Embed Size (px)
Citation preview
Chronic Suppurative Otitis Media
Dr. Gangaprasad Waghmare
MS
Chronic Suppurative Otitis Media
• Chronic inflamation of middle ear causing
irreversible changes like perforation
• Can cause deafness
• Seen mostly in low socio-economic people
Causes • Attack of ME infection
• Measels, diptheria, inflenza infection
• Disorders of ventilation
• Retraction pocket formation
• Long standing SOM
• Bacteriological
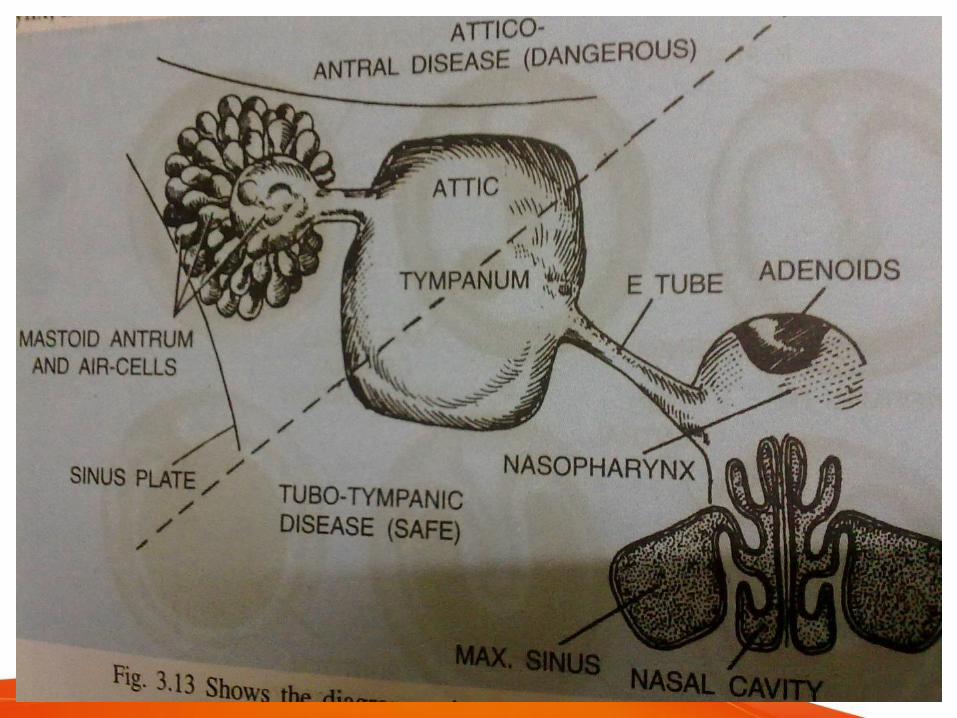
Types
• Tubo tympanic
• Attico antral
Tubo Tympanic
• Involves antero inferior part of me
• Sread of infection from septic focci near
naso pharynx like
Rhinitis
Tonsilitis
Sinusitis
Adenoids
From external ear through perforated ear
drum
Malnutrition & hypogamaglobulinaemia
Clinical featurs
• Recurrent otorrhea: watery & mucoid
• Deafness: conductive type
• Pain: absent
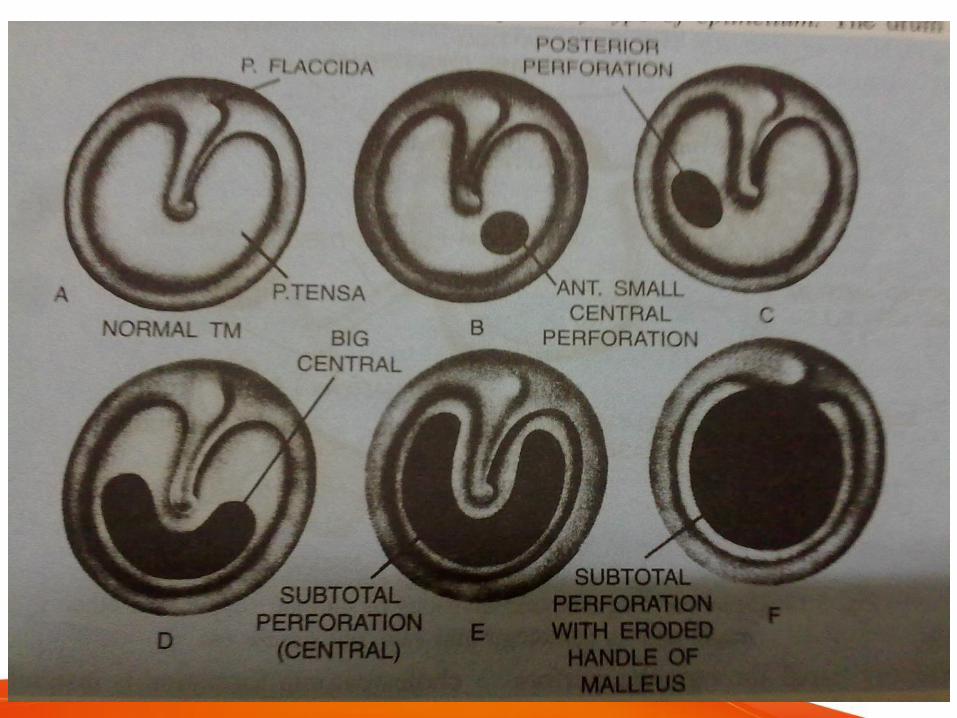
• Otoscopy : perforation of tympanic
membrane
• Infection like :rhinitis, sinusitis,adenoids
Pathological changes
• Perforation : central perforation due to
necrosis of part having less blood supply
• Ossicles : discontinuity of chain due to
necrosis
• Tympano sclerosis : white chalky deposit
on ossicular joint due to hyline
degenaration
• Polyp : from perforated ear drum
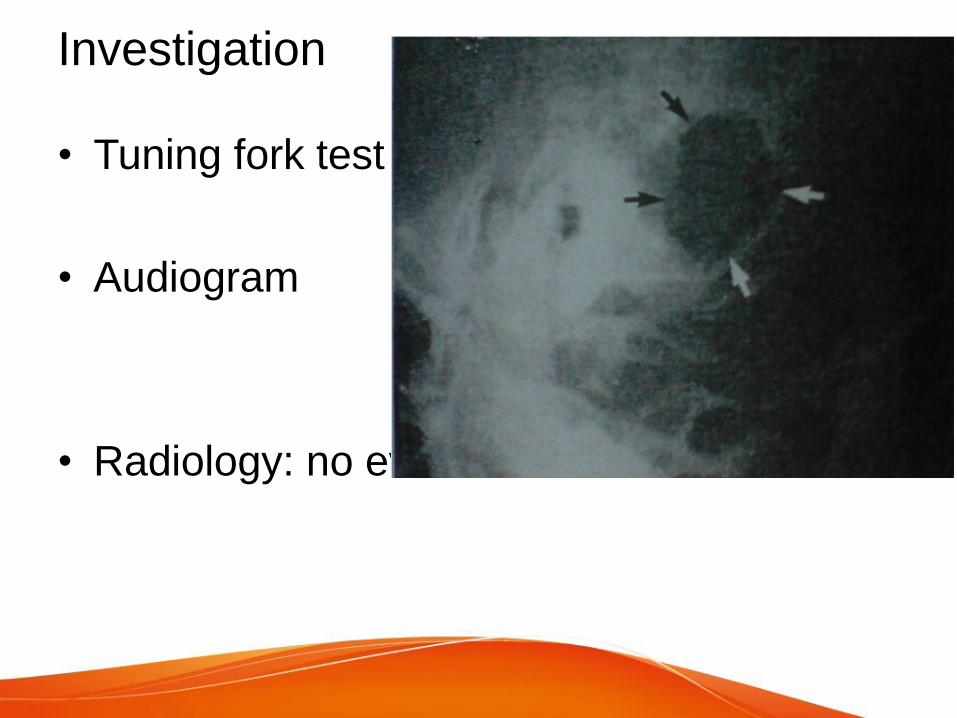
Investigation
• Tuning fork test
• Audiogram
• Radiology: no evidence of erosion
treatment
• Septic focci
• Aural toilet
• Antibiotic ear drops
• Systemic antibiotics
• Surgical: polyp should surgically removed
tympanoplasty
Attico antral or Tympano Mastoid
• Postero superior part of ME
• Pathalogical changes : formation of
cholesteotoma
• polyps
• granuation
• partial or total necrosis
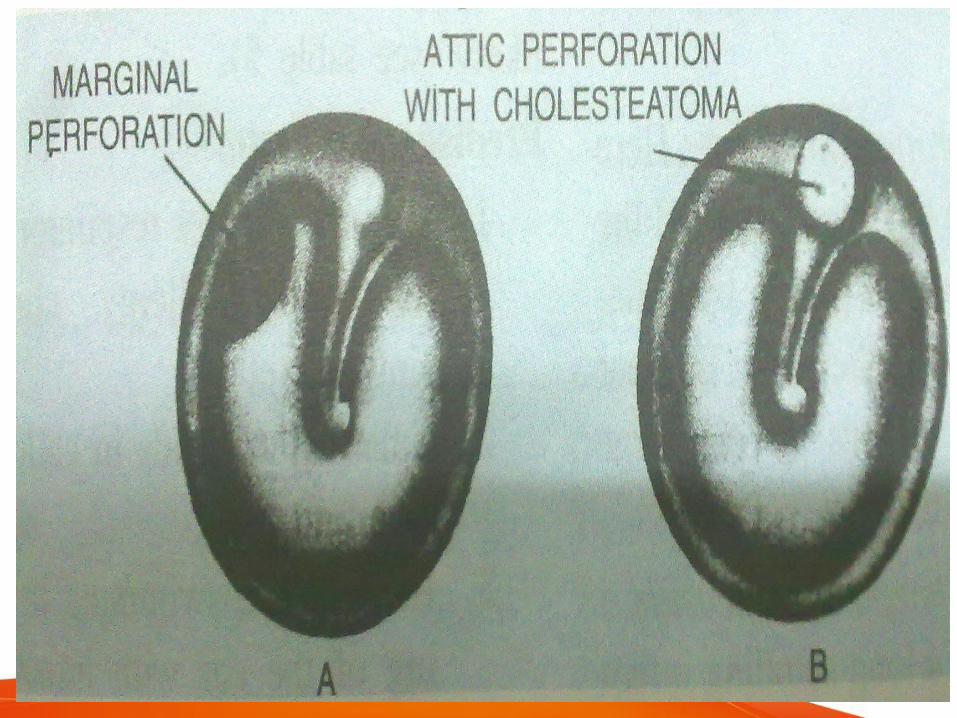
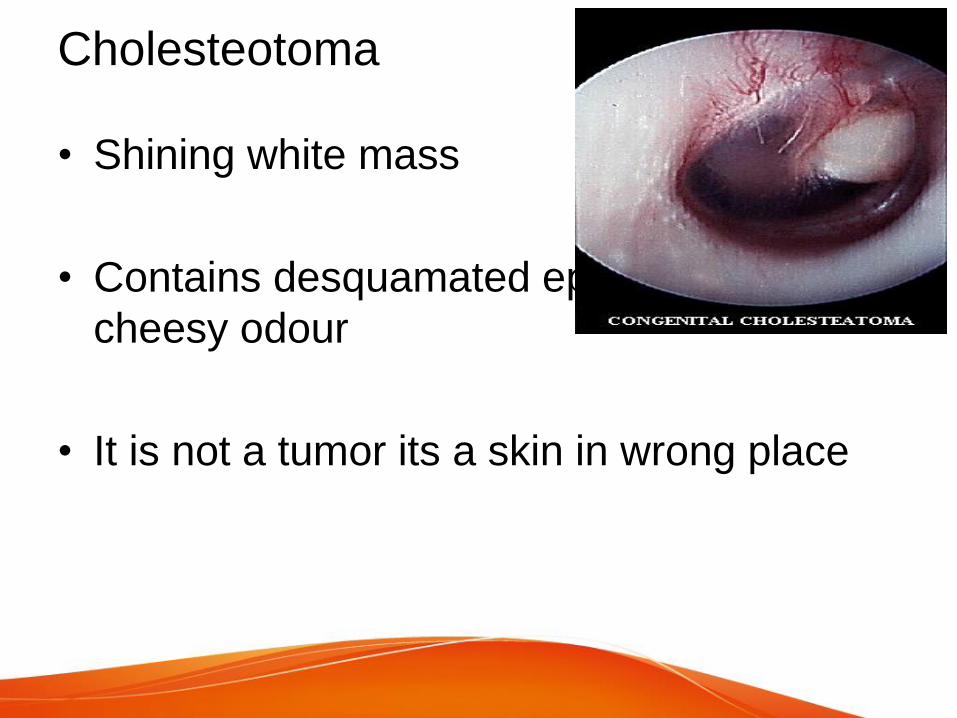
Cholesteotoma
• Shining white mass
• Contains desquamated epithelium with
cheesy odour
• It is not a tumor its a skin in wrong place
Formation
• Acquired :
Increase ME pressure with OM
Increase Negative pressure
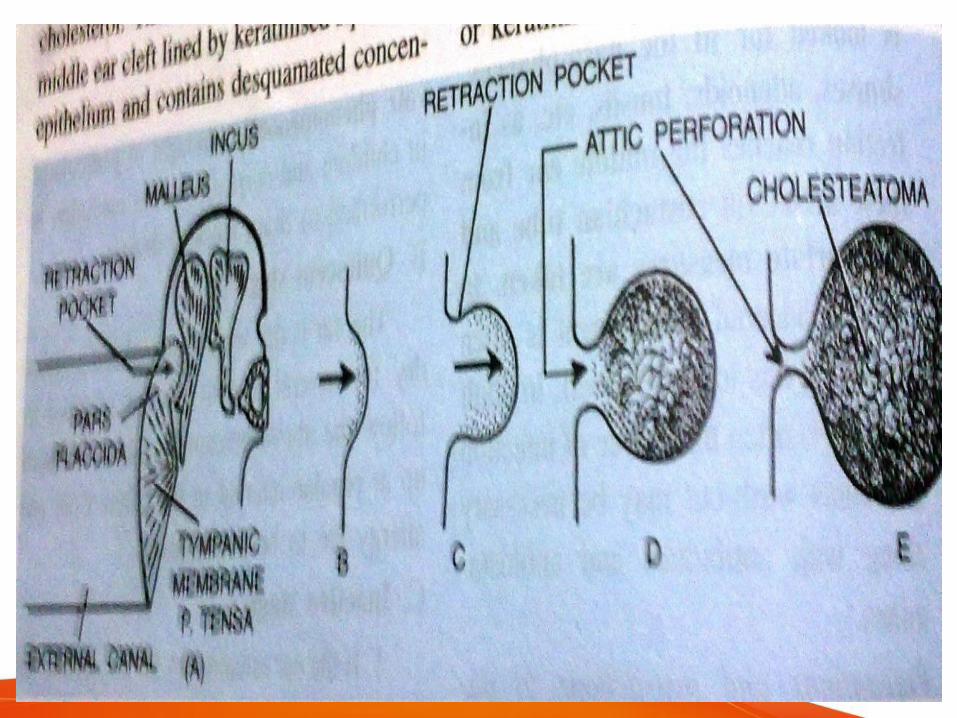
Retraction of pars flacida
Pouch neck get closed
Sac and skin get localised
• Invasion : growth of epithelium from
external auditory canal
• Metaplasia: metaplasia of epithelium of
middle ear cleft due to suppuration
Bone erodation
• By liberation of chemical
• Ischaemic necrosis theory
• Enzymatic theory: collagenase, acid
phoaphate and proteolytic enzyme
• Passes from aditus to antrum of mastoid
further spread causing many complication
• Hence called as dangerous om
Clinical Features
• Otorrhoea: scanty & foetid
• Deafness: conductive & mild initially
• Bleeding : from granulation or polyp
Otoscopic examination
• Perforation in pars flacida
• Granulation
• Cholesteatoma
• Cholesterol granuloma [black drum]
• Retraction pocket
• Symptoms of complication- earache,
vertigo, temporal headache, tinnitus, facial
palsy, abscess around ear.
Investigation
• Audiometry : Moderate to severe
conductive deafness
• Radiology: mastoid bone sclerosis with
bone erosion
• Culture & sensitivity of discharge
Treatment
• Ostruction of eustachian tube
• Aural toilet: a small cholesteoma can be
removed by suction
• Surgery : granulation polyp should be
surgically removed
mastoidectomy
Tympanoplasty