Embed Size (px)
Citation preview

S4 Journal of Pain and Symptom Management Vol. 38 No. 2S August 2009
Special Article
Chronic Pain Management in Older Adults:Special ConsiderationsPerry G. Fine, MDPain Research Center, Department of Anesthesiology, University of Utah School of Medicine, Salt Lake
City, Utah, USA
Abstract
The rising prevalence of neuropathic pain and the multifaceted sequelae of pain particularlywithin older adults are part of the increasing challenges in providing good geriatric painmanagement. Aging can lead to a higher sensitivity to pain within older adults, whereasphysiological changes modify the absorption, bioavailability, and transit time ofpharmaceutical agents. Ultimately, these differences within older adults require clinicianstreating them to provide individually tailored analgesic approaches. Progressive age increasesthe variance in physiology among people; thus, the management approach should reflect anindividual’s unique requirements and limitations based on findings at the time ofassessment. J Pain Symptom Manage 2009;38:S4eS14. � 2009 U.S. Cancer PainRelief Committee. Published by Elsevier Inc. All rights reserved.Key Words
Analgesia, assessment, guidelines, inappropriate prescribing, older adults, side effectsThe Epidemiology of Neuropathic Painin Older Adults
Neuropathic pain, defined as pain arising asa direct consequence of a lesion or diseaseaffecting the somatosensory system, is a conse-quence of various diseases and conditions,most commonly diabetes, herpes zoster infec-tions, cancer, arthritis, and back injuries.1,2
Older adults are particularly prone to chronicpainful conditions, especially arthritis, degener-ative spine disease, peripheral neuropathies,and bone and joint disorders.3 Because of theincreasing prevalence of diabetes, the incidenceof painful diabetic neuropathy is increasing.4
Address correspondence to: Perry G. Fine, MD, PainResearch Center, Suite 200, 615 Arapeen Drive,Salt Lake City, UT 84108, USA. E-mail: [email protected]
Accepted for publication: May 20, 2009.
� 2009 U.S. Cancer Pain Relief CommitteePublished by Elsevier Inc. All rights reserved.
Overall, there is a distinct lack of data de-scribing the prevalence of neuropathic painwithin the general American population.Most recently, a 1998 study estimated that3.8 million Americans suffered from this disor-der.5 Surveys conducted in the United King-dom and France within the last three yearsindicated a 7%e8% prevalence,6 and a compa-rable prevalence of neuropathic pain withinthe United States would affect as many as 24million Americans. Predictably, as the percent-age of older adults increases within the overallpopulation because of aging of the ‘‘BabyBoomer’’ generation, so will the prevalenceof neuropathic pain. This demographic shiftis a global phenomenon, with estimates that,by the year 2025, approximately 1.2 billionpeople worldwide will be aged 60 years orolder.7 An Austrian prospective surveyfound an eightfold higher prevalence rate ofneuropathic pain among 51- to 60-year-old
0885-3924/09/$esee front matterdoi:10.1016/j.jpainsymman.2009.05.002

Vol. 38 No. 2S August 2009 S5Chronic Pain Management in Older Adults
participants (24%) than within the generalAustrian population (3%).8
Furthermore, chronic pain of all causeshas reached epidemic proportions within theUnited States, as an estimated 50 million Amer-icans suffer from daily chronic pain and fourout of 10 patients treated do not receive ade-quate relief.9 Moreover, a survey conductedfrom 1999 to 2001 of 2,779 adults in homecare aged 65 years or older found that approxi-mately 48% (n¼ 1,329) of the participantsexperienced daily pain, and one-fifth (21.6%)of this group received no analgesic.10 Substan-tial pain is often undertreated, especially in old-er adults and even more commonly in nursinghome residents.3
Patient perceptions of suboptimal pain man-agement have caused one out of four sufferersof chronic pain of all ages in the United Statesto change doctors at least three times since theirinitial visit.11 This highlights the need for coor-dinated interdisciplinary care of chronic pain,especially including the involvement of primarycare practitioners (PCPs). Seventy-nine percentof individuals that regularly take pain medica-tions see PCPs.3 The need to better educatefamily physicians and nurse practitioners aboutmanaging chronic pain in particular12 is illus-trated by considering the very low ratio ofboard-certified pain specialists to patients withchronic pain (four to six per 100,000),13 dem-onstrating the impossibility of providing skillfulpain management by pain specialists alone.Furthermore, the number of certified geriatri-ciansdapproximately one per 5,000 Americansaged 65 years and olderdfalls far short of thecurrent need.14 Although substantial progresshas been made in the field of geriatric medicinein the past three decades, further collaborationsamong medical professionals of various fieldswill be required to meet the needs of the rapidlyincreasing U.S. population aged 65 years andolder, which is predicted to exceed 70 millionby year 2030.14
Persistent pain can have striking conse-quences on an individual’s quality of life. A2007 self-report questionnaire taken by 260individuals of all ages with neuropathic painresponded that their pain ‘‘strongly/mostly’’restricted daily activities and disturbed sleepin 65% and 60% of those surveyed, respec-tively.8 Other common sequelae of chronicpain in older adults include depression and
anxiety, as well as reduced socialization and im-paired ambulation.3
Pain and the Biology of AgingWith advancing age, the perception of pain is
altered, which may be related in part to brain at-rophy.13 However, studies of brain activity com-paring young (26� 3 years) and older (79� 4years) individuals after administration of nox-ious pressure indicate that other mechanismsalso may lead to greater sensitivity to pain (i.e.,a lower pain threshold) within older adults.The involvement of central endogenous pain in-hibitory systems was linked to reduced toleranceto pain with advancing age by magnetic reso-nance imaging data, which showed the loweredactivity of structures involved in pain process-ing, such as the contralateral caudate and puta-men, in older adults.15 These changes could notbe fully explained by age-related reductions intissue volumes of the striatal structures.
Aging and associated diseases affect gastroin-testinal anatomy and physiological processes,including motility, secretions, blood flow, andabsorptive surface.16 These changes can havean effect on drug absorption, bioavailability,and transit time, as can reductions in plasmaalbumin, increased fat to lean mass ratios, anddecreased total body water.16,17 In addition,liver mass, liver blood flow, and the glomerularfiltration rate of the kidneys decrease with age.Of particular clinical importance, reducedrenal clearance leads to a decline in the excre-tion of water-soluble drugs.17 Lowered activitiesof most of the cytochrome P450 enzymes alsoreduce the drug-elimination clearance rate ofthe liver, especially in the presence of chronicdisease.15
Aging also leads to degenerative changeswithin all structures of the spine, involving bio-chemical, microstructural, and gross structuralalterations that can lead to pain.18 Nociceptorswithin degenerated discs can be a source oflow back pain, whereas facet hypertrophy andenlargement of the ligamentum flavum com-bine to narrow the spinal canal and are themain causes of neurogenic claudication andradiculopathy in older adults. In addition, age-associated osteoporosis weakens bones by in-ducing remodeling and rotatory deformities.18
Finally, because aging affects individuals dif-ferently, particular attention to individualized

S6 Vol. 38 No. 2S August 2009Fine
treatment is required in older adults basedon findings at the time of assessment. Progres-sive age increases the variance in physiologyamong people; thus, the managementapproach should reflect an individual’s uniquerequirements and limitations.
The Assessment of Painin Older Adult Populations
Because of certain obstacles associated withboth diagnosis and treatment, pain is particu-larly inadequately controlled in older adults.Pain assessment can be adversely affectedby many factors, including patient cognitiveimpairment, patient reluctance to discloserelevant symptoms, and the overlap of pain-related behaviors with those of dementingillnesses and/or depression. Some olderpatients fail to self-report pain because of be-liefs that pain is an inescapable element of ag-ing or part of their atonement for pastfailings.3 Some individuals avoid medical carebecause of fears about the implications ofpain as a signal of a serious illness, or trepida-tion over diagnostic tests, whereas the use ofstrong analgesics can be hindered by patientfears of side effects or addiction.
In addition, patient cognitive impairmentcan have a detrimental impact on painassessment.19e22 A study of 181 nursing homepatients found that individuals with variouscauses of dementia had significantly morepain, yet received less analgesia than cognitivelyhealthy controls (P< 0.005).19 Another study ofnursing home residents in Canada concludedthat the presence of cognitive impairment didnot alter the prevalence of conditions likely tocause pain, nor an individual’s sensitivity topain, but the prevalence of identified painamong patients with cognitive impairment waslower.20 Moreover, patients with cognitive defi-cits are subject to delayed or incorrect diagnoses,and treatments to control problematic behaviorsthat are associated with burdensome adverse ef-fects and complications, such as delirium, boweldysfunction, and prolonged hospital stays.21 Cer-tainly, the potential diagnostic complications,the risk of negative outcomes, and prevalenceof uncontrolled pain underscore the impor-tance of conducting both a thorough cognitiveevaluation and pain assessment.21
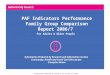
Despite the lack of widespread use of formaltools to assess pain in patients who have cogni-tive impairment, its integration into painassessment has been supported in recentbest-practice guidelines.22 Selection of anappropriate pain scale is critical, as those thatmeasure social behaviors (e.g., communication,social interactions) and symptoms shared withdepression (e.g., sleep and appetite distur-bance) may yield results that are confoundedby delirium/depression.22 A 2007 publicationdetailed the consensus recommendations ofan interdisciplinary panel of experts for assess-ment of pain in older adults.23 Specific recom-mendations were given regarding multiplepotential aspects of a comprehensive diagnosticworkup for an older adult, including a thoroughmedical and pain history with a detailed medica-tion review, use of self-report procedures forassessing pain, special pain assessment ap-proaches for patients with dementia, functionalassessment evaluation, assessment of emotionalfunctioning, special issues relating to neuro-pathic and nociceptive pain symptoms andsigns, and a general and focused physical/neu-rological examination (Fig. 1). Commonlyencountered pain problems during a physicalexamination of an older adult were listedaccording to their associated disease/condition(Table 1), and specific assessment tool recom-mendations were discussed.23 Validated toolsare available, such as the short-form McGillPain Questionnaire and the Brief Pain Inven-tory, that can be administered in 10 minutesand provide a reliable assessment of pain quali-ties, intensity, interference with function (phys-ical, relational, and psychological), location,medication use, and perceived relief frompain (Table 2).23
Pain Treatment Guidelinesfor Older Adults
Collectively, the currently available random-ized controlled trial data in the literature caneffectively guide the management of patientspresenting with neuropathic pain. The firstevidence-based algorithm for treating neuro-pathic pain was synthesized in 2005 by painspecialists in Denmark,24 followedbya worldwidecollaboration under the auspices of theInternational Association for the Study of Pain,which created an evidence-based set of

Behavioral Observationsof Pain
UnidimensionalMeasures
MultidimensionalMeasures
Self Reports of PainInitial determinationand/or ongoingmonitoring of pain
Inflammation
Pain AssessmentDuring Physical Exam
Physical Examination
FunctionalAssessment
PharmacologyAssessment
Sensory Impairment
Age-SpecificPhysical Concerns
Medical,pharmacological,and functionalassessment of pain-related concerns
Personality
Coping
Psychosocial Comorbidities &Complicating Factors
Affective Processes
Pain-relatedDisability
InterpersonalProcesses
General Site-Specific
CognitiveProcesses
General Pain-Specific
Psychological Well-Being
Assessment ofpsychosocialfactors contributingto pain complaint
Fig. 1. Aspects of a comprehensive pain assessment.23
Vol. 38 No. 2S August 2009 S7Chronic Pain Management in Older Adults
recommendations in 2007.25 Pharmacothera-peutic recommendations include the use of anti-convulsants, sodium channel modulators,antidepressants, and m-receptor agonist anddual-mechanism opioid analgesics, as well assome other miscellaneous agents (Table 3).Both guidelines recommend tricyclic antidepres-sants (TCAs) and the calcium channel a2-dligands, gabapentin, and pregabalin.24,25 Trama-dol and pure m opioids are generally recommen-ded as second-line options because of theirpotential side effects, with the exception of cer-tain clinical circumstances where they may bepreferred as first-line agents.24,25 Still, these rec-ommendations were developed based on evi-dence mainly generated from younger cohorts;specific treatment recommendations for neuro-pathic pain tailored for the needs of older adultsis thoroughly discussed in the following article inthis supplement, ‘‘Pharmacological Manage-ment of Neuropathic Pain in Older Adults: AnUpdate on Peripherally and Centrally ActingAgents.’’
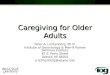
Because of the highly variable signs and symp-toms associated with neuropathic pain, the bestmanagement strategy derives from identifyingthe underlying disease process and then tailor-ing the treatment to the presenting pain condi-tion, whenever possible. Toward this end,current pain management algorithms subdi-vide neuropathic pain into peripheral andcentral subtypes. Originally, topical lidocainewas recommended as a first-line agent only forpostherpetic neuralgia and focal neuropathy,24
but more recent guidelines expand the recom-mended uses of this modality to peripherallocalized neuropathic pain (Fig. 2).25 For cen-tral neuropathies, TCAs are considered first-line agents; however, in older adults (especiallythose who have had a stroke), TCAs are oftennot well tolerated and, therefore, gabapentinor pregabalin is recommended (Fig. 3).24 It isanticipated that future editions of guidelinesfor pain in older patients will place strong cau-tions against the use of TCAs in the geriatricpopulation because of common and potentially

Table 1Typical Findings from the Physical Evaluation for Common Pain Issues in Older Adults23
Common Pain Problems Findings Comments
Nociceptive conditions (e.g., osteoarthritisof the spine and weight-bearing joints)
Localized and referred pain; usually deep and aching.Radiographic findings are usually pathognomonic.
Depending on the disorder being evaluated, physicalexamination findings (i.e., reduced range of motion) maybe weakly associated with pain.
Neuropathic conditionsHerpetic neuralgia Symptoms often appear before rash. Physical findings may be
unrevealing before rash. Rash is an acute inflammatory skinreaction with typical nociceptive pain superimposed onneuropathic symptoms.
Decreased sensory thresholds can be observed in intact skin inthe area of the rash, although scarring can lead to areas ofhypoesthesia.
Postherpetic neuralgia Diminished primary sensory modalities, greater in worstaffected areas.
Allodynia, hyperalgesia, and hyperpathia may be present.
Allodynia is pain elicited by gentle brushing or application ofcool or warm stimuli.
Hyperalgesia is increased response to a painful stimulus.Hyperpathia is associated with an increased reaction to
a stimulus, especially a repetitive stimulus, and a decreasedthreshold. The pain is often explosive.
Central post-stroke pain Reduction in spinothalamic function (warm and cold).Frequently associated with allodynia, hyperalgesia, and
hyperpathia.Posterior column function (vibration and position sense) is
preserved.There may be proximal referral of pain.
Proximal referral of paindpressure over a distal site in handor foot may be felt in the shoulder or upper limb orproximal thigh.
Trigeminal neuralgia Sensory examination of the face is normal. Pain may bespontaneous or precipitated by non-noxious stimuli.
Pain paroxysmal with short volleys.
Radicular and referred pain secondaryto degenerative disease of the spine
Reduced range of movement of the spine.Focal mechanical hyperalgesia, neurologic signs in affected
areas.Nerve stretch, such as straight leg raises, may evoke or
exacerbate pain.Painful peripheral neuropathy Sensory abnormalities in affected limbs. Hyperalgesia and
hyperpathia may be present. Occurs in w20%e25% ofpatients. Abnormalities may be thermal only in nature.
Lower limbs are more likely to be affected than upper limbs,in a glove and stocking distribution.
S8V
ol.3
8N
o.2
SA
ugu
st2
00
9Fin
e

Table 2Consensus Recommendations for Seniors with Limitations in Ability to Communicate Because of Dementia23
General recommendations1. Take into account patient history, interview information, and results of physical examinations.2. Use assessment approaches that include both self-report and observational measures when possible.3. The CAS, the 21-point box scale or NRS and the VDS should be attempted with seniors whose cognitive functioning ranges
from intact to mildly or moderately impaired. The FPS is an alternate tool that is preferred by some older persons, particularlyAfrican Americans and Asians.
4. At this point, assessment scales are under development and consensus could not be reached regarding the definitiverecommendation of any particular scale. The PACSLAC seems to be a promising tool for assessing pain among persons withcognitive impairments. Nonetheless, more research regarding the psychometric properties of this tool is needed. Althoughthe initial psychometric findings are encouraging, the scale should be used with caution until additional data becomeavailable. Among the shorter instruments, the Doloplus seems to be promising. Further research undertaking a directcomparison of various observer rated scales is needed to identify the relative strengths and weaknesses of currently availabletools.
5. Pain assessment during a movement-based task is more likely to identify an underlying persistent pain problem and offersenhanced measurement sensitivity and specificity.
6. Examine whether the use of analgesic medications leads to a reduction of behavioral indicators of pain.7. A comprehensive pain assessment also should include evaluations of other related aspects of patient functioning (e.g., mood,
quality of life, coping resources, social support).8. Among persons with dementia, it would be important to solicit the assistance of a knowledgeable informant to accomplish
this goal and identify typical pain behaviors for the individual patient.9. Several instruments contain items that need to be assessed over time (e.g., changes in sleeping, eating). With the possible
exceptions of the PADE and the NOPPAIN, this should not preclude their use in primary care settings because the health careprovider may solicit the assistance of caregivers in completing these tools.
Specific recommendations following the selection of suitable assessment tools10. Use an individualized approach collecting baseline scores for each patient.11. Solicit the assistance of caregivers familiar with the patients.12. If assessment tools are used to monitor pain levels over time, they must be used under consistent circumstances (e.g., during
a structured program of physiotherapy, over the course of a typical evening).13. Most of the assessment tools reviewed in this section are screening instruments and, as such, they cannot be considered to
represent definitive indicators of pain.
CAS¼ Colored Analog Scale; FPS¼ Functional Pain Scale; NOPPAIN¼Noncommunicative Patient’s Pain Assessment Instrument;PACSLAC¼ Pain Assessment Checklist for Seniors with Limited Ability to Communicate; PADE¼ Pain Assessment for the Dementing Elderly;VDS¼ Verbal Descriptor Scale.
Vol. 38 No. 2S August 2009 S9Chronic Pain Management in Older Adults
highly deleterious adverse effects (Ferrell B,American Geriatrics Society [AGS] Pain Guide-line Chair, personal communication). It isnoteworthy that more recent guidelines recom-mend selective serotonin and norepinephrinereuptake inhibitors for first-line treatment ofneuropathic pain.25 In many cases, combina-tions of the aforementioned drugs are the main-stay of current therapy for chronic pain; thisstrategy can allow lower doses of each class ofdrug, providing synergistic or additive thera-peutic effects along with reductions in dose-limiting adverse effects. However, because ofthe increased likelihood of drug-drug anddrug-disease interactions in older adults witheach additional medication taken, frequentmonitoring is critical within this population.3
A key strategy when prescribing medicationsfor older adults is to ‘‘start low and go slow’’when initiating and titrating pharmacother-apies. Overall, the first-line agents have demon-strated similar efficacies for treating multipletypes of neuropathic pain; therefore, sideeffects and drug interactions are a primary
consideration when choosing treatments forolder adults.26,27
As a corollary, topical agents should be con-sidered as a single therapy or a coadjuvant inparticular for the older adult population, as sig-nificant analgesia can be obtained with minimalside effects.28 As an example, side effects associ-ated with the lidocaine patch 5% tend to benonsystemic, mild to moderate in nature, andmost commonly limited to application-site reac-tions,29,30 thus making this topical analgesica good option for older adult populations.This, and even compounded topical creams/ointments, are preferred alternatives for olderadults (except, perhaps, in the treatment of anacute severe pain crisis) before trying othertypes of systemically active medications.
The number needed to treat (NNT) andnumber needed to treat to harm (NNH) statis-tics for agents used in the treatment of neuro-pathic pain offer a comparison of the efficacyand safety, respectively, of the treatment alterna-tives.24,31 The NNT is ‘‘the number of patientsneeded to treat with a specific drug to obtain

Table 3Recommended Medication Groups
for Treating Neuropathic Pain
Anticonvulsants� Pregabalin� Gabapentin� Carbamazepine� Lamotrigine� Valproic acid
Antidepressants� Tricyclicsdamitriptyline, nortriptyline, desipramine,
imipramine, clomipramine� SNRIsdduloxetine, venlafaxine, desvenlafaxine� Mirtazapine
Opioid receptor-binding analgesics� Mixed-mechanism: tramadol, tapentadol� Partial agonist: buprenorphine� m agonist: fentanyl, hydrocodone, hydromorphone,
levorphanol, methadone, morphine, oxycodone,oxymorphone
Sodium channel modulators� Lidocaine patch 5%� Mexiletine
Other agents� a2-Receptor agonist: clonidine, tizanidine� NMDA receptor antagonist: ketamine, memantine� Cannabinoid receptor agonist: cannabinoids� Vanilloid receptor ligands: topical capsaicin
SNRI¼ serotonin and norepinephrine reuptake inhibitors;NMDA ¼ N-methyl-D-aspartate.
S10 Vol. 38 No. 2S August 2009Fine
1 patient with a defined degree of pain relief.’’31
Typically, NNTs range between 3.7 and 5patients for the first-line agents, which illus-trates the need to use combination therapeutic
Lidocaine patch
noyes Postherpetic neuralgiaand focal neuropathy
Peripheral neuropathic
Gabapentin/pregabalin
TCA(SNR)
TCA contraindication
T
no
Fig. 2. An evidence-based algorithm for trea
approaches when managing patients with neu-ropathic pain to provide adequate analgesia.The NNT data for analgesics provided evidencetoward generating a treatment algorithm forneuropathic pain, most recently in 2007.31 Fur-thermore, NNH data for a number of analgesicshave been reported in several Cochrane Collab-orative reviews. The results within the 95% con-fidence interval (CI) for minor harm associatedwith anticonvulsants used to treat acute andchronic pain were: 3.7 (95% CI: 2.4e7.8) forcarbamazepine; 2.5 (95% CI: 2.0e3.2) for gaba-pentin; and 3.2 (95% CI: 2.1e6.3) for pheny-toin.32 The NNH for major adverse effects(i.e., an event leading to withdrawal froma study) associated with TCA agents used to treatneuropathic pain was 28 for amitriptyline (95%CI: 17.6e68.9) and 16.2 for venlafaxine (95%CI: 8e436). The NNH for minor adverse effectswas 6 for amitriptyline (95% CI: 4.2e10.7), and9.6 for venlafaxine (95% CI: 3.5e13).32 In com-parison, the NNHs for opioids used to relieveneuropathic pain were calculated comparedwith an active control or placebo for the mostcommon opioid-related side effects. The NNHfor both nausea and constipation was 4.2 (33%opioid vs. 9% control), 6.2 for drowsiness(29% opioid vs. 12% control), 7.1 for dizziness(21% opioid vs. 6% control), and 8.3 for vomit-ing (15% opioid vs. 3% control).33
pain
Gabapentin/pregabalin
TCA(SNR)
TCA contraindication
ramadol, oxycodone
yes
no
yes
ting peripheral neuropathic pain.24

Lidocaine patch
and
recommendations
as before
TCA
(SNRI)
Gabapentin/
Pregabalin
Gabapentin/
Pregabalin
Central neuropathic pain
yes
TCA
(SNRI)
yes
Tramadol, Opioids
TCA
contra-
indication
noyesTCA
contra-indication
no
no
Fig. 3. An evidence-based algorithm for treating central neuropathic pain.24
Vol. 38 No. 2S August 2009 S11Chronic Pain Management in Older Adults
A consensus statement on prescribing opi-oids for older adults who have pain was createdby an international panel of experts in 2008.34
Although no studies with older adult cohortshave been published, growing evidence sup-ports the use of opioids for chronic noncancerpain. A sound principle of practice is thatdose titration needs to be individually consid-ered and tailored based on the pharmacoki-netics of the drug, its formulation, and thespecific medical/social circumstances of eachpatient.34 Also, because renal and hepaticfunction typically decline with advancing age,the duration of the activity of most opioidsand their metabolites may be prolonged. Inolder patients, the potential for drug accumu-lation and increased central nervous system(CNS) sensitivity increase the risks for cogni-tive impairment and respiratory depression,especially in conjunction with concomitantCNS medications or with an underlying pul-monary condition.34
Polypharmacy can be a confounding riskfactor when prescribing pain medications, espe-cially for older adults, as members of this popu-lation commonly require multiple medications.In fact, individuals aged 60 years or older areprovided with an average of 40.8 prescriptionsper year, according to the 2006 findings of a Brit-ish National Health Service study.17,35 With poly-pharmacy, dose-limiting adverse effects of pain-relieving drugs may limit the potential achiev-able efficacy. This tends to be the major
limitation for treating the aging population. Fur-thermore, the incidence of adverse effects is di-rectly correlated to the number of prescribingphysicians involved in the care of older adults.36
Therefore, all medicationsdespecially CNSactive drugsdshould be reviewed routinely todetermine which ones, if any, could be discon-tinued or reduced in dosage.
Treatment adherence among older adultpatients is influenced by perceptions.37 Forinstance, the decision to take an analgesic isaffected by fear of side effects, other illnesses,the characteristics of the pain, family membersupport, and the information provided to thepatient by health care professionals andothers. Among older adults, medication costhas a powerful impact on adherence to a pre-scription, especially with individuals who havepoor health, multiple morbidities, and limiteddrug coverage through insurance.38
Inappropriate Prescribingfor Older Adults
Inappropriate medications have been de-fined as ‘‘drugs that pose more risks than bene-fits to patients, and for which there is a goodalternative drug available.’’39,40 The consensusguideline for inappropriate medications forolder adults, otherwise known as the Beerscriteria, was first published in 1991 and lastupdated in 2003.41,42 These recommendations,

S12 Vol. 38 No. 2S August 2009Fine
compiled by a panel of experts, list the drugsthat are particularly problematic for olderadults,42e44 although they are not comprehen-sive and need updating.45 According to themost current version of the Beers criteria, inap-propriate analgesic medications because ofage-associated increased incidences of adverseevents include TCAs (particularly in patientswith glaucoma), nonsteroidal anti-inflamma-tory drugs (especially in hypertensive patientsand those who have had heart attacks or chronicrenal failure), and propoxyphene.44,45 Basedon the details described in the most recentguidelines, the most frequently prescribed inap-propriate analgesics include long-acting benzo-diazepines and amitriptyline. A significantlyhigher risk of bone fractures has been linkedto higher doses of benzodiazepines and a longerduration of use (14e90 days) in a population-based cohort study of 7,983 older adults (oddsratio: 3.45; 95% CI: 1.38e8.59).46
According to recent publications, inappro-priate prescribing for older adults is a substan-tial problem.40,44 An observational study ofacute admissions of older adults found thatinappropriate prescribing occurred in 32% ofpatients (n¼ 191), and 49% of these patientswere admitted with adverse effects because ofthe inappropriate medications.44 A Norwegianstudy of 454 general practitioners who treated85,836 patients aged 70 years or older foundthat 18.4% of these patients received at leastone potentially harmful prescription.47 Poly-pharmacy and hospitalization were associatedwith inappropriate prescribing. A nationalsurvey assessed the impact of inappropriate pre-scribing on patient outcomes using the MedicalExpenditure Panel Survey data collected in1996.39 Older adults who used inappropriateprescriptions reported a significantly worsehealth status than individuals who were notusing inappropriate medications (P< 0.01).39
Recent studies have indicated that inappro-priate prescribing can be reduced throughimplementation of multiple types of methodol-ogies. A Cochrane review concluded that educa-tional outreach is a promising approach toimprove the prescribing practices of healthcare professionals.48 A study of 2,753 outpatientveterans aged 65 years and older, who wereprescribed at least one high-risk medication,considered a twofold approach to reduce inap-propriate prescribing.49 Real-time warnings
were combined with personally addressedletters from the chief medical officer askingprescribing clinicians to discontinue treatmentwith high-risk medications, along with a copy ofthe Beers criteria article, a list of suggestedalternatives, and a list of older patients receivingthe high-risk medications who had upcomingappointments. After the intervention, approxi-mately 50% of the patients studied had theirhigh-risk medications discontinued, which sig-nificantly decreased the number of patients pre-scribed high-risk medications (P< 0.001).
Another strategy that has been demon-strated to reduce inappropriate prescribing isthat of generating quarterly practice perfor-mance reports followed by onsite visits.50 Arecent discussion of approaches for reducinginappropriate prescribing noted that multidis-ciplinary teams, including a geriatrician andother health care clinicians with specializedgeriatrics training, pharmacists, and computer-ized decision support, improved the quality ofprescribing to older adults.51
What We Know and Do Not KnowAbout Pain in Older Adults
Chronic pain has reached epidemic propor-tions, particularly among older adults, whereasinappropriate prescribing for older adults isa substantial, yet manageable problem.Specifically within this population, side effects,drug-drug interactions, cognitive and socialproblems, and patient nonadherence to treat-ment because of perceptions and drug costhave limited the attainment of effective analge-sia. Yet, with focused skill building andattention to guideline recommendations, sig-nificant improvements in pain managementfor older adults are imminently achievable. Im-portantly, treatments should be individualizedand monitored regularly in older-aged patientsto account for the variance in their physiologyand metabolism, and resulting differences indrug bioavailabilities and clearance.
Notwithstanding the capacity for readilyachievable improvements, significant gaps inour current knowledge of chronic pain mech-anisms and treatments in older adults suggestfuture directions for much-needed research.Clinical trials of analgesics need to be con-ducted in older adult populations, particularly

Vol. 38 No. 2S August 2009 S13Chronic Pain Management in Older Adults
for long-term use, to assess their overall effec-tiveness and risks. Research is needed to de-velop more effective strategies for assessingand managing pain among older adults withcognitive impairment. Lastly, an update ofthe Beers criteria or a similar analysis of phar-macotherapies for older patients is overdue.With these basic considerations in mind, wecan proceed now to a more detailed discussionof neuropathic pain in older individuals.
References1. Galluzzi KE. Managing neuropathic pain. J Am
Osteopath Assoc 2007;107(10 Suppl 6):ES39eES48.
2. Loeser JD, Treede RD. The Kyoto protocol ofIASP basic pain terminology. Pain 2008;137(3):473e477.
3. AGS Panel on Persistent Pain in Older Persons.The management of persistent pain in older per-sons. AGS panel on persistent pain in olderpersons. J Am Geriatr Soc 2002;50(6 Suppl):S205eS224.
4. Hall GC, Carroll D, McQuay HJ. Primary careincidence and treatment of four neuropathic painconditions: a descriptive study, 2002-2005 [abstract].BMC Fam Pract 2008;9:26e34.
5. Bennett GJ. Neuropathic pain: new insights,new interventions. Hosp Pract (Minneap) 1998;33(10):95e98. 101e104, 107e110.
6. Bennett MI, Bouhassira D. Epidemiology ofneuropathic pain: can we use the screening tools?Pain 2007;132(1e2):12e13.
7. Heath I. Multiple health problems in elderlypeople: never had it so good? BMJ 2008;336(7650):950e951.
8. Gustorff B, Dorner T, Likar R, et al. Prevalenceof self-reported neuropathic pain and impact onquality of life: a prospective representative survey.Acta Anaesthesiol Scand 2008;52(1):132e136.
9. Wiener K. Pain is an epidemic. Sonora, CA: Amer-ican Academy of Pain Management. Available at:http://www.aapainmanage.org/literature/Articles/PainAnEpidemic.pdf. Accessed July 16, 2009.
10. Maxwell CJ, Dalby DM, Slater M, et al. The prev-alence and management of current daily painamong older home care clients. Pain 2008;138(1):208e216.
11. American Pain Society. Chronic pain in America:roadblocks to relief. Glenview, IL: American Pain Soci-ety, 2005. Available from: http://painreliefnetwork.org/blog/the-magnitude-of-the-problem-roadblocks-to-relief-study. Accessed July 3, 2009.
12. Darer JD, Hwang W, Pham HH, et al. Moretraining needed in chronic care: a survey of US phy-sicians. Acad Med 2004;79(6):541e548.
13. Breuer B, Pappagallo M, Tai JY, et al. U.S.board-certified pain physician practices: uniformityand census data of their locations. J Pain 2007;8(3):244e250.
14. Besdine R, Boult C, Brangman S, et al. Caringfor older Americans: the future of geriatricmedicine. J Am Geriatr Soc 2005;53(6 Suppl):S245eS256.
15. Cole LJ, Farrell MJ, Gibson SJ, Egan GF.Age-related differences in pain sensitivity andregional brain activity evoked by noxious pressure.Neurobiol Aging 2008 May 28. [Epub ahead ofprint].
16. Perucca E. Clinical pharmacokinetics of new-generation antiepileptic drugs at the extremes ofage. Clin Pharmacokinet 2006;45(4):351e363.
17. Milton JC, Hill-Smith I, Jackson SH. Prescribingfor older people. BMJ 2008;336(7644):606e609.
18. Benoist M. Natural history of the aging spine.Eur Spine J 2003;12(Suppl 2):S86eS89.
19. Husebo BS, Strand LI, Moe-Nilssen R, et al.Who suffers most? Dementia and pain in nursinghome patients: a cross-sectional study. J Am MedDir Assoc 2008;9(6):427e433.
20. Proctor WR, Hirdes JP. Pain and cognitive statusamong nursing home residents in Canada. Pain ResManag 2001;6(3):119e125.
21. Kelley AS, Siegler EL, Reid MC. Pitfalls and rec-ommendations regarding the management of acutepain among hospitalized patients with dementia.Pain Med 2008;9(5):581e586.
22. Hadjistavropoulos T, Voyer P, Sharpe D, et al.Assessing pain in dementia patients with comorbiddelirium and/or depression. Pain Manag Nurs2008;9(2):48e54.
23. Hadjistavropoulos T, Herr K, Turk DC, et al. Aninterdisciplinary expert consensus statement onassessment of pain in older persons. Clin J Pain2007;23(1 Suppl):S1e43.
24. Finnerup NB, Otto M, McQuay HJ, et al. Algo-rithm for neuropathic pain treatment: an evidencebased proposal. Pain 2005;118(3):289e305.
25. Dworkin RH, O’Connor AB, Backonja M, et al.Pharmacologic management of neuropathic pain: evi-dence-based recommendations. Pain 2007;132(3):237e251.
26. Dworkin RH, Backonja M, Rowbotham MC,et al. Advances in neuropathic pain: diagnosis,mechanisms, and treatment recommendations.Arch Neurol 2003;60(11):1524e1534.
27. McQuay HJ, Tramer M, Nye BA, et al. A system-atic review of antidepressants in neuropathic pain.Pain 1996;68(2e3):217e227.
28. de Leon-Casasola OA. Multimodal approachesto the management of neuropathic pain: The roleof topical analgesia. J Pain Symptom Manage 2007;33(3):356e364.

S14 Vol. 38 No. 2S August 2009Fine
29. Gimbel J, Linn R, Hale M, et al. Lidocaine patchtreatment in patients with low back pain: results ofan open-label, nonrandomized pilot study. AmJ Ther 2005;12(4):311e319.
30. Gammaitoni AR, Alvarez NA, Galer BS. Safetyand tolerability of the lidocaine patch 5%, a targetedperipheral analgesic: a review of the literature.J Clin Pharmacol 2003;43(2):111e117.
31. Finnerup NB, Otto M, Jensen TS, et al. Anevidence-based algorithm for the treatment ofneuropathic pain. MedGenMed 2007;9:36.
32. Saarto T, Wiffen PJ. Antidepressants for neuro-pathic pain. Cochrane Database Syst Rev 2007;4:CD005454.
33. Eisenberg E, McNicol E, Carr DB. Opioids forneuropathic pain. Cochrane Database Syst Rev2006;3:CD006146.
34. Pergolizzi J, Boger RH, Budd K, et al. Opioidsand the management of chronic severe pain inthe elderly: consensus statement of an InternationalExpert Panel with focus on the six clinically mostoften used World Health Organization step IIIopioids (buprenorphine, fentanyl, hydromorphone,methadone, morphine, oxycodone). Pain Pract2008;8(4):287e313.
35. The Information Centre for Health and SocialCare (Health Care). Prescriptions dispensed in thecommunity. Statistics for 1996 to 2006. London:The NHS Information Centre, 2007. Available from:http://www.parliament.uk/deposits/depositedpapers/2008/DEP2008-0875.pdf. Accessed July 3, 2009.
36. Green JL, Hawley JN, Rask KJ. Is the number ofprescribing physicians an independent risk factorfor adverse drug events in an elderly outpatient pop-ulation? Am J Geriatr Pharmacother 2007;5(1):31e39.
37. Carnes D, Anwer Y, Underwood M, et al. Influ-ences on older people’s decision making regardingchoice of topical or oral NSAIDs for knee pain: qual-itative study. BMJ 2008;336(7636):142e145.
38. Soumerai SB, Pierre-Jacques M, Zhang F, et al.Cost-related medication nonadherence amongelderly and disabled medicare beneficiaries: anational survey 1 year before the medicare drugbenefit. Arch Intern Med 2006;166(17):1829e1835.
39. Fu AZ, Liu GG, Christensen DB. Inappropriatemedication use and health outcomes in the elderly.J Am Geriatr Soc 2004;52(11):1934e1939.
40. van der Hooft CS, Jong GW, Dieleman JP, et al.Inappropriate drug prescribing in older adults: the
updated 2002 Beers criteriada population-basedcohort study. Br J Clin Pharmacol 2005;60(2):137e144.
41. Beers MH, Ouslander JG, Rollingher I, et al.Explicit criteria for determining inappropriate med-ication use in nursing home residents. UCLA Divi-sion of Geriatric Medicine. Arch Intern Med 1991;151(9):1825e1832.
42. Fick DM, Cooper JW, Wade WE, et al. Updatingthe Beers criteria for potentially inappropriate med-ication use in older adults: results of a US consensuspanel of experts. Arch Intern Med 2003;163(22):2716e2724.
43. Beers MH. Explicit criteria for determiningpotentially inappropriate medication use by theelderly. An update. Arch Intern Med 1997;157(14):1531e1536.
44. Gallagher PF, Barry PJ, Ryan C, et al. Inappro-priate prescribing in an acutely ill population ofelderly patients as determined by Beers’ Criteria.Age Ageing 2008;37(1):96e101.
45. O’Mahony D, Gallagher PF. Inappropriateprescribing in the older population: need for newcriteria. Age Ageing 2008;37(2):138e141.
46. van der Hooft CS, Schoofs MW, Ziere G, et al.Inappropriate benzodiazepine use in older adultsand the risk of fracture. Br J Clin Pharmacol 2008;66(2):276e282.
47. Brekke M, Rognstad S, Straand J, et al. Pharma-cologically inappropriate prescriptions for elderlypatients in general practice: how common? Baselinedata from The Prescription Peer Academic Detail-ing (Rx-PAD) study. Scand J Prim Health Care2008;26(2):80e85.
48. O’Brien MA, Rogers S, Jamtvedt G, et al. Educa-tional outreach visits: effects on professional prac-tice and health care outcomes. Cochrane DatabaseSyst Rev 2007;4:CD000409.
49. Zillich AJ, Shay K, Hyduke B, et al. Qualityimprovement toward decreasing high-risk medica-tions for older veteran outpatients. J Am GeriatrSoc 2008;56(7):1299e1305.
50. Wessell AM, Nietert PJ, Jenkins RG, et al. Inap-propriate medication use in the elderly: resultsfrom a quality improvement project in 99 primarycare practices. Am J Geriatr Pharmacother 2008;6(1):21e27.
51. Spinewine A. Adverse drug reactions in elderlypeople: the challenge of safer prescribing. BMJ2008;336(7650):956e957.