Embed Size (px)
Citation preview

1
International Journal of Medical and Dental Case Reports (2015), Article ID 030915, 5 Pages
C A S E R E P O R T
Cleidocranial dysplasia: Two unique casesT. Chaudhari Narendra1, A. Amale Kavita2, K. Sethy Saroj3
1Department of Oral Pathology and Microbiology, Government Dental College and Hospital, Mumbai, India, 2Department of Oral Medicine, Diagnosis and Radiology, Government Dental College and Hospital, Mumbai, India, 3Department of Oral and Maxillofacial Surgery, Government Dental College and Hospital, Mumbai, India
AbstractCleidocranial dysplasia (CCD) is a rare autosomal dominant disorder aff ecting skeletal and dental tissues. The diagnosis of this syndrome is usually delayed, but the prognosis is good if appropriately managed. The involvement of facial bones, altered eruption patterns and presence of multiple supernumerary teeth warrants a clinical concern for dental health professionals. Due to complex nature of CCD a multidisciplinary approach is required for treatment. Early diagnosis is of utmost important to ensure better prognosis. We present two cases of CCD and a brief review.
Keywords: Autosomal, cleidocranial dysplasia, multidisciplinary, skeletal, supernumerary
Correspondence Dr. T. Chaudhari Narendra, Nirman Park Phase 3, A-6, Room No - 4, Santoshi Mata Road, Kalyan West - 421 301. Phone: +91-9969529473. Email: [email protected]
Received 02 August 2015;Accepted 10 September 2015
doi: 10.15713/ins.ijmdcr.30
How to cite the article: Narendra TC, Kavita AA, Saroj KS. Cleidocranial dysplasia: Two unique cases. Int J Med Dent Case Rep 2015;1:1-5.
Introduction
Cleidocranial dysplasia (CCD) is usually inherited as an autosomal dominant trait,[1] nonetheless around 35% of cases show no apparent inheritance which may be due to spontaneous mutations.[2] Even though CCD was fi rst accurately described by Scheuthauer, clavicular defects were reported in the literature from 1765.[3] CCD is a rare syndrome with a prevalence of 0.5/100,000 live births.[4] The characteristic features of CCD are clavicular aplasia, excessive development of the transverse diameter of the cranium, delayed closure of the fontanells, and disorders of the jaws and dentition,[5] which lead to introduction of term “dysostose cléidocrânienne héréditaire” (cleidocranial dysostosis) by Marie and Sainton in 1898.[3] Since, CCD shows generalized dysplasia of bones and teeth “dysplasia” is more appropriate instead of “dysostosis”.[6]
Prominent supraorbital and infraorbital ridges, exorbitism due to defi cient orbital volume and frontal bone thickening results in the characteristic skull appearance in CCD known as “Arnold head.”[2] This appearance is similar to descendants of a Chinese family named Arnold. Earlier it was believed that CCD aff ects only bones of membranous origin, but recent investigations suggest that it is a generalized skeletal dysplasia aff ecting the entire skeleton along with the clavicles and skull.[3]
CCD often shows complications in skeletal, orthopedic, respiratory, dental, auditory, and pregnancy.[7] It has striking clinical and radiographic features but often is diagnosed late. Early identifi cation of this syndrome helps in providing better clinical care. We discuss here two case reports of CCD.
Case Report
Case 1
A 25-year-old male presented with a chief complaint of carious and missing teeth in upper and lower jaws. Due to missing teeth, he had diffi culty in mastication and speech. The patient had no relevant family and past medical history and visited dentist few days back for removal of mobile anterior teeth.
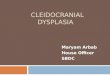
On extra oral examination, the patient showed short stature for his age. Head was large with frontal and parietal bossing. The shoulders were narrow with marked drooping, but there was no unusual mobility [Figure 1a]. Nose was deviated to left side. The base of the nose was widened with the depressed nasal bridge. Mild ocular hypertelorism and slight mandibular prognathism were also seen [Figure 1b]. Oral cavity examination revealed edentulous ridge in mandibular anterior region. This was due to the extraction of mobile primary lower incisors. Both the arches had many over-retained deciduous teeth, and several permanent teeth were missing. The teeth present showed many abnormalities such as rotation, caries, and gingival recession. Few root pieces were also present. Spacing was present between the teeth, and oral hygiene care was not proper [Figure 1c].
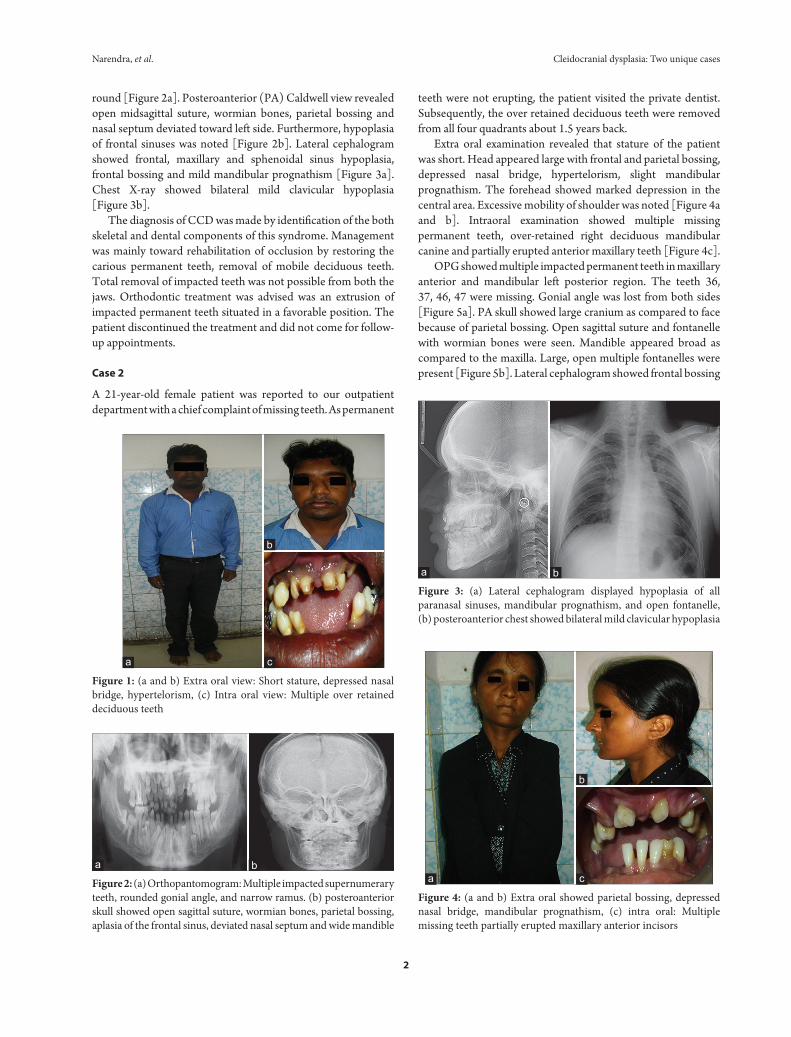
Orthopantomogram (OPG) showed over-retained deciduous teeth and numerous impacted permanent and supernumerary teeth crowded in both the arches. Twenty-seven impacted teeth were identifi ed inside the bone. Mandibular ramus was narrow and coronoid process was thin and pointed on both right and left sides. The angle and zygomatic arches were
Narendra, et al. Cleidocranial dysplasia: Two unique cases
2
round [Figure 2a]. Posteroanterior (PA) Caldwell view revealed open midsagittal suture, wormian bones, parietal bossing and nasal septum deviated toward left side. Furthermore, hypoplasia of frontal sinuses was noted [Figure 2b]. Lateral cephalogram showed frontal, maxillary and sphenoidal sinus hypoplasia, frontal bossing and mild mandibular prognathism [Figure 3a]. Chest X-ray showed bilateral mild clavicular hypoplasia [Figure 3b].
The diagnosis of CCD was made by identifi cation of the both skeletal and dental components of this syndrome. Management was mainly toward rehabilitation of occlusion by restoring the carious permanent teeth, removal of mobile deciduous teeth. Total removal of impacted teeth was not possible from both the jaws. Orthodontic treatment was advised was an extrusion of impacted permanent teeth situated in a favorable position. The patient discontinued the treatment and did not come for follow-up appointments.
Case 2
A 21-year-old female patient was reported to our outpatient department with a chief complaint of missing teeth. As permanent
teeth were not erupting, the patient visited the private dentist. Subsequently, the over retained deciduous teeth were removed from all four quadrants about 1.5 years back.
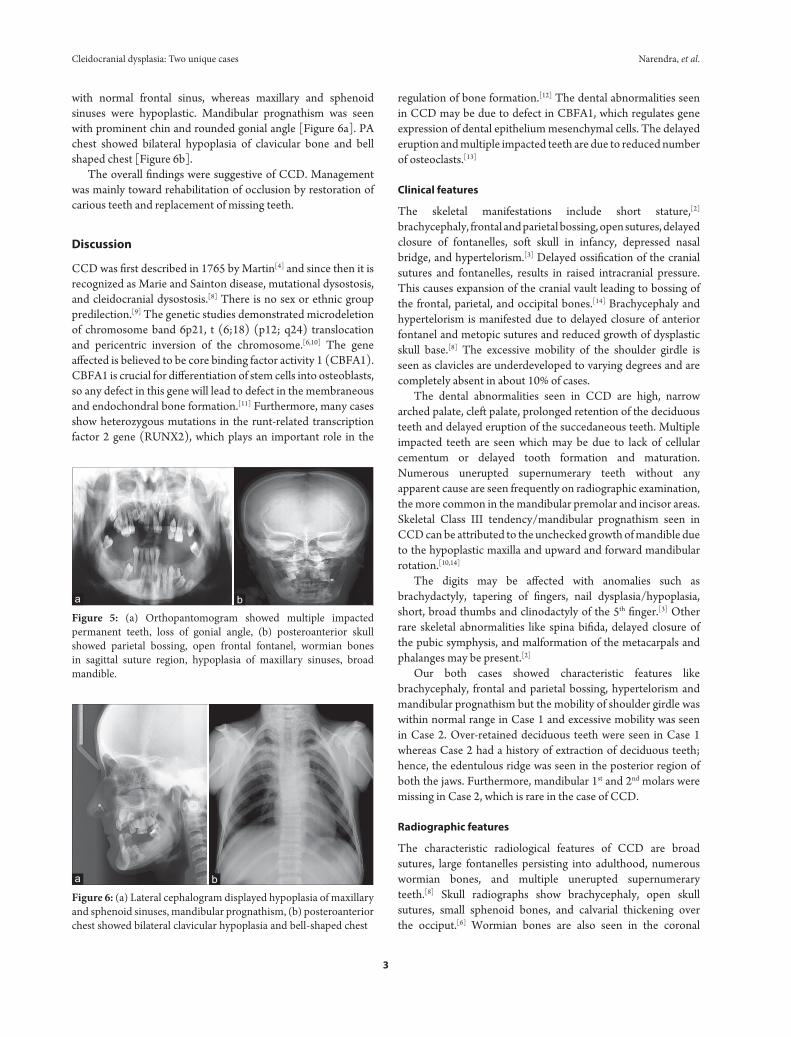
Extra oral examination revealed that stature of the patient was short. Head appeared large with frontal and parietal bossing, depressed nasal bridge, hypertelorism, slight mandibular prognathism. The forehead showed marked depression in the central area. Excessive mobility of shoulder was noted [Figure 4a and b]. Intraoral examination showed multiple missing permanent teeth, over-retained right deciduous mandibular canine and partially erupted anterior maxillary teeth [Figure 4c].
OPG showed multiple impacted permanent teeth in maxillary anterior and mandibular left posterior region. The teeth 36, 37, 46, 47 were missing. Gonial angle was lost from both sides [Figure 5a]. PA skull showed large cranium as compared to face because of parietal bossing. Open sagittal suture and fontanelle with wormian bones were seen. Mandible appeared broad as compared to the maxilla. Large, open multiple fontanelles were present [Figure 5b]. Lateral cephalogram showed frontal bossing
Figure 2: (a) Orthopantomogram: Multiple impacted supernumerary teeth, rounded gonial angle, and narrow ramus. (b) posteroanterior skull showed open sagittal suture, wormian bones, parietal bossing, aplasia of the frontal sinus, deviated nasal septum and wide mandible
Figure 1: (a and b) Extra oral view: Short stature, depressed nasal bridge, hypertelorism, (c) Intra oral view: Multiple over retained deciduous teeth
c
b
a
ba
Figure 3: (a) Lateral cephalogram displayed hypoplasia of all paranasal sinuses, mandibular prognathism, and open fontanelle, (b) posteroanterior chest showed bilateral mild clavicular hypoplasia
ba
Figure 4: (a and b) Extra oral showed parietal bossing, depressed nasal bridge, mandibular prognathism, (c) intra oral: Multiple missing teeth partially erupted maxillary anterior incisors
c
b
a
Cleidocranial dysplasia: Two unique cases Narendra, et al.
3
with normal frontal sinus, whereas maxillary and sphenoid sinuses were hypoplastic. Mandibular prognathism was seen with prominent chin and rounded gonial angle [Figure 6a]. PA chest showed bilateral hypoplasia of clavicular bone and bell shaped chest [Figure 6b].
The overall fi ndings were suggestive of CCD. Management was mainly toward rehabilitation of occlusion by restoration of carious teeth and replacement of missing teeth.
Discussion
CCD was fi rst described in 1765 by Martin[4] and since then it is recognized as Marie and Sainton disease, mutational dysostosis, and cleidocranial dysostosis.[8] There is no sex or ethnic group predilection.[9] The genetic studies demonstrated microdeletion of chromosome band 6p21, t (6;18) (p12; q24) translocation and pericentric inversion of the chromosome.[6,10] The gene aff ected is believed to be core binding factor activity 1 (CBFA1). CBFA1 is crucial for diff erentiation of stem cells into osteoblasts, so any defect in this gene will lead to defect in the membraneous and endochondral bone formation.[11] Furthermore, many cases show heterozygous mutations in the runt-related transcription factor 2 gene (RUNX2), which plays an important role in the
regulation of bone formation.[12] The dental abnormalities seen in CCD may be due to defect in CBFA1, which regulates gene expression of dental epithelium mesenchymal cells. The delayed eruption and multiple impacted teeth are due to reduced number of osteoclasts.[13]
Clinical features
The skeletal manifestations include short stature,[2] brachycephaly, frontal and parietal bossing, open sutures, delayed closure of fontanelles, soft skull in infancy, depressed nasal bridge, and hypertelorism.[3] Delayed ossifi cation of the cranial sutures and fontanelles, results in raised intracranial pressure. This causes expansion of the cranial vault leading to bossing of the frontal, parietal, and occipital bones.[14] Brachycephaly and hypertelorism is manifested due to delayed closure of anterior fontanel and metopic sutures and reduced growth of dysplastic skull base.[8] The excessive mobility of the shoulder girdle is seen as clavicles are underdeveloped to varying degrees and are completely absent in about 10% of cases.
The dental abnormalities seen in CCD are high, narrow arched palate, cleft palate, prolonged retention of the deciduous teeth and delayed eruption of the succedaneous teeth. Multiple impacted teeth are seen which may be due to lack of cellular cementum or delayed tooth formation and maturation. Numerous unerupted supernumerary teeth without any apparent cause are seen frequently on radiographic examination, the more common in the mandibular premolar and incisor areas. Skeletal Class III tendency/mandibular prognathism seen in CCD can be attributed to the unchecked growth of mandible due to the hypoplastic maxilla and upward and forward mandibular rotation.[10,14]
The digits may be aff ected with anomalies such as brachydactyly, tapering of fi ngers, nail dysplasia/hypoplasia, short, broad thumbs and clinodactyly of the 5th fi nger.[3] Other rare skeletal abnormalities like spina bifi da, delayed closure of the pubic symphysis, and malformation of the metacarpals and phalanges may be present.[2]
Our both cases showed characteristic features like brachycephaly, frontal and parietal bossing, hypertelorism and mandibular prognathism but the mobility of shoulder girdle was within normal range in Case 1 and excessive mobility was seen in Case 2. Over-retained deciduous teeth were seen in Case 1 whereas Case 2 had a history of extraction of deciduous teeth; hence, the edentulous ridge was seen in the posterior region of both the jaws. Furthermore, mandibular 1st and 2nd molars were missing in Case 2, which is rare in the case of CCD.
Radiographic features
The characteristic radiological features of CCD are broad sutures, large fontanelles persisting into adulthood, numerous wormian bones, and multiple unerupted supernumerary teeth.[8] Skull radiographs show brachycephaly, open skull sutures, small sphenoid bones, and calvarial thickening over the occiput.[6] Wormian bones are also seen in the coronal
Figure 5: (a) Orthopantomogram showed multiple impacted permanent teeth, loss of gonial angle, (b) posteroanterior skull showed parietal bossing, open frontal fontanel, wormian bones in sagittal suture region, hypoplasia of maxillary sinuses, broad mandible.
ba
Figure 6: (a) Lateral cephalogram displayed hypoplasia of maxillary and sphenoid sinuses, mandibular prognathism, (b) posteroanterior chest showed bilateral clavicular hypoplasia and bell-shaped chest
ba

Narendra, et al. Cleidocranial dysplasia: Two unique cases
4
and lambdoid regions because of the abnormal ossifi cation pattern.[14] Chest radiography shows a narrow thorax, oblique ribs and,[6] hypoplastic, aplastic, or discontinuous clavicles.[3] Bell shaped small thoracic cage having short ribs is also seen.[8]
OPG shows a narrow ascending ramus, slender and pointed coronoid process, thin zygomatic arch with a severe downward tilt, small or absent maxillary sinuses, coarse trabeculation of the mandible, and increased density of the alveolar crestal bone over unerupted teeth. The cellular cementum is completely absent, and acellular cementum is increased on the roots of the aff ected teeth.[6] Underdeveloped paranasal sinuses are also noted. Vertebral defects with scoliosis, kyphosis or lordosis, pelvic bony abnormalities and anomalies of phalangeal, tarsal, metatarsal, carpal and metacarpal bones are also present.[8] A wide pubic symphyseal space with a “chef’s hat” appearance of the femoral head is also seen.[6]
Both the cases had large fontanelles persisting into adulthood, numerous wormian bones, brachycephaly, open skull sutures, loss of gonial angle, zygomatic arch with a downward tilt and hypoplasia of maxillary sinuses. Multiple impacted supernumerary teeth were seen in Case 1, whereas Case 2 showed impacted permanent teeth, but there was only one supernumerary tooth, and mandibular 1st and 2nd molars were missing. These fi ndings diff er from other cases reported in the literature. Chest radiography revealed normal clavicle in Case 1 whereas Case 2 showed hypoplastic clavicle causing abnormal shoulder mobility.
Diff erential diagnosis
The lesions considered while diagnosis of CCD is osteogenesis imperfecta (frequent fractures), pycnodysostosis (skeletal density), and congenital hypothyroidism (disturbed thyroid metabolism). Gardner syndrome, Hallerman-Streiff syndrome (narrow face, hypotrichosis, mi- crophthalmia),[15] hypohidrotic ectodermal dysplasia (hypohidrosis, anomalous dentition, onychodysplasia, and hypotrichosis), focal dermal hypoplasia (relative focal absence of the dermis, skin atrophy, streaky pigmentation, multiple mucosal papillomas, and deformity of the extremities), apert syndrome (craniosynostosis, craniofacial abnormalities and symmetrical syndactly of the hands and feet), and craniofacial dysostosis (premature craniosynostosis with other abnormalities).[6]
Complications
CCD may show complications such as pes planus, genu velgum, shoulder and hip dislocation, recurrent sinus and ear infections, upper airway complications, hearing loss, dental caries, osteomyelitis of jaws, and respiratory distress in infants.[16]
Management
There is no specifi c treatment for CCD. The bony abnormalities cause little problem, so no treatment is required for the skull and clavicular deformities, but dental problems are most important complications and represent a major cause of functional and
esthetic morbidity. Treatment of clediocranial dysplasia is mainly focused on reducing the dentofacial deformity and correcting the malocclusion. A multidisciplinary approach consisting of pedodontist, an orthodontist, and an oral surgeon is required. Genetic counseling is recommended for people with a family history of CCD.
Treatment usually comprises of restoration or removal of retained carious primary teeth, surgical removal of supernumerary teeth, surgical exposure of permanent teeth, and orthodontic treatment for malalignment and appliances for growth modulation of jaws. Orthognathic surgery is required in severe skeletal Class III malocclusion cases or if a submucosal cleft is present. Guided eruption by orthodontic means is unsuccessful due to lack of cellular cementum.
The prognosis of patients is usually good with normal life expectancy. If proper treatment is not provided, the retained deciduous dentition begins to rapidly deteriorate in early adulthood, leading to premature aged facial appearance. Follow-up radiographs should be made to check for the development of new supernumerary teeth which may arise in the early to mid-teens.[2,10]
Conclusion
We presented two cases and discussed several pathognomic features of CCD. Case 1 showed predominant dental features, whereas Case 2 had skeletal abnormalities. Furthermore, few teeth were congenitally missing in Case 2 which is rare in CCD. CCD can be easily recognized if dental health care professionals are aware of its presentation. Early diagnosis and prompt management are important to correct aesthetic and functional problems and maintain the psychological and physiological well-being of the patient.
References
1. Wang S, Zhang S, Wang Y, Chen Y, Zhou L. Cleidocranial dysplasia syndrome: Clinical characteristics and mutation study of a Chinese family. Int J Clin Exp Med 2013;6:900-7.
2. Jayakumar N, Mohan S, Vimalraj R, Chhag S. Clinical spectrum of cleidocranial dysplasia. Health Sci 2014;3:1-5.
3. Mundlos S. Cleidocranial dysplasia: Clinical and molecular genetics. J Med Genet 1999;36:177-82.
4. Surej Kumar LK, Varun Menon P. Cleidocranial dysplasia: A case report. Integr J Br 2015;1:68-71.
5. Salem G. Nonfamilial cleidocranial dysplasia (dysostosis): A case report. Saudi Dent J 1990;3:112-5.
6. Mohan RP, Suma GN, Vashishth S, Goel S. Cleidocranial dysplasia: Clinico-radiological illustration of a rare case. J Oral Sci 2010;52:161-6.
7. Cooper SC, Flaitz CM, Johnston DA, Lee B, Hecht JT. A natural history of cleidocranial dysplasia. Am J Med Genet 2001;104:1-6.
8. Sakhi P, Yadav P, Susmitha R, Chawla A, Yadav CJ, Gupta J. Clinical spectrum of cleidocranial dysplasia: A case report. Natl J Community Med 2010;2:162-5.

Cleidocranial dysplasia: Two unique cases Narendra, et al.
5
9. Urzal V, Ferreira AP, Figueiredo A. Cleidocranial dysostosis: Case report of a multidisciplinary approach. Rev Odontol UNESP 2011;1:53-7.
10. Sharma A, Sharma S. Cleidocranial dysplasia: Report of a case. J Oral Health Community Dent 2009;3:62-5.
11. Toptancı IR, Colak H, Koseoglu S. Cleidocranial dysplasia: Etiology, clinicoradiological presentation and management. J Clin Exp Invest 2012;1:133-6.
12. Callea M, Bellacchio E, Di Stazio M, Fattori F, Bertini E, YavuzI, et al. A case of cleidocranial dysplasia with peculiar dental features: Pathogenetic role of the RUNX2 mutation and long
term follow-up. Oral Health Dent Manag 2014;13:548-51.13. Kolokitha OE, Papadopoulou AK. Cleidocranial dysplasia:
Etiology, clinical characteristics, diagnostic information and treatment approach. Hell Orthod Rev 2008;11:21-33.
14. Verma P, Verma KG, Gupta SD. Cleidocranial dysplasia: A dilemma in diagnosis? Arch Orofac Sci 2010;2:61-4.
15. Sekerci AE, Balta B, Bahadir O, Sisman Y, Dundar M, Tokmak TT. Cleidocranial dysplasia with a rare mutation: Study of a family with review of literature. Open J Stomatol 2013;3:402-10.
16. Dixit R, Dixit K, Paramez AR. Cleidocranial dysplasia. Lung India 2010;27:176-7.