Embed Size (px)
DESCRIPTION
Imaging in podiatry. Radiography, Ultrasonography
Citation preview
CE
DIRECTED READING. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
25RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
ELIZABETH J CHURCH, JD
Imaging in Podiatry
After completing this article, readers should be able to:■ Understand the anatomy of and various functions performed by the foot.■ Describe in general terms the injuries and diseases to which the foot is susceptible, including
complications common among patients with diabetes.■ Discuss which imaging modalities are most useful in the diagnosis of specific foot problems.■ Be aware of why the complexity of the foot’s anatomy poses particular imaging challenges.■ Explain how imaging assists in assessing the success of different treatments for foot disorders.
This article examines the vulnerability of the foot to injury and disease and the role imaging plays in ferreting out the causes of pain and dysfunction. The discussion includes a broad overview of foot disorders and describes the expanding role played by imaging in the diagnosis and management of foot disorders.
This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your area of interest. For access to other quizzes, go to www.asrt.org/store.
In the United States, approximately 40% of adults suffer from foot problems.1 Chronic foot pain is not only common but also can affect everyday activities such as walking,
standing and driving. Even when patients provide detailed histories and clinicians conduct careful physical examinations, an accurate diagnosis can remain elusive, given the plethora of possible causes.
Imaging is capable of illuminating biomechanics and tissue swelling, and it can help confirm clinical suspicions, distinguish lesions and contribute other facts relevant to the diagnostic puzzle.2 Sometimes, imaging proves useful in early identification of a degenerative disease process such as rheumatoid arthritis, and it assists in evaluating the effectiveness of different available treatments.
Although the entire spectrum of foot disorders is beyond the scope of this arti-cle, a solid range of diseases and anoma-lies will be examined. Because the com-plicated, overlapping anatomy of the foot can pose difficulties in terms of patient positioning, choice of imaging modality and interpretation of imaging studies, this article also includes a discussion of practical considerations in the context of each foot disorder.3
Foot FundamentalsFunction
The foot is one of the harder-working, if underappreciated, portions of human anatomy. Feet support us; they permit us to walk, run, jump, skip, dance, climb and kick. The importance of the foot is reflected in our language, in which it can be a unit of measurement or a descriptor, such as swift of foot, feet first, foot soldier, underfoot, footman, foot traffic, foot-bridge and footstool.4 A person can be knocked off his feet, put her foot in her mouth or, if lucky, get a foot in the door. To evolutionary biologists, the foot is what puts homo sapiens in an upright position, gives us eyes that face forward and helps us remain at the top of the food chain.5
The human foot evolved to withstand and adapt to a range of stresses resulting from locomotion; it acts both as a shock absorber and rigid lever.6 Progressive evo-lutionary changes in the skeletal and soft tissue composition of the foot resulted in a reduction in grasping function, formerly assigned to the big toe (the “prehensile role”), and certain bones enlarged over time to form a sturdy yet flexible struc-ture.5,6 Development of the heel led to the unique arch of the human foot, forming a structure that provides humans with the
R0908_PodDR_25-44.indd 25R0908_PodDR_25-44.indd 25 8/28/08 1:45:26 PM8/28/08 1:45:26 PM
CEIMAGING IN PODIATRY
26 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Pediatric Foot DisordersAt birth, the human foot appears flat, and a child’s
foot is relatively shorter and wider than that of an adult.7 The flat appearance is due to a fatty pad on the sole of the foot that is absorbed gradually during the first year of a child’s life. The shape of a child’s foot also differs from that of an adult in that the heel and hindfoot are less developed than the forefoot. As previously stated, the heel is largely responsible for our ability to stand, balance and walk; when that portion of a child’s foot becomes more developed, he or she can begin to walk, balance and stand. The ultimate shape of an individual’s
posterior support and stability upon which to balance an upright body.6
Basic AnatomyFeet come in a variety of shapes.
Thanks to genetic contributions, some feet are long and narrow and thus more likely to be structurally unstable.6 Others are short and broad, while still others are triangular with a broad fore-foot and narrow heel (reportedly the most vulnerable of the 3 foot types).6 Because the foot falls at the end of a kinetic chain (“the foot bone’s con-nected to the ankle bone . . . ”), it is particularly responsive to variations in normal anatomy and all pathologi-cal disorders that fall above it.7 Often, this means that what appears to be a foot disorder might instead represent a reaction or adaptation to a pathology present in the body above the foot.
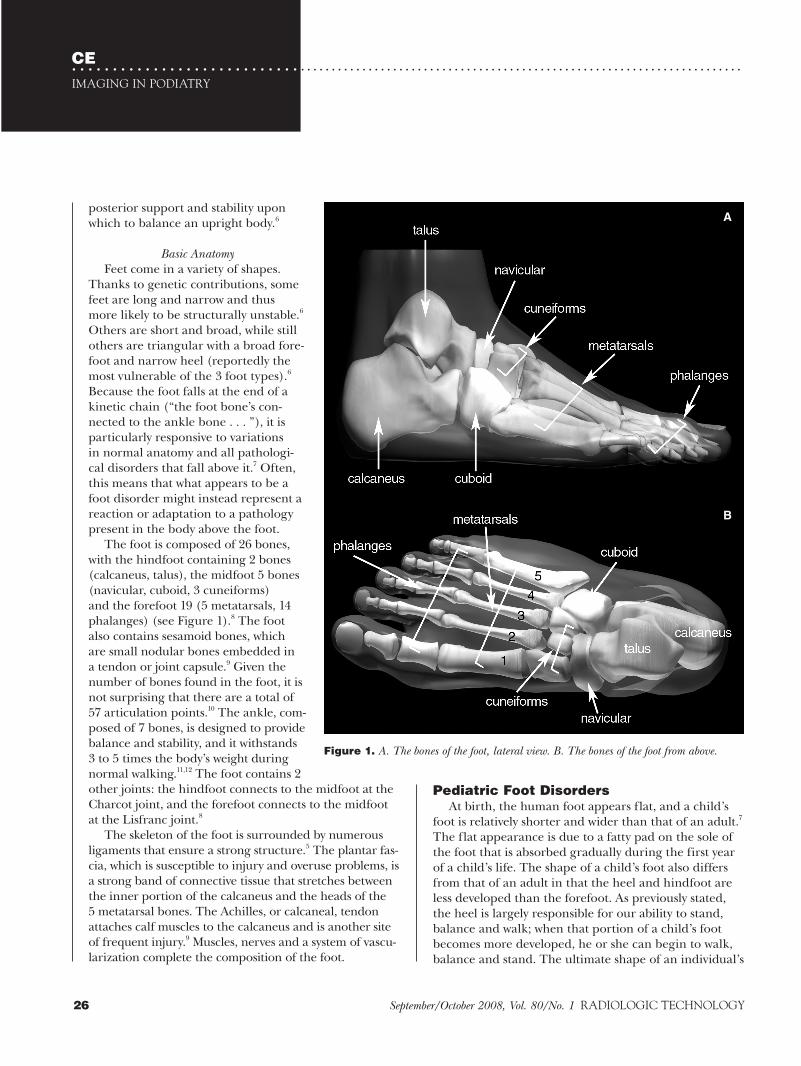
The foot is composed of 26 bones, with the hindfoot containing 2 bones (calcaneus, talus), the midfoot 5 bones (navicular, cuboid, 3 cuneiforms) and the forefoot 19 (5 metatarsals, 14 phalanges) (see Figure 1).8 The foot also contains sesamoid bones, which are small nodular bones embedded in a tendon or joint capsule.9 Given the number of bones found in the foot, it is not surprising that there are a total of 57 articulation points.10 The ankle, com-posed of 7 bones, is designed to provide balance and stability, and it withstands 3 to 5 times the body’s weight during normal walking.11,12 The foot contains 2 other joints: the hindfoot connects to the midfoot at the Charcot joint, and the forefoot connects to the midfoot at the Lisfranc joint.8
The skeleton of the foot is surrounded by numerous ligaments that ensure a strong structure.5 The plantar fas-cia, which is susceptible to injury and overuse problems, is a strong band of connective tissue that stretches between the inner portion of the calcaneus and the heads of the 5 metatarsal bones. The Achilles, or calcaneal, tendon attaches calf muscles to the calcaneus and is another site of frequent injury.9 Muscles, nerves and a system of vascu-larization complete the composition of the foot.
A
B
Figure 1. A. The bones of the foot, lateral view. B. The bones of the foot from above.
R0908_PodDR_25-44.indd 26R0908_PodDR_25-44.indd 26 8/29/08 10:45:14 AM8/29/08 10:45:14 AM

CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
27RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
vascular injury or an abnormality of the intrauterine environment.14 Risk factors include a family history of the condition and being male: Boys are affected twice as often as are girls.
One or both feet may be affected. When clubfoot is present, the foot turns inward and downward and resists realignment. The calf muscle and the foot also may be slightly smaller than normal.15 Two types of the disorder are recognized: those which respond to early fixation in a corrected position and those which do not respond, thus requiring surgical treatment.7 When required, sur-gery typically is performed very early on, between the ages of 3 and 6 months. Clubfoot that is not treated suc-cessfully in infancy can cause problems for adults when pressure is distributed improperly over the foot, particu-larly along the outer border. An inadequately corrected clubfoot can cause problems with footwear and long-term degenerative changes in foot joints.16 This painful condition can require several corrective surgeries.7
Clubfoot is identified by physical examination.15 Although aggressive surgical interventions once were favored by the medical community, the results tended to be unsatisfactory — significant stiffness and limitation of motion often resulted from postoperative scarring.14 Now, nonsurgical approaches such as those described by Hippocrates have come back into favor, with claimed success rates of up to 90%. The current approach to treatment involves moving the foot into the correct position and using a cast to maintain the position.15 This is accomplished as soon as possible after birth, when the foot is most malleable. Gentle stretching and recasting is performed on a weekly basis and repeated from 5 to 10 times. The final cast is kept in place for 3 weeks, and once the foot is positioned properly, the child wears a special brace, full time, for close to 3 months. Thereafter, the brace is used only at night and during naps for 2 to 4 years.14 Sometimes, an outpatient procedure is required to release the Achilles tendon, which may be tight because of the altered foot position. Children typically are monitored until they are fully grown to ensure that the realignment results in proper function.15
Although physical examination generally is used to identify clubfoot, some practitioners assert that radio-graphic assessment is more accurate.14 A drawback to such assessment is the lack of ossification of key bones in the infant foot and the inability of radiographs to visualize soft tissue. MR imaging permits good visualiza-tion of soft tissue and cartilage, even through casts, but it can be cost prohibitive and may require sedation. For
feet is not determined until growth is complete, at about 20 years of age; adult shoe sizes are usually reached by 14 years of age.7
Children are susceptible to the same foot disorders as are adults, but some juvenile foot disorders merit special mention. In addition, interpretation of imaging studies may differ when the patient is a child and often requires a knowledge of when certain aspects of the body reach maturity. For example, high-signal T2-weighted bone marrow changes are seen often on magnetic resonance (MR) images of children’s ankles and feet.13 These observed changes can be caused by various factors such as trauma, inflammation, infection, arthritis, cancer, biomechanical and developmental abnormalities and vascular problems.
In a study designed to identify the reason for the observed bone marrow changes, authors described the process of marrow conversion from mostly hematopoi-etic marrow (marrow devoted to forming red blood cells) in the newborn to mostly fatty marrow after age 20 years.9,13 The authors concluded that the high-signal T2 changes seen on MR images of children’s feet and ankles are actually a normal finding. They report that the sig-nal may be caused by regions of residual hematopoietic marrow or physiological stress related to weight bearing (added weight with growth) and altered biomechanics associated with normal growth. The pattern, which is often seen particularly in the calcaneus and talus prior to age 15 years, can be misdiagnosed as a stress or trau-matic injury rather than what it is: a normal maturation process.13 Thus, it is important to understand not only foot anatomy but also the different foot disorders that commonly affect children.
ClubfootSome children are born with structural deformi-
ties such as extra toes (polydactyly) or a malformation known as clubfoot (ie, congenital talipes equinovarus).7 Clubfoot is the most common congenital malforma-tion of the legs, and it occurs in 0.5 to 7 out of 1000 live births.14,15 The abnormality has long been documented in medical literature. Hippocrates described physical manipulation and serial casting of the foot as a pre-ferred treatment, and this approach remained the stan-dard treatment until well into the 19th century.14
Although clubfoot sometimes is associated with cer-tain syndromes and chromosomal abnormalities, most children born with this malformation have no other associated abnormalities. Experts continue to debate the cause of the deformity, with possibilities including
R0908_PodDR_25-44.indd 27R0908_PodDR_25-44.indd 27 8/28/08 1:45:26 PM8/28/08 1:45:26 PM

CEIMAGING IN PODIATRY
28 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
cases, the ossification center fuses with the talus within a year of formation, but in 7% of the population, the center fails to fuse.18 This separate center is called the os trigonum; when it is subjected to repetitive microtrauma or acute forced plantar flexion of the foot, it can be injured, resulting in a chronic stress fracture or acute fracture. The condition, known as os trigonum syn-drome, can be viewed in lateral radiographs but is more readily visible on MR images, which are capable of show-ing inflammatory changes such as edema and fluid.18 The failure of ossification centers to fuse can be asymp-tomatic or symptomatic in adults, depending to some degree upon the forces placed upon the adult foot.
Freiberg DiseaseFreiberg disease, a rare cause of chronic foot pain, is
a condition usually diagnosed in adolescents and charac-terized by pain, tenderness, swelling and limited motion in the affected metatarsophalangeal joint.1 The cause of the disease remains unknown, although traumatic injury (acute or repetitive) and vascular compromise most often are identified as the culprits. Girls are more likely to suffer from the disease, by a ratio of 3 or 4 to 1.Radiographs show characteristic changes such as increased density of the metatarsal head, widening of the metatarsophalangeal joint, flattening, collapse and cystic changes. Bone scans reveal decreased uptake in the early stages of the disease. MR imaging is used for preopera-tive evaluation to ascertain the extent of the lesion.
Joint DiseaseAny joint can be affected by secondary osteoarthritis
resulting from trauma, infection or other joint disease, and the feet are no exception to this rule.19 The most common joint diseases seen in children are juvenile chronic arthritis and septic arthritis. Rheumatoid arthri-tis generally strikes older patients, although juvenile rheumatoid arthritis is seen in children and can, over time, result in joint immobility.2 On the other hand, osteoarthritis and calcium pyrophosphate dehydrate deposition disease generally are found in older patients.19
Stress FracturesChildren are also susceptible to fatigue or stress
fractures. Such fractures are most often seen in athletic children who participate in sports or dance, and the fractures most commonly occur in the second and third metatarsal shafts.7 The fractures might not be visible on a radiograph until 3 weeks or more after the onset of symptoms, and so diagnosis can be delayed.
these reasons, many experts encourage the use of ultra-sound because it does not expose the child to radiation, permits visualization of soft tissue and cartilage and is less costly.14 As recently as 2007, some study authors pro-moted the use of dynamic sonography to assess anato-my and foot flexibility, as well as to classify degrees of malformation.14
The degree of treatment success is measured objec-tively by range of ankle movement, leg and foot muscle strength, proper distribution of pressure throughout the foot, and gait.17 Many practitioners promote the use of radiographs to determine whether management is successful, although there is some evidence that radio-graphs are no more accurate than a patient’s subjective assessment of outcome.17 Typically, radiologists have measured the angle between the talus and the calca-neus as a means of determining foot flexibility, but such measurements are difficult to obtain using radiographs because overlying bones (tibia and fibula) obscure the view — particularly in older children. Others have found success with this practice, using lateral and anteropos-terior (AP) radiographs to measure 3 specific angles/articulations.17
Imaging can be particularly helpful in assessing the success of surgical interventions. Recognized complica-tions of clubfoot surgery include extreme overcorrection and avascular necrosis (cell death due to a deficient blood supply).9,16 MR imaging of the ankle and foot is capable of alerting surgeons to avascular and necrotic changes, while plain radiographs fail to provide this vital information.16
The outcome is good for the majority of patients. Subjectively, girls and their families tend to report worse outcomes, which has led some researchers to believe that girls suffer from a worse form of clubfoot than boys.17 Recently, however, at least 1 study using objective measurements of clubfoot treatment showed that boys and girls experience the same good outcome.17 The study authors theorized that parents might be less satis-fied with imperfect cosmetic results in girls, and that this tendency alone could account for the discrepancies in subjective assessments of success.
Os Trigonum Syndrome As children’s feet mature, cartilage and fibrous tissue
convert to bone or a bony substance. The places where this transformation occurs are referred to as ossification centers, and the foot contains several of these areas.9,18 For example, between 8 years and 13 years of age, an ossification center forms posterior to the talus. In most
R0908_PodDR_25-44.indd 28R0908_PodDR_25-44.indd 28 8/28/08 1:45:26 PM8/28/08 1:45:26 PM

CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
and its causes are unknown. Almost any bone of the body can be involved (thus, the “multifocal” aspect of the disease), although sometimes only 1 site might be symptomatic. A mean of 6 sites of involvement has been reported, and before a diagnosis can be confirmed biop-sy may be required to exclude other conditions, such as tumors. Primarily, this disease must be distinguished from simple osteomyelitis, and MR imaging is “an excel-lent non-ionizing means of investigation” in children and young adults.21 MR imaging is characterized as both sensitive and specific, with the chronic form of osteo-myelitis distinguished from simple osteomyelitis by the absence of abscess formation on MR images. Even after the disease has run its course, MR images still might reveal bone that is abnormal in appearance.21
Hereditary Foot AilmentsGout
As Shakespeare wrote, “A pox of this gout! or a gout of this pox! for the one or the other plays the rogue with my great toe.”22 Although Henry VIII might be remem-bered most often for his uncanny ability to dispose of unwanted wives, he also typically comes to mind when gout is mentioned. King Henry’s court physician recom-mended wearing dog skin hose as a cure for the ailment, and references to gout appear as far back as 2600 bc when Egyptians described gouty arthritis.23 In 1931, gout was pegged as an “inborn error of metabolism” — a product of heredity. Today, the medical community still struggles to find effective treatments for the malady; recent studies indicate both severity and prevalence may be increasing.2
Classic gout is characterized by acute, episodic arthritis of the first metatarsophalangeal joint (the big toe joint).24 Although less common, gout also is seen in the upper limbs (primarily the hands), particularly when there is a long history of the disease. The pain is reported to be agonizing, and attacks are accompanied by swelling, tenderness and warmth of the affected joint. Sometimes called “the great mimicker,” gout must be distinguished from rheumatoid arthritis, osteoarthritis, joint and soft tissue infections, skin cancer, nerve com-pression syndromes, soft tissue tumors and septic arthri-tis.24 The advent of the 21st century has witnessed a renewed interest in investigating and better understand-ing the causes of gout and a continued search for an adequate treatment for the often debilitating disease.23
Gout is caused by deposits of urate crystals in joints.25 An acute or longstanding presence of high urate levels can cause uric acid crystals to form and deposit in the
Kohler DiseaseThe last bone in the foot to ossify is the navicular, the
bone that is situated above the cuboid and anterior to the talus and calcaneus.20 Kohler disease, which is a self-limiting avascular necrosis of the navicular bone, affects children. It is seen most often in boys, and the age of onset is 4 years for boys and 5 years for girls. Although the exact cause is unknown, experts theorize that the delayed maturation of the bone renders it particularly vulnerable to compressive damage, particularly during weight-bearing activities. The compressive forces can block blood flow in the vessels of the soft, immature tissue. When the blood flow is blocked or diminished, cell death occurs and the bone may collapse. Children suffering from this disorder exhibit a painful limp, shift weight to the lateral edge of the foot to relieve pressure, and experience tenderness and swelling in the navicular area. Radiographs reveal irregularity and atrophy of the navicular bone. In about 30% of cases, radiographs demonstrate disease in both feet, although only 1 foot might be symptomatic. The prognosis is excellent; the navicular bone usually regains its normal shape before foot growth is complete, and normal ossification contin-ues, with completion in about 2 years.20
Juvenile Hallux ValgusBunions, commonly associated with old age, can
appear in children and are known as juvenile hallux valgus.7 The condition is described more fully later, but it is important to note that corrective surgery should not be undertaken until the skeleton of the foot is mature, at about 14 years of age. Although footwear typically is blamed for the presence of the condition in teenagers, it is not the cause of bunions. In almost all patients, there is a strong family history of this particular foot deformity. Experts note that “footwear may aggravate an established tendency” for the deformity, and it can increase friction over the involved bones and joint, but it does not cause the condition.7 Radiographs are used to evaluate whether surgery is appropriate and to determine what surgical procedure is likely to be most effective.
OsteomyelitisOsteomyelitis is an inflammation of the bone — a
skeletal infection.9 A form of osteomyelitis known as chronic recurrent multifocal osteomyelitis usually is seen in children and young adults, but it can present in individuals 9 months to 55 years of age.21 The disease can last for as long as 6 months and does not respond to antibiotics. It is twice as common in girls as boys,
R0908_PodDR_25-44.indd 29R0908_PodDR_25-44.indd 29 8/28/08 1:45:26 PM8/28/08 1:45:26 PM

CEIMAGING IN PODIATRY
30 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Tophi appear as soft tissue lumps or ulcerative skin lesions and can cause nerve compression, joint destruc-tion and loss of joint function, as well as deformity.24 When urate crystals are deposited in the renal tract, they can lead to impaired kidney function.28
Conditions associated with gout include obesity, dia-betes, hypertension, heart failure, myocardial infarction, coronary artery disease, alcoholism and renal insufficien-cy.28 The apparent strong link between gout and cardio-vascular disease has led experts to argue that a diagnosis of gout should serve as a red flag, calling for physicians to assess these patients for cardiovascular risk.28
A long-term history of gout can result in significant physiological damage. Gout causes joint erosion in affected joints, and there is a strong association between gout and osteoarthritis.32 What has puzzled researchers is whether gout precedes osteoarthritis or whether osteoarthritis precedes gout. Authors of a study
joints, thereby inducing inflammation.23 Uric acid is a metabolic byproduct that, in most mammals, is convert-ed to another substance.25 It is not converted in humans and the great apes — species in which the genes respon-sible for the conversion process have mutated and ceased to function.
Currently, scientists are examining the evolutionary role of uric acid to determine what survival advantage might have resulted. One theory is that uric acid assists injured cells in sending a signal to the immune system that a response is required.23 Other researchers charac-terize the evolutionary purpose of uric acid as providing humans with an ability to limit tissue damage.26 Still others connect uric acid levels with hypotension, theo-rizing that upright mammals who formerly subsisted on vegetarian diets low in sodium needed higher uric acid levels for preventing hypotensive crises.23 Whatever ben-eficial purposes uric acid might serve, the human body’s inability to convert uric acid effectively can result in a buildup known as hyperuricemia. Hyperuricemia does not always lead to gout; in the majority of people with hyperuricemia, the condition is asymptomatic.25,27
In 2002, symptomatic cases of gouty arthritis led to approximately 3.9 million outpatient visits in the United States.25 The prevalence of gout in the U.S. population is increasing; between 1990 and 1999, the rate of increase was reported to be 80%, although this might reflect in part the aging of the American public.28 More recently, studies report that the rate of gout has doubled over the past several decades, with the rising obesity level being linked to the increase.23 In men older than 40 years, gout is the most common cause of arthritis (see Box 1).
An acute attack of gout generally begins while the patient is sleeping, when a lower body temperature fos-ters urate crystal deposition.25 The joint becomes hot, red and swollen, and patients report excruciating pain that escalates over a 6- to 12-hour period.27,29 During gout attacks, patients may be unable to tolerate wearing socks or having the bed sheets touch the affected area.25 Patients sometimes exhibit fever and chills, and the skin over the affected joint may become scaly and slough off.25,27 Attacks occur more frequently over time (acute intermittent gout or “gout flares”), and the affected joint is damaged further with each attack, so that a degree of pain or discomfort eventually is omnipresent.28,29
After 10 or more years, other joints can become affect-ed, leading to the development of tophi and chronic tophaceous gout.27 Tophi are chalky deposits of sodium urate that most often develop around joints and in soft tissue; they even can appear in the helix of the ear.9,25
Box 1Who Is Likely To Suffer From Gout?2,23,25,29-31
Current research and epidemiologic studies indicate that symptomatic hyperuricemia is more likely if a person:
• Is male.• Has a family history of the disease (the disease has
a genetic basis in more than half of all cases).• Is obese.• Is older than 30 years for men or 50 years for
women. • Is hypertensive.• Consumes a high-purine diet (beef, pork, lamb and
foods with a significant amount of yeast; high-purine vegetables do not appear to have the same negative impact).
• Consumes alcohol or seafood.• Has psoriasis.
Possible triggers for a gout attack include:• Injury.• Surgical operations.• Excessive exercise.• Infection.• Alcohol consumption (more than a moderate
consumption of 1 to 2 drinks per day, with beer and spirits being more detrimental than wine).
• Consumption of sweetened soft drinks and other high-fructose foods (apples, oranges, juices).
• Intravenous contrast media.• Initiation of chemotherapy.
R0908_PodDR_25-44.indd 30R0908_PodDR_25-44.indd 30 8/28/08 1:45:26 PM8/28/08 1:45:26 PM
CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
Prophylactic measures and typical management of the disease involve uric acid lowering therapy and regular testing for serum uric acid levels to permit proper adjustment of medication levels.28 Despite available drug treatments, many patients continue to experience frequent gout flares. These suboptimal results recently have led researchers to focus on other methods of controlling the disease.33 Newer adjunct approaches to disease management include consuming vitamin C, which has been shown to have a mild urate-lowering effect at a dosage of 500 mg per day; limiting consumption of high-purine foods such as meat (especially organ meat) and seafood (particularly shellfish and anchovies); limiting alcohol intake; and avoiding sodas, fruits and juices high in fructose.27,31 A number of medications, including aspirin, should be avoided because they can cause hyperuricemia.27
Bunions and Hammer, Mallet and Claw ToesHallux valgus, also known as bunions, is another
common hereditary foot malady (see Figure 3).34 A bunion is a bony bump or prominence on the joint at the base of the big toe.35 The metatarsophalangeal joint literally becomes dislocated, with the metatarsal bone gravitating toward the midline of the body while the big toe moves inward, toward the other toes.34 Tissues
published in 2007 concluded that an osteoarthritic joint may predispose the deposit and buildup of uric acid crystals, thus determining which joints are subjected to acute gout attacks.32 Gout is capable of eroding the calcaneus, enlarging and even rupturing the Achilles tendon.2 Gout can bring about bursitis, which is an inflammation of the bursa (a sac or sac-like cavity filled with fluid and designed to limit friction in tissues).9
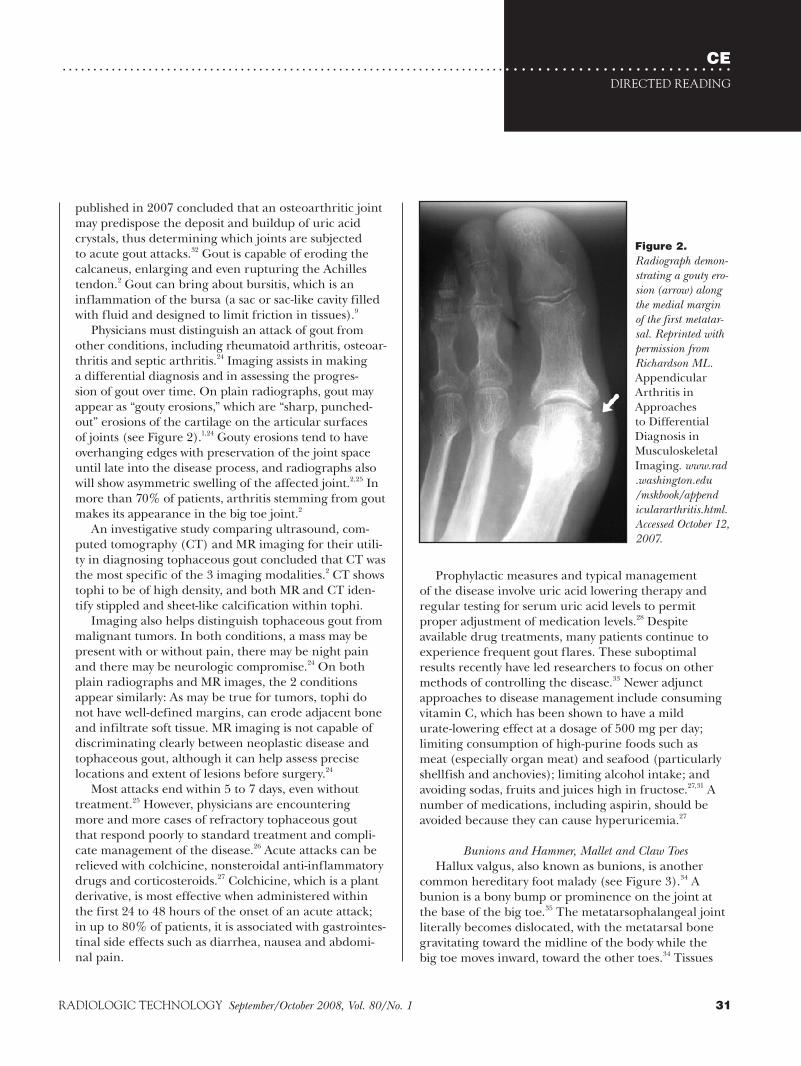
Physicians must distinguish an attack of gout from other conditions, including rheumatoid arthritis, osteoar-thritis and septic arthritis.24 Imaging assists in making a differential diagnosis and in assessing the progres-sion of gout over time. On plain radiographs, gout may appear as “gouty erosions,” which are “sharp, punched-out” erosions of the cartilage on the articular surfaces of joints (see Figure 2).1,24 Gouty erosions tend to have overhanging edges with preservation of the joint space until late into the disease process, and radiographs also will show asymmetric swelling of the affected joint.2,25 In more than 70% of patients, arthritis stemming from gout makes its appearance in the big toe joint.2
An investigative study comparing ultrasound, com-puted tomography (CT) and MR imaging for their utili-ty in diagnosing tophaceous gout concluded that CT was the most specific of the 3 imaging modalities.2 CT shows tophi to be of high density, and both MR and CT iden-tify stippled and sheet-like calcification within tophi.
Imaging also helps distinguish tophaceous gout from malignant tumors. In both conditions, a mass may be present with or without pain, there may be night pain and there may be neurologic compromise.24 On both plain radiographs and MR images, the 2 conditions appear similarly: As may be true for tumors, tophi do not have well-defined margins, can erode adjacent bone and infiltrate soft tissue. MR imaging is not capable of discriminating clearly between neoplastic disease and tophaceous gout, although it can help assess precise locations and extent of lesions before surgery.24
Most attacks end within 5 to 7 days, even without treatment.25 However, physicians are encountering more and more cases of refractory tophaceous gout that respond poorly to standard treatment and compli-cate management of the disease.26 Acute attacks can be relieved with colchicine, nonsteroidal anti-inflammatory drugs and corticosteroids.27 Colchicine, which is a plant derivative, is most effective when administered within the first 24 to 48 hours of the onset of an acute attack; in up to 80% of patients, it is associated with gastrointes-tinal side effects such as diarrhea, nausea and abdomi-nal pain.
Figure 2. Radiograph demon-strating a gouty ero-sion (arrow) along the medial margin of the first metatar-sal. Reprinted with permission from Richardson ML. Appendicular Arthritis in Approaches to Differential Diagnosis in Musculoskeletal Imaging. www.rad.washington.edu/mskbook/appendiculararthritis.html. Accessed October 12, 2007.
R0908_PodDR_25-44.indd 31R0908_PodDR_25-44.indd 31 8/28/08 1:45:26 PM8/28/08 1:45:26 PM

CEIMAGING IN PODIATRY
32 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
hammer toe, and it also can become dislocated in more extreme cases. Other toes may become abducted and clawed, and the raised joints of these toes are subject to friction pressures from overlying shoes. Hammer, claw and mallet toes are caused by an imbalance in the muscles that the control the toes; they almost always occur in toes other than the big toe.37 Other less com-mon causes of hammer, claw and mallet toes include congenital foot deformities, injury, joint diseases such as rheumatoid arthritis and poor blood flow to the feet, as well as brain, spinal cord and nerve injuries (eg, stroke, cerebral palsy).
All of these deformities subject skin and soft tissues to trauma, and patients are more likely to develop corns, bursitis, calluses, ulceration, infection and nail deformi-ties.36 Callus, also known as traumatic hyperkeratosis, is a thickened layer of skin that serves a protective, padding function.38 Corns are painful areas of callus complicated by a deep, central mass of “cornified” cells called a nucleus. The nucleus presses into the underly-ing layer of the skin and can cause significant pain.
surrounding the joint become swollen and tender, and in more severe cases the big toe moves into a position where it either overlaps or underlaps the second toe. The same condition can occur on the opposite side of the foot, at the base of the little toe, and is known as a bunionette or tailor’s bunion.35
Some bunions are asymptomatic, with the exception of the accompanying aesthetic drawbacks of the malfor-mation.34 Symptomatic bunions can be quite painful, and patients sometimes limit activities such as walking and standing. The pain is likely due to ligamentous strain or muscular spasm associated with the foot’s abnormal functioning.36 Associated arthritis and significant pain of the great toe joint are common, and patients often expe-rience limitation of flexion in the joint. At the very least, bunions make shoe fitting problematic.34
As much as 70% of the population is subject to bun-ions, which are most prevalent in mature females.36 The degree of malformation increases with age, and other toes become involved as the deformity becomes more pronounced. The second toe may contract to form a
Figure 3. Radiographs of right foot before and after bunionectomy. A. AP projection before surgery. B. AP projection after surgery. C. Oblique projection before surgery. D. Oblique projection after surgery. Images courtesy of Katherine Ott, Albuquerque, NM.
A CB D
R0908_PodDR_25-44.indd 32R0908_PodDR_25-44.indd 32 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
Hammer, claw and mallet toes first are treated by changing footwear, using padding or taping the toes to force them into a normal position, ingestion of pain relievers, injecting corticosteroids and performing foot exercises that stretch the toes and keep them more flex-ible.37 When surgery is required, several options exist: part or all of the toe bone may be removed, the joints
Corns indicate the occurrence of concentrated, intermit-tent pressure and result from deformity or dysfunction of the foot and toes.38 Over time, the foot’s instability and abnormal biomechanics lead to osteoarthritis and degeneration in the joints.36 In their more severe forms, these foot deformities also can cause problems in bal-ance and affect a person’s ability to walk.37
Although heredity generally is accepted as the pri-mary cause of bunions, for years experts have debated what role, if any, footwear plays in bunion formation (see Box 2). The deformity runs the gamut from mild to severe, and the degree of pain and limitation is similarly variable.36 When bunions are symptomatic and interfere with daily functioning, corrective surgery may be advis-able. Radiographs reveal the biomechanics underlying the deformity, help rule out other causes of pain and swelling such as gout, rheumatoid arthritis or joint infec-tion and assist in determining the need for and type of surgery.34
Bunions are classified as normal, mild, moderate and severe according to the degree of bone deformity.35 Weight-bearing radiographs permit a podiatrist to mea-sure and classify degree of malformation via the bunion and intermetatarsal angles. Radiographs also are used to determine placement of 2 tiny sesamoid bones, which lie beneath the big toe joint in a normal foot. The sesa-moid bones are classified as to degree of dislocation. A podiatrist also assesses the range of motion remaining in the joint, and, with the patient, will determine which of the many corrective surgical procedures would be most appropriate.
A bunionectomy does not repair the damage done within the toe joint; thus, pain caused by that degen-eration can continue after surgery.34 In general terms, a bunionectomy involves removing the bump of bone from the medial side of the metatarsal head. The first metatarsal then is cut so that the bone can be shifted and realigned with the joint. A pin or screw holds the bone in the correct position while it is healing, and any sharp points are removed to avoid irritation and permit smooth joint functioning (see Figure 3). Postsurgical radiographs taken at regular intervals permit observa-tion of the healing process and ensure successful surgi-cal results. Surgical realignment of the joint may achieve improved motion and limitation of further damage, but the foot may not be pain free even after surgery. Patients often are prescribed orthotics in an effort to correct the abnormal gait and foot motion likely to have been responsible for the deformity and to prevent the malfor-mation from recurring.
Box 2Are Women’s Feet Fashion Victims?34-37,39
Abnormal pronation generally is accepted as the prima-ry cause of bunions. In a normal gait pattern, a person’s foot rolls moderately inward; a more extreme degree of pronation puts pressure on the big toe joint, causing damage and injury.
Ninety percent of those who seek surgery for functional or cosmetic reasons are women, although this gender discrepancy is not seen in children or adolescents.
People are more likely to develop bunions if they:• Have abnormally pronated feet.• Inherit a foot shape that puts pressure on the big toe
joint. Narrow feet are more likely to develop bunions.• Have a leg length discrepancy. Bunions more
typically form on the longer limb.• Have flat feet.• Are obese or otherwise overload the foot.• Experience some trauma to the soft tissue struc-
tures around the great toe.• Have rheumatoid arthritis.
Studies have been conducted in shod and unshod populations. The prevalence of bunions is higher in shod populations, lending some credence to the theory that shoes contribute to the formation of bunions.
Although they do not create bunions, tight or constricting shoes — in particular women’s narrow-toed high heels — can exacerbate the problem. Excessive heel height alters normal gait by transferring weight from the sturdy heel to the more vulnerable toes; it forces the medial edge of the foot rather than the outer edge to carry the majority of the body’s weight, thus inducing or increas-ing pronation. In high-heeled shoes, the toes are sub-jected to additional compressive forces because the foot tends to slide forward, pressing the toes up against the narrow toe of the shoe. Hammer, claw and mallet toes are more common in women who wear tight shoes.
Certainly, bunion pain can be at least somewhat relieved by wearing shoes with a wide, deep toe box and avoid-ing high-heeled shoes.
R0908_PodDR_25-44.indd 33R0908_PodDR_25-44.indd 33 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEIMAGING IN PODIATRY
34 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
include limitation of motion, pain and tenderness in the affected area.1 Although patients can present with all the symptoms of a stress fracture, these types of fractures do not become visible on plain radiographs until a few weeks after injury. Because stress fractures can mimic more dire abnormalities, other imaging modalities may be required to confirm a diagnosis.42
Statistics indicate that more and more ankle fractures are treated each year throughout the world, that in patients older than 50 years ankle fractures are result-ing from relatively minor trauma, and that more serious fracture combinations are increasingly seen in EDs.44 Ankle fractures often are diagnosed in postmenopausal women, although these fractures are not necessarily a result of osteoporosis. Interestingly, radiographs for ankle injuries are not cost effective because fewer than 15% of patients with ankle pain have fractures. When radiographs are appropriate, 3 projections are ordered (AP, mortise [15º to 20º internal oblique] and lateral), although some experts argue that in 95% of cases only 2 images (lateral and mortise) are needed to diagnose ankle fractures.41
In the mortise projection, the foot is rotated approxi-mately 15º internally to permit better visualization of the joint. Stress views help assess the joint’s stability and evaluate possible injury to ankle ligaments but usually are not ordered during an initial ED evaluation.41,44 A more experienced physician may inject the suspect joint or painful area with a local anesthetic and then apply stress to the ankle. In some settings, mechanical stress-ing devices are used to promote consistency with respect to the degree of stress applied.41
CT and MR imaging studies can help assess the com-plexity of the fracture, including injuries to ligaments and articulation points, although they are employed more often for outpatient management.44 Ultrasound, given its relatively lower cost, has gained acceptance in evaluating the motion of tendons.41 When stress frac-tures, infections and neoplastic lesions are suspected in the ankle, a bone scan may be appropriate.44
When axial and coronal CT images of the ankle and foot are ordered, scout views are recommended, and most examinations use a 3- to 5-mm slice thickness.41 For axial images, the patient’s feet are positioned per-pendicular to the gantry table, with knees extended straight and great toes together. Sometimes a foot board is used to reduce motion. In coronal images, the patient’s knees are bent with the feet flat against the gantry table. To facilitate viewing of certain bones and joints, a foot wedge can be used and the gantry can be
may be fused, and tendons may be cut or removed to allow the toe to straighten. As is true for bunions, radiographs guide surgical decisions and postsurgical follow-up.37
Traumatic and Sports-related Foot InjuriesTraumatic Fractures
Ten percent of all bone fractures occur in the foot.8 Fractures can occur in any of the bones of the foot and at any of the foot joints.40 Traumatic injuries may be due to direct or indirect trauma or may result from overuse.8 The possible causes of traumatic foot injury are innumerable, including work-related injuries, motor vehicle accidents and falls. Toe fractures in particular are exceedingly common and tend to heal within 3 to 8 weeks with little or no therapy.
Possible fractures of foot bones and joints other than the toes are likely to require thorough examination and treatment. Emergency department (ED) physicians com-monly order radiographs; ankle radiographs alone cost the American health system an estimated $500 000 per year.41 The ED physician takes a patient history, includ-ing identification of the mechanism of injury.8 Physical examination includes an inspection for bruising, swell-ing, deformity or open wounds, as well as a comparison with the uninjured foot. Foot pulses, capillary refill, range of motion and neurologic function also are assessed.
Radiographs are by far the imaging study of choice to evaluate possible foot fractures, and most fractures are well documented on plain films (see Table 1).8,42 Routine radiographs of the foot include AP, lateral and oblique projections.41 Because some fractures are occult on radiographs, other imaging modalities such as bone scans, CT, MR and ultrasound often are ordered. Some experts postulate that CT in particular soon may be used routinely to assess acute foot fractures, given CT’s ability to delineate complex fractures and joint align-ment.45 The complex anatomy of the articulations of the rear foot may call for multidirectional projections or CT-positioned films.41 Second-line imaging studies gener-ally will be performed only after the ED physician has consulted with an orthopedic surgeon.8
Fractures caused by repetitive stress most commonly occur in the second and third metatarsals, along with the navicular and calcaneus bones.1,43 Several stress fractures may be present in the same foot. Over time, a small crack develops in the outer shell of the bone. In the absence of treatment, this crack can progress until it becomes a through-and-through break. Symptoms
R0908_PodDR_25-44.indd 34R0908_PodDR_25-44.indd 34 8/28/08 1:45:27 PM8/28/08 1:45:27 PM
CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
35RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
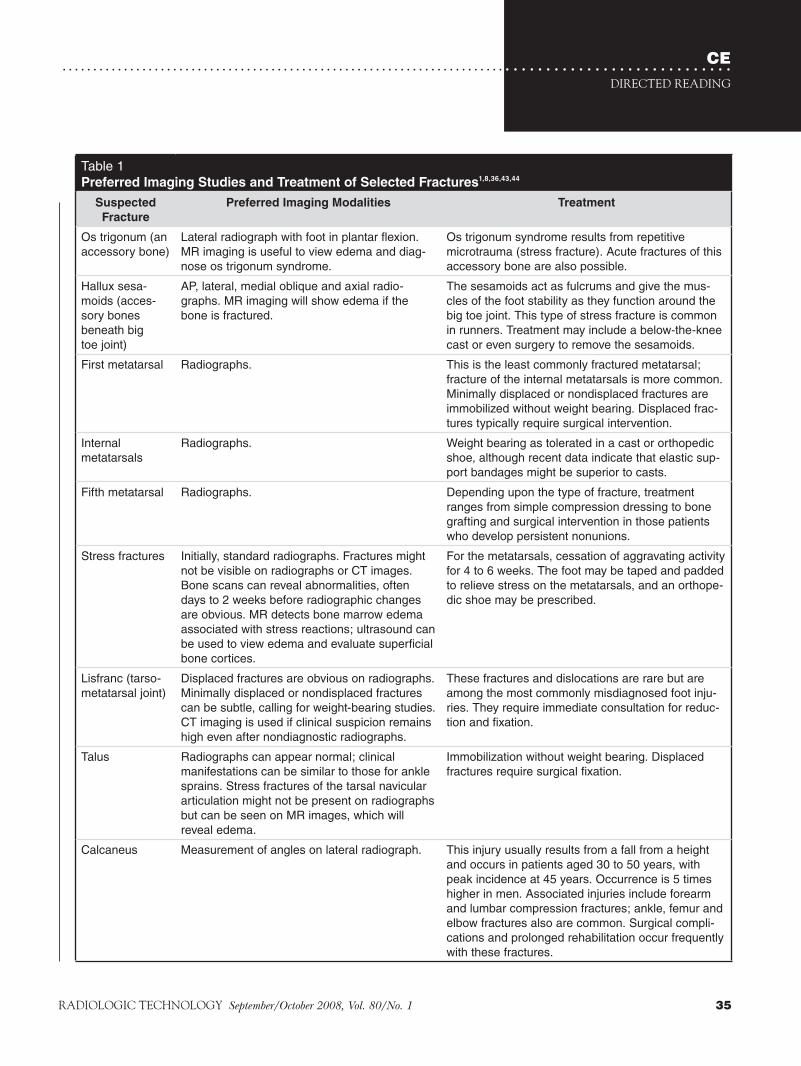
Table 1Preferred Imaging Studies and Treatment of Selected Fractures1,8,36,43,44
Suspected Fracture
Preferred Imaging Modalities Treatment
Os trigonum (an accessory bone)
Lateral radiograph with foot in plantar flexion. MR imaging is useful to view edema and diag-nose os trigonum syndrome.
Os trigonum syndrome results from repetitive microtrauma (stress fracture). Acute fractures of this accessory bone are also possible.
Hallux sesa-moids (acces-sory bones beneath big toe joint)
AP, lateral, medial oblique and axial radio-graphs. MR imaging will show edema if the bone is fractured.
The sesamoids act as fulcrums and give the mus-cles of the foot stability as they function around the big toe joint. This type of stress fracture is common in runners. Treatment may include a below-the-knee cast or even surgery to remove the sesamoids.
First metatarsal Radiographs. This is the least commonly fractured metatarsal; fracture of the internal metatarsals is more common. Minimally displaced or nondisplaced fractures are immobilized without weight bearing. Displaced frac-tures typically require surgical intervention.
Internal metatarsals
Radiographs. Weight bearing as tolerated in a cast or orthopedic shoe, although recent data indicate that elastic sup-port bandages might be superior to casts.
Fifth metatarsal Radiographs. Depending upon the type of fracture, treatment ranges from simple compression dressing to bone grafting and surgical intervention in those patients who develop persistent nonunions.
Stress fractures Initially, standard radiographs. Fractures might not be visible on radiographs or CT images. Bone scans can reveal abnormalities, often days to 2 weeks before radiographic changes are obvious. MR detects bone marrow edema associated with stress reactions; ultrasound can be used to view edema and evaluate superficial bone cortices.
For the metatarsals, cessation of aggravating activity for 4 to 6 weeks. The foot may be taped and padded to relieve stress on the metatarsals, and an orthope-dic shoe may be prescribed.
Lisfranc (tarso-metatarsal joint)
Displaced fractures are obvious on radiographs. Minimally displaced or nondisplaced fractures can be subtle, calling for weight-bearing studies. CT imaging is used if clinical suspicion remains high even after nondiagnostic radiographs.
These fractures and dislocations are rare but are among the most commonly misdiagnosed foot inju-ries. They require immediate consultation for reduc-tion and fixation.
Talus Radiographs can appear normal; clinical manifestations can be similar to those for ankle sprains. Stress fractures of the tarsal navicular articulation might not be present on radiographs but can be seen on MR images, which will reveal edema.
Immobilization without weight bearing. Displaced fractures require surgical fixation.
Calcaneus Measurement of angles on lateral radiograph. This injury usually results from a fall from a height and occurs in patients aged 30 to 50 years, with peak incidence at 45 years. Occurrence is 5 times higher in men. Associated injuries include forearm and lumbar compression fractures; ankle, femur and elbow fractures also are common. Surgical compli-cations and prolonged rehabilitation occur frequently with these fractures.
R0908_PodDR_25-44.indd 35R0908_PodDR_25-44.indd 35 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEIMAGING IN PODIATRY
36 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Symptoms associated with metatarsal stress fractures dif-fer from most other forefoot injuries in that they come on quickly, are more intense and are associated with significant swelling.47
Pain in the ball of the foot is a common, disabling foot problem for almost any athlete, as a large propor-tion of stress is placed on this area of the foot. Stress overload in this area of the foot can be compounded if the athlete also suffers from a bunion malformation and wears inadequate footwear. Fractures of the sesam-oid are common in ballet dancers, aerobic enthusiasts, hurdlers and runners — all of whom are required to remain on the balls of their feet for longer periods of time.47 In contrast to metatarsal stress fractures, sesam-oid fractures manifest with an aching pain during and after exercise; the pain, which is due to irritation of the sesamoidal joint cartilage, is akin to that associated with gout and osteoarthritis of the big toe joint.
Optimal treatment of foot injuries in athletes requires that the treating physician have a good sense of the athlete’s training regimen and attributes such as shoe gear, running surfaces, diet and sleep.47 To stop some athletes from continuing to put stress on their feet, it might be necessary to place the foot in a plaster cast and to force the use of crutches to give the fractures an opportunity to heal. Any return to activity should be delayed until radiographs indicate fractures have healed completely.
SprainsThe most common injury associated with sports is
a sprained ankle, which is a more serious injury than generally is believed.40 Up to 73% of athletes who suf-fer an ankle sprain will experience recurrent sprains of the weakened structure, and chronic problems such as pain, instability, stiffness and recurrent swell-ing are experienced by nearly 50% of patients who have sprained an ankle.48 Nearly 3000 inversion ankle injuries occur each day in the United States; they are particularly common to those who participate in bas-ketball, soccer, volleyball or other sports that are played on uneven surfaces where the ankle can lose stability.48 Female athletes are 25% more likely than their male counterparts to suffer from ankle injuries. Lateral ankle sprains account for 45% of all basketball-related injuries. A lateral ankle sprain occurs when the foot turns inward; sometimes a pop is heard or felt. Bruising and swelling begin immediately, and the injury is usual-ly to the lateral ankle ligaments. Radiographs are taken immediately to rule out fracture.
angled. Optimal positioning is of particular importance for imaging the hindfoot. CT can be useful in assessing the extent of foot and ankle lesions and trauma-induced injuries, although it is not particularly valuable for assessing soft tissue injuries.
MR imaging is considered to be exceptional for view-ing the complex, soft tissue components of the foot and ankle, and physicians realize that essential diagnostic information and treatment planning could be available only by means of MR.42 One of the major advantages of MR is that it is capable of imaging multiple planes.41 Patients are imaged most effectively using the most closely coupled coil as is practical, along with a field of view that optimizes image quality.41 Patients should be positioned and coils selected with the suspected disorder in mind; for example, when a tendon tear is suspected, enough area must be included to permit viewing of both ends of the tendon. When the midfoot and forefoot are to be evaluated, patients may be examined in the prone position, which helps to eliminate motion. The prone position also is preferred for evaluating posterior soft tis-sues, as this position lessens soft tissue compression and thus anatomic distortion.41 The supine position, with the foot in a neutral position to avoid tendon distortion, is preferred for ankle and hindfoot studies. Motion studies are most often performed using coupled flat coils, which allow for improved signal and foot movement. For both foot and ankle studies, coronal, axial and sagittal image planes are used most commonly.41
In contrast to adults, children’s forefeet are both flexible and resilient to injury. Fractures are neverthe-less more common than sprains in children because the ligaments of their feet are relatively stronger than are their bones and cartilage.8 Radiologists must take particular care in interpreting children’s imaging stud-ies because of the several growth centers found in the foot. For these reasons, comparison images of the child’s uninjured foot often are ordered.
Stress-related FracturesSixteen percent of all sports injuries involve the
foot.46 Not surprisingly, sports that involve continual pounding and vibration to the feet can, over time, result in stress-related injuries.47 Three categories of stress fractures are recognized: stress reactions, fatigue fractures and insufficiency fractures.1 Fatigue fractures result from a prolonged, cyclical application of abnor-mal mechanical stress to the foot such as running and marching. Dancing has been characterized by some as exerting a mild, continued trauma to the feet.5
R0908_PodDR_25-44.indd 36R0908_PodDR_25-44.indd 36 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
37RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
mities. Weight should be placed as equally as possible on both feet so that any preference for the uninjured side does not skew results. Comparison views with the unin-jured foot also are recommended. The radiologist exam-ines the way the bones line up to determine whether a Lisfranc injury is present.8 Observation of fractures at the base of any of the metatarsals calls for added vigi-lance and greater suspicion of a Lisfranc injury.46
More advanced imaging modalities such as MR per-mit diagnosis of mild Lisfranc injury because edema and partial disruption can be seen.46 CT also may be appropriate, although some experts advise that it should be used for preoperative planning instead of diagno-sis.8,46 For those patients who do not seek medical atten-tion until several weeks after the injury first occurred, bone scans may be used to show increased uptake at the Lisfranc joint.46 Less severe Lisfranc injuries are treated with orthotics or a nonweight-bearing cast, and progress is measured through follow-up radiographs. For Lisfranc injuries that display greater displacement, surgery may be required.46
Tendon InjuriesOne of the most common reasons for performing MR
imaging studies of the foot and ankle is to examine the tendons, which are susceptible to injury during sports or through trauma.42 Injuries to tendons can be direct or result from overuse. For example, ballet dancers often exhibit inflammation of the sheath of the flexor hallucis longus tendon, which is the tendon responsible for these dancers’ ability to maneuver upon pointed toes. The consequent injury is due to the extreme flexion posi-tions they maintain over long periods of time.42
Physicians focus on distinguishing a torn tendon from a tendon that has been disrupted completely, as surgical intervention is required for a total disruption. Some tendons actually split lengthwise, causing a chron-ic condition that requires surgical repair.40 Except for the Achilles tendon, in which a partial tear is common and presents a clear clinical picture, the clinical picture for other tendon injuries does not adequately permit a distinction to be made between a torn tendon and one that has been disrupted completely. Imaging studies pro-vide key diagnostic information (see Table 2).
Statistics indicate that there is an increase in Achilles tendon disorders after 35 years of age.47 This tendon, which is associated with the 2 muscles responsible for leg deceleration in all activities, has poor circulation and thus requires additional stretching and warm-up. Scientists theorize that because the already poor
Lisfranc InjuryA less common injury, but one that can end an ath-
letic career, is injury to the Lisfranc joint, the point at which the tarsal and metatarsal bones articulate.9 Jacques Lisfranc described this injury in cavalry soldiers who fell from their horses with their feet still trapped in stirrups and who were then dragged alongside their horses.46 It is an injury often underestimated by both the athlete and medical care providers, as it can be difficult both to identify the injury and to provide proper treat-ment.46 Athletes have a tendency to try to “walk off” this injury, which can further delay diagnosis and treatment.
A Lisfranc injury involves disruption of the liga-ments at the tarsal-metatarsal joints, most commonly at the base of the first and second metatarsals. The injury often is seen in high-speed motor vehicle acci-dents in which the foot was placed on the brake pedal or floor of the car at the time of impact in an effort to block forward momentum. The foot then is forced into hyperplantarflexion, resulting in a dislocation of the Lisfranc joint. The injury can lead to gross instability of the foot and neurovascular damage.46 A Lisfranc injury associated with a vehicle accident is characterized as a high-velocity injury; when it occurs in the context of a sports activity, it is considered a low-velocity injury. The low-velocity injury presents differently, with less obvious symptoms, and thus is more difficult to diagnose.
As with cavalry soldiers, today’s sports-related Lisfranc injuries are seen in athletes who use foot straps (eg, surfers, windsurfers and horseback riders).46 The mechanism of injury is the same as that described by Lisfranc. Other athletes, such as football players, are also prone to the problem by means of a different injury mechanism. The lineman’s stance during a block com-bined with a force directed down onto the heel (a tackle from behind, for example) can force the foot into hyper-plantarflexion. Baseball players are injured similarly when they slide into a base, and parachutists who land with a plantarflexed foot can suffer a Lisfranc injury. If both feet were under the same physical forces at the time of injury, both feet could sustain a Lisfranc injury.
Because symptoms of a low-velocity Lisfranc injury can be subtle (and other more obvious ankle and foot injuries could distract the physician from diagnosing the Lisfranc injury), experts urge providers to examine the Lisfranc joint in all athletes who complain about a sprained ankle or foot.46 Plain-film radiographs generally are ordered with a minimum of 3 projections (AP, 30º oblique and lateral). If the patient is capable of tolerating them, weight-bearing projections will accentuate defor-
R0908_PodDR_25-44.indd 37R0908_PodDR_25-44.indd 37 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEIMAGING IN PODIATRY
38 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Plantar fasciitis is most common in athletes and middle-aged and overweight adults and is caused by overloading and overuse.50 In athletes, the condition is attributed to inflammation and microtearing of the fascia.1 High-arched feet and overpronation also can contribute to the problem, which includes the following symptoms:
■ A deep, tender spot of pain on the bottom or inside margin of the heel.
■ Pain that is worse on arising in the morning and after sitting.
■ Pain that is aggravated by prolonged weight bear-ing (standing, walking).
■ Pain that is capable of limiting activity severely.36,49 People who have occupations that require long peri-
ods of standing often report this type of pain.50 The incidence of the condition increases during the fifth and sixth decades of life.36 Plantar fasciitis is treated by cushioning the heel to redistribute pressure, applying heat and injecting an anti-inflammatory, such as a corti-costeroid.
Imaging is not required for diagnosis of this condi-tion, although radiologic findings include fascial tear, marrow edema and the plantar calcaneal spur already mentioned.1 The American College of Radiology Appropriateness Criteria Scale for chronic foot pain imaging rates plain radiography (AP and lateral projec-tions to rule out other conditions) and MR imaging as the most appropriate imaging studies for diagnosis of this condition. MR imaging findings associated with this condition include thickening of the fascia, inflam-mation, adjacent soft-tissue edema, fluid collection adja-cent to the insertion site of the fascia in the calcaneus, and rupture at mid or proximal segments of the fascia. Ultrasound can be used in place of MR imaging; use of bone scans and CT is discouraged.1
circulation decreases by about 40% after 35 years of age, the tendon is injured more easily. Numerous sports activities place an additional burden upon the Achilles tendon; running uphill and downhill, for example, alters the torque on the tendon. Hamstring tightness can stress the tendon further. When the tendon has not received sufficient warm-up, it can be ruptured by a forward lunge. In contact sports such as basketball, rugby and football, a direct blow can cause tendonitis. The on-again off-again running and stopping associated with racquetball, handball and basketball also can lead to Achilles tendon problems, as can the side-to-side lunging common in tennis.
Complete disruption of the Achilles tendon is seen commonly not only in athletes but also in men older than 40 years. Presently, there is controversy in the medical community over how the injury should be treated: Should it be casted or should surgery be per-formed to reunite the tendon? Many surgeons base their decision upon the size of the gap between the 2 ends of the tendon, using MR imaging to visualize the degree of injury.
Plantar FasciitisThis condition, in which the broad band of fibrous
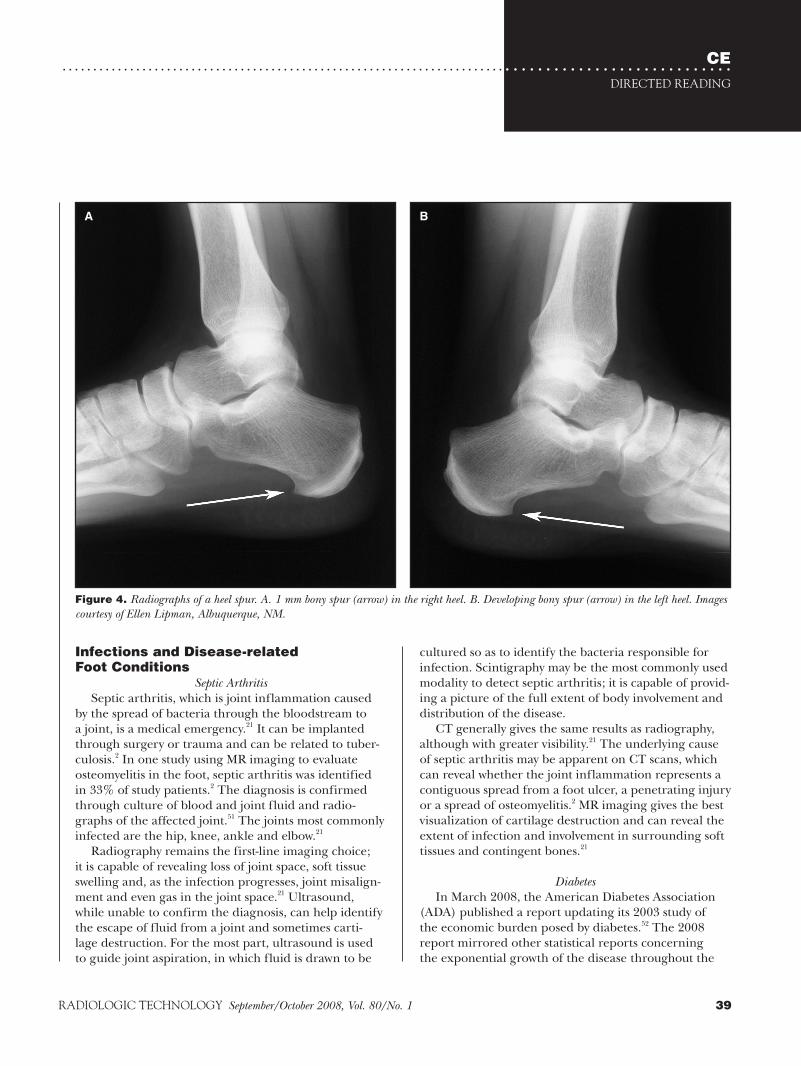
tissue that runs along the bottom of the foot (the plan-tar fascia) becomes inflamed, is the most common cause of deep foot pain on the bottom surface of the heel.49 The plantar fascia helps form the arch of the foot, and it stretches from the calcaneus to the 5 metatarsal heads.5 When the condition is of long duration, it leads to deposits of calcium at the spot where the fascia insert into the calcaneus. On a radiograph, the calcium depos-it appears as a bony heel spur. Such spurs, which are seen in about 10% of the population, are not the source of pain (see Figure 4).36
Table 2MR Imaging of Tendons of the Foot and Ankle1,9,42,47
Injury Appearance on MR Imaging
Tenosynovitis (inflammation of the tendon sheath) Seen as fluid in the tendon sheath; the underlying tendon appears normal.
Tendonitis (inflammation of the tendon and tendon-muscle attachments) or partial tendon tear
Seen as focal or spindle-shaped swelling on the tendon. A more severe form of tendonitis is one in which the tendon is thin and attenuated. It can be viewed on MR.
Tendon rupture For most tendons, it is best viewed on axial MR images; there is an absence of tendon on 1 or more images. The Achilles tendon is an exception to this and is best seen on sagittal images.
R0908_PodDR_25-44.indd 38R0908_PodDR_25-44.indd 38 8/28/08 1:45:27 PM8/28/08 1:45:27 PM
CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
39RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
cultured so as to identify the bacteria responsible for infection. Scintigraphy may be the most commonly used modality to detect septic arthritis; it is capable of provid-ing a picture of the full extent of body involvement and distribution of the disease.
CT generally gives the same results as radiography, although with greater visibility.21 The underlying cause of septic arthritis may be apparent on CT scans, which can reveal whether the joint inflammation represents a contiguous spread from a foot ulcer, a penetrating injury or a spread of osteomyelitis.2 MR imaging gives the best visualization of cartilage destruction and can reveal the extent of infection and involvement in surrounding soft tissues and contingent bones.21
DiabetesIn March 2008, the American Diabetes Association
(ADA) published a report updating its 2003 study of the economic burden posed by diabetes.52 The 2008 report mirrored other statistical reports concerning the exponential growth of the disease throughout the
Infections and Disease-related Foot Conditions
Septic ArthritisSeptic arthritis, which is joint inflammation caused
by the spread of bacteria through the bloodstream to a joint, is a medical emergency.21 It can be implanted through surgery or trauma and can be related to tuber-culosis.2 In one study using MR imaging to evaluate osteomyelitis in the foot, septic arthritis was identified in 33% of study patients.2 The diagnosis is confirmed through culture of blood and joint fluid and radio-graphs of the affected joint.51 The joints most commonly infected are the hip, knee, ankle and elbow.21
Radiography remains the first-line imaging choice; it is capable of revealing loss of joint space, soft tissue swelling and, as the infection progresses, joint misalign-ment and even gas in the joint space.21 Ultrasound, while unable to confirm the diagnosis, can help identify the escape of fluid from a joint and sometimes carti-lage destruction. For the most part, ultrasound is used to guide joint aspiration, in which fluid is drawn to be
Figure 4. Radiographs of a heel spur. A. 1 mm bony spur (arrow) in the right heel. B. Developing bony spur (arrow) in the left heel. Images courtesy of Ellen Lipman, Albuquerque, NM.
A B
R0908_PodDR_25-44.indd 39R0908_PodDR_25-44.indd 39 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEIMAGING IN PODIATRY
40 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
problems can hinder the patient’s ability to observe signs of infection and skin breakdown on the feet.)
■ Cardiovascular disease, including hypertension and heart failure.
■ Foot and leg amputation because of severe infec-tion.52,54,60,61
Between the 2003 and 2008 ADA reports, more than 5 million Americans were diagnosed with the disease, reflecting an aging population and rising prevalence of overweight patients.52 In 2001, nearly 75% of all newly diagnosed cases occurred in children.62
The nerve and vascular diseases brought on by diabe-tes contribute to the high rate of amputation in diabetic patients.63 Foot ulcers can lead to abscess, gangrene and osteomyelitis, all of which increase the likelihood of amputation.2 Osteomyelitis occurs in 20% of diabetic
world and reported the current number of Americans diagnosed with diabetes at 17.5 million.52,53 The ADA emphasized that the financial impact of diabetes affects all aspects of society through higher insurance premi-ums, reduced earnings and lost productivity, in addition to reduced quality of life for those who have the disease and for those who care for them. The national burden was estimated to exceed $174 billion dollars — a figure that does not encompass pain and suffering, the cost to nonpaid caregivers and excess medical costs attrib-uted to undiagnosed diabetes. The report, which may be accessed online, gives figures for individual states. For example, in New Mexico diabetes occurs in 6.1% of the population, with the total cost being an astounding $1.25 billion each year. In California, the incidence is lower (5.6%); however, the total cost of the disease is practically incomprehensible at $24.42 billion annually.
Diabetes affects the nervous, vascular and immune systems.54 High blood sugar injures nerves, resulting in pain, burning and eventually numbness. The damage begins in those areas of the body farthest from the brain and spinal cord — the feet. Nerves that conduct messag-es of pain and temperature are affected first. Peripheral neuropathy, the damage to nerves in the peripheral areas of the body such as the feet, limits a person’s abil-ity to feel pain from injuries; thus, minor injuries such as blisters or small cuts can lead to ulcers and limb-threatening infections. The situation is further compli-cated by another effect of diabetes — reduced blood flow to the feet, or peripheral arterial disease. The lack of adequate blood flow limits the body’s ability to heal wounds and can impede antibiotics from reaching the infection. Ischemic ulcers, those foot ulcers caused not by injury but by limited blood flow, occur in about 10% of patients with diabetes.55
Patients with diabetes are exposed to the following complications:
■ Foot ulceration (the loss of skin and underlying tissue over areas of pressure).
■ Peripheral neuropathy (damage to the nerves that results in a loss of sensation).
■ Charcot joint disease (peripheral neuropathy and destruction of this foot joint) (see Box 3).
■ Osteolysis (resorption of bone, especially in the forefoot).
■ Osteomyelitis (infection of bone, usually stemming from an overlying foot ulcer).
■ Cerebrovascular disease, including stroke.■ Renal complications.■ Eye disorders, including blindness. (These eye
Box 3Imaging Diabetic Neuropathy and Joint Destruction (Charcot Foot)1,55-59
Diminished pain sensation resulting from diabetic neu-ropathy can leave a joint without protection from repeat-ed microtrauma. The patient does not perceive any pain and thus continues an activity that causes destruction.
Fracture and dislocation of the Lisfranc joint is a com-mon result of diabetic neuropathy; other joints (includ-ing those of the forefoot, hindfoot and ankle joint) also are prone to injury. Charcot first described neuropathic joint destruction (“Charcot Joint” or “Charcot Foot”) in 1868. The clinical image of this painless but severe joint destruction will include swelling, fluid collection and deformity.
Neuropathic changes to the foot’s anatomy are best detected by radiography, although early changes are diagnosed more easily using MR imaging or bone scans. It can be difficult to distinguish this condition from osteomyelitis on MR images, and so some experts are investigating the usefulness of fluorodeoxyglucose (FDG)-PET imaging, which appears to have a distinc-tive uptake pattern when Charcot foot is compared with osteomyelitis.
Recent studies suggest that both ultrasound and MR imaging are capable of demonstrating atrophy of the small foot muscles, which could signal early changes occasioned by neuropathy. Atrophy of these muscles leads to altered biomechanics that, in turn, can lead to the prominence of certain bones and the thinning of fat pads — all changes that can increase the risk of foot ulcers.
R0908_PodDR_25-44.indd 40R0908_PodDR_25-44.indd 40 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
41RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
In another study limited to 20 patients, MR was shown to be superior to F-fluorodeoxyglucose positron emission tomography (PET) and 99mTc-labelled mono-clonal antigranulocyte antibody scintigraphy.64 The authors reported that other studies had shown PET is a highly sensitive method for detecting areas of infec-tion, and that more recent studies of the use of PET to discern musculoskeletal infections were promising. Last, study authors noted that there was a high prevalence of osteomyelitis in study patients who had foot ulcers but no clinical signs of infection — a particularly concern-ing finding, given the need for quick action to prevent loss of limb.
Still other experts caution that the reviews are mixed for the use of MR in diagnosing osteomyelitis in the foot of patients with diabetes.42 They report that MR is highly accurate in predicting the absence of osteomyelitis, but that it can be so specific that it leads to suspicion of infection where there may be none. Thus, these experts characterize MR for the purposes of diagnosing osteo-myelitis in the foot and ankle as “very sensitive but not very specific.”42 Scintigraphy can be an excellent nega-tive predictor, as a normal bone scan essentially excludes the presence of infection.21
Scientists are looking into the use of scanning laser-Doppler imaging techniques to identify patients at risk for tissue ischemia and poor healing because of impaired circulatory function in the legs and feet.65 This scanning method, in which a laser light is projected onto the skin by a computer-controlled mirror, is likely to assist physicians in determining the prognosis for post-surgical wound healing and may prove particularly help-ful for surgeons who are considering the feasibility of amputation. The scan is painless, rapid and noninvasive.
Imaging also is used to help prevent ulceration, infec-tion and amputation in patients with diabetes. Recently, more emphasis has been placed on the beneficial impacts of diet and physical activity.53 Studies have dem-onstrated that exercise improves blood flow to the lower limbs of patients with diabetes, thus lessening the nega-tive effects of arterial insufficiency.66 In one study, color duplex imaging was used to discern the status of arterial disease both before and after a brief period of lower limb exercise. In all patient groups blood flow increased, resulting in improved delivery of oxygen to tissue and removal of the waste product carbon dioxide from tis-sue. Perhaps the most optimistic result of the study was a finding that even several minutes after exercise ceased, diabetic patients’ blood flow remained significantly higher than pre-exercise levels.66
patients with foot wounds, and the overall risk of ampu-tation for diabetic patients is estimated to be 15% to 25%.64 Nearly 60% of patients who undergo amputation have their other limb amputated within 3 to 5 years of the first amputation.55 Within 3 years of a first amputa-tion, 20% to 50% of patients die. Imaging is playing a growing role in the fight to change these dire statistics.
Diabetic wounds and ulcers on the feet can lead to life-threatening infections quickly, and the course of deterioration can be rapid.55 With osteomyelitis, bone marrow changes occur next to an overlying ulcer; it is more common near pressure points such as the heel, metatarsal heads and tips of toes.21 Diagnosis of osteo-myelitis in diabetic feet is difficult due to several factors, including diabetic patients’ altered sensation — they can neither report certain symptoms nor respond to stimuli that assist clinical diagnosis in patients without diabetes. Imaging permits clinicians to determine the existence of infection, grade the severity of infection and recom-mend treatment options.2
Standard radiographs can assist in diagnosing bone infection, but MR imaging is considered to be more sen-sitive and more specific for confirmation of osteomyeli-tis.55 Although radiographs are not sufficiently sensitive to show early osteomyelitis, standard radiographs are taken for new patients and used as a baseline and to rule out bony abnormalities, gas and foreign bodies. Because bone infection can be present for extended periods of time, some clinicians use baseline radiographs followed by serial radiographs to ascertain the progression of bone changes.55
Some experts report that MR imaging is the imag-ing modality of choice for radiologic assessment of the feet in patients with diabetes, particularly for studying infection.2 MR has been shown to be superior to CT for its sensitivity for osteomyelitis, although the 2 modalities appear to be equal with respect to both accuracy and specificity. When MR imaging is either unavailable or cannot be performed, CT is a viable option, and it has a demonstrated ability to reveal soft tissue gas associated with cell death and the status of bone involvement. It is expected that high-resolution, thin-section multidetec-tor CT will improve the ability of CT to detect bone erosion.2 Even when CT is negative for infection, MR or nuclear medicine imaging should be performed if the clinician remains suspicious of osteomyelitis. CT proves useful in planning for surgery when there is a history of chronic osteomyelitis. MR also can be a useful surgical tool, as it helps to limit the extent of surgical resections, leaving a patient with a better ability to ambulate.21
R0908_PodDR_25-44.indd 41R0908_PodDR_25-44.indd 41 8/28/08 1:45:27 PM8/28/08 1:45:27 PM

CEIMAGING IN PODIATRY
42 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
alert clinician will rule out metastatic disease by means of radiographs and MR imaging.
ConclusionImaging’s role in the diagnosis and management of
foot disorders will no doubt broaden over the coming years. New imaging modalities, along with refinement of existing modalities, should help health care providers in their efforts to remedy congenital foot disorders, prevent malformation and disease, and ameliorate chronic foot pain. Education, too, should come to play a more promi-nent role in podiatry, given how many foot disorders are caused or aggravated by obesity, overuse and the dic-tates of fashion.
References1. Ahn JM, El-Khoury GY. Radiologic evaluation of chronic
foot pain. Am Fam Physician. 2007;76(7):975-982. 2. Johnson PT, Fayad LM, Fishman EK. CT of the foot:
selected inflammatory arthridites. J Comput Assist Tomogr. 2007;31(6):961-969.
3. Berquist TH, Knudsen JM, Burnett OL, Bender CD, Karstaedt N, Williams HJ. Diagnostic techniques. In: Berquist TH, ed. Radiology of the Foot and Ankle. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2000.
4. Oxford English Dictionary. 3rd ed. New York, NY: Oxford University Press; 1973.
5. Santanelli F, Grippaudo FR, Tenna S, Paolini G, Cigna E. Lower extremity reconstruction, foot. www.emedicine.com/plastic/TOPIC200.HTM. Published July 22, 2005. Accessed December 4, 2007.
6. Boyd PM, Rendall G. Structure and function. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London, England: Churchill Livingstone; 1993.
7. Anderson EG. The growing foot. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London, England: Churchill Livingstone; 1993.
8. Silbergleit R. Fractures, foot. www.emedicine.com/EMRG/topic195.htm. Published August 29, 2006. Accessed December 4, 2007.
9. Dorland’s Medical Dictionary. 26th ed. Philadelphia, PA: WB Saunders Co; 1981.
10. McStay CM, Davenport M, Carey MJ. Dislocations, foot. www.emedicine.com/emerg/TOPIC141.HTM. Published April 3, 2006. Accessed December 4, 2007.
11. Keany JE. Dislocations, ankle. www.emedicine.com/EMERG/topic140.htm. Published August 13, 2007. Accessed December 4, 2007.
12. Gray’s Anatomy. 29th ed. Philadelphia, PA: Running Press; 1974.
13. Shabshin N, Schweitzer ME, Morrison WB, Carrino JA,
Other imaging modalities are used to diagnose, evaluate and manage peripheral arterial disease. Useful modalities include: duplex ultrasonographic examina-tion, which combines Doppler waveform analysis and Doppler velocities; MR angiography, which does not expose patients to ionizing radiation; CT angiography, which can visualize calcification well; and contrast angiography, which currently is used for evaluation of candidates for surgical revascularization.67
CancerMost foot and ankle masses are benign, and foot
tumors are considered rare; malignancy occurs in only about 1 out of every 1000 growths.68 Certain malignant tumors tend to appear in the ankle and foot, including melanomas and other cancers of the skin, bone and soft tissue.5 Some tumors appear in tendon sheaths, includ-ing the giant-cell tumor of tendon sheath (GCTTS), which is a benign, slow-growing, soft-tissue growth.69 Even benign tumors can cause significant problems if they press on nerves and other surrounding structures, causing pain and loss of proper function.42 Recently, scientists established a correlation between previous trauma and mass growth, although the etiology of con-ditions such as GCTTS remains unknown.69
MR imaging has been proven of significant value in the evaluation of these conditions.42 MR can help delin-eate treatable lesions, and it can distinguish between irregular, hereditary muscle anomalies and true tumor masses, thus sparing many patients from unnecessary biopsy and worry. MR imaging cannot provide an exact diagnosis (histopathology must take on that task), but, along with CT, it is recommended for preoperative diagnosis.69
Clear-cell sarcoma is one of the cancers that has a predilection for the foot and ankle.70 This rare cancer is more prevalent in women and tends to appear between the ages of 20 and 50 years. Radiographs usually are normal, and both CT and MR imaging are used to detect and characterize the cancer. Lesions tend to be well defined, and there are histological similarities between this cancer and melanoma. Bone destruction occurs in up to 10% of cases, and the most common sites of metastasis are the lungs and skeleton.
Foot drop, in which ankle weakness combined with toe position results in dragging of the foot during ambu-lation, is highly suggestive of nerve impingement and for unknown reasons is more common in people with head and neck cancer.71 It also can signal neurological impairment due to metastatic disease in the spine. An
R0908_PodDR_25-44.indd 42R0908_PodDR_25-44.indd 42 8/28/08 1:45:27 PM8/28/08 1:45:27 PM
CEDIRECTED READING
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
43RADIOLOGIC TECHNOLOGY September/October 2008, Vol. 80/No. 1
29. Davies M. Circulatory disorders. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London: Churchill Livingstone; 1993.
30. Choi HK, Curhan G. Alcohol and gout. Am J Med. 2007;120: e5. doi:10.1016/j.amjmed.2006.09.025.
31. Choi HK, Curhan G. Soft drinks, fructose consumption, and the risk of gout in men: prospective cohort study. BMJ. 2008;336:309-312. doi:10/1136/bmj.39449.819271.BE. Published January 31, 2008.
32. Roddy E, Zhang W, Doherty M. Are joints affected by gout also affected by osteoarthritis? Ann Rheum Dis. 2007;66:1374-1377. doi:10.1136/ard.2006.063768.
33. Doherty M, Bardin T, Pascual E. International survey on the diagnosis and management of gout. Ann Rheum Dis. 2007;66:1685-1686. doi:10.1136/ard.2007.071530.
34. Calgary Foot Clinic. Foot disorders: bunions. www.foottalk.com/d_bunions.html. Published 2005. Accessed October 12, 2007.
35. WebMD. Bunions. www.webmd.com/a-to-z-guides/bunions-topic-overview. Published March 20, 2006. Accessed December 18, 2007.
36. Boyd PM, Neale D, Rendall G. The adult foot. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London, United Kingdom: Churchill Livingstone; 1993.
37. WebMD. Hammer, claw, and mallet toes. www.webmd.com/a-to-z-guides/hammer-claw-and-mallet-toes-topic-overview. Published July 11, 2007. Accessed February 23, 2008.
38. Whiting MF. Skin and subcutaneous tissues. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London, United Kingdom: Churchill Livingstone; 1993.
39. Lorimer DL and Neale D. The common foot disorders: their nature and origins. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London, United Kingdom: Churchill Livingstone; 1993.
40. Calgary Foot Clinic. Foot disorders: ankle, injuries. www.foottalk.com/d_ankle.html. Published 2005. Accessed October 12, 2007.
41. Berquist TH, Knudsen JM, Burnett OL, Bender CD, Karstaedt N, Williams HJ. Diagnostic techniques. In: Berquist TH, ed. Radiology of the Foot and Ankle. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2000.
42. Helms CA. Magnetic resonance imaging of the foot and ankle. In: Brant WE, Helms CA, eds. Fundamentals of Diagnostic Radiology. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
43. Calgary Foot Clinic. Foot disorders, stress fracture. www.foottalk.com/d_fractures.html. Published 2005. Accessed October 12, 2007.
44. Naradzay JF. Fractures, ankle. www.emedicine.com/EMERG/topic188.htm. Published November 15, 2007. Accessed December 4, 2007.
45. Johnson PT, Fayad LM, Fishman EK. Sixteen-slice CT
Keller MS, Grissom LE. High-signal T2 changes in the bone marrow of the foot and ankle in children: red mar-row or traumatic changes? Pediatr Radiol. 2007;36:670-676. doi:10.1007/s00247-006-0129-y.
14. Coley BD, Shiels II WE, Kean J, Adler BH. Age-dependent dynamic sonographic measurement of pediatric clubfoot. Pediatr Radiol. 2007;37:1125-1129. doi:10/1007/s00247 -007-0601-3.
15. Medical Encyclopedia: Clubfoot. www.nlm.nih.gov/med lineplus/ency/article/001228.htm. Published October 8, 2007. Accessed December 27, 2007.
16. El-Deeb KH, Orth DC, Ghoneium AS, El-Adwar KL, Orth MC, Khalil AA. Is it hazardous or mandatory to release the talocalcanel interosseous ligament in clubfoot surgery? J Pediatr Orthop. 2007;27(5):517-521.
17. Chesney D, Barker S, Maffulli N. Subjective and objective outcome in congenital clubfoot; a comparative study of 204 children. BMC Musculoskelet Disord. www.medscape.com/viewarticle/563409. Published October 4, 2007. Accessed December 4, 2007.
18. Kalantari, Seger, Chow, Motamedi. Accessory ossicles and sesamoid bones: spectrum of pathology and imaging evalu-ation. Appl Radiol. 2007;36(10):28-37. www.medscape.com/viewarticle/564711. Published October 26, 2007. Accessed December 4, 2007.
19. Richardson ML. Appendicular Arthritis in Approaches to Differential Diagnosis in Musculoskeletal Imaging. www.rad.washington.edu/mskbook/appendiculararthritis.html. Accessed October 12, 2007.
20. Case of the Day, Five-year-old boy with pain. http://education .auntminnie.com. Accessed December 18, 2007.
21. Lalam RK, Cassar-Pullicino VN, Tins BJ. Magnetic reso-nance imaging of appendicular musculoskeletal infection. Top Magn Reson Imaging. 2007;18(3):177-191.
22. Shakespeare W. Henry IV, Part II, I ii.23. Pillinger MH, Rosenthal P, Abeles AM. Hyperuricemia and
gout: new insights into pathogenesis and treatment. Bull of NYU Hosp for Joint Diseases. 2007;65(3):215-221.
24. Chui CH, Lee JY. Diagnostic dilemmas in unusual presenta-tions of gout. Aust Fam Phys. 2007;36(11):931-934.
25. Eggebeen AT. Gout: an update. Am Fam Physician. 2007;76:801-812. www.aafp.org/afp/20070915/801.html. Published September 15, 2007. Accessed December 8, 2007.
26. Terkeltaub R. Learning how and when to employ uricase as bridge therapy in refractory gout. www.jrheum.com/subscribers/0710/1955.html. Published October 2007. Accessed December 8, 2007.
27. Keith MP, Gilliland WR. Updates in the management of gout. Am J Med. 2007;120(3)221-224.
28. Annemans L, Spaepen E, Gaskin M, et al. Gout in the UK and Germany: prevalence, comorbidities and man-agement in general practice 2000-2005. Ann Rheum Dis. Published November 2, 2007. Accessed December 15, 2007. doi:10.1136/ard.2007.076232.
R0908_PodDR_25-44.indd 43R0908_PodDR_25-44.indd 43 8/28/08 1:45:27 PM8/28/08 1:45:27 PM
CEIMAGING IN PODIATRY
44 September/October 2008, Vol. 80/No. 1 RADIOLOGIC TECHNOLOGY
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
thropathy from osteomyelitis and soft-tissue infection? Nucl Med Commun. 2007;28(6):465-472.
60. Yadlapalli NG, Vaishnav A, Sheehan P. Conservative man-agement of diabetic foot ulcers complicated by osteomy-elitis. Wounds. 2002;14(1):31-35. www.medscape.com/view article/430893. Accessed December 4, 2007.
61. Wall B. Management of diabetic and other high risk patients. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London, United Kingdom: Churchill Livingstone; 1993.
62. American Diabetes Association. Standards of medical care for patients with diabetes mellitus. Diabetes Care. 2001;24(1s):s33. www.medscape.com/viewarticle/433745. Accessed December 4, 2007.
63. WebMD. Diabetes health center. http://diabetes.webmd.com/feet-can-last-lifetime. Accessed December 18, 2007.
64. Schwegler B, Stumpe KDM, Weishaupt D, et al. Unsuspected osteomyelitis is frequent in persistent diabetic foot ulcer and better diagnosed by MRI than by 18F-FDG PET or 99mTc-MOAB. J Internal Med. 2008;263:99-106. doi:10.1111/j.1365-2796.2007.01877.x.
65. Kunkel, CF, Figoni SF, Baumgarten JM, et al. Scanning laser-Doppler imaging of leg- and foot-skin perfusion in normal subjects, analysis of age, gender, site, and laser-type effects. Am J Phys Med Rehabil. 2007;86(4):262-271.
66. Williams DT, Harding KG, Price PE. The influence of exercise on foot perfusion in diabetes. Diabetic Med. 2007;24:1105-1111. doi:10.1111/j.1464-5491.2007.02218.x.
67. Begelman SM, Jaff MR. Noninvasive diagnostic strate-gies for peripheral arterial disease. Cleveland Clinic J Med. 2006;73(4s):s22-s29.
68. Calgary Foot Clinic. Foot disorders, soft tissue masses. www.foottalk.com/d_softtissue.html. Published 2005. Accessed October 12, 2007.
69. Vasconez HC, Nisanci M, Lee EY. Giant cell tumour of the flexor tendon sheath of the foot. J Plast Reconstr Aesthet Surg. 2007. doi:10.1016/j.bjps.2006.09.006. (article in press).
70. Al-Nakshabandi NA, Munk PL. Radiology for the surgeon, musculoskeletal case 38. J Can Chir. 2007;50(1)58-59.
71. Borress RS, Maccabee P, Har-El G. Foot drop in head and neck cancer. Am J Otolaryngology – Head and Neck Medicine and Surgery. 2007;28(5):321-324. doi:10.1016/j.amjoto .2006.10.003.
Elizabeth J Church, JD, has practiced law for more than 25 years, emphasizing issues of mental health and disability law.
Reprint requests may be sent to the American Society of Radiologic Technologists, Communications Department, 15000 Central Ave SE, Albuquerque, NM 87123-3909, or e-mail [email protected].
©2008 by the American Society of Radiologic Technologists.
with volumetric analysis of foot fractures. Emerg Radiol. 2006;12(4):171-176.
46. Lattermann C, Goldstein JL, Wukich DK, Lee S, Bach BR. Practical management of Lisfranc injuries in athletes. Clin J Sport Med. 2007;17(4):311-315.
47. Boyd PM, Bogdan RJ. Sports injuries. In: Lorimer DL, ed. Neale’s Common Foot Disorders, Diagnosis and Management. 4th ed. London, United Kingdom: Churchill Livingstone; 1993.
48. Richards CF. Ankle injury, soft tissue. www.emedicine.com/EMERG/topic30.htm. Published September 13, 2007. Accessed December 4, 2007.
49. Calgary Foot Clinic. Foot disorders, heel pain (plantar fas-ciitis). www.foottalk.com/d_heelpain.html. Published 2005. Accessed October 12, 2007.
50. Irving DB, Cook JL, Young MA, Menz HB. Obesity and pronated foot type may increase the risk of chronic plantar heel pain: a matched case-control study. BMC Musculoskelet Disord. 2007;8:41. www.medscape.com/viewarticle/559871. Published July 30, 2007. Accessed December 4, 2007.
51. Medline Plus Medical Encyclopedia: septic arthritis. www.nlm.nih.gov/medlineplus/ency/article/000430.htm. Published February 20, 2008. Accessed February 29, 2008.
52. American Diabetes Association. Economic costs of diabe-tes in the U.S. in 2007. Diabetes Care. 2008;31(3):596-615. http://care.diabetesjournals.org/cgi/content/full/31 /3/596. Published February 2008. Accessed March 4, 2008. doi: 10.2337/dc08-9017.
53. Winocour PH, Ainsworth A, Williams R. Association of British Clinical Diabetologists (ABCD) survey of secondary care services for diabetes in the UK, 2000. 1. Methods and major findings. Diabet Med. 2002;19:327-333.
54. Calgary Foot Clinic. Foot disorders, diabetic foot. www.foottalk.com/d_diabetic.html. Published 2005. Accessed October 12, 2007.
55. Mulder G, Armstrong D, Seaman S. Standard, appropriate, and advanced care and medical-legal considerations: part one – diabetic foot ulcerations. Wounds. 2003;15(4):92-106. www.medscape.com/viewarticle/456305. Updated June 9, 2003. Accessed December 4, 2007.
56. Severinsen K, Anderson H. Evaluation of atrophy of foot muscles in diabetic neuropathy – a comparative study of nerve conduction studies and ultrasonogra-phy. Clin Neurophysiol. 2007;118:2172-2175. doi:10.1016/ j.clinph.2007.06019.
57. Severinsen K, Obel A, Jakobsen J, Anderson H. Atrophy of foot muscles in diabetic patients can be detected with ultra-sonography. http://care.diabetesjournals.org. Published September 5, 2007. Accessed December 4, 2007.
58. Lundy KC, Genez B, Pratt K. Clinical quiz. Appl Radiol. 2002;31(4):41-43. www.medscape.com/viewarticle/433089. Accessed December 4, 2007.
59. Basu S, Chryssikos T, Houseni M, et al. Potential role of FDG PET in the setting of diabetic neuron-osteoarthropa-thy: can it differentiate uncomplicated Charcot’s neuroar-
R0908_PodDR_25-44.indd 44R0908_PodDR_25-44.indd 44 8/28/08 1:45:27 PM8/28/08 1:45:27 PM