Embed Size (px)
Citation preview

Surg Today Jpn J Surg (1996) 26:225-229
~ SUI~EI~¥TooA¥ © Springer-Verlag 1996
Original Articles
Chronological Changes in the Complement System in Sepsis HAJIME NAKAE, 1 SHIGEATSU ENDO, 1 KATSUYA INADA, 2 and MASAO YOSHIDA 2
* Critical Care and Emergency Center and 2 Department of Bacteriology, Iwate Medical College, 19-1 Uchimaru, Morioka, Iwate 020, Japan
Abstract: The time courses of serum complement levels and the severity of sepsis were compared in two groups of septic patients, one in which the patients survived (surviving group) and one in which they did not (nonsurviving group). The components of the complement system, namely, C3a, C4a, CSa, CHS0, 123, 174, and CS, were measured at several points in time after the diagnosis of sepsis had been established. A 2- antibody radioimmunoassay was used to measure C3a, C4a, and C$a; the latex agglutination test was used to measure C3 and 124; nephelometry was used to measure 175; and Meyer's 50% hemolysis method was used to measure CHS0. Following the diagnosis of sepsis, the levels of CHS0, t73, and C4 were significantly lower in the nonsurviving than the surviving group, while the levels of C3a and C4a were significantly higher in the nonsurviving than the surviving group. The CSa levels were significantly higher in the nonsurviving than the surviving group, although no significant intergroup differ- ences were subsequently noted. These results suggest that the serum levels of C3a, C4a, C$a, CHS0, C3, and C4 could serve as indices of the severity of sepsis. Thus, monitoring the complement system may be useful for predicting the outcome of patients with sepsis.
Key Words: complement system, sepsis, chronological change, severity
Introduction
Patients who develop disseminated intravascular coagu- lation (DIC) and sepsis have reduced serum levels of the complement components as a result of the consump- tion of these complements, 1-4 but enhanced comple- ment activity. 5,6 Recent advances in radioimmunoassay techniques have made it possible to measure the me-
Reprint requests to: H. Nakae (Received for publication on Feb. 17, 1995; accepted on Nov. 7, 1995)
tabolites of the activated complements, C3a, C4a, and C5a. 7,8 Although changes have been reported in the complement system of animals over short periods of time, no clinical reports of long-term chronological studies of the entire complement system have been pub- lished? ,9,1° In a previous study, we reported activation of the complement system in sepsis: 4 therefore, in the present study, we compared the time course of the complement levels during the 2-week period following the diagnosis of sepsis, between patients with severe sepsis who died (nonsurviving group) and those who survived (surviving group), to determine whether sig- nificant differences existed between the two groups. We conducted this study to examine the relationship be- tween the chronological changes in serum complement levels and the severity of sepsis. Seve.rity was then sepa- rately evaluated in the surviving and nonsurviving groups.
Materials and Methods
Informed consent for participation in this study was obtained from all patients or their families and approval was given by the Ethics Committee of Iwate Medical University. A total of 14 patients who developed sepsis, being 8 men and 6 women ranging in age from 26 to 76 years, with a mean age of 52.9 _+ 16.5 years, were stud- ied. The underlying causes of sepsis were multiple inju- ries in 6 patients, perforation of the digestive tract in 3, pneumonia in 3, poisoning in 1, and 98% total surface area burns in 1. Of the 14 patients, 6 died during the study period (Table 1), whereas the surviving-group patients completely recovered and were discharged. The nonsurviving-group patients died of sepsis irrespec- tive of the interval between the diagnosis of sepsis and death. The mean age of the surviving group was 50.3 _ 15.8 years and that of the nonsurviving group was 56.5 _+ 18.2, without significant difference.

226
Taibe 1. Clinical characteristics of the 14 patients with sepsis
Patient Age Sex Main causes of sepsis Outcome
1 ~ 28 M Multiple trauma Survived 2 a,b 76 M Perforation of the digestive tract Died (*6 days) 3 a,b 61 M Perforation of the digestive tract Died ('14 days) 4 26 F Pneumonia Died ('61 days) 5 b 52 F Poisoning Died (*8 days) 6 63 M Perforation of the digestive tract Survived 7 b 54 M Multiple trauma Survived 8 51 F Multiple trauma Survived 9 36 F Multiple trauma Survived
10 72 M Pneumonia Survived 11 a,b 73 M Multiple trauma Died ('17 days) 12 b 63 F Multiple trauma Survived 13 a,b 51 M Burn (**98%) Died ('14 days) 146 35 F Pneumonia Survived
~ Septic shock b Multiple organ failure * Period from the time when sepsis was diagnosed to death ** Total burn surface area
H. Nakae et al.: Complement System in Sepsis
The diagnostic criteria for sepsis, septic shock, and multiple organ failure are shown in Table 2.11 Samples were serially obtained six times, at the diagno- sis of sepsis, then 1, 3, 5, 7, and 14 days later. Blood samples were immediately centrifuged at 3,000 rpm for 10min and the serum obtained stored at - 80°C until assayed.
The serum levels of C3a, C4a, and C5a were mea- sured using a two-antibody radioimmunoassay kit (Amersham, Buckinghamshire, UK). These assays are based on the competition between unlabelled C3a (C4a, C5a) and C3a (C4a, C5a) des Arg and a fixed quantity of [125I]-labelled C3a (C4a, C5a) des Arg for a limited number of binding sites on a specific antibody. The standard ranges were 50-200ng/ml for C3a, 50-250ng/ ml for C4a, and below 10ng/ml for C5a. The serum levels of C3 and C4 were measured with the latex agglu- tination test (Eikenkagaku, Tokyo, Japan). Immedi- ately after the addition of a specific antibody bound with latex particles, C3 and C4 initiate the antigen-anti- body reaction, resulting in an increase in the coagula- tion of masses of latex particles. When the coagulation masses are irradiated with light at a certain wavelength, the scattering light increases in proport ion to the size of the coagulation masses, and this increase in scattering light is quantified by the rate assay. The standard range of C3 was 60-116mg/dl and that of C4, 15-44mg/dl. Serum levels of C5 were measured by nephelometry, the standard range being 8.0-15.0mg/dl. By using this method, the antigen-antibody reaction occurs in the so- lution, and the resulting antigen-antibody precipitates are irradiated with the appropriate light. The resultant scattering light is measured, and the antigen concen- tration is determined from its intensity. CH50 was measured using Meyer 's 50% hemolysis method, the
Table 2. Diagnostic criteria
Sepsis: Definite site of infection or positive blood culture Temperature ->38.5°C or -<35.5°C Leukocyte count ->15,000 or -<3,000/mm 3
Septic shock: Sepsis with hypotension despite adequate fluid resuscitation, with perfusion abnormalities which may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration in mental status. Patients who are on inotropic or vasopressor agents may not be hypotensive at the time that perfusion abnormalities are measured.
Hypotension: Systolic blood pressure <90mmHg or a reduction of >40mmHg from the baseline in the absence of other causes for hypotension.
Multiple organ failure: Presence of altered organ function in an acutely ill patient such that homeostasis cannot be maintained without intervention.
standard range being 30.0-40.0U/ml. In the reaction solution, sensitized sheep erythrocytes are reacted with serum samples. After incubation, the reaction solution is then centrifuged, and the amount of hemoglobin ox- ide in the supernant, eluted as a result of hemolysis by the complements, is colorimetrically determined at 541 nm.
The values for each parameter was expressed as means + the standard deviation (SD). The significance of differences for each day was tested using the un- paired Wilcoxon test, and chronological change was determined by analysis of variance (ANOVA) for re- peated measures. A level of P < 0.05 was considered statistically significant.

H. Nakae et al.: Complement System in Sepsis 227
Results
CH50 Levels
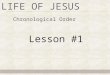
The CH50 levels, measured at the diagnosis of sepsis, were significantly lower in the nonsurviving group than in the surviving group at 31.1 +__ 11.4 and 45.2 +_ 10.1 U/ ml, respectively (P = 0.040). This parameter continued to be significantly lower in the nonsurviving group than in the surviving group (P = 0.0186), as shown in Fig. la.
C3 and C3a Levels
The C3 levels measured at the time of diagnosis did not differ significantly between the surviving and nonsurviving groups at 87.5 +- 17.5 and 65.0 _ 24.3 mg/ dl, respectively (P +__ 0.0660). When measured sub- sequently, this parameter was significantly lower in the nonsurviving group than in the surviving group
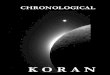
(P = 0.0007), as shown in Fig. lb. The C3a levels at the time of diagnosis were significantly higher in the nonsurviving group than in the surviving group at 1091.5 -+ 500.5 and 628.6 _+ 192.5mg/dl, respectively (P = 0.0326). This parameter subsequently continued to be significantly higher in the nonsurviving group than in the surviving group (P < 0.0001), as shown in Fig. 2a.
C4 and C4a Levels
The C4 levels at the time of diagnosis were significantly lower in the nonsurviving group than in the surviving group at 22.3 +- 2.5 and 30.5 + 8.6mg/dl, respectively (P = 0.0451). This parameter continued to be significantly lower in the nonsurviving group than in the surviving group (P = 0.0014), as shown in Fig. lc. The C4a levels at the time of diagnosis were significantly higher in the nonsurviving group than in the surviving group at
* U / m h
71~ "
1~ [ •
5~ '
4() '
~l)
2<~ '
111 '
q)
" ~ - Survivor~
~ Nollg~I~ivt)rg
(¢tab t
~1 I 3 5 7 14
TIME
a. C H 5 0
tlllg/,lll
~)
~q)
219
•
I q ~ "
:k
--O-- Survivors
~ Nonsurvivors
0 I 3 5 7 14 I,l.t~. I
TIME
C. C4
Fig. la-d. Time course of the complement levels, a CH50 levels were significantly lower in the nonsurviving group than in the surviving group, b C3 levels were significantly lower in the nonsurviving group than in the surviving group. c C4 levels were significantly lower in the nonsurviving group
mag/dh
! _
I (K I " I
g,
. . . . . . . . . . . . .
- -O- Sur~ i',~)rs
~ ~OIISU~ ~ OrS
. ,, . ,,
0 l 3 5 7 14 (,l:ty~
TIME
b. C3
hn~dl~
I0
- , 0 - Surx i~t~r,
~ ~OllsurM~ orx
f~ I 3 5 7 14 I,lay~
TIME
d. C5
than in the surviving group, d No significant intergroup differences were observed in the course of C5 levels over time. *P < 0.05; **P < 0.0001. Open circles, survivors; closed circles, nonsurvivors. Values are expressed as means +_ SD

228 H. Nakae et al.: Complement System in Sepsis
~ H X I
3(XW)
~", 2(WW) r j
HXX)
t n~lmll
•L•• 1 .-O- Survivors ~ Nonsurvivors
~ ** . . . . . . . . .
1~ I 3 5 7 14 Itlay)
TIME
a. C3a mg/mb
Inldml)
611(11) '
[ -~" Survivors 5(wxl
-., * *
I ( ~ ) " ,
~ . ~ ~ ........... ~ . ' .............. - = : : = .
-II~) 0 I 3 5 7 14 I(~y~
~ME
b. C4a
LO " ••! i "O- Survivors --O,- N t~nsurvi'.,~w',
1
.N.$.
(I 1 3 5 7 14
TIME
Iday~
c. C5a
Fig. 2a-c. Time course of the metabolites of the activated complement levels, a C3a levels were significantly higher in the nonsurviving group than in the surviving group, b C4a levels were significantly higher in the nonsurviving group
than in the surviving group, e No significant intergroup differences were observed in the course of C5a levels over time. *P < 0.05; **P < 0.0001. Open circles, survivors; closed circles, nonsurvivors. Values are expressed as means _+ SD
2,385.0 +_ 1,697.7 and 631.1 _+ 545.8ng/dl, respectively (P = 0.0017). This parameter continued to be signifi- cantly higher in the nonsurviving group (P < 0.0001), as shown in Fig. 2b.
C5 and C5a Leve~
The C5 levels at the time of diagnosis did not differ significantly between the surviving and nonsurviving groups with values of 12.3 + 1.3 and 10.5 +_ 3.7mg/ml, respectively (P = 0.2233). This parameter subsequently tended to be lower in the nonsurviving group than in the surviving group, although the differences were not sig- nificant (P = 0.0722), as shown in Fig. ld. The C5a levels at the time of diagnosis were significantly higher in the nonsurviving group than in the surviving group at 10.0 _+ 2.9 and 6.1 _+ 1.9 mg/ml, respectively (P = 0.010). No significant intergroup differences were subsequently noted in this parameter (P = 0.0703), as shown in Fig. 2c.
Discussion
In the present study, we found that the serum levels of C3a and C4a measured at the time that sepsis was diag- nosed were significantly higher in patients who did not survive than in those who did. Thus, these two param- eters reflected the severity of sepsis. Moreover, when they were followed over time, they continued to be significantly higher in the nonsurviving group than in the surviving group. These results suggest the impor- tance of C3a and C4a measurements, not only in diag- nosing sepsis, but also in determining the prognosis of septic patients.
C5a has been reported to show the highest biological activity as an anaphylatoxin, and because it enhances the endotoxin-induced production of cytokines it is thought to play an important role in sepsis. 12,~3 In the present study, the C5a levels measured when sepsis was diagnosed were significantly higher in the nonsurviving group than in the surviving group, reflecting the severity

H. Nakae et al.: Complement System in Sepsis 229
of sepsis. Interestingly, the measurement of this param- eter at subsequent points failed to reveal any significant differences between the two groups. However , the dis- appearance of significant intergroup differences in this pa ramete r with t ime is probably due to the short half- life of C5a, since it rapidly binds to the receptors on polymorphonuclear leukocytes. TM
The concentrations of CH50, C3, and C4 at multiple points after the diagnosis of sepsis were significantly lower in the nonsurviving group than in the surviving group. A decrease in complement levels is repor ted to reduce opsonin activity 1~ and the body's defense mecha- nisms, leading to an exacerbat ion of disease. Therefore, monitoring the levels of CH50, C3, and C4 also seems to be important for determining the prognosis of septic patients.
The alternative pathway is thought to be activated in the early stages of sepsis when no changes in hemody- namics are evident, whereas the classical pathway is activated in the later stages. 2,3 When only the alternative pathway is activated, the C4 levels remain unchanged, while C3 decreases and C3a increases. All of our pa- tients demonstra ted elevated levels of C4a when sepsis was diagnosed, indicating that both pathways of the complement system were activated at that time. These findings suggest that both pathways are often activated before the diagnosis is made in cases of severe sepsis ultimately leading to death. In fact, in the patients who died, the complement levels were not only high at the time when sepsis was diagnosed, but they remained per- sistently high thereafter. This persistence of the activity of the complement system may have further aggravated the general condition of the patient, increasing the se- verity of the disease. In conclusion, the results of this study strongly indicate that the complement system is closely related to the course of severe sepsis, and that its measurement , levels, and activity may be useful for de- termining the prognosis of individual patients who de- velop this disorder.
Acknowledgments. This research was supported in part by grants for the development of characteristic education by the Japan Private School Promotion Foundation and the Marumo Emergency Medical Research Fund, Japan.
References
1. Kane MA, May JE, Frank MM (1990) Interaction of the classical and alternative complement pathway with endotoxin in li- popolysaccharide. J Clin Invest 52:370-376
2. Leon C, Rodrigo MJ, Tomasa A, Gallart MT, Latorre F J, Rius J, Brugues J (1982) Complement activation in septic shock due to gram-negative and gram-positive bacteria. Crit Care Med 10:308- 310
3. Sprung CL, Schultz DR, Marcial E, Caralis PV, Gelbard MA, Arnold PI, Long WM (1986) Complement activation in septic shock patients, Crit Care Med 14:525-528
4. Nakae H, Endo S, Inada K, Takakuwa T, Kasai T, Yoshida M (1994) Serum complement levels and severity of sepsis. Res Commun Chem Pathol Pharmacol 84:189-195
5. Langlois PF, Gawryl MS (1988) Accentuated formation of the terminal CSb-9 complement complex in patient plasma precedes development of the adult respiratory distress syndrome. Am Rev Respir Dis 138:368-375
6. Hack CE, Nuijens JH, Felt-Bersma RJF, Schreuder WO, Eerenberg-Belmer AJM, Paardekooper J, Thijs LG (1989) El- evated plasma levels of the anaphylatoxins C3a and C4a are associated with a fatal outcome in sepsis. Am J Med 86:20-26
7. Chenoweth DE, Hugli TE (1980) Techniques and significance of C3a and C5a measurement. In: Future perspectives in clinical laboratory immunoassays. Nakamura RM, Alan R (eds) Liss, New York, pp 443-460
8. Gorski JP (1981) Quantitation of human complement fragment C4a in physiological fluids by competitive inhibition radioimmu- noassay. J Immunol Methods 47:61-73
9. Dofferhoff AS, deJong HJ, Born VJ, van der Meer J, Limburg PC, de Vries-Hospers HG, Marrink J, Mulder PO, Weits J (1992) Complement activation and the production of inflammatory me- diators during the treatment of severe sepsis in humans. Scand J Infect Dis 24:197-204
10. McCabe WR (1992) Serum complement levels in bacteremia due to gram-negative organisms. New Engl J Med 288:21-23
11. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee (1992) Definitions for sepsis and organ failure and guidelines for the use of innova- tive therapies in sepsis. Crit Care Med 20:864-874
12. Cavaillon JM, Fitting C, Haeffner-Cavaillon N (1990) Recombi- nant C5a enhances interleukin-1 and tumor necrosis factor release by lipopolysaccharide-stimulated monocytes and mac- rophages. Eur J Immunol 20:253-257
13. Scholz W, McClurg MR, Cardenas GJ, Smith M, Noonan DJ, Hugli TE, Morgan EL (1990) C5a-mediated release o f interleukin-6 by human monocytes. Clin Immunol Immunopathol 57:297-307
14. Huey R, Hugli TE (1985) Characterization of a C5a receptor on intact human polymorphonuclear leukocytes (PMN). J Immunol 135:2063-2068
15. Alexander JW, McClellan MA, Ogle CK, Ogli JD (1976) Con- sumptive opsoninopathy. Ann Surg 184:672-678