Embed Size (px)
Citation preview

Vol. 2, 883-888, May 1996 Clinical Cancer Research 883
4 The abbreviations used are: FISH. fluorescence in situ hybridization;DAPI, 4’,6-diamidino-2-phenylindole dihydrochloride.
Chromosome-specific Aneusomy in Carcinoma of the Breast1
Diane L. Persons,2 Robert A. Robinson,
Ping H. Hsu, Steven A. Seelig, Thomas J. Borell,
Lynn C. Hartmann, and Robert B. Jenkins3
Departments of Laboratory Medicine and Pathology [D. L. P.,T. J. B., R. B. J.l and Medical Oncology [L. C. H.], MayoClinic/Foundation, Rochester, Minnesota 55905; Department ofPathology, University of Iowa Hospital, Iowa City, Iowa 52242[R. A. R.]; and Vysis, Inc., Downers Grove, Illinois 60515[P. H. H., S. A. 5.1
ABSTRACT
Fluorescence in situ hybridization was performed on
touch preparations from 55 primary infiltrating ductal car-
cinomas of the breast to determine numeric chromosome
abnormalities. The frequency of aneusomy, measured by
both nondisomy and chromosomal gain, was determined for
chromosomes X, 4, 6-12, 17, and 18 with the use of chro-
mosome-specific, a-satellite DNA probes. The presence of
chromosome-specific numeric abnormalities was correlated
with established clinicopathological parameters, including
tumor size, lymph node involvement, tumor grade, estrogen
receptor level, and menopause status. In addition, a case-
control study was performed to explore a possible associa-
tion between chromosome-specific aneusomy and recur-
rence in lymph-node-negative patients.
Although chromosomes 8 and 6 were most frequently
aneusomic, numeric abnormalities of chromosomes 4 and 11
were most strongly associated with established prognostic
factors. For chromosomes 4 and 11, strong associations were
found with tumor involvement of lymph nodes and in-
creased tumor size, along with a weaker association with
tumor grade. In addition, numeric abnormalities of the
following chromosomes were associated with the corre-
sponding prognostic factors: chromosomes X, 7, and 12 with
lymph node status; chromosomes 10, 17, and 6 with tumor
size; and chromosomes 7, 12, 17, and X with tumor grade.
No correlations were observed with estrogen receptor level
or menopause status. In the case-control study performed on
isolated nuclei of paraffin-embedded tissue from lymph
node-negative breast cancer patients (19 cases and 19 con-
trols), the gain of chromosome 4 was correlated with disease
progression. These findings suggest that chromosome-
specific aneusomy is associated with certain established
prognostic factors and may be associated with disease pro.
gression.
Received 7/3 1/95; revised 12/28/95: accepted 1/24/96.I This work was supported in part by a grant from Vysis, Inc.2 Present address: Department of Pathology and Laboratory Medicine.
the University of Kansas Medical Center, Kansas City, KS 66160.3 To whom requests for reprints should be addressed, at LaboratoryGenetics, 970 Hilton, Mayo Clinic, 200 1st Street SW., Rochester, MN
55905. Phone: (507) 284-4696; Fax: (507) 284-0043.
INTRODUCTION
Breast cancer is the most common life-threatening malig-
nant neoplasm in women. An estimated 182,000 new cases will
be identified, and 46,000 deaths will occur in U.S. women in
I 994 ( I ). As with other solid tumors, technical difficulties have
resulted in limited cytogenetic information on cultured breast
tumors (2). Efforts to avoid culturing by performing direct
cytogenetic analysis on breast tumors have been hampered by
low mitotic rates and poor chromosome morphology. Chromo-
somes that have thus far been found to be relatively frequently
involved in structural alterations in breast cancer include chro-
mosomes 1, 3, 6, and I 1, whereas numeric abnormalities report-
edly often involve chromosomes 7, 8, 18, and 20 (3-7).
FISH4 using chromosome-specific, a-satellite DNA probes
can be used to evaluate aneusomy in interphase and/or metaphase
cells (8). Large numbers of uncultured interphase cells can be
evaluated rapidly. Several studies have used FISH for analysis of
aneuploidy in solid tumors (9-12). In situ hybridization studies in
breast cancer have been limited to evaluation of aneuploidy in the
breast cancer cell line MCF-7 (13, 14) and the study of seven
primary tumors for abnormalities of chromosomes I and 18 (13).
Using FISH, touch preparations of 55 primary infiltrating
ductal breast carcinomas were analyzed for numeric abnormal-
ities ofchromosomes X, 4, 6-12, 17. and 18 (for which directly
labeled a-satellite probes were available) at two collaborating
institutions. In addition, a case-control study using isolated
nuclei from paraffin-embedded tissue was performed to exam-
inc possible associations between chromosome-specific aneu-
somy and disease progression in node-negative breast carci-
noma. In this report, we present the chromosome aneusomy
results detected by FISH and correlate the findings with clini-
copathological data.
MATERIALS AND METHODS
Tissue Samples and Slide Preparation. Tumor samples
for FISH analysis of touch preparations were obtained from pa-
tients with primary breast carcinoma at the time of diagnosis. None
of the patients had received prior therapy. Samples were collected
at the two study sites (Mayo Clinic, site 1; and University of Iowa,
site 2) between January 1992 and December 1993. The study was
limited to infiltrating ductal carcinomas. Intaductal carcinoma was
present in a minority of cases; however, the infiltrating component
was the major component in all cases. Fresh tissue from 10 normal
breasts was used as control specimens. Touch preparations were
made from tissue samples obtained adjacent to areas where histo-
logical frozen sections verified the presence of tumor cells. Touch
preparations made from each tissue sample were fixed in cold
methanol for 20 mm, air dried, and stored at -20#{176}Cuntil in situ
hybridization was performed.
Research. on August 17, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

884 Aneuploidy in Breast Carcinoma
In the retrospective case-control study, isolated nuclei were
obtained from paraffin-embedded breast carcinoma from lymph
node-negative cases. Nineteen cases of node-negative breast
carcinoma were matched by tumor size (within 0.5 cm) and
surgical date. Cases were defined by evidence of disease pro-
gression within the first 3 years following surgery, whereas
control patients, who had been followed for a minimum of 6.5
years, showed no evidence of progression.
In Situ Hybridization with Centromere Enumeration
Probes. Detailed FISH methods for touch preparations have
been described previously (15). Briefly, frozen slides of touch
preparations were thawed, fixed for 20 mm in 3: 1 methanol:acetic
acid, dehydrated in an ethanol series, and air dried. For paraffin-
embedded tissue, isolated nuclei were prepared by the method of
Hedley et a!. (16) from two to four 40-p.m sections of tissue. The
sections were deparaffinized in Histo-Clear (National Diagnostics,
Atlanta, GA) for 10 mm (three times), dehydrated for 5 mm in
100% ethanol (twice), and rinsed in distilled water for S minutes
(twice). Two ml of an 8.5-mg/mi pepsin solution [P-70l2; Sigma
Chemical Co., St. Louis, MO; 8.5 mg/ml in 0.9% NaCl (pH 1.5)]
were added, and the sections were incubated at 37#{176}Cfor 2-2.5 h
with vortexing every 30 mm. The digested material was filtered
through 40.jam nylon mesh (Tetko, Briarcliff Manor, NY) and
centrifuged at 2400 rpm for 5 mm. The material was washed twice
in PBS, resuspended in 200-500 �xl PBS, and dropped onto Su-
perfrost/Plus slides (Fischer Scientific, Pittsburgh, PA). The cell
suspension was spread over an approximately 22 X 22-mm area
and oven dried at 60#{176}Cfor 10 mm.
Fluorescent, directly labeled a-satellite DNA probes for
chromosomes X, 4, 6-12, 17, and 18 and the hybridization
solution were provided by Vysis, Inc. Probes were used in either
single-color or in two-color combinations. A total of 10 p.1 probe
and hybridization mix was placed on the slide, which was
coverslipped and sealed with rubber cement. Following simul-
taneous denaturing of the probe and target DNA in a 90#{176}Coven
for 1 mm for touch preparations, the slides were incubated
overnight at 41#{176}Cin a moist chamber. For isolated nuclei from
paraffin-embedded tissue, slides were denatured at 80#{176}Cfor 10
mm and incubated at 50#{176}Cfor approximately I h. Posthybrid-
ization washes (10 mm each) for touch preparations included
three 50% formamide washes in 2X SSC (300 mmol/L sodium
chloride and 30 mmol/L sodium citrate) at 45#{176}Cand single
washes in 2X SSC at 45#{176}C,2X SSC-0.l% NP4O at 45#{176}C,and
2X SSC-0. 1% NP4O at room temperature. Times for posthy-
bridization washes for isolated nuclei were reduced to 1-5 s in
one 50% formamide wash and 5-10 s in 2X SSC at 45#{176}C,2X
SSC-0.l% NP4O at 45#{176}C,and 2X SSC-0.l% NP4O at room
temperature. Nuclei were counterstained with 1 jxg/ml DAPI in
the antifade p-phenylenediamine dihydrochloride.
Analysis of Interphase in Situ Hybridization. Hybrid-
ization signals were enumerated within 500 interphase nuclei per
specimen. Criteria for analysis of nuclei have been described pre-
viously (15). Overlapping nuclei and nuclei lacking any hybridiza-
tion signals were excluded from analysis. All specimens had more
than approximately 85% ofnuclei with hybridization signals. Anal-
ysis and photography were performed on fluorescence microscopes
equipped with a triple-pass filter (DAPI/Green/Orange; Vysis) for
simultaneous detection of SpectrumGreen, SpectrumOrange, and
DAPI, or a dual-pass filter (DAPI/Orange) for detection of Spec-
trumOrange and DAPI.
Two methods of analysis were used to evaluate the signif-
icance of numerical chromosome abnormalities. In method 1,
the presence of significant aneusomy was determined by using
a cutoff value of 40% nondisomy (any signal pattern other than
two signals) for each chromosome. In method 2, the presence of
25% of the nuclei with more than two signals was considered
abnormal for any given chromosome. The associations between
chromosome-specific aneusomy by either method and clinico-
pathological variables were determined by x2 analysis (lymph
node status, estrogen receptor status, and menopause status) and
ANOVA (tumor size and tumor grade). A one-tailed, paired
test was performed for analysis of cases and their corresponding
controls in the case-control study.
RESULTS
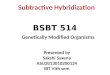
Touch Preparation Studies. The use of dual-color FISH
for chromosome centromere enumeration is illustrated in Fig. 1.
The numbers of centromeric signals (one, two, three, four, etc.)
for the 1 1 chromosomes were counted in each of 55 breast
carcinoma touch preparations. It should be emphasized that the
use of centromere probes identifies the copy numbers of mdi-
vidual chromosomes but does not determine whether the chro-
mosomes are structurally normal or abnormal.
Because a standard approach for analysis of chromosome-
specific aneusomy has not been developed, the chromosome
copy number data were analyzed by two methods. In the first
method, the frequency of chromosome-specific aneusomy
within the 55 cases was determined by using a cutoff value
based on normal controls. The mean nondisomy (patterns other
than two signals) among the 1 1 chromosomes in the I 0 normal
breast touch preparations varied between 9 and 14%. The mean
nondisomy values plus 3 SD varied between 26 and 37% (data
not shown). Therefore, to assure identification of only signifi-
cant aneusomic populations, a 40% cutoff value was chosen.
Significant aneusomy (>40% nondisomy) for at least one of the
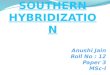
chromosomes examined was observed in 44 of 55 cases. Fig. 2
is an example of the pattern of the percentage of nondisomic
cells observed in one case for the I I chromosomes. In this case,
chromosomes 6, 7-12, and 18 were classified as aneusomic.
The second method of analysis of numeric chromosome ab-
normalities focused on specific chromosome gains (more than than
two signals). In control specimens, the mean gain for individual
chromosomes varied between 1 .5 and 7.2%. The mean values plus
3 SD varied between 1.9 and 10.4%. Observing more than two
signals for a specific chromosome reflects either endoreduplication
of the specific chromosome or a tetraploidization event resulting in
doubling of the number of all chromosomes. This method was
chosen because cytogenetic evidence has suggested that trisomies
may be relevant as early changes in breast cancer (7). In addition,
it was thought that analyzing the chromosomal gain would be a
sensitive measurement of aneusomy that would avoid certain tech-
nical artifacts, such as decreased hybridization efficiency and ran-
dom chromosomal loss.
The frequency of aneusomy by both methods for each
chromosome in the cohort of 55 cases is illustrated in Fig. 3. The
most commonly aneusomic chromosome was chromosome 8,
Research. on August 17, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

U,
U
C.)
E0U,
C0zCa0
C,a.
60
50
11ftII
U,aU,U,
C.)
Caaaa.
I Ir- � 0, 0 ‘-
Clinical Cancer Research 885
S
.
4
00
“V.
I
Y
Fig. I Photomicrograph ( X630) illustrating(SpectrumOrange) and 1 1 (SpectrumGreen).
100
90
80
70
60
50
40
Chromosome
nuclei with tour signals and nuclei with two signals for the centromeres of chromosomes 6
Fig. 2 Example of chromosome-specific aneusomy (percentage ofnondisomic nuclei ) for I 1 chromosomes in an individual case of infil-
trating breast carcinoma. Horizo,,tal li,,e, 40% cutoff value for signifi-
cant aneusomy.
which had an abnormal copy number (nondisomy) in 53% of
cases and was gained in 58% of the cases. Likewise, chromo-
some 6 was aneusomic in a higher proportion of cases (47C/�
nondisomic and 50% gain) than were the remaining chromo-
somes. Nondisomy and/or gain of the remaining nine chromo-
somes was observed in 24-44% of the cases.
Clinicopathological data, including lymph node status. tu-
mor size, tumor grade, estrogen receptor status, and menopausal
status for the 55 cases, are summarized in Table 1 . Significant
[iri[IrI.rI[1.x 4 6 7 8 9 10 11 12 17 18
Chromosome
Fig. 3 Frequency (percentage of cases) of chromosome-specific aneu-
somy (LI, nondisomy. #{149},gain) in 55 cases of brcast carcinoii�a.
statistical correlations (P < 0.05) between the clinicopatholog-
ical variables and the frequency of aneusomy (40% nondisomy)
and gain (more than two signals in 25% cells) for each chro-
mosome are shown in Table 2. Aneusomy for chromosomes 4
(P = 0.007, nondisomy; P 0.009. gain) I 1 (P 0.05,
nondisomy: P = 0.001, gain). and X (P = 0.006. nondisoniy:
P = 0.01. gain) was found to be significantly associated with
tumor involvement of lymph nodes. An association with lymph
node status was also observed with the gain of chromosomes 7
(P = 0.005) and 12 (P = 0.03).
Research. on August 17, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Table 1 Clinicopathological patient data (n = 55)
Characteristic No. of patients
Table 2 Chromosome-specific aneusomy: associations withclinicopathological variables
See text for description of methods I and 2. All values P < 0.05.
ChromosomeMethod 1
(40% Nondisomy)Method 2
(>2 signals)
Lymph node status4 0.007 0.0097 0.00511 0.05 0.001
12 0.03
X 0.006 0.01
Tumor size4 0.04 0.00056 0.01
10 0.0002 0.00111 0.01 0.0003
17 0.03 0.002
Tumor grade4 0.05
7 0.03 0.004
11 0.0212 0.009 0.02
17 0.03
X 0.02
886 Aneuploidy in Breast Carcinoma
Age (yr)<4040-49
50-59
60-69
>69Lymph nodes
PositiveNegative
Tumor size (cm)<2
2-5>5
Tumor grade2
3
4
Estrogen receptorPositiveNegative
MenopauseBefore
After
4
5
12
1618
21
34
12
394
8
20
27
45
10
4510
Increasing tumor size was found to be associated with
numeric chromosome abnormalities determined by both meth-
ods involving chromosomes 4 (P = 0.04, nondisomy; P =
0.0005, gain), 10 (P = 0.0002, nondisomy; P = 0.001, gain), 11
(P = 0.01, nondisomy; P = 0.0003, gain), and 17 (P = 0.03,
nondisomy; P = 0.002, gain). In addition, chromosome 6 (P =
0.01) was associated with tumor size.
Tumor grade was associated with abnormal chromosomes
7 (P = 0.03, nondisomy; P - 0.004, gain) and 12 (P = 0.009,
nondisomy; P = 0.02, gain), as determined by both methods.
Nondisomy of chromosome X (P = 0.02) was also associated
with tumor grade, as was the gain of chromosomes 4 (P = 0.05),I 1 (P = 0.02), and 17 (P = 0.03).
No associations were observed between aneusomy by ci-
ther method for any of the 1 1 chromosomes and estrogen
receptor or menopause status.
Lymph Node-negative Case-Control Study. Table 3
summarizes the results of aneusomy of specific chromosomes in
breast carcinomas from node-negative patients whose disease
progressed in the first 3 years following diagnosis (cases) com-
pared with matched control patients (controls), in whom no
evidence of disease progression was observed within at least 6.5
years following diagnosis. The difference in the mean percent-
age of aneusomic (other than two signals) cells and the differ-
ence in the mean percentage of gain (more than two signals)
between matched cases and controls are illustrated for each
chromosome. The most significant difference in the mean values
for both aneusomy and gain was observed with chromosome 4
(P = 0.09 and 0.05, respectively).
DISCUSSION
In this study, we have described chromosome-specific,
numeric abnormalities in a group of 55 primary infiltrating
ductal carcinomas of the breast. Most previous cytogenetic
studies of breast cancer have suggested that most breast tumors
have clonal chromosomal abnormalities (17-22). In contrast,
other authors have reported that a substantial proportion of
primary tumors has a normal diploid karyotype (23, 24). The
difference in these results could be due to a number of factors,
including case selection and various culture artifacts. The use of
FISH on uncultured tumor nuclei provides the advantage of
accurately reflecting the in vivo chromosome complement. In
addition, culture artifacts, such as overgrowth of normal diploid
cells or selection of subclones possessing in vitro growth ad-
vantages, are avoided. The observation of significant aneusomy
for at least one of the chromosomes examined in 44 of 55 of the
tumors in this study supports the previous reports of the pres-
ence of clonal abnormalities in a large fraction of primary breast
tumors. Because our method detected only numeric abnormal-
ities and examined only one-half of the chromosomes, it is likely
that an even higher proportion of primary tumors contains either
structural and/or numeric clonal abnormalities.
In this study, chromosomes 8 and 6 were found to be the most
freq uently aneusomic chromosomes in the 55 breast carcinomas.
Both the gain and loss of chromosome 8 have been described as
frequent aneusomy in breast cancer cytogenetic studies (25-27).
Rohen et aL (7) recently described trisomy 8 as a clonal aberration
in 10 of 39 clonally abnormal breast carcinomas. In addition, they
reported trisomy 8 as the most frequent nonclonal aberration. The
investigators performed FISH in two cases in which nonclonal
trisomy 8 was observed. Three signals for the centromere of chro-
mosome 8 were present in 1 1 and 14% of the nuclei of the two
cases. The authors suggested that their findings indicated that
trisomy 8 was present in microclones. The present study confirms
previous reports and shows that an abnormal copy number of
chromosome 8 was present in more than 50% of the cases.
Chromosome 6 is one of the most frequently structurally
abnormal chromosomes present in breast cancer (2 1 ). However,
the gain or loss of the entire chromosome has not been reported
as a frequent finding by conventional cytogenetic studies. In
addition, 6q is a frequent site of loss of heterozygosity in breast
tumors (28). Numeric abnormalities of chromosome 6, includ-
Research. on August 17, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 887
Table 3 Node-negativ e breast cancer case- control study
Nondisomy
(%; mean ± SD) DifferenceI test
one-tailedCases Controls
Chromosome (ii 19) (n = 19) (mean ± SE) P
4 21.3 ± 15.1 15.9 ± 8.6 5.4 ± 3.7 0.09
6 27.1 ± 19.9 20.4 ± 16.8 6.7 ± 6.3 0.157 22.4 ± 16.1 21.2 ± 20.9 1.1 ± 5.8 0.43
8 26.7 ± 18.7 22.3 ± 17.1 4.4 ± 7.0 0.27
9 18.3 ± 15.3 22.1 ± 21.6 -3.8 ± 6.4 0.72
10 19.0 ± 15.2 18.8 ± I 1.4 0.1 ± 4.6 0.491 1 21.9 ± 16.5 19.3 ± 16.2 2.6 ± 6.0 0.34
12 18.0 ± 13.8 19.3 ± 18.0 -1.3 ± 5.7 0.59
17 21.5 ± 16.3 20.7 ± 13.5 0.8 ± 5.2 0.45
18 21.8 ± 15.7 17.1 ± 6.1 4.7 ± 4.2 0.14X 24.0 ± 16.2 23.3 ± 16.8 0.7 ± 6.2 0.46
ing those that were possibly structurally abnormal, were de-
tected in approximately 50% of the cases in this study.
Aneusomy, as evaluated by either specific chromosome
nondisomy or chromosomal gain, was found to be associated
with select prognostic factors. Evaluation of chromosome-spe-
cific gain seemed to be a more sensitive measurement than
nondisomy for correlating aneusomy with prognostic variables.
It is of interest that the chromosomes that most commonly had
numeric abnormalities, chromosomes 8 and 6, were not found to
be associated with prognostic factors, with the exception of a
weak association of chromosome 6 with tumor size. In contrast,
some of the other less commonly aneusomic chromosomes
showed strong associations with recognized prognostic factors
in this disease, namely, lymph node status (chromosomes 4, 7,
11, 12, and X), tumor size (chromosomes 4, 10, 11, and 17), and
tumor grade (chromosomes 4, 7, 1 1, 12, 17, and X).
Numeric abnormalities of chromosome 4 were strongly
associated with lymph node status. A statistically significant
association with tumor size and a weak association with tumor
grade were also found. Lu et a!. (5) reported the loss of chro-
mosome 4 to be a relatively common finding (5 of 22 cases) by
direct cytogenetic analysis of primary breast tumors. In this
study, however, a significant association with the prognostic
factors was seen with the gain of the chromosome, along with
nondisomy. In the retrospective case-control study comparing
disease progression and chromosome-specific aneusomy in
lymph node-negative cases, disease progression was found to be
most closely associated with abnormalities of chromosome 4.
Although (due to the small sample size) the finding was not
statistically significant with nondisomy (P = 0.09), marginally
significant associations were observed with the gain of chromo-
some 4 and disease progression (P = 0.05).
Chromosome 1 1 had a similar pattern of association with the
same prognostic factors as chromosome 4. Structural abnormalities
of chromosome 1 1, including loss of chromosomal material and
amplification of sequences, have been reported in breast cancer.
Mackay et a!. (29) correlated the loss of sequences at 1 lpl3-lS to
the lack of estrogen receptors and increased tumor size. Another
study (30) reported associations between the loss of sequences on
1 lp and grade III tumors, distal metastases, and the lack of estrogen
and progesterone receptors. Amplification of sequences harboring
the genes int-2, bcl-l, and hst, located at 1 1q13, has been reported
in 4-17% of breast tumors (31, 32).
Strong associations between tumor size and abnormal copy
numbers of chromosomes 10 and 17 were observed. Although not
a frequent finding, clonal numeric abnormalities of chromosome 17
have occasionally been reported in conventional cytogenetic stud-
ies of breast tumors (21, 33). Abnormalities of chromosome 17 are
of great interest for several reasons. A region on the short arm of
chromosome 17, including the TP53 gene, has the highest fre-
quency of allele loss (deleted in >50% of informative cases) in
primary breast carcinomas (28, 34-36). Furthermore, approxi-
mately 40% of breast carcinomas have loss of heterozygosity on
the long arm of chromosome 17 (34, 36). Several candidate tumor
suppressor genes reside on l7q, including BRCA-1 (37), the pro-
hibitin gene (38), nm23 (39), and Wnt-3 (40).
Numeric abnormalities, especially gains, of chromosome 7
were found to be associated with lymph node status and tumor
grade. Trisomy 7 has been described as a frequent clonal and
nonclonal abnormality in primary breast carcinomas (7). It has
also been noted as the sole cytogenetic abnormality in some
breast tumors (21, 41).
This study demonstrated a high frequency of chromosome
copy number aberrations in breast carcinoma. Although chro-
mosomes 8 and 6 were the most frequently abnormal chromo-
somes, chromosomes 4 and I I showed the strongest associa-
tions with established prognostic factors. For both chromosomes
4 and I I , strong associations were noted with lymph node status
and tumor size. In addition, aneusomy of chromosome 4 was
most closely associated with disease progression in node-nega-
tive breast cancer patients.
REFERENCES
1. Boring, C. C., Squires, T. S., Tong, T., and Montgomery, S. Cancerstatistics, 1994. CA Cancer J. Clin., 44: 7-26, 1994.
2. Mitelman, F. (ed). Catalog of Chromosome Aberrations in Cancer,Ed. 4. New York: Wiley-Liss, Inc., 1991.
3. Trent, J. M. Cytogenetic and molecular biologic alterations in humanbreast cancer: a review. Breast Cancer Res. Treat., 5: 22 1-229, 1995.
4. Gebhart, E., Bruderlein, S., Augustus, M., Siebert, E., Feldner, J., andSchmidt, W. Cytogenetic studies on human breast carcinomas. BreastCancer Res. Treat., 8: 125-138, 1986.
5. Lu, Y-J., Xiao, S., Yan, Y-S., Fu, S-B., Liu, Q-Z., and Li, P. Directchromosome analysis of 50 primary breast carcinomas. Cancer Genet.
Cytogenet., 69: 91-99, 1993.
6. Pandis, N., un, Y., Gourunova, L., Petersson, C., Bardi, G., Idvall, I.,Johansson, B., Ingvar, C., Mar,dahl, N., Mitelman, F., and Heim, S. Chro-
Research. on August 17, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

888 Aneuploidy in Breast Carcinoma
mosome analysis of 97 primary breast carcinomas: identification of eightkaryotypic subgroups. Genes Chromosomes & Cancer, 12: 173-185, 1995.
7. Rohen, C., Meyer-Bolte, K., Bonk, U., Ebel, T., Staats, B.,Leuschner, E., Gohla, G., Caselitz, J., Bartnitzke, S., and Bullerdiek, J.Trisomy 8 and 18 as frequent clonal and single-cell aberrations in 185primary breast carcinomas. Cancer Genet. Cytogenet., 80: 33-39, 1995.
8. Pinkel, D., Straume, T., and Gray, J. W. Cytogenetic analysis usingquantitative, high-sensitivity, fluorescence hybridization. Proc. Natl.Acad. Sci. USA, 83: 2934-2938, 1986.
9. Hopman, A. H. N., Poddighe, P. J., Smeets, A. W. G. B., Moesker,0., Beck, J. L. M., Vooijs, G. P., and Ramaekers, F. C. S. Detection ofnumerical chromosome aberrations in bladder cancer by in situ hybrid-ization. Am. J. Pathol., 135: 1 105-1 117, 1989.
10. Hopman, A. H. N., Moesker, 0., Smeets, A. W. G. B., Pauwels,R. P. E., Vooijs, G. P., and Ramaekers, F. C. S. Numerical chromosome1, 7, 9, and 11 aberrations in bladder cancer detected by in situ hybrid-ization. Cancer Res., 51: 644-651, 1991.
I I. Waldman, F. M., Carroll, P. R., Kerschmann, R., Cohen, M. B.,Field, F. G., and Mayall, B. H. Centromeric copy number of chromo-some 7 is strongly correlated with tumor grade and labeling index inhuman bladder cancer. Cancer Res., 51: 3807-3813, 1991.
12. Arnoldus, E. P. J., Noordermeer, I. A., Peters, A. C. B., Voormolen,J. H. C., Bots, G. 1. A. M., Ran, P. A. K., and van der Ploeg, M.Interphase cytogenetics of brain tumors. Genes Chromosomes & Can-
cer, 3: 101-107, 1991.
13. Devilee, P., Thierry, R. F., Kievits, T., Kolluri, R., Hopman,A. H. N., Willard, H. F., Pearson, P. L., and Cornelisse, C. J. Detection
of chromosome aneuploidy in interphase nuclei from human primarybreast tumors using chromosome-specific repetitive DNA probes. Can-cer Res., 48: 5825-5830, 1988.
14. Balazs, M., Mayall, B. H., and Waldman, F. R. Simultaneousanalysis of chromosomal aneusomy and 5-bromodeoxyuridine incorpo-
ration in MCF-7 breast tumor cell line. Cancer Genet. Cytogent., 57:
93-102, 1991.
15. Persons, D. L., Hartmann, L. C., Herath, J. F., Borell, T. J., Cliby,W. A., Keeney, G. L., and Jenkins, R. B. Interphase molecular cytoge-
netic analysis of epithelial ovarian carcinomas. Am. J. Pathol.. 142:733-741, 1993.
16. Hedley, D. W., Friedlander, M. L., Taylor, I. W., Rugg, C. A., and
Musgrove, E. A. Method for analysis of cellular DNA content ofparaffin-embedded pathological material using flow cytometry. J. His-
tochem. Cytochem., 31: 1333-1335, 1983.
17. Rodgers, C. S., Hill, S. M., and Hulten, M. A. Cytogenetic analysis in
human breast carcinoma. I. Nine cases in the diploid range investigatedusing direct preparations. Cancer Genet. Cytogenet., 13: 95-1 19, 1984.
18. Hill, S. M., Rodgers, C. S., and Hulten, M. A. Cytogenetic analysisin human breast carcinoma. II. Seven cases in the triploid/tetraploid
range investigated using direct preparations. Cancer Genet. Cytogenet.,24: 45-62, 1987.
19. Gerbault-Seureau, M., Vielh, P., Zafrani, B., Salmon, R., andDutrillaux, B. Cytogenetic study of twelve human near-diploid breastcancers with chromosomal changes. Ann. Genet., 30: 138-145, 1987.
20. Hainsworth, P. J., Raphael, K. L., Stillwell, R. G., Bennett, R. C.,
and Garson, 0. M. Cytogenetic features of twenty-six primary breastcancers. Cancer Genet. Cytogenet., 52: 205-218, 1991.
21. Thompson, F., Emerson, J., Dalton, W., Yang, J-M., McGee, D.,
Villar, H., Knox, S., Massey, K., Weinstein, R., Bhattacharyya, A., and
Trent, J. Clonal chromosome abnormalities in human breast carcinomasI. Twenty-eight cases with primary disease. Genes Chromosomes &Cancer., 7: 185-193, 1993.
22. Trent, J., Yang, J-M., Emerson, J., Dalton, W., McGee, D., Massey,K., Thompson, F., and Villar, H. Clonal chromosome abnormalities inhuman breast carcinomas II. Thirty-four cases with metastatic disease.
Genes Chromosomes & Cancer., 7: 194-203, 1993.
23. Wolman, S. R., Smith, H. S., Stampfer, M., and Hackett, A. J.Growth of diploid cells from breast cancers. Cancer Genet. Cytogenet.,16: 49-64, 1985.
24. Zhang, R., Wiley, J., Howard, S. P., Meisner, L. F., and Gould,M. N. Rare clonal karyotypic variations in primary cultures of human
breast carcinoma cells. Cancer Res., 49: 444-449, 1989.
25. Bullerdiek, J., Leuschner, E., Taquia, E., Bonk, U., and Bartnitzke,S. Trisomy 8 as a recurrent clonal abnormality in breast cancer? CancerGenet. Cytogenet., 65: 64-67, 1993.
26. Rodgers, C. S., Hill, S. M., and Hulten, M. A.. Cytogenetic analysis
in human breast carcinoma. I. Nine cases in the diploid range investi-
gated using direct preparations. Cancer Genet. Cytogenet., 13: 95-1 19,1984.
27. Hill, S. M., Rodgers, C. S., and Hulten, M. A. Cytogenetic analysisin human breast carcinoma. II. Seven cases in the triploid/tetraploidrange investigated using direct preparation. Cancer Genet. Cytogenet.,24: 45-62, 1987.
28. Devilee, P., van Vliet, M., van Sloun, P.. Kuipersj-Dijkshoorn, N.,
Hermans, J., Pearson, P. L., and Cornelisse, C. J. Allelotype of humanbreast carcinoma: a second major site for loss of heterozygosity is onchromosome 6q. Oncogene, 6: 1705-171 1, 1991.
29. Mackay, J., Elder, P. A., Porteous, D. J., Steel, C. M., Hawkins,R. A., Going, J. J., and Chetty, U. Partial deletion of chromosome 1 lp
in breast cancer correlates with size of primary tumour and oestrogenreceptor level. Br. J. Cancer., 58: 7 10-7 14, 1988.
30. Ali, I. U., Lidereau, R., Theiliet, C., and Callahan, R. Reduction to
homozygosity of genes on chromosome 1 1 in human breast neoplasia.
Science (Washington DC), 238: 185-188, 1987.
31. Ali, I. U., Merlo, G., Callahan, R., and Lidereau, R. The amplifi-
cation unit on chromosome 1 1q13 in aggressive primary human breasttumors entails the bcl-1, int-2, and hst loci. Oncogene, 4: 89-92, 1989.
32. Adnane, J., Gaudray, P., Simon, M. P., Simony-Lafontaine, J.,
Jeanteur, P., and Theillet, C. Proto-oncogene amplification and humanbreast tumor phenotype. Oncogene, 4: 1389-1395, 1989.
33. Geleick, D., Hansjakob, M., Matter, A., Torhorst, J., and Regenass,
U. Cytogenetics of breast cancer. Cancer Genet. Cytogenet., 46: 217-
229, 1990.
34. Sato, T., Tanigami. A., Yamakawa, K.. Akiyama. F.. Kasumi. F.,
Sakamoto, G., and Nakamura, Y. Allelotype of breast cancer: cumula-tive allele losses promote tumor progression in primary breast cancer.
Cancer Res., 50: 7 184-7 1 89, 1990.
35. Larsson, C., Bystrom, C., Skoog, L., Rotstein, S., and Nordenskjold,
M. Genomic alterations in human breast carcinomas. Genes Chromo-somes & Cancer., 2: 191-197, 1991.
36. Varley, J. M., Brammar, W. J., Lane, D. P., Swallow, J. E., Dolan, C..
and Walker, R. A. Loss of chromosome I 7pl 3 sequences and mutation of
p53 in human breast carcinomas. Oncogene, 6: 413-421, 1991.
37. HaIl. J. M., Lee, M. K.. Newman, B., Morrow, J., Anderson, L., Huey,
B., and King, M-C. Linkage of early-onset familial breast cancer to chro-
mosome 17q21. Science (Washington DC), 250: 1684-1689, 1990.
38. Sato, T., Saito, H., Swenso, J., Olifant, A., Wood, C., Danner, D.,
Sakamoto, T., Takita, K., Kasumi, F., Miki, Y., Skolnick, M., and Naku-
mum, Y. The human prohibitin gene located on chromosome I 7q2 1 is
mutated in sporadic breast cancer. Cancer Res., 52: 1643-1646, 1992.
39. Leone, A., McBride, 0. W., Weston, A., Wang, M. G., Anglard, P.,
Cropp, C. S., Goepel, J. R., Lidereau, R., Callahan, R., Linehan, W. M.,
Harris, C. C., Liotta, L. A., and Steeg, P. S. Somatic allelic deletion of
nm23 in human cancer. Cancer Res., 51: 2490-2493. 1991.
40. Roelink, H., Wagenaar, E., Lopes da Silva, S.. and Nusse, R.Wnt-3, a gene activated by proviral insertion in mouse mammary
tumors, is homologous to int-I/Wnt-/ and is normally expressed inmouse embryos and adult brain. Proc. NatI. Acad. Sci. USA, 87:
4519-4523, 1990.
41. Pandis, N., Heim, S., Bardi, G., Idvall, I., Mandahl, N., and
Mitelman, F. Chromosome analysis of 20 breast carcinomas: cytoge-netic multiclonality and karyotypic-pathologic correlations. Genes
Chromosomes & Cancer, 6: 51-57, 1993.
Research. on August 17, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1996;2:883-888. Clin Cancer Res D L Persons, R A Robinson, P H Hsu, et al. Chromosome-specific aneusomy in carcinoma of the breast.
Updated version
http://clincancerres.aacrjournals.org/content/2/5/883
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/2/5/883To request permission to re-use all or part of this article, use this link
Research. on August 17, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from