Embed Size (px)
Citation preview
The linked image cannot be displayed. The file may have been moved, renamed, or deleted. Verify that the link points to the correct file and location.
Chronische lymphatische Leukämie
Prof. Claudia Lengerke Abteilung für Hämatologie
Universitätsspital Basel

medArt basel ̀ 15
CLL ist eine Neoplasie der differenzierten B-Zellen
T h e
T h e
T h e
ERYTHROZYTEN)))THROMBOZYTEN)
GRANULOZYTEN)
MONOZYTEN)))STAMMZELLE)
T000LYMPHOZYTEN)
B)))LYMPHOZYTEN)
SELBST)))/ERNEUERUNG)
DIFFERENZIERUNG/UND/PROLIFERATION/(EXPANSION))
CLL: unkontrollierte A
kkumulation von
malignen B
-Lymphozyten in B
lut und Organen
(v. a. Knochenm
ark, Lymphknoten, M
ilz)
medArt basel ̀ 15C
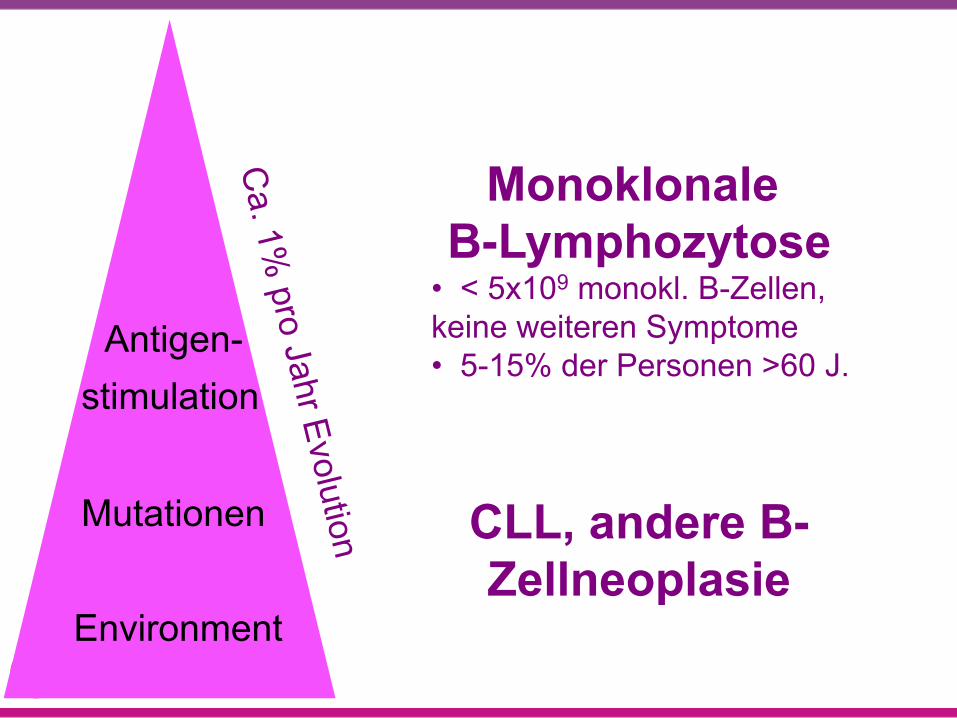
a. 1% pro Jahr Evolution
Monoklonale B-Lymphozytose
• < 5x109 monokl. B-Zellen, keine weiteren Symptome • 5-15% der Personen >60 J.
CLL, andere B-Zellneoplasie
Antigen- stimulation Mutationen
Environment
medArt basel ̀ 15
Fallvignette 43 jähriger Patient, ansonsten gesund, stellt sich mit Halsschmerzen und trockenem Husten beim Hausarzt vor. Fieber wird verneint. Geröteter Rachenraum ohne Beläge, zervikale Lymphadenopathie (bis 2 cm, indolent, anamnestisch seit mehreren Wochen bestehend). Blutbild: Hb 145 g/dl, Tc 360 x109/l G/l, Leukozyten 35 x109/l (v. a. Lymphozyten) Was unternehmen Sie? (A) Es liegt am ehesten ein viraler Infekt der oberen Atemwege mit Begleitleukozytose vor. Klinische Kontrolle nach einer Woche. (B) Sofortige stationäre Einweisung mit Verdacht auf Leukämie (C) Körperliche Untersuchung, Hand-Differentialblutbild (E) Einweisung zum HNO-Spezialisten zur Abklärung der zervikalen LK
medArt basel ̀ 15
Lymphozytose Definition: Absolutzahl Lymphozyten >4.0x109/l
„Reaktiv“ ² Virale Infekte
– Mononukleose – Andere virale Erkrankungen
² Bakterielle Infekte – Bordetella pertussi/parapertussi – Bartonella henselae
² Parasiteninfekte (Protozoen) – Toxoplasmose – Babesiosis
² Nicht infektiöse Ursachen – Kollagenosen – Serum-Krankheit – Medikamentenallergie – Postsplenektomie
u Reifzellige B-Lymphozyten Neoplasien
– CLL – Prolymphozytenleukämie – Haarzellenleukämie – Plasmazellmyelom/-leukämie – Follikuläres Lymphom – Mantelzell-Lymphom – Marginalzonen-Lymphom – Morbus Waldenström
u Reifzellige T-Lymphozyten Neoplasien
– LGL (large granular lymphocyte) Leukämie – Adulte T-NHL – Prolymphozytenleukämie – Mycosis fungoides (Sézary) – Angioimmunoblastische T-NHL – Hepatosplenische T-NHL
NHL = Non-Hodgkin Lymphom
medArt basel ̀ 15
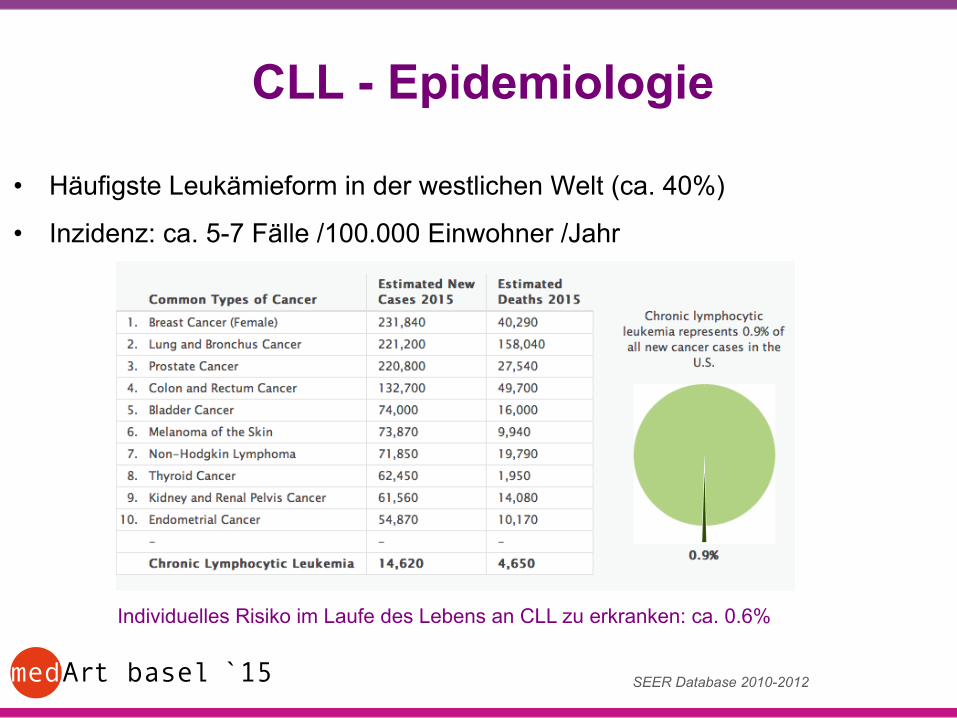
• Häufigste Leukämieform in der westlichen Welt (ca. 40%)
• Inzidenz: ca. 5-7 Fälle /100.000 Einwohner /Jahr
CLL - Epidemiologie
SEER Database 2010-2012
Individuelles Risiko im Laufe des Lebens an CLL zu erkranken: ca. 0.6%
medArt basel ̀ 15
• Häufigste Leukämieform in der westlichen Welt (ca. 40%)
• Inzidenz: ca. 5-7 Fälle /100.000 Einwohner /Jahr
• Mehr Männer betroffen (m:w = 1,7:1)
• Medianes Alter bei Diagnosestellung: 70 Jahre
• Risiko bei Exposition zu Benzol u.ä., sonst keine klare Assoziation mit Umweltfaktoren
• Abhängig von genetischen Faktoren (häufiger in USA/Europa, weniger in Afrika, kaum in Asien), Vererbbarkeit?
- familiäre Häufung beobachtet - Personen mit Verwandten 1. Grades mit CLL: 8.5fach erhöhtes Erkrankungsrisiko
CLL - Epidemiologie
Goldin LR et al, Br J Haematol, 2010
medArt basel ̀ 15
Fallvignette 43 jähriger Patient, ansonsten gesund, stellt sich mit Halsschmerzen und trockenem Husten beim Hausarzt vor. Fieber wird verneint. Geröteter Rachenraum ohne Beläge, zervikale Lymphadenopathie (bis 2 cm, indolent, anamnestisch seit mehreren Wochen bestehend). Blutbild: Hb 145 g/dl, Tc 360 x109/l G/l, Leukozyten 35 x109/l (v.a. Lymphozyten) Was unternehmen Sie? (A) Es liegt am ehesten ein viraler Infekt der oberen Atemwege mit
Begleitleukozytose vor. Klinische Kontrolle in einer Woche. (B) Sofortige stationäre Einweisung mit Verdacht auf Leukämie (D) Körperliche Untersuchung, Hand-Differentialblutbild (F) Einweisung zum HNO-Spezialisten zur Abklärung der zervikalen LK

medArt basel ̀ 15
Morphologie der Lymphozyten
Normaler Lymphozyt
Neoplastischer Lymphozyt
Atypischer Lymphozyt
Verdacht auf CLL (Typisch: Gumprecht Schollen)
Morphologie der Lymphozyten
Gumprecht Schollen
medArt basel ̀ 15
Fallvignette Körperliche Untersuchung: Lymphknoten bis 2 cm inguinal und axillär, ansonsten keine Auffälligkeiten. Differentialblutbild: absolute Lymphozytose (32x109/l), die Verteilung der sonstigen Leukozyten-Subgruppen ist normal. Hand-Differentialblutbild: Vermehrung kleiner differenzierter Lymphozyten und einzelne Kernschatten. Was ist der nächste diagnostische Schritt? (A) Immunphänotypisierung im peripheren Blut (B) Knochenmarkpunktion (C) Ganzkörper-PET/CT bei Verdacht auf Lymphom (D) Biopsie der vergrösserten zervikalen Lymphknoten
medArt basel ̀ 15
Bestätigung der Diagnose CLL
• Blutbild: ≥ 5 x 109/l B-Lymphozyten im peripheren Blut ≥ 3 Monate
• Differentialblutbild
• Immunphänotypisierung
Hallek M, et al. Blood 2008; 111:5446-5456.

medArt basel ̀ 15
Fallvignette Körperliche Untersuchung: Lymphknoten bis 2 cm inguinal und axillär, ansonsten keine Auffälligkeiten. Differentialblutbild: absolute Lymphozytose (32x109/l), die Verteilung der sonstigen Leukozyten-Subgruppen ist normal. Hand-Differentialblutbild: Vermehrung kleiner differenzierter Lymphozyten und einzelne Kernschatten. Was ist der nächste diagnostische Schritt? (A) Immunphänotypisierung im peripheren Blut (B) Knochenmarkpunktion (C) Ganzkörper-PET/CT bei Verdacht auf Lymphom (D) Biopsie der vergrösserten zervikalen Lymphknoten
medArt basel ̀ 15
Imm
unph
änot
pysi
erun
g: E
rken
nung
von
Pro
tein
en a
uf d
er Z
ello
berfl
äche
dur
ch
Kop
plun
g m
it Fl
uore
szen
z-tra
gend
en A
ntik
örpe
rn
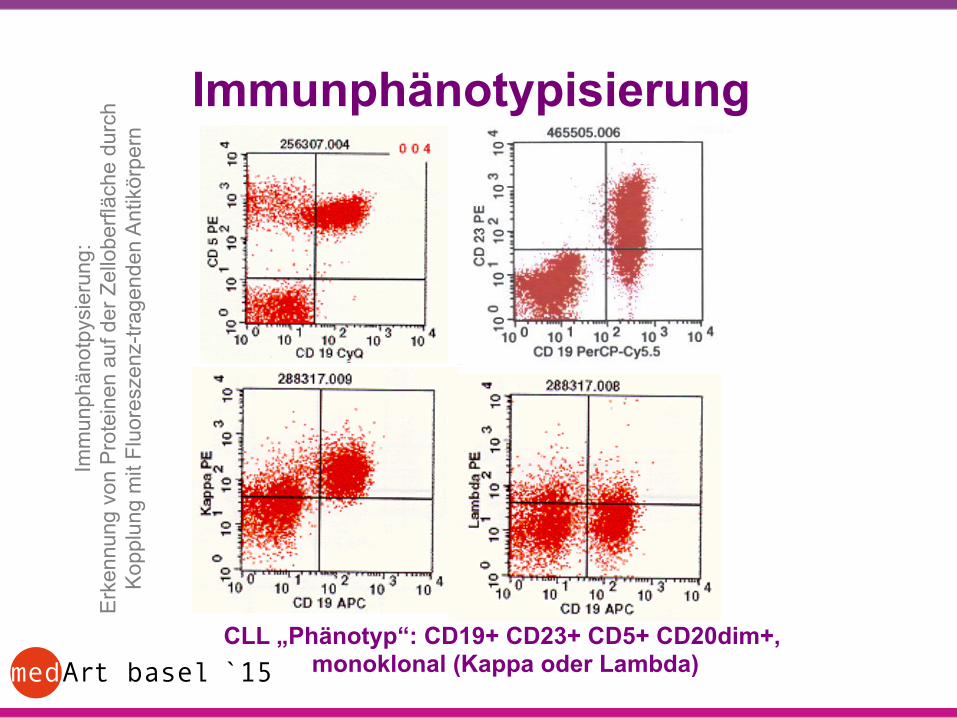
CLL „Phänotyp“: CD19+ CD23+ CD5+ CD20dim+, monoklonal (Kappa oder Lambda)
Immunphänotypisierung
medArt basel ̀ 15
Weitere Diagnostik • Anamnese, körperliche Untersuchung
medArt basel ̀ 15
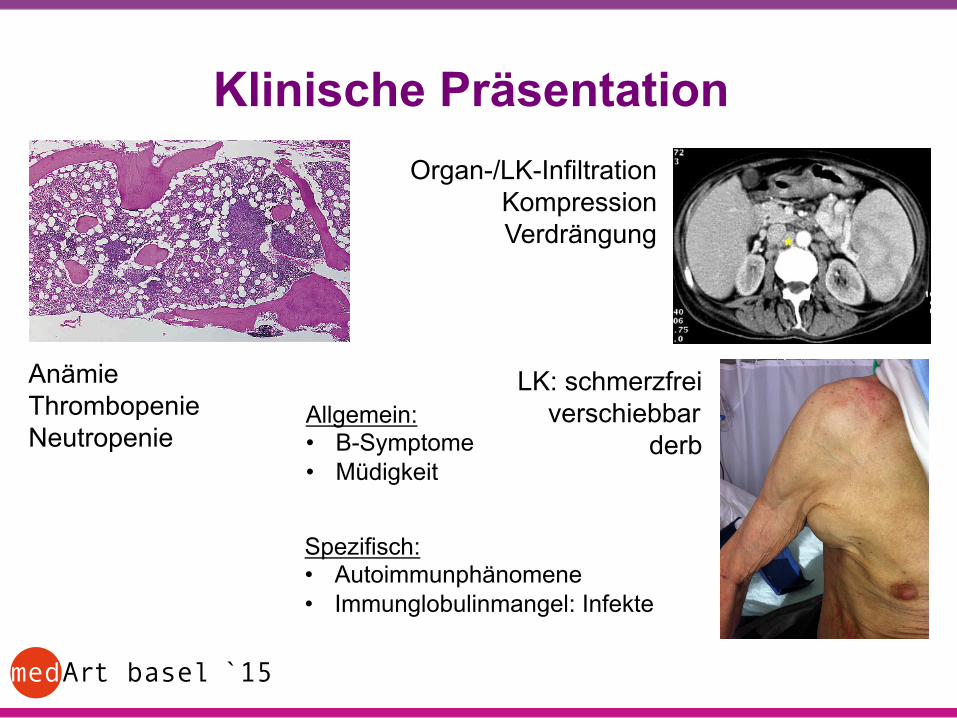
Klinische Präsentation
Anämie Thrombopenie Neutropenie
Organ-/LK-Infiltration Kompression Verdrängung
LK: schmerzfrei verschiebbar
derb Allgemein: • B-Symptome • Müdigkeit
Spezifisch: • Autoimmunphänomene • Immunglobulinmangel: Infekte
medArt basel ̀ 15
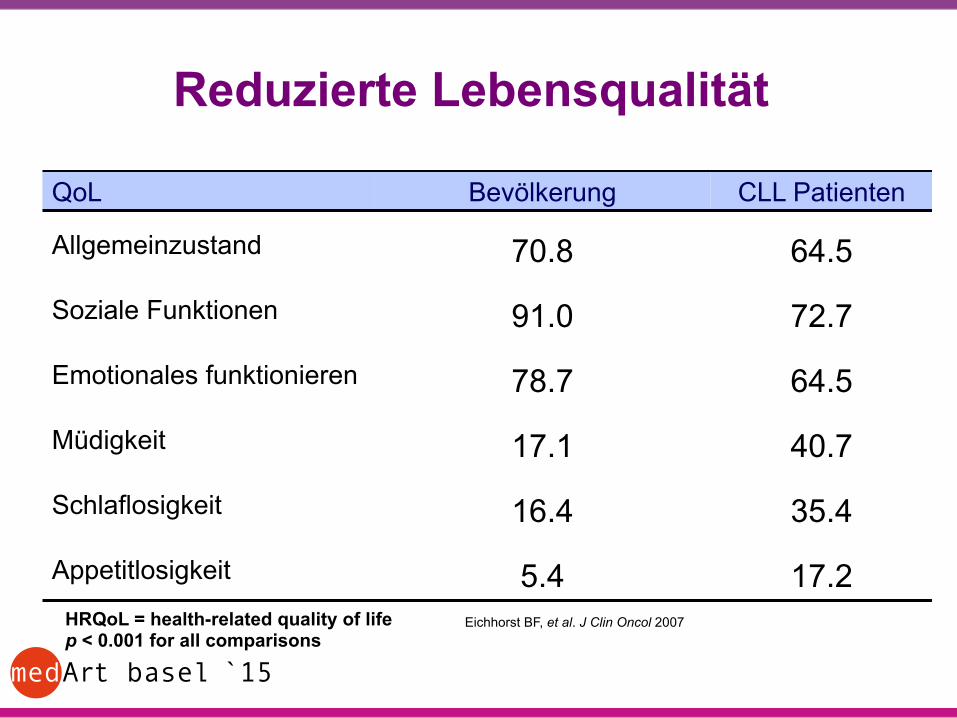
Reduzierte Lebensqualität
Eichhorst BF, et al. J Clin Oncol 2007
QoL Bevölkerung CLL Patienten
Allgemeinzustand 70.8 64.5
Soziale Funktionen 91.0 72.7
Emotionales funktionieren 78.7 64.5
Müdigkeit 17.1 40.7
Schlaflosigkeit 16.4 35.4
Appetitlosigkeit 5.4 17.2 HRQoL = health-related quality of life p < 0.001 for all comparisons
medArt basel ̀ 15
Infekte, Autoimmunphänomene • Infekte - durch Immunglobulin-Mangel, Neutropenie, T-/NK-Zelldysregulation - Massnahmen: Impfungen (Influenza, Pneumokokken) Immunglobuline bei Infektneigung (>2 bakt. Infekte/Jahr) u. IgG<4g/l • Autoimmunphänomene - durch Dysregulation des Immunsystems, Auto-Ak werden
wahrscheinlich vom leukämischen Klon produziert - bis zu 10-25% der Patienten - vor allem gegen Blutzellen: 5-10% AIHA, 2-3% ITP, PRCA, selten
Autoimmunneutropenie

medArt basel ̀ 15
Weitere Diagnostik • Anamnese, körperliche Untersuchung • Retikulozytenzahl, Chemogramm (Nierenfunktion?, LDH, ..) • Immunglobuline quantitativ im Serum • Elektrophorese, Immunfixation im Serum und Urin • Coombs-Test, Haptoglobin • Abdomensonographie Vor Therapiebeginn empfohlen: • Knochenmarkuntersuchung: Evaluation von Zytopenien • Genetik: Zytogenetik, FISH (del17p13), TP53 Mutationsanalyse • Lymphknoten-Biopsie: falls Diagnose nicht gesichert Bei spezifischer Fragestellung, in klinischen Studien: • CT-Untersuchung: Lymphome, Organbefall, Infektherde? • „Investigational“: Thymidinkinase, Beta2 Mikroglobulin, IgHV Mutationsstatus,
CD38, ZAP70, u.a.
medArt basel ̀ 15
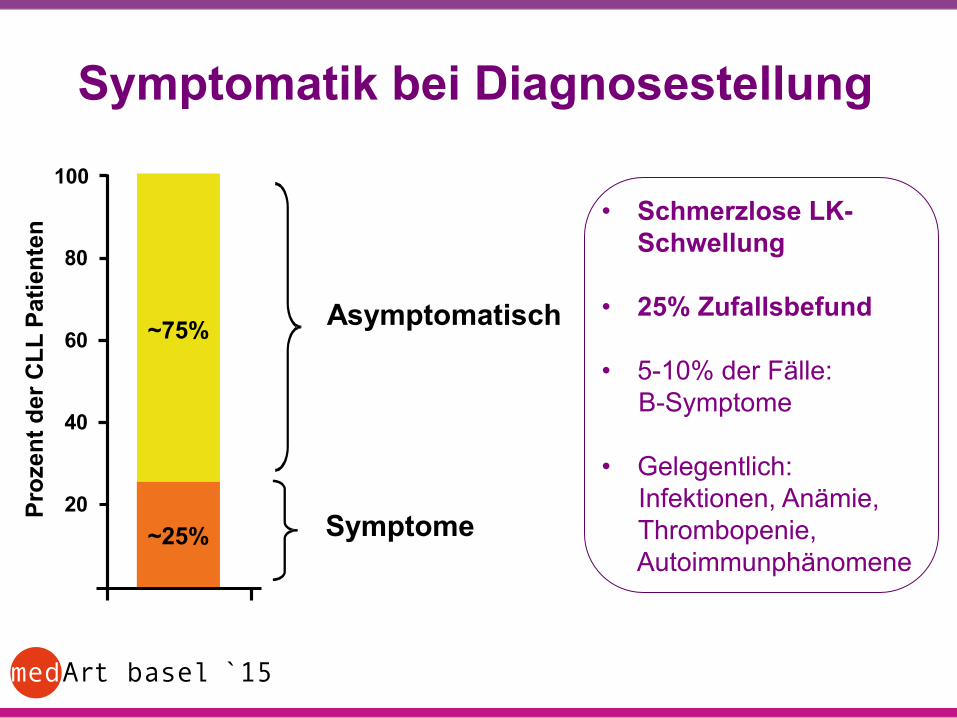
Symptomatik bei Diagnosestellung Pr
ozen
t der
CLL
Pat
ient
en
80
60
40
20
100
~75%
~25%
Asymptomatisch
Symptome
• Schmerzlose LK-
Schwellung • 25% Zufallsbefund • 5-10% der Fälle: B-Symptome • Gelegentlich: Infektionen, Anämie, Thrombopenie, Autoimmunphänomene

medArt basel ̀ 15
Klinische Stadien
Stadium Organvergrösserung * Hämoglobin g/l Thrombozyten G/l
A (50-60%) <3 Regionen befallen >100 >100
B (30%) >3 Regionen befallen >100 >100
C (<20%) irrelevant <100 oder <100
Nach Binet:
*Lymphknoten >1.5 cm Hals, Axilla, inguinal oder Milz/Lebervergrösserung
Stadium A meist nicht behandlungsbedürftig Stadium B und C meist behandlungsbedürftig A 14-17
B 5-7 C 3
Überlebens- wahrscheinlichkeit
in Jahren
Stadieneinteilung nach Rai Stadien 0 – IV (low risk 0, interm. I-II, high III-IV)

medArt basel ̀ 15
Indikation zur Behandlung der CLL
- Zytopenien (neu aufgetreten oder progredient) - B-Symptome - Massive und progr./symptomatische Organomegalie - Massive und progr./symptomatische Adenopathie - Lymphozytenverdopplungszeit < 6 Monate* - Autoimmunphänomene - Rezidivierende Infekte
* cave: nicht alleine gültig bei initialen Lymphozyten < 30 x 109/l
Herausforderung: sehr heterogene klinische Verläufe - indolent über viele Jahre versus rasch progressiv -
medArt basel ̀ 15
Progression durch Transformation • ca. 5% der CLL Patienten • Klinische „Alarmzeichen“:
- rasch progrediente LK / Zytopenien - B-Symptome, neue Beschwerden (Kompression?)
- LDH-Anstieg • „Richter-Transformation“ in ein aggressives Lymphom, meist
ein diffus grosszelliges B-NHL • Assoziation mit anderen Lymphomen möglich: - M. Hodgkin, T-PLL • Vorgehen:
- Diagnostische Sicherung (Biopsie!) - rasche Einleitung einer Entität-spezifischen Therapie

medArt basel ̀ 15
Pathogenese der CLL
T-Zell unabhängige Immunanwort
IgHV%
%Nicht mutierte CLL
T-Zell-abhängige Immunanwort (GC)
IgHV%Mutierte CLL
HSC Pro-B Naive-B
VDH'''!Rekombina1on!
Selek1on!(Muta'onen,!Interak'on!mit!Umgebung!etc.)!
Initiale Genmutationen? Ursprungszelle der CLL?
nach Stefford JC, Brit J Haematol, 2015 (Adaptation: J. Schwaller)
T-Zell unabhängige Immunanwort
IgHV%
%Nicht mutierte CLL
T-Zell-abhängige Immunanwort (GC)
IgHV%Mutierte CLL
HSC Pro-B Naive-B
VDH'''!Rekombina1on!
Selek1on!(Muta'onen,!Interak'on!mit!Umgebung!etc.)!
Initiale Genmutationen? Ursprungszelle der CLL?
HSC = hematopoietic stem cell SHM = somatic hypermutation CSR = Class-switch recombination
VDJ recombination
medArt basel ̀ 15
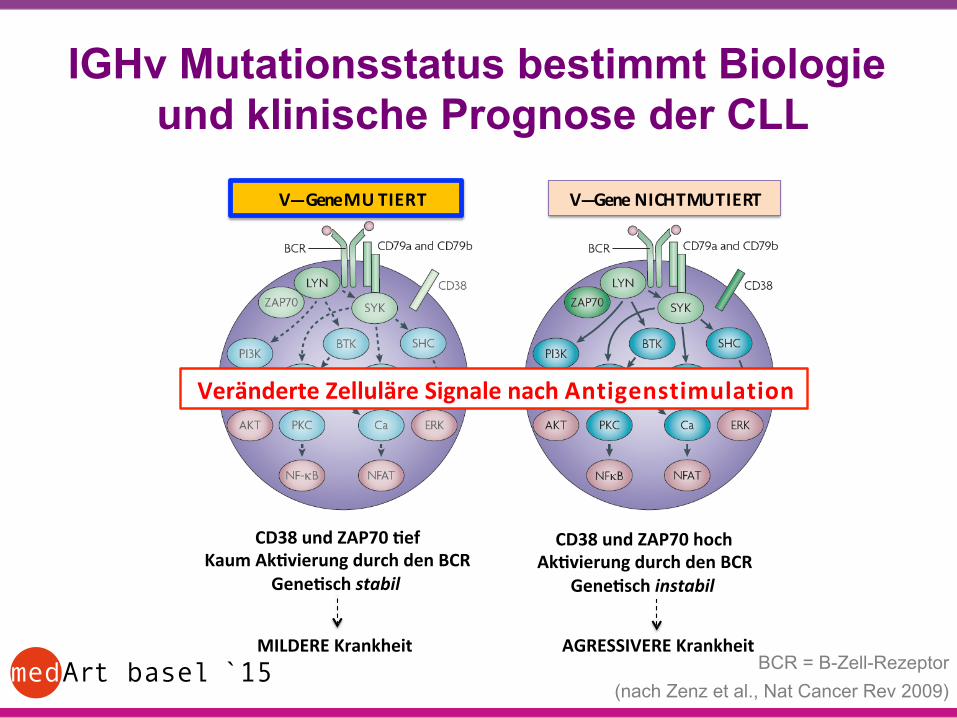
IGHv Mutationsstatus bestimmt Biologie und klinische Prognose der CLL DER$IGHV%%MUTATIONSSTATUS$BESTIMMT$DIE$BIOLOGIE$DER$CLL$
MILDERE$Krankheit! AGRESSIVERE$Krankheit!
Veränderte$Zelluläre$Signale$nach$A$n$t$i$g$e$n$s$t$i$m$u$l$a$t$i$o$n!
VEEE$Gene$M$U$$T$I$E$R$T! VEEEGene$$N$I$CH$T$MU$T$I$E$RT!
CD38$und$ZAP70$Lef$Kaum$AkLvierung$durch$den$BCR$
GeneLsch$stabil%
CD38$und$ZAP70$hoch$AkLvierung$durch$den$BCR$
GeneLsch$instabil%
BCR!=!B&Zell&Rezeptor! Nach$Zenz$et$al.,$Nat$Cancer$Rev$2009!
BCR = B-Zell-Rezeptor (nach Zenz et al., Nat Cancer Rev 2009)
medArt basel ̀ 15
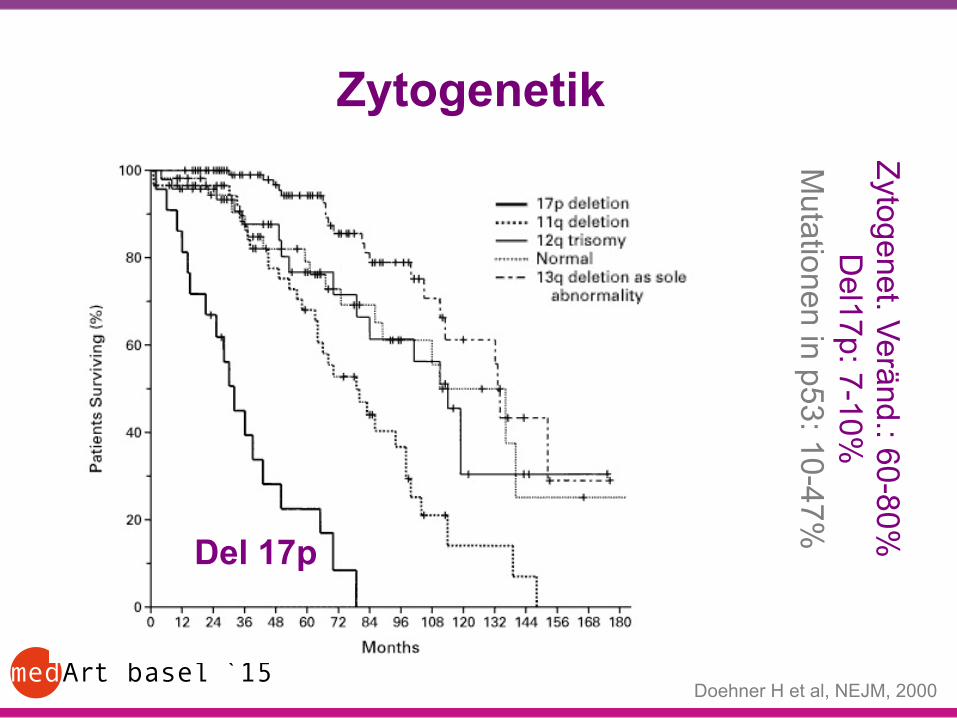
Zytogenetik
Doehner H et al, NEJM, 2000
Del 17p
Zytogenet. Veränd.: 60-80% D
el17p: 7-10% M
utationen in p53: 10-47%

medArt basel ̀ 15
Therapie der CLL • Richtet sich nach der „Fitness“ des Patienten (Comorbiditäten, Alter) • Und nach del17p oder p53 Mutation JA/NEIN
Group A • Functionally independent • No comorbidity • Normal life expectancy
Group C • Severely handicapped • High comorbidity • Reduced life expectancy
Group B • Intermediate • Moderate comorbidity • Reduced quality of life
Hämatologie
‘physically fit” Intensive therapy
Go-Go
u Long-lasting remissions!
u Cure?
‘impaired’ Moderate to Mild therapy:
Slow Go
u Long lasting remissions
u Control of symptoms
‘frail’ Supportive care
No Go
medArt basel ̀ 15
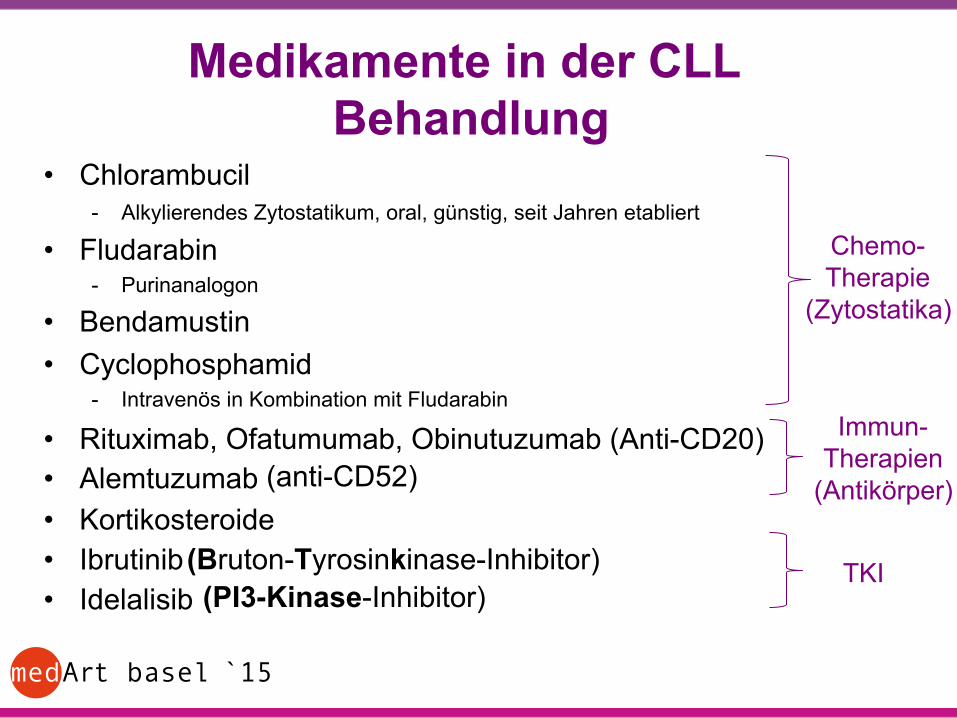
Medikamente in der CLL Behandlung
• Chlorambucil - Alkylierendes Zytostatikum, oral, günstig, seit Jahren etabliert
• Fludarabin - Purinanalogon
• Bendamustin • Cyclophosphamid
- Intravenös in Kombination mit Fludarabin
• Rituximab, Ofatumumab, Obinutuzumab (Anti-CD20) • Alemtuzumab • Kortikosteroide • Ibrutinib • Idelalisib
Chemo- Therapie
(Zytostatika)
Immun- Therapien
(Antikörper)
TKI (Bruton-Tyrosinkinase-Inhibitor)
(anti-CD52)
(PI3-Kinase-Inhibitor)
medArt basel ̀ 15
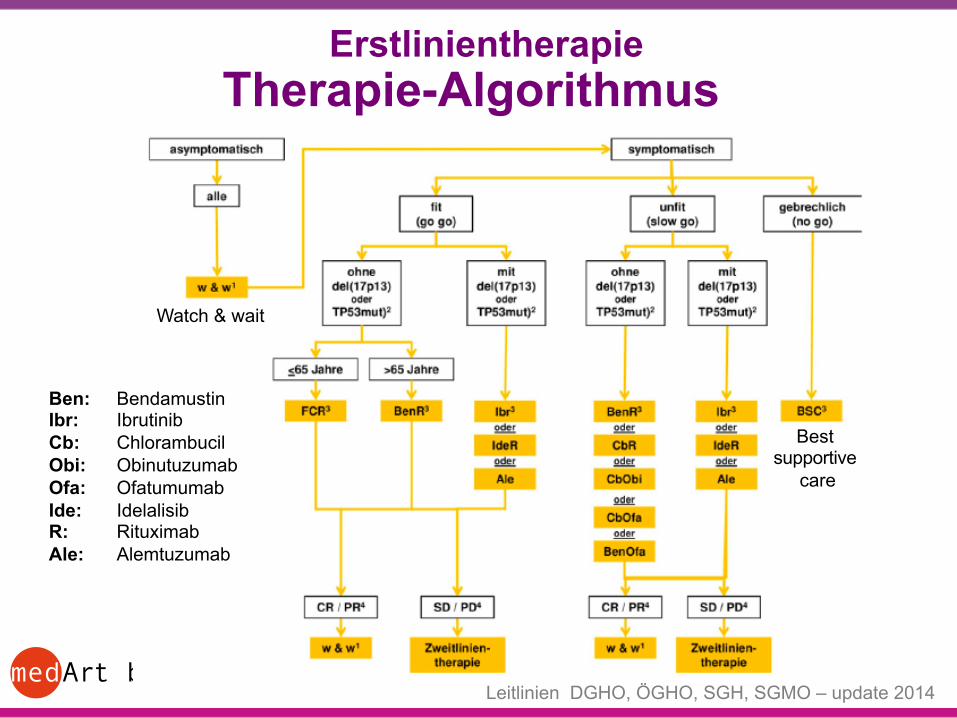
Therapie-Algorithmus
Watch & wait
Best supportive
care
Ben: Bendamustin Ibr: Ibrutinib Cb: Chlorambucil Obi: Obinutuzumab Ofa: Ofatumumab Ide: Idelalisib R: Rituximab Ale: Alemtuzumab
Erstlinientherapie
Leitlinien DGHO, ÖGHO, SGH, SGMO – update 2014
medArt basel ̀ 15
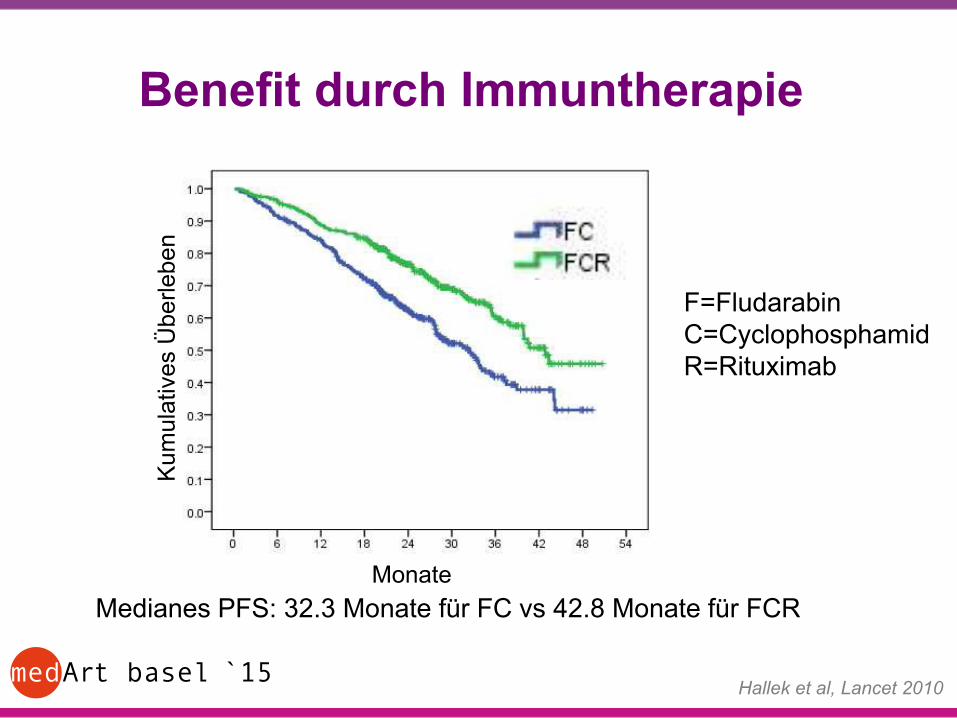
Benefit durch Immuntherapie
Medianes PFS: 32.3 Monate für FC vs 42.8 Monate für FCR
Hallek et al, Lancet 2010
F=Fludarabin C=Cyclophosphamid R=Rituximab
Kum
ulat
ives
Übe
rlebe
n
Monate
medArt basel ̀ 15
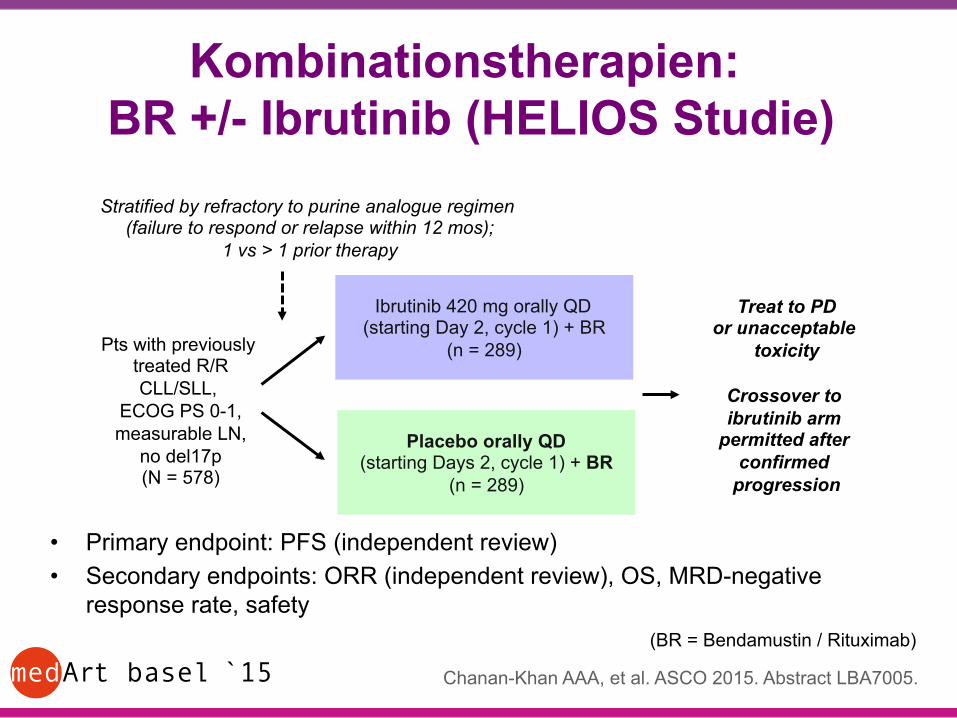
Kombinationstherapien: BR +/- Ibrutinib (HELIOS Studie)
• Primary endpoint: PFS (independent review) • Secondary endpoints: ORR (independent review), OS, MRD-negative
response rate, safety
Ibrutinib 420 mg orally QD (starting Day 2, cycle 1) + BR
(n = 289) Pts with previously treated R/R CLL/SLL,
ECOG PS 0-1, measurable LN,
no del17p (N = 578)
Stratified by refractory to purine analogue regimen (failure to respond or relapse within 12 mos);
1 vs > 1 prior therapy
Chanan-Khan AAA, et al. ASCO 2015. Abstract LBA7005.
Placebo orally QD (starting Days 2, cycle 1) + BR
(n = 289)
Treat to PD or unacceptable
toxicity
Crossover to ibrutinib arm
permitted after confirmed
progression
(BR = Bendamustin / Rituximab)
medArt basel ̀ 15
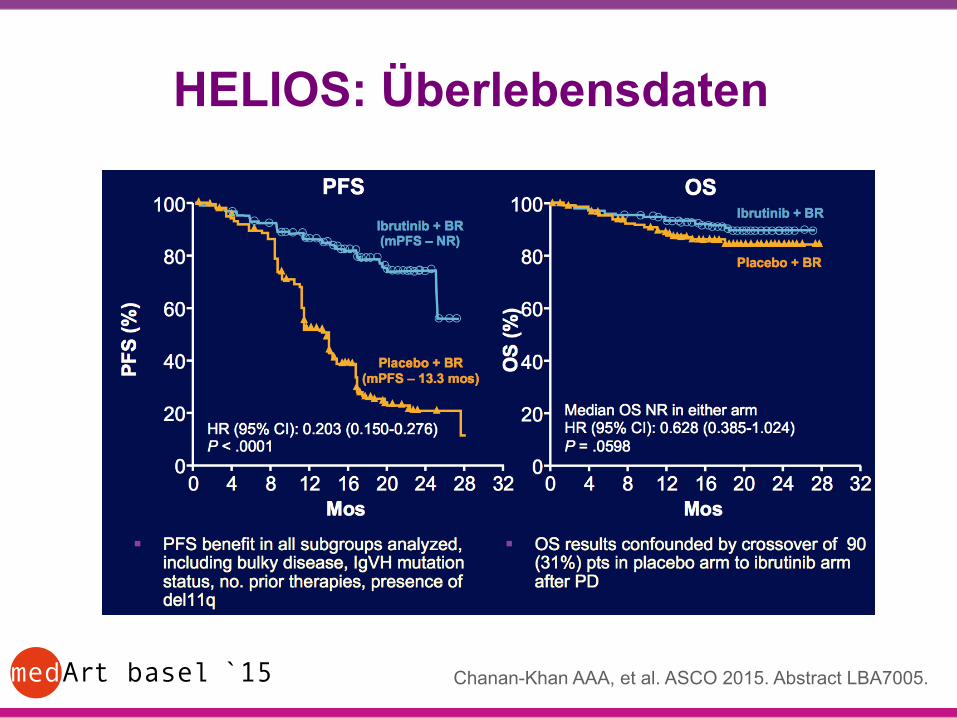
HELIOS: Überlebensdaten
Chanan-Khan AAA, et al. ASCO 2015. Abstract LBA7005.

medArt basel ̀ 15
HELIOS: Safety
Outcome, % Ibrutinib + BR (n = 289)
Placebo + BR (n = 289)
Treatment discontinuation § Progression or relapse § AE
29.1 4.8
14.2
64.7 45.0 11.8
Grade 3/4 treatment-emergent AE ≥ 5% of pts § Neutropenia § Thrombocytopenia § Anemia
(n = 287)
53.7 15.0 3.5
(n = 287)
50.5 15.0 8.0
Any grade bleeding § Major hemorrhage
31.0 3.8
14.6 1.7
Atrial fibrillation § Grade 3/4
7.3 2.8
2.8 0.7
Chanan-Khan AAA, et al. ASCO 2015. Abstract LBA7005.
medArt basel ̀ 15
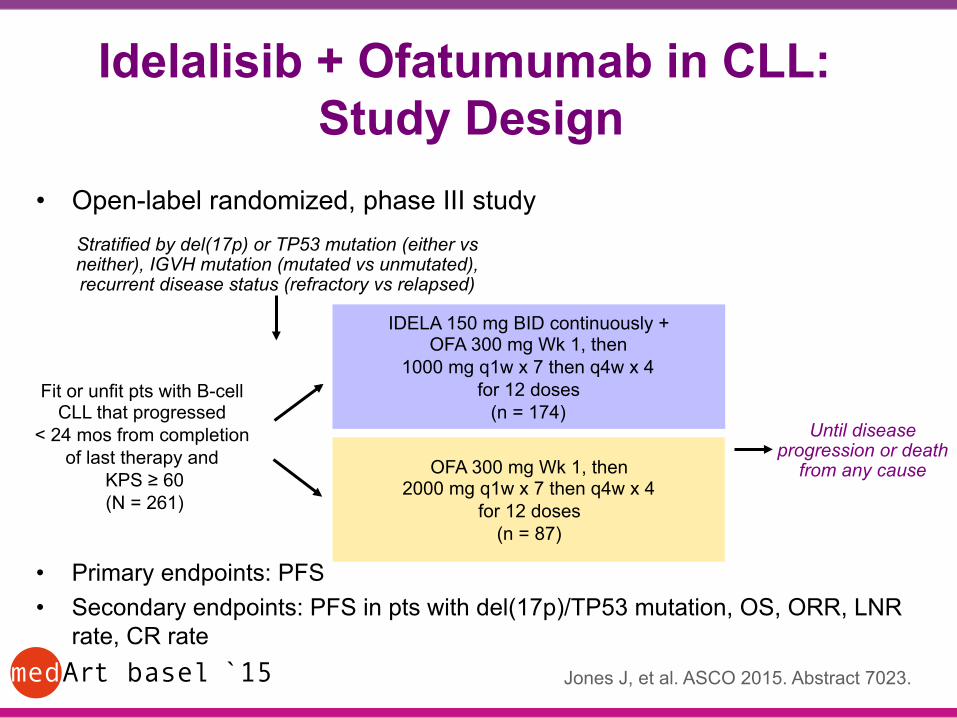
Idelalisib + Ofatumumab in CLL: Study Design
• Open-label randomized, phase III study
• Primary endpoints: PFS • Secondary endpoints: PFS in pts with del(17p)/TP53 mutation, OS, ORR, LNR
rate, CR rate
Fit or unfit pts with B-cell CLL that progressed
< 24 mos from completion of last therapy and
KPS ≥ 60 (N = 261)
IDELA 150 mg BID continuously + OFA 300 mg Wk 1, then
1000 mg q1w x 7 then q4w x 4 for 12 doses
(n = 174)
OFA 300 mg Wk 1, then 2000 mg q1w x 7 then q4w x 4
for 12 doses (n = 87)
Until disease progression or death
from any cause
Stratified by del(17p) or TP53 mutation (either vs neither), IGVH mutation (mutated vs unmutated), recurrent disease status (refractory vs relapsed)
Jones J, et al. ASCO 2015. Abstract 7023.
medArt basel ̀ 15
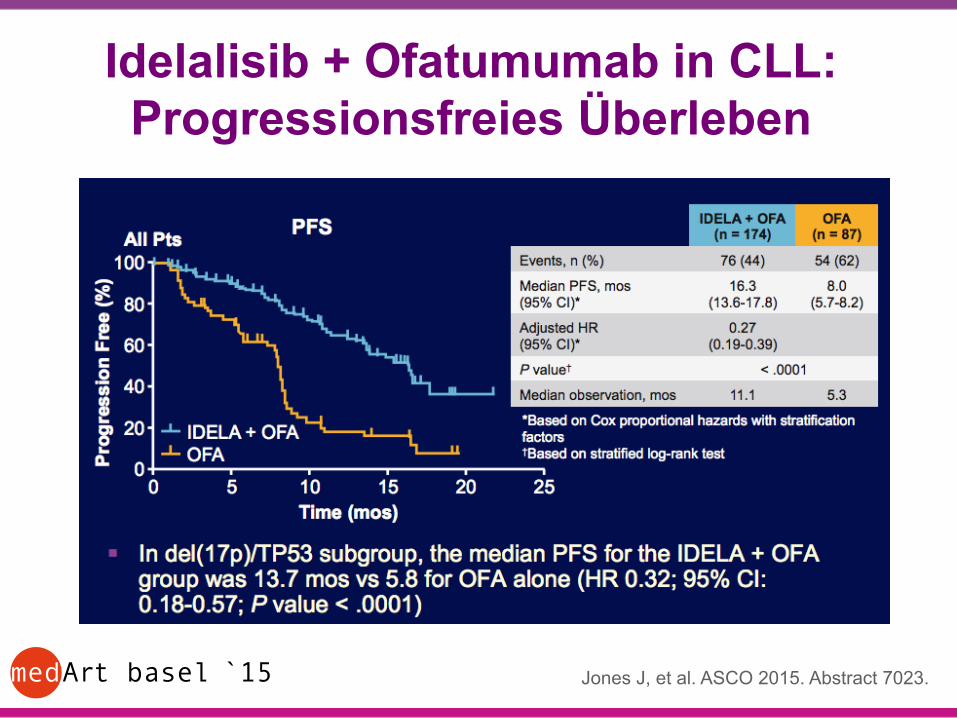
Idelalisib + Ofatumumab in CLL: Progressionsfreies Überleben
Jones J, et al. ASCO 2015. Abstract 7023.
medArt basel ̀ 15
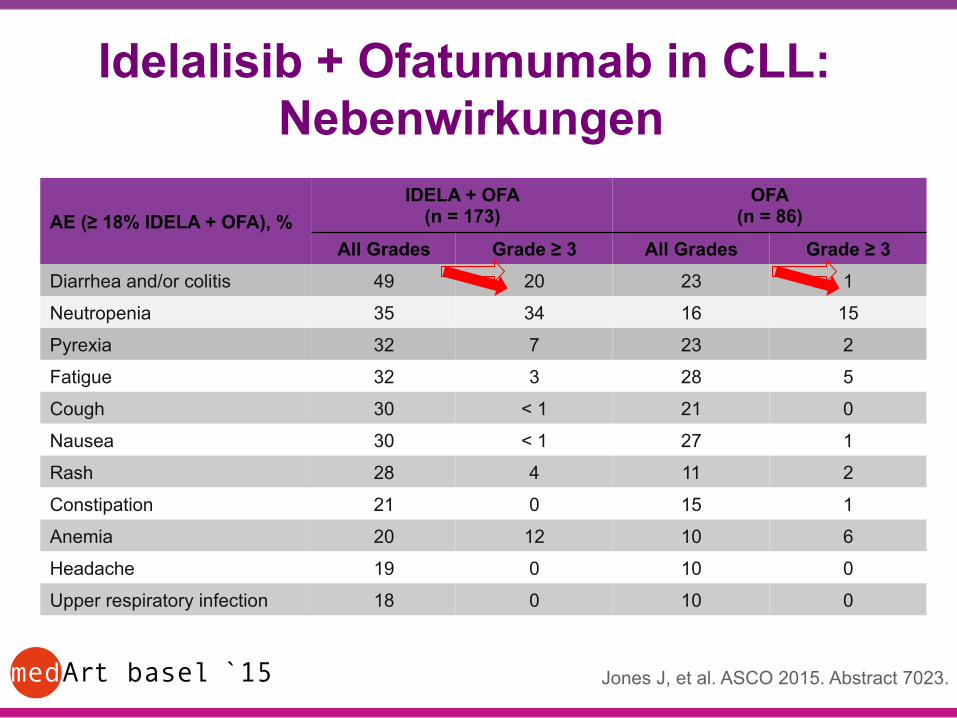
Idelalisib + Ofatumumab in CLL: Nebenwirkungen
AE (≥ 18% IDELA + OFA), % IDELA + OFA
(n = 173) OFA
(n = 86)
All Grades Grade ≥ 3 All Grades Grade ≥ 3 Diarrhea and/or colitis 49 20 23 1
Neutropenia 35 34 16 15
Pyrexia 32 7 23 2
Fatigue 32 3 28 5
Cough 30 < 1 21 0
Nausea 30 < 1 27 1
Rash 28 4 11 2
Constipation 21 0 15 1
Anemia 20 12 10 6
Headache 19 0 10 0
Upper respiratory infection 18 0 10 0
Jones J, et al. ASCO 2015. Abstract 7023.
medArt basel ̀ 15
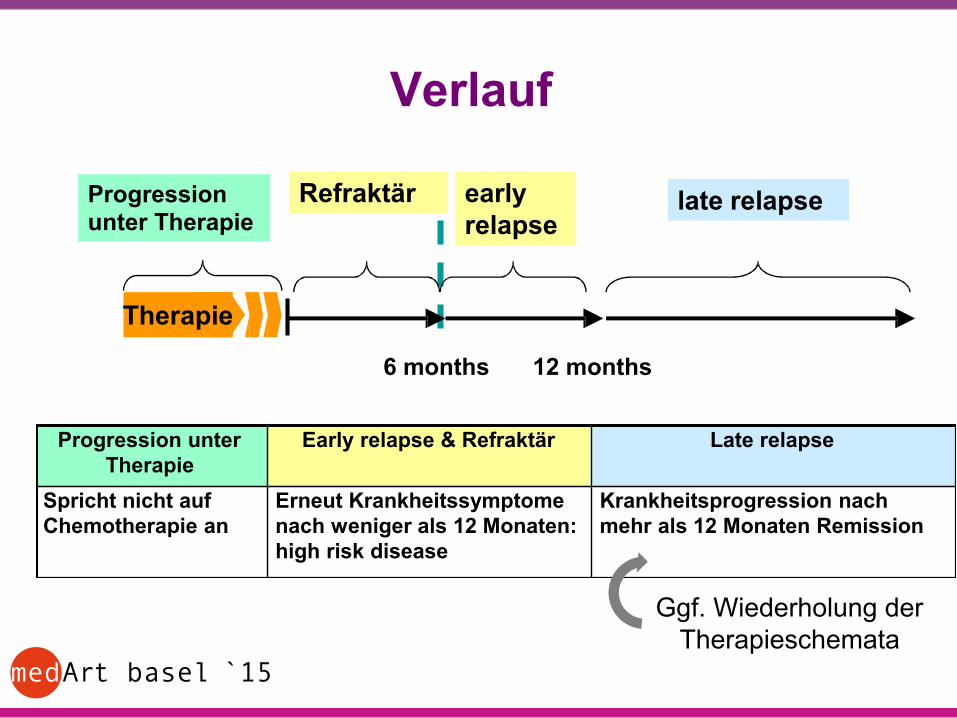
Verlauf
6 months
Progression unter Therapie
late relapse early relapse
12 months
Therapie
Refraktär
Progression unter Therapie
Early relapse & Refraktär Late relapse
Spricht nicht auf Chemotherapie an
Erneut Krankheitssymptome nach weniger als 12 Monaten: high risk disease
Krankheitsprogression nach mehr als 12 Monaten Remission
Ggf. Wiederholung der Therapieschemata

medArt basel ̀ 15
Rezidiv / Refraktärität Hochrisiko-CLL:
- refraktär bzw. mit frühes Rezidiv (<12 Monate) nach Purinanalogon-haltiger Therapien oder im Rezidiv (<24 Monate) nach Purinanalogon-Kombinationsbehandlung oder ähnlich intensive Behandlung; del17p oder p53 Mutation behandlungsbedürftig.
- Überleben median ca. 1-2 Jahre nach Start der Salvage Therapie - Optionen: • Idelalisib/Rituximab • Ibrutinib • (Alemtuzumab) • Ofatumumab (bei Progress unter Fludarabin-haltiger Therapie und
Alemtuzumab mono) • Bei „fittem" Patienten: allogene Transplantation – bisher einzig
kurative Option
seit 03/2015 in der Schweiz zugelassen

medArt basel ̀ 15
Referenzen • Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a
report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood 111:5446-5456, 2008.
• Dreger P, Schetelig J, Andersen N et al: Managing high-risk chronic lymphocytic leukemia during transition to a new treatment era: Stem cell transplantation or novel agents. A position statement of the European Research Initiative on CLL (ERIC) and the European Society for Blood and Marrow Transplantation (EBMT). Blood. 2014 Dec 18;124(26):3841-9.
• Fischer K, Cramer P, Busch R, et al: Bendamustine in combination with rituximab for previously untreated patients with chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol 30:3209-3216, 2012.
• Goede V, Fischer K, Busch R, et al: Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med 370:1101-1110 , 2014.
• Byrd JC, Brown JR, O’Brien S, et al: Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med 371:213-223, 2014.
• Furman RR, Sharman JP, Coutre SE, et al: Idelalisib and rituximab in relapsed chronic lymphocytic leukemia. N Engl J Med 370:997-1007, 2014.
• Byrd JC, Furman RR, Coutre SE, at al: Ibrutinib Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369:32-42, 2013.
• Hodgson K, Ferrer G, Pereira A et al.: Autoimmune cytopenia in chronic lymphocytic leukemia: diagnosis and treatment. Brit J Haematol 154:14-22, 2011.
• Clive S. Zent and W. Richard BurackMutations in chronic lymphocytic leukemia and how they affect therapy choice: focus on NOTCH1, SF3B1, and TP53. Hematology 2014 2014:119-124.
• Adrian Wiestner. BCR pathway inhibition as therapy for chronic lymphocytic leukemia and lymphoplasmacytic lymphoma. Hematology 2014 2014:125-134;