Embed Size (px)
DESCRIPTION
hello
Citation preview
ADVANCED RENAL TECHNOLOGIES Product Manual
CITRASATE®
ART

A D V A N C E D R E N A L T E C N O L O G I E S
Citrasate ®
© Advanced Renal Technologies 40 lake Bellevue, Suite 100
Bellevue, WA 98005


Table of Contents
C H A P T E R 1 Citrasate®
Innovative dialysis solution
Introduction 2
Citric Acid 3
Chemical composition 5
C H A P T E R 2 Citrasate®
Superior Therapeutic performance
Hemodialysis delivered dose 6
Citrasate® and dose adequacy 7
Citrasate® and metabolic acidosis 9
Citrasate® and calcium 10
C H A P T E R 3 Citrasate®
Local anticoagulant
Adequate anticoagulant 12
Citrasate® (Dialzate with anticoagulant) 13 Citrasate® and dialyzer Biocompatibility 15
C H A P T E R 4 Citrasate®
Dialyzer reusability
Citrasate® improves the reusability 18
C H A P T E R 5 Packages
Packages 20
C H A P T E R 6 Reference
Reference 22


2 C I T R A S A T E ®
Introduction
Citrasate® innovative dialysis solution
or many years, the composition of the dialysate used in Haemodialysis remained stable, until a decade ago when bicarbonate was substituted for acetate. Recently, Advanced Renal Technologies (ART) introduced a new chemical formulation of dialysate that can improve dialysis
treatment. Citrasate® is the first new dialysate formulation in decades, and DRYalysate® is the dry version of this new formulation. The new formulation in Citrasate® contains the natural substance citric acid in place of acetic acid, which all other dialysates have. Citric acid is a physiological acid that is rapidly metabolized in muscle, liver and kidney. It is important as an intermediate in the citric acid cycle and therefore occurs in the metabolism of almost all living cells. Citric acid also is a well known anticoagulant it has a long and safe history of use in medicine, most notably as an anticoagulant used in the collection and storage of blood for transfusion.
Chapter
1
F
3 C I T R A S A T E ®
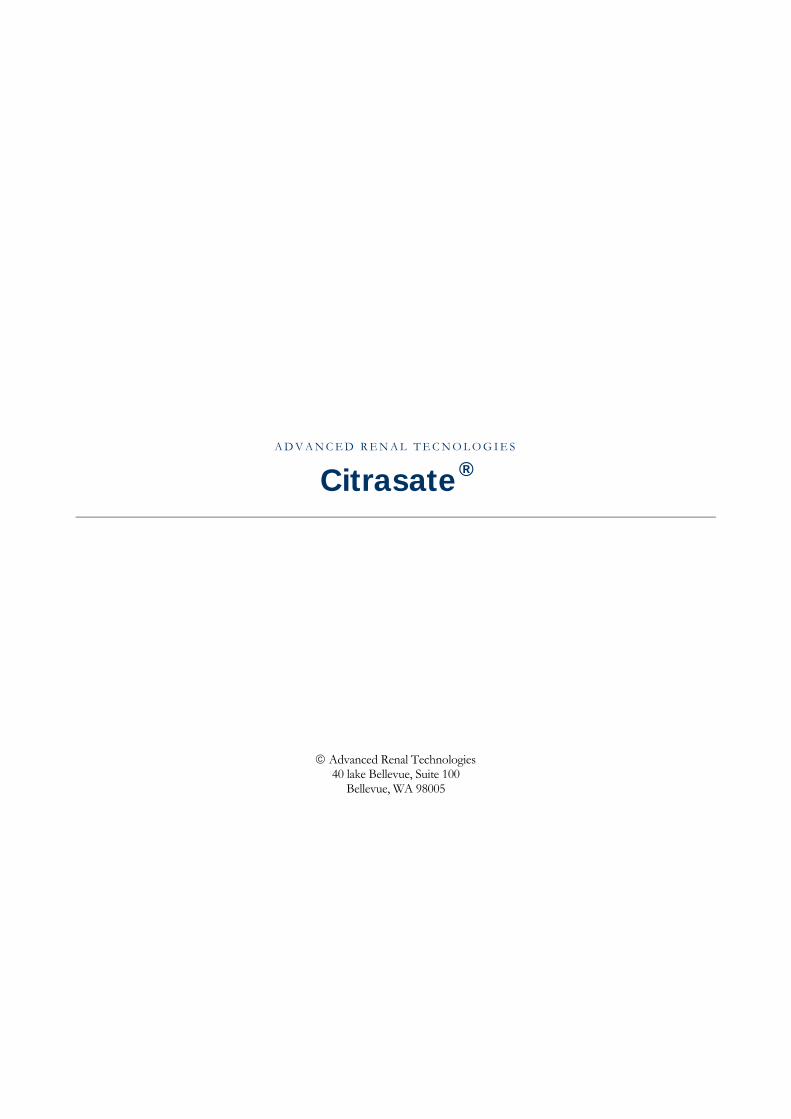
Citric Acid Citric acid is a physiological acid that is rapidly metabolized in muscle, liver and kidney. It is important as an intermediate in the citric acid cycle and therefore occurs in the metabolism of almost all living things. The citric acid cycle (also known as the tricarboxylic acid cycle, the TCA cycle, or the Krebs cycle) is a series of chemical reactions of central importance in all living cells. Citric acid cycle is part of a metabolic pathway involved in the chemical conversion of carbohydrates, fats and proteins into carbon dioxide and water to generate a form of usable energy
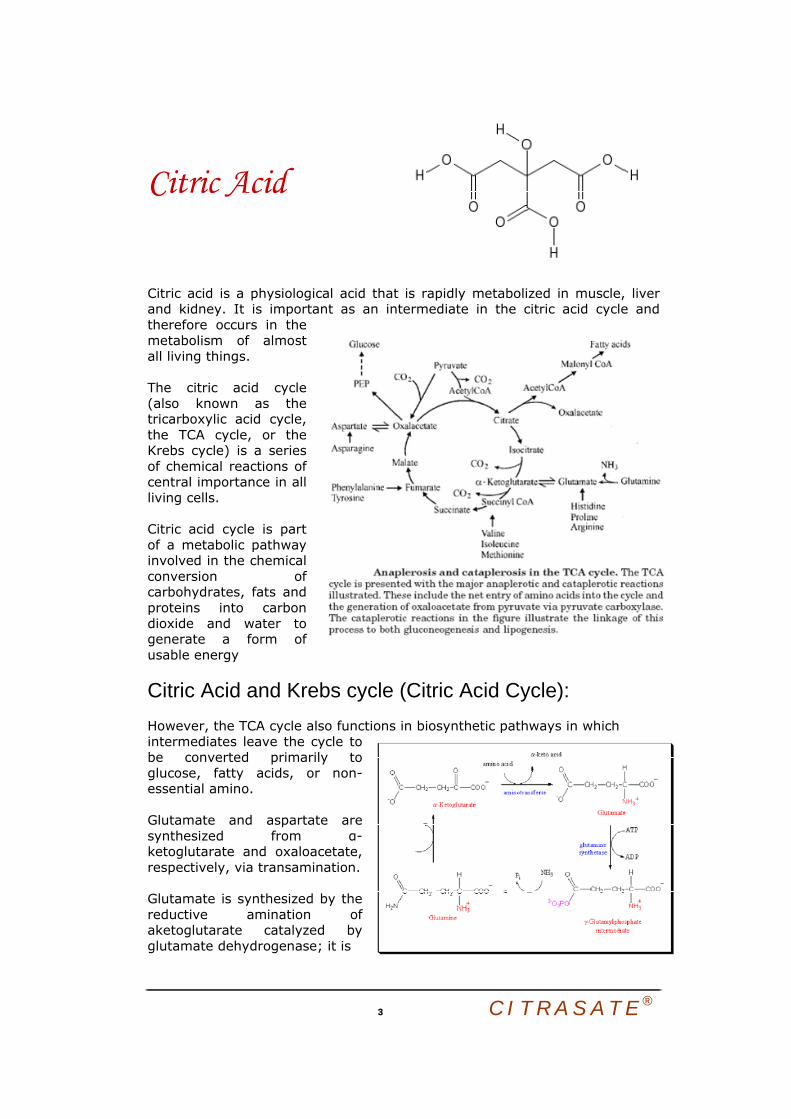
Citric Acid and Krebs cycle (Citric Acid Cycle): However, the TCA cycle also functions in biosynthetic pathways in which intermediates leave the cycle to be converted primarily to glucose, fatty acids, or non-essential amino. Glutamate and aspartate are synthesized from α-ketoglutarate and oxaloacetate, respectively, via transamination. Glutamate is synthesized by the reductive amination of aketoglutarate catalyzed by glutamate dehydrogenase; it is

4 C I T R A S A T E ®
thus a nitrogen-fixing reaction. In addition, glutamate arises by aminotransferase reactions, with the amino nitrogen being donated by a number of different amino acids. Thus, glutamate is a general collector of amino nitrogen. Aspartate is formed in a transamintion reaction catalyzed by aspartate transaminase, AST. This reaction uses the aspartate a-keto acid analog, oxaloacetate, and glutamate as the amino donor. Aspartate can also be formed by deamination of asparagine catalyzed by asparaginase. Asparagine synthetase and glutamine synthetase, catalyze the production of asparagine and glutamine from their respective a-amino acids. Glutamine is produced from glutamate by the direct incorporation of ammonia; and this can be considered another nitrogen fixing reaction. Asparagine, however, is formed by an amidotransferase reaction. Aminotransferase reactions are readily reversible. The direction of any individual transamination depends principally on the concentration ratio of reactants and products. Systemic acid-base changes cause striking changes in citrate clearance and metabolism. Recent evidence suggests that the effects of acid-base changes are mediated by alteration in the pH gradient across the inner mitochondrial membrane. Metabolic alkalosis causes cytoplasmic pH and bicarbonate to increase, resulting in a decrease in the mitochondrial pH gradient. This change inhibits the tricarboxylate carrier, slowing entry of citrate into the mitochondrial matrix compartment. The level of citrate in the cytoplasm increases, tubular and peritubular citrate uptake are reduced, and citrate clearance increases. Opposite changes occur in acidosis. Change in the mitochondrial pH gradient provides a sensitive mechanism for regulating renal substrate metabolism. The renal clearance of citrate is greatly increased during metabolic Alkalosis. All of the citrate filtered through the glomerulus is reabsorbed in the nephron with only small quantities escaping into the urine. In the presence of metabolic alkalosis the tubular reabsorption of citrate is inhibited, and the excretion of citrate increases manyfold with little concomitant change in the plasma level. The physiologic characteristics of this phenomenon have been described in numerous reports, but the cellular mechanism responsible for it has not been defined. Citrate Normal anticoagulant: Citrate is a well known anticoagulant that functions by binding serum calcium thereby reducing the calcium available to participate in the blood’s clotting cascade. It has a long and safe history of use in medicine, most notably as an anticoagulant used in the collection and storage of blood for transfusion.

5 C I T R A S A T E ®
Chemical composition Citrasate®, a new acid concentrate for bicarbonate dialysis, in which the primary acidifying agent is Citric acid instead of acetic acid.
Citrasate® Regular Dialysate
Sodium (mEg/L) 137.3 137
Chloride (mEg/L) 103.25 – 106.75 103.25 – 106.75
Calcium (mEg/L) 2.5 OR 3.0 2.5 OR 3.0
Magnesium (mEg/L) 0.75 0.75
Potassium (mEg/L) 0 – 3 0 – 3
Dextrose (g/L) 2 2
Bicarbonate (mEg/L) 37 37
Acetate (mEg/L) 0.3 4
Citrate (mEg/L) 2.4 None
The indications for use of Citrasate®:
• Citrasate® is suitable for all Haemodialysis patients: o Aiming to achieve adequate dialysis dose, or have chronic
acidosis maintaining the normal body electrolyte level. o patients with a risk of bleeding from the use of systemic anti-
coagulation (Heparin) (i.e., ICU and Post-operative patient) ; o When it’s contraindicated to use Heparin (I.e., Patient with
heparin-induced thrombocytopenia ”HIT”), o Patient with an antibody to (intolerance to) Heparin whose
dialyzers clot despite large amounts of heparin; o Patient achieves limited dialyzer reuse due to extensive clotting
within the dialyzer during dialysis; increasing the effective surface area and improving the dialyzer biocompatibility.
6 C I T R A S A T E ®
Citrasate® Superior therapeutic performance
The dose of dialysis in terms of urea clearance is marginal in many Hemodialysis patients, and metabolic acidosis as determined by the pre-dialysis serum HCO3 level is common. CITRASATE® rather than acetic acid as acidifying agent provides superior performance properties.1
Hemodialysis Delivered dose.
umerous studies outcomes have demonstrated a correlation between the delivered dose of Hemodialysis and the patient's mortality and morbidity.2,3. Evidences have shown that mortality among ESRD patients is lower when sufficient Hemodialysis treatments are
provided. Clinical signs and symptoms alone are not reliable indicators of Hemodialysis adequacy.4,5
To see whether dialysis is removing enough urea, the clinic should periodically—normally once a month—test a patient's blood to measure dialysis adequacy. Blood is sampled at the start of dialysis and at the end. The levels of urea in the two blood samples are then compared. Two methods are generally used to assess dialysis adequacy, URR and Kt/V.
Chapter
2
N
7 C I T R A S A T E ®
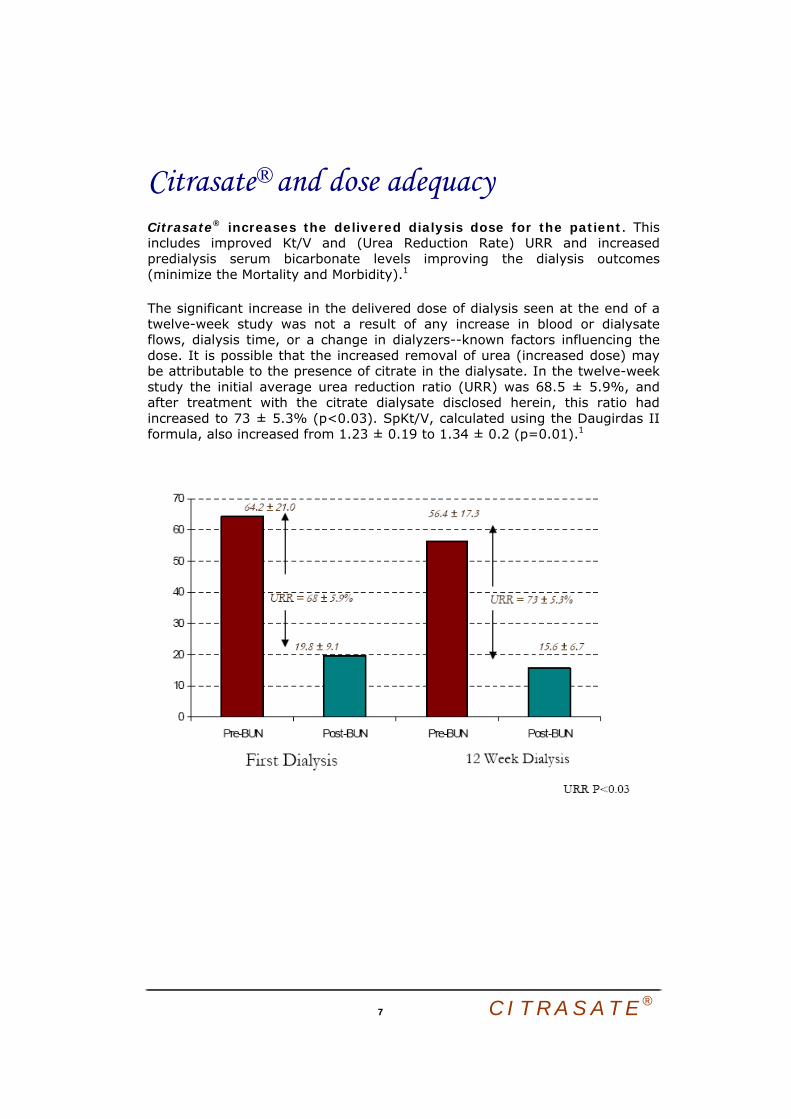
Citrasate® and dose adequacy Citrasate® increases the delivered dialysis dose for the patient. This includes improved Kt/V and (Urea Reduction Rate) URR and increased predialysis serum bicarbonate levels improving the dialysis outcomes (minimize the Mortality and Morbidity).1
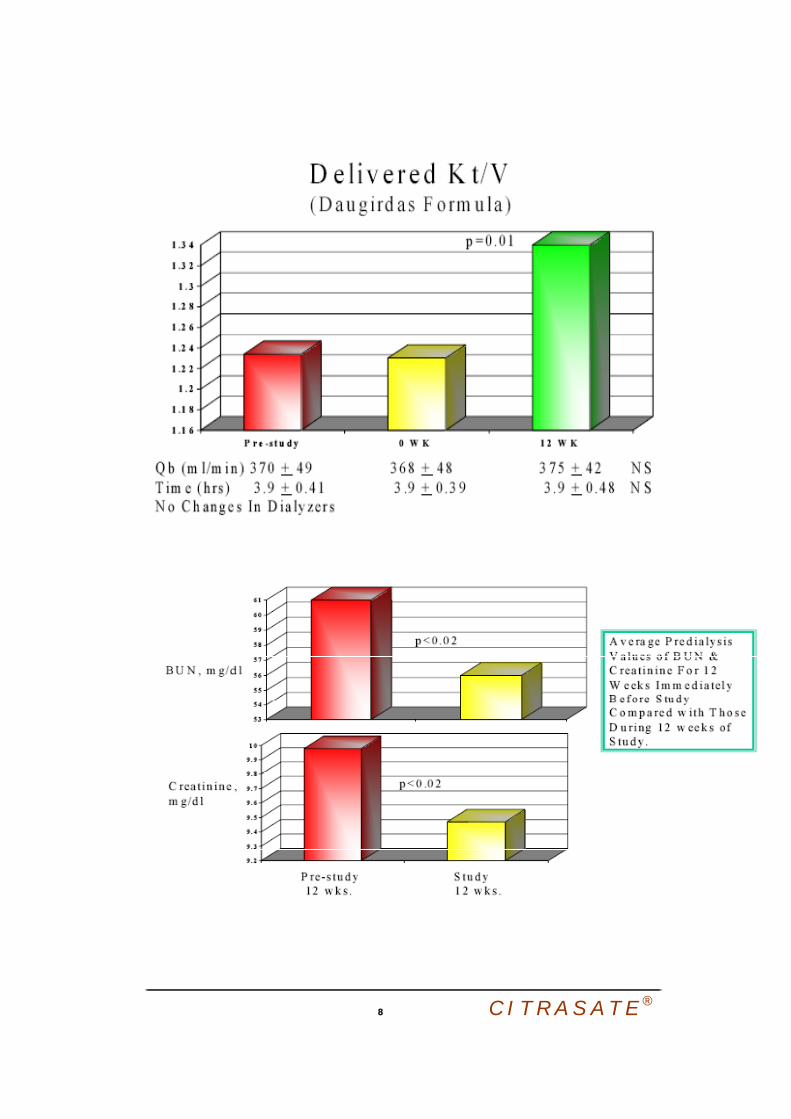
The significant increase in the delivered dose of dialysis seen at the end of a twelve-week study was not a result of any increase in blood or dialysate flows, dialysis time, or a change in dialyzers--known factors influencing the dose. It is possible that the increased removal of urea (increased dose) may be attributable to the presence of citrate in the dialysate. In the twelve-week study the initial average urea reduction ratio (URR) was 68.5 ± 5.9%, and after treatment with the citrate dialysate disclosed herein, this ratio had increased to 73 ± 5.3% (p<0.03). SpKt/V, calculated using the Daugirdas II formula, also increased from 1.23 ± 0.19 to 1.34 ± 0.2 (p=0.01).1
8 C I T R A S A T E ®

9 C I T R A S A T E ®
Citrasate® and Metabolic Acidosis
Persistent metabolic acidosis in dialysis patients has been associated with increased protein catabolism7, increased turnover of ß2 microglobulin8, bone metabolism problems9 and abnormal muscle functions10. Correction of metabolic acidosis has been attempted either by increasing dialysate bicarbonate concentration11 or by prescribing oral bicarbonate12, but both approaches have associated practical and clinical problems. Citrate is metabolized in liver and muscle to produce bicarbonate, and patients getting massive blood transfusions are known to develop alkalosis as a result of the increased citrate load13.
Thus, citrate metabolism alone may explain the increase in serum bicarbonate level. However, increased intradialytic bicarbonate transfer from the dialysate to the blood might also be a factor as the result of a possible effect of citric acid on the dialyzer membrane. The increase in pre-dialysis serum HCO3 may be attributed to the increase of the delivered dose and the production of HCO3
from citric acid.1
Pre-dialysis mean serum HCO3 level mEq/L
1 0 C I T R A S A T E ®
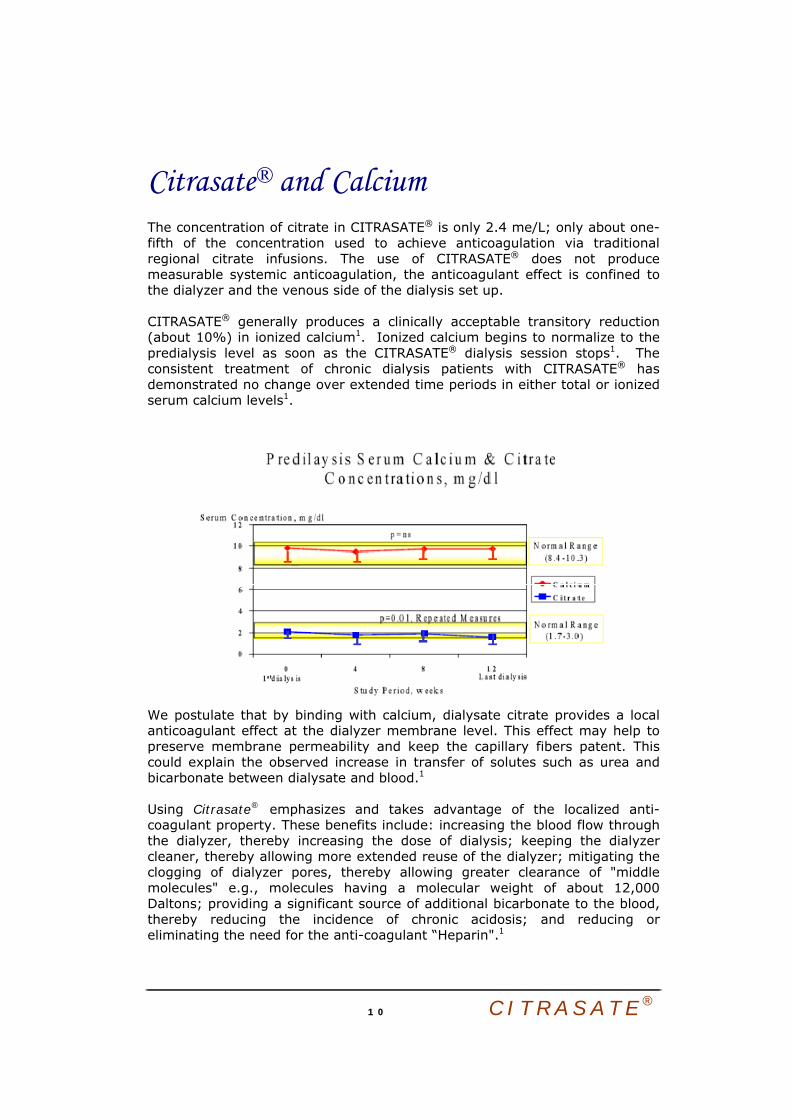
Citrasate® and Calcium The concentration of citrate in CITRASATE® is only 2.4 me/L; only about one-fifth of the concentration used to achieve anticoagulation via traditional regional citrate infusions. The use of CITRASATE® does not produce measurable systemic anticoagulation, the anticoagulant effect is confined to the dialyzer and the venous side of the dialysis set up. CITRASATE® generally produces a clinically acceptable transitory reduction (about 10%) in ionized calcium1. Ionized calcium begins to normalize to the predialysis level as soon as the CITRASATE® dialysis session stops1. The consistent treatment of chronic dialysis patients with CITRASATE® has demonstrated no change over extended time periods in either total or ionized serum calcium levels1.
We postulate that by binding with calcium, dialysate citrate provides a local anticoagulant effect at the dialyzer membrane level. This effect may help to preserve membrane permeability and keep the capillary fibers patent. This could explain the observed increase in transfer of solutes such as urea and bicarbonate between dialysate and blood.1 Using Citrasate® emphasizes and takes advantage of the localized anti-coagulant property. These benefits include: increasing the blood flow through the dialyzer, thereby increasing the dose of dialysis; keeping the dialyzer cleaner, thereby allowing more extended reuse of the dialyzer; mitigating the clogging of dialyzer pores, thereby allowing greater clearance of "middle molecules" e.g., molecules having a molecular weight of about 12,000 Daltons; providing a significant source of additional bicarbonate to the blood, thereby reducing the incidence of chronic acidosis; and reducing or eliminating the need for the anti-coagulant “Heparin".1

1 1 C I T R A S A T E ®

1 2 C I T R A S A T E ®
Citrasate® Local anticoagulant
Adequate anticoagulant dequate anticoagulation is a precondition to prevent extracorporeal blood clotting and to improve biocompatibility during Hemodialysis14.
Heparin is widely used for prevention and treatment of thromboembolic disorders and to prevent clotting within the extracorporeal circuit during Hemodialysis. However, the systemic nature of heparin anticoagulation increases the risk of bleeding complications and, therefore, cannot be safely used in post-surgical patients or in those who are actively bleeding. Some acutely ill patients develop severe thrombocytopenia with the use of heparin. In these patient groups, if Hemodialysis is needed, heparin cannot be safely used, and successful completion of the Hemodialysis procedure can often become quite challenging, since without anticoagulation the system frequently clots. In recent years, Citrate has gained more popularity as an anticoagulant during Hemodialysis especially in patients with increased bleeding risks, because of the advantages of an efficient anticoagulation that is exclusively confined to the extracorporeal circulation and also improvement of the biocompatibility by inhibition of activation of blood cells.15
Chapter
3
A
1 3 C I T R A S A T E ®
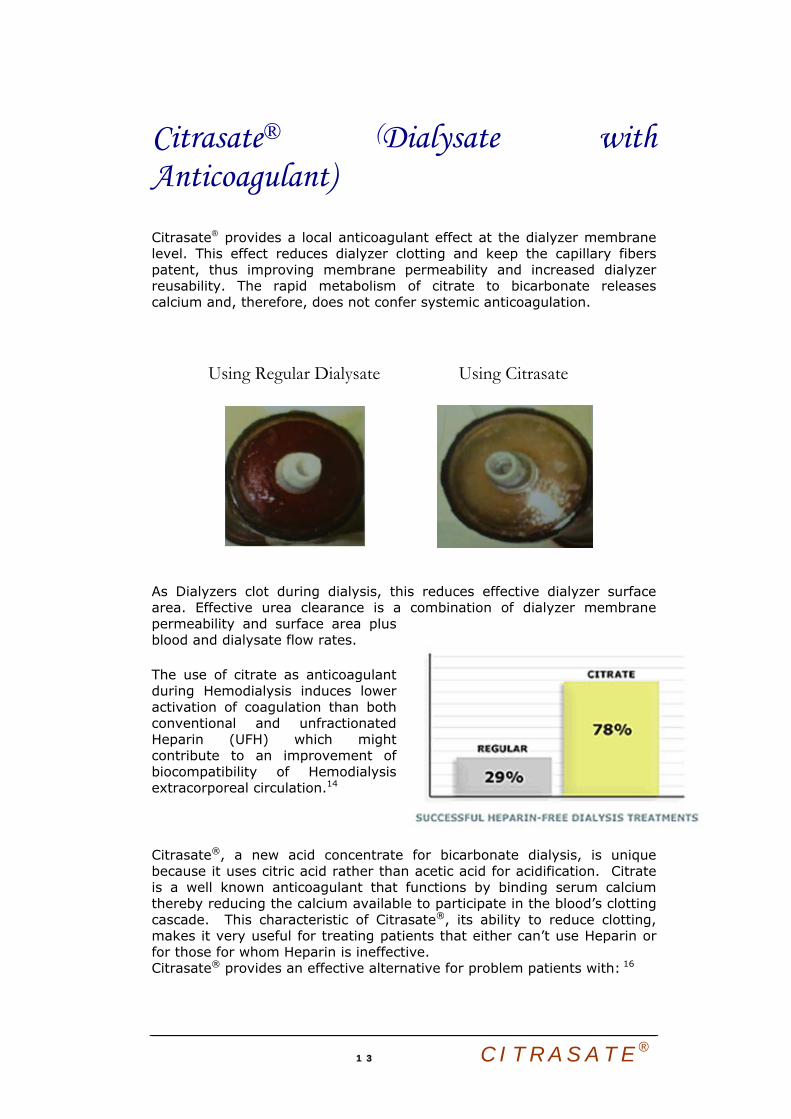
Citrasate® (Dialysate with Anticoagulant) Citrasate® provides a local anticoagulant effect at the dialyzer membrane level. This effect reduces dialyzer clotting and keep the capillary fibers patent, thus improving membrane permeability and increased dialyzer reusability. The rapid metabolism of citrate to bicarbonate releases calcium and, therefore, does not confer systemic anticoagulation.
Using Regular Dialysate
Using Citrasate
As Dialyzers clot during dialysis, this reduces effective dialyzer surface area. Effective urea clearance is a combination of dialyzer membrane permeability and surface area plus blood and dialysate flow rates.
The use of citrate as anticoagulant during Hemodialysis induces lower activation of coagulation than both conventional and unfractionated Heparin (UFH) which might contribute to an improvement of biocompatibility of Hemodialysis extracorporeal circulation.14
Citrasate®, a new acid concentrate for bicarbonate dialysis, is unique because it uses citric acid rather than acetic acid for acidification. Citrate is a well known anticoagulant that functions by binding serum calcium thereby reducing the calcium available to participate in the blood’s clotting cascade. This characteristic of Citrasate®, its ability to reduce clotting, makes it very useful for treating patients that either can’t use Heparin or for those for whom Heparin is ineffective. Citrasate® provides an effective alternative for problem patients with: 16

1 4 C I T R A S A T E ®
• a risk of bleeding from the use of systemic anti-coagulation (Heparin) for example ICU and post operative patient;
• When it’s contraindicated to use Heparin (I.e., Patient with heparin-induced thrombocytopenia ”HIT”),
• Patient with an antibody to Heparin (intolerance) whose dialyzers clot despite large amounts of heparin;
CITRASATE® retaining the patient's ability to clot blood
Citrasate® is particularly useful in instances where patients should be heparin-free during dialysis. For example, post-operative patients may undergo acute kidney failure due to the kidney's response to the anesthesia, and thereafter need dialysis treatment until kidney recovery occurs. Heparin or other anti-coagulant should not be delivered systemically to these patients because retaining the patient's ability to clot blood is an important part of the healing process. With traditional dialysate, undesirable blood clotting will occur within the dialyzer, unless the patient receives some anti-coagulant. However, with the Citrasate®, a patient with acute kidney failure can undergo successful dialysis without systemic administration of anti-coagulant. A patient with acute kidney failure may also experience more rapid recovery of kidney function upon exposure to Citrasate®, in comparison to conventional dialysate, because Citrasate® has fewer tendencies to activate complement formation, where complement formation tends to slow down kidney recovery.1
Citrasate® Minimize the use of Systemic Anti-Coagulant
Citrasate® reduces or eliminates the need for the anti-coagulant “Heparin" without adverse effects. 1

1 5 C I T R A S A T E ®
Citrasate® and Dialyzer Biocompatibility The biocompatibility of the dialyzer membranes and whole blood is of major concern. Both proteins and cells adhere to the membrane surface. This contact, in turn, causes a number of deleterious responses, which resemble those of assaults to the patient's immune system in the form of severe allergic reactions. The responses are numerous and in some instances life threatening. They include: Platelet adhesion, agglomeration & damage, Thrombosis and erythrocyte adhesion. Complement activation (C3/C.5) the clinical manifestations are also numerous and in some cases lead to morbidity and mortalities.
Coagulation activation presents one of the main determinants of biocompatibility. Coagulation activation is obviously one of the most important barriers to adequacy of dialysis delivery. Recently, Shegal et al analyzed patient-related and technical factors determining dialysis delivery in 1836 treatments provided to 721 randomly selected patients on regular Hemodialysis therapy17. Their study concluded that beside dialysis prescription problems with vascular access and clotting are the most important limits to dialysis adequacy.

1 6 C I T R A S A T E ®
Citrasate® inhibit blood coagulation locally at the dialyzer membrane surface resulting in better dialyzer clearance, As Dialyzers clot during dialysis, this reduces effective dialyzer surface area. Effective urea clearance is a combination of dialyzer membrane permeability and surface area plus blood and dialysate flow rates and improve the biocompatibility. Clotting not only reduces the efficiency of dialysis therapy by mechanical obstruction of the dialysis membrane, but causes activation of other cascade systems activation of cellular elements besides platelets and especially polymorphonuclear neutrophils, the release of vasoactive hormones, such as thromboxane, of mediators such as tumor necrosis factor α and enzymes such as elastase. 14

1 7 C I T R A S A T E ®
1 8 C I T R A S A T E ®
Citrasate® Dialyzer reusability
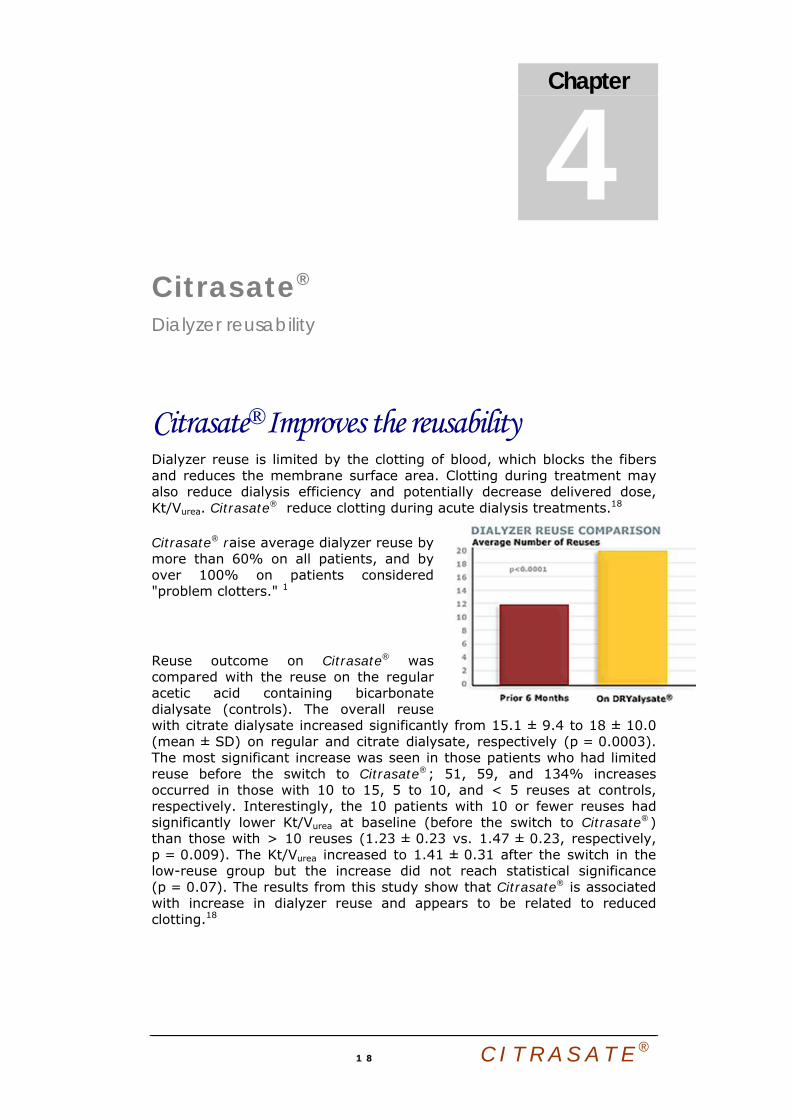
Citrasate® Improves the reusability Dialyzer reuse is limited by the clotting of blood, which blocks the fibers and reduces the membrane surface area. Clotting during treatment may also reduce dialysis efficiency and potentially decrease delivered dose, Kt/Vurea. Citrasate® reduce clotting during acute dialysis treatments.18
Citrasate® raise average dialyzer reuse by more than 60% on all patients, and by over 100% on patients considered "problem clotters." 1
Reuse outcome on Citrasate® was compared with the reuse on the regular acetic acid containing bicarbonate dialysate (controls). The overall reuse with citrate dialysate increased significantly from 15.1 ± 9.4 to 18 ± 10.0 (mean ± SD) on regular and citrate dialysate, respectively (p = 0.0003). The most significant increase was seen in those patients who had limited reuse before the switch to Citrasate®; 51, 59, and 134% increases occurred in those with 10 to 15, 5 to 10, and < 5 reuses at controls, respectively. Interestingly, the 10 patients with 10 or fewer reuses had significantly lower Kt/Vurea at baseline (before the switch to Citrasate®) than those with > 10 reuses (1.23 ± 0.23 vs. 1.47 ± 0.23, respectively, p = 0.009). The Kt/Vurea increased to 1.41 ± 0.31 after the switch in the low-reuse group but the increase did not reach statistical significance (p = 0.07). The results from this study show that Citrasate® is associated with increase in dialyzer reuse and appears to be related to reduced clotting.18
Chapter
4

1 9 C I T R A S A T E ®

2 0 C I T R A S A T E ®
Citrasate® Packages Citrasate® • Citrasate® is ready to use liquid concentrate in convenient gallon jugs. • Package information: 4.5 - 5 Liter bottle. • The following concentrations are listed in mEq/L, except for Dextrose which is in mg/dl, and represent the concentration in dialysate after proper dilution before including the ionic contribution of the bicarbonate concentrate.
Concentration Sodium Chloride Calcium Magnesium Potassium Dextrose Acetate Citrate 36.83X 81.3 84.5 2.5 1 0 200 0.3 2.4 36.83X 81.3 85.5 2.5 1 1 200 0.3 2.4 36.83X 81.3 86.5 2.5 1 2 200 0.3 2.4 36.83X 81.3 85 3 1 0 200 0.3 2.4 36.83X 81.3 86 3 1 1 200 0.3 2.4 36.83X 81.3 87 3 1 2 200 0.3 2.4 36.83X 81.3 85.5 3.5 1 0 200 0.3 2.4 45X 100.3 103.5 2.5 1 0 200 0.3 2.4 45X 100.3 104.5 2.5 1 1 200 0.3 2.4 45X 100.3 105.5 2.5 1 2 200 0.3 2.4 45X 100.3 104 3 1 0 200 0.3 2.4 45X 100.3 105 3 1 1 200 0.3 2.4 45X 100.3 106 3 1 2 200 0.3 2.4 45X 100.3 104.5 3.5 1 0 200 0.3 2.4 35X 100.3 103.5 2.5 1 0 200 0.3 2.4 35X 100.3 104.5 2.5 1 1 200 0.3 2.4 35X 100.3 105.5 2.5 1 2 200 0.3 2.4 35X 100.3 104 3 1 0 200 0.3 2.4 35X 100.3 105 3 1 1 200 0.3 2.4 35X 100.3 106 3 1 2 200 0.3 2.4 35X 100.3 104.5 3.5 1 0 200 0.3 2.4
Chapter
5

2 1 C I T R A S A T E ®
DRYalysate® • A dry powdered acid concentrate that needs to be mixed with water prior to use. • Each box of DRYalysate® will reconstitute into fifty (50) liters of acid concentrate. • The following concentrations are listed in mEq/L, except for Dextrose which is in mg/dl, and represent the concentration in dialysate after proper dilution before including the ionic contribution of the bicarbonate concentrate.
Concentration Sodium Chloride Calcium Magnesium Potassium Dextrose Acetate Citrate 45X 100.3 103.5 2.5 1 0 200 0.3 2.445X 100.3 104.5 2.5 1 1 200 0.3 2.445X 100.3 105.5 2.5 1 2 200 0.3 2.445X 100.3 104 3 1 0 200 0.3 2.445X 100.3 105 3 1 1 200 0.3 2.445X 100.3 106 3 1 2 200 0.3 2.445X 100.3 104.5 3.5 1 0 200 0.3 2.436.83X 81.3 84.5 2.5 1 0 200 0.3 2.4

Reference
1. A Ahmad S, Callan R, Cole JJ, Blagg CR. Dialysate made from dry chemicals using citric acid increases dialysis dose. Am J Kidney Dis 2000; 35:493-499
2. Owen WF, Lew NL, Liu Y, Lowrie EG, Lazarus JM: The urea reduction ratio and serum albumin concentration as predictors of mortality in patients undergoing Hemodialysis . N Engl J Med 329:1001-1006, 1993
3. Owen WF, Chertow G, Lazarus JM, and Lowrie EG: The dose of Hemodialysis: Mortality responses by race and gender. JAMA 280:1-6, 1998
4. Delmez JA, Windus DW, St. Louis Nephrology Study Group: Hemodialysis prescription and delivery in a metropolitan community. Kidney Int 41:1023-1028, 1992
5. Lindsay RM, Heidenheim AP, Spanner E, Baird J, Simpson K, Allison ME: Urea monitoring during dialysis: the wave of the future. A tale of two cities. ASAIO Trans 37:49-53, 1991
6. Hofbauer R, Moser D, Frass M, Oberbauer R, Kaye AD et al. Effect of anticoagulation on blood membrane interactions during Hemodialysis . Kidney Int (Oct) 56:1578-1583 1999
7. Reaich et al., Am. J. Physiol. 265:E230-E235 (1993) 8. Sonikian et al., J. Am. Soc. Nephrol. 7:350-356 (1996) 9. Lin et al., ASAIO J. 40:M440-M444 (1994) 10. Guest et al., J. Am. Soc. Nephrol. 8:236A (1997) 11. Ahmad et al., Trans. Am. Soc. Artif Intem. Organs 26:318-321 (1980) 12. Brady and Hasbargen, Am. J. Kid. Dis. 31:35-40 (1998) 13. Dzik and Kirkley, Trans. Med. Rev. 2:76-94 (1988) 14. Hofbauer R, Moser D, Frass M, Oberbauer R, Kaye AD et al. Effect of anticoagulation on blood membrane
interactions during Hemodialysis. Kidney Int (Oct) 56:1578-1583 1999 15. BOEHLLER J. SCHOLLMYER P, DRESSL B, DOBOS G, HOERL WH: Reduction of granulocyte
activation during Hemodialysis with regional citrate anticoagulation: Dissociation of complement activation and neutropenia from neutrophil degranulation. J Am Soc Nephrol 7:234-241, 1996
16. Annie Tu, MS, ARNP, CNN; Ahmad S.,: Heparin-free hemodialysis with citrate-containing dialysate in intensive care patients. Dialysis & Trans. V.29, No. 10 Oct. 2000
17. SEHGAL AR, SNOW RJ, SINGER ME, AMINI SB, DEOREO PB, SILVER MR, CEBUL RD: Barriers to adequate delivery of Hemodialysis. Am J Kidney Dis 31:593-601, 1998
18. Ahmad S, Callan R, Cole JJ, Blagg CR. Increased dialyzer reuse with citrate dialysate. Hemodialysis International V. 9 Issue 3 Page 264 - July 2005 doi:10.1
Chapter
6



A D V A N C E D R E N A L T E C N O L O G I E S
© Advanced Renal Technologies 40 lake Bellevue, Suite 100
Bellevue, WA 98005