Embed Size (px)
Citation preview

Special Article
Clear Lens Extraction for Axial Myopia
An Appraisal
MORTON F. GOLDBERG, MD
Abstract: Optional surgery requires a higher degree of safety than that performed for medical necessity. This ethical principle is particularly applicable to axial myopes, who have higher-than-normal rates of operative and postoperative complications if they undergo lens extraction. Moreover, several noninvasive, extraocular, and reversible techniques now exist for the correction of myopia. Currently, it would appear that the possible optical benefits of clear lens extraction in axial myopia are usually outweighed by the severity of the risks and by the availability of safer alternatives. [Key words: cataract, clear lens extraction, cystoid macular edema, epikeratophakia, myopia, refractive error, retinal detachment.] Ophthalmology 94:571-582, 1987
There has been a traditional reluctance and, indeed, trepidation, to perform intraocular surgery on eyes with extreme axial myopia, even when such eyes have diseases requiring therapy. Recently, it has been proposed that optical improvement in highly myopic eyes should be attempted via extraction of a clear lens. Presumably, there are exceptional patients whose emotional or financial stability is so threatened by their demonstrated inability to wear contact lenses or spectacles that invasive surgical risks, some of which are sight-threatening, might be worth taking (assuming that the patient is competent to give truly informed consent). As in most clinical decision making, therapy must be individualized for each patient.
From the Department of Ophthalmology, University of Illinois College of Medicine at Chicago.
Supported in part by training grant 7038 and core grant 1792 from the National Eye Institute, Bethesda, Maryland, and by an unrestricted research grant from Research to Prevent Blindness, Inc., New York.
Presented at the American Academy of Ophthalmology Annual Meeting, New Orleans, November 1986.
The statements are the opinion of the author and represent the substance of a point-counterpoint "debate" held at the 1986 Annual Meeting of the American Academy of Ophthalmology.
Reprint requests to Morton F. Goldberg, MD, Department of Ophthalmology, Eye and Ear Infirmary, 1855 West Taylor Street, Chicago, IL 60614.
But, before advising clear lens extraction in axial myopia, we should carefully evaluate what can be learned from the natural course of such eyes without surgery, the known risks of cataract extraction in any eye, the risks of cataract extraction in myopic eyes, the current knowledge of clear lens extraction in axial myopia, and the available (or soon-to-be available) noninvasive alternatives.
THE NATURAL COURSE OF UNOPERATED AXIAL MYOPIA
High myopia, associated with axial elongation of the globe, has a notorious reputation for causing blinding complications, even when such eyes are unoperated. In highly myopic eyes, for example, the volume of the globe may be increased by over 50%,1 and the presence of posterior staphylomata may alter the globe's symmetry considerably. As a result, there are varying degrees of traction on, stretching of, and degeneration of the retina. The vitreous is often totally or partially detached and syneretic, and there is a high incidence of very thin sclera, open angle glaucoma, lattice degeneration of the retina, atrophy of the retina and choroid, retinal holes and tears, macular hemorrhages, macular scarring, and macular holes. Terms such as malignant myopia and progressive myopia have been used to emphasize the severity of some of these problems.
571

OPHTHALMOLOGY • MAY 1987 • VOLUME 94 • NUMBER 5
Adding to the evidence that incriminates myopia in the pathogenesis of RD is its marked over-representa-tion in the RD population. Myopia affects 35 to 79% of
0.75 o.s8oll patients with RD, whereas the incidence of myopia in
.... c Cll 0.50 C)
"' Cll ll.
0.25
0.002'1 0.00
H.75D to
Plano
0.020'1
Plano to
-•.75D
0.080'1
-5.000 to
-9.75D
Refractive Error
> -IO.OOD
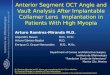
Fig 1. Influence of myopia on rates of phakic retinal detachments.
A large body of epidemiologic evidence incriminates axial myopia as a leading cause ofvitreoretinal degeneration and retinal detachment (RD). Retinal breaks, for example, affect about 6% of the general population, but the incidence almost doubles (to about 11%) in asymptomatic myopic eyes.2·3 As the myopia increases, so does the prevalence of retinal breaks, and the type ofbreak is disproportionately of a more serious kind. Although atrophic holes occur about twice as commonly in the myopic eye as compared with the nonmyopic eye, tractional tears in the retina are about five times more common in the myopic eye.4 Furthermore, most giant tears occur in highly myopic eyes.4
Although RD develops in only about 0.005 to 0.010% ofphakic individuals3
•5 annually (5-10 per 100,000 pop
ulation, or about 1 per 10,000 to 20,000 individuals), the frequency rises to about 1% (and possibly much higher) for phakic myopes, depending on the reported series4 (a roughly 100-fold, or higher, increase). This rise is similar in magnitude to that conferred by extracapsular cataract extraction (ECCE), per se, in the general population. These increased rates are at least partially additive. The higher the myopia, the greater the probability of retinal detachment. 6•
7 Perkins studied the probability of phakic RD for var
ious refractive errors, using data from Moorfields Eye Hospital, and predicted the following annual incidence rates: 0 to +4.75 diopters (D), 0.002%; 0 to -4.75 D, 0.02%; -5.00 to -9.75 D, 0.08%; and greater than -10.00 D, 0.68%6 (Fig 1). The incidence in very high myopia is approximately 34 times greater than that in low myopia. Older data also suggest that when the refractive error is greater than -10 D, the frequency of phakic RD is about 45 times greater than for nonmyopes.8 The estimated lifetime risk of RD in persons with myopia greater than -5.00 D who live to be age 60 is about 2.4%, compared with 0.06% for emmetropes,4 a roughly 40-fold increase. Furthermore, RD in high myopia occurs at a younger age than in the non-myopic population. 9•
10
572
the general white population of European origin is only about 5 to 18%.4·6-
8
THE RISKS OF CATARACT SURGERY REGARDLESS OF REFRACTIVE ERROR
As a result of cataract surgery, either intracapsular or extracapsular, definite degenerative changes occur in the vitreous. In axially myopic eyes, these changes more often eventuate in retinal breaks and detachments than in non-myopic eyes.
HISTOPATHOLOGY OF EYES HAVING HAD CATARACT SURGERY
McDonnell et al 11 histopathologically studied 146 eyes that had undergone intracapsular cataract extraction (ICCE), 30 eyes with various refractive errors that had had ECCE with surgical discission of the posterior capsule, and 25 eyes with ECCE and intact posterior capsule. Posterior vitreous detachment occurred in 84, 76, and 40%, respectively. Macular edema was found in 2.1, 4.0, and 0% of these eyes; epiretinal membranes were noted in 12.3, 8.0, and 6.7%.
Thus, although the intracapsular technique was associated with the highest complication rates, the extracapsular approach, even with an intact posterior capsule, was also associated with potentially important vitreous and retinal changes.
CLINICAL OBSERVATIONS
Retinal detachment. Aphakia and, to a somewhat lesser extent, pseudophakia are major risk factors for the development of RD, even in the absence of myopia (though myopia worsens the risk; see below). Rhegmatogenous RD develops in approximately 0.005 to 0.01% of all phakic eyes, versus 1 to 3% of all aphakic eyes having had ICCE (i.e., an approximately 100-fold increase in this type ofaphakia). 12-14 Moreover, Hawkins15 studied such aphakic eyes (which compose only about 2.9% of all adult eyes) and calculated that as many as 35% of all RDs developed in those eyes.
Folk and Burton, 16 emphasizing the causative role of lens extraction in inducing RD, noted that "patients with unilateral aphakia and an ipsilateral detachment had a low risk of detachment in the phakic fellow eye, but this risk rose significantly if the lens was removed" (mostly by ICCE). Benson and associates17 similarly found that the frequency of RD in the fellow eye of patients with a history of contralateral RD increased almost four times after ICCE in comparison with those eyes that remained phakic (26 versus 7% ). In 1985, Coonan et al 18 showed that the incidence of RD in aphakic patients with a history of contralateral RD was

GOLDBERG • CLEAR LENS EXTRACTION
as high as 5.9%, even when an extracapsular procedure was done.
Coonan and colleagues18 reported results from a prospective study of 842 consecutive ECCEs. Of these, about one third had intraocular lens implants (IOLs) inserted (mostly in the posterior chamber [PC]). The overall incidence of RD was 1.4%. The incidence was 0.8% if the posterior capsule was intact and there were no surgical complications. In eyes requiring secondary capsulotomy, RDs occurred in 3.2%, a threefold increase over the incidence in eyes having intact posterior capsules.
The overall surgical complication rate was 7 .4%. Vitreous loss occurred in a substantial proportion (4.2%) of cases, and of these, RD developed in 8%. Vitreous loss thus increased the rate of RD approximately tenfold compared to eyes with intact posterior capsules. Previous studies of RD rates after different types of ECCE (Jaffe and co-workers, 19 0.66%; Girard,Z0 1.7%; Wetzig et al,21 0.45%; Hurite and associates,22 1.6%; Kratz,23
0.02%; and Binkhorst,24 1.0%) could well have underestimated the rate of RD. The studies either purposely omitted high risk patients (such as those being considered for clear lens extraction) or operative complications or lacked appropriate follow-up.
In 1978, Wilkinson et al25 reported RD rates after phacoemulsification of 1500 consecutive eyes. RDs developed in 3.6%. Vitreous loss occurred in 4.2%, and in this group of eyes, the incidence of RD was 14% (a fourfold increase compared to eyes without vitreous loss). Of the 3.6% of eyes sustaining RD, the vast majority had posterior capsule surgery performed at the time ofphacoemulsification. The detachment rate was higher than in previous reports, probably due to the follow-up, which was longer than in many of the older studies. Even this comprehensive study by Wilkinson and colleagues, however, must have underestimated the RD rate because 685 of the 1500 patients who underwent phacoemulsification (46%) had a follow-up interval of less than 1 month.
( 1) Delayed development of RD. It has been claimed that rates of RD after ECCE or clear lens removal are acceptably low,Z6 and that follow-up intervals limited to approximately 1 year are valid for purposes of judging the incidence of RD after such operations. Thus, RD rates of0.02 to 3.6% occurring during the first year after ECCE have been considered representative oflong-term results18 and acceptable. In fact, many RDs develop after this initial postoperative interval, but nevertheless can be blamed on the aphakic or pseudophakic status, especially in high myopia (Table 1). This delayed development is particularly important when one considers lens removal in young individuals with extended life spans.
Folk and Burton 16 found, for example, that the average duration of aphakia before the onset of an RD was between 43 and 54 months. Of these eyes, 44% did not detach until after 24 months of aphakia. Ashrafzadeh and co-workers27 found that slightly over half of aphakic RDs occurred after 1 year. Similar results were reported
Table 1. Duration of Aphakia Longer Than 1 Year Before Diagnosis of Retinal Detachment
Reference
Ashrafzadeh et al, 197327
Folk and Burton, 198316
Ho and Tolentino, 198429
Jaffe et al, 198419
%of Eyes
51 66 43 62.5
Table 2. Retinal Detachment after Prophylactic Obliteration of Retinal Breaks in Phakic High Myopia
Reference
Kanski and Daniel, 197534
Stein et al, 197239
Yanoff, 197735
Robertson and Norton, 197336
cf. Campbell & Rittler, 197238
(Aphakic)
%of Eyes
1.0-13.7 2.5 3.0 6.0
41.3
by Winter and Dannheim.28 Ho and Tolentino29 noted that RD developed in eyes (after the eyes have had ECCE and implantation of a PC IOL) after a 12-month postoperative interval in 43% of instances. In the series reported by Jaffe et al, 19 five of eight aphakic RDs occurred later than 1 year after cataract extraction.
Furthermore, opening of the posterior capsule is often substantially delayed.3° Follow-up for RD must be even more careful and prolonged once capsulotomy is performed because after an opening in the capsule is made, either by knife or by laser, the risk of subsequent RD is increased. Long-term follow-up is essential to assess the safety of clear lens extraction quantitatively, especially in very young individuals and high myopes,22·31·32 with or without posterior chamber IOLs. Available evidence indicates that RD after lens extraction is a potential late complication.
(2) Equivocal benefits of prophylaxis of RD. Verzella33 has claimed that prophylactic photocoagulation can prevent RD in high myopes. This is an over-simplication.
Prophylactic treatment of retinal breaks in high myopia is thought to be "indispensable" by Curtin,4 but data proving its safety and effectiveness are limited. Prophylactic therapy may not only fail to eliminate RD, but may also contribute to its development and to other visually disabling complications, such as macular pucker. The incidence of RD after prophylactic treatment of retinal breaks ranges from 1 to 13.7% of 2459 eyes collected from ten clinical series34 (Table 2). Kanski and Daniel reported a 4. 7% incidence in their personal series of 70 1 eyes treated with cryotherapy and photocoagulation.34 New retinal breaks occurred in 8% of treated eyes, and 3% lost two or more lines of vision. Causes of visual loss included macular edema or pucker, keratopathy, and anterior segment necrosis. Over one
573

OPHTHALMOLOGY • MAY 1987 • VOLUME 94 • NUMBER 5
third of the RDs occurred in nontreated areas of the retina, and 25% of retinal breaks were located in areas that were previously free of clinically suspicious vitreoretinal lesions. Despite prophylactic cryocoagulation in 100 eyes, Yanoff noted three subsequent RDs. 35
Robertson and Norton36 used either photocoagulation or cryocoagulation to treat 301 eyes with retinal breaks. New retinal breaks occurred in 8%, and RD was diagnosed in 6%. Benson et al37 noted several types of complications after prophylactic cryotherapy of lattice degeneration, including the following: flap tears torn free from the treated retina; retinal tears posterior to the treated area; operculated tears arising in a previously flat treated area; flap tears that arose in and extended through an area of treatment; and flap tears in areas of retina that appeared clinically normal, 180° away from a treated area.
Campbell and Rittle~8 used prophylactic cryotherapy and laser photocoagulation in eyes in which RD would likely develop. Although they suggest that their results were better than without any intervention, RDs occurred in as many as 31 of 75 (41.3%) cases, despite prophylaxis before cataract extraction. In virtually all of these eyes, breaks developed in retinal areas that previously appeared to be normal. Often the breaks were both peripheral and posterior; they were located near previous treatment sites and in remote areas; and several were actually within previously treated areas. It is thus impossible to eliminate prophylactically all areas of potential retinal break formation before cataract extraction because these areas cannot be reliably identified by ophthalmoscopic criteria.
An attempt to treat the entire retinal circumference was carried out by Stein et al,39 who studied 374 highly myopic eyes before cataract extraction (including 28 eyes scheduled for clear lens extractions). Retinal holes developed in the posterior pole of nearly 30% of eyes, including macular holes. The inability to differentiate dangerous from innocent retinal lesions was again apparent. Despite extensive chorioretinal adhesions, the rate of postoperative RD remained substantial (2.5%), though apparently reduced in comparison with nontreated (but nonrandomized) eyes.
Ramen and Singer40 found that RD still developed in 3.2% ofphotocoagulated eyes (aphakic and phakic; myopic and nonmyopic). They also noted that new breaks developed far from previously treated areas. Saracco et al41 performed circumferential argon laser photocoagulation in 300 of 600 eyes that were already aphakic. Retinal detachment developed in only 0.33% versus 2% of untreated (but nonrandomized) eyes.
Davis42 studied 222 phakic and aphakic eyes with retinal breaks not undergoing prophylactic obliteration. In the case of breaks with free-floating opercula and holes without opercula in patches of lattice degeneration, results of prophylaxis culled from the literature did not demonstrate any significant improvement in comparison with the untreated eyes in his series. With regard to flap tears, however, eyes treated prophylactically and reported by others elsewhere in the literature progressed
574
to RD less often than did the untreated eyes described by Davis.
Robertson and Priluck43 performed 360° of prophylactic cryocoagulation but nevertheless found that RD developed in two of six eyes before cataract extraction. Preretinal membranes were noted in three of the six eyes. In other studies, the incidence of macular pucker has ranged from 0 to 3% after photocoagulation and from 0 to 1% after cryocoagulation. 36
•44 Visual acuity
was noted to worsen in 4% of 231 eyes treated prophylactically with photocoagulation or cryocoagulation by Chignell and Shilling.45
In summary, prophylactic therapy (photocoagulation or cryocoagulation) of vitreoretinal lesions known to predispose to RD may be indicated in some highly myopic eyes before cataract surgery. But properly randomized, prospective clinical trials have not yet been carried out, and the appropriate use or possible value of prophylaxis cannot be stated with certainty at this time. Furthermore, prophylaxis is not universally successful and it induces its own set of visually disabling potential complications, including RD itself. Removal of the lens creates a finite additional risk of postoperative RD, especially in axial myopia. Despite prior prophylaxis in predisposed eyes, this risk is substantially higher than in similar but phakic eyes. 38
•39
(3) Results of RD surgery in aphakia. As many other retinal consultants46
-52 have pointed out, the peripheral
view of the fundus is not optimal after extracapsular cataract surgery, with or without posterior chamber IOLs, even when the surgery is technically well done. This is true when pupillary dilation is normal and when the posterior capsule is free of opacifications. Frequently, however, the pupil does not dilate fully, and there are translucent or opaque peripheral opacifications in the posterior lens capsule.
In a series of 252 pseudophakic RDs, Freeman et al53
could not find retinal breaks in 18%. Under the best of circumstances, the optics of the IOL do not allow clear visualization of the oral region with the Goldmann contact lens because as Irvine has pointed out, 54 the observer must look at the fundus tangentially through the relatively flat IOL from one edge.
Despite technically excellent cataract surgery and despite prophylactic photocoagulation or cryocoagulation before cataract surgery, RDs continue to occur postoperatively, especially in eyes with axial myopia. To help determine if the risk of clear lens extraction is worth taking, it is important to know the anatomic and visual results of surgical repair of those RDs that occur after cataract extraction (Table 3). For example, in a series of 122 consecutive cases of pseudophakic RD reported by Ho and Tolentino,55 the overall success rate was 82%. The reattachment rate was highest in a small group of eyes having PC IOL implants (all14 eyes ofthis small subset were successfully reattached), but postoperative vision was less than 20/40 in 50% of these eyes. Significant lenticular and capsular remnants were observed in approximately 7% of all eyes having undergone extracapsular types of extractions. Retinal breaks were not

GOLDBERG • CLEAR LENS EXTRACTION
found in about 7% of such eyes. A substantial number of eyes (21%) having undergone implantation of PC IOLs plus ECCE required more than one buckling procedure.
Ruben and Rajpurohit56 studied aphakia when superimposed on myopia and compared visual acuities in eyes after retinal surgery with those in eyes not requiring retinal surgery. There was an almost fourfold increase in the rate of legal blindness, and over 80% of eyes having undergone retinal surgery had postoperative acuities worse than 20/60.
In a series of 1350 aphakic and pseudophakic eyes with RDs (580 of which had PC IOLs), Tasman57 found that the reattachment rate was only 78%, and a high proportion (74%) of patients had visual acuity of 20/50 or worse after retinal reattachment, even though retinal breaks could be found in most patients. Failure to reattach the retina was usually due to proliferative vitreoretinopathy, which appeared to be more common in pseudophakic eyes than in aphakic eyes.
Snyder et al51 reported more favorable retinal reattachment results, with success rates of 97% in both aphakia and pseudophakia. However, acuity results were significantly worse with pseudophakic than with aphakic RDs.
Sethi et al58 reported a series of 1200 IOL implants with a postoperative RD rate of 1.5%. All patients had intracapsular lens extractions with primary lens implants of the iris plane or iris clip type. The success rate for retinal reattachment was 88%, but 77% had visual acuity of 20/50 or worse.
In the series of 252 pseudophakic RDs reported by Freeman et al, 53 80% of retinas were reattached. Postoperative visual acuity was 20/50 or worse in 65% of eyes. Most eyes had had intracapsular surgery, and a variety of implants had been used.
In a series of 94 pseudophakic RDs, poor visibility of the fundus and initial surgery failures forced Hagle~9 to perform multiple surgical procedures in 30 cases (31.9%). Eventually, the reattachment rate and the degree of visual improvement were comparable to those of an aphakic series. As in the series of Freeman et al, 53
most eyes had intracapsular surgery, and several types of implants had been used.
In 1986, Wilkinson60 reported results of retinal reattachment surgery after cataract extraction (mostly extracapsular) and IOL implantation (using different types of implants) in 154 eyes. The anatomic success rate was similar to that reported by the same author after repair of aphakic RDs.61 However, there were substantial exclusions in the later report, including 40 eyes requiring primary vitrectomy, those with a history of an unsuccessful buckling procedure, and so on. Over 90% of the eyes included in the primary buckling series had retinal reattachment, but about 48% of eyes achieved less than 20/50 vision postoperatively. All of the failures in this series were caused by proliferative vitreoretinopathy, and most demonstrated preretinal membranes preoperatively. Wilkinson noted that the anterior and posterior surfaces of the IOLs produced disturbing reflexes, which reduced the view of the fundus. Deposits on the implant
Table 3. Visual Results after Repair of Retinal Reattachment
Campbell and Rittler, 197238
Ho and Tolentino, 198429
ECCE and PC IOL Ruben and Rajpurohit, 197656
ICCE and ECCE Tasman, 198357
Aphakia and psuedophakia Sethi et al, 198358
ICCE and iris-clip IOL Freeman et al, 197953
Pseudophakia, several types Wilkinson, 198660
Pseudophakia, several types Winter and Dannheim, 198528
Pseudophakia, several types Coonan et al, 198518
Phacoemulsification
Visual Acuity of Eyes (%)
<20/40 (44)
<20/40 (50)
<20/60 (80)
<20/50 (74)
<20/50 (77)
<20/50 (65)
<20/50 (48)
<20/50 (58)
<20/50 (59)
ECCE = extracapsular cataract extraction; PC IOL = posterior chamber intraocular lens; ICCE = intracapsular cataract extraction.
surfaces and the relatively opaque vitreous debris frequently associated with implants also inhibited fundus visualization. Retained peripheral lens cortex and capsule material, along with a miotic pupil, further aggravated the situation. Placement of intraocular gas at the time of vitrectomy surgery for proliferative vitreoretinopathy was compromised by the presence of an IOL. Because of difficulty visualizing the peripheral, detached retina, extensive cryotherapy and larger buckles were more frequently required in pseudophakic eyes than in aphakic eyes. Wilkinson concluded that pseudophakic eyes with RDs recovered less vision than identical aphakic cases.
Winter and Dannheim, 28 in operating on pseudophakic RDs, noted that cases without obvious retinal holes were twice as frequent as those with aphakic detachments. Decreased visualization of the peripheral fundus also contributed to intra-operative technical problems. Despite these difficulties, the prognosis for reattachment was comparable to that in simple aphakic detachments. Visual acuity, however, was 20/60 or worse in 58% of eyes.
In summary, the consequences of an ECCE and the presence of an IOL test the retinal surgeon's ophthalmoscopic and manipulative skills. In some series, the anatomic and visual success rates have not been as good as in conventional aphakic (ICCE) series. In other reports, the anatomic results have appeared comparable, but only after more numerous and more extensive operative procedures. Despite anatomic success, large proportions of patients have been left with visual acuities less than those required for conventional reading or for passing driver's license tests. As Jaffe et al19 emphasized, "the visual acuity results after retinal detachment surgery were relatively unfavorable."
Opacification of the posterior capsule and complications of capsulotomy. Opening of the posterior capsule
575

OPHTHALMOLOGY • MAY 1987 • VOLUME 94 • NUMBER 5
Table 4. Rates of Discission of Posterior Capsule after Extracapsular Surgery
Reference
Coonan et al, 198518
Pearce, 198566
Percival, 198531
Wilhelmus and Emery, 198067
Verzella, 198633
Sinskey and Cain, 197830
%of Eyes
60.7 50 45 50
50-60 20-43*
*Average, 26 months after cataract surgery.
( 1) increases the risk of aphakic or pseudophakic RD (by as much as three times), 18·31·62 especially in myopia31 , (2) may increase the risk of cystoid macular edema63·6\ and (3) may cause glaucoma in myopic eyes.65 These complications adversely influence visual results and patient morbidity. It is thus worth emphasizing that the extracapsular lens extraction recommended for axial myopes has a high rate of posterior capsular opacification requiring discission (Pearce,66 50%; Percival,31 45%; Coonan et al, 18 60.7%; Wilhelmus and Emery,67 50%; and Verzella,33 50 to 60%) (Table 4). This is particularly true of young individuals likely to be considered for extraction of clear lenses. In the series reported by Sinskey and Cain, 30 the rate of disabling capsular opacification was 20 to 43%, and importantly, discission was not performed until an average of 26 months after cataract surgery. The aphakic (and pseudophakic) interval before capsulotomy in the series of Coonan et al 18 was 24.3 months. The postoperative interval during which rates of RD are calculated, therefore, cannot be confined to the first year or two after cataract extraction because the "RD clock" may not begin ticking in earnest until after an opening has been made in the posterior capsule. 11
•46
Even when the discission is done with a laser rather than with a knife, substantial disruption of the anterior hyaloid face may occur ( 19% in the series by Stark and colleagues68). Furthermore, the presence of an IOL apparently does not provide sufficient protection against subsequent RD,32·46·62·69-71 even though it theoretically offers a mechanical barrier to forward shifting of the vitreous. For example, in 17 cases of RD after neodymium: Y AG laser capsulotomy reported by Ober et al, 72
82.4% had IOLs in place at the time of capsulotomy. Their presence in the PC clearly did not prevent development of the RD.
Cystoid macular edema (CME). The rate of clinically important CME is probably about 5% or less when an uncomplicated ECCE and implantation of a PC IOL are performed.21·73 The rate ofangiographic CME is about 9 to 18%.74 The incidence of CME is lowest when the posterior capsule and vitreous face are intact.63·64 Once it occurs in pseudophakic eyes, however, CME is one of the most important causes (along with RD) of reduced visual acuity after lens removal. 75 Moreover, resolution of CME is somewhat slower after extracapsular than
576
after intracapsular surgery.75 Wilkinson found that resolution of CME in aphakic and pseudophakic eyes without vitreous adhesions occurred in 79% of the former but in only 44% of the latter. The visual impact is severe when CME does persist because no predictably successful therapy exists currently.
When complications such as vitreous loss, capsular rupture, and zonular dialysis occur (and they do occur in over 12% of cases performed by experienced surgeons76), the rate of angiographic CME rises to about 29.5% and that of clinically apparent CME increases to about 18.0%.
Vitreous loss repeatedly emerges in the recent literature as a relatively common and serious operative complication during extracapsular cataract surgery. Hurite et al22 reported vitreous loss in 3.8% and inadvertent rupture of the posterior capsule in 6.5% of2095 phacoemulsifications. Wilkinson75 reported vitreous loss during 4.2% of phacoemulsifications, and Coonan et al18 also reported a 4.2% incidence of vitreous loss after ECCE. Praeger77 reported a 4.9% incidence of vitreous loss in myopic eyes undergoing phacoemulsification. Armstrong and Lichtenstein 78 were required to perform anterior vitrectomy for posterior capsular rupture in 10% of myopic eyes undergoing ECCE. Consequences of this type of complication may be severe because of the development of CME, and also because of an increased rate of RD. Conservatism is therefore indicated in the proposed surgical extraction of crystalline lenses in axial myopia because both Verzella26 and Curtin 79 have emphasized the weakness of the lens capsule and zonules in such eyes.
Other complications. In addition to vitreous loss, RD, opacification of the posterior capsule, and CME, a variety of other complications inevitably discolors any large operative series of lens extractions. Although the individual incidences of such problems as endophthalmitis, sympathetic ophthalmia, corneal decompensation, IOL dislocation, and so on are low, their visual consequences for the involved patient are often severe, and the value of therapy is frequently limited.
THE KNOWN RISKS OF CATARACf EXTRACfiON IN MYOPIA
Curtin4 has summarized early knowledge of complications related to ICCE in myopia. Postoperative RD is the major problem. Incidence rates for RD ranged from 6.2 to 8.1 %. Hyams and co-workers, for example, studied the effect ofiCCE on the incidence of postoperative RD in both myopic (> -6.0 D) and non-myopic eyes. The incidence of retinal breaks in 103 aphakic myopes was 18.4%, a substantial increase over that of phakic myopes (11% V RD occurred in 6. 7% of myopic and in 0.28% of non-myopic eyes, a roughly 24-fold increase in the eyes characterized by both myopia and aphakia. Clayman et al70 studied 819 consecutive ICCEs (including placement of an iris-clip IOL). Ofthose eyes having

GOLDBERG • CLEAR LENS EXTRACTION
15 .-----------------------------------------------------~
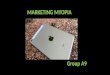
Fig 2. Rates of retinal detachment after ECCE. Notice influence of myopia and of opened posterior capsule.
10
5
0 ...._ __ __.
14%
.UI Myopic Non- Myopic Non- Myopic Myopic
Myopic (Moet with
capeulotomy)
.UI lztracapeular refracUn eztracUon
errore with RefracUn Myopic
lrrore (MoeUy with
lA tact capeule) (Moet with "ritreOill lOll
capeulotomy) or rupture4 zonule
Coonan. et at. 18 JCraff an4 Bul41n an4 1J.D4etrom S.
18811
Pru1er 77 111711
WllkiDeon 25 11185 San4ere 11178
(pen. communlc. 11188)
follow-up information, the incidence of postoperative pseudophakic RD was 0. 7% for axial lengths less than 25 mm, but 5% for axial lengths greater than or equal to 25 mm (a sevenfold difference). These incidence rates are likely to be lower than what one would observe in more comprehensive patient populations because the authors excluded "severe myopia or a history of an RD in either eye."
Jaffe et al19 reported RD rates in myopic eyes after both ICCEs (122 eyes) and ECCEs (151 eyes) (without IOL implants) that were studied over two sequential time intervals. RD occurred in 5.7% of ICCEs and 0.66% of ECCEs. Interestingly, all eyes with RD in the extracapsular series had intact posterior capsules. The number of eyes lost to follow-up after 1 year is not reported. In Armstrong and Lichtenstein's78 series of 40 myopic eyes (-0.5 to -7.0 D; axial lengths, 24.0-29.7 mm), most of which received IOL implantation, RD developed in three eyes (7 .5% ). Two had sustained posterior capsular rents during surgery, and one had a history of previous RDs in the same eye.
Coonan et al18 studied 842 consecutive ECCEs. The incidence of RD in patients with myopia greater than -8 D (about 3.5%) was almost three times more than in their non-myopic cases (Fig 2).
In 1983, Percival et aC' reported an incidence of aphakic RD of 11.1% in myopic eyes undergoing ICCE (8 of 72 eyes) and an incidence of 2.2% after planned ECCE (1 of 46 eyes). Eyes having had vitreous loss and subsequent RD were regrettably excluded from consid-
eration. Detailed follow-up intervals and percentages of eyes lost to follow-up are not given. The incidence of RD was 1.9% of 482 eyes with ICCEs, and 4.8% of 185 eyes containing iris-clip lenses. The authors concluded that the theoretical protection from anterior vitreous prolapse provided by this type of IOL could not be substantiated by their data. In 1985, Percival31 reported additional data showing that RDs after extracapsular cataract surgery were mainly associated with high myopia. The incidence of RD did not appear abnormally high as long as the posterior capsule remained intact, but once a capsulotomy had been performed, the incidence of RD approximated that after intracapsular cataract surgery.
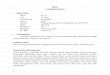
Ruben and Rajpurohit56 studied 944 eyes undergoing cataract extraction over a 3-year period. Most had had intracapsular surgery. Of these, 46 had preoperative myopia between -10.00 and -20.00 D, and 16 of 33 ( 48.5%) eyes developing RD had refractive errors greater than -10.00 D. Calculated probabilities of aphakic RD were 3.5% for refractive errors ofO to -4.00 D, 4.2% for -5.00 to -9.00 D, and 40.0% for -10.00 to -20.00 D (Fig 3).
In summary, retention of an intact posterior capsule generally confers some protection against aphakic RD. Acceptable evidence that a PC implant provides substantial additional protection is lacking.46 The presence of myopia raises the postoperative rate of RD by several orders of magnitude, even after an extracapsular type of operation. The higher the myopia, the higher the risk for RD.
577

OPHTHALMOLOGY • MAY 1987 • VOLUME 94 • NUMBER 5
.... s:: CD s '§ ~0 ol .... CD
Q .-I 30 ol s:: ..... .... :. 20 .<:: .... . .; "' Cll 10 CD
3.5::1 » r.l
'c: oL_I•••L_j .... s:: Plano
to -•.oon -5.00D -!O.OOD
to to -9.00D -20.00D
CD 0 ~ CD ~ Refractive Error
Fig 3. Influence of myopia on aphakic retinal detachments.
CURRENT KNOWLEDGE OF CLEAR LENS EXTRACTION IN AXIAL MYOPIA
FAVORABLE OPINIONS
Because Verzella and Roncagli80 have been the major proponents of clear lens extraction in high myopia, their data deserve objective scrutiny. Over an 8-year interval (January 1977 to December 1985), they report examining 4479 eyes with myopia greater than -10 D: 763 ( 17% of the total) underwent clear lens extraction by phacoemulsification; 354 received a primary IOL implant; and 182 received a secondary implant. Cataracts were removed from 1020 highly myopic eyes (22.8% of the total); 427 of them received a primary IOL implant, and 199 received a secondary implant. The intervals between surgery and secondary implantation were not specified.
Lens extraction was not done unless the retina appeared stable. No definition of stability was offered, therefore the retinal status could not be independently evaluated in this series. Prophylaxis by argon laser photocoagulation was carried out in 47% of the patients with clear lenses and in 20% of the patients with cataracts.
Follow-up examinations are stated to have occurred no less frequently than 1 day, 1 month, 2 months, 6 months, and 1, 2, and 3 years after surgery. The percentage of eyes seen at each of these intervals is not reported, nor is the overall rate of loss to follow-up. Of the unreported eyes, the number having had transient or permanent complications is unknown.
Although Verzella and Roncagli warn against several technical problems in performing phacoemulsification in highly myopic eyes (such as easy rupture of the lens capsule and of the zonule), intra-operative complication rates are not reported. In one report, Verzella points out that "the zonular capsular diaphragm . . . is very weak even in young patients with clear lenses,"81 and he also states that "the zonular capsular diaphragm . . . has
578
proven to be particularly weak in elderly patients with degenerative myopia."26 If this structure indeed is weak in both age groups, what are the incidence and type of operative complications in both young and old myopic individuals? How do they influence postoperative complications?
The following results are presented80: in the clear lens
population, opacified posterior capsules developed in 43%, and 20.7% have required capsulotomies to date (with an unknown number yet to come). Analogous percentages in the older, cataractous population were 23.8 and 16.3%. Younger patients, represented by the series of clear lens extractions, therefore appear to be at higher risk for this complication than the cataractous group . RDs were known to have occurred in 5 of 763 (0.66%) clear lens extractions and in 15 of 1020 ( 1.5%) cataract extractions. Of these 20 retinas, five detached after a 12-month postoperative interval. The number of patients who went elsewhere for retinal diagnosis and therapy is unreported and is presumably unknown.
After clear lens or cataract extraction, 19% of all eyes still had refractive errors greater than -4 D. Visual acuity was worse than 20/40 in 500 (49%) cataractous eyes and in about 330 (43.3%) eyes having had extraction of clear lenses. Reasons for these high rates of poor vision are not described, so it is impossible to determine how many instances are due to operative or postoperative complications and how many from abnormalities (such as myopic maculopathy) that pre-existed the lens surgery.
Verzella warns about difficulties with near vision after such surgery, due presumably to absence of accommodation, a new optical system to which the patient must adapt, and so on.81 In particular, he indicates that "low vision patients may have to learn a new reading technique." The frequency and severity of such problems are not defined. The percentages of patients still required to wear spectacles or contact lenses postoperatively are also not reported.
Some inconsistencies appear in Verzella's series of clinical reports. The 1986 report80 states that "Y AG posterior capsulotomy is performed after one year ... ," whereas the 1983 report indicates that 72% of capsulotomies occurred within 6 months.82 Figure & ofthe 1986 report actually shows that approximately 36 clear lens cases and about 58 cataract cases underwent capsulotomy between 0 and 6 months. In 1985, Verzella83
stated that his indications for clear lens extraction included myopia greater than -15 D, whereas his other reports state that the indication is myopia greater than -10 D. In either case, data from other series6
•56 indicate
that such higl1ly myopic eyes are at substantial risk of RD, especially after cataract extraction.
UNFAVORABLE INFORMATION
Data and conclusions different from those of Verzella are provided by Curtin, 79 Clayman et al, 70 Praeger, 77
Sanders and Kraff (written communication, February 11, 1986), and Huldin and Lindstrom84 (Fig 2). Older

GOLDBERG • CLEAR LENS EXTRACTION
series of RD after mostly ICCE in myopia report incidences of 6.2 to 11%.4 Praeger's rate of RD after phacoemulsification in myopic eyes having axial lengths greater than 27 mm was 6.5%. Most had primary capsulotomy performed. Between 1978 and 1985, Kraff and Sanders (written communication, February 11, 1986) performed ECCE by a variety oftechniques in 4636 eyes with axial lengths 25 mm or less and in 545 eyes with axial lengths greater than 25 mm. The rate of postoperative RD was 0.9% in non-myopic eyes and 2.8% in myopic eyes (an approximately threefold increase in the myopic eyes).
In the series ofHuldin and Lindstrom,84 collected between 1980 and 1985, 73 cataractous myopes with axial lengths greater than 25 mm underwent ECCE or phacoemulsification and were followed up for 6 to 54 months. In addition, 54 age- and sex-matched controls ( <25 mm in axial length) were similarly treated and followed up. Almost all (97%) had primary insertion of a PC IOL implant. No RDs occurred in the non-myopic control group, whereas 7 of 7 3 (9 .6%) of the my opes had detachments after intervals of 1 to 36 months (3 of the 7 retinas detached after 1 year, 6 of the 7 had PC IOLs, and 5 of the 7 had intact PCs). The presence of a PC implant and of an intact posterior capsule obviously did not protect against RD in the majority of these myopic eyes.
ALTERNATIVES TO REMOVAL OF CLEAR LENSES
Alternatives to clear lens extraction are available for the optical management of axial myopia. A physician obtaining informed consent is obligated to describe these alternatives. Some, such as spectacles, contact lenses, or low vision aids, are completely noninvasive, and some surgical procedures, such as epikeratophakia, have the advantages of being external and reversible. Other experimental procedures, such as myopic keratomileusis and intrastromal implant procedures are interesting and require substantial further investigation. In choosing any of these surgical procedures, oneshould, as in the case of clear lens extraction, adopt the principle of primum non nocere, and first exhaust the possibilities provided by spectacles or contact lenses. The article evaluating radial keratotomy in Forbes Magazine (Myopic Haste, May 6, 1985) is still applicable: "If today the only means available for correcting myopia consisted of (surgery) and tomorrow somebody invented glasses or contacts, he'd win the Nobel Prize hands down."
Curtin4 offers the following useful suggestions for the successful dispensing of highly myopic spectacles: ( 1) the vertex distance of new lenses should always be specified; (2) lightweight frames and plastic lenses should be attempted; (3) glass lenses with a high refractive index (1. 7) can sometimes be useful; ( 4) thick lens edges should be camouflaged by coloring them the same as the frame; and ( 4) base curves and lens thicknesses should not be changed in a successful spectacle wearer.
Contact lenses have the beneficial effect of increasing the image size by 27 to 50% for axial myopes. Both small hard lenses as well as extended wear lenses can be used. In one extended wear series, Stark and Martin85 found that over 95% of 207 myopic eyes saw 20/40 or better with perfilcon A lenses worn with an "extended" regimen for 3 to 8 years. Lens-related problems, such as follicular conjunctivitis, forced discontinuation of lens use in 9% of patients, but there were no serious complications in this series. Corneal ulcers, however, have been reported subsequently in some cases. 86•8
7
Low-vision aids can also be successfully used, especially by young, motivated myopes. Reading aids are often unnecessary because most patients can read at their far point. Telescopic lenses, including some small devices that can be inserted eccentrically in a spectacle, can be used for viewing television and for other distance functions.4
Radial keratotomy continues to undergo refinement. Problems such as accuracy of predictability, fluctuation in postoperative acuity, troublesome glare, and delayed bacterial keratitis, have not been eliminated. However, radial keratotomy is a surgical alternative for myopic patients who are intolerant to contact lenses and spectacles and who have refractive errors from about-2 to -5 0.88
-90 Extreme axial myopes (such as those for whom
clear lens extraction is being contemplated) cannot be corrected by radial keratotomy.
Epikeratophakia has recently been used for myopia as low as -4 to -5 D as well as for very high degrees of myopia. Currently, the range of refractive correction with epikeratophakia exceeds that available with myopic keratomileusis. Epikeratophakia also has the advantages of being relatively simple, technically, as well as potentially reversible. Most importantly, it is external.88
Moreover, accommodation is preserved. Refractive errors as high as -38 D have been corrected, but extensive long-term data are not yet available. Although published experience with axial myopia is limited, preliminary results are encouraging, not only for myopia but also for aphakia and keratoconus.91 The full range and extent of complications are currently unknown but include some inaccuracy in predictability of postoperative refractive error, impermanence of the refractive change, production of glare and interface opacities, reduction of best-corrected vision, and possibly others. Nonetheless, this technique is promising and appears to confer a substantially improved risk/benefit ratio in comparison to that of clear lens extraction. More data and longer follow-up are required before this new technique can be unequivocally recommended for axial myopes.
Myopic keratomileusis represents another surgical alternative to clear lens extraction. It is technically more complicated than myopic epikeratophakia, relatively more irreversible, and cannot correct myopia greater than about -15 to -16 0.92•93 In 23 operations of this type, Maxwell and Nordan94 obtained an average refractive change of -10.09 D. Complications include epithelial inclusions, perforations, and irregular astigmatism. In addition, there may be, on average, a slight
579

OPHTHALMOLOGY • MAY 1987 • VOLUME 94 • NUMBER 5
worsening of vision postoperatively, as reported by Nordan and Fallor.92 In the series reported by Swinger and Barker,93 however, no patient had a decrease in bestcorrected acuity postoperatively. Evidence of postoperative RDs is limited, but an RD developed in one case in Nordan's experience six days postoperatively,95 possibly due to distortion of the sclera by the suction ring used to stabilize the eye during surgery. Swinger and Barker93
reported 42 eyes undergoing myopic keratomileusis. The average reduction in myopia was about -11.6 D. After myopic keratomileusis, further optical correction, including contact lenses93•
95 and radial keratotomy95•96
have been used, suggesting that myopic keratomileusis is often not a definitive operation. Nonetheless, accommodation is maintained. The complexities of this technique may preclude its widespread acceptance.
Additional highly experimental techniques include intrastromal corneal implants97
- 99 and anterior chamber lenses with retention of the crystalline lens.4 Such procedures require objective and ethical investigations before they can be adequately assessed.
EPILOGUE
Published evidence concerning postoperative complications after extracapsular lens extraction (with and without PC IOLs) must be interpreted with reservation. Most reported series do not give sufficient information. In the report by Sinskey and Cain, 30 for example, 28% of eyes were lost to follow-up, and in Wilkinson's series,25
46% of eyes were lost to follow-up. The percentage of RDs developing in such eyes and other complications is unknown. Postoperative endophthalmitis, if it were to occur after elective surgery, would be particularly tragic.
Data regarding the loss to follow-up at 1 or more years are often not available or stated in most published reports. Serious complications, such as RD, will occur after 1 year, 16
•19•27
•29 especially after delayed capsular
opacification that requires subsequent capsulotomy. Follow-up must include the large number of eyes undergoing late posterior capsulotomy because their incidence of RD will almost certainly increase once the posterior capsule is opened, even with a laser.72 Long-term follow-up, with as little attrition as possible, is badly needed to assess properly the incidence of late-onset RD, the anatomic reattachment rate, and the eventual visual acuity (which may be reduced secondary to all manner of complications, including detachment of the macula before retinal surgery). These data are particularly needed in the young, highly myopic population for whom clear lens extraction is being contemplated. Furthermore, most patients having this procedure will need it performed on both eyes, or they will not be able to use the two eyes together because of substantial aniseikonia. Thus, both eyes may be placed at risk.
Previous reports of operative and postoperative data have not been sufficiently stratified into groups with differing degrees of axial elongation. Nonetheless,
580
enough is known about the biology of high myopia to conclude that individuals (such as those with approximately ~ 15 D of myopia) who optically might benefit the most from clear lens extraction are also those most likely to have the highest operative and postoperative complication rates. These high rates are easily obscured in published values that are averaged and derived from groups of eyes extending over a large range of myopic refractive errors.
Some series of lens extractions, such as that of Drews100 and those of Verzella,33•80- 83 appear to show low rates of complications, including RD. Other series, such as those of Huldin and Lindstrom,84 Praeger,77
Coonan et al, 18 Clayman et al/0 and Kraff and Sanders (personal communication, 1986), report rates that are substantially higher (up to 9.6%, or possibly higher in extreme axial myopia56) than in non-myopic populations. The interpretation of these complication rates is subject to personal bias. A water glass may appear half full to some observers and half empty to others. Moreover, the absolute rates of postoperative complications may appear low to some individuals, but these complications, if they do occur, are serious. They often result in permanently reduced vision, despite our best therapeutic efforts. 18
•28
•29
•38
•53
•56
-58
•60 Effective and safe prophy
laxis is far from certain. 34-36
•38
•39 Even if the complica
tion rates are interpreted to be low in absolute terms, they are certainly greater than those in patients having no invasive surgery at all. The time-honored physician's principle of primum non nocere is reinforced by the availability of alternatives (including nonsurgical refractive devices) that are safer than clear lens extraction. Based on the available evidence, therefore, I conclude that the risk/benefit ratio for this operation is currently too high for it to be recommended.
REFERENCES
1. Meyer-Schwickerath G, Gerke E. Biometric studies of the eyeball and retinal detachment. Br J Ophthalmol1984; 68:29-31.
2. Hyams SW, Bialik M, Neumann E. Myopia-aphakia: I. Prevalence of retinal detachment. Br J Ophthalmol 1975; 59:480-2.
3. Hyams SW, Neumann E, Friedman Z. Myopia-aphakia: II. Vitreous and peripheral retina. Br J Ophthalmol1975; 59:483-5.
4. Curtin BJ. The Myopias: Basic Science and Clinical Management. Philadelphia: Harper & Row, 1985; 277-385, 403-35.
5. Cockerham WD, Freeman HM. Molehills, mountains and prophylaxis of retinal detachment. (editorial). Arch Ophthalmol 1968; 79:655-6.
6. Perkins ES. Morbidity from myopia. Sightsav Rev 1979; 49:11-9. 7. Schepens CL, Marden BA. Data on the natural history of retinal
detachment: further characterization of certain unilateral nontraumatic cases. Am J Ophthalmol1966; 61:213-26.
8. Blach RK. Degenerative myopia. In: Krill AE, ed. Krill's Hereditary Retinal and Choroidal Diseases. Vol 2. Clinical Characteristics. Hagerstown, Maryland: Harper & Row, 1977; 911-37.
9. Cambiaggi A. Myopia and retinal detachment: statistical study of some of their relationships. Am J Ophthalmol1964; 58:642-50.
10. Kaufmann T. Myopie und Amotio retinae: statistische Analyse von 800 Fallen. Ophthalmologica 1969; 157:249-62.

GOLDBERG • CLEAR LENS EXTRACTION
11. McDonnell PJ, Patel A, Green WR. Comparison of intracapsular and extracapsular cataract surgery. Histopathologic study of eyes ob
tained postmortem. Ophthalmology 1985; 92:1208-25. 12. Edmund J, Seedorf! HH. Retinal detachment in the aphakic eye.
Acta Ophthalmol 197 4; 52 323-33. 13. Norton EWD. Retinal detachment in aphakia. Am J Ophthalmol
1964; 58:111-24. 14. Scheie HG, Morse PH, Aminlan A. Incidence of retinal detachment
following cataract extraction. Arch Ophthalmol1973; 89:293-5. 15. Hawkins WR. Aphakic retinal detachment. Ophthalmic Surg 1975;
6(2)66-74. 16. Folk JC, Burton TC. Bilateral aphakic retinal detachment. Retina
1983; 3:1-6. 17. Benson WE, Grand MG, Okun E. Aphakic retinal detachment. Man
agement of the fellow eye. Arch Ophthalmol1975; 93:245-9. 18. Coonan P, Fung WE, Webster RG Jr, et al. The incidence of retinal
detachment following extracapsular cataract extraction: a ten-year
study. Ophthalmology 1985; 92:1096-101. 19. Jaffe NS, Clayman HM, Jaffe MS. Retinal detachment in myopiC
eyes after intracapsular and extracapsular cataract extraction. Am J
Ophthalmol 1984; 97:48-52. 20. Girard LJ. Pars plana lensectomy by ultrasonic fragmentation: re·
suits of a retrospective study. Ophthalmology 1981; 88:434-6. 21. Wetzig PC, Thatcher DB, Christiansen JM. The intracapsular versus
the extracapsular cataract technique in relationship to retinal prob·
lems. Trans Am Ophthalmol Soc 1979; 77:339-47. 22. Hurite FG, Sorr EM, Everett WG. The incidence of retinal detach
ment following phacoemulsification. Ophthalmology 1979;
862004-6. 23. Kratz RP. Complications associated with posterior chamber lenses.
Ophthalmology 1979; 86:659-61. 24. Binkhorst CD. Five hundred planned extracapsular extractions with
irido-capsular and iris clip lens implantation in senile cataract. Oph·
thalmic Surg 1977; 8(3):37-44. 25. Wilkinson CP, Anderson LS, Little JH. Retinal detachment following
phacoemulsification. Ophthalmology 1978; 85:151-6. 26. Verzella F. Microsurgery of the lens in h1gh myopia for optical pur·
poses. Cataract1984; 1(2):8-12. 27. Ashrafzadeh MT, Schepens CL, Elzeneiny II, et al. Aphakic and
phakic retinal detachment: 1. Preoperative findings. Arch Ophthalmol
1973; 89:476-83.
28. Winter R, Dannheim F. Netzhautablosungen nach Kunstlinsen1m·
plantation. Fortschr Ophthalmol1985; 82172-4.
29. Ho PC, Tolentino Fl. Pseudophakic retinal detachment: surgical suc
cess rate with various types of IOLs. Ophthalmology 1984; 91:847-
52.
30. Sinskey RM, Cain W Jr. The posterior capsule and phacoemulsifi
cation. Am Intraocular Implant Soc J 1978; 4:206-7.
31. Percival SPB. Long term complications from extracapsular cataract
surgery. Trans Ophthalmol Soc UK 1985; 104:915-8
32. Harris WS, Kogan I. Retrospective study of retinal complications with posterior chamber lenses. Contact Intraocular Lens Med J
1981; 7341-4.
33. Verzella F. P. E. and transparent lenses. In: Verzella F, ed. Atlas of Extracapsular Technique. Phaco Emulsification and Intraocular
Lenses. Bologna, Italy: Lens Editions. 1981; 98-108.
34. Kanski JJ, Daniel R. Prophylaxis of retinal detachment. Am J
Ophthalmol 1975; 79197-205. 35. Yanoff M. Prophylactic cryotherapy of retinal breaks. Ann Ophthal·
mol 1977; 9:283-6 36. Robertson OM, Norton EWD Long-term follow-up of treated ret1nal
breaks. Am J Ophthalmol1973; 75395-404
37. Benson WE, Morse PH, Nantawan P. Late complications follow1ng cryotherapy of lattice degeneration Am J Ophthalmol 1977;
84:514-6.
38. Campbell CJ, Rittler MC. Cataract extraction in the retinal detach· ment-prone patient. Am J Ophthalmol1972; 73:17-24.
39. Stein R, Pinchas A, Traister G. Prevention of retinal detachment by a
circumferential barrage prior to lens extraclion in high-myopic eyes. Ophthalmologica 1972; 165:125-36.
40. Ramen M, Singer L. Long-term follow-up of photocoagulated breaks. Br J Ophthalmol 1978; 62:240-2.
41. Saracco JB, Estachy GM, Gastaud P, Maymard I. La prevention du decollement de reline de l'aphaque par photocoagulation au laser a l'argon: a propos de 600 cas. Ophthalmologica 1980; 181:142-8.
42. Davis MD. The natural history of retinal breaks without detachment. Trans Am Ophthalmol Soc 1973; 71:343-72.
43. Robertson OM, Priluck lA. 360° prophylactic cryoretinopexy. A clin· ical and experimental study. Arch Ophthalmol1979; 97:2130-4.
44. Mortimer CB. The prevention of retinal detachment. Can J Ophthal· mol1966; 1206-11.
45. Chignell AH, Shilling J. Prophylaxis of retinal detachment. Br J Ophthalmol 1973; 57:291-8.
46. Irvine AR. The pathogenesis of aphakic retinal detachment. Ophthalmic Surg 1985; 16:101-7.
47. Shafer OM. Retinal detachment after phacoemulsification. Trans Am Acad Ophthal Otolaryng 1974; 78:0P28-30.
48. Heimann K. lntraokulare Linse und Netzhautablosung Fortschr Ophthalmol 1985; 82: 168-71 .
49. Jungschaffer OH. Retinal detachments after intraocular lens Implants. Arch Ophthalmol1977; 95:1203-4.
50. Freeman HM. Discussion of presentation by Dr. William Snyder, et al. Ophthalmology 1979; 86:239-41.
51. Snyder WB, Bernstein I, Fuller D, et al. Retinal detachment and pseudophakia Ophthalmology 1979; 86:229-41.
52. Schindler RH. Posterior segment complications. In: Ginsberg SP, ed. Cataract and Intraocular Lens Surgery. A compendium of modern theories and techniques. Vol. 2. Birmingham, Alabama; Aesculapius Publishing Co, 1984; 364-85.
53. Freema11 riM, Dobbie JG, Friedman MW, et al. Pseudophakic retinal detachment. Mod Probl Ophthalmol 1979; 20:345-53.
54 Irvine A, comment on, Ho PC, Tolentino Fl. Retinal detachment following extracapsular cataract extraction and posterior chamber
intraocular lens implantation. (Br J Ophthalmol1985; 69:650-3) Surv Ophthalmol1986; 31:76-7.
55. Ho PC, Tolentino Fl. Retinal detachment following extracapsular cataract extraction and posterior chamber intraocular lens implantation. Br J Ophthalmol 1985; 69:650-3.
56 Ruben M, Rajpurohit P. Distribution of myopia in aphakic retinal detachments. Br J Ophthalmol1976; 60:517-21.
57. Tasman WS. Pseudophakic retinal detachment. Ophthalmic Forum 1983; 1(3) 20-1.
58. Sethi SK, Howard R, Milewski SA, et al. Pseudophakic retinal de· tachments. J Ocular Therapy Surg 1983; 2:180-1.
59. Hagler WS. Pseudophakic retinal detachment. Trans Am Ophthal· mol Soc 1982; 80:45-63.
60. Wilkinson CP. Retinal detachment following intraocular lens implantation. Graefes Arch Clin Exp Ophthalmol1986; 224:64-6.
61. Wilkinson CP. Retinal detachment after phacoemulsification. Am J Ophthalmol 1979; 87 628-31.
62. Lindstrom RL, Harris WS. Management of the posterior capsule
following postenor chamber lens implanation. Am Intraocular Implant Soc J 1980; 6:255-8.
63 Percival P. Clinical factors relating to cystoid macular edema after lens implanat1on. Am Intraocular Implant Soc J 1981; 7:43-5.
64. Kraff MC, Sanders DR, Jampol LM, Lieberman HL. Effect of primary capsulotomy with extracapsular surgery on the inc1dence of pseudophakic cystoid macular edema. Am J Ophthalmol1984; 98:166-70.
65 Schubert HD. Capsulotomy, myopia, and unexpected intraocular pressur8 rise. (Letter) Arch Ophthalmol1986; 104:22--3.
581

OPHTHALMOLOGY • MAY 1987 • VOLUME 94 • NUMBER 5
66. Pearce JL. Capsular fixated posterior chamber lenses in high myopia. Trans Ophthalmol Soc UK 1985; 104:586-7.
67. Wilhelmus KR, Emery JM. Posterior capsule opacification following phacoemulsification. Ophthalmic Surg 1980; 11:264-7.
68 Stark WJ, Worthen D, Holladay JT, Murray G. Neodymium:YAG lasers an FDA report. Ophthalmology 1985; 92:209-12.
69. Galin MA, Poole TA, Obstbaum SA. Retinal detachment in pseudophakia. Am J Ophthalmol 1979; 88 49-51.
70 Clayman HM, Jaffe NS, Light DS, et al. Intraocular lenses, axial length, and retinal detachment. Am J Ophthalmol1981; 92:778-80.
71. Percival SPB, Anand V, Das SK. Prevalence of aphakic retinal detachment Br J Ophthalmol 1983; 67:43-5.
72. Ober RR, Wilkinson CP, Fiore JV Jr, Maggiano JM. Rhegmatogenous retinal detachment after neodymium-Y AG laser capsulotomy in phakic and pseudophakic eyes. Am J Ophthalmol 1986; 101 81-9
73. Berrocal JAR. Incidence of cystoid macular edema after different cataract operations. Mod Probl Ophthalmol1977; 18:518-20.
74. Kraft MC, Sanders DR, Jampol LM, Lieberman HI. Effect of an ultraviolet-filtering intraocular lens on cystoid macular edema. Ophthalmology 1985: 92:366-9.
75. Wilkinson CP. A long-term follow-up study of cystoid macular edema 1n aphakic and pseudophakic eyes. Trans Am Ophthalmol Soc 1981; 79:810-39.
76. Jaffe NS, Clayman HM, Jaffe MS. Cystoid macular edema after intracapsular and extracapsular cataract extraction with and without an intraocular lens. Ophthalmology 1982; 89:25-9.
77. Praeger DL. Five years' follow-up in the surgical management of cataracts 1n high myopia treated with the Kelman phacoemulsification technique. Ophthalmology 1979; 86:2024-33.
78. Armstrong T A, Lichtenstein SB. Intraocular lenses in myopes. Ophthalmic Surg 1984; 15:653-7.
79. Curtin BJ. Pathologic myopia. Ophthalmic Forum 1985; 3:192-5. 80. Verzella F, Roncagli V. Myopic lens extraction. (Unpublished data,
1986.) 81. Verzella F. High myopia: in-the-bag refractive implantation. Ophthal
mic Forum 1985; 3(3):174-5. 82. Verzella F. High myopia: microsurgical extracapsular extraction of
the lens for optical purposes. Read before the Keratorefractive Society, Chicago, October 29-30, 1983.
582
83. Verzella F. Lensectomy. Ophthalmic Forum 1985; 3(3):191-2. 84. Huldin J, Lindstrom RL. Retinal detachment in axial myopia. (Un
published data, 1986.) 85. Stark WJ, Martin NF. Extended-wear contact lenses for myopic
correction Arch Ophthalmol 1981; 99:1963-6. 86. Hassman G, Sugar J. Pseudomonas corneal ulcer with extended
wear soft contact lenses in myopia. Arch Ophthalmol 1983; 101:1549-50.
87. Stenson S. Soft contact lenses and corneal infection. Arch Ophthalmol1986; 104:1287-9.
88. McDonald MB, Klyce SD, Suarez H, et al. Epikeratophakia for myopia correction. Ophthalmology 1985; 92:1417-22.
89. Waring GO Ill. Review: the changing status of radial keratotomy for myopia: Part I. J Refract Surg 1985; 1(2):81-6.
90. Waring GO Ill. Review: the changing status of radial keratotomy for myopia: Part II. J Refract Surg 1985; 1 (3): 119-37.
91. McDonald MB, Kaufman HE, Durrie DS, et al. Epikeratophakia for keratoconus: the nationwide study. Arch Ophthalmol 1986; 1 04: 1294-300.
92. Nordan LT, Failor MK. Myopic ke1atomileusis: 74 consecutive nonamblyopic cases with one year of follow-up. J Refract Surg 1986; 2(3): 124-8.
93. Swinger CA, Barker BA. Prospective evaluation of myopic keratomileusis. Ophthalmology 1984; 91:785-92.
94. Maxwell WA, Nordan LT. Myopic keratomileusis: early experience. J Refract Surg 1985; 1(3):99-103.
95. Nordan LT. Keratomileusis. Ophthalmic Forum 1985; 3(3):188-90.
96. Nordan L T, Havins WE. Undercorrected radial keratotomy treated with myopic keratomileusis. J Refract Surg 1985; 1(2):56-8.
97. McCarey BE, Andrews DM. Refractive keratoplasty with intrastromal hydrogel lenticular implants. Invest Ophthalmol Vis Sci 1981; 21:107-15.
98. Lane SS, Lindstrom RL, Williams PA, et al. Polysulfone intracorneal lenses. J Refract Surg 1985; 1 (5):207 -16.
99. Werblin TP, Blaydes JE, Fryczkowski A, Peiff R. Refractive corneal surgery: the use of implantable alloplastic lens material. Aust J Ophthalmol1983; 11:325-31.
100. Drews RC. Results in patients with high and low power intraocular lenses. J Cataract Refract Surg 1986; 12:154-7.