Embed Size (px)
Citation preview

CI
MM
*
BqctbOrwnqaffHaMivcdmwthc13Cmalr
KS
B4wrMbpifho
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:979–985
irrhotic Patients Are at Risk for Health Care–Associated Bacterialnfections
ANUELA MERLI,* CRISTINA LUCIDI,* VALERIO GIANNELLI,* MICHELA GIUSTO,* OLIVIERO RIGGIO,*ARCO FALCONE,‡ LORENZO RIDOLA,* ADOLFO FRANCESCO ATTILI,* and MARIO VENDITTI‡
Division of Gastroenterology, Department of Clinical Medicine, ‡Department of Infectious Diseases and Tropical Medicine, “Sapienza” University of Rome, Rome, Italy
etdcgitt(nrwsmditp
apmrmca
eHbbcvn
fiHmt
ACKGROUND & AIMS: Bacterial infections are a fre-uent and serious burden among patients with cirrhosis be-ause they can further deteriorate liver function. We assessedhe epidemiology, risk factors, and clinical consequences ofacterial infections in hospitalized cirrhotic patients. METH-DS: In a cohort of hospitalized cirrhotic patients (n � 150)
eferred to a tertiary care setting, all episodes of bacterial infectionsere recorded prospectively. Infections were classified as commu-ity-acquired (CA), health care–associated (HCA), or hospital-ac-uired (HA). Site of infection, characteristics of bacteria, and prev-lence of antibiotic resistance were reported; consequences for liverunction and patient survival were evaluated. RESULTS: Fifty-our infections were observed among 50 patients (12 CA, 22CA, and 20 HA). Bacterial resistance was more frequent
mong patients with HCA or HA infections (64% of isolates).ortality was 37% from HA, 36% from HCA, and 0% from CA
nfections. Independent predictors of infection included a pre-ious infection within the past 12 months (P � .0001; 95%onfidence interval [CI], 2.2–10.6), model of end-stage liverisease score �15 (P � .01; 95% CI, 1.3– 6.1), and proteinalnutrition (P � .04; 95% CI, 1.5–10). Infectious episodesorsened liver function in 62% of patients. Patients with infec-
ion more frequently developed ascites, hepatic encephalopathy,yponatremia, hepatorenal syndrome, or septic shock. Childlass C (P � .006; 95% CI, 1.67–23.7), sepsis (P � .005; 95% CI,.7–21.4), and protein malnutrition (P � .001; 95% CI, 2.8 –8.5) increased mortality among patients in the hospital.ONCLUSIONS: In hospitalized cirrhotic patients, theost frequent infections are HCA and HA; these infections
re frequently resistant to antibiotics. As infections worsen,iver function deteriorates and mortality increases. Cir-hotic patients should be monitored closely for infections.
eywords: Sepsis; Survival; Multidrug Resistance; Nutritionaltatus.
acterial infections are a frequent and severe complicationin cirrhotic patients.1 Episodes of infection are reported in
0% of hospitalized cirrhotic patients.2 Infections are associatedith a longer hospital stay and a higher risk of death; infection-
elated mortality rate, in fact, ranges between 15% and 19%.2,3
ost of the infections in cirrhotic patients are caused by entericacteria.4 This suggests that the defense mechanisms of theseatients fail to prevent the microorganisms present in the
ntestinal lumen from reaching the systemic circulation. Sepsisavors acute decompensation of cirrhosis and may lead toepatic encephalopathy, renal insufficiency, shock, and “acute
n chronic liver failure.”1The possible risk factors for infections have been scarcelyvaluated in chronic liver disease and a recent review indicatedhat a Child–Pugh C score can be considered the only indepen-ent predictor.5 In most of the studies, bacterial infections inirrhotic patients are caused, in large prevalence (70%– 80%), byram-negative cocci. In the past decade, however, infectionsnduced by gram-positive bacilli have increased, owing to long-erm antibiotic prophylaxis with quinolones recommended forhose patients with previous spontaneous bacterial peritonitisSBP) episodes,6,7 which prevents infections caused by gram-egative bacilli but not those caused by gram-positive cocci. Itecently has been proposed that infections occurring in patientsho have had previous recent contact with the health care
ystem can be classified as health care–associated (HCA) anday have a worse prognosis.8 Patients with advanced liver
isease frequently need to be hospitalized and therefore may bencluded in this risk category. No information is available abouthe prevalence and consequences of HCA infections in cirrhoticatients.
The current study consists of a prospective investigationimed at determining, in a large cohort of hospitalized cirrhoticatients, the following: (1) the prevalence and etiology of com-unity-acquired (CA), HCA, and hospital-acquired (HA) bacte-
ial infections; (2) the risk factors associated with the develop-ent of bacterial infections; (3) the short-term clinical
onsequences of infection; and (4) patient survival 6 monthsfter hospital discharge.
Patients and MethodsPatientsFrom October 2008 to June 2009, we consecutively
nrolled all cirrhotic patients hospitalized at our Universityospital (a tertiary referral center). Diagnosis of cirrhosis was
ased on liver biopsy, when available, or on obvious clinical,iochemical, or ultrasonographic and endoscopic features. Ex-lusion criteria were a concomitant human immunodeficiencyirus infection, high-dose corticosteroid treatment, and immu-osuppressive therapy. The study was approved by the local
Abbreviations used in this paper: CA, community-acquired; CI, con-dence interval; HA, hospital-acquired; HCA, health care–associated;CC, hepatocellular carcinoma; HRS, hepatorenal syndrome; MDR,ultidrug resistant; OR, odds ratio; SBP, spontaneous bacterial peri-
onitis; SIRS, systemic inflammatory response syndrome.© 2010 by the AGA Institute
1542-3565/$36.00
doi:10.1016/j.cgh.2010.06.024
Es
wsotapwtirrsmswe(nmaatnw
trcotraitfl
tmchccbdadi
pmp
lmcsmw6
w
wfcdoof
wdct
paTrAif
cShwai
uAptmf
h
icwds
Pa
980 MERLI ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 8, No. 11
thical Committee Review Board, and written informed con-ent was signed by all the participants.
Clinical Evaluation and ManagementDemographic, clinical, and biochemical parameters
ere recorded for each patient in a preformed digitalized data-et. At admission, previous relevant clinical data, such as originf liver disease, history of alcohol abuse, ascites, encephalopa-hy, gastrointestinal bleeding, acute or chronic renal failure,nd coexistence of other diseases, were recorded. Previous hos-italizations (within 6 mo), episodes of infections diagnosedithin the past 12 months, and therapy administered during
he past 4 weeks also was noted. The main cause of hospital-zation was identified and basal clinical and biochemical pa-ameters were assessed to define the severity of liver disease,enal function, and electrolyte imbalance. Mean arterial pres-ure, heart rate, respiratory rate, and body temperature were
easured and the presence of systemic inflammatory responseyndrome (SIRS) was investigated.9 The severity of liver diseaseas assessed using the Child–Pugh score10 and the model of
nd-stage liver disease (MELD) score.11 Hepatorenal syndromeHRS) was diagnosed according to international criteria.12 Theutritional status was assessed in all the patients by anthropo-etric measurements.13 Complications of cirrhosis were treated
ccording to recent guidelines.14 Antibiotic prophylaxis wasdministered in patients with previous SBP or recent gastroin-estinal bleeding.15,16 Overt hepatic encephalopathy was diag-osed according to the West Haven criteria17 and treated onlyhen the symptoms were clinically evident.
Diagnosis and Management of InfectionBacterial infections were actively looked for in all pa-
ients based on the following assessment: (1) medical historyeporting symptoms of infection; (2) physical examination fo-used on symptoms and signs suggestive of infection; (3) lab-ratory tests including erythrocyte sedimentation rate, C-reac-ive protein level, polymorphonucleater cell count, hepatic andenal function tests, and urinary sediment; (4) analysis of thescitic fluid when present; (5) chest radiograph; and (6) abdom-nal ultrasound. When a bacterial infection was suspected, fur-her investigations (cultures of blood, urine, sputum, asciticuid, or purulent secretions) were performed.
SBP was defined as a polymorphonucleater cell count greaterhan 250/mm3 in the ascitic fluid � a positive culture; pneu-
onia was defined as the presence of radiologic evidence ofonsolidation plus at least 2 of the following criteria: feverigher than 38°C or hypothermia less than 35°C, dyspnea,ough and purulent sputum, pleuritic chest pain, or signs ofonsolidation on physical examination. Urinary tract infections,iliary tract infections, cellulitis, and gastroenteritis were alliagnosed according to congruent symptoms and biochemicalnd imaging parameters following standard criteria.18 The evi-ence of a positive blood culture without a recognized site of
nfection was defined as spontaneous bacteremia.
Study Design, Follow-Up Evaluation, andOutcomesA complete patient assessment was performed at hos-
ital admission and at discharge. If a diagnosis of infection wasade during hospitalization, the patient assessment was re-
eated at that time. Main outcomes were modifications of the f
iver function, development of kidney dysfunction, develop-ent of hepatic encephalopathy, gastrointestinal bleeding, as-
ites, hyponatremia, length of hospital stay, and in-hospitalurvival. Patients were re-evaluated as outpatients at 1, 3, and 6
onths or until death or liver transplant. The study was closedhen the last patient enrolled had completed at least the-month follow-up evaluation.
DefinitionsInfections were classified as follows.
Infections were classified as HA if the diagnosis of infectionas made after more than 48 hours of hospital stay.
Infections were classified as HCA if the diagnosis was madeithin 48 hours of hospitalization in patients with any of the
ollowing criteria: (1) had attended a hospital or a hemodialysislinic, or had received intravenous chemotherapy during the 30ays before infection; or (2) were hospitalized for at least 2 days,r had undergone surgery during the 180 days before infection;r (3) had resided in a nursing home or a long-term careacility.8
Infections were classified as CA if the diagnosis of infectionas made within 48 hours of hospitalization and the patientid not fulfill the criteria for HCA infection8 (ie, had no recentontact with the health care system and was not hospitalized inhe past 6 months).
Patients with infections were treated immediately with em-iric large-spectrum antibiotics, based on the site of infectionnd according to standard guidelines and local epidemiology.he antibiotic treatment then was modified according to the
esults of cultures (if available) and in case of treatment failure.ll patients with infection underwent a consultation by an
nfectious diseases specialist with expertise in nosocomial in-ections.
Patients were considered to have SIRS when they fulfilled theriteria established by the most recent international guidelines.epsis was diagnosed in the presence of SIRS and a known orighly suspected infection. Septic shock was defined as sepsisith hypotension refractory to intravascular volume loading,ssociated with perfusion abnormalities that required the use ofnotropes.9
The definition of a multidrug resistant (MDR) pathogen wassed to describe a methicillin-resistant Staphylococcus aureus, ancinetobacter baumannii, an extended-spectrum �-lactamases–roducing gram-negative strain, or any bacterial isolate resis-ant to at least 3 classes of antimicrobial agents.19,20 Protein
alnutrition was diagnosed when the midarm muscle circum-erence was below the fifth percentile of the referral standard.13
Statistical AnalysisEach patient was considered only once during the first
ospitalization.To evaluate liver function modifications induced by the
nfection, the tests performed at the time of diagnosis wereompared either with recent previous results (when available) orith the liver function test at the first outpatient control afterischarge (1 month), when the infection had completely re-olved.
All the values are reported as means � standard deviations;values less than .05 were considered significant. Data were
nalyzed as continuous or categoric by using the Student t test
or parametric data and the Mann–Whitney U test or the Wil-
cfstwviuS
ttaccb3ahee(2ahtpstpoq
jdMpwco
5obi
iih.n
wr
aqgciboipt
Mgvtm
isc
dm1pt
mih5ha
iC(ist((tm1rlfw
w.s
November 2010 BACTERIAL INFECTIONS IN CIRRHOTIC PATIENTS 981
oxon test for nonparametric data; the chi-square test was usedor the comparison of dichotomous data. The logistic regres-ion analysis was used to identify possible predictors of infec-ion and in-hospital mortality. Univariate analysis (log rank)as used to identify prognostic factors of survival, and the
ariables selected by this analysis were included in a multivar-ate analysis according to a Cox regression model. The softwaresed for the analysis was NCSS (Number Cruncher Statisticalystem, Kaysville, UT) 2007.
ResultsPatientsFour patients were excluded, 1 for high-dose steroid
herapy and 3 because of a recurrence of cirrhosis after liverransplantation. A total of 150 patients was enrolled: 48 womennd 102 men, with a mean age of 64 � 13 years. The origin ofirrhosis was hepatitis C in 51% of cases, alcohol abuse in 19%,ryptogenetic in 15%, autoimmune in 5%, hepatitis B in 4%, andoth hepatitis B and C in 3.3% of patients. Child class was A in0%, B in 39%, and C in 31% of patients. The mean MELD scoret admission was 13.5 (range, 5– 40). The main reasons forospital admission were as follows: ascites in 37 patients (25%),lective procedures in 33 (22%), suspected infection in 21 (14%),ncephalopathy in 20 (13%), gastrointestinal bleeding in 128%), renal failure in 5 (3%), and other reasons in the remaining2 patients (15%). Forty-nine patients had clinical evidence ofscites at the time of hospitalization, and 82 were known toave esophageal varices (48 small and 34 large varices). Fifty-wo patients reported a previous documented infection in theast 12 months (19 urinary tract infections, 13 pneumonia, 4pontaneous bacteremia, 4 biliary tract infections, 3 gastroin-estinal, 3 skin infections, 2 SBP, and 6 in other sites). Seventeenatients received antibiotics in the preceding 30 days, 9 becausef a recent infectious episode and 8 because of prophylaxis withuinolones.
Thirteen patients had been treated previously with trans-ugular intrahepatic portosystemic shunt. Twenty-six cases had aiagnosis of hepatocellular carcinoma (HCC), 18 were within theilan criteria,21 and 8 exceeded the Milan criteria (3 of these
atients also had portal thrombosis). The 26 patients with HCCere hospitalized either for diagnostic purposes (3 cases), to re-
eive locoregional treatment (21 cases), or for other complicationsf cirrhosis (2 patients).
A total of 54 episodes of bacterial infection were recorded in0 patients (33%); 4 patients presented more than one episodef infection during hospitalization. Demographic, clinical, andiochemical characteristics of the patients with and without
nfection are shown in Table 1.The degree of liver impairment was significantly more severe
n the patients with infection. The patients who developed annfection had significantly lower albumin levels (P � .001),igher bilirubin levels (P � .002), higher creatinine levels (P �
001), and lower sodium levels (P � .008) than those who didot.
Bacterial Infections, Systemic InflammatoryResponse Syndrome, and SepsisAmong the 54 episodes of infection, 12 were CA, 22
ere HCA, and 20 were HA. The infections most commonly
ecorded were urinary tract infections (37%), pneumonia (22%), snd spontaneous bacteremia (13%). Table 2 shows the fre-uency of the different sites of infection in the 3 epidemiologicroups. Twenty-six infections were documented microbiologi-ally. Gram-negative organisms, particularly Escherichia coli, weresolated more frequently (62%) than gram-positive ones (38%),ut gram-positive bacteria were prevalent in HA infections (64%f isolates). Blood cultures were positive in 12 episodes of
nfection: 3 urinary infections, 4 cases of cholangitis, 2 cases ofneumonia, 1 case of SBP, and 2 cases of spontaneous bac-eremia.
As shown in Table 2, 16 patients had an infection caused byDR bacteria. Six of the 16 patients (37.5%) with MDR patho-
ens died during their hospital stay (3 HRS, 2 septic shock, 1ariceal bleeding). Among the 17 patients undergoing antibioticherapy in the preceding 30 days, MDR pathogens were isolated
ore frequently (5 of 7 infectious episodes; P � .002).SIRS was diagnosed in 43 patients and sepsis was diagnosed
n 31 patients. The type of infection more often leading toepsis was pneumonia. SIRS unrelated to infection mostly oc-urred in those patients undergoing invasive treatments.
Risk Factors for the Development of InfectionThe variables examined as possible risk factors for the
evelopment of infection or sepsis are reported in Table 3. Atultivariate analysis, a history of previous infection in the past
2 months, a MELD score of 15 or greater, and a diagnosis ofrotein malnutrition were independent predictors for infec-ions and sepsis (Table 4).
Potential risk factors that could be involved in the develop-ent of HA infections also were evaluated. The number of
nvasive procedures during hospitalization was significantlyigher (P � .02) in patients who developed HA infections (Table). We also found that HA infections were associated withospitalization in rooms in which there was a need to placedditional beds (P � .0002) (Table 5).
Clinical FeaturesA worsening of liver function frequently was observed
n patients with infection, especially in those with sepsis. Thehild–Pugh score deteriorated in 62% of cases with infection
mean increase in Child score, �1.9 � 0.8; range, 1–2) andn 71% of patients with sepsis (mean increase in Childcore, �2.5 � 0.7; range, 1– 4), whereas the MELD score inhe same patients showed a mean increase of �3.8 � 2.7range, 1– 4) in patients with infection and of �4.9 � 2.7range, 1–12) in those with sepsis. The parameters that de-eriorated more often were as follows: bilirubin (�4.4 � 12
g/dL), albumin (�0.34 � 0.9 g/dL), creatinine (�0.6 �.8 mg/dL), and serum sodium (�3.3 � 6.1 mEq/L) levels,espectively. Moreover, episodes of ascites, hepatic encepha-opathy, hyponatremia, HRS, and septic shock were morerequent in patients with infection as compared with thoseho were not infected (Table 6).
OutcomesOverall in-hospital mortality was 12%; 14 patients
ith and 4 patients without infection died (28% vs 4%; P �00007). The mortality rate was higher in the patients withepsis (12 of 31; 38%) than in those with infection but no
epsis (2 of 19, 10%; P � .00000).
fr((
iCdnM[.(dppcw3
eaauerdt
cstalt
T
AMAO
M
HMCMHRTWHPASSISBSSS
H
982 MERLI ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 8, No. 11
Patient mortality was related to the epidemiology of in-ection: patients with HA infections, in fact, had a mortalityate (37%) similar to that of patients with HCA infections36%), whereas none of the patients with CA infections diedP � .046).
Univariate analysis showed that sepsis (P � .00000), bacterialnfections (P � .00002), MELD score of 15 or greater (P � .03),hild class C (P � .00004), protein malnutrition (P � .000001),evelopment of antibiotic resistance (P � .00009), and hypo-atremia (P � .002) were related significantly to mortality.ultivariate analysis selected Child class C (P � .006; odds ratio
OR], 6.3; 95% confidence interval [CI], 1.67–23.7), sepsis (P �0056; OR, 6.01; 95% CI, 1.7–21.46), and protein malnutritionP � .0004; OR, 10.44; 95% CI, 2.8 –38.5) as independent pre-ictors of in-hospital death. Causes of in-hospital death inatients with infections were HRS (6 patients), septic shock (5atients), hemorrhagic shock (2 patients), severe arrhythmiaausing cardiovascular arrest (1 patient). All of the 4 patientsho died without infection died of end-stage liver failure, and
able 1. Demographic, Clinical, and Biochemical CharacterisPresence of Infection During Their Hospitalization
VariablesPatients without
(n � 10
ge, y 63 � 1ale/females 64/36ctive alcohol abusers, n (%) 21 (21rigin of liver diseaseAlcohol, n (%) 19 (19HCV-related, n (%) 56 (56HBV-related, n (%) 6 (6)Other, n (%) 19 (19ain cause of admissionElective procedure, n (%) 31 (31Ascites, n (%) 30 (30Suspected infection, n (%) 0 (0)Encephalopathy, n (%) 11 (11Gastrointestinal bleeding, n (%) 9 (9)Renal failure, n (%) 2 (2)Other, n (%) 17 (17
CC, n (%) 20 (20ELD score 11.8 � 4hild–Pugh score 7.6 � 2ean arterial pressure, mm Hg 88 � 1eart rate, beats/min 75 � 1espiratory rate, breaths/min 15 � 2emperature, �37.5°C 6 (6)hite blood cells, cell/mm3 5297 � 2emoglobin level, g/dL 11.6 � 2latelets, num/mm3 � 103 120 � 9lanine aminotransferase level, IU/L 57 � 6erum bilirubin level, mg/dL 3.1 � 5erum albumin level, mg/dL 3.3 � 0
nternational normalized ratio 1.5 � 1erum creatinine level, mg/dL 0.91 � 0lood urea nitrogen level, mg/dL 23.2 � 1erum sodium level, mmol/L 135.7 � 5erum potassium level, mmol/L 4.4 � 0edimentation rate, mm/h 21 � 1
CV, hepatitis C virus; HBV, hepatitis B virus.
of them also had a diagnosis of advanced HCC. l
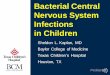
The overall mortality in the following 6 months also wasvaluated. The mortality rate at 3 months was 34% versus 6%,nd at 6 months was 50% versus 11% in patients with infections compared with those without infection (Supplementary Fig-re 1). The main causes of death after hospital discharge werend-stage liver failure (7 patients), variceal bleeding (4 patients),enal failure (4 patients), septic shock (2 patients), and myocar-ial infarction (1 patient); 5 patients underwent liver transplan-ation.
DiscussionCirrhosis presently may be considered one of the most
ommon immunodeficiency-acquired conditions and previoustudies reported an infection rate of 40% to 50% among hospi-alized cirrhotic patients, with consequent significant morbiditynd mortality rates.2,5 In the present study, we found the fol-owing: (1) the large majority of bacterial infections in hospi-alized cirrhotic patients are HCA or HA; (2) the high preva-
of Patients Included in the Study Classified According to the
tions Patients with infections(n � 50) P value
65 � 13 .338/12 .114 (28) .6
10 (20) .821 (42) .15 (10) .37
14 (28) .09
2 (4) �.0017 (14) �.001
21 (42) �.0019 (18) .163 (6) .43 (6) .145 (10) .157 (14) .36
17.1 � 7.4 �.0018.7 � 2.1 �.00184 � 20 .0882 � 14 �.00118 � 4 .00137 (74) .016
9229 � 5973 .00110.9 � 3.6 .13123 � 88 .9
58 � 79 .97.6 � 12.0 .0022.7 � 0.7 �.0011.5 � 0.4 .54
1.57 � 1.58 .00137.9 � 30.5 �.001
130.0 � 19.6 .0084.2 � 0.2 .737 � 26 �.001
tics
infec0)
3
)
))
)
))
)
)).5.013
754.352.6.6.3.448.2.1.79
ence of these epidemiologic categories contributes to a higher

p(mdsec
tlson
ho
fqtrsftgoffibtnpfctrcir
T
S
M
I
M
T
P
P
CMPT
R
A
D
T
P
M
P
T
P
I
P
a
crc
November 2010 BACTERIAL INFECTIONS IN CIRRHOTIC PATIENTS 983
revalence of antibiotic-resistant strains and a worse outcome;3) in addition to the severity of the liver disease, protein
alnutrition is an important independent risk factor for theevelopment of infections in cirrhosis; and (4) infection andepsis induce liver deterioration and increase the risk of hepaticncephalopathy, renal failure, hyponatremia, and mortality inirrhotic patients.
In our experience, the most common sites of infection werehe urinary (35%) and the lower respiratory (22%) tracts. Theseatter infections were those more frequently leading to a sepsisyndrome. In all the patients hospitalized with clinical evidencef ascites (49 cases), the peritoneal fluid was analyzed foreutrophil cell count and bacterial culture, and 4 (8%) patients
able 2. Characteristics of the 54 Episodes of InfectionsAccording to the Epidemiology Classification
CA(n � 12)
HCA(n � 22)
HA(n � 20)
ites of infectionUrinary tract infections, n (%) 4 (33) 4 (18) 9 (45)Pneumonia, n (%) 3 (25) 5 (23) 4 (20)Spontaneous bacteriemia, n (%) 1 (8) 4 (18) 2 (10)Spontaneous bacterial
peritonitis, n (%)1 (8) 2 (9) 1 (5)
Biliary tract infections, n (%) 1 (8) 2 (9) 1 (5)Other infections, n (%) (eg,
skin, gastrointestinal,lymphangitis, bursitis)
2 (16) 4 (18) 2 (10)
icrobiologically documentedinfections
4 (33) 11 (50) 11 (55)
solated pathogensStaphylococcus aureus 0 1 4Coagulase-negative
Staphylococci1 1 3
Enterococcus faecalis 1 0 2Enterobacteriaceae (E coli,
Klebsiella, Proteus)2 9 2
DR 2 (16) 9 (41) 5 (23)
able 3. Variables Associated With Infection at UnivariateAnalysis in the Patients Included in the Study
Variables
Patients withoutinfections
(100)
Patients withinfections
(50)P
value
revious hospitalizations(past 6 months), n (%)
37 (37) 33 (66) .006
revious infections (past12 months), n (%)
26 (26) 26 (52) .002
hild–Pugh class C, n (%) 24 (24) 22 (44) .012ELD score, �15, n (%) 25 (25) 25 (50) .002rotein malnutrition, n (%) 19 (19) 26 (52) .001ransjugular intrahepaticportosystemic shunt,n (%)
5 (5) 12 (24) .02
ecent gastrointestinalbleeding (�7 d), n (%)
6 (6) 4 (8) .64
ntibiotic therapy in thepreceding 30 days
9 (9) 8 (16) .2
iabetes, n (%) 29 (29) 16 (32) .8t
ad a diagnosis of SBP, a rate similar to that reported previ-usly in other Italian studies.3
Enteric gram-negative cocci were the microorganisms morerequently isolated, whereas gram-positive ones were more fre-uent in the HA infection group. It has recently been proposedhat antibiotic resistances are increasing in hospitalized cir-hotic patients and this has been attributed to the larger diffu-ion of quinolone prophylaxis for SBP.6 In the present study weound a consistent (64%) number of MDR pathogens amonghe isolates. This high prevalence was probably related to thereat number of HCA and HA infections that were diagnosed inur series, because the patients with advanced liver diseaserequently are in need of hospital care. Previous studies, per-ormed on noncirrhotic patients, showed that HA and HCAnfections are caused more frequently by antibiotic-resistantacteria and are associated with a more severe clinical coursehan CA infections.8,22 A different empiric treatment for thisew epidemiologic category has been suggested. The presentrospective and observational study reports data on HCA in-ections in cirrhotic patients. We confirm that, as in otherategories, in cirrhotic patients HCA infections also are similaro HA infections with regard to the prevalence of antibiotic-esistant pathogens, severe clinical course, and unfavorable out-ome (in-hospital mortality in our series was 37% in HCA, 36%n HA, and none of the patients with CA infections died). In aecent meta-analysis, only the severity of liver disease has been
able 4. Variables Independently Associated With Infectionand Sepsis at Multivariate Analysis
Infections Sepsis
revious infections(past 12 months)
OR, 4.795% CI, 2.2–10.6P � .000
OR, 3.495% CI, 1.3–8.1P � .007
ELD score, �15 OR, 2.895% CI, 1.3–6.1P � .001
OR, 4.495% CI, 1.8–10P � .001
rotein malnutrition OR, 495% CI, 1.5–10P � .004
OR, 495% CI, 1.5–10P � .004
able 5. Prevalence of Factors That May Be Involved in theDevelopment of HA Infections
Variables
Patients withoutinfections
(100)
Patients withHA
infections (16)P
value
atients undergoinginvasive procedures,n (%)
66 (74) 14 (75) .08
nvasive procedures,number per patienta
1.77 � 1.1 2.4 � 1.7 .02
atients hospitalized in aroom with anadditional bed, n (%)
19 (19) 10 (62) �.001
Invasive procedures were as follows: paracentesis, dialysis, urinaryatheter, endoscopic variceal ligation, sclerotherapy, endoscopic ret-ograde cholangiopancreatography, percutaneous transhepaticholangiography, locoregional treatments of HCC, and placement of a
ransjugular intrahepatic portosystemic shunt.
rWe(aiarhp
ii
idaihn
diaimtoam
hhfcild
iSmBit
hb
noj
1
1
T
HHHAVHSI
984 MERLI ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 8, No. 11
ewarded as a reliable risk factor for infections and sepsis.5
hen the factors associated with both these conditions werexamined, we could confirm that the severity of the liver diseaseindicated by a MELD score of �15) is a good predictor, but welso found that additional parameters (a previous episode ofnfection in the past 12 months and protein malnutrition) mayllow identification of a subgroup of cirrhotic patients at highisk of infection. All these parameters are easy to identify atospital admission through the clinical history, simple anthro-ometric measurements, and biochemical data.
Malnutrition is known to be a negative prognostic factor forn-hospital morbidity and mortality in cirrhotic patients23 andncreases the rate of infection in liver recipients.24
As previously reported, the consequences of infection/sepsisn cirrhotic patients are highly detrimental.3 The liver functioneteriorated in about two thirds of the patients who developedn infection: these patients showed a worsening of the mainndicators of hepatic function (bilirubin and albumin) and aigher risk of encephalopathy, ascites, renal dysfunction, hypo-atremia, and hemodynamic shock.
The mechanism through which infections induce a furthereterioration of liver function in cirrhotic patients has not been
nvestigated extensively as yet. Infections, and especially sepsis,re accompanied by a downright cytokine storming, mostlynterleukin-6 and tumor necrosis factor-�. These latter are the
ajor hepatic triggers for the production of acute-phase pro-eins.25 It is conceivable that a cirrhotic liver facing an infectionr an increased endotoxin blood level may be overwhelmed byn increased demand of acute-phase reaction protein,26 and thisay lead to an exhaustion of the hepatocytes’ reserve function.It is worth noting that the in-hospital mortality rate was
igher in those patients who had an episode of infection duringospitalization. Moreover, survival was worse in this group even
or those who were discharged from the hospital. The mainauses of death in this setting were liver failure, variceal bleed-ng, and renal failure: the episode of infection by deterioratingiver function seems to accelerate the natural history of theisease.
In conclusion, the results of our study show that the major-ty of infections in hospitalized cirrhotic patients are HCA.evere liver disease, malnutrition, and infection in the past 12onths are parameters that identify patients at higher risk.
ecause infection and sepsis are highly detrimental in hospital-zed patients with cirrhosis and frequently are caused by resis-
able 6. Clinical Complications in 150 Cirrhotic Patients WithTheir Hospitalization
Patients withinfection (50)
Patientswithout
infection (10
RS type 1, n (%) 7 (14) 0RS type 2, n (%) 4 (8) 2 (2)epatic encephalopathy, n (%) 19 (38) 15 (15)scites, n (%) 33 (66) 51 (51)ariceal bleeding, n (%) 7 (14) 6 (6)yponatremia, n (%) 19 (38) 14 (14)hock, n (%) 6 (12) 0
n-hospital mortality, n (%) 14 (28) 4 (4)
ant pathogens the identification of the criteria to select a 1
igh-risk group may help in planning a different empiric anti-iotic approach in this category.
Supplementary MaterialNote: To access the supplementary material accompa-
ying this article, visit the online version of Clinical Gastroenter-logy and Hepatology at www.cghjournal.org, and at doi:10.1016/.cgh.2010.06.024.
References
1. Gustot T, Durand F, Lebrec D, et al. Severe sepsis in cirrhosis.Hepatology 2009;50:2022–2033.
2. Borzio M, Salerno F, Piantoni L, et al. Bacterial infection inpatients with advanced cirrhosis: a multicentre prospectivestudy. Dig Liver Dis 2001;33:41–48.
3. Fasolato S, Angeli P, Dallagnese L, et al. Renal failure andbacterial infection in patients with cirrhosis: epidemiology andclinical features. Hepatology 2007;45:223–229.
4. Wong F, Bernardi M, Balk R, et al. International Ascites Club.Sepsis in cirrhosis: report on the 7th meeting of the internationalascites club. Gut 2005;54:718–725.
5. Christou L, Pappas G, Falagas ME. Bacterial infection-relatedmorbidity and mortality in cirrhosis. Am J Gastroenterol 2007;102:1510–1517.
6. Fernández J, Navasa M, Gómez J, et al. Bacterial Infection incirrhosis: epidemiological changes with invasive procedures andNorfloxacin prophylaxis. Hepatology 2002;35:140–148.
7. Fernández J, Ruiz del Arbol L, Gómez C, et al. Norfloxacin vsceftriaxone in the prophylaxis of infections in patients with ad-vanced cirrhosis and haemorrhage. Gastroenterology 2006;131:1049–1456.
8. Venditti M, Falcone M, Corrao S, et al. Study Group of the ItalianSociety of Internal Medicine. Outcomes of patients hospitalizedwith community-acquired, health care-associated, and hospital-acquired pneumonia. Ann Intern Med 2009;150:19–26.
9. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Cam-paign: international guidelines for management of severe sepsisand septic shock: 2008. Crit Care Med 2008;36:296–327.
0. Pugh RN, Murray-Lyon IM, Dawson JL, et al. Transection of theoesophagus for bleeding oesophageal varices. Br J Surg 1973;60:646–649.
1. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predictsurvival in patients with end-stage liver disease. Hepatology2001;33:464–470.
Without Infections and With and Without Sepsis During
P valuePatients withsepsis (31)
Patients withoutsepsis (119) P value
�.001 5 (16) 2 (1.6) �.001.05 4 (13) 2 (1.6) .004.0015 11 (35) 23 (19) .05.08 23 (74) 61 (51) .02.2 5 (16) 8 (6.7) .2
�.001 13 (42) 8 (6.7) �.001�.001 6 (19) 0 �.001�.001 12 (38) 6 (5) �.001
and
0)
2. Salerno F, Gerbes A, Ginès P, et al. Diagnosis, prevention and

1
1
1
1
1
1
1
2
2
2
2
2
2
2
R
GUe
A
E
C
F
November 2010 BACTERIAL INFECTIONS IN CIRRHOTIC PATIENTS 985
treatment of hepatorenal syndrome in cirrhosis. Gut2007;56:1310–1318.
3. Merli M, Riggio O, Dally L. Policentrica Italiana Nutrizione Cirrosi.Does malnutrition affect survival in cirrhosis? Hepatology 1996;23:1041–1046.
4. Garcia-Tsao G, Lim JK. Members of Veterans Affairs Hepatitis CResource Center Program. Management and treatment of pa-tients with cirrhosis and portal hypertension. Am J Gastroenterol2009;104:1802–1829.
5. Runyon BA. Management of adult patients with ascites due tocirrhosis: an update. Hepatology 2009;49:2087–2107.
6. Garcia-Tsao G, Sanyal AJ, Grace ND, et al. Prevention and man-agement of gastroesophageal varices and variceal hemorrhage incirrhosis. Hepatology 2007;43:922–933.
7. Conn HO, Leevy CM, Vlahcevic ZR, et al. Comparison of lactuloseand neomycin in the treatment of chronic portal systemic enceph-alopathy. A double blind controlled trial. Gastroenterology 1977;72:573–583.
8. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance defi-nition of health care-associated infection and criteria for specifictypes of infections in the acute care setting. Am J Infect Control2008;36:309–332.
9. Falagas ME, Koletsi PK, Bliziotis IA. The diversity of definitions ofmultidrug-resistant (MDR) and pandrug-resistant (PDR) Acineto-bacter baumannii and Pseudomonas aeruginosa. J Med Micro-biol 2006;55:1619–1629.
0. Rupp ME, Fey PD. Extended spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae: considerations for diagnosis, pre-vention and drug treatment. Drugs 2003;63:353–365.
1. Mazzaferro V, Regalio E, Doci R, et al. Liver transplantation forthe treatment of small hepatocellular carcinomas in patients with
cirrhosis. N Engl J Med 1996;334:693–699. v2. Friedman ND, Kaye KS, Stout JE, et al. Health care associatedbloodstream infections in adults: a reason to change the ac-cepted definition of community-acquired infections. Ann InternMed 2002;137:791–797.
3. Sam J, Nguyen GC. Protein-calorie malnutrition as a prognosticindicator of mortality among patients hospitalized with cirrhosisand portal hypertension. Liver Int 2009;29:1396–1402.
4. Merli M, Giusto M, Gentili F, et al. Nutritional status: its influenceon the outcome of patients undergoing liver transplantation. LiverInternational 2010;30:208–214.
5. Trautwein C, Boker K, Manns MP. Hepatocyte and immune sys-tem: acute phase reaction as a contribution to early defencemechanism. Gut 1994;35:1163–1166.
6. Gabay C, Kushner I. Acute-phase proteins and other systemicresponses to inflammation. N Engl J Med 1999;340:448–454.
eprint requestsAddress requests for reprints to: Professor Manuela Merli, MD,
astroenterologia II, Dipartimento di Medicina Clinica, “Sapienza”niversità di Roma, Viale dell’Università 37, 00185 Rome, Italy.-mail: [email protected]; fax: (39) 064453319.
cknowledgmentsThe authors thank Mrs Maria Teresa Barbieri for assistance with the
nglish revision.
onflicts of interestThe authors disclose no conflicts.
undingSupported by a research grant C26FO9BMAN from �Sapienza� Uni-
ersity of Rome.

Stueshowed a higher rate of mortality (P � .0001).
November 2010 BACTERIAL INFECTIONS IN CIRRHOTIC PATIENTS 985.e1
upplementary Figure 1. Survival in 150 hospitalized cirrhotic pa-ients according to the presence of infection. Curves were estimatedsing the Kaplan–Meier method. A period of 6-months follow-up wasxamined. Patients with diagnosis of infection at the time of enrollment