-
Chronic Pain Management and the Pharmacist's Role
Sukhvir Kaur, PharmD, BCACPDirector of Assessment and Assistant
Professor
California Northstate University College of Pharmacy
-
Disclosure
I or my spouse have no actual or potential conflict of interest
in relation to this program.
-
Discuss the role of a pharmacist in the management of chronic
pain.
Perform an appropriate pain assessment taking into account the
characteristics and nature of the pain stimuli.
Discuss non pharmacologic and pharmacologic options available
for the treatment of chronic pain including its place in therapy
and potential risks with their use.
Develop a therapeutic plan for patients with chronic pain that
maximizes patient response while minimizing adverse events and
other drug-related problems.
Educate and advocate for patients about effective pain
management strategies.
Learning Outcomes
-
Defined as “any pain that persists beyond the anticipated time
of healing”
Nociceptive pain or neuropathic pain
International Association for the Study of Pain (IASP) states
that pain is “an unpleasant sensory or emotional experience
associated with actual or potential tissue damage, or described in
terms of such damage”
Highly SUBJECTIVE
Chronic Pain
-
Chronic Pain
-
EpidemiologyMore than 100 million people in United States live
with chronic pain.
Estimated economic burden of chronic pain exceeds 500 billion
dollars.
Despite all the efforts to treat pain adequately, it remains
INAPPROPRIATELY treated. ◦ Reduces a patient’s independence and
ability to perform many daily activities◦ Places strains on
social relationships,
mood, and sleep patterns.
-
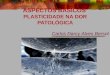
Biopsychosocial concept of Chronic Pain
http://image.slidesharecdn.com/chronicpain-150128073452-conversion-gate01/95/chronic-pain-managment-17-638.jpg?cb=1423812958
-
Characteristics Acute Pain Chronic Pain
Relief of pain Highly desirable Highly desirable
Dependence and tolerance to medication Unusual Common
Psychological component Usually not present Major problem
Organic cause Common May not be present
Environmental/ family issue Small Significant
Insomnia Unusual Common
Treatment goal Pain reduction Functionality
Depression Uncommon Common
Description Obvious distress (trauma) No noticeable trauma
Symptoms Sharp, dull, shock like, tingling, shooting, radiating,
fluctuating in intensity, varying in location
Sharp, dull, shock like, tingling, shooting, radiating,
fluctuating in intensity, varying in location
Comorbid condition None Insomnia, anxiety and depression
Lab test No specific test, subjective to the patient No specific
test, but can test for past trauma, VitD, TSH, and B12
Classification of Pain
-
Rapid pain relief or reduction in pain intensity is NOT the
Goal
Improve or maintain the patient’s level of functionalitySet
goals with the patient for functional improvement, and document
them for future monitoring purposes to determine efficacy
Improving pain and function by ~30% is a success
Goal of Chronic Pain Management
-
1) Make diagnosis with a differential
2) Conduct psychological assessment, screening for addiction
potential
3) Obtain informed consent
4) Utilize a treatment agreement
5) Conduct pre- and post intervention assessment pain level and
function
6) Conduct an appropriate trail of opioid therapy with or
without adjuvants
7) Conduct reassessment of pain score and level of function
8) Regularly assess “the 4 A’s of pain”
9) Periodically review all comorbid conditions
10) Document evaluations and follow-up appointments
The 10 Steps of Universal Precautions in Pain Medicine
Barbee J, Chessher Jaclyn, Greenlee, Max. Pain Management: The
Pharmacist’s Evolving Role. Pharmacy Times.
2015.http://www.pharmacytimes.com/publications/health-system-edition/2015/july2015/pain-management-the-pharmacists-evolving-role.
Accessed July 5, 2016.
http://www.pharmacytimes.com/publications/health-system-edition/2015/july2015/pain-management-the-pharmacists-evolving-role
-
Help minimize risk for patients using pain medications.◦ Assess
and properly plan to minimize patient risk of Pain Medicine
◦ Proper Pain Assessment to understand pain and provide highly
effective treatment while minimizing risk
◦ Educate the patients of the role of opioids in the treatment
of chronic pain
Help patients live meaningful and productive lives with
adequately managed pain
Monitor patient’s 4 As:◦ Analgesia
◦ Activities of daily living
◦ Adverse events
◦ Aberrant drug behaviors
Pharmacist’s Role
-
Pain Interview
-
Pain Interview “PQRST”
Provoke: What makes the pain worse?
Palliate: What makes the pain better?
Quality: Describe the pain?
Radiation/ Location: Where is the pain?
Severity/ Pain score: How does this pain compare with other pain
you have experienced? What are the activities that you would like
to perform that you cannot, due to the pain?
Timing/ onset/ duration: When did it began and how long has it
been? Does the intensity of pain change with time?
-
Treatment of Chronic Pain - Video
https://www.theacpa.org/a-car-with-four-flat-tires
-
Treatment approaches to Management of Chronic pain
NON-PHARMACOLOGICAL THERAPY
Acupuncture
Local electrical stimulation including TENS
Brain stimulation
Surgery
Psychotherapy
Relaxation and medication therapies
Biofeedback
Behavior modification
Placebos?
PHARMACOLOGIC THERAPY
NSAIDs
Antidepressants
Anticonvulsants
Topical agents
Cannabinoids
Non-Opioids
Opioids
Intrathecal drug delivery systems
-
Non-pharmacological therapy Evidence/ Potential Place in
Therapy
Acupuncture Evidence is conflicting and clinical studies to
investigate its benefits are ongoing
Biofeedback Evidence for headache and back pain; Often used in
combination without side effects
Chiropractic Evidence for chronic back pain relief
Cognitive-behavioral therapy Strong evidence for chronic pain,
postoperative pain, cancer pain, and the pain of childbirth
Counseling Can be of help to learn about the physiological
changes produced by pain
Electrical stimulations including transcutaneous electrical
stimulation (TENS)
Can help reduce pain
Exercise Evidence with chronic pain for overall well being
including light to moderate; shown efficacy to relief low back
pain
Hypnosis Speculated to help a person concentrate and relax or is
more responsive to suggestion
Low-power lasers Used by some physical therapists but method is
NOT without controversy
Magnets Increasingly popular with athletes to control
sport-related pain or other pain conditions
Nerve blocks Interventional to relieve nerve pain and pains
related to cancer
Physical therapy and rehabilitation To increase function,
control pain and gain recovery
Placebo Employed in studies, work by stimulating the brain’s own
analgesics
R.I.C.E.—Rest, Ice, Compression, and Elevation Temporary muscle
or joint injuries
Surgery Limited evidence to show which procedures work best for
their indications
http://www.ninds.nih.gov/disorders/chronic_pain/detail_chronic_pain.htm#3084_15
-
Chronic Pain Medications and Dangers
-
Pain Algorithm Identify pain source if possible; Assess pain
severity and quality using consistent method such as numeric rating
scale (NRS); scale 0-10 out of 10
Mild (Score 1-4/10) Moderate (Score 5-7/10) Severe (Score
8-10/10)
APAP +/- NSAIDs when risk doesn’t outweigh benefits
Combo Opioid AND APAP/NSAID
Opioid Analgesics tailored to pain severity and patient
characteristics
If pain relief is not adequate, step up therapy is
recommended
Always monitor pain frequency and status, anticipate side
effects, properly titrate doses based on patient characteristics,
PO is preferred when possible, Consider around the clock dosing
when appropriate, and PRN regimens for breakthrough or highly
variable pain
-
Nonsteroidal Anti-inflammatory DrugsPlace in Therapy • Effective
in the treatment of chronic low back pain as well as chronic pain
due to osteoarthritis
• Modest effect In treating lumbar radiculopathy• The addition
of an NSAID to a pain management regiment can have an
opioid-sparing effect of
between 20-35%
Comments/Concerns • Minimal effect in treating neuropathic pain
states
-
AntidepressantsPlace in Therapy • Effectiveness for
antidepressants in the treatment of chronic pain disorders with
a
strong neuropathic component has long been established in the
literature• TCAs (Amitriptyline, imipramine, nortriptyline and
desipramine):
• Shown to be effective in treating a variety of painful
neuropathic conditions such as diabetic peripheral neuropathy
(DPN), postherpectic neuralgia (PHN), painful polyneuropathy,
postmastectomy pain, and centeral poststroke pain
• Analgesic effects are independent of the presence of any
changes in depression or mood state.• Side effects that can be
significant include postural hypotension, dry mouth, and sedation
for
which reason these medications are typically taken at bedtime
especially in the elderly population leading to increase risk of
fall.
• Duloxetine and venlafaxine• Have shown efficacy in treating
peripheral neuropathic pain and other chronic pain conditions.
• Duloxetine• Treatment of painful DPN, fibromyalgia, and
chronic musculoskeletal pain• Mood-elevating effects have a
significant contribution to the reported decreases in pain
scores
-
AnticonvulsantsPlace in Therapy Side effects/concerns
Carbamazepine Trigeminal neuralgia but has NOT been shown to be
as effective in treating other neuropathic pain disorders
somnolence, dizziness, and gaitDisturbanceMore serious adverse
reactions that have been reported includeStevens-Johnson syndrome,
toxic epidermal necrolysis, and blood dyscrasias
Valproic acid, oxcarbazepine, topiramateand lamotrigine
Inconsistent evidence of efficacy in treating neuropathic
pain
Gabapentin DPN, PHN, painful polyneuropathy, neuropathic
cancerpain, central poststroke pain, and spinal cord injury
pain.
dizziness, somnolence,and ataxia, peripheral edema
Pregabalin *First line for treating neuropathic pain dizziness,
somnolence,and ataxia.>Peripheral edema
-
Topical AgentsPlace in Therapy
Lidocaine (5% gel or patch) Peripheral neuropathic pain
conditions with allodynia as well as PHN with allodynia
Topical NSAIDs (diclofenac, ibuprofen, and ketoprofen)
Short-term pain relief in the treatment ofSoft tissue injuries
and chronic joint-related pain.
Topical high-dose capsaicin (8%) Effective in providing rapid
and sustained pain relief in patients with PHN and painful human
immunodeficiency virus (HIV)-associated neuropathies
-
CannabinoidsPlace in Therapy Mechanism of Action
Medicinal marijuana Neuropathic pain Activation of CB2 receptors
on peripheral inflammatory cells has beenshown to decrease
inflammatory cell mediator release, plasma extravasation, and the
sensitization of afferent terminal.
-
OpioidsPlace in Therapy • Strong evidence in supporting the
short-term use of opiates in managing BUT long-term use for
non-
cancer pain is not strong.• Current recommendations for
initiating chronic opiate therapy are intended to better identify
patients
at risk for abusing and/or misusing opiate medications or from
suffering their adverse physical effects. This includes a detailed
medical history, psychiatric history, and substance use history as
well as establishing a physical diagnosis and the medical necessity
for chronic opiate therapy. Urine drug screening as well as
establishing an agreement between the provider and patient in which
the goals and expectations of the therapy are clearly stated
reduces misuse, abuse, or diversion of opiate medications.
Comments/Concerns Unwanted adverse effects, such as opioid
tolerance, dependence, constipation,respiratory depression,
impaired cognitive ability, immune suppression, andopioid-related
endocrinopathies, are only some of the known physical
alterationsassociated with the chronic use of opiate
medications.
-
Cost of chronic pain adds up to 635 billion each year.
It affects over 100 million adults.
About 41% of chronic pain patients reports that their pain is
uncontrolled.
Facts about Chronic pain and Opioid treatment
-
Legislation and Regulatory Policies Should Limit Inappropriate
Prescribing But Should Not Discourage Or Prevent Prescription Of
Opioids Where Medically Indicated And Appropriately Managed.
Prescription Of Opioids For Chronic, Intractable Pain Is
Appropriate When More Conservative Methods Are Ineffective And The
Treatment Plan Is Reasonably Designed To Avoid Diversion,
Addiction, And Other Adverse Effects.
Physicians Should Be Sensitive To And Seek To Minimize The Risks
Of Addiction, Respiratory Depression And Other Adverse Effects,
Tolerance, And Diversion. However, Some Commonly Held Assumptions
About These Issues Need To Be Reviewed.
Opioids Should Be Prescribed Only After A Thorough Evaluation Of
The Patient, Consideration Of Alternatives, Development Of A
Treatment Plan Tailored To The Needs Of The Patient And
Minimization of Adverse Effects, And On-Going Monitoring And
Documentation.
Use of Opioids for the Treatment of Chronic Pain
Use of Opioids for the Treatment of Chronic Pain. American
Academy of Pain Medicine. 2013.
http://www.painmed.org/files/use-of-opioids-for-the-treatment-of-chronic-pain.pdf.
Accessed August 3, 2016
http://www.painmed.org/files/use-of-opioids-for-the-treatment-of-chronic-pain.pdf
-
Why do you think prescribing opioids could be challenging for
doctors?
What do you think is the role of a pharmacist is in opioid
dispensing?
Questions to Think about?
-
Challenging◦Why?
◦ Under prescribing: due to fear of adverse effects as well as
addiction.
◦ Over prescribing: due to multiple failed therapeutic
response.
Issues with prescribing opioids.
-
Agents of choice for moderate to severe chronic pain as well as
cancer related chronic pain
Dosing is based on patient’s previous history of opioid
analgesic used, the specific patient’s needs, and on the delivery
system being utilized.
Classified by:◦ Activity at the receptor site
◦ Pain intensity treated
◦ Duration of action (short acting vs. long acting)
Opioids
-
Patient is experiencing pain despite having a reasonable trial
of both non-opioid analgesics and adjuvants
Severe pain that requires rapid relief
Patient has contraindication to the use of other analgesics
Patient Selection
-
Patient selection Opioid regimen should be individualized
Opioid naïve patients should be started on low dose
In July 2012, FDA requires REMS for all extended release and
long acting opioid analgesics.
-
Generic Brand Agonist/antagonist or mixed
Histamine release that would cause N/V/itchiness
Route of Administration
Comments
Morphine Avinza Morphine like Agonist +++ IM, PO, IV, SR, Rectal
Drug of choice for severe pain
Hydromorphone Dilaudid, Exalgo Morphine like Agonist IM, PO, IV,
rectal Use in severe pain, more potent than morphineREMS
program
Oxymorphone Opana Morphine like Agonist IM, IV, SQ, PO Severe
pain, immediate with controlled, extended release to stop
misuse
Codeine Morphine like Agonist +++ IM, PO CODEINE is metabolized
by CYP2D6
Hydrocodone Norco Morphine like Agonist PO most effective when
used with aspirin and acetaminophen,
Oxycodone Oxycontin, oxecta, Roxicodone
Morphine like agonist PO
Meperidine Demerol Meperidine like agonist +++ IM, PO Severe
pain, oral is not recommended, should not be used for chronic
pain
Commonly Prescribed Opioids
-
Generic Brand Agonist/antagonist or mixed
Histamine release that would cause N/V/itchiness
Route of Administration
Comments
Fentanyl Sublimaze, duragesic, lazanda, abstral. Actiq, onsolis,
fentora, subsys
Meperidine like agonist IM, transdermal, buccal, transmucosal,
sublingual, nasal inhaled
Severe pain, do not use patch in acute pain, always titrate the
dose, can be used for breakthrough pain; TM, IN, SL are available
through a REMS program.
Methadone Dolophine NMDA antagonistSNRI
IM/IV, PO Reverse opioid tolerance
Naloxone Narcan Antagonist IV
Tramadol Ultram, Antagonist Inhibits reuptake of serotonin and
ER , used for neuropathic pain
PO Decreased dose in renally and hepatic insufficient patients
and elderly.
Tapentadol Nucynta Antagonist PO REMS required.
Commonly Prescribed opioids
-
Frequency Stage of Pain
Around THE CLOCK (QD, BID etc.) Initial stage of pain Persistent
chronic pain
As needed (prn) As the painful state subsides and the need for
medication is decreased.Also for patients that may present with
pain that is intermittent or sporadic in nature.
Around the clock and as needed (conjunction)
When patient experiences breakthrough pain.
Administration of Opioids
-
Route of Administration When to Uses
Oral (PO) Mostly commonly used and preferred method in most
cases
Continuous IV infusion Postoperative pain
Epidural or intrathecal/ subarachnoid Control of acute, chronic
non-cancer, and cancer pain
Route of Administration
-
Before initiating chronic opioid therapy, must assess risk vs.
benefit for the patient.
Based on history, physical examination, assessment of risk of
substance abuse, misuse or addiction.
Personal and family history of alcohol or drug abuse
Personal history of alcohol or drug abuse may be considered
contraindicated for long term opioid therapy.
Evaluation prior to initiating Opioid regimen
-
DefinitionPhysical dependence- rapid discontinuation of opioid
following prolonged administration, usually one month or longer,
will result in withdrawal symptoms such as dysphoria, anxiety, and
volatility of mood, as well as physical findings such as
hypertension, tachycardia, and sweating.
Tolerance- is present when increasing amounts of opioid are
required to produce an equivalent level of efficacy
Addiction- is a form of physiological dependence and refers to
the extreme behavior patterns that are associated with procuring
and consuming the drug.
-
Effect Manifestation
Mood changes Dysphoria, euphoria
Somnolence Lethargy, drowsiness, apathy, inability to
concentrate
Stimulation of chemoreceptor trigger zone Nausea, vomiting
Respiratory depression Decreased respiratory rate
Decreased gastrointestinal motility Constipation
Increase in sphincter tone Biliary spasm, urinary retention
Histamine release pruritus,
Tolerance Larger doses for same effect
Dependence Withdrawal symptoms upon abrupt discontinuation
Major Adverse effects of opioid analgesics
-
Monitoring should occur during each visit
Documentation of pain intensity, functional status, progress
toward therapy goals, side effects and adherence is critical.
Monitoring of Chronic Pain Management
-
Help minimize risk for patients using pain medications.◦ Assess
and properly plan to minimize patient risk of Pain Medicine
◦ Proper Pain Assessment to understand pain and provide highly
effective treatment while minimizing risk
◦ Educate the patients of the role of opioids in the treatment
of chronic pain
Help patients live meaningful and productive lives with
adequately managed pain
Monitor patient’s 4 As:◦ Analgesia
◦ Activities of daily living
◦ Adverse events
◦ Aberrant drug behaviors
Revisit a Pharmacist’s Role in Chronic Pain Management
-
A. Provide rapid pain relief or reduction in pain intensity is
NOT the Goal
B. Report providers of the authorities who prescribe opioids to
the authorities
C. Help patients live meaningful and productive lives with
adequately managed pain
D. Manage patient’s chronic pain with the use of non-opioids
Which of the following statement describes the role of a
pharmacist in chronic pain management?
-
A. Norco
B. Morphine
C. Duloxetine
D. Pregabalin
What is the preferred drug of choice in the treatment of chronic
neuropathic pain?
-
A. NSAID
B. Antidepressant
C. Anticonvulsant
D. Cannabinoids
The addition of this class of pain medication has shown to have
an opioid-sparing effect of between 20-35%.
-
Appropriate Opioid Use. Pharmacist’s Letter. 2015;
31(4):310407.
ACPA Recourse Guide to Chronic Pain Treatment: An Integrated
Guide to Physical, Behavioral and Pharmacologic Therapy. 2016.
https://theacpa.org/uploads/documents/ACPA_Resource_Guide_2016.pdf.
Accessed August 10, 2016.
Barbee J, Chessher Jaclyn, Greenlee, Max. Pain Management: The
Pharmacist’s Evolving Role. Pharmacy Times. 2015.
http://www.pharmacytimes.com/publications/health-system-edition/2015/july2015/pain-management-the-pharmacists-evolving-role.
Accessed July 5, 2016.
Baumann TJ, Herndon CM, Strickland JM. Chapter 44. Pain
Management. In:DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG,
Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 9e. New
York, NY: McGraw-Hill; 2014.
http://accesspharmacy.mhmedical.com/content.aspx?bookid=689&Sectionid=45310494.
Accessed August 16, 2016.
Beal BR, Wallace MS. An Overview of Pharmacologic Management of
Chronic Pain. Med Clin North Am. 2016;100(1):65-79.
Pain: Hope Through Research. Available at:
http://www.ninds.nih.gov/disorders/chronic_pain/detail_chronic_pain.htm#3084_15.
Accessed August 5, 2016.
Use of Opioids for the Treatment of Chronic Pain. American
Academy of Pain Medicine. 2013.
http://www.painmed.org/files/use-of-opioids-for-the-treatment-of-chronic-pain.pdf.
Accessed August 3, 2016
References
https://theacpa.org/uploads/documents/ACPA_Resource_Guide_2016.pdfhttp://www.pharmacytimes.com/publications/health-system-edition/2015/july2015/pain-management-the-pharmacists-evolving-rolehttp://www.painmed.org/files/use-of-opioids-for-the-treatment-of-chronic-pain.pdf
-
1. Write down the course code. Space has been provided in the
daily program-at-a-glance sections of your program book.
2. To claim credit: Go to www.cshp.org/cpe before December 1,
2016.
Session Code: