compassionate, and the like. A small minority of 10-
20% of patients rated nurses to be disrespectful, unprofessional, uncaring
and the like.
A second noteworthy trend relates to the different ratings of nurses and
doctors. Results are in line with earlier findings, namely, that doctors
consistently get more positive or higher ratings than nurses � within a
range of 15�20% on all dimensions.
Although these figures, in broad outline, do present a positive picture and
might give cause for complacency, it is still worth pointing out the
following:
• 15% of patients viewed nurses and doctors as being disrespectful
• 22% of patients viewed nurses as being unprofessional
• 20% of patients experienced nurses as being uncaring and cold
• 19% of patients said nurses were unapproachable
• 20% of patients rated nurses as being distrusting.

81
If one were to generalise, this would mean that one in every five patients
have not had particularly favourable experiences of nurses in particular.
Expressed as numbers of patients, these findings relate to the actual
experiences of hundreds of patients (more than 500) in the hospital at
any given time.
10.2 Levels of satisfaction with various aspects of hospital
services
Patients were subsequently asked to indicate their levels of satisfaction
with various aspects of hospital services they had received. Findings are
summarised in Tables 10.1 to 10.5 below.
Table 10.1: Assistance by nurses on day duty
Frequency Percent Valid Percent
Cumulative Percent
Valid Very satisfied 106 51.7 55.8 55.8 Quite satisfied 36 17.6 18.9 74.7 Somewhat satisfied 26 12.7 13.7 88.4 Quite dissatisfied 9 4.4 4.7 93.2 Very dissatisfied 13 6.3 6.8 100.0 Total 190 92.7 100.0 Missing System 15 7.3 Total 205 100.0
Table 10.2: Assistance by nurses on night duty
Frequency Percent Valid Percent Cumulative
Percent
Valid Very satisfied 76 37.1 41.5 41.5 Quite satisfied 42 20.5 23.0 64.5 Somewhat satisfied 26 12.7 14.2 78.7 Quite dissatisfied 13 6.3 7.1 85.8 Very dissatisfied 26 12.7 14.2 100.0 Total 183 89.3 100.0
Missing System 22 10.7 Total 205 100.0

82
Table 10.3: Quality of medical treatment received
Frequency Percent Valid Percent Cumulative Percent
Valid Very satisfied 112 54.6 61.9 61.9 Quite satisfied 22 10.7 12.2 74.0 Somewhat satisfied 30 14.6 16.6 90.6 Quite dissatisfied 9 4.4 5.0 95.6 Very dissatisfied 8 3.9 4.4 100.0 Total 181 88.3 100.0
Missing System 24 11.7 Total 205 100.0
Table 10.4: Linen on your bed
Frequency Percent Valid percent Cumulative percent
Valid Very satisfied 84 41.0 48.3 48.3Quite satisfied 16 7.8 9.2 57.5Somewhat satisfied
29 14.1 16.7 74.1
Quite dissatisfied 15 7.3 8.6 82.8Very dissatisfied 30 14.6 17.2 100.0Total 174 84.9 100.0
Missing System 31 15.1Total 205 100.0
Table 10.5: Quality of food
Frequency Percent Valid Percent Cumulative Percent
Valid Very satisfied 86 42.0 49.4 49.4 Quite satisfied 20 9.8 11.5 60.9 Somewhat satisfied 33 16.1 19.0 79.9 Quite dissatisfied 12 5.9 6.9 86.8 Very dissatisfied 23 11.2 13.2 100.0 Total 174 84.9 100.0
Missing System 31 15.1 Total 205 100.0
Table 10.6: The room you are in
Frequency Percent Valid Percent Cumulative Percent
Valid Very satisfied 87 42.4 47.0 47.0 Quite satisfied 28 13.7 15.1 62.2 Somewhat satisfied 25 12.2 13.5 75.7 Quite dissatisfied 16 7.8 8.6 84.3 Very dissatisfied 29 14.1 15.7 100.0 Total 185 90.2 100.0
Missing System 20 9.8 Total 205 100.0

83
Summary
In order of satisfaction (combining �very satisfied� and �quite satisfied�),
patients indicated that they were the most satisfied with the following:
• Assistance received from nurses on day duty (74.7%)
• Quality of medical treatment received (74.0%)
• Assistance received from nurses on night duty (64.5%)
• Their rooms (62.2%)
• Quality of food (60.9%)
• Linen on their beds (57.5%)
10.3 Experience of unethical behaviour by hospital staff
In this section, we report on incidents of unethical or unprofessional
behaviour as experienced by patients. Table 10.7 below summarises
results with regard to the following issues: incidents of verbal and physical
abuse; breach of confidentiality of patient information; professional
negligence; and substandard medical care.
Concerning aspects of abuse, minorities of patients reported that they had
been physically abused - either by doctors (3.4%), nurses (8.9%), or
other staff (8.3%). Disconcertingly high proportions of patients reported
verbal abuse, by especially nurses (39%) but also other staff (27.3%). In
addition, a small percentage (7.6%) indicated that doctors had verbally
abused them.
Patients must be able to believe that any private information about
themselves and their medical condition would be treated in confidence. A
small but significant percentage (12.5%) indicated that they had
experienced breaches of such confidentiality.
In respect of professionalism and quality of medical care, nearly a quarter
of patients (23%) reported experiencing negligence in care, with a similar
proportion (26%) indicating having received substandard medical care at
least once.

84
There are unacceptably high levels of verbal abuse, especially by nurses
and support staff, one in eight patients having had confidentiality of
private information breached, and quality of health care and
professionalism leave much to be desired. These results are cause for
grave concern and require immediate action by hospital management.
Table 10.7: Incidents of unethical behaviour experienced by patients
Never Once or
twice
Three times
or more
Verbal abuse by a nurse 61 18.7 20.3
Verbal abuse by a doctor 92.4 6.5 1.1
Verbal abuse by another CHBH employee
(such as porters)
73.7 12.2 15.1
Physical abuse by a nurse 91.2 6.1 2.8
Physical abuse by a doctor 96.7 1.7 1.7
Physical abuse by another CHBH employee
(not nurse/doctor)
91.7 6.1 2.2
Breach of confidentiality of patient
information
87.5 8.5 4.0
Professional negligence in patient care 77.6 13.2 9.3
Substandard medical care 74.9 17.3 7.8
10.4 Treatment by student nurses and student doctors
An important aspect of patients� experiences - especially of the quality of
care they receive � relates to their being treated by student nurses and
student doctors. Tables 10.8 and 10.9 summarise patients� responses to
questions regarding this aspect. Boxes 10.1 and 10.2 list some of the
reasons for their concerns.

85
Table 10.8: Do you mind being cared for by student nurses?
Frequency Percent Valid Percent
Cumulative Percent
Valid Yes 42 20.5 22.6 22.6No 144 70.2 77.4 100.0Total 186 90.7 100.0
Missing System 19 9.3Total 205 100.0
Box 10.1 Treatment by student nurses Female patient: �I mind because she is not a professional nurse, she is still a student. She is not a qualified nurse, she is still learning. The best way she must go together with qualified nurse.� Female patient: �I do mind because sometimes a student nurse can make mistakes, she can inject you with a wrong injection, or she/he can use a rectal thermometer instead of an oral one (in the mouth).� Male patient: �Quite number of student nurses not qualified when it comes to examining the patient. They are unprofessional; as a matter of fact, they did not complete the course.� Female patient: �Because she goes out looking for someone to ask, and they are wasting my time. I want a real nurse who knows his or her job.� Female patient: �They might give me the wrong medication.� Male patient: �As a patient or human being, my well-being must be taken care of by someone who is qualified or professional.� Female patient: �Because student nurses are not professionals, they sometimes give patients wrong information or medical treatment, so I do mind.� Male patient: �Because I do not trust that they know what they are doing.�
Table 10.9: Do you mind being examined by student doctors?
Frequency Percent Valid Percent
Cumulative Percent
Valid Yes 36 17.6 19.7 19.7No 147 71.7 80.3 100.0
Total 183 89.3 100.0Missing System 22 10.7
Total 205 100.0

86
Box 10.2 Treatment by student doctors Female patient: �Yes because it took a long time to examine you, as student doctors want to examine you the way he or she wants.� Male patient: �They give wrong medication; often examine the patient, which leads to death.� Male patient: �Sometimes they don�t listen to your problems.� Female patient: �I feel that they are not professional enough and feel that they will not examine me the way I want to be.� Female patient: �Because I don�t feel safe they might give me the wrong diagnosis.� Male patient: �I was once drugged by a student doctor and my hand was swollen for about 7-9 days.� Female patient: �They make lots of mistakes; they are not yet professional.� Female patient: �Especially when coming to operations, I also mind, because they can put your life in danger without being aware that they have done something wrong.� Female patient: �It is hard to trust or believe their judgement unless a full doctor will be consulted afterwards.�
Discussion
Relatively small proportions of patients indicated reservations about being
examined by student nurses and doctors. Slightly more than 20% said
that they had concerns about being examined by student nurses, with a
similar proportion (19%) expressing reservations about being examined
by student doctors. An inspection of the qualitative comments shows that
the common reasons for these reservations relate to perceived lack of
professionalism, inexperience, and possible lack of quality care.
10.5 Various ethical issues
A number of statements were put to patients in order to assess their
general views on various ethical issues as well as the moral implications of
patient care. These issues refer to possible bribery, overworked staff,
ethical issues about informed consent, and adequate patient briefings. The
results are summarised in Tables 10.10 to 10.15 below.

87
Table 10.10: Patients who give money to staff at CHBH for services or treatment act wrongly
Frequency Percent Valid Percent Cumulative
PercentValid Strongly agree 117 57.1 63.2 63.2
Tend to agree 11 5.4 5.9 69.2Tend to disagree 10 4.9 5.4 74.6Strongly disagree 30 14.6 16.2 90.8No opinion 17 8.3 9.2 100.0Total 185 90.2 100.0
Missing System 20 9.8 Total 205 100.0
Table 10.11: Staff at CHBH do not have sufficient time to treat
patients with the necessary compassion and understanding
Frequency Percent Valid percent Cumulative percent
Valid Strongly agree 108 52.7 58.7 58.7Tend to agree 23 11.2 12.5 71.2Tend to disagree 12 5.9 6.5 77.7Strongly disagree 24 11.7 13.0 90.8No opinion 17 8.3 9.2 100.0Total 184 89.8 100.0
Missing System 21 10.2Total 205 100.0
Table 10.12: Language barriers make it difficult for staff to convey to patients proper information about their diagnosis and treatment
Frequency Percent Valid
Percent
Cumulative Percent
Valid Strongly agree 117 57.1 64.3 64.3Tend to agree 18 8.8 9.9 74.2Tend to disagree 10 4.9 5.5 79.7Strongly disagree 18 8.8 9.9 89.6No opinion 19 9.3 10.4 100.0Total 182 88.8 100.0
Missing System 23 11.2Total 205 100.0

88
Table 10.13: I sometimes find it difficult to understand what doctors tell me about my illness
Frequency Percent Valid Percent Cumulative Percent
Valid Strongly agree 116 56.6 63.7 63.7Tend to agree 16 7.8 8.8 72.5Tend to disagree 7 3.4 3.8 76.4Strongly disagree 27 13.2 14.8 91.2No opinion 16 7.8 8.8 100.0Total 182 88.8 100.0
Missing System 23 11.2Total 205 100.0
Table 10.14: I am always told what is wrong with me and why certain medicines are given to me
Frequency Percent Valid Percent Cumulative Percent
Valid Strongly agree 33 16.1 21.9 21.9Tend to agree 12 5.9 7.9 29.8Tend to disagree 9 4.4 6.0 35.8Strongly disagree 88 42.9 58.3 94.0No opinion 9 4.4 6.0 100.0Total 151 73.7 100.0
Missing System 54 26.3Total 205 100.0
Table 10.15: I usually find it easy to understand what nurses tell me about my illness
Frequency Percent Valid Percent Cumulative Percent
Valid Strongly agree 69 33.7 37.3 37.3Tend to agree 45 22.0 24.3 61.6Tend to disagree 24 11.7 13.0 74.6Strongly disagree 33 16.1 17.8 92.4No opinion 14 6.8 7.6 100.0Total 185 90.2 100.0
Missing System 20 9.8Total 205 100.0

89
Salient points
• The vast majority of patients (70%) agreed that giving money to
staff for treatment was wrong.
• A similar proportion of patients (71%) agreed that hospital staff did
not have sufficient time to treat them properly.
• Language barriers between staff and patients are a serious
problem, given that three-quarters of patients said that such
barriers posed difficulties for mutual understanding. A similar
proportion of patients (72%) indicated that they had had problems
understanding what doctors had told them about their illness.
• Nearly two-thirds of patients (64%) claimed that they had not told
or informed what was wrong with them and why they had received
certain kinds of medication.
• There seems to be better communication between patients and
nurses, with 62% of patients indicating that they found it easy to
understand what nurses told them about their illness. By contrast,
almost three-quarters of patients (72,5%) sometimes found it hard
to understand what doctors tried to communicate to them about
their illness.
One�s overarching impression is that most patients are not well informed
about their illness, or the reason for the treatment or medication they
receive. Given that these are basic patients� rights, it is imperative that
the hospital addresses these issues as a matter of urgency.
10.6 Concluding comments
We conclude this section on patient perspectives by highlighting key
findings:
• Majorities of patients (ranging between 65 and 75%) rated nurses
as being respectful, professional, relaxed, compassionate, and the
like. A small minority of between 10 and 20% of patients rated
nurses to be disrespectful, unprofessional, uncaring, and the like.
However, it is interesting � and a cause for concern � that nurses
and doctors consistently received different ratings for clinical care.
These results are in line with earlier findings - doctors get more

90
positive ratings � within a range of 15�20% higher ratings on all
dimensions.
• Patients are mostly satisfied with the assistance and quality of
medical treatment they received. They are less satisfied with their
rooms and the quality of food, and least satisfied with the linen on
their beds.
• There are unacceptably high levels of verbal abuse, especially by
nurses and support staff, patient information is not always treated
in confidence, and quality of health care and professionalism leave
much to be desired. These results are cause for grave concern and
require immediate action by hospital management.
• Relatively small proportions of patients indicated reservations about
being examined by student nurses and student doctors. Common
reasons for such reservations relate to perceived lack of
professionalism, inexperience, and possible lack of quality care.
• Concerning informed consent and general sharing of medical
information, most patients are not well informed about their illness
or the reasons for treatment or medication regimes.

91
SECTION 11 CONCLUSIONS AND RECOMMENDATIONS
11.1 Conclusions
Given the nature of its mission, a hospital should embody the highest
human values with the aim of optimal professionalism and quality patient
care. (See Appendix 9 for the mission statement of CHBH.) Further,
because a hospital is an organisation, one would expect a commitment to
other organisational values, such as good staff relations, a good
organisational work ethic, and the like. In short, one would expect to find
the �usual� organisational values, and, in addition, values peculiar to a
�hospital�.
It is important to realise that organisational culture and values are, among
other things, embedded in sets of material conditions - organisations are
not merely institutions that �house� people, their beliefs and values, but
also consist of buildings, infrastructure, equipment, and supplies. Unless
the required material conditions are in place and functioning well, no
institution can operate effectively and efficiently.
We represent the relationship between the material and physical
�foundation�, on the one hand, and more symbolic culture and values, on
the other, in Diagram 11.1 below. But our interest, ultimately, in this
audit, is in how the material/physical conditions, together with the
organisational culture and values, impact on professional conduct of staff
in their relationships with patients. Stated differently: how does the place
where people work, and the values and beliefs prevalent in that
organisation, affect the manner in which they interact with and care for
patients? It is within this context that we examined the nature and extent
of instances of misconduct at CHBH.

92
If we take the diagrammatic representation below (Diagram 11.1) as our
point of reference, it becomes possible to summarise the main findings of
the study as follows:
Diagram 11.1: A hospital as an institution: Foundation, cultural
pillars, and pinnacle
The foundation
Evidence from the survey identified serious problems relating to the
physical plant (neglect and poor maintenance; perceptions of
uncleanliness), lack of safety and security, insufficient management of
supplies (linen and medicine), and insufficient and outdated equipment.
PROFESSIONAL
CONDUCT
FIRST PILLAR
GENERAL
ORGANISATIONAL CULTURE
AND VALUES
SECOND PILLAR
HOSPITAL-SPECIFIC
CLINICAL CARE CULTURE
AND VALUES
MATERIAL AND PHYSICAL CONDITIONS

93
First pillar: General organisational culture
CHBH staff does not believe it is a hospital with a good working
environment, there is clearly no positive work ethic, and staff relations are
characterised mainly as distrusting, dishonest, and disloyal. Staff displays
unhappiness about the lack of participative management and inadequate
channels of communication. But the biggest concerns relate to staff
shortages and poor conditions of service.
Second pillar: Clinical care culture special to a hospital as an
institution
Concerning staff-patient relationships, there is insufficient recognition of
patients� rights, little mutual respect exists between staff and patients
(abuse is widespread), and, generally, insufficient attention is given to
professional and quality of care.
The pinnacle
The nature and extent of misconduct at CHBH is of grave concern. Staff
and patients reported extensive verbal and physical abuse (by both
patients and staff), bribery and fraud are not unanimously condemned,
and patients� rights are often violated, resulting in substandard quality of
overall patient care.
11.2 Recommendations
The following twenty-six recommendations are premised on our conviction
that appropriately addressing concrete organisational issues would
substantially improve the ethics culture at CHBH � in terms of the beliefs
and values that inform conduct or action, as well as conduct or action
itself.
The ideal is to achieve a good institutional or organisational ethics culture,
for the benefit of all stakeholders - internal (patients, staff, etc.) and
external (the community served by CHBH, contractors, vendors, visitors,
etc.). We do not claim that our recommendations are exhaustive, or that
their implementation alone would achieve this end. They represent the
94
understanding we have gained concerning some salient issues raised by
CHBH staff in the course of our ethics audit.
We are, however, convinced that no attempt at addressing the very real
organisational and ethical issues at CHBH could succeed without coming to
terms with our main findings and conclusions, as well as the following core
recommendations emanating from them.
MANAGEMENT AND LEADERSHIP
Recommendation 1:
Managing such an enormous and complex institution
requires that the authority and powers of the CEO and
central hospital management be on a par with those of their
peers in private-sector hospitals, rather than be centralised
in a (distant) government department. In short, substantive
powers should be conferred upon and exercised by central
hospital management (for example, internal budgetary
powers, and powers of hiring and firing, and discipline).
Remarks: New powers26 have indeed recently been delegated to
public-hospital central management, but it is unclear exactly how
these powers would be exercised in Gauteng. Most importantly,
disciplinary powers (for example, powers of dismissal for
misconduct) should not disappear in an administrative or appeals
�black hole�. Still, they should always conform to the canons of
justice and fairness.
26 Gauteng Provincial Government Department of Health: Delegation of Powers and Assignment of Duties in terms of the Public Finance Management Act (Act 1, 1999). Johannesburg, 26 September 2001.

95
Recommendation 2:
Management expertise and professionalism on all levels
should be of the highest order and, to this end, there should
be ongoing sharing of expertise and experiences between
the public and private sectors, and academia.
Remarks: Private hospital groups should see it as part of their social
responsibility to assist public hospitals. Similarly, universities and
technikons, as training facilities for future health-care professionals,
need to shoulder some responsibility for improving management
expertise and professionalism. For example, CHBH would benefit
from relevant research undertaken by business schools and
technikons into management and operations, in essence leading to
useful partnerships.
Recommendation 3:
Management on all levels should, as a matter of urgency,
review the prevailing management style and culture of the
hospital, and should put in place conditions for consultative
leadership, constructive communication, and participatory
decision making at all levels in the hospital.
Remarks: Initiatives such as the following should be considered:
open and free access to official forms of communication, recognition
by superiors, structured and regular feedback from superiors,
freedom of expression without fear of reprisal (including reporting
of misconduct); and creating an atmosphere of joint responsibility,
accountability, and transparency. Ultimately, initiatives are not the
sole responsibility of central hospital management, but are likewise
that of management at all levels of the organisation (heads of
academic departments, laboratory services, nursing services,
cleaning services, etc.)

96
HUMAN RESOURCES
Recommendation 4:
Staff numbers should be reviewed as a matter of urgency
with a view to an increased budget allocation, and such a
review could be done with the assistance of private-sector
hospital groups as a social-responsibility initiative.
Remarks: The key criterion in such a review process should be
quality patient care conforming to accepted standards of care. It
stands to reason that existing staff be deployed optimally.
Moreover, organisational initiatives should be directed at creating a
working environment conducive to employee productivity and job
satisfaction as well as thoroughgoing professionalism at all levels
(see recommendations below). Importantly, some sectors of the
hospital (such as general admissions and discharge, casualty
admissions, and the pharmacy or dispensary) seem to experience
particularly acute staff shortages, and such shortages appear to be
at the root of many other problems in the hospital. In addition,
clerical staff must be appointed in admission wards, such as Ward
20, on a 24-hour basis.
Recommendation 5:
Review of staff development should become a matter of high
priority, through in-service and continuing education and
training.
Remarks: Aspects of staff development that need attention relate
communication and other interpersonal skills, (cultural) diversity
training and education, and ethics and human rights. The goals of
staff development should always be informed by the needs of both
staff and patients.

97
Recommendation 6:
Institute staff enrichment programmes, through team-
building workshops and other initiatives, with a view to
assuring cooperation, professionalism, and quality service on
all levels.
Remarks: Enrichment (in addition to skills development) focuses on
building competence and self-confidence on a bottom-up level and
with a view to problem solving and effective decision making. It is
worth noting that a pilot study being undertaken in some of the
wards at Kalafong Hospital, Gauteng, may yield a useful model for
such exercises.
Recommendation 7:
Conditions of service of staff should be reviewed
periodically, and this should be done in an open process with
all stakeholders, including staff.
Remarks: Pressing issues relate to general remuneration,
remuneration for overtime work and night duty, accommodation at
or near the hospital, transport, a crèche, and the quality of food.
Recommendation 8:
Structured performance evaluation with a view to
adjustment of remuneration, in particular, should be done in
terms of fair and just criteria, and in an interactive process,
based on regular and constructive feedback, spelling out
avenues for performance improvement, and introducing
incentives.
Remarks: Dissatisfaction with remuneration appears to have more
to do with unilateral changes than public-private sector
discrepancies. Performance evaluation, for example, appears to
cause serious dissatisfaction. Annual salary increases were replaced
by performance evaluations leading to notch increases and leg

98
(rank) promotions, but these have reportedly been withheld by the
Gauteng Department of Health.
Recommendation 9:
Induction or orientation programmes should be put in place
to educate new staff about all relevant values statements,
codes of ethics, and rules and procedures; and opportunities
should be created for renewing the understanding and
commitment of incumbents to those documents and the
values they represent.
Remarks: The health professions have international and local
guiding documents in the form of value oriented ethics statements
and compliance oriented codes of conduct. In addition, each
organisation or institution has its own statements, codes and
procedural and disciplinary rules, which should be reviewed and
updated on an ongoing basis.
MATERIAL RESOURCES
Recommendation 10:
The hospital as a physical plant � in terms of appearance,
maintenance, cleanliness, hygiene, and the like � should be
upgraded as a matter of urgency.
Remarks: Many aspects of the physical condition and appearance of
the hospital can be attended to with relatively little expenditure.
Painting walls and keeping wards clean require material resources,
commitment and pride, and some effort.

99
Recommendation 11:
Security in and around the hospital needs urgent review in
order to protect material and human resources; and a
thorough security audit conducted by an independent
security facility needs to be done with a view to putting the
best possible systems in place.
Remarks: Security is a huge concern for respondents,
understandably so. Violent social conditions in the country make
security a top priority. Disregard for others� or the state�s material
possessions (through theft, pilfering, reckless handling, or
destruction) and violence against the person (such as verbal abuse
or physical abuse, assault, etc.) are wholly antithetical to what a
hospital as an institution is supported to stand for. Issues such as
rights of admission, searches upon leaving hospital premises,
identifying marks on equipment, installing surveillance cameras,
introducing effective punitive action, and the like, need to be
explored.
Recommendation 12:
The desirability and feasibility of outsourcing or privatising
certain services - such as security, linen, cleaning, or porters
� need to be investigated. Alternatively, such services need
to be reviewed by independent outside companies, with a
view to skills training, monitoring performance, and the like.
Recommendation 13:
A thorough audit of the state and adequacy of all equipment
necessary for quality patient care and services needs to be
done, with a view to budgeting for repairs, maintenance,
replacement, upgrading, and the like.
Remarks: The state of repair of equipment in the hospital, outdated
equipment, and ordering patterns appear to be a very important
concern to a wide spectrum of employees.

100
Recommendation 14:
The management, control and logistics of the linen supply
need thorough review as a matter of high priority.
Remarks: Overall, linen appears to be an issue more important than
medicine. This is not surprising, since in-patients� bodies are in
almost constant contact with linen, and linen may be regarded as
symbolic of cleanliness, comfort, and personal caring. There
appears to be widespread mismanagement of the supply, cleaning
and security of linen.
Recommendation 15:
There should be a review of the adequacy of medicine supply
in the hospital as a whole, the desirability and feasibility of
decentralising the pharmacy to specialist wards, and security
of stock holding and dispensing.
Recommendation 16:
Given increasing HIV/AIDS admissions, the hospital will
need to obtain, and base policies on, reliable data with a
view to addressing infrastructural consequences for bed
occupancy rates, length of stay, linen, food, and the like.
Remarks: With increasing numbers of very sick patients likely to
become dependent on and dying in public hospitals, the
demographics of such hospitals will increasingly take on a shape
unlike that of hospitals in the past or in other parts of the world.

101
ADMISSIONS
Recommendation 17:
Admissions criteria need to be reviewed with a view to
putting in place clear policies, or proclaiming and justifying
existing ones.
Remarks: Staff is concerned about several aspects of admissions,
such as referrals from feeder institutions (clinics and other
hospitals); intake with no apparent match between patient numbers
and hospital capacity; intake of foreigners or non-South Africans;
and members of medical schemes who claim free treatment. The
issue of foreigners came up repeatedly in the open-ended questions
(qualitative data), and raises the spectre of xenophobia. Clear
admissions policies should be enunciated to all stakeholders.
Recommendation 18:
Admissions clerks must be supervised effectively on a 24-hour
basis.
Remarks: It is unacceptable that clerks are absent from duty, or, when on
duty, are unfit to discharge their responsibilities for whatever reason.
DISCIPLINE AND ETHICS
Recommendation 19:
The hospital should develop and adopt an aspirational
(general) values statement.
Remarks: Such a values statement should be brief, set out commitments
to basic ethical values, be displayed, publicised and promoted, and be
reinforced at all opportunities. In short, it should be a living document,
developed by all stakeholders, in a joint process.

102
Recommendation 20:
The hospital should systematically develop new, or review
existing, compliance oriented codes of ethics (conduct), or
disciplinary codes, for all categories of employees; and
sanctions for transgressions should be enforced in fair and
just disciplinary hearings.
Recommendation 21:
Given the recently conferred powers of the CEO and central
hospital management,27 disciplinary committees should be
constituted, their brief should be widely publicised, and they
should operate in an environment of transparency and
fairness. Importantly, disciplinary powers should be in line
with practices negotiated between management and labour
in the private sector.
Remarks: Care should be taken that the appeals procedure in terms
of central management�s newly delegated powers28 does not
become a novel administrative or appeals �black hole� into which
disciplinary cases disappear. Appeals procedures should be fair,
efficient, and speedy.
Recommendation 22:
It is crucially important that appropriate mechanisms be put
in place to protect or shield any employee who reports
unethical or unlawful conduct of fellow employees from
breach of confidentiality, intimidation, or victimisation.
Moreover, at all times every employee should be protected
against intimidation and victimisation through disciplinary
measures.
27 Gauteng Provincial Government Department of Health (26 September 2001): Delegation of Powers and Assignment of Duties in terms of the Public Finance Management Act (Act 1, 1999). Johannesburg. 28 Ibid.

103
Recommendation 23:
The hospital should consider constituting a hospital or
institutional ethics committee that would serve as an
advisory body on ethical issues, including clinical practice, to
which all stakeholders, including patients, can appeal.
Remarks: The purpose of such a committee would be to encourage
a culture of reflection and debate about the complexities of
institutional and clinical decision making, and to advise in disputes.
PATIENT CARE
Recommendation 24:
Health-care professionals at all levels should be thoroughly
conversant with patients� rights as set out in all relevant
documents.
Remarks: Established patients� rights to respect, promotion of
welfare, privacy, confidentiality, informed consent, and the like, are
non-negotiable. There are strong indications that even these basic
rights are not practised adequately in the hospital. Relevant
documents setting out these rights are, for example, the National
Patients� Rights Charter of the national Department of Health (see
Appendix 8) and Nurses and Human Rights (International Council of
Nurses, 1998).
Recommendation 25:
Patients should be made aware of all their rights, and
importantly, their responsibilities upon admission, or at the
bedside when appropriate, and they should have access to
formalised complaints procedures without fear of
victimisation.

104
GAUTENG DEPARTMENT OF HEALTH AND THE TREASURY
Recommendation 26:
Since many of these recommendations rely on the
availability of resources, central hospital management
should approach the Gauteng Department of Health with
strong, socially motivated, appeals for budgetary allocations.
Remarks: A provincial Department of Health has a crucial advocacy
role on behalf of its public hospitals in respect of the national
Treasury.

105
APPENDICES
APPENDIX 1 LETTER ACCOMPANYING QUESTIONNAIRES, ADDRESSED TO RESPONDENTS

106
Ethics Institute of South Africa (EthicSA) Chris Hani Baragwanath Hospital Sanlam Gables, 1209 cnr Schoeman Old Potchefstroom Road & Duncan Streets, HATFIELD Diepkloof Zone 6, SOWETO PO Box 2427 PO Birkham BROOKLYN SQUARE, 0075 2013 Tel +27(0)12 342 2799 Tel +27(0)11 933 8000 Fax +27(0)12 342 2790 Fax +27(0)11 933 3135
August 2001
An ethics audit at Chris Hani Baragwanath Hospital (CHBH)
Dear Respondent Almost on a daily basis, media reports describe the conditions of public hospitals in South Africa as �appalling�, �shocking�, or, putting it more strongly, as being in �dire straits�. Health-care professionals, in particular doctors and nurses in public-sector hospitals, are reported to work in harsh and often squalid conditions. Budget cuts, the effects of the Aids pandemic, and many other factors all impact on the effective functioning of a public hospital. It is against this background that I have requested the Ethics Institute of South Africa to undertake an ethics audit of CHBH. The aim of the audit is to focus on questions regarding ethical values and beliefs, knowledge of ethical and unethical conduct, and ethical practices and their implications in order to establish (a) whether the moral conduct and attitudes of various subgroups within CHBH are affected by the environment in which they work; and, (b) if so, in what respects. Other issues to be covered include items on job satisfaction, relations between staff and patients, attitudes towards management and labour unions, security and the physical environment in which staff work. The audit will be conducted amongst all staff at CHBH. I would like to urge you to give your fullest co-operation to the research team during the study which will be conducted in July and August of this year. I also wish to emphasize that your responses to this questionnaire are anonymous (you will not be asked to add your name to the questionnaire) and that your responses will be treated with the utmost confidentiality. Yours sincerely,
Dr. Reg Broekmann CEO: Chris Hani Baragwanath Hospital

107
APPENDIX 2 QUESTIONNAIRE: MANAGEMENT © EthicSA 2001

108
QUESTIONNAIRE FOR MANAGEMENT SECTION A: ORGANISATIONAL ISSUES Organisational culture 1. Interpersonal relations (i.e. how people behave or act towards each other when they are together)
can be rated on various dimensions. For each pair of adjectives below, please circle the number that, in your view, best characterises interpersonal relations among staff at CHBH in general. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that relations among staff are totally honest, you will circle a 1; if you believe that it is totally dishonest, you will circle a 7. If you believe that it is only somewhat dishonest, you will circle a 5.) PLEASE COMPLETE THE FOLLOWING: (a) Honest 1 2 3 4 5 6 7 Dishonest (b) Respectful 1 2 3 4 5 6 7 Disrespectful (c) Loyal 1 2 3 4 5 6 7 Disloyal (d) Trusting 1 2 3 4 5 6 7 Distrusting (e) Professional 1 2 3 4 5 6 7 Unprofessional (f) Relaxed 1 2 3 4 5 6 7 Tense and stressed
2. Below is a list of six organisational values. Please rate how much CHBH cares about each right now:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Serving the greatest number of patients as possible 1 2 3 4 5 (b) Avoiding bad publicity 1 2 3 4 5 (c) Not having strikes and social unrest 1 2 3 4 5 (d) Good work ethic 1 2 3 4 5 (e) Balancing the books 1 2 3 4 5 (f) Providing the best possible working environment 1 2 3 4 5
3. Below is a list of four professional values in service delivery to patients. To what extent are they practiced at CHBH? In each case distinguish between how much doctors and nurses respectively give expression to these values
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Doctors 1 2 3 4 5 (a) Compassion for patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (b) Confidentiality of patient information Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (c) Respect for dignity of patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (d) Respect for well-being of patients Nurses 1 2 3 4 5

109
Leadership and management
4. Please rate how much you agree or disagree with the following statements concerning leadership and management practices at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) The hospital management takes suggestions from below seriously. 1 2 3 4
(b) There are proper incentives in place to improve staff performance. 1 2 3 4
(c) Staff members have a say in matters of decision-making. 1 2 3 4 (d) The hospital management is clear about the career
prospects of employees. 1 2 3 4
(e) Top management has no secrets from employees. 1 2 3 4 (f) Management at CHBH is basically powerless. 1 2 3 4
Channels of communication 5. Please rate how much you agree or disagree with the
following statements concerning communication practices at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) Employees are not allowed to say what they really think. 1 2 3 4 (b) Clear guidelines exist regarding staff members�
responsibilities. 1 2 3 4
(c) My supervisor effectively follows up on complaints that I direct via him/her. 1 2 3 4
(d) My supervisor regularly gives me feedback about my performance. 1 2 3 4
(e) I am always last to be informed about decisions that concern my work. 1 2 3 4
(f) There is a system in place that employees can use to report instances of misconduct without being victimised. 1 2 3 4
(g) Rumour (the �grapevine�) is a common source of information at CHBH.
1 2 3 4
Resources 6(a). Do you experience an under-supply of medicine at CHBH?
Yes 1 No 2 Don�t know 3
6(b) If Yes, to what extent do the following contribute tothe under-supply of medicine at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Over-ordering of medicines by ward sisters 1 2 3 4 5 (b) Theft of medicines from hospital stocks by staff 1 2 3 4 5 (c) Influx of non-South African patients 1 2 3 4 5 (d) HIV/AIDS pandemic 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5
(f) Other (Please specify:����������.�
�.��������������������.
1 2 3 4 5

110
7(a). Do you experience a general shortage of linen at CHBH?
Yes 1 No 2 Don�t know 3
7(b). If Yes, to what extent do the following contribute tothe linen shortages at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Stealing of linen by hospital staff 1 2 3 4 5 (b) Linen theft committed by patients 1 2 3 4 5 (c) Increased patient population related to the
HIV/AIDS pandemic 1 2 3 4 5
(d) Ineffective logistical and practical arrangements 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5
(f) Other: (Please specify:���������.�
��������������������.
1 2 3 4 5
Job satisfaction
8. Some jobs are more interesting and satisfying than others. We want to know how you feel about your job. For each of the following statements please circle one of the alternatives which best describes your opinion. St
rong
ly
agre
e
Ten
d to
agr
ee
Ten
d to
di
sagr
ee
Stro
ngly
disa
gree
(a) I am often bored with my job. 1 2 3 4 (b) I am satisfied with my job for the time being. 1 2 3 4 (c) Each day of work seems like it will never end. 1 2 3 4 (d) I find real enjoyment in my work. 1 2 3 4 (e) It feels as if I am working in a �second-class� hospital. 1 2 3 4 (f) I feel proud to be associated with CHBH. 1 2 3 4 (g) My opinion of myself increases when I do my job well. 1 2 3 4 (h) I frequently think of quitting my job. 1 2 3 4
9. Overall, how satisfied are you with each of the following?
Ver
y sa
tisfie
d
Qui
te
satis
fied
Som
ewha
t sa
tisfie
d
Qui
te
diss
atis
fied
Ver
y
diss
atis
fied
(a) Your salary? 1 2 3 4 5 (b) Cooperativeness of colleagues? 1 2 3 4 5 (c) Your conditions of service, e.g. leave and fringe benefits?
1 2 3 4 5
(d) Your workload? 1 2 3 4 5

111
Physical environment 10. On a scale of 1 to 7, how do you rate the physical environment at CHBH in terms of the following
dimensions? (The closer a number to a value, the more that value represents your experience. For instance, if you believe that CHBH is very clean, you will circle a 1; if you believe that it is very dirty, you will circle a 7. If you believe that it is somewhat dirty, you will circle a 5.)
(a) Clean 1 2 3 4 5 6 7 Dirty (b) Safe 1 2 3 4 5 6 7 Unsafe (c) Attractive 1 2 3 4 5 6 7 Unattractive (d) Depressing 1 2 3 4 5 6 7 Cheerful
11. Please rate how much you agree or disagree with the
following statements concerning security and safety at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) The security screening of visitors leaves much to be desired. 1 2 3 4
(b) The unsafe environment at CHBH can be related to the influx of non-South African patients. 1 2 3 4
(c) The number of security staff at CHBH is sufficient to combat crime. 1 2 3 4
(d) Security staff at CHBH is well equipped with the necessary skills and facilities to combat crime. 1 2 3 4
(e) The security screening of applicants for employment leaves much to be desired. 1 2 3 4
(f) It is the responsibility of government to ensure a safe environment at CHBH. 1 2 3 4
Admission criteria 12. (a) According to what criteria are patients admitted to CHBH?
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� (b) In your view, do you believe that the admission criteria are strictly adhered to?
Yes 1 No 2 Don�t know 3
13. Should CHBH adopt the policy of other hospitals to close their doors when beds are not available?
Yes 1 No 2 Don�t know 3

112
Labour unions 14. (a) Do you think it is useful to have unions operating within the hospital?
Yes � unions are useful in every aspect 1 Yes and no � unions are useful in some ways but problematic in others 2 No � unions are not useful at all 3
(b) Please give a reason for your answer to Question 17(b):
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� 15. In your view, to what extent do the unions influence the decisions made at CHBH?
Very great extent 1 Great extent 2 Moderate extent 3 To some extent 4 Very little extent 5
16. Please rate how much you agree or disagree with the following statements concerning labour unions at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) The unions at CHBH serve to enhance discipline. 1 2 3 4 (b) Unions are responsible for much of the chaos at CHBH. 1 2 3 4
SECTION B: MISCONDUCT AND STANDARDS OF CARE
17. During the past year, how often have you witnessed the following happening at CHBH?
Onc
e
Tw
ice
Thr
ee
times
or
mor
e
Nev
er
No
opin
ion
(a) Over-ordering of medicine 1 2 3 4 5 (b) Patients/visitors bribing staff 1 2 3 4 5 (c) Moonlighting by staff 1 2 3 4 5 (d) Staff verbally abusing patients 1 2 3 4 5 (e) Staff physically abusing patients 1 2 3 4 5 (f) Patients verbally abusing staff 1 2 3 4 5 (g) Patients physically abusing staff 1 2 3 4 5 (h) Lack of informed consent 1 2 3 4 5 (i) Breach of confidentiality of patient information 1 2 3 4 5 (j) Lack of compassion for patients 1 2 3 4 5 (k) Special groups of patients getting different levels of care
(TOP, AIDS, Aliens, Pregnant women, TB, Teenage pregnancy)
1 2 3 4 5
(l) Professional negligence in patient care 1 2 3 4 5 (m) Substandard postoperative care 1 2 3 4 5

113
18. Please rate how much you agree or disagree with the following statements:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) Payment to employees at CHBH by patients or their family for services or treatment given is fraud. 1 2 3 4 5
(b) Employees who engage in threatening or violent behaviour on the job are seldom subjected to immediate disciplinary action.
1 2 3 4 5
(c) Misconduct at CHBH relates mainly to lack of discipline. 1 2 3 4 5 (d) Disciplinary measures at CHBH are not �visible�. 1 2 3 4 5 (e) Health professionals at CHBH do not have sufficient time
to treat patients with the necessary compassion and understanding.
1 2 3 4 5
(f) Language barriers make it difficult for health care professionals to convey to patients proper information about their diagnosis and treatment.
1 2 3 4 5
(g) Because of the heavy workload at CHBH it is fair for employees to ask for small incentives (�tips�) for services.
1 2 3 4 5
(h) A hospital ethics committee would assist in guiding health professional conduct. 1 2 3 4 5
SECTION C: PROBLEMS AND SOURCES OF STRESS
19. Please rate the extent to which you consider the following as a problem or source of stress at CHBH:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Resource related (a) Poor/outdated equipment 1 2 3 4 5 (b) Not enough medicine 1 2 3 4 5 (c) Linen shortage 1 2 3 4 5 Staff related (d) Poor remuneration 1 2 3 4 5 (e) Long shifts 1 2 3 4 5 (f) Night duty 1 2 3 4 5 (g) General shortage of staff 1 2 3 4 5 (h) Poor staff communication 1 2 3 4 5 (i) Supervision/issues of authority 1 2 3 4 5 Patient related (j) Patients with low levels of schooling 1 2 3 4 5 (k) Long-stay patients 1 2 3 4 5 (l) Impossible/demanding patients 1 2 3 4 5 (m) Substandard care because of large numbers 1 2 3 4 5 (n) Language difficulties in dealing with patients 1 2 3 4 5 (o) AIDS patients 1 2 3 4 5 Environment related (p) Unsanitary/unhygienic conditions 1 2 3 4 5 (q) Poor maintenance of buildings 1 2 3 4 5 (r) Lack of safety 1 2 3 4 5 (s) Vandalism 1 2 3 4 5

114
SECTION D: SUGGESTIONS FOR IMPROVEMENT 20. What suggestions do you have for improving the functioning of CHBH in respect of the following?
(a) Resource management (medicine, linen, equipment. etc.): ��������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(b) Staff relations: ����������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(c) Staff-patient relations .��������������������������.��
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(d) General and clinical misconduct: ���������������������.�.,,�
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(e) Safety and security: ��������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(f) Service quality: ��������������������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

115
(g) Admission and discharge of patients
��������������..��������.������������������.
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� SECTION E: DEMOGRAPHICS 21. Gender:
Male 1 Female 2
22. Age:
20 years and younger 1 21-30 years 2 31-40 years 3 41-50 years 4 51-60 years 5 Older than 60 years 6
23. Home language: ��������������������������������.. 24. Highest formal qualification obtained: ������������������������ 25. How long have you been an employee at CHBH? �������� (years) 26. How many years working experience do you have in total? ��.����� (years) 27. Is there anything else that you would like to raise? Anything not covered by this questionnaire or
maybe something about the questionnaire itself?
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
THANK YOU VERY MUCH FOR YOUR CO-OPERATION!

116

117
APPENDIX 3 QUESTIONNAIRE: DOCTORS © EthicSA 2001

118
QUESTIONNAIRE FOR DOCTORS SECTION A: ORGANISATIONAL ISSUES Organisational culture 1. Interpersonal relations (i.e. how people behave or act towards each other when they are together)
can be rated on various dimensions. For each pair of adjectives below, please circle the number that, in your view, best characterises interpersonal relations among staff at CHBH in general. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that relations among staff are totally honest, you will circle a 1; if you believe that it is totally dishonest, you will circle a 7. If you believe that it is only somewhat dishonest, you will circle a 5.) PLEASE COMPLETE THE FOLLOWING: (a) Honest 1 2 3 4 5 6 7 Dishonest (b) Respectful 1 2 3 4 5 6 7 Disrespectful (c) Loyal 1 2 3 4 5 6 7 Disloyal (d) Trusting 1 2 3 4 5 6 7 Distrusting (e) Professional 1 2 3 4 5 6 7 Unprofessional (f) Relaxed 1 2 3 4 5 6 7 Tense and stressed
2. Below is a list of six organisational values. Please rate how much CHBH cares about each right now:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Serving the greatest number of patients as possible 1 2 3 4 5 (b) Avoiding bad publicity 1 2 3 4 5 (c) Not having strikes and social unrest 1 2 3 4 5 (d) Good work ethic 1 2 3 4 5 (e) Balancing the books 1 2 3 4 5 (f) Providing the best possible working environment 1 2 3 4 5
3. Below is a list of four professional values in service delivery to patients. To what extent are they practiced at CHBH? In each case distinguish between how much your fellow doctors and nurses respectively give expression to these values V
ery
grea
t ex
tent
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Doctors 1 2 3 4 5 (a) Compassion for patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (b) Confidentiality of patient information Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (c) Respect for dignity of patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (d) Respect for well-being of patients Nurses 1 2 3 4 5

119
Leadership and management
4. Please rate how much you agree or disagree with the following statements concerning leadership and management practices at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) The hospital management takes suggestions from below seriously. 1 2 3 4
(b) There are proper incentives in place to improve staff performance. 1 2 3 4
(c) Staff members have a say in matters of decision-making. 1 2 3 4 (d) The hospital management is clear about the career
prospects of employees. 1 2 3 4
(e) Top management has no secrets from employees. 1 2 3 4 (f) Management at CHBH is basically powerless. 1 2 3 4
Channels of communication 5. Please rate how much you agree or disagree with the following statements concerning communication practices at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) Employees are not allowed to say what they really think. 1 2 3 4 (b) Clear guidelines exist regarding staff members�
responsibilities. 1 2 3 4
(c) My supervisor effectively follows up on complaints that I direct via him/her. 1 2 3 4
(d) My supervisor regularly gives me feedback about my performance. 1 2 3 4
(e) I am always last to be informed about decisions that concern my work. 1 2 3 4
(f) There is a system in place that employees can use to report instances of misconduct without being victimised. 1 2 3 4
(g) Rumour (the �grapevine�) is a common source of information at CHBH.
1 2 3 4
Resources 6(a). Do you experience an under-supply of medicine at CHBH?
Yes 1 No 2 Don�t know 3
6(b) If Yes, to what extent do the following contribute to the under-supply of medicine at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Over-ordering of medicines by ward sisters 1 2 3 4 5 (b) Theft of medicines from hospital stocks by staff 1 2 3 4 5 (c) Influx of non-South African patients 1 2 3 4 5 (d) HIV/AIDS pandemic 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5 (f) Other 1 2 3 4 5 (Please specify:�������������.� ��������������������.

120
7(a). Do you experience a general shortage of linen at CHBH?
Yes 1 No 2 Don�t know 3
7(b). If Yes, to what extent do the following contribute tothe linen shortages at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Stealing of linen by hospital staff 1 2 3 4 5 (b) Linen theft committed by patients 1 2 3 4 5 (c) Increased patient population related to the
HIV/AIDS pandemic 1 2 3 4 5
(d) Ineffective logistical and practical arrangements 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5
(f) Other: (Please specify:���������.�
��������������������.
1 2 3 4 5
Job satisfaction
8. Some jobs are more interesting and satisfying than others. We want to know how you feel about your job. For each of the following statements please circle one of the alternatives which best describes your opinion. St
rong
ly
agre
e
Ten
d to
agr
ee
Ten
d to
di
sagr
ee
Stro
ngly
disa
gree
(a) I am often bored with my job. 1 2 3 4 (b) I am satisfied with my job for the time being. 1 2 3 4 (c) Each day of work seems like it will never end. 1 2 3 4 (d) I find real enjoyment in my work. 1 2 3 4 (e) It feels as if I am working in a �second-class� hospital. 1 2 3 4 (f) I feel proud to be associated with CHBH. 1 2 3 4 (g) My opinion of myself increases when I do my job well. 1 2 3 4 (h) I frequently think of quitting my job. 1 2 3 4
9. Overall, how satisfied are you with each of the following?
Ver
y sa
tisfie
d
Qui
te
satis
fied
Som
ewha
t sa
tisfie
d
Qui
te
diss
atis
fied
Ver
y
diss
atis
fied
(a) Your immediate supervisor? 1 2 3 4 5 (b) Your salary? 1 2 3 4 5 (c) Cooperativeness of colleagues? 1 2 3 4 5 (d) Your conditions of service? 1 2 3 4 5 (e) Your workload? 1 2 3 4 5 (f) Your career progress at CHBH thus far? 1 2 3 4 5 (g) Your prospects for promotion? 1 2 3 4 5

121
Physical environment 10. On a scale of 1 to 7, how do you rate the physical environment at CHBH in terms of the following
dimensions? (The closer a number to a value, the more that value represents your experience. For instance, if you believe that CHBH is very clean, you will circle a 1; if you believe that it is very dirty, you will circle a 7. If you believe that it is somewhat dirty, you will circle a 5.)
(a) Clean 1 2 3 4 5 6 7 Dirty (b) Safe 1 2 3 4 5 6 7 Unsafe (c) Attractive 1 2 3 4 5 6 7 Unattractive (d) Depressing 1 2 3 4 5 6 7 Cheerful
11. Please rate how much you agree or disagree with the following statements concerning security and safety at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The security screening of visitors leaves much to be desired. 1 2 3 4 5
(b) The unsafe environment at CHBH can be related to the influx of non-South African patients. 1 2 3 4 5
(c) The number of security staff at CHBH is sufficient to combat crime. 1 2 3 4 5
(d) Security staff at CHBH is well equipped with the necessary skills and facilities to combat crime. 1 2 3 4 5
(e) The security screening of applicants for employment leaves much to be desired. 1 2 3 4 5
(f) It is the responsibility of government to ensure a safe environment at CHBH. 1 2 3 4 5
Labour unions 12. (a) Do you think it is useful to have unions operating within the hospital?
Yes � unions are useful in every aspect 1 Yes and no � unions are useful in some ways but problematic in others 2 No � unions are not useful at all 3
(b) Please give a reason for your answer to Question 17(b):
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� 13. In your view, to what extent do the unions influence the decisions made at CHBH?
Very great extent 1 Great extent 2 Moderate extent 3 To some extent 4 Very little extent 5

122
14. Please rate how much you agree or disagree with the following statements concerning labour unions at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The unions at CHBH serve to enhance discipline. 1 2 3 4 5 (b) I am under pressure to support union decisions
although I don�t want to. 1 2 3 4 5
SECTION B: MISCONDUCT AND STANDARDS OF CARE
15. During the past year, how often have you witnessed the following happening at CHBH?
Onc
e
Tw
ice
Thr
ee
times
or
mor
e
Nev
er
No
opin
ion
(a) Over-ordering of medicine 1 2 3 4 5 (b) Patients/visitors bribing staff 1 2 3 4 5 (c) Moonlighting by staff 1 2 3 4 5 (d) Staff verbally abusing patients 1 2 3 4 5 (e) Staff physically abusing patients 1 2 3 4 5 (f) Patients verbally abusing staff 1 2 3 4 5 (g) Patients physically abusing staff 1 2 3 4 5 (h) Lack of informed consent 1 2 3 4 5 (i) Breach of confidentiality of patient information 1 2 3 4 5 (j) Lack of compassion for patients 1 2 3 4 5 (k) Special groups of patients getting different levels of care
(TOP, AIDS, Aliens, Pregnant women, TB, Teenage pregnancy)
1 2 3 4 5
(l) Professional negligence in patient care 1 2 3 4 5 (m) Substandard postoperative care 1 2 3 4 5
16. Please rate how much you agree or disagree with the following statements:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) Payment to employees at CHBH by patients or their family for services or treatment given is fraud. 1 2 3 4 5
(b) Employees who engage in threatening or violent behaviour on the job are seldom subjected to immediate disciplinary action.
1 2 3 4 5
(c) Misconduct at CHBH relates mainly to lack of discipline.
1 2 3 4 5
(d) Disciplinary measures at CHBH are not �visible�. 1 2 3 4 5 (e) Health professionals at CHBH do not have sufficient
time to treat patients with the necessary compassion and understanding.
1 2 3 4 5
(f) Language barriers make it difficult for health care professionals to convey to patients proper information about their diagnosis and treatment.
1 2 3 4 5
(g) Because of the heavy workload at CHBH it is fair for employees to ask for small incentives (�tips�) for services.
1 2 3 4 5
(h) A hospital ethics committee would assist in guiding health professional conduct. 1 2 3 4 5

123
SECTION C: PROBLEMS AND SOURCES OF STRESS
17. Please rate the extent to which you consider the following as a problem or source of stress at CHBH:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Resource related (a) Poor/outdated equipment 1 2 3 4 5 (b) Not enough medicine 1 2 3 4 5 (c) Linen shortage 1 2 3 4 5 Staff related (d) Poor remuneration 1 2 3 4 5 (e) Long shifts 1 2 3 4 5 (f) Night duty 1 2 3 4 5 (g) General shortage of staff 1 2 3 4 5 (h) Poor staff communication 1 2 3 4 5 (i) Supervision/issues of authority 1 2 3 4 5 Patient related (j) Patients with low levels of schooling 1 2 3 4 5 (k) Long-stay patients 1 2 3 4 5 (l) Impossible/demanding patients 1 2 3 4 5 (m) Substandard care because of large numbers 1 2 3 4 5 (n) Language difficulties in dealing with patients 1 2 3 4 5 (o) AIDS patients 1 2 3 4 5 Environment related (p) Unsanitary/unhygienic conditions 1 2 3 4 5 (q) Poor maintenance of buildings 1 2 3 4 5 (r) Lack of safety 1 2 3 4 5 (s) Vandalism 1 2 3 4 5
SECTION D: SUGGESTIONS FOR IMPROVEMENT 18. What suggestions do you have for improving the functioning of CHBH in respect of the following
(where applicable to you)?
(a) Resource management (medicine, linen, equipment. etc.): ��������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(b) Staff relations: ����������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

124
(c) Staff-patient relations .�������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(d) General and clinical misconduct: ���������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(e) Safety and security: ��������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(f) Service quality: ��������������������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(g) Admission and discharge of patients: �����������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

125
SECTION E: DEMOGRAPHICS 19. Gender:
Male 1 Female 2
20. Age:
20 years and younger 1 21-30 years 2 31-40 years 3 41-50 years 4 51-60 years 5 Older than 60 years 6
21. Home language: ��������������������������������.. 22. Highest formal qualification obtained: ������������������������ 23. How long have you been an employee at CHBH? �������� (years) 24. How many years working experience do you have in total? ��.����� (years) 25. Is there anything else that you would like to raise? Anything not covered by this questionnaire or
maybe something about the questionnaire itself?
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
THANK YOU VERY MUCH FOR YOUR COOPERATION!

126

127
APPENDIX 4 QUESTIONNAIRE: ALLIED HEALTH PROFESSIONALS © EthicSA 2001

128
QUESTIONNAIRE FOR ALLIED HEALTH PROFESSIONALS SECTION A: ORGANISATIONAL ISSUES Organisational culture 1. Interpersonal relations (i.e. how people behave or act towards each other when they are together)
can be rated on various dimensions. For each pair of adjectives below, please circle the number that, in your view, best characterises interpersonal relations among staff at CHBH in general. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that relations among staff are totally honest, you will circle a 1; if you believe that it is totally dishonest, you will circle a 7. If you believe that it is only somewhat dishonest, you will circle a 5.) PLEASE COMPLETE THE FOLLOWING: (a) Honest 1 2 3 4 5 6 7 Dishonest (b) Respectful 1 2 3 4 5 6 7 Disrespectful (c) Loyal 1 2 3 4 5 6 7 Disloyal (d) Trusting 1 2 3 4 5 6 7 Distrusting (e) Professional 1 2 3 4 5 6 7 Unprofessional (f) Relaxed 1 2 3 4 5 6 7 Tense and stressed
2. Below is a list of six organisational values. Please rate how much CHBH cares about each right now:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Serving the greatest number of patients as possible 1 2 3 4 5 (b) Avoiding bad publicity 1 2 3 4 5 (c) Not having strikes and social unrest 1 2 3 4 5 (d) Good work ethic 1 2 3 4 5 (e) Balancing the books 1 2 3 4 5 (f) Providing the best possible working environment 1 2 3 4 5
3. Below is a list of four professional values in service delivery to patients. To what extent are they practiced at CHBH? In each case distinguish between how much doctors and nurses respectively give expression to these values V
ery
grea
t ex
tent
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Doctors 1 2 3 4 5 (a) Compassion for patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (b) Confidentiality of patient information Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (c) Respect for dignity of patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (d) Respect for well-being of patients Nurses 1 2 3 4 5
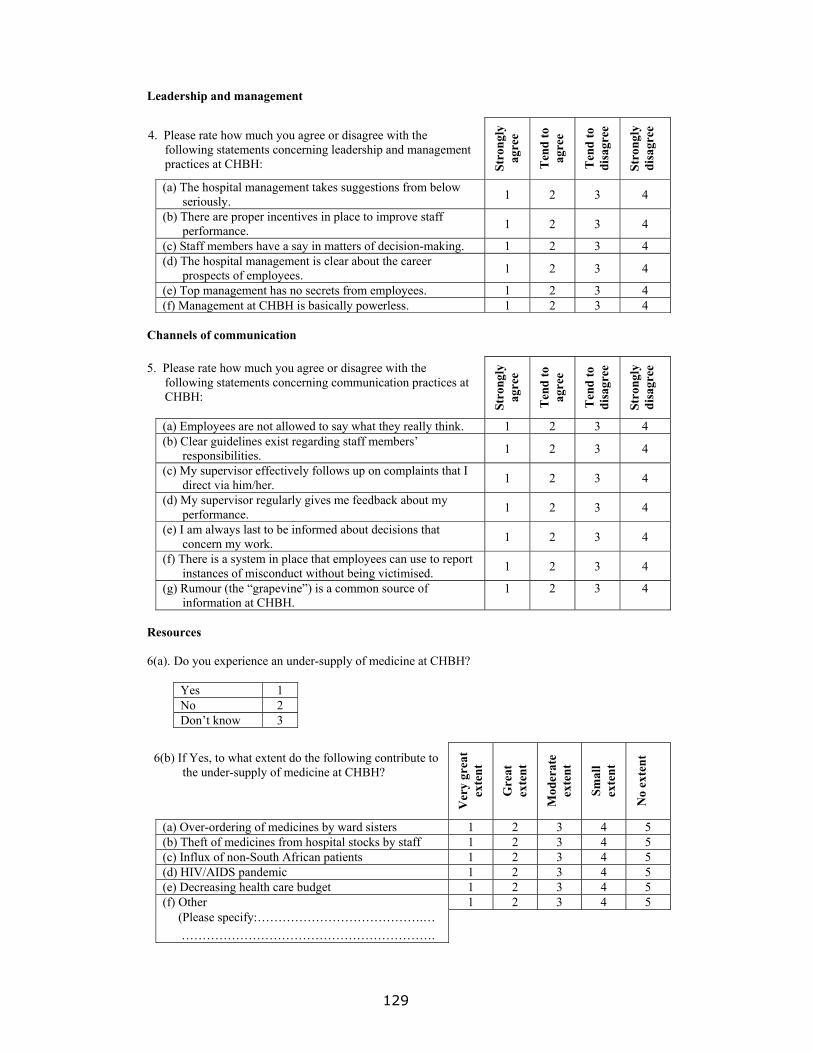
129
Leadership and management
4. Please rate how much you agree or disagree with the following statements concerning leadership and management practices at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) The hospital management takes suggestions from below seriously. 1 2 3 4
(b) There are proper incentives in place to improve staff performance. 1 2 3 4
(c) Staff members have a say in matters of decision-making. 1 2 3 4 (d) The hospital management is clear about the career
prospects of employees. 1 2 3 4
(e) Top management has no secrets from employees. 1 2 3 4 (f) Management at CHBH is basically powerless. 1 2 3 4
Channels of communication 5. Please rate how much you agree or disagree with the
following statements concerning communication practices at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) Employees are not allowed to say what they really think. 1 2 3 4 (b) Clear guidelines exist regarding staff members�
responsibilities. 1 2 3 4
(c) My supervisor effectively follows up on complaints that I direct via him/her. 1 2 3 4
(d) My supervisor regularly gives me feedback about my performance. 1 2 3 4
(e) I am always last to be informed about decisions that concern my work. 1 2 3 4
(f) There is a system in place that employees can use to report instances of misconduct without being victimised. 1 2 3 4
(g) Rumour (the �grapevine�) is a common source of information at CHBH.
1 2 3 4
Resources 6(a). Do you experience an under-supply of medicine at CHBH?
Yes 1 No 2 Don�t know 3
6(b) If Yes, to what extent do the following contribute to the under-supply of medicine at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
Smal
l ex
tent
No
exte
nt
(a) Over-ordering of medicines by ward sisters 1 2 3 4 5 (b) Theft of medicines from hospital stocks by staff 1 2 3 4 5 (c) Influx of non-South African patients 1 2 3 4 5 (d) HIV/AIDS pandemic 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5 (f) Other 1 2 3 4 5 (Please specify:�������������.� ��������������������.

130
7(a). Do you experience a general shortage of linen at CHBH?
Yes 1 No 2 Don�t know 3
7(b). If Yes, to what extent do the following contribute tothe linen shortages at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Stealing of linen by hospital staff 1 2 3 4 5 (b) Linen theft committed by patients 1 2 3 4 5 (c) Increased patient population related to the
HIV/AIDS pandemic 1 2 3 4 5
(d) Ineffective logistical and practical arrangements 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5
(f) Other (Please specify:����������.�
�.��������������������.
1 2 3 4 5
Job satisfaction
8. Some jobs are more interesting and satisfying than others. We want to know how you feel about your job. For each of the following statements please circle one of the alternatives which best describes your opinion. St
rong
ly
agre
e
Ten
d to
agr
ee
Ten
d to
di
sagr
ee
Stro
ngly
disa
gree
(a) I am often bored with my job. 1 2 3 4 (b) I am satisfied with my job for the time being. 1 2 3 4 (c) Each day of work seems like it will never end. 1 2 3 4 (d) I find real enjoyment in my work. 1 2 3 4 (e) It feels as if I am working in a �second-class� hospital. 1 2 3 4 (f) I feel proud to be associated with CHBH. 1 2 3 4 (g) My opinion of myself increases when I do my job well. 1 2 3 4 (h) I frequently think of quitting my job. 1 2 3 4
9. Overall, how satisfied are you with each of the following?
Ver
y sa
tisfie
d
Qui
te
satis
fied
Som
ewha
t sa
tisfie
d
Qui
te
diss
atis
fied
Ver
y
diss
atis
fied
(a) Your immediate supervisor? 1 2 3 4 5 (b) Your salary? 1 2 3 4 5 (c) Cooperativeness of colleagues? 1 2 3 4 5 (d) Your conditions of service? 1 2 3 4 5 (e) Your workload? 1 2 3 4 5 (f) Your career progress at CHBH thus far? 1 2 3 4 5 (g) Your prospects for promotion? 1 2 3 4 5

131
Physical environment 10. On a scale of 1 to 7, how do you rate the physical environment at CHBH in terms of the following
dimensions? (The closer a number to a value, the more that value represents your experience. For instance, if you believe that CHBH is very clean, you will circle a 1; if you believe that it is very dirty, you will circle a 7. If you believe that it is somewhat dirty, you will circle a 5.)
(a) Clean 1 2 3 4 5 6 7 Dirty (b) Safe 1 2 3 4 5 6 7 Unsafe (c) Attractive 1 2 3 4 5 6 7 Unattractive (d) Depressing 1 2 3 4 5 6 7 Cheerful
11. Please rate how much you agree or disagree with the following statements concerning security and safety at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The security screening of visitors leaves much to be desired. 1 2 3 4 5
(b) The unsafe environment at CHBH can be related to the influx of non-South African patients. 1 2 3 4 5
(c) The number of security staff at CHBH is sufficient to combat crime. 1 2 3 4 5
(d) Security staff at CHBH is well equipped with the necessary skills and facilities to combat crime. 1 2 3 4 5
(e) The security screening of applicants for employment leaves much to be desired. 1 2 3 4 5
(f) It is the responsibility of government to ensure a safe environment at CHBH. 1 2 3 4 5
Labour unions 12. (a) Do you think it is useful to have unions operating within the hospital?
Yes � unions are useful in every aspect 1 Yes and no � unions are useful in some ways but problematic in others 2 No � unions are not useful at all 3
(b) Please give a reason for your answer to Question 17(b):
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� 13. In your view, to what extent do the unions influence the decisions made at CHBH?
Very great extent 1 Great extent 2 Moderate extent 3 To some extent 4 Very little extent 5

132
14. Please rate how much you agree or disagree with the following statements concerning labour unions at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The unions at CHBH serve to enhance discipline. 1 2 3 4 5 (b) I am under pressure to support union decisions
although I don�t want to. 1 2 3 4 5
SECTION B: MISCONDUCT AND STANDARDS OF CARE
15. During the past year, how often have you witnessed the following happening at CHBH?
Onc
e
Tw
ice
Thr
ee
times
or
mor
e
Nev
er
No
opin
ion
(a) Over-ordering of medicine 1 2 3 4 5 (b) Patients/visitors bribing staff 1 2 3 4 5 (c) Moonlighting by staff 1 2 3 4 5 (d) Staff verbally abusing patients 1 2 3 4 5 (e) Staff physically abusing patients 1 2 3 4 5 (f) Patients verbally abusing staff 1 2 3 4 5 (g) Patients physically abusing staff 1 2 3 4 5 (h) Lack of informed consent 1 2 3 4 5 (i) Breach of confidentiality of patient information 1 2 3 4 5 (j) Lack of compassion for patients 1 2 3 4 5 (k) Special groups of patients getting different levels of care
(TOP, AIDS, Aliens, Pregnant women, TB, Teenage pregnancy)
1 2 3 4 5
(l) Professional negligence in patient care 1 2 3 4 5 (m) Substandard postoperative care 1 2 3 4 5
16. Please rate how much you agree or disagree with the following statements:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) Payment to employees at CHBH by patients or their family for services or treatment given is fraud. 1 2 3 4 5
(b) Employees who engage in threatening or violent behaviour on the job are seldom subjected to immediate disciplinary action.
1 2 3 4 5
(c) Misconduct at CHBH relates mainly to lack of discipline. 1 2 3 4 5 (d) Disciplinary measures at CHBH are not �visible�. 1 2 3 4 5 (e) Health professionals at CHBH do not have sufficient time
to treat patients with the necessary compassion and understanding.
1 2 3 4 5
(f) Language barriers make it difficult for health care professionals to convey to patients proper information about their diagnosis and treatment.
1 2 3 4 5
(g) Because of the heavy workload at CHBH it is fair for employees to ask for small incentives (�tips�) for services.
1 2 3 4 5
(h) A hospital ethics committee would assist in guiding health professional conduct. 1 2 3 4 5
133
SECTION C: PROBLEMS AND SOURCES OF STRESS
17. Please rate the extent to which you consider the following as a problem or source of stress at CHBH:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Resource related (a) Poor/outdated equipment 1 2 3 4 5 (b) Not enough medicine 1 2 3 4 5 (c) Linen shortage 1 2 3 4 5 Staff related (d) Poor remuneration 1 2 3 4 5 (e) Long shifts 1 2 3 4 5 (f) Night duty 1 2 3 4 5 (g) General shortage of staff 1 2 3 4 5 (h) Poor staff communication 1 2 3 4 5 (i) Supervision/issues of authority 1 2 3 4 5 Patient related (j) Patients with low levels of schooling 1 2 3 4 5 (k) Long-stay patients 1 2 3 4 5 (l) Impossible/demanding patients 1 2 3 4 5 (m) Substandard care because of large numbers 1 2 3 4 5 (n) Language difficulties in dealing with patients 1 2 3 4 5 (o) AIDS patients 1 2 3 4 5 Environment related (p) Unsanitary/unhygienic conditions 1 2 3 4 5 (q) Poor maintenance of buildings 1 2 3 4 5 (r) Lack of safety 1 2 3 4 5 (s) Vandalism 1 2 3 4 5
SECTION D: SUGGESTIONS FOR IMPROVEMENT 18. What suggestions do you have for improving the functioning of CHBH in respect of the following?
(a) Resource management (medicine, linen, equipment. etc.): ��������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(b) Staff relations: �������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

134
(c) Staff-patient relations .�������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(d) General and clinical misconduct: ����������������������.��
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(e) Safety and security: ��������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(f) Service quality: ��������������������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(g) Admission and discharge of patients: ���������..�������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

135
SECTION E: DEMOGRAPHICS 19. Gender:
Male 1 Female 2
20. Age:
20 years and younger 1 21-30 years 2 31-40 years 3 41-50 years 4 51-60 years 5 Older than 60 years 6
21. Home language: ��������������������������������.. 22. Highest formal qualification obtained: ������������������������ 23. Hospital section/division: ����������������������������� 24. Do you belong to a labour union?
Yes 1 No 2
25. How long have you been an employee at CHBH? �������� (years) 26. How many years working experience do you have in total? ��.����� (years) 27. Is there anything else that you would like to raise? Anything not covered by this questionnaire or
maybe something about the questionnaire itself?
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
THANK YOU VERY MUCH FOR YOUR COOPERATION!

136

137
APPENDIX 5 QUESTIONNAIRE: NURSES © EthicSA 2001

138
QUESTIONNAIRE FOR NURSES SECTION A: ORGANISATIONAL ISSUES Organisational culture 1. Interpersonal relations (i.e. how people behave or act towards each other when they are together)
can be rated on various dimensions. For each pair of adjectives below, please circle the number that, in your view, best characterises interpersonal relations among staff at CHBH in general. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that relations among staff are totally honest, you will circle a 1; if you believe that it is totally dishonest, you will circle a 7. If you believe that it is only somewhat dishonest, you will circle a 5.) PLEASE COMPLETE THE FOLLOWING: (a) Honest 1 2 3 4 5 6 7 Dishonest (b) Respectful 1 2 3 4 5 6 7 Disrespectful (c) Loyal 1 2 3 4 5 6 7 Disloyal (d) Trusting 1 2 3 4 5 6 7 Distrusting (e) Professional 1 2 3 4 5 6 7 Unprofessional (f) Relaxed 1 2 3 4 5 6 7 Tense and stressed
2. Below is a list of six organisational values. Please rate how much CHBH cares about each right now:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Serving the greatest number of patients as possible 1 2 3 4 5 (b) Avoiding bad publicity 1 2 3 4 5 (c) Not having strikes and social unrest 1 2 3 4 5 (d) Good work ethic 1 2 3 4 5 (e) Balancing the books 1 2 3 4 5 (f) Providing the best possible working environment 1 2 3 4 5
3. Below is a list of four professional values in service delivery to patients. To what extent are they practiced at CHBH? In each case distinguish between how much the doctors and your fellow nurses respectively give expression to these values V
ery
grea
t ex
tent
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Doctors 1 2 3 4 5 (a) Compassion for patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (b) Confidentiality of patient information Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (c) Respect for dignity of patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (d) Respect for well-being of patients Nurses 1 2 3 4 5

139
Leadership and management
4. Please rate how much you agree or disagree with the following statements concerning leadership and management practices at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) The hospital management takes suggestions from below seriously. 1 2 3 4
(b) There are proper incentives in place to improve staff performance. 1 2 3 4
(c) Staff members have a say in matters of decision-making. 1 2 3 4 (d) The hospital management is clear about the career
prospects of employees. 1 2 3 4
(e) Top management has no secrets from employees. 1 2 3 4 (f) Management at CHBH is basically powerless. 1 2 3 4
Channels of communication 5. Please rate how much you agree or disagree with the following statements concerning communication practices at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) Employees are not allowed to say what they really think. 1 2 3 4 (b) Clear guidelines exist regarding staff members�
responsibilities. 1 2 3 4
(c) My supervisor effectively follows up on complaints that I direct via him/her. 1 2 3 4
(d) My supervisor regularly gives me feedback about my performance. 1 2 3 4
(e) I am always last to be informed about decisions that concern my work. 1 2 3 4
(f) There is a system in place that employees can use to report instances of misconduct without being victimised. 1 2 3 4
(g) Rumour (the �grapevine�) is a common source of information at CHBH.
1 2 3 4
Resources 6(a). Do you experience an under-supply of medicine at CHBH?
Yes 1 No 2 Don�t know 3
6(b) If Yes, to what extent do the following contribute to the under-supply of medicine at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Over-ordering of medicines by ward sisters 1 2 3 4 5 (b) Theft of medicines from hospital stocks by staff 1 2 3 4 5 (c) Influx of non-South African patients 1 2 3 4 5 (d) HIV/AIDS pandemic 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5 (f) Other 1 2 3 4 5 (Please specify:�������������.� ��������������������.

140
7(a). Do you experience a general shortage of linen at CHBH?
Yes 1 No 2 Don�t know 3
7(b). If Yes, to what extent do the following contribute tothe linen shortages at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Stealing of linen by hospital staff 1 2 3 4 5 (b) Linen theft committed by patients 1 2 3 4 5 (c) Increased patient population related to the
HIV/AIDS pandemic 1 2 3 4 5
(d) Ineffective logistical and practical arrangements 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5
(f) Other (Please specify:����������.�
�.��������������������.
1 2 3 4 5
Job satisfaction
8. Some jobs are more interesting and satisfying than others. We want to know how you feel about your job. For each of the following statements please circle one of the alternatives which best describes your opinion. St
rong
ly
agre
e
Ten
d to
agr
ee
Ten
d to
di
sagr
ee
Stro
ngly
disa
gree
(a) I am often bored with my job. 1 2 3 4 (b) I am satisfied with my job for the time being. 1 2 3 4 (c) Each day of work seems like it will never end. 1 2 3 4 (d) I find real enjoyment in my work. 1 2 3 4 (e) It feels as if I am working in a �second-class� hospital. 1 2 3 4 (f) I feel proud to be associated with CHBH. 1 2 3 4 (g) My opinion of myself increases when I do my job well. 1 2 3 4 (h) I frequently think of quitting my job. 1 2 3 4
9. Overall, how satisfied are you with each of the following?
Ver
y sa
tisfie
d
Qui
te
satis
fied
Som
ewha
t sa
tisfie
d
Qui
te
diss
atis
fied
Ver
y
diss
atis
fied
(a) Your immediate supervisor? 1 2 3 4 5 (b) Your salary? 1 2 3 4 5 (c) Cooperativeness of colleagues? 1 2 3 4 5 (d) Your conditions of service? 1 2 3 4 5 (e) Your workload? 1 2 3 4 5 (f) Your career progress at CHBH thus far? 1 2 3 4 5 (g) Your prospects for promotion? 1 2 3 4 5

141
Physical environment 10. On a scale of 1 to 7, how do you rate the physical environment at CHBH in terms of the following
dimensions? (The closer a number to a value, the more that value represents your experience. For instance, if you believe that CHBH is very clean, you will circle a 1; if you believe that it is very dirty, you will circle a 7. If you believe that it is somewhat dirty, you will circle a 5.)
(a) Clean 1 2 3 4 5 6 7 Dirty (b) Safe 1 2 3 4 5 6 7 Unsafe (c) Attractive 1 2 3 4 5 6 7 Unattractive (d) Depressing 1 2 3 4 5 6 7 Cheerful
11. Please rate how much you agree or disagree with the following statements concerning security and safety at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The security screening of visitors leaves much to be desired. 1 2 3 4 5
(b) The unsafe environment at CHBH can be related to the influx of non-South African patients. 1 2 3 4 5
(c) The number of security staff at CHBH is sufficient to combat crime. 1 2 3 4 5
(d) Security staff at CHBH is well equipped with the necessary skills and facilities to combat crime. 1 2 3 4 5
(e) The security screening of applicants for employment leaves much to be desired. 1 2 3 4 5
(f) It is the responsibility of government to ensure a safe environment at CHBH. 1 2 3 4 5
Labour unions 12. (a) Do you think it is useful to have unions operating within the hospital?
Yes � unions are useful in every aspect 1 Yes and no � unions are useful in some ways but problematic in others 2 No � unions are not useful at all 3
(b) Please give a reason for your answer to Question 17(b):
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� 13. In your view, to what extent do the unions influence the decisions made at CHBH?
Very great extent 1 Great extent 2 Moderate extent 3 To some extent 4 Very little extent 5

142
14. Please rate how much you agree or disagree with the following statements concerning labour unions at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The unions at CHBH serve to enhance discipline. 1 2 3 4 5 (b) I am under pressure to support union decisions although
I don�t want to. 1 2 3 4 5
SECTION B: MISCONDUCT AND STANDARDS OF CARE
15. During the past year, how often have you witnessed the following happening at CHBH?
Onc
e
Tw
ice
Thr
ee
times
or
mor
e
Nev
er
No
opin
ion
(a) Over-ordering of medicine 1 2 3 4 5 (b) Patients/visitors bribing staff 1 2 3 4 5 (c) Moonlighting by staff 1 2 3 4 5 (d) Staff verbally abusing patients 1 2 3 4 5 (e) Staff physically abusing patients 1 2 3 4 5 (f) Patients verbally abusing staff 1 2 3 4 5 (g) Patients physically abusing staff 1 2 3 4 5 (h) Lack of informed consent 1 2 3 4 5 (i) Breach of confidentiality of patient information 1 2 3 4 5 (j) Lack of compassion for patients 1 2 3 4 5 (k) Special groups of patients getting different levels of
care (TOP, AIDS, Aliens, Pregnant women, TB, Teenage pregnancy)
1 2 3 4 5
(l) Professional negligence in patient care 1 2 3 4 5 (m) Substandard postoperative care 1 2 3 4 5
16. Please rate how much you agree or disagree with the following statements:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) Payment to employees at CHBH by patients or their family for services or treatment given is fraud. 1 2 3 4 5
(b) Employees who engage in threatening or violent behaviour on the job are seldom subjected to immediate disciplinary action.
1 2 3 4 5
(c) Misconduct at CHBH relates mainly to lack of discipline. 1 2 3 4 5 (d) Disciplinary measures at CHBH are not �visible�. 1 2 3 4 5 (e) Health professionals at CHBH do not have sufficient time
to treat patients with the necessary compassion and understanding.
1 2 3 4 5
(f) Language barriers make it difficult for health care professionals to convey to patients proper information about their diagnosis and treatment.
1 2 3 4 5
(g) Because of the heavy workload at CHBH it is fair for employees to ask for small incentives (�tips�) for services.
1 2 3 4 5
(h) A hospital ethics committee would assist in guiding health professional conduct. 1 2 3 4 5

143
SECTION C: PROBLEMS AND SOURCES OF STRESS
17. Please rate the extent to which you consider the following as a problem or source of stress at CHBH:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Resource related (a) Poor/outdated equipment 1 2 3 4 5 (b) Not enough medicine 1 2 3 4 5 (c) Linen shortage 1 2 3 4 5 Staff related (d) Poor remuneration 1 2 3 4 5 (e) Long shifts 1 2 3 4 5 (f) Night duty 1 2 3 4 5 (g) General shortage of staff 1 2 3 4 5 (h) Poor staff communication 1 2 3 4 5 (i) Supervision/issues of authority 1 2 3 4 5 Patient related (j) Patients with low levels of schooling 1 2 3 4 5 (k) Long-stay patients 1 2 3 4 5 (l) Impossible/demanding patients 1 2 3 4 5 (m) Substandard care because of large numbers 1 2 3 4 5 (n) Language difficulties in dealing with patients 1 2 3 4 5 (o) AIDS patients 1 2 3 4 5 Environment related (p) Unsanitary/unhygienic conditions 1 2 3 4 5 (q) Poor maintenance of buildings 1 2 3 4 5 (r) Lack of safety 1 2 3 4 5 (s) Vandalism 1 2 3 4 5
SECTION D: SUGGESTIONS FOR IMPROVEMENT 18. What suggestions do you have for improving the functioning of CHBH in respect of the following?
(a) Resource management (medicine, linen, equipment. etc.): ��������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(b) Staff relations: ����������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

144
(c) Staff-patient relations .�������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(d) General and clinical misconduct: ���������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(e) Safety and security: ��������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(f) Service quality: ��������������������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(g) Admission and discharge of patients: �����������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

145
SECTION E: DEMOGRAPHICS 19. Gender:
Male 1 Female 2
20. Age:
20 years and younger 1 21-30 years 2 31-40 years 3 41-50 years 4 51-60 years 5 Older than 60 years 6
21. Home language: ��������������������������������.. 22. Highest formal qualification obtained: ������������������������ 23. Hospital section/division: ����������������������������� 24. Do you belong to a labour union?
Yes 1 No 2
25. How long have you been an employee at CHBH? �������� (years) 26. How many years working experience do you have in total? ��.����� (years) 27. Is there anything else that you would like to raise? Anything not covered by this questionnaire or
maybe something about the questionnaire itself?
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
THANK YOU VERY MUCH FOR YOUR COOPERATION!

146

147
APPENDIX 6 QUESTIONNAIRE: SUPPORT STAFF © EthicSA 2001

148
QUESTIONNAIRE FOR SUPPORT STAFF SECTION A: ORGANISATIONAL ISSUES Organisational culture 1. Interpersonal relations (i.e. how people behave or act towards each other when they are together)
can be rated on various dimensions. For each pair of adjectives below, please circle the number that, in your view, best characterises interpersonal relations among staff at CHBH. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that relations among staff are totally honest, you will circle a 1; if you believe that it is totally dishonest, you will circle a 7. If you believe that it is only somewhat dishonest, you will circle a 5.) PLEASE COMPLETE THE FOLLOWING: (a) Honest 1 2 3 4 5 6 7 Dishonest (b) Respectful 1 2 3 4 5 6 7 Disrespectful (c) Loyal 1 2 3 4 5 6 7 Disloyal (d) Trusting 1 2 3 4 5 6 7 Distrusting (e) Professional 1 2 3 4 5 6 7 Unprofessional (f) Relaxed 1 2 3 4 5 6 7 Tense and stressed
2. Below is a list of six organisational values. Please rate how much CHBH cares about each right now:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Serving the greatest number of patients as possible 1 2 3 4 5 (b) Avoiding bad publicity 1 2 3 4 5 (c) Not having strikes and social unrest 1 2 3 4 5 (d) Good work ethic 1 2 3 4 5 (e) Balancing the books 1 2 3 4 5 (f) Providing the best possible working environment 1 2 3 4 5
3. Below is a list of four professional values in service delivery to patients. To what extent are they practiced at CHBH? In each case distinguish between how much doctors and nurses respectively give expression to these values V
ery
grea
t ex
tent
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Doctors 1 2 3 4 5 (a) Compassion for patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (b) Confidentiality of patient information Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (c) Respect for dignity of patients Nurses 1 2 3 4 5
Doctors 1 2 3 4 5 (d) Respect for well-being of patients Nurses 1 2 3 4 5

149
Leadership and management
4. Please rate how much you agree or disagree with the following statements concerning leadership and management practices at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) The hospital management takes suggestions from below seriously. 1 2 3 4
(b) There are proper incentives in place to improve staff performance. 1 2 3 4
(c) Staff members have a say in matters of decision-making. 1 2 3 4 (d) The hospital management is clear about the career
prospects of employees. 1 2 3 4
(e) Top management has no secrets from employees. 1 2 3 4 (f) Management at CHBH is basically powerless. 1 2 3 4
Channels of communication 5. Please rate how much you agree or disagree with the
following statements concerning communication practices at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
(a) Employees are not allowed to say what they really think. 1 2 3 4 (b) Clear guidelines exist regarding staff members�
responsibilities. 1 2 3 4
(c) My supervisor effectively follows up on complaints that I direct via him/her. 1 2 3 4
(d) My supervisor regularly gives me feedback about my performance. 1 2 3 4
(e) I am always last to be informed about decisions that concern my work. 1 2 3 4
(f) There is a system in place that employees can use to report instances of misconduct without being victimised. 1 2 3 4
(g) Rumour (the �grapevine�) is a common source of information at CHBH.
1 2 3 4
Resources 6(a). Do you experience an under-supply of medicine at CHBH?
Yes 1 No 2 Don�t know 3
6(b) If Yes, to what extent do the following contribute to the under-supply of medicine at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Over-ordering of medicines by ward sisters 1 2 3 4 5 (b) Theft of medicines from hospital stocks by staff 1 2 3 4 5 (c) Influx of non-South African patients 1 2 3 4 5 (d) HIV/AIDS pandemic 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5
(f) Other (Please specify:����������.�
�.��������������������.
1 2 3 4 5

150
7(a). Do you experience a general shortage of linen at CHBH?
Yes 1 No 2 Don�t know 3
7(b). If Yes, to what extent do the following contribute tothe linen shortages at CHBH?
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
(a) Stealing of linen by hospital staff 1 2 3 4 5 (b) Linen theft committed by patients 1 2 3 4 5 (c) Increased patient population related to the
HIV/AIDS pandemic 1 2 3 4 5
(d) Ineffective logistical and practical arrangements 1 2 3 4 5 (e) Decreasing health care budget 1 2 3 4 5
(f) Other (Please specify:����������.�
�..��������������������.
1 2 3 4 5
Job satisfaction
8. Some jobs are more interesting and satisfying than others. We want to know how you feel about your job. For each of the following statements please circle one of the alternatives which best describes your opinion. St
rong
ly
agre
e
Ten
d to
agr
ee
Ten
d to
di
sagr
ee
Stro
ngly
disa
gree
(a) I am often bored with my job. 1 2 3 4 (b) I am satisfied with my job for the time being. 1 2 3 4 (c) Each day of work seems like it will never end. 1 2 3 4 (d) I find real enjoyment in my work. 1 2 3 4 (e) It feels as if I am working in a �second-class� hospital. 1 2 3 4 (f) I feel proud to be associated with CHBH. 1 2 3 4 (g) My opinion of myself increases when I do my job well. 1 2 3 4 (h) I frequently think of quitting my job. 1 2 3 4
9. Overall, how satisfied are you with each of the following?
Ver
y sa
tisfie
d
Qui
te
satis
fied
Som
ewha
t sa
tisfie
d
Qui
te
diss
atis
fied
Ver
y
diss
atis
fied
(a) Your immediate supervisor? 1 2 3 4 5 (b) Your salary? 1 2 3 4 5 (c) Cooperativeness of colleagues? 1 2 3 4 5 (d) Your conditions of service? 1 2 3 4 5 (e) Your workload? 1 2 3 4 5 (f) Your career progress at CHBH thus far? 1 2 3 4 5 (g) Your prospects for promotion? 1 2 3 4 5

151
Physical environment 10. On a scale of 1 to 7, how do you rate the physical environment at CHBH in terms of the following
dimensions? (The closer a number to a value, the more that value represents your experience. For instance, if you believe that CHBH is very clean, you will circle a 1; if you believe that it is very dirty, you will circle a 7. If you believe that it is somewhat dirty, you will circle a 5.)
(a) Clean 1 2 3 4 5 6 7 Dirty (b) Safe 1 2 3 4 5 6 7 Unsafe (c) Attractive 1 2 3 4 5 6 7 Unattractive (d) Depressing 1 2 3 4 5 6 7 Cheerful
11. Please rate how much you agree or disagree with the following statements concerning security and safety at CHBH:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The security screening of visitors leaves much to be desired. 1 2 3 4 5
(b) The unsafe environment at CHBH can be related to the influx of non-South African patients. 1 2 3 4 5
(c) The number of security staff at CHBH is sufficient to combat crime. 1 2 3 4 5
(d) Security staff at CHBH is well equipped with the necessary skills and facilities to combat crime. 1 2 3 4 5
(e) The security screening of applicants for employment leaves much to be desired. 1 2 3 4 5
(f) It is the responsibility of government to ensure a safe environment at CHBH. 1 2 3 4 5
Labour unions 12. (a) Do you think it is useful to have unions operating within the hospital?
Yes � unions are useful in every aspect 1 Yes and no � unions are useful in some ways but problematic in others 2 No � unions are not useful at all 3
(b) Please give a reason for your answer to Question 17(b):
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� 13. In your view, to what extent do the unions influence the decisions made at CHBH?
Very great extent 1 Great extent 2 Moderate extent 3 To some extent 4 Very little extent 5

152
14. Please rate how much you agree or disagree with the following statements concerning labour unions at CHBH: St
rong
ly
agre
e
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) The unions at CHBH serve to enhance discipline. 1 2 3 4 5 (b) I am under pressure to support union decisions
although I don�t want to. 1 2 3 4 5
SECTION B: MISCONDUCT AND STANDARDS OF CARE
15. During the past year, how often have you witnessed the following happening at CHBH?
Onc
e
Tw
ice
Thr
ee
times
or
mor
e
Nev
er
No
opin
ion
(a) Over-ordering of medicine 1 2 3 4 5 (b) Patients/visitors bribing staff 1 2 3 4 5 (c) Moonlighting by staff 1 2 3 4 5 (d) Staff verbally abusing patients 1 2 3 4 5 (e) Staff physically abusing patients 1 2 3 4 5 (f) Patients verbally abusing staff 1 2 3 4 5 (g) Patients physically abusing staff 1 2 3 4 5 (h) Lack of informed consent 1 2 3 4 5 (i) Breach of confidentiality of patient information 1 2 3 4 5 (j) Lack of compassion for patients 1 2 3 4 5 (k) Special groups of patients getting different levels of
care (TOP, AIDS, Aliens, Pregnant women, TB, Teenage pregnancy)
1 2 3 4 5
(l) Professional negligence in patient care 1 2 3 4 5 (m) Substandard postoperative care 1 2 3 4 5
16. Please rate how much you agree or disagree with the following statements:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) Payment to employees at CHBH by patients or their family for services or treatment given is fraud. 1 2 3 4 5
(b) Employees who engage in threatening or violent behaviour on the job are seldom subjected to immediate disciplinary action.
1 2 3 4 5
(c) Misconduct at CHBH relates mainly to lack of discipline.
1 2 3 4 5
(d) Disciplinary measures at CHBH are not �visible�. 1 2 3 4 5 (e) Health professionals at CHBH do not have sufficient
time to treat patients with the necessary compassion and understanding.
1 2 3 4 5
(f) Language barriers make it difficult for health care professionals to convey to patients proper information about their diagnosis and treatment.
1 2 3 4 5
(g) Because of the heavy workload at CHBH it is fair for employees to ask for small incentives (�tips�) for services.
1 2 3 4 5
(h) A hospital ethics committee would assist in guiding health professional conduct. 1 2 3 4 5

153
SECTION C: PROBLEMS AND SOURCES OF STRESS
17. Please rate the extent to which you consider the following as a problem or source of stress at CHBH:
Ver
y gr
eat
exte
nt
Gre
at
exte
nt
Mod
erat
e ex
tent
To
som
e ex
tent
Ver
y lit
tle
exte
nt
Resource related (a) Poor/outdated equipment 1 2 3 4 5 (b) Not enough medicine 1 2 3 4 5 (c) Linen shortage 1 2 3 4 5 Staff related (d) Poor remuneration 1 2 3 4 5 (e) Long shifts 1 2 3 4 5 (f) Night duty 1 2 3 4 5 (g) General shortage of staff 1 2 3 4 5 (h) Poor staff communication 1 2 3 4 5 (i) Supervision/issues of authority 1 2 3 4 5 Patient related (j) Patients with low levels of schooling 1 2 3 4 5 (k) Long-stay patients 1 2 3 4 5 (l) Impossible/demanding patients 1 2 3 4 5 (m) Substandard care because of large numbers 1 2 3 4 5 (n) Language difficulties in dealing with patients 1 2 3 4 5 (o) AIDS patients 1 2 3 4 5 Environment related (p) Unsanitary/unhygienic conditions 1 2 3 4 5 (q) Poor maintenance of buildings 1 2 3 4 5 (r) Lack of safety 1 2 3 4 5 (s) Vandalism 1 2 3 4 5
SECTION D: SUGGESTIONS FOR IMPROVEMENT 18. What suggestions do you have for improving the functioning of CHBH in respect of the following?
(a) Resource management (medicine, linen, equipment. etc.): ��������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(b) Staff relations: �����������������������������.��
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
154
(c) Staff-patient relations .�������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(d) General and clinical misconduct: ���������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(e) Safety and security: ���������������������������.��
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(f) Service quality: ��������������������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(g) Admission and discharge of patients: �����������������.�����
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������

155
SECTION E: DEMOGRAPHICS 19. Gender:
Male 1 Female 2
20. Age:
20 years and younger 1 21-30 years 2 31-40 years 3 41-50 years 4 51-60 years 5 Older than 60 years 6
21. Home language:
���������������������������������.. 22. Highest formal qualification obtained:
������������������������� 23. Hospital section/division:
������������������������������ 24. Do you belong to a labour union?
Yes 1 No 2
25. How long have you been an employee at CHBH? �������� (years) 26. How many years working experience do you have in total? ��.����� (years) 27. Is there anything else that you would like to raise? Anything not covered by this questionnaire or
maybe something about the questionnaire itself?
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
THANK YOU VERY MUCH FOR YOUR COOPERATION!

156

157
APPENDIX 7 QUESTIONNAIRE: PATIENTS © EthicSA 2001

158
QUESTIONNAIRE FOR PATIENTS SECTION A: QUALITY OF CARE 1. How would you describe the nurses� relationship towards you? For each pair of adjectives below,
please circle the number that, in your view, best characterises the nurses at CHBH. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that the nurses are totally honest, you will circle a 1; if you believe that they are totally dishonest, you will circle a 7. If you believe that they are only somewhat dishonest, you will circle a 5.) PLEASE COMPLETE THE FOLLOWING: (a) Respectful 1 2 3 4 5 6 7 Disrespectful (b) Professional 1 2 3 4 5 6 7 Unprofessional (c) Relaxed 1 2 3 4 5 6 7 Tense (d) Caring 1 2 3 4 5 6 7 Non-caring (e)Compassionate 1 2 3 4 5 6 7 Cold (f) Approachable 1 2 3 4 5 6 7 Unapproachable (g) Trusting 1 2 3 4 5 6 7 Distrusting
2. How would you describe the doctors� relationship towards you? For each pair of adjectives below,
please circle the number that, in your view, best characterises the doctors at CHBH. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that the doctors are totally disrespectful, you will circle a 1; if you believe that they are totally respectful, you will circle a 7. If you believe that they are only somewhat respectful, you will circle a 5.) (a) Disrespectful 1 2 3 4 5 6 7 Respectful (b) Professional 1 2 3 4 5 6 7 Unprofessional (c) Relaxed 1 2 3 4 5 6 7 Tense (d) Caring 1 2 3 4 5 6 7 Non-caring (e) Cold 1 2 3 4 5 6 7 Compassionate (f) Approachable 1 2 3 4 5 6 7 Unapproachable (g) Trusting 1 2 3 4 5 6 7 Distrusting
3. Overall, how satisfied are you with the following?
Ver
y sa
tisfie
d
Qui
te
satis
fied
Som
ewha
t sa
tisfie
d
Qui
te
diss
atis
fied
Ver
y
diss
atis
fied
(a) The assistance by the nurses on day duty? 1 2 3 4 5 (b) The assistance by the nurses on night duty? 1 2 3 4 5 (c) The quality of the medical treatment received? 1 2 3 4 5 (d) The linen on your bed? 1 2 3 4 5 (e) The quality of the food 1 2 3 4 5 (e) The room that you are in? 1 2 3 4 5

159
4. Being a patient at CHBH, how often have you experienced the
following?
Onc
e
Tw
ice
3 tim
es
or m
ore
Nev
er
(a) Verbal abuse by a nurse 1 2 3 4 (b) Verbal abuse by a doctor 1 2 3 4 (c) Verbal abuse by another CHBH employee (such as porters) 1 2 3 4 (d) Physical abuse by a nurse 1 2 3 4 (e) Physical abuse by a doctor 1 2 3 4 (f) Physical abuse by another CHBH employee (not nurse/doctor) 1 2 3 4 (g) Breach of confidentiality of patient information 1 2 3 4 (h) Professional negligence in patient care 1 2 3 4 (i) Substandard medical care 1 2 3 4
5. (a) Do you mind being cared for by student nurses?
Yes 1 No 2
(b) If Yes, please give explanations why:
�����������������������������������������
�����������������������������������������
����������������������������������������� 6. (a) Do you mind being examined by student doctors?
Yes 1 No 2
(b) If Yes, please give explanations why:
�����������������������������������������
�����������������������������������������
����������������������������������������� 7. Please rate how much you agree or disagree with the following statements:
Stro
ngly
ag
ree
Ten
d to
ag
ree
Ten
d to
di
sagr
ee
Stro
ngly
di
sagr
ee
No
opin
ion
(a) Patients who give money to staff at CHBH for services or treatment act wrongly. 1 2 3 4 5
(b) Staff at CHBH do not have sufficient time to treat patients with the necessary compassion and understanding. 1 2 3 4 5 (c) Language barriers make it difficult for staff to convey to patients proper information about their diagnosis and treatment.
1 2 3 4 5
(d) I sometimes find it difficult to understand what the doctors are telling me about my illness. 1 2 3 4 5
(e) I am always told what is wrong with me and why certain medicines are given to me.
(f) I usually find it easy to understand what the nurses are telling me about my illness. 1 2 3 4 5

160
8. On a scale of 1 to 7, how do you rate the physical environment at CHBH in terms of the following dimensions? The environment here refers to the hospital as whole, that is, the wards, the theatres, outpatient departments and so on. (The closer a number to a value, the more that value represents your experience. For instance, if you believe that CHBH is very clean, you will circle a 1; if you believe that it is very dirty, you will circle a 7. If you believe that it is somewhat dirty, you will circle a 5.)
(a) Clean 1 2 3 4 5 6 7 Dirty (b) Safe 1 2 3 4 5 6 7 Unsafe (c) Attractive 1 2 3 4 5 6 7 Unattractive (d) Cheerful 1 2 3 4 5 6 7 Depressing
9. What suggestions do you have for improving the functioning of CHBH in respect of the following?
(a) Relations between staff and patients:..��������������������.��
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(b) Safety and security: ��������������������������.���
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
(c) The quality of the service and care that you receive: �������.�����.����
�����������������������������������������
�����������������������������������������
�����������������������������������������
����������������������������������������� SECTION B: DEMOGRAPHICS 10. Gender:
Male 1 Female 2
11. Age:
20 years and younger 1 21-30 years 2 31-40 years 3 41-50 years 4 51-60 years 5 Older than 60 years 6

161
12. Home language: ��������������������������������.. 13. Highest formal qualification obtained: ������������������������ 14. (a) Are you a South African citizen?
Yes 1 No 2
(b) If No, please specify your country below: ���������������������������������������. 15. (a) Is this your first time as a patient at CHBH?
Yes 1 No 2
(b) If No, how many times have you been a patient at CHBH? (Your present stay excluded.)
Once before 1 Twice before 2 Three times before 3 Four or more times before 4
16. What is the length of your current stay at CHBH? (From the day of admittance until now.) �����������������������������.. 17. In which section of the hospital are you a patient? ������������������..����������� 18. Is there anything else that you would like to raise? Anything not covered by this questionnaire or
maybe something about the questionnaire itself?
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
�����������������������������������������
THANK YOU VERY MUCH FOR YOUR COOPERATION!

162

163
APPENDIX 8 NATIONAL PATIENTS� RIGHTS CHARTER (NATIONAL DEPARTMENT OF HEALTH)

164
165

166

167
APPENDIX 9 MISSION STATEMENT: CHRIS HANI BARAGWANATH HOSPITAL

168

169
![global health, epidemiology and genomics...the Chris Hani Baragwanath Hospital, South Africa [12]. The geographic regions of these centres are shown in Fig. 1, and a brief historical](https://img.pdfslide.net/doc/110x75/5f2f9566204a2609e5469ac3/global-health-epidemiology-and-genomics-the-chris-hani-baragwanath-hospital.jpg)