Embed Size (px)
Citation preview

Click to edit Master title style
Working and living in an ongoing hazard context: influences on adjustment and migration of healthcare staff in Montserrat, West Indies
Victoria Sword-Daniels, Tiziana Rossetto, John Twigg, David Johnston, Thomas Wilson, Susanne Sargeant, Susan Loughlin,
Paul Cole

Click to edit Master title style• In disasters, community healthcare must be combined with emergency
medical care. To do this healthcare systems must remain functional.• Past disasters show that disruptions may stem from:
– Loss of utilities: power outages, air conditioning, communications, water, wastewater (earthquake and hurricane)
– Structural and non-structural damage (flood and earthquake damage)– Damage to equipment and supplies and isolation of facilities (hurricane,
flooding)– Overburden from high service demand and staff shortages (snowfalls)– Loss of personnel: leaving an affected area because of school
interruptions, partners’ jobs (hurricane)
Healthcare and disasters: a background
(Achour & Price, 2010; Berggren & Curiel, 2006; Kirsch et a., 2010; Rodriguez & Aguirre, 2006; PAHO, 2000; Mc Daniels et al., 2008)
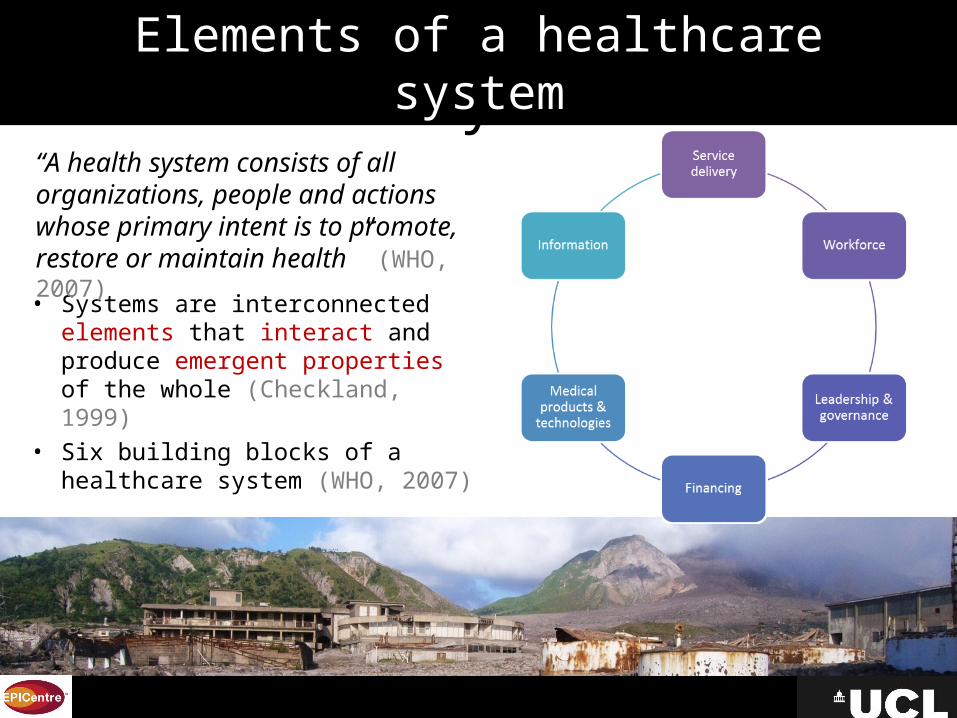
Click to edit Master title styleElements of a healthcare system
• Systems are interconnected elements that interact and produce emergent properties of the whole (Checkland, 1999)
• Six building blocks of a healthcare system (WHO, 2007)
“A health system consists of all organizations, people and actions whose primary intent is to promote, restore or maintain health” (WHO, 2007)

Click to edit Master title style• Research on healthcare systems in disasters focuses on hospitals (little
on wider healthcare systems), often single event high-impact hazards.
• There are no studies of the impacts of volcanic hazards on healthcare systems, or studies in long-term hazard/extended disaster contexts.
– What factors influence the function of the healthcare system in an ongoing volcanic hazard context?
– What are the challenges for staff working and living alongside a long-term volcanic eruption?
Research opportunity and questions

Click to edit Master title styleMontserrat as a case study
9x16km
Source: Seismic Research Unit
British Overseas Territory – locally elected Government and UK-appointed Governor
Small island context (colonial history, basic infrastructure systems and services, no duplication, small economy)
Volcanic eruption since 1995 (ongoing), relocation in 1996 (lack of housing and infrastructure)
Large-scale emigration: population was 10,639 in 1991, 4,922 in 2011 (GoM, 1991; 2011)
Villages 5-10 km from volcano: intermittently affected by ashfalls, gases, acid rain (mainly proximal, north west)
Low-middle income (financially supported by DFID, UK)

Click to edit Master title styleRelocation effects2012
• Hospital relocated to a school in St John’s
• Formerly 12 clinics, reduced to four
• Live-in district nursing has reduced (lack of available facilities)
• The number of registered nurses fell from 40 (1994) to 13 (1998) due to emigration

Click to edit Master title style
• Single exploratory case study (Field visits: 2010, 2011, 2012)• Qualitative methods:‒ 23 semi-structured interviews in healthcare‒ Four focus groups (n=28)‒ Four observation sessions (clinics) & fieldnotes• Topics: Effects of the eruption on the healthcare system, consequences
of ash, risk reduction approaches, benefits and challenges of living and working in Montserrat, future outlook
• Thematic analysis
Methods and analysis

Click to edit Master title styleResults: influences on healthcare system function (empirical themes)
Click to edit Master title style• Influences on decision-making to leave
– Circumstances: choices of others, lack of housing (long-term living in shelters), school interruption, loss of livelihoods, early retirement
• Influences on decision-making to stay– Circumstances: finances, care of children & elderly family membersN Opportunities for promotion: upward mobilityN Motivation to re-buildN Returning to island (challenges overseas)
• Emigration-immigration tensions: experience, language & culture
Original decisions to stay: push-pull factors

Click to edit Master title style• Influences on dynamic decision-making for staying or leaving
N Staff turnover is dynamic and increases during eruptions N Changes in hazards or circumstances promotes staff turnover (for
those who have choices)N High turnover of new staff – colleagues offer support and advice for
new staff membersN External perceptions (family, friends, other Islands) increases resolveN Benefits of staying (lifestyle; increased qualifications; civil service
employment; climate)
Dynamic tipping points: push-pull
‘Staff turnover increases during eruptions, people get fed-up and leave if it is prolonged and just say “I can’t take it anymore”.’ (Healthcare manager)
‘‘…I say look at me going England? I nearly have thirty years in Government, give up that for what now? I say no, me no want it…if I am to give up that then what happens?’ (Nurse)

Click to edit Master title styleLiving with hazards: psychosocial adjustment
2. Consequences of living and working with extensive risk
• Mixed feelings about eruptions• Comparing other hazards and past volcanic events: moderating fear• Choosing to accept hazards: individual points of acceptance• Feelings about ash: depression, decreased motivation, frustration
N ‘Ashing’ changes every aspect of life, ‘disgusting’, ‘a nuisance’N Ash gets in food, in clothes, and dries skin and hair
• Adjustments: staying indoors, cleaning approaches (dry/wet/coarse)• Personal coping mechanisms (exercise, breaks off-island, writing, faith)• Culture of preparedness (files updated, covering equipment)
‘I am scared of hurricanes more than I’m scared of the volcano. Because I had the bad experience with Hugo … I don’t want to even hear the word hurricane, I’m so fearful of it. The volcano? … once it’s not a threat, I’m happy.’ (Nurse)
‘People have to wear masks, which a lot of people don’t like - they feel like they are suffocating. So for me the biggest thing is the frame of mind it creates for people; I think people just become very depressed with the ash... Everywhere just ash and dust and the place looks so dismal.’ (Healthcare Manager)
Click to edit Master title styleLiving with hazards: work-life interactions
2. Consequences of living and working with extensive risk
• Balancing work and life: competing priorities during eruptionsN Collecting children to have them near (temporary clinic
closures, staff availability)N Emergency duties at work, leaving family at home to clean
• Cumulative effectsN Cleaning at work and cleaning at homeN Treating depression at work and feeing depressed

Click to edit Master title style• Several social and psychosocial factors influence people’s ability to live
and work in an ongoing hazard context• Staff migration affects the healthcare system though loss of
experienced staff, increased turnover and need for retraining – in a small island context this can mean loss of specialist services (single-trained staff)
• The extent to which individuals are able to adjust to living with hazards affects staff turnover
• Availability of staff in disasters depends on personal circumstances
Summary: influences on healthcare systems’ staff

Click to edit Master title style• Functioning healthcare systems are essential, especially in disasters. We need
to understand and account for the complex influences on healthcare systems in disasters
• Relocation and resettlement may reduce resources available for successful recovery (staff numbers, facilities, social and economic context)
• Small island healthcare systems are particularly vulnerable to disasters as there are few resources and limited specialist services
• Need to understand push-pull factors for migration, personal adjustment and work-life interactions to understand healthcare system function amid extended crises: these complexities of everyday life within the context help to understand effects of disruption as well as capacities to cope
Healthcare systems in small islands

Click to edit Master title style
• Participants in Montserrat• Senior healthcare management, Montserrat • Montserrat Volcano Observatory (MVO)• EPSRC• UCL Centre for Urban Sustainability and Resilience (USAR) & EPICentre• British Geological Survey (BGS)• University of Canterbury, New Zealand• Joint Centre for Disaster Research, New Zealand
Acknowledgements