Embed Size (px)
DESCRIPTION
Presentation that I created for a Prospect Client.
Citation preview

Presentation for the City of Woodhaven
03.30.2010
Presented By:

Table
• HR Connection 5.0 Presentation • HR Connection 5.0 Overview • What is an HRA? • Zywave Rx Fact Sheet • Perspectives • Legislative Brief—Electronic Disclosures • Legislative Brief—COBRA Answers for Employ‐ers
• Trends Fact Sheet • Agent Call List

INTRODUCTION TO HRCONNECTION® 5.0Rated HR for Human Resourceful.
1

THE PROBLEMS HR & EMPLOYEES FACE
• Employers need to educate and empower employees.
• Employees need benefit information.• Newer, more efficient ways of communicating
benefits and other company information are becoming more prevalent.
2

THE SOLUTION: HRCONNECTION 5.0
• Cornerstone Benefit Plans, Inc. is pleased to bring you the solution to your HR and benefits communication challenges.
• HRconnection – the most powerful HR communication system available – helps you deliver company information in one secure and convenient location that is easily viewed by employees.
• It’s customizable to your needs and preferences.
3

HRCONNECTION HELPS . . .
• EMPLOYERS manage company information in one secure and convenient location that employees can view from any computer with Internet access.
• EMPLOYEES reach a comprehensive resource for company and benefits information, any time of the day or night, by answering most questions that would normally be directed to the HR department.
• HUMAN RESOURCES personnel to function more efficiently and devote more time to strategic issues.
• Obtain up-to-date company and benefits information and useful forms.• Connect to comprehensive human resources information 24 hours a day, 7
days a week.• Access real-time answers to frequently asked questions on important issues
and topics.
4

HRCONNECTION HELPS HUMAN RESOURCES . . .
• Showcase benefit programs to employees and their families• Provide centralized employee self-service, any time, reducing inquiries
directed to HR.
• Reduce printing and distribution costs by providing materials online.• Communicate important company information to all employees in a
consistent, timely, and useful manner.
• Attract and retain valued employees by portraying a high-quality image.• Provides a wealth of information for employees in an easy-to-use and
understandable format, which includes:- Company Information - Human Resources- My Information - Setup and Administration- Vacation Administration
5

HOME PAGE
Each employee will have there own user ID and
Password
Employees & Employers can track Vacation & Sick Day’s
Employer can add Employee Documents. Ex: Expense Reports, Mileage Reimbursement Forms, ect.
If an Employer would like online Election’s made by the Employee, this can be done for a fee.
Here the Employee can access HR document, company bulletin, and Benefit Designs
This site is brought to you by:
6

COMPANY INFORMATION
This site is brought to you by:
This site is brought to you by:
HR will be able to list there Contact Information. HR & Employees will be able to post bulletins, and even
access the employee directory!
7

EMPLOYEE INFORMATION
• Empower employees to manage personal information, including the ability to:– Add, review or update personal information, as well as
emergency contacts, dependents and beneficiaries– Manage time-off requests and view a summary by type– Enter life events– Manage/view benefit elections
8

EMPLOYEE INFORMATION
This site is brought to you by:
This site is brought to you by:
Employees will be able to access there own Personal Information. They will be able to track vacation and sick days, change there address, view there medical plan, and even notify HR if there is a Change in Life Status.
9

COMPANY INFORMATION
• Educate and assist employees on company-specific information, including:– Company history– Holiday and event listings– Departmental contacts– Employee directory– Company bulletin board– Provides employees online access to:
• Job descriptions/postings• Company handbook• Forms• Recommended links• Policies and procedures• Career growth, such as training opportunities
Eliminates the need for distributing bulky and costly employee materials.
10

COMPANY INFORMATION
This site is brought to you by:
This site is brought to you by
Employees can access the following at any time: -Job Postings-Company Handbook-Policies & Procedures
11

BENEFIT PLANS
• Bundles everything employees want to know about their benefit plans in one secure location. Benefits are listed by type, and employees can obtain detailed plan information and benefit summary information, including the ability to:
• View plan design information, including rates & eligibility• Access Summary Plan Descriptions (SPDs)• Compare plan benefits• Obtain plan form• View carrier contact information• Access Frequently Asked Questions
12

BENEFIT PLANS
Employees will be able to view all plansthe company is currently offering.
13

WHY HRCONNECTION?
• Easy navigation and interactive features for employees.• Easy to set up and update; fast and flexible administrative functions.• Delivering targeted employee information is easy with a customizable home
page that includes an at-a-glance design to display:– A welcome message and seasonal announcements.– A list of links to employer-recommended Web resources.– Targeted employee communication campaigns.– A dashboard of upcoming time off and time remaining, personalized to
the user.
14

ADMINISTRATION
• From portal setup, to uploading custom content, to reporting... HRconnection offers administrators the following capabilities:
• Upload employee data• Add, edit or delete benefit plan data• Administer life events• Schedule, approve and track vacation• Publish content• Select portal look, feel and functionality• Create election and employee reports
15

WITH HRCONNECTION . . .
...you educate and empower your employees!– It’s flexible and secure – choose the features that make
sense for you– Provides easy online access to users– Allows HR to do more with less
Get resourceful today with HRconnection 5.0!
16

Cornerstone Benefit Plans, Inc. is pleased to provide City of Woodhaven with HRconnection®, an intuitive HR communication Web portal that helps you deliver company information in one secure and convenient location that is easily viewed by employees. Customizable to your needs and preferences, HRconnection offers you the following flexible features and benefits.
CHOOSE YOUR OPTIONS
Customization of portal look, feel and menu options Self-serve access to company and employee communication information
including City of Woodhaven’s history, handbooks, forms, directories and policies
Online benefits elections including standard and customizable reporting Anytime access to benefit plan information Time-off approval, tracking and reporting capabilities Database of employee information useful for reporting Select portal functionality is optional based on preferences
TRAINING AND SUPPORT
A customized implementation and access to a dedicated Cornerstone Benefit Plans, Inc. Account Manager
On-screen, context-sensitive Help
Online Quick Reference Guides
Visit www.CornerstoneBenefits.com

© Copyright 2009 Zywave, Inc.
CUSTOM PORTAL DESIGN CAPABILITES
Unsurpassed custom design options include the ability to:
Select from three portal design layouts Choose from 12 standard color schemes or easily customize
your own Control images including company logo, name and stock photos Offer different information for different groups of employees Create your own sub-menu items such as a job descriptions
page, custom messages page, etc.
WELCOME
Delivering targeted employee communications is easy with a customizable home page that includes:
Home page welcome message and seasonal announcements Links to employer-recommended Web resources Scheduled employee communication campaigns Quick view of upcoming time off and time remaining,
personalized to the user
COMPANY INFORMATION
Educate and assist employees on company-specific information including:
Employee directory Departmental contacts Holiday and event listing Mission statement and vision Company history

© Copyright 2009 Zywave, Inc.
MY INFORMATION
Empower employees to manage personal information including the ability to:
Add, review or update personal information Manage time-off requests and view a summary by type, such as
vacation, personal or sick day Update life event changes such as beneficiary, dependent or marital
status formation Manage and review benefit elections View both current and future personal elections throughout the year
HUMAN RESOURCES
Helps you eliminate the need for distributing bulky and costly company materials and provide online access to career information to employees including:
Handbooks Forms Directories Policies and procedures Career growth, job posting and training information
BENEFIT PLANS
Bundles everything employees want to know about their benefit plans in one secure location. Benefits are listed by type such as medical, dental, vision, etc. Within each plan type, employees can obtain detailed plan information and benefit summary information including the ability to:
View plan design information including rates and eligibility Access Summary Plan Descriptions Compare plan benefits Obtain plan forms View carrier contact information Access Frequently Asked Questions

© Copyright 2009 Zywave, Inc.
REPORTING OVERVIEW
By capturing employee and plan information in HRconnection 5.0, administrators have the ability to create the following standard reports quickly and easily in a variety of formats.
Election Reports
Benefit Comparison Report - Use this report to compare employee elections at two points in time
Carrier Extract Report - Extract election information for submission to carriers
Census Report - Create an employee census for any line of coverage
Election Changes Report - Extract employee, dependent and plan information for employees whose elections changed due to life events, open enrollment or terminations
Elections Summary - Create an election summary for an individual or all employees (available to employees in the benefit plans section of the portal)
Flexible Spending Report - Extract annual and per pay period FSA contributions by employee
Payroll Extract Report - Pull payroll information
Personal Instruction Sheet - Generate a personal instruction sheet for employees to use during open enrollment and for employees who do not have access to the internet to make their elections
Plan Design Report - Provides detailed information, including rates and benefits, on any of the plan offerings
Premium Report - Reconcile a carrier’s monthly billing
Projected 401(k) Premium Report - Show projected employee 401(k) contributions
Employee Reports
Employee Changes - Monitor changes to information
Employee Username - Useful for distributing portal login information
Employee Vacation Requests - Extract request details
Employee Vacation Totals - Create a new upload for a subsequent time period

ADMINISTRATION
From portal setup to uploading custom content to reporting, HRconnection 5.0 offers administrators the ability to:
Select portal’s look, feel and functionality with a full range of customization options
Upload employee data including dependent information, addresses, phone numbers, emergency contacts, job titles and custom fields from a spreadsheet
Add, edit or delete benefit plan data Administer life events including opening up enrollment
periods for life event changes or for new hires, creating a mass life event for new hires and sending benefit election reminders
Manage all aspects of vacation tracking including the ability to do accruals
Publish portal content according to type such as bulletin board posting, policy, handbook, welcome page message, etc.
Generate reports and manage data imports Update and maintain broker access information Access online, self-serve Help for all “How do I...?”
questions
© Copyright 2009 Zywave, Inc.
HRconnection® 5.0 SYSTEM REQUIREMENTS
• Microsoft® Windows® Vista or Windows® XP operating system
• Microsoft® Internet Explorer® internet browser 6.x or higher, or Mozilla® Firefox® internet browser 3.x or higher
• Dedicated, high-speed internet connection recommended
• Minimum monitor resolution of 1024 x 768
• HRconnection 5.0 is not supported on Apple® Macintosh® computers

What is a Health Reimbursement Arrangement?
A Health Reimbursement Arrangement (HRA) is an employer-funded account that is designed to reimburse employees for qualified medical expenses that are paid for out-of-pocket. There are no annual contribution limits on HRAs; however, the employer usually sets the contribution below the annual deductible. HRAs are often designed to operate with a high deductible health plan (HDHP), thereby reducing premium costs while encouraging employees to spend wisely.
Your employer sets up the HRA, determines the amount of money available in each employee’s HRA for the coverage period, and establishes the types of expenses the funds can be used for. What are the benefits of an HRA?
You may enjoy several benefits from having an HRA:
- Contributions made by your employer can be excluded from your gross income.
- Reimbursements may be tax-free if you pay qualified medical expenses.
- Any unused amounts in the HRA can be carried forward for reimbursements in later years.
Who is eligible for an HRA?
HRAs are employer-established benefit plans. These may be offered in conjunction with other employer-provided health benefits. Employers have complete flexibility to offer various combinations of benefits in designing their plan. You do not have to be covered under any other health care plan to participate. Self-employed persons are not eligible for an HRA. Certain limitations may apply if you are a highly-compensated participant.
An HRA may reimburse medical care expenses only if they are incurred by employees or former employees (including retirees) and their spouses and tax dependents. HRA coverage must be in effect at the time the expense is incurred. Are HRAs really best only for the young and healthy?
No. HRAs and other HDHPs are well-suited for a very wide demographic of people. According to Aetna, the average age of its HRA plan members is 42, the same average age as those who opted for more traditional plans. What is a High Deductible Health Plan (HDHP)?
A HDHP has:
- A higher annual deductible than typical health plans; and
- A maximum limit on the sum of the annual deductible and out-of-pocket medical expenses that you must pay for covered expenses. Out-of-pocket expenses include copayments and other amounts, but do not include premiums.

An HDHP may provide preventive care benefits without a deductible or with a deductible below the minimum annual deductible. Preventive care includes, but is not limited to, the following:
1. Periodic health evaluations.
2. Routine prenatal and well-child care.
3. Child and adult immunizations.
4. Tobacco cessation programs.
5. Obesity weight-loss programs.
6. Screening services (i.e. cancer, heart and vascular diseases, infectious diseases, etc.)
Amount of Contribution
Your employer funds the account, so it costs you nothing out-of-pocket. There is no limit on the amount of money your employer can contribute to the accounts. Additionally, the maximum reimbursement amount credited under the HRA in the future may be increased or decreased by amounts not previously used. The maximum annual contribution is determined by your employer’s plan document. There may also be a cap amount for the HRA. Your employer can choose to fund your HRA with an annual contribution or on a monthly basis. Distributions from an HRA
Distributions from an HRA must be paid to reimburse you for qualified medical expenses you have incurred. The expense must have been incurred on or after the date you are enrolled in the HRA.
Debit cards, credit cards and stored value cards given to you by your employer can be used to reimburse participants in an HRA. If the use of these cards meets certain substantiation methods, you may not have to provide additional information to the HRA.
If any distribution is, or can be, made for other than the reimbursement of qualified medical expenses, any distribution (including reimbursement of qualified medical expenses) made in the current tax year is included in gross income. For example, if an unused reimbursement is payable to you in cash at the end of the year, or upon termination of your employment, any distribution from the HRA is included in your income. This also applies if any unused amount upon your death is payable in cash to your beneficiary or estate, or if the HRA provides an option for you to transfer any unused reimbursement at the end of the year to a retirement plan.
If the plan permits amounts to be paid as medical benefits to a designated beneficiary (other than the employee's spouse or dependents), any distribution from the HRA is included in income. However, if before August 15, 2006, the plan contains such a provision, this rule will not apply until plan years beginning after December 31, 2008.
Reimbursements under an HRA can be made to the following persons:
1. Current and former employees
2. Spouses and dependents of those employees
3. Employees’ covered tax dependents
4. Spouses and dependents of deceased employees

Qualified Medical Expenses
Qualified medical expenses are those specified in the plan that would generally qualify for the medical and dental expenses deduction. Examples include amounts paid for doctors' fees, prescription and non-prescription medicines, and necessary hospital services not paid for by insurance. You can use your HRA funds for deductibles, copayments and coinsurance. Balance in an HRA
Amounts that remain at the end of the year may be carried over to the next year depending on your employer’s plan design. Your employer is not permitted to refund any part of the balance to you. These amounts may never be used for anything but reimbursements for qualified medical expenses. What if I terminate my employment during the Plan Year?
If you cease to be an Eligible Employee (e.g. you die, retire or terminate employment), your participation in the HRA Plan will end unless you elect COBRA continuation coverage. You will be reimbursed for any medical care expenses incurred prior to your termination date, up to your account balance in the HRA, provided that you comply with the plan reimbursement request procedures required under the plan. Any unused portions will be unavailable after termination of employment. The rules regarding COBRA are contained within your Summary Plan Description. Will I have any administrative costs under the HRA plan?
Generally, no. Your employer bears the entire cost of administering the HRA plan while you are an employee. How long will the HRA plan remain in effect?
Although your employer expects to maintain the HRA plan indefinitely, it has the right to terminate the HRA plan at any time. Your employer also has the right to amend the HRA plan at any time and in any manner that it deems reasonable, in its sole discretion. Are my benefits taxable?
The HRA plan is intended to meet certain requirements of existing federal tax laws, under which the benefits that you receive under the HRA Plan generally are not taxable to you. Your employer cannot guarantee the tax treatment to any given participant, since individual circumstances may produce differing results. What is the difference between an HRA and FSA?
HRAs are employer-funded, which means your employer determines the amount that goes into the HRA account. FSAs are employee-funded, which means the funds are deducted from your salary. You determine the amount to go into your FSA account. What does the IRS require me to report on my taxes concerning my HRA?
Nothing. Your HRA is a health benefit.
Content © 2007-2009 Zywave, Inc. All rights reserved.

Content © 2008 Zywave, Inc. All rights reserved. The information contained herein, including its attachments, contains proprietary and confidential information. Any distribution of these materials to third parties is strictly prohibited. ZywaveRx™ is a registered trademark of Zywave, Inc.
ZywaveRx™ A cure for the common PBM
You know that health care costs are rising, fast.
You know there’s no slowdown in sight. But, do
you know that pharmacy benefits are one of the
biggest contributors to those rising health care
costs?
In fact, drug benefit costs are raising 15 – 20%
per year, and account for 10 – 15% of total
health care expenditures. Clearly, keeping drug
benefits costs in line can go a long way toward
improving your overall health benefits costs. But,
drug benefits are popular, highly utilized
benefits; simply slashing or eliminating them
isn’t the right answer.
Cornerstone Benefit Plans, Inc. has the solution
for you: ZywaveRx.
ZywaveRx was formed by leveraging the buying power of a nationwide network of employee benefits brokers — including Cornerstone Benefit Plans, Inc. — that collectively represents over 1.3 million self-funded lives. ZywaveRx lets you compare your current pharmacy benefits manager (PBM) to two leading national PBMs, Express Scripts and Systemed. With ZywaveRx, Cornerstone Benefit Plans, Inc. can provide you access to exclusive, extremely favorable terms for your pharmacy benefits.
The highlights of the ZywaveRx™ program include zero dollar administrative fees, low dispensing fees, deep pharmacy discounts, and aggressive rebates. Using ZywaveRx’s exclusive online savings calculators, Cornerstone Benefit Plans, Inc. can compare your current PBM, Express Scripts, and Systemed to determine the most cost-effective program for you.
ZywaveRx lets us meet several critical objectives for your pharmacy benefits program:
Choice. We don’t limit your choice to one PBM. With ZywaveRx, you can choose between two of the nation’s leading firms.
Accountability. Express Scripts and Systemed know that we are presenting more than one option to our clients. We expect nothing but the highest level of service from them both in order to win your trust.
Support. Express Scripts and Systemed are dedicated to helping Cornerstone Benefit Plans, Inc. and our clients understand their organizations, their products, and the ZywaveRx terms.
Favorable terms. Express Scripts and Systemed can provide extremely favorable terms for our clients. You will be able to retain a cost-effective pharmacy benefits program for your employees for years to come.

1
PPPEEERRRSSSPPPEEECCCTTTIIIVVVEEESSS PROVIDING INSIGHT INTO TODAY'S EMPLOYEE BENEFITS ISSUES
Increasing Healthcare Costs
and Your Employee Health Plan
Ninth Edition
HEALTHCARE costs, and consequently employee health benefits costs, have been increasing at an alarming rate for nearly a decade. While the upward trend in healthcare costs seems to be slowing, cost increases that are outpacing the rate of inflation are still commonplace; costs increased in 2008 and are expected to increase slightly in 2009. Avoiding rising healthcare costs is nearly impossible, but you can learn about why they continue to rise and what you can do to minimize the fallout for your organization and your employees.
The next few pages will discuss the latest healthcare cost figures, the factors leading to nearly a decade of unprecedented rate hikes, and some solutions that firms around the U.S. are undertaking to help soften the blow. National Healthcare Cost and Renewal Rate Projections
Overall national healthcare costs have been skyrocketing for over a decade, and are now just beginning to level off. From 1994 to 1998, average annual healthcare cost increases hovered around 2 percent. From 1999 to 2000, however, costs leapt 9.4 percent and the annual percent change then entered and stayed in the double digits until finally taking a slight downturn from 2005 to 2007.
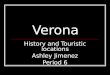
Exhibit 1A, right, depicts the percent change in average annual healthcare cost increases from 2001 to 2009. Cost increased to 6 percent in 2008. Hewitt projects healthcare costs for 2009 to be around 6.4 percent, compared to 6 percent in 2008.
The overall cost of healthcare has a direct impact on the rates employers pay for employee health benefits. Still, health benefits costs have varied widely across the country for the last several years, hitting some metropolitan areas much harder than others. Exhibit 1B, right, illustrates healthcare cost increases (or in one case, decrease) in major metropolitan areas in 2008.
A
B
Annual Healthcare Cost Increases,
National Averages 2001-2009 15.2% 14.7%
12.3%
9.2%7.9%
5.3%6.0% 6.4%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
2001‐02 2002‐03 2003‐04 2004‐05 2005‐06 2006‐07 2007‐08 2008‐09 (proj.)
A
Source: Hewitt Health Value Initiative™, 2008
2008 Healthcare Cost Increases, Major Metropolitan Areas
6.7%7.1%
6.7%8.1%
9.2%8.7%9.1%
7.5%2.6%
7.5%5.3%
8.1%3.7%
4.5%7.2%
0.0% 2.0% 4.0% 6.0% 8.0% 10.0%
Washington, D.C.
Tampa Bay Area
San Francisco
Philadelphia
Orlando
New York City
Minneapolis
Los Angeles
Houston
Detroit
Denver
Dallas/Ft. Worth
Chicago
Boston
Atlanta
Source: Hewitt Health Value Initiative™, 2008
Exhibit 1
B

2
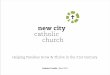
While the rate increase has slowed in recent years, experts expect significant annual increases in healthcare costs to continue indefinitely. According to the 2008 Hewitt Health Value Initiative, the average cost of healthcare benefits for active employees rose to $8,331 per year in 2008 and is expected to grow to $8,863 in 2009.
Exhibit 2A, below, shows the average total health benefit costs for active employees for the years 2002 to 2007. Exhibit 2B below depicts the 2008 healthcare costs per employee in U.S. major metropolitan areas.
According to the survey, employers see consumerism and health management as the most effective way to manage health benefit costs for the future, as opposed to the simple cost-shifting measures that have been used traditionally. Shift to Consumerism Yields CDHP Growth The percentage of all employers offering a consumer-directed health plan (CDHP) based on either a health reimbursement account (HRA) or a health savings account (HSA) continues to rise; in 2008, it increased from 7 percent to 9 percent, as small employers continue to adopt these new types of plans. Growth in CDHPs was strongest among larger employers, where offerings rose from 14 percent to 20 percent among employers with 500 or more employees, and from 41 percent to 45 percent among
jumbo employers (20,000 or more employees). Nationally, enrollment in CDHPs jumped from 5 percent to 7 percent of all covered employees. This migration into lower cost CDHPs is one factor helping to hold down benefit cost increases. CDHPs delivered substantially lower costs per employee than either PPOs or HMOs in 2008. CDHP costs averaged $6,207 per employee, compared to $7,768 for HMOs and $7,815 for PPOs.
Employer account contributions are a standard feature of HRAs but not HSAs. Over a third of large HSA sponsors do not contribute. Of those that do, the average contribution is approximately $694. With deductibles in traditional PPOs rising, the CDHP is becoming a more attractive option for employees who have a choice. Factors Leading to Increased Healthcare Costs Why are U.S. healthcare costs skyrocketing? Several market conditions working in tandem have lead to a decade of unrelenting increases. Understanding why your annual health plan renewal rates may be significantly higher than the previous year is the key to formulating alternatives and solutions to your particular plan’s challenges. It is also the key to educating your employees about the reasons behind any plan or contribution changes you may decide to introduce.
Exhibit 2
B
A
Annual Healthcare Costs Per Employee, National Averages 2002-2009
$4,914 $5,639
$6,334 $6,915
$7,464 $7,857 $8,331
$8,863
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
$9,000
$10,000
2002 2003 2004 2005 2006 2007 2008 2009 (proj.)
2008 Healthcare Costs Per Employee, Major Metropolitan Areas
$7,552$8,331$8,696$8,634
$7,573$8,540$8,766
$7,296$8,740
$8,374$8,062
$9,277$8,147
$9,477$7,677
$0 $1,000 $2,000 $3,000 $4,000 $5,000 $6,000 $7,000 $8,000 $9,000 $10,000
Washington, D.C.Tampa Bay Area
San FranciscoPhiladelphia
OrlandoNew York CityMinneapolisLos Angeles
HoustonDetroitDenver
Dallas/Ft. WorthChicagoBostonAtlanta
Source (both): Hewitt Health Value Initiative™, 2008

One of the major factors driving up the cost of
healthcare is the growth of healthcare providers.
Demographics: The Aging of America It is an inescapable fact: the U.S. population is aging. As a result, there is a subsequent rise in the occurrence of chronic diseases like asthma, heart disease, and cancer, and a resultant need for more resources to fight these diseases. This leads to elevated utilization of prescription drugs and other medical services, and an overall rise in dollar expenditures on healthcare. Dramatic Rise of Prescription Drug Costs Please turn to the attached Special Report: Prescription Drug Costs and Your Employee Health Plan for a discussion of why prescription drug costs are on the rise. Expansion of Providers One of the major factors driving up the cost of healthcare is the growth of healthcare providers. While these systems provide many benefits to the communities they serve, they also require a great deal of capital to fuel their growth. These capital expenditures by hospital systems and other providers place upward pressure on the costs of many medical services. Consolidation of Managed Care Companies The landscape of the managed care industry has changed. Years of under-pricing, weak underwriting, and the costly process of assimilating acquisitions has lead to serious dips in profitability and stock prices for a large number of carriers. Those who couldn’t make the cut have either sold off their managed care operations to a bigger fish, or have completely gone out of business. Companies that haven’t exited the market altogether are now faced with much less competition and a renewed commitment to achieving healthy returns. This has ultimately resulted in increased rates. Political Environment and Government Regulation Healthcare issues, particularly those surrounding health plans and medical liability, have become one of the most hotly debated topics in the political arena, while health insurance is one of the most regulated insurance sectors on both the state and federal levels. State and federal mandates have increased twenty-five-fold over the last three decades. Often these mandates duplicate or conflict with each other, and they almost always come with increased costs for the healthcare system. On the political front, concerns about timely access to quality healthcare services and calls for federal laws to protect consumers led to a variety of legislative initiatives, including the now defunct Patients’ Bill of Rights. Homeland security interests, a slowing economy, the war in Iraq, and other domestic issues have since forced most of the political debate to the backburner. However, if the Patients’ Bill of Rights were resurrected or other legislation regarding medical liability were initiated, the negative impact on healthcare costs is expected to be significant.
Issues such as prescription drugs for seniors, Medicare reform, and coverage for the uninsured will also continue to play a big role on political and legislative agendas in the coming years, and will undoubtedly continue to place upward pressure on costs.
Increased Utilization and Consumer Demand
Utilization of many healthcare services has risen over the decade. A number of factors such as improvements in medical procedures and technology, the influence of managed care, elevated consumer awareness and demand, and a boost in the number of practicing physicians, caused health services like the number of surgical procedures and the number of prescription drugs dispensed to rise significantly. Other services, such as breast cancer screenings, immunizations for children, and diagnostic procedures like CT and MRI have also experienced sharp utilization increases. New Medical Technology Life expectancy and disease-specific mortality rates in the U.S. are steadily improving. Old techniques are being replaced with new, often expensive treatments using new medical devices, diagnostic products, drugs, and surgical procedures. These include everything from digital mammography to hip replacement to radioactive “seeds” used to treat prostate cancer. It is not surprising that these new procedures come with hefty price tags, and therefore drive the overall cost of healthcare — and subsequently health benefits costs — upward. Weakening of the Managed Care System The booming economy of the late 1990s, consumer demand, and the regulatory environment discussed above have led to a general weakening of the managed care system. During the economic boom of the late 1990s, patients and employers migrated away from the tightest forms of managed care, HMOs. Employers seeking to hire the best employees in the tight job market moved towards offering plans that allow patients to see doctors that are “out-of-network” or have much less strict referral processes, such as Point-of-Service (POS) plans. In addition, many employers making health plan purchase decisions focused on keeping employees happy by ensuring that most doctors in an area were in the chosen network, rather than choosing narrower networks with deeper discounts.
Provider contracting has also placed a strain on the managed care system. Many hospitals that have taken a beating due to the Balanced Budget Act of 1997 — which cut billions of dollars from Medicare managed care payments — and by other financial difficulties are now willing to walk away from health plans that they view as offering insufficient reimbursement rates and prohibitive payment practices. In many cases, these threats have won hospitals and other providers significant increases in reimbursement for the first time in several years. These actions are having a domino effect as other providers become more courageous and attempt to exert power during negotiations with
3

health plans. With the level of premium increases seen over the last several years, employers have backed away from offering rich benefits, and instead have employed a number of tactics to reduce costs. Healthcare Spending and Medical Cost Inflation Overall healthcare spending and medical cost inflation are ascending, often due to many of the factors discussed above. Employers React — What Can You Do? You and other employers are undoubtedly trying to determine how to keep accelerating health plan rates from having debilitating repercussions on your organization. After years of trying to absorb most of the costs because of attraction and retention issues, many firms are now trying to attack the root causes of rising costs with sustained, systemic changes. Small businesses in particular continue to face the critical decision to raise employee contributions or to discontinue offering the coverage altogether. Many employers plan to make significant investments in longer term solutions aimed at improving the health and productivity of their workers. These strategies involve introducing more consumer-driven plans, value-based design, improving employee education, influencing positive employee behavior changes through condition management and wellness programs, and improving the amount and quality of data available on healthcare costs and quality. Introducing or Expanding Consumerism
While basic cost-shifting remains a prevalent means for managing costs, there is evidence of a movement toward more consumer-oriented solutions. Those companies that want to balance costs and employee relations are incorporating more of a consumerist focus into their plans. Value-Based Plan Design Employers are beginning to acknowledge that cost-shifting and cost-cutting strategies are not enough. In addition to the consumerism plan designs, employers are looking at new models, such as value-based design. This option incentivizes employees to use appropriate care and services to manage their health. According to Hewitt’s research, almost 20 percent of large employers have implemented a value-based design and another 40 percent are interested in learning more about these plans.
Improving Employee Education and Communication Studies agree that the only way for consumer-driven
strategies to have their desired impact (to drive smarter consumer behavior among employees) is for companies to also invest heavily in the communication, education, and decision support tools that will result in better decision-making by employees and their dependents. Requiring active enrollment is increasing, as are decision support tools that can help employees evaluate their options.
Increasing Disease Management and Wellness Programs The number of companies using disease management programs and wellness programs continues to grow, according to the 2008 Kaiser/HRET Employer Health Benefit Survey:
• 54 percent of firms offering health benefits offer at least some type of wellness program.
• Among firms offering health benefits and wellness programs, 33 percent of employers report their primary reason for offering wellness programs is to improve the health of employees and reduce absenteeism.
Other Strategies for Reducing Costs The following are some additional tactics that employers are using to reduce healthcare costs. CONTRIBUTION STRATEGIES
Employers are looking for ways to control costs by evaluating how they differentiate contributions for employees and their dependents. Pay-based contribution models are also commonly used. DEPENDENT COVERAGE CHANGES
Changing the rules for dependent coverage may be one way to influence employee behavior. The most common practices include:
implementing higher cost sharing for dependents; providing flexible credits for opting out of coverage; requiring additional contribution if an employee’s working
spouse does not accept coverage from his or her own employer; and
requiring an employee’s working spouse to accept coverage from his or her own employer.
CHANGE PRESCRIPTION DRUG COVERAGE Efforts to control overall healthcare costs by making changes
to prescription drug benefits include: using a three-tier design, increasing coinsurance, requiring step therapy, requiring the use of generics, requiring mail order of certain drugs, and using a therapeutic MAC/reverse copay design.
Requiring active enrollment is increasing, as are decision support tools that can help employees evaluate their
options.
4

5
Which Solution is Right for You?
Should you pass costs on to employees at the risk of losing some of them? Or, should you try to manage costs in some of the other ways discussed in this report? Ultimately, it is a decision that you need to come to through thoughtful and detailed analysis of your plans and with the advice of your broker-consultant. Below are some questions you can address in order to begin developing an effective strategy that is right for your organization.
Is our program structure, plan design, and pricing appropriate? Do we have the right vendors, services, contracting, and funding in place? Are our employee communication efforts appropriate and effective? Do we have the right disease and case management programs for our employees? Do our pricing and plan design features encourage cost-conscious behavior on the part of our employees? Do our employee communication efforts and resources motivate our employees to become educated and effective healthcare consumers?
What Should I Tell My Employees? It’s a fact: healthcare costs and health benefit costs continue
to increase at exceptionally high rates from year to year. You want to continue to offer valuable health benefits to your current and future employees, and you want those benefits to help you attract and retain good employees. However, you also need to consider the cost-effectiveness of those benefits at a time when hefty rate hikes are the norm, rather than the exception.
The information contained in this report is designed to help
you understand why your renewal rates may have increased, and to consequently help you educate your employees about the reasons for any plan or contribution changes you may have to make. If your employees understand current trends in the healthcare industry, they will be more supportive of any such changes and will appreciate the resources required to provide them with their healthcare benefits. ◊
Perspectives is provided to [B_Officialname] clients for informational purposes. Please seek qualified and appropriate counsel for advice on how to apply the topics discussed herein to your employee benefits plan. Content © 2007-2009 Zywave, Inc.

6
PPPEEERRRSSSPPPEEECCCTTTIIIVVVEEESSS PROVIDING INSIGHT INTO TODAY'S EMPLOYEE BENEFITS ISSUES
Special Report: Prescription Drug Trends Ninth Edition
Overview Prescription drug costs continue to represent an increasingly large portion of healthcare expenditures. Understanding the pharmaceutical market is key to determining new approaches for addressing these rising costs. According to the Centers for Medicare & Medicaid Services (CMS), spending in the U.S. for prescription drugs was $216.7 billion in 2006, more than 5 times the $40.3 billion spent in 1990.1 While prescription drug spending has been a fairly small proportion of national health care spending compared to spending for hospital and physician services (10% in 2006, compared to 31% and 21%, respectively) it has been one of the fastest-growing components, until recently growing at double-digit rates compared to single-digit rates for hospital and physician services. In 2006, the annual rate of increase in prescription spending was 9%, compared to 7% for hospital care and 6% for physician services2 (Figure 1).
Figure 1: Average Annual Percentage Change in Selected National Health Expenditures, 1996‐2006
34
35
68 8 8
7 7 7
45
65
79
89
7 76
13 1314
18
15 1514
11
86
9
02468
101214161820
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Hospital Care Physician & Clinical Services Prescription Drugs
Source: Kaiser Family Foundation calculations using National Health Expenditure historical data from Centers for Medicare & Medicaid Services.
Prescription spending growth slowed from 1999 to 2005 because of the increased use of generic drugs, the increase in tiered copayment benefit plans, changes in the types of drugs used, and a decrease in the number of new drugs introduced. However, the growth in drug spending in 2006 resulted from the increased use of prescription drugs believed to be because of the implementation of Medicare Part D, new indications for existing drugs, strong growth in several therapeutic classes,
and increased use of specialty drugs; lower rebates from drug manufacturers; and changes in the therapeutic mix of drugs.3
The portion of prescription drug expenses paid by private health insurance has increased substantially over the past 16 years (from 26% in 1990 to 44% in 2006). This trend has contributed to a decline in the share that people pay out of their own pockets (from 56% in 1990 to 22% in 2006.) The government’s share of expenditures remained fairly constant. However, according to the U.S. Department of Health and Human Services (HHS), the implementation of the Medicare Part D drug program in 2006 significantly changed the mix of funding sources, as the government’s share rose from 28% in 2005 to 34% in 2006, the private insurance portion fell from 48% to 44%, and the consumer out-of-pocket share declined from 24% to 22% (Figure 2).
Figure 2: Percent of Total National Prescription Drug Expenditures by Type of Payer, 1990‐2006
56
4943
35 31
Notes: Consumer Out-of-Pocket includes direct spending by consumers for health care goods and services not covered by a health plan and cost-sharing amounts (coinsurance, copayments, deductibles) required by public and private health plans. It does not include consumer premium payments and cost sharing paid by supplementary Medicare policies, which are included in the Private Health Insurance category. May not add to 100% due to rounding.
Within public funds, the funding shares changed from 7% Medicare and 68% Medicaid in 2005, to 53% Medicare and 26% Medicaid in 2006 (Figure 3, next page).
28 2628
34
2631
36
4348 49 50 48
44
18 20 22 21 22 2325 25 22
0
10
20
30
40
50
60
1990 1992 1994 1996 1998 2000 2002 2004 200
Consumer Out‐of‐Pocket
Private Health Insurance
6
Public Funds
Source: Kaiser Family Foundation calculations using National Health Expenditure historical data from Centers for Medicare & Medicaid Services.

7
Notes: “Medicaid” includes federal and state funds for Medicaid and the Medicaid State Children’s Health Insurance Program (SCHIP) expansion: “Other Public” includes other federal, state, and local expenditures and the Medicaid SCHIP program.
Driving Forces According to the Kaiser Family Foundation’s September 2008 “Prescription Drug Trends” report, changes in prescription drug spending are primarily driven by three main factors: changes in the number of prescriptions dispensed (utilization), price changes, and changes in the types of drugs used.
Increased Utilization. It is a fairly simple concept: More people are using more prescription drugs, thereby driving overall spending upward. From 1997 to 2007, the number of prescriptions purchased increased 72% (from 2.2 billion to 3.8 billion), compared to a U.S. population growth of 11%. The average number of retail prescriptions per capita increased from 8.9 in 1997 to 12.6 in 2007.4 The percent of the population with a prescription drug expense in 2005 was 59% for those under age 65, and 91% for those 65 and older. The percentage of these populations with a drug expense has remained basically steady since 1997, when they were 59% for those under age 65, and 86% for those 65 and older.5
Increased Prices. Prescription drug prices increased at 3.5% in 2006 – the same rate as in 2005.6 Retail prescription prices7 (which reflect both manufacturer price changes for existing drugs and changes in use to newer, higher-priced drugs) increased an average of 6.9% a year from 1997 to 2007 (from an average price of $35.72 to $69.91), more than two-and-a-half times the average annual inflation rate of 2.6% over the same decade. In 2007, the average brand name prescription price in was over three times the average generic price ($119.51 versus $34.34). Manufacturers received 78% of the average retail prescription price of $69.91, retailers received 19%, and wholesalers received 4% in 2007.8
Changes in Types of Drugs Used. When new drugs enter the market and existing drugs lose patent protection, prescription drug spending is affected. If new drugs are used in place of older, less expensive medications, they can increase overall drug spending. In addition, if new drugs supplement rather than replace existing drug treatments, or if they treat a
condition not previously treated with drug therapy, they can also lead to increased drug spending. However, new drugs can reduce drug spending if they enter the market at a lower price than existing drug therapies, for instance, if a new drug enters a therapeutic category with one or two dominant brand competitors. The number of new drugs approved by the U.S. Food and Drug Administration (FDA) has fluctuated over the past decade, with 39 approvals in 1997, 27 in 2000, 20 in 2005, and 18 in 2006.9
Figure 3: Distribution of Total Public Prescription Drug Expenditures by Type of Payer, 2005 & 2006
Source: Kaiser Family Foundation calculations using National Health Expenditures historical data from Centers for Medicare & Medicaid Services.
68%
21%
7%
Drug spending can also be reduced when existing brand drugs lose patent protection and face competition from new, lower cost generic substitutes. Analysis by the FDA shows that generic competition is linked with lower drug prices: on average, the first generic competitor prices its product only slightly lower than the brand-name manufacturer; the second generic manufacturer reduces the average generic price to nearly half the brand name price; and then prices continue to fall at a slower pace as additional generic manufacturers market the product. The average generic price falls to 20% or lower of a brand’s price for medications with a large number of generic equivalents.10
26%
53%
25%
0% 10% 20% 30% 40% 50% 60% 70% 80%
2006
2005
Other Public Medicaid Medicare
About 75% of FDA-approved drugs have generic counterparts. In 2007, 21% of total prescription drug sales and 65% of total prescriptions dispensed were generic medicines. From 2005 to 2006, generic sales rose to 8%.11 Federal legislation allowing FDA approval of generic substitutes for brand name biologic drugs was initiated in 2007 but has yet to be enacted.
Advertising. Prescription use in general and movement to higher-priced drugs can be influenced by advertising. The total amount manufacturers spent on advertising declined from 2004 to 2005 ($11.9 billion to $11.4 billion), rose to $12 billion in 2006, and declined sharply in 2007 to $10.4 billion. This fluctuation is a new trend, as advertising spending had increased every year from 1996 to 2004. Advertising directed toward consumers (television, radio, magazines, newspapers, and outdoor billboards) decreased from 2006 to 2007 (from $4.8 to $3.7 billion), and the share directed toward physicians (through pharmaceutical representatives and professional journals) also decreased (from $7.2 to $6.7 billion). However, spending for consumer advertising in 2007 was more than four times the amount spent in 1996 ($3.7 billion vs. $0.8 billion), while 2007 physician advertising was almost two times the 1996 amount ($6.7 billion vs. $3.5 billion).12 Changes to prescription advertising rules are currently being considered by the FDA and Congress.
Profits. From 1995 to 2002, the number one most profitable industry in the nation (profits as a percent of revenues) was pharmaceutical manufacturing. It ranked third in 2003 and 2004, fifth in 2005, second in 2006, and third in 2007 – with profits of 15.8%, compared to 5.7% for all Fortune 500 firms in 2007.13 Increasing only 3.8% from 2006, prescription drug sales were $286.5 billion in 2007 – the smallest growth rate since 1961. According to IMS Health, the slower sales growth is attributed to loss of exclusivity of brand name medicines, fewer new product approvals, the leveling of year-over-year growth from the Medicare Part D program, and the impact of safety issues.14

8
Insurance Coverage Lack of insurance coverage for prescription drugs can be detrimental to the industry. An April 2008 survey found that uninsured adults ages 18-64 are more than twice as likely as those who are insured to say that they or a family member did not fill a prescription (45% compared to 22%), cut up pills or skipped doses of medicine (38% compared to 18%) in the past year because of the cost.15
Prescription drug coverage comes from several sources, both private and public:
Employer Coverage. The main source of health coverage in the U.S. are employers, providing coverage for 177 million (59%) of Americans in 2007.16 Sixty percent of employers offered health insurance to their employees in 2007, and 65% of employees in those firms are covered by their employer’s health plan.17 Other employees likely obtained coverage through a spouse. Nearly all (98%) of covered workers in employer-sponsored plans had a prescription drug benefit in 2007.18
Medicare. Previous to January 1, 2006, the traditional Medicare program (the federal health program for the elderly and disabled) did not provide coverage for outpatient prescription drugs. As a result, 27% of seniors age 65 and older, and one-third of poor (34%) and near-poor (33%) seniors, had no drug coverage in 2003.19 The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 put into effect a voluntary Medicare outpatient prescription drug benefit (Part D), under which the 44 million Medicare beneficiaries can enroll in private drug plans.
HHS data shows that as of January 2008, approximately 90% of Medicare beneficiaries have drug coverage; 25.4 million beneficiaries have Medicare Part D drug coverage from either a stand-alone prescription drug plan (17.4 million, including 6.2 million low-income seniors and people with disabilities, known as dual eligibles, who were transferred from Medicaid drug coverage to Medicare Part D drug coverage), a Medicare Advantage drug plan (7.6 million), or other Medicare health plan types (0.4 million). Another 10.2 million beneficiaries have coverage from creditable employer or union retiree plans (including FEHB and TRICARE retiree coverage.) About 4 million beneficiaries have creditable drug coverage from the VA and other sources, and around 4.6 million beneficiaries did not have creditable coverage (were not enrolled in a Part D drug plan or a source of creditable coverage.)20
Medicaid. Medicaid is the joint federal-state program that pays for medical assistance to 60 million low-income individuals and is the main source of outpatient pharmacy services to the low-income population. There are differences in state policies in regard to copayments, preferred drugs and amount of prescriptions which can be filled, but all state Medicaid programs provide coverage for prescription drugs. In 2006, about 6 million dual eligibles were transferred from Medicaid drug coverage to Medicare Part D drug coverage, representing an estimated 14% of Medicaid beneficiaries and accounting for about 45% of Medicaid prescription drug spending in FY2003.21 States have been required to make payments to Medicare to help finance Medicare drug coverage for these transferred and future dual eligibles since January 1, 2006.
Response A variety of public and private strategies have been employed to try to contain rising prescription drug costs.
Utilization Management Strategies. Health plans have excluded certain drugs from coverage, used quantity dispensing limits, and increased enrollee cost-sharing amounts. In 2007, 75% of workers with employer-sponsored coverage had a cost-sharing arrangement with three or four tiers, almost three times the proportion in 2000 (27%).22 Copayments for nonpreferred drugs climbed from an average of $29 in 2000 to $43 in 2007 (an increase of 48%). Copayments for preferred drugs increased by 67%, from an average of $15 in 2000 to $25 in 2007 (Figure 4).
Figure 4: Among Covered Workers with Three‐ or Four‐Tier Prescription Drug Cost Sharing, Average Copayments, 2000‐2007
Source: Kaiser/HRET Survey of Employer‐Sponsored Health Benefits, 2000‐2007, Exhibit 9.4
815
29
918
10
32
22
38
11
59
25
43
59
11
25
43
010
20304050
607080
Generic Preferred Nonpreferred Fourth‐Tier*
71
2000 2002 2004 2006 2007
Dollars
Red numbers=Estimate is statistically different from estimate for the previous year shown at p <.05. *Fourth-tier drug copay information was not obtained prior to 2004. Discounts and Rebates. Drug programs, both private and public, negotiate with pharmaceutical manufacturers (often using pharmacy benefit managers, which are contracted organizations) to receive discounts and rebates which are applied based on volume, prompt payment, and market share. Manufacturers who want their drugs covered by Medicaid must provide rebates to state Medicaid programs for the drugs they purchase. Somestates have also negotiated additional rebates, or supplemental rebates.
The Department of Veterans Affairs, the Defense Department, the Public Health Service, and the Coast Guard – as well as other government agencies – participate in a program called the Federal Supply Schedule, where they purchase drugs from manufacturers at prices equal to or lower than those charged to their “most-favored” nonfederal purchasers. In order to participate in Medicaid, another program, the Section 304B Program, requires manufacturers to provide drugs to certain nonfederal entities (such as community health centers and disproportionate share hospitals) at reduced prices. This program may be expanded, as federal legislation was introduced in 2007, but nothing has yet been enacted.
Medicaid. Prescription drugs have been one of the fastest-growing Medicaid services. The Deficit Reduction Act of 2005 gave states more authority to control Medicaid drug spending through increased cost sharing for non-preferred drugs, changes in the way Medicaid pays pharmacists, allowing pharmacists to refuse prescriptions for beneficiaries

9
who don’t pay their cost sharing, and inclusion of authorized generic drugs in the calculation of “best price” for drugs. A 2006 survey of 50 states and D.C. found that more than half had Medicaid pharmacy cost containment measures in place in FY2006, including preferred drug lists and prior authorization programs (about 75% of states), supplemental rebates from manufacturers (about 70% of states), and state Maximum Allowable Cost (MAC) programs for generic and multi-source brand drugs (about 60%); smaller proportions of states were members of multi-state purchasing coalitions (about 25%) or had limits on quantities dispensed per prescription (about 20%).23 By 2007, most states had already implemented many of these approaches, so new action to control drug spending slowed.24
The Centers for Medicare & Medicaid Services issued a rule referred to as the AMP Rule in July 2007 that would have set limits on federal government reimbursements to states for Medicaid prescriptions; however, in December 2007, a U.S. District Court issued a preliminary injunction against this change. Several bills have since been introduced in Congress to address this issue.
Medicare. The Medicare Part D drug benefit moved spending from the private sector and Medicaid to Medicare, making Medicare the nation’s largest public payer of prescription drugs in 2006 – when Medicare spending rose from 2% in 2005 to 18% in 2006 – of total U.S. prescription spending.25 Medicare is prohibited from directly negotiating drug prices or rebates with manufacturers under the Medicare Part D legislation, but will rely on the private Part D drug plans to negotiate these discounts/rebates. In 2007, the 110th Congress considered but did not pass legislation to allow or require Medicare to negotiate drug prices with drug makers.
Purchasing Pools. Some public and private organizations have banded together to form prescription drug purchasing pools to increase their purchasing power through higher volume and shared expertise. Examples include joint purchasing by the Department of Defense and VA; multi-state bulk buying pools through which states purchase drugs for their Medicaid, state employees, senior/low-income/uninsured pharmacy assistance programs, or other public programs; and individual state purchasing pools.26
Consumers. In order to reduce their prescription costs, consumers are turning to a variety of methods,27 such as requesting cheaper drugs or generic drugs from their physicians and pharmacies, using the Internet and other sources to make price comparisons, using the Internet to purchase drugs, buying at discount stores, buying over-the-counter (OTC) instead of prescribed drugs, buying drugs in bulk and pill-splitting, using mail-order pharmacies,28 and using pharmaceutical company or state drug assistance programs. Over half of physicians say they frequently talk with patients about the out-of-pocket costs of medicines they prescribe; 62% say they switch patients to less expensive drugs, and 58% say they give patients office samples.29
Importation. The high cost of prescriptions has led some to suggest that individuals be permitted to purchase prescription products from distributors in Canada or other countries. This is referred to as “importation,” or “reimportation” if the drug
is manufactured in the U.S. Although it is generally not legal for individuals or commercial entities such as pharmacies or wholesalers to purchase prescription drugs from other countries, the government does not always act to stop individuals from purchasing drug products across the border. Importation of pharmaceutical products from Canada through Internet sales and travel to Canada totaled about $700 million in sales in 2003 – 0.3% of total U.S. prescription sales. The same amount of prescription drugs was estimated to have entered the U.S. from the rest of the world, mostly through the mail and courier services.30 Legislation enacted in 2006 allows U.S. residents to transport up to a 90-day supply of qualified drugs from Canada to the U.S. Actual savings amounts, drug safety, and marketplace competition and pricing are importation issues being debated. Outlook HHS projects U.S. prescription drug spending to increase from $216.7 billion in 2006 to $515.7 billion in 2017, a 138% increase. The average annual increase in drug spending from the previous year is expected to decline from 8.5% in 2006 to 6.7% in 2007 because of a drop in drug price growth, but then rise to 9.6% in 2017 (or an 8.2% average annual increase over the 11-year period). Drug spending as a percent of overall health spending is projected to increase from 10% in 2006 to 12% in 2017. HHS asserts that over the next 10 years, drug spending growth will accelerate due to a leveling off of growth in the use of generic drugs, rising utilization rates, and a mild increase of new drugs coming onto the market.31 ◊ Reprinted with Permission from the Kaiser Family Foundation. The Henry J. Kaiser Family Foundation is a non-profit, private operating foundation dedicated to providing information and analysis on health care issues to policymakers, the media, the health care community, and the general public. The Foundation is not associated with Kaiser Permanente or Kaiser Industries. Perspectives is provided to [B_Officialname] clients for informational purposes. Please seek qualified and appropriate counsel for advice on how to apply the topics discussed herein to your employee benefits plan. © 2007-2009 Zywave, Inc.
1 All spending amounts in this report are in current dollars (i.e., not adjusted for inflation). 2 Centers for Medicare & Medicaid Services, National Health Expenditure Accounts, Historical, www.cms.hhs.gov/NationalHealthExpendData. 3 Aaron Catlin et al., “National Health Spending in 2006: A Year of Change For Prescription Drugs,” Health Affairs 27, no. 1, (January/February 2008). 4 Kaiser Family Foundation calculations using data from IMS Health, www.imshealth.com (About Us, Press Room, US Top-Line Industry Data), and Census Bureau, www.census.gov. The per capita number may differ from the number reported at KFF’s website www.statehealthfacts.org because of differing data sources which use

10
different retail pharmacy definitions (e.g., IMS Health includes mail order, Verispan does not.) 5 Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey Component Data, “Prescription Medicines – Mean and Median Expenses per Person with Expense and Distribution of Expenses by Source of Payment,” table 2, 1997 and 2005, www.meps.ahrg.gov/mepsweb. 6 Aaron Catlin et al., “National Health Spending in 2006: A Year of Change for Prescription Drugs,” Health Affairs 27, no. 1, (January/February 2008). 7 Retail prescription prices reflect the prices paid by insured and uninsured patients, and do not reflect rebates, discounts, and other payments that in effect lower the cost of prescriptions. 8 Kaiser Family Foundation calculations using data from the National Association of Chain Drug Stores, “Industry Facts-at-a-Glance,” www.nacds.org (based on data from IMS Health), and Consumer Price Index, U.S. City Average, All items, from the Bureau of Labor Statistics, www.bls.gov. 9 U.S. Food and Drug Administration, www.fda.gov/cder/rdmt; 2004-2007 data include new BLAs (biologic license applications) for therapeutic biologic products transferred from FDA’s Center for Biologics Evaluation and Research to its Center for Drug Evaluation and Research. 10 U.S. Food and Drug Administration, Center for Drug Evaluation and Research, “Generic Competition and Drug Prices,” www.fda.gov/cder/ogd/generic_competition.htm. 11 Generic Pharmaceutical Association, www.gphaonline.org/Content/NavigationMenu/AboutGenerics/Statistics/default.htm. 12 IMS Health, www.imshealth.com (About Us, Press Room, 2007 US Top-Line Industry Data); Kaiser Family Foundation, Prescription Drug Trends, a chartbook, (July 2000), ex. 3.13, www.kff.org/rxdrugs/3019-index.cfm. The data on spending for advertising directed toward physicians excludes the retail value of drug samples left at sales visits to physicians’ offices, which totaled about $16 billion in 2004, the last year such data were available online from IMS Health. 13 Fortune 500 online, http://money.cnn.com/magazines/fortune/fortune500/2008/performers/industries/profits/index.html, and personal communication; April issues of Fortune magazine. 14 “Moderating Growth Reflects Impact of Patent Expirations, Fewer Product Approvals, Maturing Medicare Part D Program, and Safety Issues,” IMS Health Press Release (March 12, 2008), http://imshealth.com/ims/portal/front/articleC/0,2777,6599_3665_83470499,00.html 15 Kaiser Family Foundation, Kaiser Public Opinion Survey Brief, Economic Problems Facing Families (April 2008), p.4, www.kff.org/kaiserpolls/upload/7773.pdf. 16 U.S. Census Bureau, Income, Poverty and Health Insurance Coverage in the United States: 2007 (August 2008), Table C-1, p.61, www.census.gov/prod/2008pubs/p60-235.pdf. 17 Kaiser Family Foundation and Health Research and Educational Trust, Employer Health Benefits 2007 Annual Survey (September 2007), pp.36 and 51, www.kff.org/insurance/7672/upload/76723.pdf. 18 Ibid, p.134, www.kff.org/insurance/7672/upload/76723.pdf. 19 Dana Gelb Safran et al., “Prescription Drug Coverage and Seniors: Findings from a 2003 National Survey,” Health Affairs, Web Exclusive (April 19, 2005): W5-160, www.kff.org/medicare/med041905pkg.cfm.
20 Kaiser Family Foundation, The Medicare Prescription Drug Benefit, (February 2008), www.kff.org/medicare/upload/7044_08.pdf. 21 Kaiser Family Foundation calculations using data from John Holahan and Arunabh Ghosh, Dual Eligibles: Medicaid Enrollment and Spending for Medicare Beneficiaries in 2000 (Kaiser Commission on Medicaid and the Uninsured, July 2005), 8,10,21, www.kff.org/medicaid/7346.cfm. 22 Kaiser Family Foundation and Health Research and Educational Trust, op. cit., Ex. 9.1, www.kff.org/insurance/7672/sections/ehbs07-9-1.cfm. 23 Kaiser Family Foundation calculations using data from Vernon Smith et al., Low Medicaid Spending Growth Amid Rebounding State Revenues: Results from a 50-State Medicaid Budget Survey, State Fiscal Years 2006 and 2007 (Kaiser Commission on Medicaid and the Uninsured, October 2006), 39, fig. 24, www.kff.org/medicaid/upload/7569.pdf. 24 Kaiser Commission on Medicaid and the Uninsured, Few Options for States to Control Medicaid Spending in a Declining Economy (April 2008), p.3, www.kff.org/medicaid/upload/7769.pdf. 25 Aaron Catlin et al., op.cit., ex.4, p.19. 26 National Conference of State Legislatures, “Pharmaceutical Bulk Purchasing: Multi-state and Inter-agency Plans, 2008 edition” (updated May 8, 2008), www.ncsl.org/programs/health/bulkrx.htm. 27 Devon Herrick, National Center for Policy Analysis, Shopping for Drugs: 2004, National Center for Policy Analysis, Policy Report No. 270 (October 2004), www.ncpa.org/pub/st/st270. 28 U.S. mail services sales have increased 54% since 2003, though their share of total U.S. prescription sales has increased only slightly – 2007: $44.6 billion in sales, 16% of total prescription sales; 2003: $28.9 billion in sales, 13% of total prescription sales. IMS Health, www.imshealth.com (About Us, Press Room, US Top-Line Industry Data, 2007 U.S.). 29 Kaiser Family Foundation, Prescription Drugs: Advertising, Out-of-Pocket Costs, and Patient Safety from the Perspective of Doctors and Pharmacists (November 2006), www.kff.org/kaiserpolls/upload/7583.pdf. 30 U.S. Department of Health and Human Services Task Force on Drug Importation, Report on Prescription Drug Importation (December 2004), ix, www.hhs.gov/importtaskforce/Report1220.pdf. 31 Sean Keehan et al., “Health Spending Projections Through 2017: The Baby-Boom Generation is Coming to Medicare,” Health Affairs, Web Exclusive (February 26, 2008), w145-w155.

Legislative Brief Electronic Distribution of ERISA Disclosures
Department of Labor (DOL) regulations contain a safe harbor under which ERISA plans may use electronic means to distribute certain documents and other required ERISA information. Thus, summary plan descriptions (SPDs), summaries of material modifications (SMMs), summary annual reports (SARs), COBRA notices, qualified domestic relations orders (QDROs), and qualified medical child support orders (QMCSOs), for example, can all be distributed electronically if certain conditions are met. This issue of the [b_officialname] Legislative Brief summarizes the regulations permitting electronic distribution of disclosures required under Title I of ERISA. What type of disclosures can a plan administrator send electronically? The regulations allow plan administrators to electronically send disclosures required under Title I of ERISA. Such disclosures include:
• SPDs, SMMs, and SARs, • Individual benefit statements, • COBRA notifications, • QDRO notifications, • QMCSO notices, • Information regarding participant loans under ERISA 401(b)(1), and • HIPAA certificates of creditable coverage.1
• May plan administrators electronically distribute ERISA disclosures to all recipients? The regulations set forth guidelines for providing disclosures to a) employees with work-related computer access, and b) other plan participants and beneficiaries who consent to receive disclosures electronically. Employees With Work-Related Computer AccessERISA disclosures may be delivered electronically to employees that • have the ability to effectively access documents furnished in electronic form at any location where the employee
is reasonably expected to perform his duties, and • are expected to have access to the employer's electronic information system as an integral part of those duties.2 • Beneficiaries and Other Plan Participants Who Consent to Receive Disclosures ElectronicallyA plan administrator must obtain written consent prior to electronically delivering ERISA disclosures to beneficiaries and other plan participants who do not have work-related access to a computer. The consent may be received in either electronic or paper form. Prior to consenting, an individual must be given a clear and conspicuous statement that explains: • The types of documents to which the consent will apply; • That consent can be withdrawn at any time without charge; • The procedures for withdrawing consent and for updating the address used for receipt of electronically furnished
documents;
1 The electronic distribution standards do not alter any requirements related to what individuals are entitled to a disclosure, the content of the disclosure, or the timing of the disclosure. 2 Merely providing employees access to a computer in a common area (e.g., computer kiosks) is not a permissible means by which to deliver documents required to be furnished to plan participants.

Legislative Brief Electronic Distribution of ERISA Disclosures
• The right to request and obtain a paper version of an electronically furnished document, including whether the paper version will be provided free of charge; and
• Hardware or software needed to access and retain the documents delivered electronically. Where the electronic distribution is made through the Internet, the individual must affirmatively consent in a manner that reasonably demonstrates his or her ability to access information in the electronic form that would be used. If the plan administrator changes its hardware or software requirements, it must provide a new notice and obtain a new consent. What general disclosure requirements apply to all electronic disclosures? Plan administrators are required to use measures reasonably calculated to ensure actual receipt of the material by plan participants and beneficiaries. The regulations provide some guidance on what measures are reasonably calculated to ensure actual receipt when electronic delivery is used.
• Notices. A notice must be sent either electronically or in paper form to each plan participant or beneficiary at the time the document is provided electronically. The notice must a) indicate the significance of the document when it is not otherwise reasonably evident as transmitted, and b) explain the participant's right to request a paper copy.
• Confirmation of Receipt. The plan administrator must make use of electronic mail features such as return-receipt or notice that the email was not delivered. The plan must also conduct periodic reviews to confirm receipt of the transmitted information.
• Confidentiality. When personal information pertaining to an individual's benefits or accounts is transmitted electronically, steps must be taken to protect the confidentiality of the information.
• Style, Format and Content Requirements. Documents delivered electronically must continue to be furnished in a manner consistent with the applicable style, format and content requirements contained within ERISA. For example, summary plan descriptions provided electronically must contain all the disclosures otherwise required by ERISA's disclosure requirements. The DOL's comments within the preamble to the regulations indicate that the appearance of paper and electronic versions need not be identical.
• Paper Copy. Plan participants and beneficiaries are entitled to receive a paper copy of any ERISA disclosure provided electronically. Where a plan participant or beneficiary requests a paper copy of a document originally provided electronically, the general rules governing whether a plan administrator may or may not charge for paper copies apply.
• Can benefit and claim determinations be provided electronically? Yes. The regulations allow that benefit and claims determinations related to a specific individual may be communicated electronically to that individual. However, where the information contained within the communication is confidential in nature or protected health information subject to the HIPAA Privacy Rules, the plan administrator must take appropriate and necessary steps to ensure that the information remains confidential. The regulations do not provide any guidance on what measures must be used to protect the confidentiality of this information. What forms of electronic disclosure are permissible? The regulations do not require the use of any specific form of electronic media. Examples of permissible forms of electronic disclosure include delivery of documents by email, attachment to an email, posting documents on a company Web site, or on CD-ROM or DVD. May a plan administrator electronically deliver ERISA notices by placing the information on a company Web site? Under the guidelines contained within the regulations, merely placing an SPD on a company Web site available to employees will not by itself satisfy ERISA's disclosure requirements. The plan administrator must also send a notice, either electronically or in paper form, that notifies the employee that the SPD is available on the Web site. A plan administrator that intends to distribute SPDs, SMMs, and SARs electronically might do the following:

Legislative Brief Electronic Distribution of ERISA Disclosures
• Post SPDs, SMMs, and SARs on a company Web site available to all employees.
• Obtain consent to electronically deliver SPDs, SMMs, and SARs from employees and COBRA participants that do not have regular work-related computer access. For example, employees working for a manufacturer in the plant may agree to access the Web site from his or her home computer.
• Send an email notice to all employees that have work-related computer access or that have provided consent each time an SPD, SMM, or SAR is posted on the Web site. Use email features such as return receipt and notice of non-delivery.
• Continue to provide in paper form copies of SPDs, SMMs, and SARs to employees that do not have regular work-related computer access and that have not provided consent.
• Continue to provide in paper form copies of SPDs, SMMs, and SARs upon request free of charge.
Note: The plan administrator is generally not required to distribute SPDs, SMMs, or SARs to each beneficiary under the plan. Therefore, the plan administrator is not required to obtain consent from each beneficiary under the plan (e.g., spouses, dependents). May a plan administrator electronically deliver COBRA notices by placing the information on a company Web site or sending them via email? Yes, the rules allow plan administrators to provide COBRA notices electronically. However, because COBRA notices must be provided via first-class mail to the home address where a spouse or dependent is also covered under the plan, the plan administrator must obtain consent from the spouse or dependent before delivering COBRA notices electronically. Therefore, providing COBRA notices electronically may not be as practical as electronically delivering SPDs, SMMs, or SARs. Please contact your [b_officialname] representative with any questions.
RHK 10/02; JMS 11/08
This [b_officialname] Legislative Brief is not intended to be exhaustive nor should any discussion or opinions be construed as legal advice. Readers should contact legal counsel for legal advice.
Content copyright © 2002-2008 Zywave, Inc. Images copyright © 2000-2004 Getty Images, Inc. All rights reserved.

Sample E-mail Notice for Use with Each Electronic Disclosure
Important Information Regarding Your Benefits
Dear Plan Participant:
As a plan participant, you are entitled to a comprehensive description of your rights and obligations under the [group health plan - list all that apply]. We've recently posted a copy of the summary plan description (SPD) to our Web site at [www.myresourcesite.com]. In order to ensure that you fully understand the benefits available to you and your obligations as a plan participant, it is imperative that you familiarize yourself with the information contained within the SPD.
If you would like to receive a paper copy of the SPD, you may email [[email protected]] or call [444-444-4444] and one will be provided to you free of charge.
[Company Group Health Plan] [Date]
Sample Consent for Electronic Delivery to Beneficiaries and Other Plan Participants without Work-Related Computer Access
Consent to Receive Electronic Notices Name Social Security #
□ Health □ Dental □ Vision □ Other _________ Email Address
Employee Address
City State Zip
I understand that:
1. The following documents and/or notices may be provided to me electronically:
• Summary Plan Descriptions • Summaries of Material Modifications • Summary Annual Reports • COBRA Notices
2. I may provide notice of a revised email address or revoke my consent at any time without charge by sending an email to [[email protected]] or calling [444-444-4444].
3. I am entitled to request and obtain a paper copy of any electronically furnished document free of charge by contacting [[email protected]] or calling [444-444-4444].
4. In order to access information provided electronically, I must have • A computer with Internet access, • An email account that allows me to send and receive emails, • Microsoft Word 2000 (or higher) or Adobe Acrobat Reader 6.0 (or higher).
I hereby agree to electronic delivery of notices provided to me.
Please return to: Attn: HR, ABC Company City, State ZIP
Date Signature
These sample notices are provided as a starting point to develop tailored documents which reflect the procedures followed by the plan administrator. This Legislative Brief is not intended to be exhaustive nor should any discussion or opinions be construed as legal advice. Readers should contact legal counsel for legal advice.

Legislative Brief COBRA Premium Subsidy Answers for Employers: Administration and Eligibility
Under the American Recovery and Reinvestment Act of 2009 (ARRA), certain individuals who are eligible for COBRA continuation health coverage, or similar coverage under State law, may receive a subsidy for 65 percent of the premium. These individuals are required to pay only 35 percent of the premium. The employer may recover the subsidy provided to assistance-eligible individuals by taking the subsidy amount as a credit on its quarterly employment tax return. The employer may provide the subsidy — and take the credit on its employment tax return — only after it has received the 35 percent premium payment from the individual. The following questions and answers reflect guidance from the Internal Revenue Service regarding administration of and eligibility for the COBRA premium subsidy. Additional Legislative Briefs provide information on taxability and recapture, form preparation, and reporting and documentation. Please note that the IRS issued this guidance before recent extensions to the premium subsidy laws were adopted. We have noted where the original guidance is affected by the extensions. Please contact your COBRA Administration representative with any questions. Now that the COBRA Premium subsidy legislation has passed, how is this going to be communicated to the employer/payroll community?The IRS will continue to provide updated information through this Web site as it becomes available. What individuals are eligible for the COBRA subsidy? An assistance-eligible individual can be any COBRA qualified beneficiary associated with the related covered employee, such as a dependent child of an employee, who is covered immediately prior to the qualifying event. The qualifying event for purposes of eligibility for the subsidy is involuntary termination of the covered employee’s employment that occurs during the period beginning September 1, 2008, and ending December 31, 2009February 28, 2010 March 31, 2010. The individual must also be eligible for COBRA coverage, or similar state coverage, during this period. Note: the premium subsidy extension law clarified that COBRA eligibility during this period is no longer a factor, although individuals must timely elect COBRA. In some cases, employees who experienced a reduction in hours before their termination may also be eligible for the subsidy. Is this provision for employees who involuntarily lose their jobs — or will it apply to all employees even if they leave voluntarily?The credit applies only to involuntarily terminated employees and their family members who are qualified beneficiaries. Note: The subsidy now also applies to individuals who lose coverage due to a reduction in hours of employment and were later involuntarily terminated at any time from March 2, 2010 through March 31, 2010 . Is the employer required to provide the COBRA subsidy?The subsidy requirement applies to group health plans that are subject to the Federal COBRA continuation coverage requirements or to similar requirements under State law. If you are an employer with such a plan and you receive a 35 percent payment from an assistance-eligible individual, you are required to make the remaining 65 percent payment. What if the employer’s group health plan is self-insured? Do the subsidy requirements apply?Yes, the subsidy requirements apply to all plans subject to the COBRA requirements, including self-insured plans. In that case, the employer must provide the COBRA coverage if the assistance eligible individual pays 35 percent of the otherwise required premium. The remaining 65 percent is treated as a payment of payroll taxes by the employer maintaining the plan.

Legislative Brief COBRA Premium Subsidy Answers for Employers: Administration and Eligibility
2
What other agencies will provide information about the COBRA subsidy?Information about the COBRA subsidy will also be available through the Department of Labor and the Department of Health and Human Services, which, along with the IRS, share responsibility for the COBRA requirements. Is the COBRA benefit based on the former employee’s insurance coverage? In general, COBRA coverage is based on the same coverage that the individual had at the time of the qualifying event. However, under the COBRA subsidy provision, an employer may offer an assistance eligible individual the option of choosing other coverage that is also offered to active employees and that does not have higher premiums than the coverage the individual had at the time of the qualifying event. Does the subsidy apply to medical and dental plans or medical only? The subsidy is generally available for COBRA continuation coverage under any group health plan, including medical, dental and vision coverage. However, it does not apply to a flexible spending arrangement (FSA) offered under a cafeteria plan. If an employer changes the insurance offered under its group health plan, can the subsidy apply to an assistance-eligible individual’s coverage under the new insurance? Yes, as long as the individual’s coverage under the new insurance qualifies as COBRA continuation coverage and the individual otherwise continues to be eligible for the subsidy. What is the general process by which an assistance-eligible individual applies for the subsidy? A group health plan is required to notify any individual with a qualifying event occurring during the period from September 1, 2008 through December 31, 2009 February 28, 2010 March 31, 2010, of the availability of the subsidy. If an assistance eligible individual already has COBRA coverage in effect on February 17, 2009 (date of enactment), the individual should receive a special notice of the availability of the subsidy. The notices will explain how to apply for the subsidy. What agency is responsible for providing guidance on these notice requirements? The Department of Labor (DOL) is responsible for providing guidance on notices that must be provided about the availability of the subsidy and, if applicable, the special COBRA election period. For more information on the COBRA subsidy notice requirements, visit DOL’s COBRA page at www.dol.gov/COBRA, which contains model notices and other guidance on these provisions. You can also call 1-866-444-3272 to speak with a benefits advisor from DOL’s Employee Benefits Security Administration. How will the COBRA premium subsidy be provided retroactive to September 2008? The COBRA premium subsidy is not retroactive. The earliest it can apply is for the first period of coverage beginning on or after February 17, 2009, the date of enactment of ARRA. In addition, if an individual elects COBRA coverage under the special COBRA election period, the coverage is effective only for the first period of coverage beginning on or after February 17, 2009. In the case of a health plan that provides coverage on a calendar month basis, the first period of coverage is the month beginning March 1, 2009. Can an assistance-eligible individual reduce his or her COBRA premium to 35% immediately, rather than waiting for the notice from the health plan? Yes. The subsidy applies as of an assistance eligible individual’s first period of coverage beginning on or after February 17, 2009. For example, it would apply to the premium for the period of coverage beginning March 1, 2009, in the case of coverage provided on a calendar month basis. However, because the COBRA subsidy provision was only recently enacted, systems to implement the premium reduction might not yet be in place. The assistance-eligible individual would therefore be well-advised to contact the group health plan or employer to discuss the premium reduction before sending in the reduced premium.

Legislative Brief COBRA Premium Subsidy Answers for Employers: Administration and Eligibility
3
Can an employer just reduce an assistance-eligible individual’s premiums to 35 percent, rather than notifying the individual about the subsidy? No, because an individual might not be eligible for the subsidy. For example, the individual might be eligible for coverage under another group health plan and therefore not be eligible for the subsidy. Can an employer pay an assistance-eligible individual’s 35 percent share of the premium, rather than collecting it from the individual? No. The premium subsidy provision does not allow the individual’s 35 percent share of the premium to be paid by the employer. If I am an assistance-eligible individual, is there any other way to get the subsidy besides paying reduced premiums? For example, can I take it as a credit when I file my 2009 tax return? No, the subsidy is provided to an assistance-eligible individual only in the form of reduced COBRA premiums. That is, the assistance-eligible individual only has to pay 35 percent of the premium in order to receive COBRA coverage. The employer is reimbursed for the remaining 65 percent through a credit on its payroll tax returns. Is an employer-initiated layoff an involuntary termination of employment for purposes of eligibility for the COBRA premium subsidy? Yes, an employer-initiated layoff is generally an involuntary termination of employment for purposes of eligibility for COBRA premium subsidy. Are tax-exempt entities subject to this provision? Yes, if the tax-exempt entity is required to provide COBRA continuation coverage. Moreover, an employer that is exempt from Federal income tax is generally subject to federal payroll tax requirements and required to file Form 941. As in the case of taxable employers, a tax-exempt entity can claim credit on Form 941 for the COBRA subsidy it provides. How will the COBRA credit apply in the case of a business acquisition that results in a successor employer? There is no “one size fits all” answer because the result depends on the facts and circumstances, including whether the entity that provided the subsidy continues in existence. The fact that an employer is a successor employer for purposes of applying the social security wage base does not mean that it can claim credit for the subsidy provided by the predecessor employer. Does the COBRA premium subsidy provision apply to employers in Puerto Rico, the U.S. Virgin Islands, Guam, American Samoa and the Commonwealth of the Northern Mariana Islands? Yes. Employers (or multiemployer plans or insurers, as applicable) in Puerto Rico, the U.S. Virgin Islands, Guam, American Samoa and the Commonwealth of the Northern Mariana Islands that are required to provide COBRA continuation coverage are required to provide the subsidy to assistance eligible individuals and can claim credit on Form 941-PR (for Puerto Rico) or Form 941-SS (for American Samoa, US Virgin Islands, Guam and the Commonwealth of the Northern Mariana Islands) for the amount of subsidy provided. When does the premium reduction first apply to an assistance eligible individual? The premium reduction applies as of the first period of coverage beginning on or after February 17, 2009, for which the assistance eligible individual is eligible to pay only 35 percent of the premium (as determined without regard to the premium reduction) and be treated as having made full payment. For this purpose, a period of coverage is a monthly or shorter period with respect to which premiums are charged by the plan. The exact date when the first period of coverage beginning on or after February 17, 2009, begins depends on the period with respect to which premiums are charged by the plan.

Legislative Brief COBRA Premium Subsidy Answers for Employers: Administration and Eligibility
4
Note: This question and answer is based on Q&A-30 of IRS Notice 2009-27. See Q&A-31 and -32 of IRS Notice 2009-27 for additional guidance on the first period of coverage for which the premium reduction applies. How long does the premium reduction apply to an assistance eligible individual? The premium reduction applies until the earliest of (1) the first date the assistance eligible individual becomes eligible for other group health plan coverage (with certain exceptions) or Medicare coverage, (2) the date that is nine15 months after the first day of the first month for which the ARRA premium reduction provisions apply to the individual, or (3) the date the individual ceases to be eligible for COBRA continuation coverage. Note: This question and answer is based on Q&A-33 of IRS Notice 2009-27. See Q&A-34 through -37 of IRS Notice 2009-27 for additional guidance on how eligibility for other group health plan coverage affects eligibility for the premium reduction. IRS Notice 2009-27 provides guidance on whether a termination of employment is involuntary for purposes of the COBRA premium subsidy provision. In what circumstances will the IRS accept an employer’s determination that an employee’s termination of employment was involuntary for purposes of claiming a payroll tax credit for the COBRA premium subsidy provided to the employee? If an employer’s determination that an employee’s termination of employment was involuntary for purposes of the COBRA subsidy provision is consistent with a reasonable interpretation of the applicable statutory provisions and IRS guidance, the IRS will not challenge that determination for purposes of whether the employer is entitled to claim a payroll tax credit for the COBRA premium subsidy provided to the employee. The employer must maintain supporting documentation of its determination that the employee's termination of employment was involuntary for this purpose, including an attestation by the employer of involuntary termination for each covered employee whose involuntary termination is the basis for eligibility for the subsidy. If a health plan is not subject to any “COBRA continuation coverage” requirements as defined for purposes of the COBRA premium subsidy, but the employer voluntarily provides continuation coverage, does the subsidy apply to the voluntary coverage? No. See IRS Notice 2009-27, Q&A-16. The subsidy applies only to premiums for “COBRA continuation coverage” as defined under the COBRA premium subsidy provision. Under this definition, COBRA continuation coverage consists of federal COBRA under the Internal Revenue Code (Code) or the Employee Retirement Income Security Act of 1974 (ERISA), which generally apply to plans of private employers (other than churches) with at least 20 employees, or under the Public Health Service Act (PHSA), which applies to plans of state or local government employers with at least 20 employees; temporary continuation coverage (TCC) under the Federal Employees Health Benefits Program (FEHBP); and state law continuation coverage requirements that are comparable to the Federal COBRA requirements, often referred to as state "mini-COBRA" laws. For example, the subsidy does not apply to premiums for continuation coverage under a church plan (as defined under the Code and ERISA) that is exempt from the COBRA requirements under the Code and ERISA and is also not subject to any comparable State law requirements. Similarly, the subsidy does not apply to premiums for continuation coverage under a governmental plan (as defined under the Code and ERISA) maintained by a federal instrumentality the employees of which are not covered by FEHBP, or to a plan maintained by an Indian tribal government that satisfies the requirements for a governmental plan (as defined under the Code and ERISA).

Legislative Brief COBRA Premium Subsidy Answers for Employers: Administration and Eligibility
5
If an insurer provides continuation coverage that is required under state law and is otherwise comparable to federal COBRA coverage, does it fail to be “COBRA continuation coverage” as defined under the COBRA premium subsidy provision merely because it is provided after the employer has gone out of business and the employer’s group health plan has been terminated? No. If the continuation coverage is required under state law and is otherwise comparable to federal COBRA coverage — that is, the coverage is substantially similar to the coverage that was previously provided under the group health plan and is provided at a monthly cost that is based on a specified percentage of the group health plan's cost of providing such coverage — then it qualifies as COBRA continuation coverage that is eligible for the premium subsidy even after the employer has gone out of business and the group health plan has been terminated. In the case of an employee who is hired only for a limited period, such as a seasonal worker, or a teacher hired only for one school year, can the end of employment at the end of the period be considered an involuntary termination? Yes. Under IRS Notice 2009-27, Q&A-1, an involuntary termination may include the employer’s failure to renew a contract at the time the contract expires, if the employee was willing and able to execute a new contract providing terms and conditions similar to those in the expiring contract and to continue providing the services. Thus, if an employee hired for a limited period works to the end of the period, is willing and able to continue employment, and terminates employment because of the failure of the employer to offer additional work, an involuntary termination occurs for purposes of the premium subsidy. Is an elected official involuntarily terminated at the completion of his or her term of office if the official ran for reelection and was not reelected? Yes. Is an elected official who is prohibited from running for reelection because of term limits involuntarily terminated at the completion of his or her term of office? Yes. Is an elected official who is eligible to run for reelection, but chooses not to, involuntarily terminated at the completion of his or her term of office? No. This is the result even if the official does not run for reelection because of health or other reasons. If an employee’s eligibility for health coverage under a multiemployer plan is based on a minimum number of hours of covered employment, can the employee become an assistance-eligible individual if the employee’s involuntary termination by an employer contributing to the plan results in the employee’s failing to satisfy the minimum hours requirement and losing coverage? If so, how does subsequent employment with one or more employers contributing to the plan affect the employee’s eligibility for the premium subsidy? If an employee covered by a multiemployer health plan is involuntarily terminated by an employer contributing to the plan, resulting in a reduction in the employee’s total number of hours of covered employment, which causes the employee to lose coverage and become eligible for COBRA, the employee can be an assistance-eligible individual (and eligible for the COBRA premium reduction) if the involuntary termination and COBRA eligibility occur during the period from September 1, 2008 through December 31, 2009February 28, 2010 March 31, 2010, and the individual elects COBRA coverage. This is the case even if the loss of coverage and eligibility for COBRA do not occur immediately after the involuntary termination, for example, because the employee has “banked” hours at the time of the involuntary termination. In addition, the employee does not become ineligible for the premium subsidy merely because of subsequent employment with one or more employers contributing to the plan, provided that the employee continues COBRA coverage and does not otherwise become disqualified. However, if the employee works enough hours to become eligible again for active

Legislative Brief COBRA Premium Subsidy Answers for Employers: Administration and Eligibility
6
coverage, eligibility for the premium subsidy ends when active coverage under the plan begins and COBRA coverage ends. Note: the premium subsidy extension law clarified that COBRA eligibility during this period is no longer a factor, although individuals must timely elect COBRA. Does an involuntary termination of employment occur if a member of a military Reserve unit or the National Guard who is employed by a civilian employer is called to active duty? Yes. This is the case regardless of whether the civilian employer otherwise treats the employee’s absence as a termination of employment or a leave of absence. Does eligibility for the COBRA premium reduction end if an assistance-eligible individual is eligible for or covered by TRICARE health coverage provided for members of the military and their families? No. Eligibility for coverage or coverage by TRICARE health coverage does not end an assistance-eligible individual’s period of premium subsidy. See McGee v. Funderburg, 17 F.3rd 1122 (8th Cir. 1994). If an individual who did not have a COBRA election in effect on February 17, 2009, is eligible for the extended Federal (or FEHBP) COBRA election period and elects COBRA coverage during that period, does the individual’s COBRA coverage have to be effective with the first period of coverage beginning on or after February 17, 2009? An individual who is eligible for the extended Federal (or FEHBP) COBRA election period must be offered COBRA coverage that is effective with the first period of coverage beginning on or after February 17. 2009. See IRS Notice 2009-27, Q&A-52. However, the employer or health plan may also allow the individual to elect COBRA coverage to be effective as of a later date. In that case, however, for purposes of the 15-month limit on eligibility for the premium subsidy, the 15-month period would begin with the first period of coverage beginning on or after February 17, 2009. In addition, under ARRA, the period starting with the involuntary termination and ending with the first day of the first period of coverage beginning on or after February 17, 2009, is disregarded in determining whether a break in coverage has occurred for purposes of limiting preexisting condition exclusions under subsequent group health plan coverage. However, if an individual elects COBRA coverage to be effective as of a later date, the period between the first day of the first period of coverage beginning on or after February 17, 2009, and the date when COBRA coverage is effective is not disregarded for purposes of the rules limiting preexisting condition exclusions. Notice 2009-27, Q&A-51, provides that the premium subsidy can apply to coverage provided under state requirements pursuant to a special election period similar to the extended federal (or FEHBP) COBRA election period. If state COBRA law is amended to provide such an election period, does the COBRA premium subsidy apply to coverage elected during such a period, and, if so, even if the coverage offered during such a period begins later than the first period of coverage beginning on or after February 17, 2009? If state COBRA law is amended to provide a special election period similar to the extended federal (or FEHBP) COBRA election period, the COBRA premium subsidy applies to coverage elected during such a period. Such state law can require coverage offered during such a period to be effective with the first period of coverage beginning on or after February 17, 2009, or allow it to be effective as of a later date. However, as discussed in question above, if an individual is eligible for COBRA coverage effective with the first period of coverage beginning on or after February 17, 2009, and elects COBRA coverage to be effective as of a later date, the 15-month limit on eligibility for the premium subsidy would begin with the first period of coverage beginning on or after February 17, 2009. In addition, depending on state law, the delay in the beginning of COBRA coverage could affect the application of preexisting condition limitations.

Legislative Brief COBRA Premium Subsidy Answers for Employers: Administration and Eligibility
7
If an assistance-eligible individual has the option of paying his or her COBRA premiums on a pretax basis under a health reimbursement arrangement (HRA), can the individual’s 35 percent share of the premium be paid from the HRA? COBRA premiums paid on a pretax basis from an HRA are treated as paid by the employer and are not taken into account in determining whether an individual has paid his or her 35 percent share of the COBRA premiums. See IRS Notice 2009-27, Q&A-22, Example 2. Therefore, the individual is not treated as paying the 35 percent and the subsidy does not apply.
Source: Internal Revenue Service
(6/09; KMP 3/10)
This [b_officialname] Legislative Update is not intended to be exhaustive nor should any discussion or opinions be construed as legal advice. Readers should contact legal counsel for legal advice. Content copyright © 2009-2010 Zywave, Inc. Images copyright © 2000 Getty Images, Inc. All rights reserved.

significant variation in what accounts for that extra cost. While medical supplies have remained fairly stable, there has been con-siderable fluctuation involving labor costs, and costs for other operating expenses, such as utilities, professional fees, insurance, rent, interest, bad debt, and taxes.
Hospital ExpensesThe average expenses per inpatient day range from under $900 to nearly $2,400 a day and include all operating and nonoperating costs, based on 2007 data.
RANK AVERAGE EXPENSES PER INPATIENT DAY United States $1,6961 District of Columbia $2,3812 Oregon $2,3363 Washington $2,3324 California $2,2505 Maryland $2,1136 Massachusetts $2,1137 Alaska $2,1048 Arizona $2,0399 New Jersey $2,01410 Colorado $1,99811 Connecticut $1,98812 Utah $1,95913 Rhode Island $1,92314 New Mexico $1,90015 Nevada $1,87516 New Hampshire $1,85417 Indiana $1,84918 Ohio $1,83319 Texas $1,80620 Illinois $1,79921 Delaware $1,77822 Missouri $1,76823 Maine $1,72924 Wisconsin $1,68225 New York $1,67326 Florida $1,65227 Idaho $1,64328 Michigan $1,64229 Pennsylvania $1,62630 Virginia $1,62231 South Carolina $1,55732 Hawaii $1,55633 Minnesota $1,50034 Vermont $1,43435 North Carolina $1,43336 Oklahoma $1,42437 Louisiana $1,41738 Tennessee $1,39639 Kentucky $1,39040 Arkansas $1,35341 Alabama $1,33242 Georgia $1,27943 Nebraska $1,25044 Mississippi $1,17945 West Virginia $1,17646 Iowa $1,13247 Kansas $1,09348 Montana $97549 North Dakota $95850 Wyoming $88751 South Dakota $869
SOURCe: Kaiser Family Foundation.
Upcoming Topic:» Cancer
Hospital expenses per adjusted discharge (wage index and case mix index adjusted) have been fairly steady over the past few years, increasing at an annual rate of 3%. In 2005, that expense was about $6,500. By 2008, it had grown 11% to about $7,250. But within that overall expense, there has been H
Inflation and Expense Trends
$S
PO
NS
OR
eD
SU
PP
Le
Me
NT
Composition of ExpEnsE Growth
jUNE 2009
faCt filE partnEr:
FAcT FIlE
thomsonreuters.com/healthcare
NOTe: Data based on quarterly data submission, average 470 hospitals. SOURCe: Thomson Reuters.
2005--2006
2006--2007
2007--2008
-$20 $0 $20 $40 $60 $80 $100 $120 $140 $160
(NUMBeR IN DOLLARS)
nOtheroperatingnLabornDrugsnNonmedicalsuppliesnMedicalsupplies
The key factors responsible for growing the cost of hospital expenses per adjusted discharge have varied considerably since 2005. For example, between 2005 and 2006, the largest component of growth was labor, which added an extra $84 per discharge. Drugs represented $9 of the overall increase. Other operating expenses—such as utilities, professional fees, insurance, rent, interest, bad debt, and taxes —were responsible for another $54.
A year later, labor again grew significantly, but it was the “other operating” expense category that grew the most, adding $159 to the total increase.
Between 2007 and 2008, the only growing expense was medical supplies. Hospitals are using resources more efficiently as average length of stay (case mix index adjusted) decreased 2.6% between 2007 and 2008, from 3.64 to 3.55 days.
$54
$84
$9
$2
$15
$159
$133
$7
$4
$20
$(11)
$(6)
$(6)
$(5)
$21

FAcT FIlE
$
hospital ExpEnsEs show stEady Growth … expenses per adjusted discharge have been increasing at an annual rate of 4.2% (wage index adjusted) and 3.0% (wage index and case mix index adjusted). The difference in inflation rates can be thought of as contribution of increased acuity to cost (1.2% annually).
SOURCe: Thomson Reuters.
$10,000
$9,500
$9,000
$8,500
$8,000
$7,500
$7,000
$6,500
$6,000
(EXP
ENSE
SPE
RAD
JUST
EDD
ISCH
ARGE
)
2005Q2 2005Q3 2005Q4 2006Q1 2006Q2 2006Q3 2006Q4 2007Q1 2007Q2 2007Q3 2007Q4 2008Q1 2008Q2 2008Q3 2008Q4
nWageindexadjustednCasemixandwageindexadjusted
$8,162 $8,204$8,465 $8,483 $8,613 $8,466
$8,764 $8,721 $8,753 $8,921$9,229 $9,249
$9,156 $9,326$9,534
$6,516 $6,606$6,810 $6,794 $6,858 $6,882
$7,113 $7,124 $7,104$7,294 $7,230 $7,182 $7,102 $7,284 $7,277
… But ratE of inCrEasE diminishEs Inflation of expenses is diminishing near the end of 2008, following an increase in 2007, Q3. Hospitals appear to be reducing cost growth as the recession (beginning in 2007, Q4) progresses.
SOURCe: Thomson Reuters.
7.0%
6.0%
5.0%
4.0%
3.0%
2.0%
1.0%
0.0%
-1.0%(EXP
ENSE
SPE
RAD
JUST
EDD
ISCH
ARGE
:ANN
UAL
%C
HANG
E)
2006Q2 2006Q3 2006Q4 2007Q1 2007Q2 2007Q3 2007Q4 2008Q1 2008Q2 2008Q3 2008Q4
nWageindexadjustednCasemixandwageindexadjusted
5.50%
5.20%
3.20% 3.50%2.80%
1.60%
5.30%
6.00%
4.60%
4.50%
3.30%5.40%4.20% 4.50%
4.90%
3.60%
6.00%
1.70%0.80%
0.00% -0.10%0.60%
laBor and nonlaBor ComponEnts havE similar Growth ratEs … Labor and nonlabor expense components have similar inflation rates, 2.9% and 3.4% respectively, and are roughly equal in size.
SOURCe: Thomson Reuters.
$4,100
$3,900
$3,700
$3,500
$3,300
$3,100
$2,900
$2,700
$2,500
(EXP
ENSE
SPE
RAD
JUST
EDD
ISCH
ARGE
)
2005Q2 2005Q3 2005Q4 2006Q1 2006Q2 2006Q3 2006Q4 2007Q1 2007Q2 2007Q3 2007Q4 2008Q1 2008Q2 2008Q3 2008Q4
nLabor(casemixandwageindexadjusted)nNonlabor(casemixindexadjusted)
$3,090
$3,798
…and similar diminishinG inflation ratEs in rECEnt pEriodsBoth labor and nonlabor inflation rates are slowing in parallel.
SOURCe: Thomson Reuters.
8.0%
7.0%
6.0%
5.0%
4.0%
3.0%
2.0%
1.0%
0.0%
-1.0%
-2.0%(EXP
ENSE
SPE
RAD
JUST
EDD
ISCH
ARGE
:ANN
UAL
%C
HANG
E)
2006Q2 2006Q3 2006Q4 2007Q1 2007Q2 2007Q3 2007Q4 2008Q1 2008Q2 2008Q3 2008Q4
nLabor(casemixandwageindexadjsted)nNonlabor(casemixindexadjusted)
7.40%
5.30%
$3,162
$3,361$3,283 $3,318 $3,375 $3,433 $3,456 $3,471
$3,529 $3,486 $3,480 $3,434$3,508 $3,949
$3,354$3,475 $3,459
$3,519 $3,533 $3,559 $3,640 $3,702 $3,692$3,804 $3,741 $3,760
$3,700$3,840
6.70%
2.10%
5.30%4.60%
4.60%
1.50%
0.70%-1.10% -0.60%
0.20%
2.40%
5.20%
5.20%4.50%
6.90%
2.80%
1.60%0.20%
-0.10%
2.60%