Embed Size (px)
Citation preview

281
Introduction: climate change – the need for regional assessments
While uncertainty persists about the pace of climate change, there is scientifi c consensus that the build- up of greenhouse gases has resulted in global warming and climate change. The Intergovernmental Panel on Climate Change (IPCC), an effort of a global collective of scientists, projects that the Earth’s temperature could rise by as much as 4°C by the year 2100 depending on future trends of greenhouse gas emissions [1, 2]. The magnitude of the health consequences resulting from climate change will refl ect the actual increase in temperature. The consequences of greenhouse gas emissions for climate are not simply a warming uniformly across the globe, but rather the warming is anticipated to be variable by place and over time, and extremes of weather will be enhanced. The direct weather con sequences of climate change include warmer temperatures and more extreme conditions, and an associated sea- level rise, whereas the indirect consequences are broad with implications for human health (see Table 20.1 ). Beyond the adverse consequences listed in Table 20.1 , some regions may benefi t from warming through expanded agriculture and less need for heating.
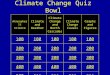
The health implications of climate change refl ect both direct and indirect pathways (see Figure 20.1 ). Climate change will not lead to new causes of morbidity and mortality, but will change the distributions of some causal factors that affect the occurrence of morbidity and mortality. For vector- borne infectious diseases (e.g. malaria), changes in the geographic distributions of vectors may lead to the emergence of diseases in places that have been previ-ously free from the particular diseases. There is concern, for example, about the potential for malaria to re- enter places where it has long been eliminated if the range of its vector, the Anopheles mosquito, expands. Changes in fl ora may bring new allergens and crop yields may drop. Air pollution may worsen from fossil fuel combustion for power generation to meet increasing cooling needs due to warming and other energy demands to adapt to climate change. Rising sea levels and weather changes with consequences for agriculture and availa-bility of water may displace people and lead to social and economic disruption with diverse potential implications for health.
The consequences of climate change for human health will be manifested differentially across broad regions of the world. The extent of change is projected to be variable, at least on
20
Climate change and health
Jonathan M. Samet and Junfeng (Jim) Zhang
26356.indb 28126356.indb 281 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
282
Table 20.1 Potential threats and health consequences of climate change
Threat Consequence
Increased frequency and intensity of heatwaves Increased mortality from heatwaves, particularly in elderly
Altered distributions of aeroallergens Increased frequency and severity of allergic diseases and symptoms
Altered distributions of vectors of infectious diseases
Spread of infectious diseases and increased frequency
Increased air pollution Increased morbidity and premature mortality Changing agricultural yields More undernourished people in low- income
countries Social and economic disruptions, displacement Various, with acute and chronic consequences
Figure 20.1 Schematic diagram of pathways by which climate change affects health, and concurrent direct- acting and modifying (conditioning) infl uences of environ-mental, social and health- system factors [2]
26356.indb 28226356.indb 282 16/12/13 7:34 PM16/12/13 7:34 PM

283
Climate change and health
the regional scale – populations vary in their vulnerability and resilience, and adaptive capacity and resources also differ. Consequently, the IPCC provides regional assessments giving specifi c insights into anticipated impacts of climate change, including effects on human health. In its Fourth Assessment Report, the IPCC includes a chapter on Asia that offers fi nd-ings used in this chapter [1, 2]. Additionally, in 2012, the World Health Organization (WHO) and the World Meteorological Organization (WMO) collaborated in the publication of the Atlas of Health and Climate , which provides useful maps that highlight the geographic diversity of the health consequences of climate change [3].
This chapter begins with an overview of the health consequences of climate change, covering effects that result through both direct and indirect paths. It considers not only the health consequences, but also the specifi c measures that might be taken to reduce impact. We then turn to the health consequences of climate change that are projected for South/East Asia. Of necessity, our coverage of this wide- ranging set of topics is brief. For further infor-mation, we recommend the reports of the IPCC, as well as the series in Lancet on climate change and health [4, 5].
Mechanisms by which climate change affects health
Climate change has been labelled as ‘the biggest global health threat of the 21st century’. In so labelling it, the Lancet and the University College London Institute for Global Health Commission cited the far reach of climate change and its diverse threats to human health [6]. Estimates of the potential burden of premature mortality and additional morbidity from climate change, while subject to great uncertainty, indicate a looming, substantial impact. For the year 2000, climate change was estimated to have caused the premature loss of about 150,000 lives and about 5.5 million disability- adjusted life- years (DALYs), representing 0.3 per cent of total deaths and 0.4 per cent of all DALYs, respectively [7].
Climate change affects health within the complex, multilevel system that determines the health of individuals and populations, including social, economic and health systems and governmental determinants (see Figure 20.1 ). The time domains of the stressor and adaptive and mitigative responses are also relevant. The acute stress of a catastrophic and large- scale weather event may overwhelm countering responses and mitigating mechanisms – the devas-tation caused by Hurricane Sandy to the East Coast of the United States (US) in 2012 is exemplary. The health status of the population affected is also a key consideration, as is the adequacy of its health system. Responses to the stressors associated with climate change may vary with the age structure of the population, the prevalence of chronic diseases and the capacity of the health system to provide care for the burden of disease that might arise from a climate- change driven event. There is concern that climate change could cause large- scale social and economic disruption through drought, famine and sea- level rise, and migration could lead to instability and confl ict. For such consequences, the geopolitics of the world at the time will be critical [8].
There is the additional conceptual complexity of determining that health consequences are attributable to climate change. The assignment of causation is based on the concept of comparing actual events to scenarios of what might have happened absent climate change – the so- called counterfactual. For weather events, for example, a comparison is between the number of extreme events with health consequences, compared with the number gener-ated by climate models in the absence of human- forced climate change. Such comparisons are conceptually challenging and not readily communicated to decision- makers and the public.
26356.indb 28326356.indb 283 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
284
Heat stress and heatwaves
Temperature has long been associated with adverse effects on health and mortality. At extreme temperatures, the well- known clinical entities of hypothermia and hyperthermia are docu-mented causes of death [9]. For climate change, exposure to heat and hyperthermia are of particular concern, given the resulting warming and increased frequency of extreme events with dangerously high temperatures. Hyperthermia occurs when temperatures are high among persons carrying out physical activities that lead to thermal stress, as well as among people who are susceptible to heat because of limited adaptive capacity, such as infants, the elderly and persons taking medications that impair responses to thermal stress (e.g. medica-tions widely used for hypertension and heart disease). Even in developed countries, excess deaths from heat and heatwaves remain common and dramatic heatwaves with large numbers of deaths continue to occur. For example, in recent decades, the dramatic and well- documented epidemics of death associated with heatwaves in Chicago in 1995 (about 750 excess deaths [10]) and in Europe in 2003 (about 35,000 or more excess deaths [11, 12]), have alerted the public to the dangers of heatwaves and led to protective actions by governments and public health agencies.
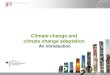
Warmer temperatures are associated with mortality even in times when heatwaves are not in progress [9, 12]. The relationship between temperature and mortality has been character-ized as ‘J-shaped’, such that mortality increases with both colder and warmer temperatures from an optimum temperature at which it is the lowest [13, 14]. Figure 20.2 provides
Figure 20.2 Temperature- mortality relative risk functions for 11 US cities, 1973–1994 [13] Note °C = 5/9 x (°F – 32)
26356.indb 28426356.indb 284 16/12/13 7:34 PM16/12/13 7:34 PM

285
Climate change and health
illustrative analyses from 11 US cities. In almost all cities, the temperature with the lowest risk for mortality is evident and the upturn with higher temperature is more prominent in northern cities. The optimum temperature varies inversely with average temperature, and hence latitude, as well as the extent to which adaptive measures, such as air conditioning, are in place for buffering warmer or colder temperatures [12, 13, 15]. This J-shaped relationship has implications for the potential overall effect of global warming consequent to climate change on heat- associated mortality. Warming would reduce the cold- associated mortality while increasing heat- associated mortality, minus the new adaptive measures [13]. However, beyond the rise in average temperature, climate change is also projected to increase the vari-ability of temperature and the frequency of heatwaves [1, 2]. There is an effect of heatwaves per se and the temperature profi le of heatwaves seems to be a critical determinant of excess mortality [16].
Evidence suggests that the risk of heat- related excess mortality has declined on longer time frames. Carson and colleagues [17] examined weekly mortality in London during the twen-tieth century and assessed temperature- associated mortality over a period during which a major shift occurred in the underlying causes of death, the population became progressively older and the proportion affected by chronic diseases increased. They found declines in susceptibility to dying from both cold and heat. Carson et al. attributed this fi nding to factors related to social and environmental conditions, behaviour and health care. Davis et al. [18] examined heat- related mortality over the period between 1964 and 1998 in the US and also found declining heat mortality, which they attributed to various adaptations, including the increased availability of air conditioning. Barnett [19] found that the association of warm temperature with cardiovascular mortality during the summer declined substantially over the period between 1987 and 2004.
Population characteristics also affect the impact of heatwaves. The elderly and persons with underlying chronic diseases, such as coronary heart disease and congestive heart failure, are particularly at risk. Additionally, individuals taking diuretics, or taking some drugs used for blood pressure control and/or other drugs may have impaired cardiovascular responses to thermal stress, as may those who are obese. In the ageing populations of the more developed countries, these at- risk groups are increasing. Epidemiological analyses have identifi ed addi-tional risk factors for mortality during heatwaves, including a lack of social support, socio- economic status and housing characteristics. In urban areas, the ‘urban heat island’ phenomenon tends to increase the risk of mortality associated with heatwaves [20]. Determinants of risk in less developed countries have received little research attention. In such countries, there is a very low prevalence of air conditioning.
Because the elderly and people with underlying chronic diseases are particularly suscep-tible, the hypothesis has been advanced that the excess mortality associated with heatwaves comes from a brief advancement of the time of dying, a phenomenon sometimes referred to as ‘mortality displacement’ or ‘harvesting’. If such mortality displacement is occurring, a reduction in mortality would be anticipated following the excess associated with the heatwave and, indeed, analytical approaches have been developed for assessing mortality displacement [21, 22]. Regarding the 2003 heatwave in France, the extent of mortality displacement was found to be modest [23]. Parallel analyses of heat- related deaths in Delhi, São Paulo and London, using distributed lag models, found some mortality displacement in London and a lesser indication of this phenomenon in Delhi [24], with the pattern being intermediate for São Paulo. These results, as well as descriptive observations on the ages of individuals dying during heatwaves, suggest that heatwaves do not affect only the most vulnerable.
26356.indb 28526356.indb 285 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
286
Where there is little evidence on temperature- associated mortality in developing coun-tries, greater excess mortality might be anticipated because of limited penetration of air conditioning, the density of megacities and limited attention to the problem by public health authorities. The ISOTHURM project examined the temperature–mortality relationship in 12 urban areas, including several in low- and middle- income countries [14]. The data from most of the cities showed the typical J-shaped relationship with temperature. In Delhi and Salvador, mortality did not increase at colder temperatures, nor did an increase occur at hotter temperatures in Chiang Mai and Cape Town.
Aeroallergens and allergic diseases
Aeroallergens – biological agents associated with allergic responses – are ubiquitous in indoor and outdoor environments. The two principal and most prevalent diseases associated with aeroallergens are allergic rhinitis, also referred to as hay fever and asthma [25]. Aeroallergens are known to exacerbate asthma and trigger attacks of allergic rhinitis.
For persons with allergic rhinitis and asthma, climate change might increase the risk of exacerbation through altered local and regional pollen production. Warming has already caused an earlier onset of the spring pollen season in the Northern Hemisphere [1, 2]. It may also lengthen the pollen season, change the spatial distribution of vegetation and possibly alter pollen production [1, 2, 26, 27]. Evidence suggests that climate change has changed expo-sures of populations to aeroallergens [1, 2, 28]. Vegetation patterns have changed and pollina-tion is occurring earlier for some species in some places. New species could potentially become successful in additional areas, leading to exposures of populations to new antigens. More prolonged and intense exposure to aeroallergens could result in more severe disease and greater morbidity, and even increased mortality from asthma. Beggs and Bambrick [27] have proposed that climate change could be contributing to the global rise in asthma as a conse-quence of greater pollen exposure.
Changes in endemic and epidemic infectious diseases
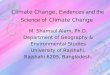
Worldwide, in both developed and developing countries, infectious agents remain a leading cause of disease and death [29]. Warming from climate change has the potential to affect the transmission of infectious diseases across the globe. The transmission of these diseases is conceptually described by the ‘epidemiological triangle’ (see Figure 20.3 ), which captures the interplay between its components: the agent, the environment and the vector. Environmental conditions that promote or extend the geographic range of the vector increase the potential for infection. In addition to potentially affecting vector- borne diseases, climate change may also extend or change the geographic regions in which an infectious agent is present. Climate change may affect both endemic disease (i.e. disease generally occurring in a population) and epidemic disease (i.e. disease occurring in excess of normal expectancy). The time frames over which climate change could affect infectious diseases extend from relatively short, as even the temperature rise to date has had apparent impact, to relatively long, as continued temperature increases would be predicted to continue to alter vector distributions and densities.
Mathematical models of infectious disease transmission provide quantitative insight into the potential for climate change to increase rates of vector- borne diseases. The potential for transmission of infectious diseases is characterized by the basic reproductive rate (R 0 ) which describes the number of new cases of infection arising from one case in a population of
26356.indb 28626356.indb 286 16/12/13 7:34 PM16/12/13 7:34 PM

287
Climate change and health
susceptible persons [30]. Values above unity imply the possibility of epidemic disease – a value of unity means that endemic disease will be maintained and a value below unity means that the disease will decline. Warming can increase R 0 through its effect on vector numbers, transmission probabilities and biting rates for insect vectors [30]. The geographic spread of vectors may also be affected by the extension of their ranges resulting from warmer condi-tions. Several vector- borne diseases are considered to be potentially sensitive to climate change [31] (see Table 20.2 ).
Waterborne and airborne diseases may also be affected by climate change. For diseases transmitted by water, warming may enlarge the geographic area in which conditions are suit-able for survival of disease- causing organisms and for propagation of infection [32, 33]. The occurrence of waterborne infections has also been linked to extreme weather events [34]. Increased air conditioning and more time spent indoors, because of warming, might affect patterns for diseases that are transmitted in indoor environments by droplets or by contact, such as infl uenza and the common cold.
Figure 20.3 The epidemiological triangle of epidemics
Table 20.2 Examples of vector- borne diseases likely to be sensitive to climate change
Vector Major diseases
Mosquitoes Malaria, fi lariasis, dengue fever, yellow fever, West Nile fever
Sandfl ies Leishmaniasis Triatomines Chagas disease Ixodes ticks Lyme disease, tick- borne encephalitis Tsetse fl ies African trypanosomiasis Blackfl ies Onchocerciasis Snails (intermediate host) Schistosomiasis
Source: [31].
26356.indb 28726356.indb 287 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
288
Cholera illustrates the complexity of understanding how climate change can alter the occurrence of infectious diseases [32, 33]. The disease- causing organism, Vibrio cholera , is endemic and widely found in water. Multiple global cholera pandemics have been docu-mented – the seventh, which began in 1961, is still ongoing. The present epidemic began with the emergence of a new biotype, the El Tor biotype of V. cholerae 01, in Indonesia. In 1991, the pandemic moved to South America, with outbreaks along the Pacifi c coast. The epidem-ic’s occurrence was linked to a plankton bloom that was driven by the El Niño Southern Oscillation (ENSO). The planktonic copepod organism harbours the V. cholera organisms on its surface. Consequently, a higher concentration of plankton increases the dose of the infec-tious agent received from drinking contaminated water. A time- series analysis of cholera in Bangladesh found a link with the ENSO phenomenon [35]. Lipp and colleagues [33] propose that climate change could affect each step in their model for cholera transmission. Checkley and colleagues [36] carried out a time- series analysis of temperature changes associated with the ENSO and all hospital admissions for diarrhoea in children in Peru. Over the period between 1993 and 1998, they found that the numbers of admissions were positively associated with temperature and also with the ENSO, which had an effect on the admissions rate beyond that expected from the temperature increase alone.
Changes in the epidemiological characteristics of other infectious diseases have been examined in relation to climate change. Dengue transmission was addressed in the IPCC report [1, 2] and in specifi c studies [37]. In Western Australia, Woodruff et al. [38] found that climate data predicted epidemics of the Ross River virus disease (which is spread by mosqui-toes) reasonably well, particularly if data on mosquitoes were incorporated into the model. Studies have also addressed tick- borne disease [39, 40] and food- borne disease [41]. The potential for malaria to increase as a consequence of climate change has been controversial and malaria is receding globally in spite of some predictions that it would intensify as the world warms [42] (see chapters 18 and 19).
Many factors determine susceptibility to infection and the severity of the resulting illness, including mortality risk. In developed countries, key factors include age, immunocompe-tence, presence of comorbid chronic diseases (e.g. coronary heart disease, chronic obstructive pulmonary disease and diabetes), access to vaccines and to medical care, and the quality of the medical care available. In developing countries, additional determinants of severity include general nutritional status and specifi c micronutrient defi ciencies. The level of sanitation, the availability and use of preventive measures (such as bed nets and vector control), and the availability of vaccinations determine transmission probabilities. In both developed and developing countries large populations are at risk for more severe infections and mortality.
Ambient air pollution
Climate change may worsen air pollution, either directly (through increased tropospheric – ground- level – ozone production) or indirectly (through greater power plant emissions as power generation increases to meet the demand for air conditioning capacity). Ozone is a secondary pollutant formed via sunlight- driven photochemical reactions involving precursor hydrocarbons and oxides of nitrogen. Together with ozone, other secondary products are generated, forming the complex mixture of photochemical smog. Ozone pollution is projected to increase because warmer temperatures increase ozone production [1, 2]. Warmer temperatures enhance the chemical reactions that generate ozone. Under various scenarios, increases of several parts per billion are projected over the next two decades [43] and up to a range of 10 to 30 parts per billion by the end of this century [44]. Fossil fuel combustion
26356.indb 28826356.indb 288 16/12/13 7:34 PM16/12/13 7:34 PM

289
Climate change and health
contaminates the atmosphere with the primary particles generated by combustion and with the secondary particles formed from gaseous components of power plant emissions through complex chemical and physical processes. Increased fossil fuel burning could also worsen particulate air pollution, beyond predictions from climate change scenarios [1, 2, 45].
The health risks of both ozone and airborne particles have been characterized in numerous epidemiological studies, with supporting evidence coming from in vivo and in vitro toxico-logical research [46, 47, 48]. Both ozone and particulate matter (PM) air pollution have been associated with an increased risk of mortality in time- series studies of daily mortality [49, 50, 51] and airborne particles have also been associated with an increased risk of death on longer time frames [47, 51 52]. Both types of pollution are also associated with morbidity, including an increased risk for hospitalization [51, 53] and other adverse outcomes [48]. A quickly expanding body of evidence links particulate air pollution to adverse cardiovascular effects [52]. As for temperature and infection, a substantial proportion of the population is at increased risk because of older age and comorbidity, particularly respiratory and cardiac diseases.
Analyses that link climate change model outputs to ozone concentrations have been carried out for cities in the US. Knowlton et al. [54] projected future increases in ozone concentration for 31 counties of the New York metropolitan region. Considering the impact of climate change alone on ozone concentration, they estimated a median 4.5 per cent increase in summertime ozone- related, acute, all- cause mortality for all the counties. Bell et al. [55] performed a similar modelling for 50 cities in eastern US. They estimated the average increase in daily one- hour maximum concentration as 4.8 parts per billion. Depending on the concen-tration–response relationship used, the increase in ozone concentration corresponded to an increase in daily, all- cause mortality of 0.11 to 0.27 per cent.
Analyses have also addressed particulate air pollution, considering potential risks of increased fossil fuel combustion and benefi ts for health of reducing air pollution through greenhouse gas mitigation [45, 56]. In one assessment, enhanced energy consumption based on fossil fuel combustion was projected as leading to substantial increase in premature mortality [45]. In a scenario of business as usual that results in increased exposure to PM air pollution, an additional 700,000 premature deaths were forecast. Similarly, in an analysis of four of the world’s major cities (Mexico City, New York City, Santiago and São Paulo), Cifuentes et al. [56] predicted that reductions of ozone and particles from mitigation would substantially reduce premature mortality.
In addition, air pollution and thermal stress may act synergistically: both affect the same susceptible populations and mean that hot temperatures will increase ozone production. A few studies have addressed such synergism. In Athens, the short- term effect of sulphur dioxide on daily mortality was independent of temperature over the period between 1975 and 1982 [57]. An analysis of mortality in Athens during a 1987 heatwave suggested synergism of air pollution with higher temperatures [58]. Filleul and colleagues [59] examined the contribu-tions of ozone and temperature to the excess mortality observed in nine French cities during the 2003 heatwave. They estimated that both ozone and heat contributed to the excess and found that the relative contributions varied from city to city. Fischer et al. [60] published similar fi ndings for the Netherlands during the 2003 heatwave. Neither analysis tested for synergism between ozone and temperature. Synergistic effects of aeroallergens and urban air pollutants (such as ozone and particulate matter) on asthma and allergenicity have been examined in epidemiological and toxicological studies [61, 62]. A recent study showed that ragweed pollen collected along high- traffi c roads induced higher allergenicity than ragweed pollen sampled in vegetated areas, suggesting that traffi c- related pollution enhances pollen allergenicity [63].
26356.indb 28926356.indb 289 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
290
Climate change and social and economic disruption
The possibility of social and economic disruption from climate change looms large for much of the world, including Asia. Climate change can threaten food security, lead to desertifi ca-tion and threaten water supplies [5]. Agricultural productivity is likely to suffer as a result. Sea- level rise may force migration from coastal areas, leading to crowding and potentially to cross- border migration. In Asia, sea- level rise would cause large- scale inundation along the vast Asian coastline and recession of fl at sandy beaches. The ecological stability of mangroves and coral reefs around Asia would be put at risk. The potential implications for health of the social and economic impacts of these broad consequences of climate change are enormous, including inadequate food and water supplies, breakdown of governmental services and failure of health systems. There is also potential for confl ict over resources, possibly water access and agricultural land.
Specifi c health outcomes and adaptation measures
The inevitable consequences of climate change, as described above, require responsible actions to mitigate the problem. Central to the mitigation debate is the reduction of CO 2 emissions by using renewable energy sources, cleaner fossil fuels and improving energy effi -ciencies. Given that CO 2 has a long- term half- life in the atmosphere, proposals to mitigate short- lived warming pollutants such as methane and black carbon have gained support in recent years, especially under the notion of ‘co- benefi ts’. In addition to having a larger warming potential than CO 2 on a per- molecule basis, methane is a precursor of troposphere ozone and black carbon (BC) is considered to be a more toxic component of airborne fi ne particulate matter. In a recent assessment of 14 specifi c emission control measures targeting BC and methane to reduce the rate of climate change over the next 20–40 years, Anenberg et al. [64] found that in addition to climate benefi ts, the methane and BC emission control measures would have substantial co- benefi ts for air quality and public health worldwide, potentially reversing trends of increasing air pollution concentrations and mortality in Africa, and South, West and Central Asia. The projected benefi ts are independent of CO 2 mitigation measures.
Perhaps more urgent than mitigating greenhouse pollutants is developing adaptation strat-egies. We consider a number of adaptation measures, at both societal and individual levels, that are specifi c to pathways through which climate change affects health outcomes. Across all pathways, assessment of the impact of climate change is the fi rst step for exploring adapta-tion strategies. In general, disease surveillance systems are essential for acquiring data needed for impact assessment. Specifi cally, monitoring of diseases, along with related meteorological data and ecological factors, is needed to track the impact of weather factors by each pathway, as shown in Table 20.3 . Disease monitoring is also necessary for assessing the effectiveness and effi ciency of adaptation measures [65]. For example, heat watch and warning systems imple-mented in the US have proven effective in helping to minimize the impact of heatwaves [66]. A similar system has been recently initiated in Shanghai, China [67].
Other adaptation strategies include improvements in assuring safe water and food distribu-tion, disaster preparedness and management, and improvements in public infrastructure, such as healthcare facilities and emergency shelters [68]. Improving socio- economic status through sustainable and equitable socio- economic development can substantially enhance social capital and reduce the vulnerability of developing countries of Asia to climate change. Adaptations to deal with sea- level rise, potentially more intense cyclones and threats to
26356.indb 29026356.indb 290 16/12/13 7:34 PM16/12/13 7:34 PM

291
Climate change and health
ecosystems and biodiversity are recommended as high- priority actions in coastal areas of temperate and tropical countries [1, 2].
Climate change in South/East Asia
In the following sections, we focus on several sub- regions of Asia: South Asia and Southeast Asia based on the defi nition in the IPCC report [1, 2]. We use the term ‘South/East Asia’ when referring non- specifi cally to South Asia and Southeast Asia.
Asia is the most populous continent, covering 30 per cent of the Earth’s land surface, but home to over 4 billion people in 2010 or about 60 per cent of the world’s total. During the twentieth century, Asia’s population nearly quadrupled. The majority of the region’s popula-tion growth is projected to come from South Asia, which is anticipated to add 570 million people in India, 200 million in Pakistan and 130 million in Bangladesh over the next 50 years [69]. The projected population growth, especially in regions with high baseline population densities, implies increased pressure on the natural resources and the environment (e.g. defor-estation, fl oods, droughts and disrupted ecosystems) [70]. For example, in the developing regions of Asia, the remaining natural fl ood plains are disappearing at an accelerating rate, due primarily to changes in land use and hydrological cycle. The most threatened fl ood plains may be those in South and Southeast Asia [71], and this loss of fl ood plains makes the region more vulnerable to climate change.
Southeast Asia is characterized by tropical rainforests, monsoon climates with high and constant rainfall, and heavily leached soils. The coastlines in monsoon Asia are cyclone- prone with approximately 40 per cent of the world’s total tropical cyclones occurring in this region [72]. This region has reportedly undergone a 0.1°C to 0.3°C increase per decade from 1951
Table 20.3 Examples of climate change- related health outcomes and possible adaptation measures
Pathways Health outcome Adaptation measures
Direct effects of heat Mortality, dehydration, hypothermia, hyperthermia
Using air conditioners, heat warning systems and shelters for the public
Effects of urban air pollution
Cardio- respiratory mortality and morbidity, adverse birth outcome
Staying indoors, adding fi lters to building ventilation systems
Effects of aeroallergens
Asthma, allergic rhinitis, sinusitis, allergies
Staying indoors, using fi lters, medical therapies
Water- borne/food- borne diseases
Diarrhoeal diseases, bacillary dysentery
Enhancing monitoring of water and food quality, enhancing personal hygiene practices
Vector- borne diseases
Malaria, dengue, Japanese encephalitis, West Nile virus
Enhancing mosquito controls, enhancing disease surveillance and infectious disease controls
Disasters (drought, fl oods, forest fi res, etc.)
Drowning, injury, mental health problems, increased susceptibility to infections
Improving public infrastructures (e.g. forecast and evacuation capacities) in response to natural disasters
Malnutrition Underweight, increased susceptibility to disease and infections
Advancing technologies to improve crop yields, especially in poor agriculture communities; implementing policies and other means to reduce poverty
26356.indb 29126356.indb 291 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
292
to 2000 [73]. Furthermore, extreme weather events associated with El Niño were reported to be more frequent and intense in the past 20 years [74, 75]. For example, increased occurrence of extreme rains caused fl ash fl oods in Vietnam, landslides and fl oods in 1990 and 2004 in the Philippines and fl oods in Cambodia in 2000 [76, 77]. Since 1970, the frequency and intensity of tropical cyclones originating in the Pacifi c have increased [78], while cyclones originating from the Bay of Bengal and Arabian Sea have decreased in frequency but increased in inten-sity [79]. In both cases, the damage caused by intense cyclones has risen signifi cantly in the affected countries, particularly India, the Philippines, Vietnam and Cambodia, as well as Japan and China [1, 2].
Temperature projections for the twenty- fi rst century, based on the Fourth Assessment Report of IPCC [1, 2], suggest a signifi cant acceleration of warming over that observed in the twentieth century [80, 81]. Given that South/East Asia has vast coastlines and consists of many islands, sea- level rise due to warming is a practical and serious concern. Fundamental thermodynamics and climate models suggest that dry regions will become drier and wet regions will become wetter in response to global warming [82]. These model results suggest that the absence of climate mitigation will further increase the intensity and frequency of typhoons, tropical storms, fl oods and landslides in South/East Asia.
Health impacts of climate change in South/East Asia
Compared to the ‘global average’, several of the pathways through which climate change affects human health may be amplifi ed in South/East Asia, with some areas already experi-encing a scarcity of resources, environmental degradation and high rates of infectious disease, in the context of weak infrastructure and overpopulation [83, 84]. In particular, tropical regions of South/East Asia will experience signifi cant changes in human–pathogen relation-ships due to climate change [85, 86]. Changing temperatures and precipitation patterns linked to climate change will further affect health by changing the ecology of various vector- borne diseases, such as malaria, dengue, chikungunya, Japanese encephalitis, kala- azar and fi lariasis [87, 88]. The numbers within the vulnerable groups are large [89, 90].
Impact on urban populations and population migration
Major cities, including Bangkok, Jakarta, Manila and Ho Chi Minh City, are at risk as the sea rises [91]. In general, cities are vulnerable to the health impacts of climate change, partly because of urban heat island effects and urban air pollution. Long heatwaves and urban smog are indeed a potent and injurious combination to which urban areas in South/East Asia are vulnerable [83, 91].
Additionally, populations in cities throughout South/East Asia are growing rapidly. Rapid population growth and urbanization force poor people to move to fragile and high- risk areas prone to natural hazards. Moreover, the rapid growth of industries in urban areas drives people to migrate from rural areas to urban/industrialized areas. Such population migration brings substantial challenges for implementing many of the adaptation measures described earlier in this chapter because it is diffi cult to expand the infrastructure at a pace matching the speed of population growth. A further complication to this socio- economic-driven migration is the expected population movement following extreme weather events. Such unplanned migration has signifi cant public health implications at its origins, along the migration routes and in the receptor areas [92]. The countries/areas that can be potentially affected by climate- induced population migration (often accompanied by pathogen migration) need to develop
26356.indb 29226356.indb 292 16/12/13 7:34 PM16/12/13 7:34 PM

293
Climate change and health
preparedness and adaptation strategies to minimize the potential for resulting catastrophic damage [93].
Impact on vector- borne and infectious diseases
Mortality and morbidity from diarrhoeal diseases and malnutrition attributable to climate change were already the largest in South/East Asian countries including Bangladesh, Bhutan, India, Maldives, Myanmar and Nepal in 2000 [94]. In this region, endemic morbidity and mortality due to diarrhoeal disease have been linked to poverty and hygiene behaviour, accel-erated by the effect of high temperatures on bacterial proliferation [36]. Incidence rates and frequency of outbreaks of diarrhoeal and other infectious diseases (e.g. cholera, hepatitis, malaria, dengue fever) have also been linked to climate- related factors, such as fl oods, droughts, rising sea- surface temperatures and rainfall. Other relevant factors include the scope of the susceptible population, e.g. children, the elderly and the impoverished; lack of access to safe drinking water; and inadequate sewer systems [1, 2, 95]. Increases in sea- surface temperature due to climate change will increase the growth of phytoplankton along the coastlines of South/East Asia. Phytoplankton blooms are excellent habitats for survival and spread of bacteria responsible for infectious diseases such as cholera [96]. Increases in the frequency and intensity of fl oods from increased precipitation and sea- level rise in the future, absent of adequate mitigation/adaptation measures, will lead to drinking water contamina-tion and consequently increased water- borne infectious diseases. Based on the trends in temperature and rainfall, it is projected that the frequency of vector- borne and water- borne infectious diseases in Southeast Asia will remain the highest in the world in 2030 [94].
The distribution of vector- borne diseases such as malaria and dengue fever is infl uenced by the spread of vectors (e.g. mosquitoes) and the climate dependence of the infectious patho-gens. A warmer and more humid climate is favourable for propagation and invasiveness of infectious insect vector. For example, evidence shows that dengue incidence in metropolitan Manila varies with changing rainfall patterns [97]. As Singapore experienced higher weekly mean temperatures and cumulative precipitation in the years 2004–2007, a signifi cant increase in intensity and number of dengue fever cases could be attributed to climate factors [98]. As the increasing trends in surface temperature and rainfalls are likely to continue in the South/East Asia, intensifi ed surveillance and control of mosquitoes during periods with high rain-falls are recommended [97].
Poverty and vulnerability
A signifi cant portion of the Asian population is living below social and economic poverty thresholds [99]. Most of the world’s poor reside in South Asia and, within the region, the majority resides in rural areas [100], although rural- to-urban migration continues to increase. The poor are highly vulnerable to climate change because of their limited access to stable livelihood opportunities and limited access to areas that are fi t for safe and healthy habitation. Consequently, those who are impoverished are more likely to be at increased risks from fl oods, droughts, and contaminated water and foods [101]. Without appropriate measures, climate change will likely exacerbate the poverty situation and increase social inequity [102], as those who live in poverty contribute far less greenhouse gases on a per capita basis than wealthier persons. Consequently, there needs to be equity in assuring that those living in poverty advance economically in order to have enhanced capacity for adaptation. Crucial infrastructure should be designed and constructed to withstand extreme events for all who
26356.indb 29326356.indb 293 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
294
will be potentially affected. Health care and education should be strengthened, inequality addressed, and resources directed to communication and surveillance systems/technologies. Intensive development in very low- lying areas should be avoided, although large numbers of people are living at sea level in South/East Asia [91].
Conclusion
South/East Asia, with vast coastal areas and vector- prone climate, is one of the most vulner-able regions, facing a range of adverse health outcomes of climate change. It has many impov-erished inhabitants and its coastal cities and megacities are at risk from the direct and indirect stressors associated with climate change. For the short- term, adaptive strategies are needed for heatwaves and other extreme weather events. For the longer term, the success of global miti-gation strategies will be critical, particularly if sea- level rise is to be slowed, and the threat to agriculture and water security minimized.
Acknowledgements
The authors thank Athena Foong, Department of Preventive Medicine, Keck School of Medicine, and Institute for Global Health, University of Southern California, USA, for editorial assistance and research support in preparing this chapter.
References 1. Intergovernmental Panel on Climate Change (IPCC). Contribution of Working Group I to the Fourth
Assessment Report of the Intergovernmental Panel on Climate Change, 2007: The Physical Science Basis . S. Solomon , D. Qin , M. Manning et al. Cambridge , Cambridge University Press ; 2007 .
2. Intergovernmental Panel on Climate Change (IPCC) . Contribution of Working Group II to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change, 2007: Impacts, Adaptation and Vulnerability . M. L. Parry , O. F. Canziani , J. P. Palutikof , P. J. van der Linden and C. E. Hanson . Cambridge , Cambridge University Press ; 2007 .
3. World Health Organization and World Meteorological Organization. Atlas of Health and Climate . Geneva , WHO Press ; 2012 .
4. Intergovernmental Panel on Climate Change (IPCC) . Intergovernmental Panel on Climate Change Assessment Reports . Available at: http://www.ipcc.ch/publications_and_data/publica-tions_and_data_reports.shtml [accessed 26 November 2012 ].
5. The Lancet . The Lancet Series on Health and Climate Change . Available at: http://www.thelancet.com/series/health- and-climate- change [accessed on 26 November 2012 ].
6. Costello , A. , M. Abbas , et al. Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission . Lancet 2009 ; 373 ( 9676 ): 1693 – 1733 .
7. Ezzati , M. , A. D. Lopez , et al. Selected major risk factors and global and regional burden of disease . Lancet 2002 ; 360 ( 9343 ): 1347 – 1360 .
8. Parenti , M. The Face of Imperialism . Boulder, CO , Paradigm Publishers ; 2011 . 9. Basu , R. and J. M. Samet . Relation between elevated ambient temperature and mortality: a review
of the epidemiologic evidence . Epidemiol Rev 2002 ; 24 ( 2 ): 190 – 202 . 10. Semenza , J. C. , C. H. Rubin , et al. Heat- related deaths during the July 1995 heatwave in Chicago .
New England Journal of Medicine 1996 ; 335 ( 2 ): 84 – 90 . 11. Vandentorren , S. , F. Suzan , et al. Mortality in 13 French cities during the August 2003 heat wave .
Am J Public Health 2004 ; 94 ( 9 ): 1518 – 1520 . 12. Kovats , R. S. , G. Jendritzky , et al. Heatwaves and human health . Climate Change and Adaptation
Strategies for Human Health . Darmstadt, Germany , Steinkopff-Verlag ; 2006 ; 63 – 97 . 13. Curriero , F. C. , K. S. Heiner , et al. Temperature and mortality in eleven cities of the eastern United
States . American Journal of Epidemiology 2002 ; 155 ( 1 ): 80 – 87 .
26356.indb 29426356.indb 294 16/12/13 7:34 PM16/12/13 7:34 PM

295
Climate change and health
14. McMichael , A. J. , P. Wilkinson , et al. International study of temperature, heat and urban mortality: the ‘ISOTHURM’ project . Int J Epidemiol 2008 ; 37 ( 5 ): 1121 – 1131 .
15. The Eurowinter Group . Cold exposure and winter mortality from ischaemic heart disease, cere-brovascular disease, respiratory disease, and all causes in warm and cold regions of Europe . Lancet 1997 ; 349 ( 9062 ): 1341 – 1346 .
16. Gasparrini , A. and B. Armstrong . The impact of heat waves on mortality . Epidemiology 2011 ; 22 ( 1 ): 68 – 73 .
17. Carson , C. , S. Hajat , et al. Declining vulnerability to temperature- related mortality in London over the 20th century . American Journal of Epidemiology 2006 ; 164 ( 1 ): 77 – 84 .
18. Davis , R. E. , P. C. Knappenberger , et al. Changing heat- related mortality in the United States . Environmental Health Perspectives 2003 ; 111 ( 14 ): 1712 – 1718 .
19. Barnett , A. G. Temperature and cardiovascular deaths in the US elderly: changes over time . Epidemiology 2007 ; 18 ( 3 ): 369 – 372 .
20. Buechley , R. W. , B. J. Van , et al. Heat island equals death island ? Environ Res 1972 ; 5 ( 1 ): 85 – 92 . 21. Zanobetti , A. , J. Schwartz , et al. The temporal pattern of mortality responses to air pollution: a
multicity assessment of mortality displacement . Epidemiology 2002 ; 13 ( 1 ): 87 – 93 . 22. Zeger , S. L. , F. Dominici , et al. Harvesting- resistant estimates of air pollution effects on mortality .
Epidemiology 1999 ; 10 ( 2 ): 171 – 175 . 23. Toulemon , L. and M. Barbieri . The mortality impact of the August 2003 heat wave in France:
investigating the ‘harvesting’ effect and other long- term consequences . Popul Stud (Camb.) 2008 ; 62 ( 1 ): 39 – 53 .
24. Hajat , S. , B. G. Armstrong , et al. Mortality displacement of heat- related deaths: a comparison of Delhi, São Paulo, and London . Epidemiology 2005 ; 16 ( 5 ): 613 – 620 .
25. Avila-Tang , E. , E. Matsui , et al. Epidemiology of asthma and allergic diseases . Allergy: Principles and Practices , 7th edn. N. F. Adkinson , W. W. Busse , B. S. Bochner , et al. Edinburgh, Mosby-Elsevier 2008.
26. Beggs , P. J. Impacts of climate change on aeroallergens: past and future . Clin Exp Allergy 2004 ; 34 ( 10 ): 1507 – 1513 .
27. Beggs , P. J. and H. J. Bambrick . Is the global rise of asthma an early impact of anthropogenic climate change ? Environmental Health Perspectives 2005 ; 113 ( 8 ): 915 – 919 .
28. Shea , K. M. , R. T. Truckner , et al. Climate change and allergic disease . J Allergy Clin Immunol 2008 ; 122 ( 3 ): 443 – 453 .
29. Nelson , K. E. , C. F. Masters Williams , et al. Infectious Disease Epidemiology: Theory and Practice . Sudbury, MA , Jones and Bartlett ; 2007 .
30. Rogers , D. J. and S. E. Randolph . Climate change and vector- borne diseases . Adv Parasitol 2006 ; 62 : 345 – 381 .
31. Haines , A. , R. S. Kovats , et al. Climate change and human health: impacts, vulnerability, and mitigation . Lancet 2006 ; 367 ( 9528 ): 2101 – 2109 .
32. Colwell , R. R . Global climate and infectious disease: the cholera paradigm . Science 1996 ; 274 ( 5295 ): 2025 – 2031 .
33. Lipp , E. K. , A. Huq , et al. Effects of global climate on infectious disease: the cholera model . Clin Microbiol Rev 2002 ; 15 ( 4 ): 757 – 770 .
34. Charron , D. , M. Thomas , et al. Vulnerability of waterborne diseases to climate change in Canada: a review . J Toxicol Environ Health 2004 ; A 67 ( 20 – 22 ): 1667 – 1677 .
35. Rodo , X. , M. Pascual , et al. ENSO and cholera: a nonstationary link related to climate change ? Proc Natl Acad Sci USA 2002 ; 99 ( 20 ): 12901 – 12906 .
36. Checkley , W. , L. D. Epstein , et al. Effect of El Nino and ambient temperature on hospital admis-sions for diarrhoeal diseases in Peruvian children . Lancet 2000 ; 355 ( 9202 ): 442 – 450 .
37. Cazelles , B. , M. Chavez , et al. Nonstationary infl uence of El Nino on the synchronous dengue epidemics in Thailand . PLoS Med 2005 ; 2 ( 4 ): e106.
38. Woodruff , R. E. , C. S. Guest , et al. Early warning of Ross River virus epidemics: combining surveillance data on climate and mosquitoes . Epidemiology 2006 ; 17 ( 5 ): 569 – 575 .
39. Lindgren , E. and R. Gustafson . Tick- borne encephalitis in Sweden and climate change . Lancet 2001 ; 358 ( 9275 ): 16 – 18 .
40. Ogden , N. H. , L. St.Onge , et al. Risk maps for range expansion of the Lyme disease vector, Ixodes scapularis, in Canada now and with climate change . International Journal of Health Geographics 2008 ; 7 ( 24 ).
26356.indb 29526356.indb 295 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
296
41. D’Souza , R. M. , G. Hall , et al. Climatic factors associated with hospitalizations for rotavirus diar-rhoea in children under 5 years of age . Epidemiol Infect 2008 ; 136 ( 1 ): 56 – 64 .
42. Gething , P. W. , D. L. Smith , et al. Climate change and the global malaria recession . Nature 2010 ; 465 ( 7296 ): 342 – 345 .
43. Dentener , F. , D. Stevenson , et al. The global atmospheric environment for the next generation . Environ Sci Technol 2006 ; 40 ( 11 ): 3586 – 3594 .
44. Wilson , S. R. , K. R. Solomon , et al. Changes in tropospheric composition and air quality due to stratospheric ozone depletion and climate change . Photochem Photobiol Sci 2007 ; 6 ( 3 ): 301 – 310 .
45. Davis , D. L. and Working Group on Public Health and Fossil-Fuel Combustion . Short- term improvements in public health from global- climate policies on fossil- fuel combustion: an interim report . Lancet 1997 ; 350 ( 9088 ): 1341 – 1349 .
46. US Environmental Protection Agency. Integrated Science Assessment of Ozone and Related Photochemical Oxidants (Third External Review Draft) . Washington, DC , US Environmental Protection Agency ; 2012 .
47. US Environmental Protection Agency . Integrated Science Assessment for Particulate Matter (fi nal report) . Washington, DC , US Environmental Protection Agency ; 2009 .
48. World Health Organization . Air Quality Guidelines: Global Update 2005–Particulate matter, ozone, nitrogen dioxide and sulfur dioxide . Copenhagen , World Health Organization ; 2006 .
49. Samet , J. M. , F. Dominici , et al. Fine particulate air pollution and mortality in 20 U.S. cities, 1987–1994 . N Engl J Med 2000 ; 343 ( 24 ): 1742 – 1749 .
50. Bell , M. L. , A. McDermott , et al. Ozone and short- term mortality in 95 US urban communities, 1987–2000 . Journal of the American Medical Association 2004 ; 292 ( 19 ): 2372 – 2378 .
51. Pope , C. A. , III and D. W. Dockery . Health effects of fi ne particulate air pollution: lines that connect . J Air Waste Manag Assoc 2006 ; 56 ( 6 ): 709 – 742 .
52. Brook , R. D. , S. Rajagopalan , et al. Particulate matter air pollution and cardiovascular disease: an update to the scientifi c statement from the American Heart Association; 2010 . Circulation 121 ( 21 ): 2331 – 2378 .
53. Dominici , F. , R. D. Peng , et al. Fine particulate air pollution and hospital admission for cardiovas-cular and respiratory diseases . Journal of the American Medical Association 2006 ; 295 ( 10 ): 1127 – 1134 .
54. Knowlton , K. , J. E. Rosenthal , et al. Assessing ozone- related health impacts under a changing climate . Environmental Health Perspectives 2004 ; 112 ( 15 ): 1557 – 1563 .
55. Bell , M. L. , F. Dominici , et al. Spatial and temporal variation in PM(2.5) chemical composition in the United States for health effects studies . Environmental Health Perspectives 2007 ; 115 ( 7 ): 989 – 995 .
56. Cifuentes , L. , V. H. Borja-Aburto , et al. Assessing the health benefi ts of urban air pollution reduc-tions associated with climate change mitigation (2000–2020): Santiago, São Paulo, Mexico City, and New York City . Environmental Health Perspectives 2001 ; 109 Suppl 3: 419 – 425 .
57. Hatzakis , A. , K. Katsouyanni , et al. Short- term effects of air pollution on mortality in Athens . Int J Epidemiol 1986 ; 15 ( 1 ): 73 – 81 .
58. Katsouyanni , K. , A. Pantazopoulou , et al. Evidence for interaction between air pollution and high temperature in the causation of excess mortality . Archives of Environmental Health 1993 ; 48 ( 4 ): 235 – 242 .
59. Filleul , L. , S. Cassadou , et al. The relation between temperature, ozone, and mortality in nine French cities during the heat wave of 2003 . Environmental Health Perspectives 2006 ; 114 ( 9 ): 1344 – 1347 .
60. Fischer , P. H. , B. Brunekreef , et al. Air pollution related deaths during the 2003 heat wave in the Netherlands . Atmospheric Environment 2004 ; 38 ( 8 ): 1083 – 1085 .
61. Knox , R. B. , C. Suphioglu , et al. Major grass pollen allergen Lol p 1 binds to diesel exhaust parti-cles: implications for asthma and air pollution . Clin Exp Allergy 1997 ; 27 : 246 – 251 .
62. Wyler , C. , C. Braun-Fahrlander , et al. Exposure to motor vehicle traffi c and allergic sensitization. The Swiss Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) Team . Epidemiology 2000 ; 11 ( 4 ): 450 – 456 .
63. Ghiani , A. , R. Aina , et al. Ragweed pollen collected along high- traffi c roads shows a higher aller-genicity than pollen sampled in vegetated areas . Allergy 2012 ; 67 ( 7 ): 887 – 894 .
64. Anenberg , S. C. , J. Schwartz , et al. Global air quality and health co- benefi ts of mitigating near- term climate change through methane and black carbon emission controls . Environmental Health Perspectives 2012 ; 120 ( 6 ): 831 – 839 .
26356.indb 29626356.indb 296 16/12/13 7:34 PM16/12/13 7:34 PM

297
Climate change and health
65. Wilkinson , P. , D. H. Campbell-Lendrum , et al. Monitoring the health effects of climate change . Climate Change and Human Health: Risks and Responses . A. J. McMichael , D. H. Campbell-Lendrum , C. F. Corvalan , et al. Geneva , World Health Organization ; 2003 : 204 – 219 .
66. Ebi , K. L. , T. J. Teisberg , et al. Heat watch/warning systems save lives – estimated costs and benefi ts for Philadelphia 1995–98 . Bulletin of the American Meteorological Society 2004 ; 85 ( 8 ): 1067 – 1073 .
67. Tan , J. G. , L. S. Kalkstein , et al. An operational heat/health warning system in Shanghai . International Journal of Biometeorology 2004 ; 48 ( 3 ): 157 – 162 .
68. Beggs , P. J. and C. M. Bennett . Climate change, aeroallergens, natural particulates, and human health in Australia: state of the science and policy . Asia Pac J Public Health 2011 ; 23 (2 Suppl): 46S – 53 .
69. UN-DESA-PD. World Population Prospects, 2002 . New York , United Nations Department of Economic and Social Affairs – Population Division ; 2002 .
70. Zeqiang , F. , C. Yunlong , et al. Research on the relationship of cultivated land change and food security in China . Journal of Natural Resources 2001 ; 16 : 313 – 319 .
71. Pulhin , J. M. , U. Chokkalingam , et al. Historical overview of forest rehabilitation in the Philippines . One Century of Forest Rehabilitation in the Philippines: Approaches, Outcomes and Lessons . U. Chokkalingam , A. P. Carandang , J. M. Pulhin , R. D. Lasco and R. J. J. Peras . Bogor, CIFOR-CFNR UPLB-FMB DENR; 2006 : 6 – 41 .
72. Ali , A . Climate change impacts and adaptation assessment in Bangladesh . Climate Research 1999 ; 12 ( 2 – 3 ): 109 – 116 .
73. Manton , M. J. , P. M. Della-Marta , et al. Trends in extreme daily rainfall and temperature in Southeast Asia and the South Pacifi c: 1961–1998 . International Journal of Climatology 2001 ; 21 ( 3 ): 269 – 284 .
74. Aldhous , P . Land remediation: Borneo is burning . Nature 2004 ; 432 ( 7014 ): 144 – 146 . 75. Trenberth , K. E. and T. J. Hoar . El Nino and climate change . Geophysical Research Letters 1997 ;
24 ( 23 ): 3057 – 3060 . 76. Cruz , R. V. O. , R. D. Lasco , et al. Climate change impact on water resources in Pantabangan
Watershed, Philippines. Assessments of Impacts and Adaptations to Climate Change (AIACC), Project No. AS 21 ; 2006 : 9 – 107 .
77. Tran , V. L. , D. C. Hoang , et al. Building of climate change scenario for Red River catchments for sustainable development and environmental protection . Preprints, Science Workshop on Hydrometeorological Change in Vietnam and Sustainable Development. Hanoi, Ministry of Natural Resource and Environment; 2005 : 70 – 82 .
78. Fan , D. D. and C. X. Li . Complexities of Chinese coast in response to climate change . Advances in Research on Climate Change 2005 ; 1 : 111 – 114 .
79. Lal , M. Tropical cyclones in a warmer world . Current Science 2001 ; 80 ( 9 ): 1103 – 1104 . 80. Christensen , J. L. , B. Hewitson , et al. Regional climate projections. Climate Change 2007: The
Scientifi c Basis. Contribution of Working Group I to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change . S. Solomon , D. Qin , M. Manning , et al. Cambridge , Cambridge University Press ; 2007 : 847 – 940 .
81. Ruosteenoja , K. , T. R. Carter , et al. Future climate in world regions: an intercomparison of model- based projections for the new IPCC emissions scenarios . Helsinki , Finnish Environment Institute ; 2003 .
82. Durack , P. J. , S. E. Wijffels , et al. Ocean salinities reveal strong global water cycle intensifi cation during 1950 to 2000 . Science 2012 ; 336 ( 6080 ): 455 – 458 .
83. Patz , J. A. , D. Campbell-Lendrum , et al. Impact of regional climate change on human health . Nature 2005 ; 438 ( 7066 ): 310 – 317 .
84. Wiley , L. F. and L. O. Gostin . The international response to climate change: an agenda for global health . JAMA 2009 ; 302 ( 11 ): 1218 – 1220 .
85. Bush , K. F. , G. Luber , et al. Impacts of climate change on public health in India: future research directions . Environmental Health Perspectives 2011 ; 119 ( 6 ): 765 – 770 .
86. Sattenspiel , L . Tropical environments, human activities, and the transmission of infectious diseases . Am J Phys Anthropol Suppl 2000 ; 31 : 3 – 31 .
87. Bhattacharya , S. , C. Sharma , et al. Climate change and malaria in India . Current Science 2006 ; 90 ( 3 ): 369 – 375 .
88. Dhiman , R. C. , S. Pahwa , et al. Climate change and malaria in India: interplay between tempera-ture and mosquitoes . Regional Health Forum 2008; 12 : 27 – 31 .
26356.indb 29726356.indb 297 16/12/13 7:34 PM16/12/13 7:34 PM

Jonathan M. Samet and Junfeng (Jim) Zhang
298
89. Ebi , K. L. and J. A. Paulson . Climate change and child health in the United States . Curr Probl Pediatr Adolesc Health Care 2010 ; 40 ( 1 ): 2 – 18 .
90. O’Neill , M. S. and K. L. Ebi . Temperature extremes and health: impacts of climate variability and change in the United States . J Occup Environ Med 2009 ; 51 ( 1 ): 13 – 25 .
91. Butler , C. D . A stormy future for population health in Southeast Asia ? Lancet 2011 ; 377 ( 9769 ): 885 – 886 .
92. Munslow , B. and T. O’Dempsey . Globalisation and climate change in Asia: the urban health impact . Third World Q 2010 ; 31 ( 8 ): 1339 – 1356 .
93. Pelling , M. The Vulnerability of Cities: Natural Disasters and Social Resilience . Sterling, VA, Earthscan Publications; 2003 .
94. McMichael , A. J. , D. Campbell-Lendrum , et al. Global Climate Change. Comparative Quantifi cation of Health Risks , Vol. 2 . Geneva , World Health Organization ; 2004 : 1543 – 1649 .
95. Chou , W. C. , J. L. Wu , et al. Modeling the impact of climate variability on diarrhea- associated diseases in Taiwan (1996–2007) . Sci Total Environ 2010 ; 409 ( 1 ): 43 – 51 .
96. Pascual , M. , M. J. Bouma , et al. Cholera and climate: revisiting the quantitative evidence . Microbes and Infection 2002 ; 4 ( 2 ): 237 – 245 .
97. Su , G. L . Correlation of climatic factors and dengue incidence in Metro Manila, Philippines . Ambio 2008 ; 37 ( 4 ): 292 – 294 .
98. Hii , Y. L. , J. Rocklov , et al. Climate variability and increase in intensity and magnitude of dengue incidence in Singapore . Glob Health Action 2 ; 2009 .
99. UN-ESCAP (United Nations Economic and Social Commission for Asia and the Pacifi c) . Achieving MDGs in Asia: a case for more aid ? New York , UN-ESCAP ; 2006 : 37.
100. Srinivasan , T. N . Poverty and under nutrition in South Asia . Food Policy 2000 ; 25 ( 3 ): 269 – 282 . 101. Adger , W. N . Social capital, collective action, and adaptation to climate change . Economic
Geography 2003 ; 79 ( 4 ): 387 – 404 . 102. Beg , N. , J. C. Morlot , et al. Linkages between climate change and sustainable development .
Climate Policy 2002 ; 2 ( 2 – 3 ): 129 – 144 .
26356.indb 29826356.indb 298 16/12/13 7:34 PM16/12/13 7:34 PM

Copyright 2014 American Medical Association. All rights reserved.
Climate ChangeChallenges and Opportunities for Global HealthJonathan A. Patz, MD, MPH; Howard Frumkin, MD, DrPH; Tracey Holloway, PhD;Daniel J. Vimont, PhD; Andrew Haines, MBBS, MD
IMPORTANCE Health is inextricably linked to climate change. It is important for clinicians tounderstand this relationship in order to discuss associated health risks with their patients andto inform public policy.
OBJECTIVES To provide new US-based temperature projections from downscaled climatemodeling and to review recent studies on health risks related to climate change and thecobenefits of efforts to mitigate greenhouse gas emissions.
DATA SOURCES, STUDY SELECTION, AND DATA SYNTHESIS We searched PubMed from 2009 to2014 for articles related to climate change and health, focused on governmental reports,predictive models, and empirical epidemiological studies. Of the more than 250 abstractsreviewed, 56 articles were selected. In addition, we analyzed climate data averaged over 13climate models and based future projections on downscaled probability distributions of thedaily maximum temperature for 2046-2065. We also compared maximum daily 8-houraverage with air temperature data taken from the National Oceanic and AtmosphericAdministration National Climate Data Center.
RESULTS By 2050, many US cities may experience more frequent extreme heat days. Forexample, New York and Milwaukee may have 3 times their current average number of dayshotter than 32°C (90°F). The adverse health aspects related to climate change may includeheat-related disorders, such as heat stress and economic consequences of reduced workcapacity; and respiratory disorders, including those exacerbated by fine particulatepollutants, such as asthma and allergic disorders; infectious diseases, including vectorbornediseases and water-borne diseases, such as childhood gastrointestinal diseases; foodinsecurity, including reduced crop yields and an increase in plant diseases; and mental healthdisorders, such as posttraumatic stress disorder and depression, that are associated withnatural disasters. Substantial health and economic cobenefits could be associated withreductions in fossil fuel combustion. For example, the cost of greenhouse gas emissionpolicies may yield net economic benefit, with health benefits from air quality improvementspotentially offsetting the cost of US carbon policies.
CONCLUSIONS AND RELEVANCE Evidence over the past 20 years indicates that climate changecan be associated with adverse health outcomes. Health care professionals have animportant role in understanding and communicating the related potential health concernsand the cobenefits from reducing greenhouse gas emissions.
JAMA. doi:10.1001/jama.2014.13186Published online September 22, 2014.
Editorial
Author Affiliations: Authoraffiliations are listed at the end of thisarticle.
Corresponding Author: Jonathan A.Patz, MD, MPH, Global HealthInstitute, University of Wisconsin,1710 University Ave, Madison, WI53726 ([email protected]).
Clinical Review & Education
Special Communication
E1
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
C urrent science highlights serious worldwide adversehealth outcomes related to climate change. Althoughuncertainty remains regarding the extent of climate
change, this uncertainty is diminishing.1 Consensus is substantialthat human behavior contributes to climate change: 97% of cli-matologists maintain that climate change is caused by humanactivities, particularly fossil fuel combustion and tropicaldeforestation.2-4 Questions remain concerning risks, vulnerabili-ties, and priorities for policies to promote adaptation (reducingadverse outcomes) and mitigation (reducing heat-inducingemissions).
About half of anthropogenic greenhouse gas emissions be-tween 1750 and 2010 occurred since 1970. The increase in green-house gas emissions has been greatest in the last decade (2.2% peryear) compared with 1.3% per year between 1970 and 2000.5 Emis-sions continue to increase; 2011 emissions exceeded those in 2005by 43%.1 Carbon dioxide from fossil fuels and industrial processesaccounted for approximately 78% of the total increase from 1970-2010. Economic and population growth contribute most to in-creases in emissions globally and have outpaced improvements inenergy efficiency. The trend toward decarbonization (cleaner fu-els) of the world’s energy since the 1970s has been reversed by in-creased coal combustion since 2000.5
Climatologists calculate that to avoid heating the earth morethan 2°C from preindustrial levels, anthropogenic carbon dioxideemissions must be significantly reduced. Some of the projected earthsystem changes—which include changes in temperature and pre-cipitation, the rise in sea levels, and acidification of the ocean—arewidely accepted as the consequences of increasing carbon dioxideconcentrations in the earth’s atmosphere (Box 1).1 Although evi-dence on global trends and the extent that climate change is re-lated to human behavior are substantial, necessary actions on emis-sion reductions have lagged.
Framing Climate Change and HealthClimate change is happening: the relationship of heat-waves,floods, and droughts along with adverse health outcomes isevident.7,8 Two broad approaches are needed to protect publichealth: mitigation, or major reductions in carbon emissions, corre-sponding to primary prevention; and adaptation, or steps toanticipate and reduce threats, corresponding to secondary pre-vention (or public health preparedness).
A wide range of solutions is available to mitigate the problemof climate change. Many of them would improve health immedi-ately. From decreasing rates of chronic diseases to reducingmotor vehicle crashes, there are many good solutions for climatedisasters and health risks. Reducing greenhouse gas, deployingsustainable energy technologies, shifting transportation patterns,and improving building design—many of which yield multiplebenefits—are feasible, cost-effective, and attractive to multipleparties. Health care professionals are uniquely positioned todevelop policies that simultaneously serve both planet andpeople.9
Climate change, as a global disturbance, can exacerbate manyenvironmental health risks familiar to clinicians and public healthprofessionals.10,11 The nature of risks and population vulnerability will
vary by region; indirect consequences such as ecosystem collapsemay overshadow more direct health effects, yet are more difficultto estimate.
Recent reviews on health effects of climate change havebeen published by the Intergovernmental Panel on ClimateChange7 and the US National Climate Assessment.8 Our goals inthis Special Communication are to provide new US-based tem-perature projections from downscaled climate modeling and toreview recent studies on climate change health risks and thecobenefits of mitigating greenhouse gas emissions. A brief list ofkey findings is summarized in Box 2.
MethodsWe reviewed the literature of international studies on climatechange and health and disease risk or the cobenefits of reducingfossil fuel emissions by searching the PubMed database andGoogle Scholar from January 2009 to April 2014. Priority forinclusion was based on peer-reviewed articles published withinthe past 3 years that focused on climate and heat-related disor-ders, reduced work capacity, respiratory disorders, infectious dis-eases, food insecurity, mental health disorders, climate changecommunications, and health cobenefits. We identified more than250 abstracts, and 56 articles are the basis of this review compo-nent of this article. In addition, we included our original analysis ofUS-based risks from heat waves and ozone air pollution (Figure 1and Figure 2). Extreme heat data were obtained from the Univer-sity of Wisconsin Probabilistic Downscaled Climate Data12 accord-ing to methods described in Kirchmeier et al.13 (Downscaling isthe process of providing locally specific information based onlarge-scale data. We took large-scale climate data from the globalclimate models and made it regionally specific using a statistical
Box 1. Overall Trends in Temperature, Precipitation, Sea Level,and Ocean Acidification
TemperatureOverall temperatures and frequency of more than 38°C (>100°F)weather are projected to increase by 2100. Increase of global meansurface temperatures for 2081-2100 are projected to likely be in theranges of 0.3°C to 4.8°C relative to 1986-2005.
PrecipitationIn the United States, precipitation in the heaviest 1% of rains in-creased 20% in the past century, while total rainfall increased 7%.In dry regions mean precipitation will decrease, while El Nino–related precipitation variability will likely intensify.6
Sea Level RiseGlobal mean sea level has risen approximately 20 cm in 100 years,far more than in the 2 previous millennia, associated with thermal ex-pansion and melting small glaciers. Although sea level is likely to risebetween 26 cm and 98 cm by 2100, “tail risk” projections give moreextreme estimates (>200 cm) due to catastrophic melting events.
Ocean AcidificationOceans have absorbed about 30% of anthropogenic carbon dioxidesurface pH has become 0.1 more acidic since the beginning of the in-dustrial era.
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E2 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
method.) Data were averaged over 13 climate models, which arerequired by the World Climate Research Programme's coupledmodel intercomparison project phase 3 multimodel data set toaccommodate the intercomparison nature of the program.14
Present-day estimates of the number of hot days are based ondownscaled probability distributions—used for future climatemodeling to establish uncertainty ranges—of daily maximum tem-perature for the years 1960 through 1999 from the Climate of the20th Century simulations. Future projections are based on down-scaled probability distributions of daily maximum temperature forthe years 2046-2065 from the IPCC A1B emissions scenario thatassumes “business as usual” or rapid economic growth and aglobal average temperature increase of 2.8°C.12-14
For ozone and temperature analysis, we used ground-levelozone measurements from the US Environmental ProtectionAgency Air Quality System database. The maximum daily 8-houraverage for each city—based on the number of monitoring siteswithin the city in operation between 1980 and 2002 during theMay through October period, when ozone concentrations arehighest—were calculated. If any monitor was higher than the75 ppb threshold, selected as the current health–protectiveozone limit from the EPA National Ambient Air Quality Standards,then the day was counted in the yearly total. Air temperature datawere taken from the US National Oceanic Atmospheric Adminis-tration (NOAA) National Climate Data Center. In an analysisapproach modeled after the Connecticut Department of Energyand Environmental Protection,15 annual values were comparedand demonstrated that relationships existed between the num-ber of high-ozone days each year and the number of hot-temperature days each year.
Heat-Related DisordersThe most direct effect of a warming planet is heat stress and asso-ciated disorders. Heat-related deaths are routinely attributed tocauses such as cardiac arrest without citing temperature as the un-derlying factor.16 Thus, the actual death toll attributable to heat isgreater than certified on death certificates. Annual certified heat-related deaths averaging 658 in the United States between 1999 and2009, represent more fatalities than all other weather eventscombined.17,18 More accurate risk estimates have compared ob-served vs expected mortality during heat events; for example,70 000 excess deaths were estimated for the 2003 European heatwave and 15 000 for the 2010 Russian heat wave.19,20
Although air conditioning has reduced heat-related deaths andillness in the United States, climatic and demographic trends sug-gest that risks may persist.21,22 Estimates from 7 climate models forthe years 2081-2100 project that more than 2000 excess heatwave–related deaths per year may occur in Chicago, Illinois.23 Morefrequent and persistent heat waves are forecast, especially in thehigh latitudes of North America and Europe.24,25 Mega heat waves(as occurred in Europe and Russia) are projected to increase in fre-quency by 5- to 10-fold within the next 40 years.26 Figure 1 showsprojected days with temperatures exceeding 32°C (90°F) per yearby midcentury for Milwaukee, Wisconsin, New York, New York, andAtlanta, Georgia, and days of temperatures exceeding 38°C (100°F)for Dallas, Texas. Data were averaged across 13 climate models forthis analysis. Frequency of hot days markedly increases across allcities; for example, New York City is projected to experience
3 times the current average number of 32°C (90°F) days by themidcentury (from 13 to 39 days).
High-risk groups include elderly persons, those living in pov-erty or social isolation, and those with underlying mental illness.27,28
Depression may be aggravated; suicide has long been observed tovary with weather.29-32 Dementia is a risk for hospitalization anddeath during heat waves.33,34 Psychotic illnesses such asschizophrenia,35-43 as well as substance abuse,44 also are associ-ated with an increased risk of death during extremely hot weather.Increased frequency of kidney stones (likely precipitated by dehy-dration) also occurs during heat waves.45
Cities with investments in early warning and response pro-grams have seen some success. For example, after Milwaukeeimplemented an extreme heat conditions plan following 91 fatali-ties during the 1995 heat wave, a subsequent heat wave in 1999resulted in only 10 deaths, or 49% less than expected.46 It is esti-mated that more proactive health adaptations in cities, such asenhanced tree canopies and more reflective, less heat-absorbingsurfaces, could reduce heat-related mortality by 40% to 99% inAtlanta, Philadelphia, Pennsylvania, and Phoenix, Arizona.47
Might fewer cold-related deaths balance mortality from heatwaves? This is a topic of active research and current uncertainty, withresults likely differing for climate zone and infrastructure character-istics. Although relative increases in heat-related deaths may ex-ceed relative decreases in cold-related deaths, this may not applyin absolute terms because the balance may depend on location,population structure (proportion of older residents), and amount ofwarming,48,49 and the Intergovernmental Panel on Climate Changeexpressed low confidence that modest reductions in cold-relatedmortality would occur.7 Reasons for this include the observation that
Box 2. Key Messages
Health Effects of Climate ChangeHeat-related disorders, including heat stress and economic conse-quences of reduced work capacity
Respiratory disorders, including those exacerbated by fine particu-late pollutants, such as asthma and allergic diseases
Infectious diseases, including vectorborne diseases, such as Lyme dis-ease, and water-borne diseases, such as childhood gastrointestinaldiseases
Food production, including reduced crop yields and an increase inplant diseases
Mental health disorders such as posttraumatic stress disorder and de-pression that are associated with natural disasters
Approaches to Climate Change AdaptationInfrastructure improvements, including more green spaces, build-ing replacement, and white roofs
Health Cobenefits From Mitigating Climate ChangeEconomic advantages of reducing fossil fuel combustion and improv-ing air quality, including a reduction in chronic diseases and their as-sociated health care costs, and economic opportunities associatedwith development of alternative forms of energy
Infrastructure improvements that reduce greenhouse emissions couldalso lead to increased physical activity that would be associated witha reduction in various chronic diseases
Climate Change and Global Health Challenges Special Communication Clinical Review & Education
jama.com JAMA Published online September 22, 2014 E3
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
many deaths related to cold temperatures do not occur during cold-est times and that there is a lag between exposure to cold tempera-tures and increased risk of death typically much longer than 1 or 2days.50
Occupational HealthOutdoor workers are affected by heat, so economic consequenceson work capacity can be substantial.51 Modeling by Kjellstromet al52 projected that by the 2050s workdays lost due to heatcould reach 15% to 18% in South-East Asia, West and CentralAfrica, and Central America.
Using industrial and military guidelines, Dunne et al53 esti-mated that ambient heat stress has reduced global population-weighted labor capacity by 10% in summer’s peak over the past fewdecades. Projected reduction may double by 2050 and may be evenlarger in the latter half of the 21st century. Locations already with hotambient conditions are particularly susceptible to heat stress lossesin labor capacity, a potential liability for fragile economies.
Respiratory DisordersThe majority of research on the climate change–pollution connec-tions has focused on ground-level ozone and particulate matter, 54
both of which vary with the weather.55 Even in the face of improv-ing emissions, a climate penalty or temperature-related worseningof pollution may be anticipated.56
We compared ground-level ozone measurements from the USEPA Air Quality System with temperature data from NOAA’s NationalClimate Data Center. The analysis displayed in Figure 2 suggests adirect relationship between temperature and ozone. The summerswith the highest number of hot days (>32°C) in Chicago, for ex-ample, strongly correlated (R2=0.57) with summers with the highestnumber of days when ozone levels exceeded 75 parts per billion byvolume (ppbv), the US threshold level for ozone.
Models demonstrate increased ground-level ozone concentra-tions by the midcentury across the eastern United States,57-60 sug-gesting that further reductions in ozone precursors would be neededto offset the effect of climate change on ground-level ozone.
Fine particulate matter less than 2.5 μm is a pollutant posinghealth risks and is influenced by weather. Fine particulate matteris formed as part of diesel exhaust, forest fire smoke, windblowndust, and chemical products of gaseous release from powerplants, vehicles, and industry. Forty-three million people in theUnited States inhabit areas that exceed EPA health-based stan-dards for fine particulate matter,61 and nearly a third of the earth’s
Figure 1. Cumulative Distribution of Days in June Through August of Daytime Maximum Temperatures Exceeding a Given Threshold, 1960-1999 and2046-2065
100
80
60
40
20
060 11070 75 80 85 90 95 105100
No
. o
f D
ays
Exc
eed
ing
Th
resh
old
Temperature Threshold, °F
65
Dallas, Texas
100
80
60
40
20
060 11070 75 80 85 90 95 105100
No
. o
f D
ays
Exc
eed
ing
Th
resh
old
Temperature Threshold, °F
65
Atlanta, Georgia
100
80
60
40
20
060 11070 75 80 85 90 95 105100
No
. o
f D
ays
Exc
eed
ing
Th
resh
old
Temperature Threshold, °F
65
New York, New York
100
80
60
40
20
060 11070 75 80 85 90 95 105100
No
. o
f D
ays
Exc
eed
ing
Th
resh
old
Temperature Threshold, °F
65
1960-1999Days exceeding threshold: 9
1960-1999Days exceeding threshold: 15
1960-1999Days exceeding threshold: 30
1960-1999Days exceeding threshold: 13
2046-2065Days exceeding threshold: 25
2046-2065Days exceeding threshold: 35
2046-2065Days exceeding threshold: 57
2046-2065Days exceeding threshold: 39
Milwaukee, Wisconsin
The dotted line indicates the temperature thresholds for each city: 90°F (32°C)in Milwaukee, Atlanta, and New York and 100° (38°C) in Dallas. The estimatespredict temperatures based on “business as usual” emissions scenario. The
curves represent the average of an analysis conducted by the University ofWisconsin, Center for Climatic Research of more than 13 models.
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E4 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
population inhabit areas that fail World Health Organizationstandards.62 Fine particulate matter exposure is highest in low-income countries, where regulations to limit particulate emissionsare lacking or unenforced.
In many regions, future temperatures most likely will increasewildfire risk by causing increased drought.63 A study on worldwidemortality estimated that 339 000 premature deaths per year (range,260 000-600 000) were attributable to pollution from forest fires,especially particulates.64
In some cases, health adaptations to one hazard, eg, air condi-tioning for heat stress, may exacerbate another risk, such as air pol-lution. For example, electricity demands during more frequent heatwaves, and associated power plant emissions may compound di-rect temperature effects on atmospheric chemistry.54,65
Allergies and PollenClimate change may exacerbate allergies by enhancing pollen pro-duction and other allergens from nature. Fifty-five percent of the USpopulation tests positive for allergens,66 and more than 34 millionhave asthma.67 Climate shifts alter abundance and seasonality ofaeroallergens, eg, earlier flowering of oaks over the past 50 years,68
and increased pollen production by ragweed (Ambrosia) with warmertemperatures and higher ambient carbon dioxide.69,70 Data alonga 2560-km (1600-mile) north-south sampling of monitoring sta-tions through mid–North America indicate that the ragweed sea-son has been lengthening by as much as 13 to 27 days north of the44th parallel since 1995.71
Infectious DiseasesVectorborne DiseasesVectorborne diseases are sensitive to climate through multiplemechanisms: first, through geographic shifts of vectors or reser-voirs; second, through changes in rates of development, survival,and reproduction of vectors, reservoirs, and pathogens; and third,through increased biting by vectors and prevalence of infection inreservoirs or vectors.72,73 All affect transmission to humans,74-77 suchthat exposure to vectorborne disease will likely worsen in a warmerworld.
Demographic trends influence the risk of vectorborne dis-eases. Warmer ambient temperatures in both the Ethiopian andColombian highlands are projected to increase malaria in denselypopulated locations.78 Similar results occur in North America:warmer temperatures increase the development rate of the Lymedisease vector, Ixodes scapularis79; and climate models predictexpansion of Lyme disease into Canada.80 Modeling shows north-ern and central Europe at risk for the Chikungunya virus due towarmer, wetter weather.81 Policy responses can yield major healthbenefits, and the Intergovernmental Panel on Climate Change7
found overall malaria declining in East Africa due to improved con-trol programs, such as use of bed nets.
Waterborne DiseasesWaterborne diseases are expected to worsen, especially due toheavier precipitation events (>90% ile) projected to occur with cli-mate changes.74 Childhood gastrointestinal illness in the UnitedStates82 and India83 have been linked to heavy rainfall. In the Neth-erlands, a 33% increase in gastrointestinal illness was associatedwith sewage overflow following heavy rain. Flood waters contained
Campylobacter, Giardia, Cryptosporidium, noroviruses, andenteroviruses.84 In the United States, by 2100, Great Lakes climatemodeling projects a 50% to 120% increase in overflow events.85 Ameta-analysis of 87 waterborne communicable disease outbreaksoccurring worldwide from 1910 to 2010 showed that communi-cable disease is associated with heavy rainfall and flooding; Vibrioand Leptospira were most often cited.86
Figure 2. Relationship Between Days of High Temperaturesand Ozone Levels
01980 1984 1988 1992 1996 2000 2004 2008 2012
60
50
No
. o
f E
xcee
dan
ce D
ays
Year
Chicago, Illinois
40
30
20
10
01980 1984 1988 1992 1996 2000 2004 2008 2012
45
40
No
. o
f E
xcee
dan
ce D
ays
Year
Madison, Wisconsin
35
30
25
20
15
5
10
01980 1984 1988 1992 1996 2000 2004 2008 2012
60
50
No
. o
f E
xcee
dan
ce D
ays
Year
Milwaukee, Wisconsin
40
30
20
10
Days >75 ppbv ozone
Days ≥90° F
Number of days in Chicago, Madison, and Milwaukee for each year (1980-2012)in which temperature exceeded 32°C (90° F) and ozone exceeded 75 ppbv(parts per billion by volume). The y-axis scale shown in blue indicates range of 0through 45 days.
Climate Change and Global Health Challenges Special Communication Clinical Review & Education
jama.com JAMA Published online September 22, 2014 E5
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
Waterborne diseases can be reduced with improved manage-ment infrastructure to better handle heavy rainfalls and through ur-ban design by reducing impermeable surface areas. Improved moni-toring can also help reduce many climate-sensitive infectious diseaserisks. The National ArboNET surveillance system tracks 8 mosquito-borne diseases, eg, West Nile virus in humans, birds, mosquitoes,and other animals.87
Food SecurityUndernutrition is one of the most important health concerns re-lated to climate change. Three mechanisms affect food security: re-duced crop yields, increased losses, and decreased nutrient con-tent. On average, climate change is projected to reduce global foodproduction by 2% per decade, even as demand increases by 14%.88
More than 800 million people currently experience chronichunger,89 concentrated where productivity could likely be mostaffected.90 Climate change is projected to reduce wheat, maize, sor-ghum, and millet yields by approximately 8% across Africa and SouthAsia by 2050.88 One estimate suggests that globally, by 2050 ap-proximately 25 million more children might be undernourishedthrough climate change,91 and rates of growth stunting92,93 couldincrease substantially. Climate change–related rapid increases in foodprices, especially for staples such as corn and rice, could more thandouble by midcentury, placing impoverished populations at fur-ther risk.94
Plant diseases caused by fungi, bacteria, viruses, and oomyce-tes, already responsible for a 16% crop loss, may substantially in-crease with climate change.95 Moreover, the nutrient value of somecrops may diminish. Whereas carbon dioxide fertilization can en-hance growth, protein content can decline in wheat and rice, as caniron and zinc content in crops such as rice, soybeans, wheat, andpeas.96
Preventive measures range from drought or salt-resistant cropsto improved technology such as drip irrigation and hoop houses (in-expensive greenhouses). Other potential adaptation strategies in-clude changing planting dates, increasing crop diversity, and com-bining different strategies.
Mental HealthDepression, anxiety, and related disorders cause major morbidityworldwide.97,98 Besides vulnerability to adverse effects from heatexposure, climate change may threaten mental health in otherways.99-102
Climate-Related DisastersPosttraumatic stress disorder, anxiety, and depression are com-mon following disasters, sometimes a major part of the healthburden.103-107 Several months after Hurricane Katrina, 49.1% ofthose surveyed in New Orleans and 26.4% in other affected areasdeveloped a Diagnostic and Statistical Manual of Mental Disorders(Fourth Edition) (DSM-IV) anxiety mood disorder; 1 in 6 had post-traumatic stress disorder (PTSD) (with considerable overlapbetween the 2 diagnoses).108 Similar outcomes have been docu-mented following other disasters likely to increase with climatechange, including floods,109,110 dam collapses,111 heat waves,34,112
and wildfires.113 Psychopathology typically declines over time fol-lowing disasters,114 but may persist for years,115 especially amongvulnerable groups.116 Risk factors include little social capital
(networks of relationships that build trust within a community)or support,112 physical injury,103 property loss,103 witnessingothers with illness or injury while they were in pain or were dyingduring the disaster, loss of family, displacement, and history ofpsychiatric illness.98,113 Children may be at special risk.114 Thesefindings suggest a variety of protective strategies,115 includingstrengthening social support networks,116 providing postdisastermental health services, and prompt insurance compensationfor loss.
Slow-moving disasters may also threaten mental health.Research in Australia during the recent decade-long droughtrevealed increases in anxiety, depression, and possibly suicidalityamong rural populations.34,117,118 Strategies to reduce this burdenincluded raising mental health literacy, building community resil-ience through social events, and disseminating drought-relatedinformation.107
Climate-Related DisplacementDisplacement may mean degradation of a familiar environment; theresulting distress has been documented among Alaskan natives invillages endangered by climate-related changes.117 More typically,displacement means relocation forced by disaster or resourcescarcity,118 creating considerable mental health effects.119 An im-portant protective strategy is keeping families, even entire commu-nities, united.120
Anxiety and Despair Related to Climate ChangeResearchers have noted that climate change may engenderdespair, anxiety, and hopelessness, although few empiricaldata are available.100,101 Although social circumstances andpolitical views help determine cognitive and emotional process-ing of climate change information, there is an essential role forcommunication—presenting the problem and solutions in waysthat engender engagement rather than despair.121 Climate adap-tation and mitigation can therefore be considered, in part, a psy-chological task,122 one that includes effective communication.
Other Climate Health and Societal ImpactsVariation in precipitation, including increased severe rainfallevents and increased frequency of droughts could create majorrisks or could have major consequences. Too little rainfall creates“dust bowl” conditions and worsens particulate matter exposure.Too much rainfall can overwhelm sewage systems, leading toincreased waterborne diseases. Too much or too little can destroycrops.123
From 2003 to 2012, an average of 115 000 people died each yeardue to natural disasters.124 For every person killed by natural disas-ter, an estimated 1000 people are affected physically, mentally, ormaterially, through loss of property or livelihood.125 Floods are themost common severe weather event worldwide, and the fre-quency of river floods has been increasing.126 Conservative esti-mates report 2.8 billion people were affected by floods between1980 and 2009, with 500 000 cumulative deaths estimated, evenas death rates declined.127
Uncertainty exists over whether hurricane frequency might in-crease, but evidence suggests that extreme hurricanes (categories
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E6 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
4 and 5) may occur more frequently.1,128-130 Sea level rise will exac-erbate storm surges, worsen coastal erosion, and inundate low-lying areas. Salinization of aquifers most likely will augment chal-lenges to coastal settlements.
Health Effects of Social Disruption and Civil ConflictIn developing regions, climate-related disasters may trigger broaddislocations, often to places ill prepared for refugees who areoverwhelmed by undernutrition and stress. Displaced groupscommonly experience violence, sexual abuse, and mentalillness.131
Increasing, but still inconclusive, evidence links climatechange and violence,132 from self-inflicted and interpersonal harmto armed conflict. A 2013 meta-analysis found that each standarddeviation of increased rainfall or warmer temperatures increaseslikelihood of intergroup conflict by 14% on average.133 The Cen-ters for Naval Analyses Military Advisory Board, comprisingretired generals, warned that climate change could catalyze insta-bility and conflict.134
Communicating Climate Change and HealthPublic Belief in Climate ChangeViews on climate change range widely. Two decades of polling sug-gest that about two-thirds of US residents believe that climatechange is occurring; of these about two-thirds (or about 40% of thetotal) believe humans cause it. About half (or about 1 in 3 overall)believe it will pose a serious threat in their lifetimes.135-137 Com-pared with other wealthy nations,138,139 US residents generally seethe issue as remote in time and space (eg, affecting the next gen-eration and in developing countries) and of low priority, well be-hind such concerns as jobs, health care, and even other environ-mental issues.140
Researchers have segmented the US population along a spec-trum ranging from “alarmed” ( ≈ 16%) to “dismissive” ( ≈ 10%), ac-cording to climate change belief, concern, and motivation.141 Manyfactors shape views of climate change: economic trends,142 cul-tural norms,143 beliefs of family and friends,144 and values and po-litical ideology,145-147 often exercised through cognitive shortcutscalled heuristics that bypass evidence.148,149 Media coveragematters.150-156 Deliberate, well-funded attempts to deceive the pub-lic and sow confusion have succeeded.152,157-160 Despite robust sci-entific consensus on climate change,2,3,161 there is widespread per-ception that scientists disagree, which in turn fuels public disbelief.162
In addition, many people are unduly influenced by personal expe-rience, such as short-term weather perturbations. A heat wave maystrengthen belief in climate change, a snowy winter may under-mine it. Interpretation of weather rests heavily on prior beliefs andsocial cues.163-167
Communicating Climate Change and HealthEffective communication may shift knowledge, attitudes, and be-havior toward reducing the risks of climate change.168,169 Researchindicates several principles of effective climate communication thatclosely resemble those used in health.170,171 Themes include 2-waycommunication,149 gearing messages to the audience,172,173 limit-ing use of fear-based messages,174,175 issuing simple lucid mes-
sages repeated often from trusted sources,169 and making health-promoting choices easy and appealing.168
Health may be a compelling frame for communication about cli-mate change,176,177 reflecting views that change threatens health.178
Although further research is needed to define the role of health inclimate communication, practical communication resources are be-coming available,179 implying an important role for health careprofessionals.180
Approach to Climate Change AdaptationPersistent elevated atmospheric carbon dioxide will continue towarm the planet for decades even after implementation of mitiga-tion strategies. A full range of adaptation options is reviewedelsewhere.181-183 The following section discusses health implica-tions of some alternatives.
In 2008, for the first time, more people worldwide resided inurban than in rural environments.184 Increasing urbanization, espe-cially in low- and middle-income countries, presents opportunitiesto redesign habitats that promote public health, climate resiliency,and sustainability.
Essential infrastructure improvement could help adaptation toclimate change. For example, vegetation, building placement, whiteroofs, and architectural design can reduce the urban heat island ef-fect and therefore electricity demands for air conditioning. A re-cent study found that waste heat from air conditioning can warmoutdoor air more than 1°C, so limiting the need for air conditioninguse has a direct influence on urban heat islands.185
In most US cities, infrastructure for potable water and waste-water management is more than 50 years old; in some cases morethan a century. These systems, which serve 80% of the popula-tion, received an average near-failing grade of D+ on the 2013 Infra-structure Report Card of the American Society of Civil Engineers.186
Under projected increases in extreme weather, cities face a daunt-ing but timely opportunity to establish healthier, environmentallysustainable infrastructure.
Optimal adaptation strategies achieve multiple objectives.Green spaces—forests and parks—not only reduce heat islands;they also are linked to stress reduction,187-189 neighborhood socialcohesion,190 and reductions in crime and violence.191-193 A recentcross-sectional study of 2427 Wisconsin individuals found thatneighborhood green space and tree canopy percentage hadstrong inverse correlation with objective measures of depression,anxiety, and stress.194 The magnitude of this influence was com-parable with other contributors to depression, including socio-economic status and health insurance. Tree species compositionof the canopy presents another strategy; red maples, forexample, emit 70% fewer biogenic volatile organic compoundsthan do oaks, an opportunity to develop green space while mini-mizing ozone-forming compounds.195
Multiple benefits and cost savings may be gained through an eco-logical approach rather than by engineering single solutions.196 Assea level rises, seawalls have frequently served to stabilize shore-lines. But in Vietnam, planting mangroves for storm surge protec-tion incurs one-seventh the cost of building and maintaining sea-wallsordikesforthispurpose.197 Thiscoastalecosystemalsopreserveswetlands and marine food chains that support local fisheries.
Climate Change and Global Health Challenges Special Communication Clinical Review & Education
jama.com JAMA Published online September 22, 2014 E7
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
Preparing for Tail Risks
The uncertainty regarding effects of climate change can be ex-pressed in probability distributions. Tails of such distributions con-tain catastrophes—rare high-consequence events.198,199 Econo-mists and risk managers have focused on tail risk in climate change,asking how much society should spend to reduce these risks.200 Thisquestion is familiar to homeowners who insure against the small butdevastating possibility of a house fire and to physicians who treatpatients when withholding treatment entails even a small risk of cata-strophic outcome. Although some issues in public health decisionmaking require a trade-off among risk management options, manyexisting climate mitigation measures have no adverse conse-quences to health or the economy (eg, energy conservation, crop-land management, waste recycling).201 This thinking asserts that thepossibility of catastrophic outcomes not only justifies but compelspreventive action now.
Health Cobenefits From Mitigating Climate ChangeThere are many social, economic, and political barriers to realizingreductions in global greenhouse gas emissions. These include diffi-culties of behavior changes; costs of implementing energy and in-dustrial policies; opposition of vested interests, especially fossil fuelindustries; and challenges of coordinating a worldwide solutionamong countries at different economic stages.
Thus, it is essential to design carbon reduction policies with an-cillary benefits, often referred to as cobenefits, such as improved airquality or fitness-promoting urban design. These may be viewed asmore near-term and politically attractive strategies than climate miti-gation alone.202 Articulating multidimensional aspects of carbon re-duction strategies also helps avoid poorly designed policies that mayhave adverse effects on public health. For example, biofuels thatcompete with crop production may contribute to increased foodcosts and insecurity.203
Economic Advantages of Reducing Fossil Fuel CombustionConcern remains over the cost of policies to shift to renewable en-ergy and reconfigure transportation systems. However, a 2014 US-based full life-cycle analysis—consideration of full supply chains forenergy, eg, from processes associated with production to transpor-tation—shows the contrary. For example, monetized human healthbenefits stemming from air quality improvements are estimated topotentially offset the cost of US carbon policies by 26% to 1050%.204
Global average monetized health cobenefits from avoided mor-tality are projected to range from $50 to $380 per ton of carbon di-oxide removed and exceed abatement costs in 2030 and 2050.205
Estimated cobenefits are $30 to $600 for the United States andWestern Europe, $70 to $840 for China, and $20 to $400 for In-dia. For East Asia, air quality–related health benefits are projectedto be 10 to 70 times the abatement costs in 2030.205 These largebenefits are not surprising, given EPA estimates of a return of $30for every dollar spent on reducing air pollution through the CleanAir Act.206
Further economic benefits likely will accrue from enhancedopportunities for physical fitness. If active transport scenarios
reached the levels of those in Copenhagen, costs averted for theEngland and Wales National Health Service would approximate$25 billion over a 20-year period207; also for just 1 region of theUnited States, $3.8 billion per year (95% CI, $2.7-$5.0 billion)would be saved through physical fitness benefits stemming fromincreased biking.208
Energy SectorIncreasing use of wind, solar, wave, and geothermal energy can yieldbenefits for both health and climate. A Wisconsin study found thatincreased efficiency and renewable generation in electrical power,designed to reduce carbon at low cost, could reduce statewide emis-sions of nitrogen oxides by 55% and sulfur dioxide by 59%.209 Re-garding biofuels, if sugar cane, fast-growing tree species, and Mis-canthus are used instead of corn, competition for food productioncould be eliminated, thus avoiding food price shocks especially af-fecting the poor.5
Strategies to address short-lived climate pollutants, especiallytropospheric ozone and black carbon, complement those that ad-dress carbon dioxide. Shindell et al210 screened 400 potential con-trol measures and identified 14 that both mitigate warming and im-prove air quality, such as reducing emissions from coal mining, oiland gas production, and municipal landfills. The measures are esti-mated to reduce global mean warming by approximately 0.5°C by2050. Health cobenefits include prevention of between 0.7 millionand 4.7 million premature deaths annually, while crop yields wouldbenefit from reduced ozone damage.
Retrofitting buildings with improved insulation, ventilation, ef-ficient appliances, and renewable sources for electricity and heat-ing could improve health and reduce greenhouse gas emissions.211
Health care is among the most energy-intensive commercial sec-tors. It represents nearly one-fifth of the US gross domestic prod-uct. Health care facilities that reduce energy use can therefore con-tribute to climate mitigation, reduce operating costs, anddemonstrate leadership. More than 6700 health care facilities haveshifted to environmentally sustainable practices and formed “Hos-pitals for a Healthy Environment.”212
Transportation and Community DesignMajor health cobenefits accrue from increased urban walking andcycling, so-called active travel. This approach may offer the most di-rect benefits by reducing health-damaging pollution emissions andenhancing personal fitness simultaneously. Physical inactivity is a riskfactor for many noncommunicable diseases and may be respon-sible for 3.2 million deaths annually.213 An increasing number of stud-ies show significant global health benefits from shifting to environ-mentally sustainable practices (key findings are summarized in theTable). For example, active commuting in Shanghai, China, was as-sociated with a reduction of colon cancer by 48% in men and 44%in women,223 and across sample populations from Europe and Asia,active transport led to an 11% reduction in cardiovascular risk.217 Forthe United States, comparing cities with highest vs lowest levels ofactive transport, obesity rates were 20% lower and diabetes rateswere 23% lower,222 and 1295 lives could be saved annually in theupper Midwest of the United States by replacing short (<4 km) cartrips with bike transport.208
Developed countries, including the United States, could ben-efit from greater levels of exercise,208,215,216,222,229 whereas low-
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E8 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
Table. Health, Environmental, and Economic Benefits of Active Commutinga
Source Location Study Population Key Findings
Cardiovascular Diseases
Woodcock et al,2142013 England (outside London) and Wales All age groups living in urban areasoutside London
Reductions in IHD disease fromincreased physical activity, with areduction in the total population diseaseburden of ≤4.1%
Maizlish et al,215 2013 San Francisco Bay area All age groups 14% Decrease in cardiovascular disease(32 466 DALYs), increased traffic injuryburden by 39% (5907 DALYs), anddecreased greenhouse gas emissions by14% with 20 min/d of activetransportation
Hankey et al,216 2012 Southern California 30 007 Residents Lower IHD mortality rates in high- vslow-walkability neighborhoods(24.9% vs 12.5%) and 7 fewer IHDdeaths/100 000/y
Hamer et al,217 2008 8 Countries in Europe and Asia 173 146 Participants Active commuting was associated withan overall 11% reduction incardiovascular risk, especially amongwomen
Hu et al,218 2007 Finland 47 840 Finnish participants aged25-64 y
Active commuting in Finland reduces10-y risk of chronic heart disease events
Forrest et al219 2001 Benin, Nigeria 799 Civil servants Commuting to work vs leisure activitiescontributed more to reported physicalactivity time and was associated withreduced coronary heart disease risk
Chronic Diseases
Jarrett et al,207 2012 England and Wales Urban populations across the UnitedKingdom
Reductions in prevalence of 7 chronicdiseases associated with physicalinactivity; would save US $26 billionwithin 20 y
Rabl and de Nazelle,220 2012 Europe Large cities across the EuropeanUnion
For every driver who switches tobicycling for a commute of 5 km (1way) 5 d/wk 46 wk/y, the annualbenefit would be €1300 from improvedphysical fitness and €30 from improvedair quality
MacDonald et al,221 2010 Charlotte, North Carolina Individuals before and after light railsystem construction
Light rail transit for commuting wasassociated with a 1.18 reduction in BMIand an 81% reduced odds of becomingobese over time
Pucher et al,222 2010 47 Large US cities Adults ≥18 y US cities with highest active transporthave 20% diabetes rate vs 23% in lowestactive transport
Hou et al,223 2004 Shanghai, China 931 Colon cancer cases vs 1552controls
High levels of daily active commutingresult in reduced risk of colon cancer by48% in men and 44% in women
Mortality and/or Economic Benefits
Macmillan et al,224 2014 New Zealand Urban population of Auckland, NewZealand (1.5 million)
System dynamic modeling showstransforming urban roads using bestpractice of physical separation andbicycle friendly speed reduction wouldyield benefits 10-25 times greater thancosts, over next 40 y
Rojas-Rueda et al,225 2012 Metropolitan Barcelona, Spain All age groups Shifting 40% of car trips to cycling andpublic transportation would avoidapproximately 99 deaths and reducecarbon dioxide emissions by 251 tonsper year
Grabow et al,208 2012 Upper midwestern United States All age groups, 11 metropolitan areas 1295 Avoided annual deaths fromautomobile emissions reduction andfitness benefit from bicycling
Lindsay et al,226 2011 Auckland, New Zealand Residents of urban Auckland Shifting 5% of vehicle kilometers tocycling would save 22 million L of fuel,avoid 122 deaths annually, and saveNew Zealand $200 million per y
de Hartog et al,227 2010 The Netherlands and England 500 000 Dutch Fitness benefits of cycling were 9 timesmore in life-years than losses due toincreased inhaled air pollution dosesand traffic crashes
Andersen et al,228 2000 Copenhagen, Denmark Men and women in all age groups Commuter cyclists have 39% lowermortality rate
Abbreviations: BMI, body mass index; DALY, daily activities of living; IHD, ischemic heart disease.a Active commuting: walking or biking to work.
Climate Change and Global Health Challenges Special Communication Clinical Review & Education
jama.com JAMA Published online September 22, 2014 E9
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
income countries with air quality problems may benefit more fromreduced pollution.229 Commuting to work by biking or walking re-duces prevalence of obesity and diabetes in the United States, withstates showing more variability in levels of active transport than cites(Figure 3).222
Agricultural Sector and Food SystemsHealth cobenefits also emerge from decreased meat consump-tion in high-consuming populations. Emissions from agriculture,livestock production, and forestry constitute approximately 24%of global greenhouse gas emissions,5 resulting principally fromanimal products. A review of 25 studies230 using the life-cycleanalysis concluded that beef (14-32 kg of carbon dioxide emissionequivalents per kilogram of meat produced) had the highest car-bon footprint, followed by pork (3.9-10 kg of carbon dioxide emis-sion equivalents per kg), then chicken (3.7-6.9 kg of carbon diox-ide emission equivalents per kg). If consumption of meat, dairyproducts, and eggs were halved, nitrogen and greenhouse gasemissions could be reduced by 25% to 40% and intake of satu-rated fat may decrease by 40%.231 A 30% reduction in livestockproduction could lead to a reduction in ischemic heart disease of15% in the United Kingdom and 16% in Sao Paulo, Brazil.232
Figure 4 compares greenhouse gas emissions from variousdiets.233 Greenhouse gas emissions to support a high–red meatdiet (>100 g/d) are nearly twice that of vegetarian diets.
Household EnergyImproved cook stoves in the developing world offer anotheropportunity for significant health cobenefits. In India, a programto introduce 150 million improved stoves over 10 years may pre-vent 2 million premature deaths.211 Additionally, rural electrifica-tion, for example, through microgrid systems (from solar, wind,small hydropower, or biogas) could provide lighting that mayenhance childhood reading and learning, and improve food andmedicine cold storage.
Access to contraception can address unmet reproductive healthneeds and improve the health of both mother and child by increas-ing birth spacing.234 Historical trends demonstrate a close relation-ship between carbon dioxide emissions from energy use and country-specific population size. Comparison of a United Nations lowpopulation growth scenario (7.4 billion) with a high population
Figure 3. Relationship Between Active Commuting Transportation andObesity, Diabetes, and Physical Activity Recommendations
65
60
55
50
45
40
350 164 6 8 10 1412
Ad
ult
s W
ith
Rec
om
men
ded
Dai
ly P
hys
ical
Act
ivit
y, %
Workers Commuting by Bicycle or Foot, %
2
States
Cities
Recommended Levels of Physical Activity
12
9
11
10
8
7
6
5
40 164 6 8 10 1412
Ad
ult
s W
ith
Dia
bet
es,
%
Workers Commuting by Bicycle or Foot, %
2
States
Cities
Diabetes
36
28
34
32
30
26
24
22
20
180 164 6 8 10 1412
Ad
ult
s S
elf-
Rep
ort
ing
as
Ob
ese,
%
Workers Commuting by Bicycle or Foot, %
2
States Cities
Self-Reported Obesity
States (n = 50)
Cities (n = 47)
Data are for all 50 US states and 47 of the largest US cities in 2007. Data arederived from Centers for Disease Control and Prevention’s Behavioral RiskFactor Surveillance System and the US Census. Data for these graphs wereprovided by Pucher et al 2010.222
Figure 4. Estimated Greenhouse Gas Emissions From Diet Types
8
4
5
7
6
3
2
Mea
n C
arb
on
Dio
xid
e E
qu
ival
ents
per
d,
kg
≥100 50-99 <50 Fish Vegetarian Vegan
Meat, g/d
Diet Type
Mean greenhouse gas emissions (in kilograms of carbon dioxide equivalents perday) comparing diet types from 55 504 individuals in the EPIC-Oxford cohortstudy. Data are for a 2000 kcal diet adjusted for sex and age. Data fromScarborough et al.233
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E10 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
growth (10.6 billion) suggests a difference in global carbon dioxideemissions of 32% by 2050.174
Future ChallengesThe relationship between climate change and health has been basedon laboratory studies, observational data, and modeling studies. Tra-ditional experimental designs to assess the effects of climate changeare not possible. This often contributes to a political and scientificatmosphere of debate. Because climate change may have impor-tant implications for the health of the world’s population, high-quality research must be conducted, and responsible, informed de-bate needs to continue. However, given that evidence over the past20 years suggests that climate change can be associated with ad-verse health outcomes, strategies to reduce climate change and avertthe related adverse effects are necessary.
Development of effective future policies will require under-standing the relationship between climate change and health anddeveloping approaches to ensure a sustainable future while pro-tecting health. Accounting for cobenefits may document thatreducing greenhouse emission yields net economic benefits,205,235
that labor productivity increases,236 and that health system costsare reduced.207 Cobenefits can provide policymakers with addi-tional incentives, beyond those of curtailing climate change, toreduce the emissions of both carbon dioxide and short-lived cli-mate pollutants.
Any policy to reduce greenhouse gas emissions should includean assessment to ensure that potential benefits or risks are in-cluded in cost estimates and that unintended harm is avoided. Hereinlies a special role for health professionals in policy decisions involv-ing energy, housing, transportation, urban planning, agriculture, foodsystems, and more.
ConclusionsEvidence over the past 20 years indicates that climate change canbe associated with adverse health outcomes. Health professionalshave an important role in understanding and communicating po-tential health concerns related to climate change, as well as the co-benefits from burning less fossil fuels.
ARTICLE INFORMATION
Published Online: September 22, 2014.doi:10.1001/jama.2014.13186.
Author Affiliations: Global Health Institute, NelsonInstitute, Madison, Wisconsin (Patz); NelsonInstitute for Environmental Studies, University ofWisconsin, Madison (Patz, Holloway); Departmentof Population Health Sciences, University ofWisconsin, Madison (Patz); School of Public Health,University of Washington, Seattle (Frumkin);Department of Atmospheric/Oceanic Sciences,University of Wisconsin, Madison (Holloway,Vimont); Nelson Institute, Center for ClimaticResearch, University of Wisconsin, Madison(Vimont); Department of Social and EnvironmentalHealth Research and Population Health, LondonSchool of Hygiene & Tropical Medicine, London,England (Haines); Department of PopulationHealth, London School of Hygiene & TropicalMedicine, London, England (Haines).
Author Contributions: Dr Patz had full access to allof the data in the study and takes responsibility forthe integrity of the data and the accuracy of thedata analysis. Dr Patz led the organization andwriting of all aspects of this manuscript. DrsFrumkin and Haines contributed to sections of thearticle and also helped edit the full draft. Dr Vimontled the US temperature analysis (results displayedin Figure 1). Dr Holloway conducted the ozone-temperature analysis (results displayed in Figure 2)and contributed to the writing and editing of themanuscript.Study concept and design: Patz, Frumkin, Haines.Acquisition, analysis, or interpretation of data: Allauthors.Drafting of the manuscript: Patz, Frumkin,Holloway, Haines.Critical revision of the manuscript for importantintellectual content: All authors.Statistical analysis: Holloway, Vimont.Administrative, technical, or material support: Patz,Vimont, Haines.Study supervision: Patz, Holloway, Vimont.
Conflict of Interest Disclosures: All authors havecompleted and submitted the ICMJE Form for
Disclosure of Potential Conflicts of Interest. DrHaines reported that he was the review editor forthe health chapter of the Intergovernmental Panelon Climate Change, Working Group II, AssessmentReport 5. Dr Patz reported that he served as leadauthor on the Midwest chapter of the third USNational Climate Assessment. No other disclosuresare reported.
Additional Contributions: We would especially liketo thank the following individuals from theUniversity of Wisconsin: David Lorenz, PhD, of theCenter for Climatic Research and the WisconsinInitiative on Climate Impacts for the analysis toproduce Figure 1; Lewis Kunik, for workdownloading data and plotting Figure 2; MaggieGrabow, PhD, of the Global Health Institute forliterature review on active transport; Mollie Overby,BA, and Eric Obscherning for literature review andmanuscript preparation. We thank Ralph Buehler(Virginia Tech), John Pucher (Rutgers University),and Andy Dannenberg (University of Washington)for the data from which Figure 3 was drawn. Finally,we thank Ed Maibach, PhD, from George MasonUniversity for assistance on the communicationsection. None of those listed received remunerationfor their contributions.
REFERENCES
1. Intergovernmental Panel on Climate Change.Climate Change 2013: The Physical Science Basis. NewYork, NY: Cambridge University Press; 2013:1535.
2. Anderegg WR, Prall JW, Harold J, Schneider SH.Expert credibility in climate change. Proc Natl AcadSci U S A. 2010;107(27):12107-12109.
3. Cook J, Nuccitelli D, Green SA, et al. Quantifyingthe consensus on anthropogenic global warming inthe scientific literature. Environ Res Lett. 2013;8(2).doi:10.1088/1748-9326/8/2/024024.
4. Molina M, McCarthy J, Wall D, et al. What WeKnow: The Reality, Risks and Response to ClimateChange. Washington, DC: American Association forthe Advancement of Science; 2014.
5. Intergovernmental Panel on Climate Change.Climate Change 2014: Mitigation of Climate Change.New York, NY: Cambridge University Press; 2014.
6. Karl TR, Melillo JM, Peterson TC, eds. Globalclimate Change Impacts in the United States. NewYork, NY: Cambridge University Press; 2009.
7. Intergovernmental Panel on Climate Change.Climate Change 2014: Impacts, Adaptation, andVulnerability. Part B: Regional Aspects. New York, NY:Cambridge University Press; 2014.
8. Climate Change Impacts in the United States.The Third National Climate Assessment.Washington, DC: US Global Change ResearchProgram; 2014:841. http://nca2014.globalchange.gov. Accessed May 21, 2014.
9. Haines A, Dora C. How the low carbon economycan improve health. BMJ. 2012;344:e1018.
10. Patz JA, Epstein PR, Burke TA, Balbus JM.Global climate change and emerging infectiousdiseases. JAMA. 1996;275(3):217-223.
11. Patz JA, McGeehin MA, Bernard SM, et al. Thepotential health impacts of climate variability andchange for the United States: executive summary ofthe report of the health sector of the US NationalAssessment. Environ Health Perspect. 2000;108(4):367-376.
12. Notaro M, Lorenz DJ, Vimont D, Vavrus S,Kucharik C, Franz K. 21st century Wisconsin snowprojections based on an operational snow modeldriven by statistically downscaled climate data. Int JClimatol. 2011;31(11):1615-1633.
13. Kirchmeier MC, Lorenz DJ, Vimont DJ.Statistical downscaling of daily wind speedvariations. J Appl Meteorol Climatol. 2014;53(3):660-675.
14. Meehl GA, Covey C, Taylor KE, et al. The WCRPCMIP3 multimodel dataset: a new era in climatechange research. Bull Am Meteorol Soc. 2007;88(9):1383-1394.
15. Connecticut Department of Energy andEnvironmental Protection. Ozone air quality levelsin Connecticut and recent trends.http://www.ct.gov/deep/lib/deep/air/regulations
Climate Change and Global Health Challenges Special Communication Clinical Review & Education
jama.com JAMA Published online September 22, 2014 E11
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
/proposed_and_reports/section_3.pdf. AccessedMay 21, 2014.
16. Donoghue ER, Graham MA, Jentzen JM,Lifschultz BD, Luke JL, Mirchandani HG; NationalAssociation of Medical Examiners Ad HocCommittee on the Definition of Heat-RelatedFatalities. Criteria for the diagnosis of heat-relateddeaths. Am J Forensic Med Pathol. 1997;18(1):11-14.
17. Centers for Disease Control and Prevention.Heat-related deaths after an extreme heatevent—four states, 2012, and United States,1999-2009. MMWR Morb Mortal Wkly Rep. 2013;62(22):433-436.
18. Luber G, McGeehin M. Climate change andextreme heat events. Am J Prev Med. 2008;35(5):429-435.
19. Robine J-M, Cheung SLK, Le Roy S, et al. Deathtoll exceeded 70 000 in Europe during the summerof 2003. C R Biol. 2008;331(2):171-178.
20. Matsueda M. Predictability of Euro‐Russianblocking in summer of 2010. Geophys Res Lett.2011;38(6). doi:10.1029/2010GL046557.
21. Li B, Sain S, Mearns LO, et al. The impact ofextreme heat on morbidity in Milwaukee,Wisconsin. Clim Change. 2012;110(3-4):959-976.
22. Bobb JF, Peng RD, Bell ML, Dominici F.Heat-related mortality and adaptation to heat in theUnited States. Environ Health Perspect.http://www.indiaenvironmentportal.org.in/files/file/heat%20related%20mortality.pdf. Published April29, 2014. Accessed September 3, 2014.
23. Peng RD, Bobb JF, Tebaldi C, McDaniel L, BellML, Dominici F. Toward a quantitative estimate offuture heat wave mortality under global climatechange. Environ Health Perspect. 2011;119(5):701-706.
24. Meehl GA, Tebaldi C. More intense, morefrequent, and longer lasting heat waves in the 21stcentury. Science. 2004;305(5686):994-997.
25. Goodess CM. How is the frequency, locationand severity of extreme events likely to change upto 2060? Environ Sci Policy. 2013;27:S4-S14.doi:10.1016/j.envsci.2012.04.001.
26. Barriopedro D, Fischer EM, Luterbacher J, TrigoRM, García-Herrera R. The hot summer of 2010:redrawing the temperature record map of Europe.Science. 2011;332(6026):220-224.
27. Bouchama A, Dehbi M, Mohamed G, MatthiesF, Shoukri M, Menne B. Prognostic factors in heatwave related deaths: a meta-analysis. Arch InternMed. 2007;167(20):2170-2176.
28. Bulbena A, Sperry L, Cunillera J. Psychiatriceffects of heat waves. Psychiatr Serv. 2006;57(10):1519.
29. Chew KS, McCleary R. The spring peak insuicides: across-national analysis. Soc Sci Med.1995;40(2):223-230.
30. Deisenhammer EA. Weather and suicide: thepresent state of knowledge on the association ofmeteorological factors with suicidal behaviour.Acta Psychiatr Scand. 2003;108(6):402-409.
31. Maes M, De Meyer F, Thompson P, Peeters D,Cosyns P. Synchronized annual rhythms in violentsuicide rate, ambient temperature and thelight-dark span. Acta Psychiatr Scand. 1994;90(5):391-396.
32. Page LA, Hajat S, Kovats RS. Relationshipbetween daily suicide counts and temperature inEngland and Wales. Br J Psychiatry. 2007;191:106-112.
33. Basu R, Samet JM. Relation between elevatedambient temperature and mortality: a review of theepidemiologic evidence. Epidemiol Rev. 2002;24(2):190-202.
34. Hansen A, Bi P, Nitschke M, Ryan P, Pisaniello D,Tucker G. The effect of heat waves on mental healthin a temperate Australian city. Environ HealthPerspect. 2008;116(10):1369-1375.
35. Shiloh R, Weizman A, Epstein Y, et al. Abnormalthermoregulation in drug-free male schizophreniapatients. Eur Neuropsychopharmacol. 2001;11(4):285-288.
36. Shiloh R, Weizman A, Stryjer R, Kahan N,Waitman D-A. Altered thermoregulation inambulatory schizophrenia patients: a naturalisticstudy. World J Biol Psychiatry. 2009;10(2):163-170.
37. Chong TW, Castle DJ. Layer upon layer:thermoregulation in schizophrenia. Schizophr Res.2004;69(2-3):149-157.
38. Epstein Y, Albukrek D, Kalmovitc B, Moran DS,Shapiro Y. Heat intolerance induced byantidepressants. Ann N Y Acad Sci. 1997;813:553-558.
39. Hermesh H, Shiloh R, Epstein Y, Manaim H,Weizman A, Munitz H. Heat intolerance in patientswith chronic schizophrenia maintained withantipsychotic drugs. Am J Psychiatry. 2000;157(8):1327-1329.
40. Eyer F, Zilker T. Bench-to-bedside review:mechanisms and management of hyperthermia dueto toxicity. Crit Care. 2007;11(6):236.
41. Martin-Latry K, Goumy M-P, Latry P, et al.Psychotropic drugs use and risk of heat-relatedhospitalisation. Eur Psychiatry. 2007;22(6):335-338.
42. Stöllberger C, Lutz W, Finsterer J. Heat-relatedside-effects of neurological and non-neurologicalmedication may increase heatwave fatalities. Eur JNeurol. 2009;16(7):879-882.
43. Cusack L, de Crespigny C, Athanasos P.Heatwaves and their impact on people with alcohol,drug and mental health conditions: a discussionpaper on clinical practice considerations. J Adv Nurs.2011;67(4):915-922.
44. Martinez M, Devenport L, Saussy J, Martinez J.Drug-associated heat stroke. South Med J. 2002;95(8):799-802.
45. Tasian GE, Pulido JE, Gasparrini A, et al. Dailymean temperature and clinical kidney stonepresentation in five US metropolitan areas:a time-series analysis; 2014. http://ehp.niehs.nih.gov/wp-content/uploads/advpub/2014/7/ehp.1307703.pdf. Accessed September 3, 2014.
46. Weisskopf MG, Anderson HA, Foldy S, et al.Heat wave morbidity and mortality, Milwaukee,Wis, 1999 vs 1995: an improved response? Am JPublic Health. 2002;92(5):830-833.
47. Stone B Jr, Vargo J, Liu P, et al. Avoidedheat-related mortality through climate adaptationstrategies in three US cities. PLoS ONE. 2014;9(6):e100852.
48. Hajat S, Vardoulakis S, Heaviside C, Eggen B.Climate change effects on human health:projections of temperature-related mortality for theUK during the 2020s, 2050s and 2080s.J Epidemiol Community Health. 2014;68(7):641-648.
49. Knowlton K, Lynn B, Goldberg RA, et al.Projecting heat-related mortality impacts under achanging climate in the New York City region. Am JPublic Health. 2007;97(11):2028-2034.
50. Ebi KL, Mills D. Winter mortality in a warmingclimate: a reassessment. Wiley Interdiscip Rev ClimChang. 2013;4(3):203-212. doi:10.1002/wcc.211.
51. Kjellstrom T, Lemke B, Hyatt O. Increasedworkplace heat exposure due to climate change:a potential threat to occupational health, workerproductivity and local economic development inAsia and the Pacific region. Asian-Pacific Newsletter.2011;18(1):6-11.
52. Kjellstrom T, Holmer I, Lemke B. Workplaceheat stress, health and productivity—an increasingchallenge for low- and middle-income countriesduring climate change. Glob Health Action. 2009;2:1-6.
53. Dunne JP, Stouffer RJ, John JG. Reductions inlabour capacity from heat stress under climatewarming. Nat Clim Change. 2013;3(6):563-566.
54. Jacob DJ, Winner DA. Effect of climate changeon air quality. Atmos Environ. 2009;43(1):51-63.
55. Holloway T, Spak SN, Barker D, et al. Change inozone air pollution over Chicago associated withglobal climate change. J Geophys Res. 2008;113(D22):306. doi:10.1029/2007JD009775.
56. Trail M, Tsimpidi AP, Liu P, et al. Sensitivity of airquality to potential future climate change andemissions in the United States and major cities.Atmos Environ. 2014;94:552-563.http://www.sciencedirect.com/science/article/pii/S1352231014004452. Accessed September 3,2014.
57. Chang HH, Zhou J, Fuentes M. Impact ofclimate change on ambient ozone level andmortality in southeastern United States. Int JEnviron Res Public Health. 2010;7(7):2866-2880.
58. Polvani LM, Waugh DW, Correa GJ, Son S-W.Stratospheric ozone depletion: the main driver oftwentieth-century atmospheric circulation changesin the southern hemisphere. J Clim. 2011;24(3):795-812. doi:10.1175/2010JCLI3772.1.
59. Liao H, Chen W, Seinfeld JH. Role of climatechange in global predictions of future troposphericozone and aerosols. J Geophys Res. 2006;111(D12):304. doi:10.1029/2005JD006852.
60. Bell ML, Goldberg R, Hogrefe C, et al. Climatechange, ambient ozone, and health in 50 US cities.Clim Change. 2007;82(1-2):61-76.
61. US Environmental Protection Agency. Summarynonattainment area population exposure report;2014. http://www.epa.gov/airquality/greenbook/popexp.html. Updated July 2, 2014. AccessedSeptember 3, 2014.
62. Brauer M, Amann M, Burnett RT, et al.Exposure assessment for estimation of the globalburden of disease attributable to outdoor airpollution. Environ Sci Technol. 2012;46(2):652-660.
63. Handmer J, Honda Y, Kundzewicz Z, et al.Changes in Impacts of Climate Extremes: HumanSystems and Ecosystems. New York, NY: CambridgeUniversity Press; 2012:231-290.
64. Johnston FH, Henderson SB, Chen Y, et al.Estimated global mortality attributable to smokefrom landscape fires. Environ Health Perspect. 2012;120(5):695-701.
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E12 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
65. Kinney PL, O’Neill MS, Bell ML, Schwartz J.Approaches for estimating effects of climatechange on heat-related deaths: challenges andopportunities. Environ Sci Policy. 2008;11(1):87-96.doi:10.1016/j.envsci.2007.08.001.
66. Allergyusa. Allergy facts and figures.http://allergyusa.com/allergy-resources/providers/allergy-facts-figures. Accessed May 21, 2014.
67. Centers for Disease Control and Prevention.National Health Interview Survey Data. Atlanta, GA:Centers for Disease Control and Prevention; 2010.
68. García-Mozo H, Galán C, Jato V, et al. Quercuspollen season dynamics in the Iberian peninsula:response to meteorological parameters andpossible consequences of climate change. AnnAgric Environ Med. 2006;13(2):209-224.
69. Rogers CA, Wayne PM, Macklin EA, et al.Interaction of the onset of spring and elevatedatmospheric CO2 on ragweed (Ambrosiaartemisiifolia L.) pollen production. Environ HealthPerspect. 2006;114(6):865-869.
70. Singer BD, Ziska LH, Frenz DA, Gebhard DE,Straka JG. Increasing Amb a 1 content in commonragweed (Ambrosia artemisiifolia) pollen as afunction of rising atmospheric CO2 concentration.Funct Plant Biol. 2005;32(7):667-670. doi:10.1071/FP05039.
71. Ziska L, Knowlton K, Rogers C, et al. Recentwarming by latitude associated with increasedlength of ragweed pollen season in central NorthAmerica. Proc Natl Acad Sci U S A. 2011;108(10):4248-4251.
72. Patz JA, Hahn MB. Climate change(communication arising): regional warming andmalaria resurgence. Nature. 2002;420(6916):627-628.
73. Patz JA, Olson SH. Malaria risk andtemperature: influences from global climatechange and local land use practices. Proc Natl AcadSci U S A. 2006;103(15):5635-5636. doi:10.1073/pnas.0601493103.
74. Patz JA, Hahn MB. Climate change and humanhealth: a one health approach. In: Mackenzie JS,Jeggo M, Daszak P, Richt JA, eds. One Health: TheHuman-Animal-Environment Interfaces in EmergingInfectious Diseases. New York, NY: Springer; 2013:141-171.
75. Kovats RS, Campbell-Lendrum DH, McMichaelAJ, Woodward A, Cox JSH. Early effects of climatechange: do they include changes in vector-bornedisease? Philos Trans R Soc Lond B Biol Sci. 2001;356(1411):1057-1068.
76. Mills JN, Gage KL, Khan AS. Potential influenceof climate change on vector-borne and zoonoticdiseases: a review and proposed research plan.Environ Health Perspect. 2010;118(11):1507-1514.
77. Reiter P. Climate change and mosquito-bornedisease. Environ Health Perspect. 2001;109(suppl1):141-161.
78. Siraj AS, Santos-Vega M, Bouma MJ, Yadeta D,Ruiz Carrascal D, Pascual M. Altitudinal changes inmalaria incidence in highlands of Ethiopia andColombia. Science. 2014;343(6175):1154-1158.
79. Altizer S, Ostfeld RS, Johnson PT, Kutz S,Harvell CD. Climate change and infectious diseases:from evidence to a predictive framework. Science.2013;341(6145):514-519.
80. Ogden NH, Radojević M, Wu X, Duvvuri VR,Leighton PA, Wu J. Estimated effects of projectedclimate change on the basic reproductive numberof the Lyme disease vector Ixodes scapularis.Environ Health Perspect. 2014;122(6):631-638.
81. Fischer D, Thomas SM, Suk JE, et al. Climatechange effects on Chikungunya transmission inEurope: geospatial analysis of vector’s climaticsuitability and virus’ temperature requirements. IntJ Health Geogr. 2013;12(1):51.
82. Uejio CK, Yale SH, Malecki K, Borchardt MA,Anderson HA, Patz JA. Drinking water systems,hydrology, and childhood gastrointestinal illness inCentral and Northern Wisconsin. Am J Public Health.2014;104(4):639-646.
83. Bush KF, O’Neill MS, Li S, et al. Associationsbetween extreme precipitation andgastrointestinal-related hospital admissions inChennai, India. Environ Health Perspect. 2014;122(3):249-254.
84. de Man H, van den Berg HH, Leenen EJ, et al.Quantitative assessment of infection risk fromexposure to waterborne pathogens in urbanfloodwater. Water Res. 2014;48:90-99.
85. Patz JA, Vavrus SJ, Uejio CK, McLellan SL.Climate change and waterborne disease risk in theGreat Lakes region of the US. Am J Prev Med. 2008;35(5):451-458.
86. Cann KF, Thomas DR, Salmon RL, Wyn-JonesAP, Kay D. Extreme water-related weather eventsand waterborne disease. Epidemiol Infect. 2013;141(4):671-686.
87. Petersen LR, Fischer M. Unpredictable anddifficult to control—the adolescence of West Nilevirus. N Engl J Med. 2012;367(14):1281-1284.
88. Intergovernmental Panel on Climate Change.Climate Change 2014: Impacts, Adaptation, andVulnerability. New York, NY: Cambridge UniversityPress; 2014.
89. Food and Agriculture Organization of theUnited Nations. The state of food insecurity in theworld 2013. http://www.fao.org/docrep/018/i3434e/i3434e.pdf. Accessed May 21, 2014.
90. Wheeler T, von Braun J. Climate changeimpacts on global food security. Science. 2013;341(6145):508-513.
91. Nelson GC, Rosegrant MW, Koo J, et al. ClimateChange: Impact on Agriculture and Costs ofAdaptation. Washington, DC: International FoodPolicy Research Institute; 2009.
92. Grace K, Davenport F, Funk C, Lerner AM. Childmalnutrition and climate in Sub-Saharan Africa: ananalysis of recent trends in Kenya. Appl Geogr.2012;35(1):405-413.
93. Lloyd SJ, Kovats RS, Chalabi Z. Climate change,crop yields, and undernutrition: development of amodel to quantify the impact of climate scenarioson child undernutrition. Environ Health Perspect.2011;119(12):1817-1823.
94. Bailey R. Growing a better future: food justicein a resource-constrained world. Oxfam Policy PractAgric Food Land. 2011;11(2):93-168.
95. Chakraborty S, Newton AC. Climate change,plant diseases and food security: an overview. PlantPathol. 2011;60(1):2-14. doi:10.1111/j.1365-3059.2010.02411.x.
96. Myers SS, Zanobetti A, Kloog I, et al. IncreasingCO2 threatens human nutrition. Nature. 2014;510(7503):139-142.
97. Whiteford HA, Degenhardt L, Rehm J, et al.Global burden of disease attributable to mental andsubstance use disorders: findings from the GlobalBurden of Disease Study 2010. Lancet. 2013;382(9904):1575-1586.
98. Kessler RC, Chiu WT, Demler O, Merikangas KR,Walters EE. Prevalence, severity, and comorbidityof 12-month DSM-IV disorders in the NationalComorbidity Survey Replication [publishedcorrection appears in Arch Gen Psychiatry.2005;62(7):709]. Arch Gen Psychiatry. 2005;62(6):617-627.
99. Berry HL, Hogan A, Owen J, Rickwood D,Fragar L. Climate change and farmers’ mentalhealth: risks and responses. Asia Pac J Public Health.2011;23(2)(suppl):119S-32.
100. Doherty TJ, Clayton S. The psychologicalimpacts of global climate change. Am Psychol. 2011;66(4):265-276.
101. Fritze JG, Blashki GA, Burke S, Wiseman J.Hope, despair and transformation: climate changeand the promotion of mental health and wellbeing.Int J Ment Health Syst. 2008;2(1):13.
102. Berry HL, Bowen K, Kjellstrom T. Climatechange and mental health: a causal pathwaysframework. Int J Public Health. 2010;55(2):123-132.
103. Goldmann E, Galea S. Mental healthconsequences of disasters. Annu Rev Public Health.2014;35(1):169-183.
104. Davidson JR, McFarlane AC. The extent andimpact of mental health problems after disaster.J Clin Psychiatry. 2006;67(suppl 2):9-14.
105. Halpern J, Tramontin M. Disaster MentalHealth: Theory and Practice. Belmont, CA: Thomson;2007.
106. North CS, Pfefferbaum B. Mental healthresponse to community disasters: a systematicreview. JAMA. 2013;310(5):507-518.
107. Oldham RL. Mental health aspects ofdisasters. South Med J. 2013;106(1):115-119.
108. Galea S, Brewin CR, Gruber M, et al. Exposureto hurricane-related stressors and mental illnessafter Hurricane Katrina. Arch Gen Psychiatry. 2007;64(12):1427-1434.
109. Ahern M, Kovats RS, Wilkinson P, Few R,Matthies F. Global health impacts of floods:Epidemiologic evidence. Epidemiol Rev. 2005;27:36-46.
110. Fewtrell L, Kay D. An attempt to quantify thehealth impacts of flooding in the UK using an urbancase study. Public Health. 2008;122(5):446-451.
111. Green BL, Grace MC, Vary MG, Kramer TL,Gleser GC, Leonard AC. Children of disaster in thesecond decade: a 17-year follow-up of Buffalo Creeksurvivors. J Am Acad Child Adolesc Psychiatry. 1994;33(1):71-79.
112. Hart CR, Berry HL, Tonna AM. Improving themental health of rural New South Walescommunities facing drought and other adversities.Aust J Rural Health. 2011;19(5):231-238.
113. McFarlane AC, Van Hooff M. Impact ofchildhood exposure to a natural disaster on adultmental health: 20-year longitudinal follow-upstudy. Br J Psychiatry. 2009;195(2):142-148.
Climate Change and Global Health Challenges Special Communication Clinical Review & Education
jama.com JAMA Published online September 22, 2014 E13
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
114. Norris FH, Tracy M, Galea S. Looking forresilience: understanding the longitudinaltrajectories of responses to stress. Soc Sci Med.2009;68(12):2190-2198.
115. Kessler RC, Galea S, Gruber MJ, Sampson NA,Ursano RJ, Wessely S. Trends in mental illness andsuicidality after Hurricane Katrina. Mol Psychiatry.2008;13(4):374-384.
116. Paxson C, Fussell E, Rhodes J, Waters M. Fiveyears later: recovery from post traumatic stress andpsychological distress among low-income mothersaffected by Hurricane Katrina. Soc Sci Med. 2012;74(2):150-157.
117. Brubaker M, Berner J, Chavan R, Warren J.Climate change and health effects in NorthwestAlaska. Glob Health Action. 2011;4. doi:10.3402/gha.v4i0.8445.
118. UN High Commissioner for Refugees. Climatechange, natural disasters and human displacement:a UNHCR perspective; 2009. http://www.unhcr.org/4901e81a4.pdf. Accessed May 21, 2014.
119. Loughry M. Climate change, human movementand the promotion of mental health: what have welearnt from earlier global stressors? In: McAdam J,ed. Climate Change and Displacement:Multidisciplinary Perspectives. Portland, OR: HartPublishing; 2010.
120. Jacob B, Mawson AR, Payton M, Guignard JC.Disaster mythology and fact: Hurricane Katrina andsocial attachment. Public Health Rep. 2008;123(5):555-566. .
121. Leiserowitz A. Communicating the risks ofglobal warming: American risk perceptions. In:Moser S, Dilling L, eds. Creating a Climate forChange: Communicating Climate Change andFacilitaing Social Change. New York, NY: CambridgeUniversity Press; 2007.
122. Reser JP, Swim JK. Adapting to and copingwith the threat and impacts of climate change. AmPsychol. 2011;66(4):277-289.
123. Haines A, Patz JA. Health effects of climatechange. JAMA. 2004;291(1):99-103.
124. Vinck P. World Disasters Report: Focus onTechnology and the Future of Humanitarian Action.Geneva, Switzerland: International Federation of RedCross and Red Crescent Societies; 2013.
125. International Federation of Red Cross and RedCresent Societies. World Disaster Report 1997. NewYork, NY: International Federation of Red Cross andRed Cresent Societies; 1998.
126. Guha-Sapir D, Vos F, Below R, Ponserre S.Annual Disaster Statistical Review 2010. Brussels,Belgium: Center for Research on the Epidemiologyof Disasters, Université Catholique de Louvain; 2011.
127. Doocy S, Daniels A, Packer C, Dick A, KirschTD. The human impact of earthquakes: a historicalreview of events 1980-2009 and systematicliterature review. PLoS Curr. 2013;5. doi:10.1371/currents.dis.67bd14fe457f1db0b5433a8ee20fb833.
128. Bender MA, Knutson TR, Tuleya RE, et al.Modeled impact of anthropogenic warming on thefrequency of intense Atlantic hurricanes. Science.2010;327(5964):454-458.
129. Webster PJ, Holland GJ, Curry JA, Chang H-R.Changes in tropical cyclone number, duration, andintensity in a warming environment. Science. 2005;309(5742):1844-1846.
130. Emanuel K, Sundararajan R, Williams J.Hurricanes and global warming: results fromdownscaling IPCC AR4 simulations. Bull AmMeteorol Soc. 2008;89(3):347-367.
131. McMichael A, McMichael C, Berry H, Bowen K.Climate-related displacement: Health risks andresponses. In: McAdam J, ed. Climate Change andPopulation Displacement: MultidisciplinaryPerspectives. Oxford, England: Hart Publishing Ltd;2010.
132. Levy BS, Sidel VW. Collective violence causedby climate change and how it threatens health andhuman rights. Health Hum Rights Int J. 2014;16(1):32-40.
133. Hsiang SM, Burke M, Miguel E. Quantifying theinfluence of climate on human conflict. Science.2013;341(6151):1235367.
134. Board CMA. National Security and theAccelerating Risks of Climate Change. Alexandria, VA:CNA Corp; 2014.
135. Jones JM. In US, most do not see globalwarming as serious threat. Gallup Politics; 2014.http://www.gallup.com/poll/167879/not-global-warming-serious-threat.aspx. Accessed March 12,2014.
136. Pew Research Center. Climate change: keydata points from Pew Research; 2014. http://www.pewresearch.org/key-data-points/climate-change-key-data-points-from-pew-research. Accessed May 21, 2014.
137. Leiserowitz AM, Roser-Renouf C, Feinberg G,Rosenthal S, Marlon J. Climate Change in theAmerican Mind: Americans’ Global WarmingBeliefs and Attitudes in November, 2013. NewHaven, CT: Yale University and George MasonUniversity; 2014. http://environment.yale.edu/climate-communication/article/Climate-Beliefs-November-2013. Accessed May 21, 2014.
138. Pugliese A, Ray J. A heated debate: globalattitudes toward climate change. Harvard Int Rev.2009;31(3):64-68.
139. Pew Research Center Global Attitudes Project.Global warming seen as a major problem aroundthe world: less concern in the US, China and Russia.http://www.pewglobal.org/2009/12/02/global-warming-seen-as-a-major-problem-around-the-world-less-concern-in-the-us-china-and-russia.Accessed May 21, 2014.
140. Leiserowitz A, Maibach E, Roser-Renauf C,Feinberg G, Rosenthal S. Public Support for Climateand Energy Policies in November 2013. New Haven,CT: Yale University and George Mason University;2014, http://environment.yale.edu/climate-communication/files/Climate-Policy-Report-November-2013.pdf. Accessed May 21, 2014.
141. Leiserowitz AM, Roser-Renouf C, HmielowskiJ. Global Warming’s Six Americas, March 2012 &Nov. 2011. New Haven, CT: Yale University andGeorge Mason University; 2012. http://environment.yale.edu/climate-communication/article/Six-Americas-March-2012. Accessed May 21, 2014.
142. Brulle R, Carmichael J, Jenkins JC. Shiftingpublic opinion on climate change: an empiricalassessment of factors influencing concern overclimate change in the US, 2002–2010. Clim Change.2012;114(2):169-188. doi:10.1007/s10584-012-0403-y.
143. Norgaard KM. Living in Denial: ClimateChange, Emotions, and Everyday Life. Cambridge, MA:MIT Press; 2011.
144. Gifford R. The dragons of inaction:psychological barriers that limit climate changemitigation and adaptation. Am Psychol. 2011;66(4):290-302. doi:10.1037/a0023566.
145. Corner A, Markowitz E, Pidgeon N. Publicengagement with climate change: the role ofhuman values. Wiley Interdiscip Rev Clim Chang.2014;5(3):411-422. doi:10.1002/wcc.269.
146. McCright AM. Political orientation moderatesAmericans’ beliefs and concern about climatechange. Clim Change. 2011;104(2):243-253.doi:10.1007/s10584-010-9946-y.
147. Zia A, Todd AM. Evaluating the effects ofideology on public understanding of climate changescience: how to improve communication acrossideological divides? Public Underst Sci. 2010;19(6):743-761.
148. Wolf J, Moser SC. Individual understandings,perceptions, and engagement with climate change:insights from in-depth studies across the world.Wiley Interdiscip Rev Clim Chang. 2011;2(4):547-569.doi:10.1002/wcc.120.
149. Pidgeon N, Fischhoff B. The role of social anddecision sciences in communicating uncertainclimate risks. Nat Clim Change. 2011;1(1):35-41.doi:10.1038/nclimate1080.
150. Trumbo C. Constructing climate change:claims and frames in US news coverage of anenvironmental issue. Public Underst Sci. 1996;5(3):269-283. doi:10.1088/0963-6625/5/3/006.
151. Hmielowski JD, Feldman L, Myers TA,Leiserowitz A, Maibach E. An attack on science?media use, trust in scientists, and perceptions ofglobal warming [published online April 3, 2013].Public Underst Sci. 2013.
152. Oreskes NC, Conway EM. Merchants of Doubt:How a Handful of Scientists Obsured the Truth onIssues From Tobacco Smoke to Global Warming. NewYork, NY: Bloomsbury; 2010.
153. Boykoff M. Who Speaks for the Climate?Making Sense of Media Reporting on ClimateChange. Cambridge, England: Cambridge UniversityPress; 2011.
154. Boykoff MT, Boykoff JM. Balance as bias:global warming and the US prestige press.Glob Environ Change. 2004;14:125-136.
155. Boykoff M, Boykoff J. Climate change andjournalistic norms: a case-study of US mass-mediacoverage. Geoforum. 2007;38(6):1190-1204.
156. Boykoff MT, Rajan SR. Signals and noise:mass-media coverage of climate change in the USAand the UK. EMBO Rep. 2007;8(3):207-211.
157. Brulle R. Institutionalizing delay: foundationfunding and the creation of US climate changecounter-movement organizations. Clim Change.2014;122(4):681-694. doi:10.1007/s10584-013-1018-7.
158. Powell JL. The Inquisition of Climate Science.New York, NY: Columbia University Press; 2011.
159. Bradley RS. Global Warming and PoliticalIntimidation: How Politicians Cracked Down onScientists as the Earth Heated Up. Amherst: Universityof Massachusetts Press; 2011.
160. Washington H, Cook J. Climate Change Denial:Heads in the Sand. New York, NY: Earthscan; 2011.
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E14 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
161. Maibach E, Myers T, Leiserowitz A. Climatescientists need to set the record straight: There is ascientific consensus that human-caused climatechange is happening. Earth Fut. 2014. doi:10.1002/2013EF000226.
162. Lewandowsky S, Gignac GE, Vaughan S. Thepivotal role of perceived scientific consensus inacceptance of science. Nat Clim Change. 2013;3(4):399-404.
163. Donner SD, McDaniels J. The influence ofnational temperature fluctuations on opinionsabout climate change in the US since 1990. ClimChange. 2013;118(3-4):537-550. doi:10.1007/s10584-012-0690-3.
164. Zaval L, Keenan EA, Johnson EJ, Weber EU.How warm days increase belief in global warming.Nat Clim Change. 2014;4(2):143-147. doi:10.1038/nclimate2093.
165. Myers TA, Maibach EW, Roser-Renouf C,Akerlof K, Leiserowitz AA. The relationshipbetween personal experience and belief in thereality of global warming. Nat Clim Change. 2013;3(4):343-347. doi:10.1038/nclimate1754.
166. Akerlof K, Maibach EW, Fitzgerald D, CedenoAY, Neuman A. Do people “personally experience”global warming, and if so how, and does it matter?Glob Environ Change. 2013;23(1):81-91. doi:10.1016/j.gloenvcha.2012.07.006.
167. Rudman LA, McLean MC, Bunzl M. When truthis personally inconvenient, attitudes change: theimpact of extreme weather on implicit support forgreen politicians and explicit climate-changebeliefs. Psychol Sci. 2013;24(11):2290-2296.
168. Abroms LC, Maibach EW. The effectiveness ofmass communication to change public behavior.Annu Rev Public Health. 2008;29(1):219-234.
169. Maibach EW, Roser-Renouf C, Leiserowitz A.Communication and marketing as climatechange-intervention assets a public healthperspective. Am J Prev Med. 2008;35(5):488-500.
170. Whitmarsh L, O’Neill S, Lorenzoni L, eds.Engaging the Public With Climate Change: BehaviorChange and Communication. New York, NY:Earthscan; 2011.
171. Moser SC, Dilling L. Creating a Climate forChange: Communicating Climate Change andFacilitating Social Change. Cambridge, England:Cambridge University Press; 2007.
172. Bostrom A, Böhm G, O’Connor RE. Targetingand tailoring climate change communications. WileyInterdiscip Rev Clim Chang. 2013;4(5):447-455.doi:10.1002/wcc.234.
173. Moser SC. Communicating climate change:history, challenges, process and future directions.Wiley Interdiscip Rev Clim Chang. 2010;1(1):31-53.doi:10.1002/wcc.11.
174. O’Neill BC, Liddle B, Jiang L, et al.Demographic change and carbon dioxideemissions. Lancet. 2012;380(9837):157-164.
175. Feinberg M, Willer R. Apocalypse soon? diremessages reduce belief in global warming bycontradicting just-world beliefs. Psychol Sci. 2011;22(1):34-38.
176. Maibach EW, Nisbet M, Baldwin P, Akerlof K,Diao G. Reframing climate change as a public healthissue: an exploratory study of public reactions. BMCPublic Health. 2010;10:299.
177. Myers T, Nisbet M, Maibach E, Leiserowitz A.A public health frame arouses hopeful emotionsabout climate change. Clim Change. 2012;113(3-4):1105-1112. doi:10.1007/s10584-012-0513-6.
178. Akerlof K, Debono R, Berry P, et al. Publicperceptions of climate change as a human healthrisk: surveys of the United States, Canada andMalta. Int J Environ Res Public Health. 2010;7(6):2559-2606.
179. Maibach E, Nisbet M, Weathers M. Conveyingthe Human Implication of Climate Change: A ClimateChange Communication Primer for Public HealthProfessionals. Fairfax, VA: George Mason UniversityCenter for Climate Change Communication; 2011,http://www.climatechangecommunication.org/report/new-climate-change-communication-primer-public-health-professionals. Accessed May21, 2014.
180. Sarfaty M, Abouzaid S. The physician’sresponse to climate change. Fam Med. 2009;41(5):358-363.
181. Burton I, Malone E, Huq S. Adaptation PolicyFrameworks for Climate Change: DevelopingStrategies, Policies and Measures. Cambridge,England: University of Cambridge; 2004.
182. Adger WN, Arnell NW, Tompkins EL.Successful adaptation to climate change acrossscales. Glob Environ Change. 2005;15(2):77-86.
183. Intergovernmental Panel on Climate Change.Managing the risks of extreme events and disastersto advance climate change adaptation: specialreport of the Intergovernmental Panel on ClimateChange; 2012. http://www.ipcc-wg2.gov/SREX/images/uploads/SREX-All_FINAL.pdf. AccessedMay 21, 2014.
184. United Nations Population Fund. UNFPA stateof the world population 2007: unleashing thepotential of urban growth; 2007.http://www.unfpa.org/webdav/site/global/shared/documents/publications/2007/695_filename_sowp2007_eng.pdf. Accessed May 21, 2014.
185. Salamanca F, Georgescu M, Mahalov A,Moustaoui M, Wang M. Anthropogenic heating ofthe urban environment due to air conditioning.J Geophys Res Atmos. 2014;119(10):5949-5965.
186. American Society of Civil Engineers. AmericanSociety of Civil Engineers’ 2013 report card forAmerica’s infrastructure. http://www.infrastructurereportcard.org. Accessed May 21,2014.
187. Roe JJ, Thompson CW, Aspinall PA, et al.Green space and stress: evidence from cortisolmeasures in deprived urban communities. Int JEnviron Res Public Health. 2013;10(9):4086-4103.
188. Aspinall P, Mavros P, Coyne R, Roe J. Theurban brain: analysing outdoor physical activitywith mobile EEG [published online March 6, 2013.Br J Sports Med. 2013:1-6.
189. Thompson CW, Roe J, Aspinall P, Mitchell R,Clow A, Miller D. More green space is linked to lessstress in deprived communities: evidence fromsalivary cortisol patterns. Landsc Urban Plan. 2012;105(3):221-229.
190. Maas J, van Dillen SM, Verheij RA,Groenewegen PP. Social contacts as a possiblemechanism behind the relation between greenspace and health. Health Place. 2009;15(2):586-595.
191. Branas CC, Cheney RA, MacDonald JM, TamVW, Jackson TD, Ten Have TR. A difference-in-
differences analysis of health, safety, and greeningvacant urban space. Am J Epidemiol. 2011;174(11):1296-1306.
192. Kuo FE, Sullivan WC. Environment and crimein the inner city: does vegetation reduce crime?Environ Behav. 2001;33(3):343-367.
193. Garvin EC, Cannuscio CC, Branas CC. Greeningvacant lots to reduce violent crime: a randomisedcontrolled trial. Inj Prev. 2013;19(3):198-203.
194. Beyer KM, Kaltenbach A, Szabo A, Bogar S,Nieto FJ, Malecki KM. Exposure to neighborhoodgreen space and mental health: evidence from thesurvey of the health of Wisconsin. Int J Environ ResPublic Health. 2014;11(3):3453-3472.
195. Drewniak BA, Snyder PK, Steiner AL, TwineTE, Wuebbles Dj. Simulated changes in biogenicVOC emissions and ozone formation from habitatexpansion of Acer rubrum (red maple). Environ ResLett. 2014;9(1):14-16.
196. Sukhdev P, Wittmer H, Schroter-Schlaack C,et al. The economics of ecosystems and biodiversitya synthesis of the approach, conclusions andreccommendations of TEEB. United NationsEnvironment Program. 2010. http://www.teebweb.org/wp-content/uploads/Study%20and%20Reports/Reports/Synthesis%20report/TEEB%20Synthesis%20Report%202010.pdf. AccessedSeptember 3, 2014.
197. Mangrove planting saves lives in Vietnam[news release]. Geneva, Switzerland: InternationalFederation of the Red Cross Red Crescent Societies;June 2002. http://www.grida.no/publications/et/ep3/page/2610.aspx. Accessed May 21, 2014.
198. Posner RA. Catastrophe: Risk and Response.New York, NY: Oxford University Press; 2004.
199. Sunstein CR. Worst-Case Scenarios. Cambridge,MA: Harvard University Press; 2007.
200. Nordhaus WD. The economics of tail eventswith an application to climate change. Rev EnvironEcon Policy. 2011;5(2):240-257.
201. Nauclér T, Enkvist P. Pathways to a low-carboneconomy: version 2 of the global greenhouse gasabatement cost curve. http://www.mckinsey.com.Published 2009. Accessed May 21, 2014.
202. Haines A, McMichael AJ, Smith KR, et al.Public health benefits of strategies to reducegreenhouse-gas emissions: overview andimplications for policy makers. Lancet. 2009;374(9707):2104-2114.
203. Hochman G, Kaplan S, Rajagopal D, ZilbermanD. Biofuel and food-commodity prices. Agriculture.2012;2(3):272-281. doi:10.3390/agriculture2030272.
204. Thompson TM, Rausch S, Saari RK, Selin NE.A systems approach to evaluating the air qualityco-benefits of US carbon policies; 2014.http://www.nature.com/nclimate/journal/vaop/ncurrent/full/nclimate2342.html. AccessedSeptember 3, 2014.
205. West JJ, Smith SJ, Silva RA, et al. Co-benefitsof mitigating global greenhouse gas emissions forfuture air quality and human health. Nat ClimChange. 2013;3(10):885-889. doi:10.1038/nclimate2009.
206. US Environmental Protection Agency. Thebenefits and costs of the Clean Air Act from 1990 to2020: summary report. http://www.epa.gov/cleanairactbenefits/feb11/summaryreport.pdf.Published March 2011. Accessed May 21, 2014.
Climate Change and Global Health Challenges Special Communication Clinical Review & Education
jama.com JAMA Published online September 22, 2014 E15
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014

Copyright 2014 American Medical Association. All rights reserved.
207. Jarrett J, Woodcock J, Griffiths UK, et al.Effect of increasing active travel in urban Englandand Wales on costs to the National Health Service.Lancet. 2012;379(9832):2198-2205.
208. Grabow ML, Spak SN, Holloway T, Stone B,Mednick AC, Patz JA. Air quality andexercise-related health benefits from reduced cartravel in the midwestern United States. EnvironHealth Perspect. 2012;120(1):68-76.
209. Plachinski SD, Holloway T, Meier PJ, et al.Quantifying the emissions and air qualityco-benefits of lower-carbon electricity production.Atmos Environ. 2014;94(0):180-191. doi:10.1016/j.atmosenv.2014.03.028.
210. Shindell D, Kuylenstierna JCI, Vignati E, et al.Simultaneously mitigating near-term climatechange and improving human health and foodsecurity. Science. 2012;335(6065):183-189.
211. Wilkinson P, Smith KR, Davies M, et al. Publichealth benefits of strategies to reducegreenhouse-gas emissions: household energy. Lancet.2009;374(9705):1917-1929.
212. Cohen G. First, do no harm. Paper presentedat a conference sponsored by the Robert WoodJohnson Foundation; September 2006.https://www.healthdesign.org/sites/default/files/First%20Do%20No%20Harm_0.pdf. AccessedMay 21, 2014.
213. Lim SS, Vos T, Flaxman AD, et al. Acomparative risk assessment of burden of diseaseand injury attributable to 67 risk factors and riskfactor clusters in 21 regions, 1990-2010:a systematic analysis for the Global Burden ofDisease Study 2010. Lancet. 2012;380(9859):2224-2260.
214. Woodcock J, Givoni M, Morgan AS. HealthEngland and Wales using an integrated transportand health impact modelling tool (ITHIM). PLoS ONE.2013;8(1).
215. Maizlish N, Woodcock J, Co S, Ostro B, Fanai A,Fairley D. Health cobenefits and transportation-related reductions in greenhouse gas emissions inthe San Francisco Bay area. Am J Public Health.2013;103(4):703-709.
216. Hankey S, Marshall JD, Brauer M. Healthimpacts of the built environment: within-urbanvariability in physical inactivity, air pollution, and
ischemic heart disease mortality. Environ HealthPerspect. 2012;120(2):247-253.
217. Hamer M, Chida Y. Active commuting andcardiovascular risk: a meta-analytic review. Prev Med.2008;46(1):9-13.
218. Hu G, Jousilahti P, Antikainen R, Tuomilehto J.Occupational, commuting, and leisure-timephysical activity in relation to cardiovascularmortality among Finnish subjects withhypertension. Am J Hypertens. 2007;20(12):1242-1250.
219. Forrest KY, Bunker CH, Kriska AM, Ukoli FA,Huston SL, Markovic N. Physical activity andcardiovascular risk factors in a developingpopulation. Med Sci Sports Exerc. 2001;33(9):1598-1604.
220. Rabl A, De Nazelle A. Benefits of shift fromcar to active transport. Transp Policy. 2012;19(1):121-131.
221. MacDonald JM, Stokes RJ, Cohen DA, KofnerA, Ridgeway GK. The effect of light rail transit onbody mass index and physical activity. Am J Prev Med.2010;39(2):105-112.
222. Pucher J, Buehler R, Bassett DR, DannenbergAL. Walking and cycling to health: a comparativeanalysis of city, state, and international data. Am JPublic Health. 2010;100(10):1986-1992. doi:10.2105/AJPH.2009.189324.
223. Hou L, Ji BT, Blair A, Dai Q, Gao YT, Chow WH.Commuting physical activity and risk of coloncancer in Shanghai, China. Am J Epidemiol. 2004;160(9):860-867.
224. Macmillan A, Connor J, Witten K, Kearns R,Rees D, Woodward A. The societal costs andbenefits of commuter bicycling: simulating theeffects of specific policies using system dynamicsmodeling. Environ Health Perspect. 2014;122(4):335-344.
225. Rojas-Rueda D, de Nazelle A, Teixidó O,Nieuwenhuijsen MJ. Replacing car trips byincreasing bike and public transport in the greaterBarcelona metropolitan area: a health impactassessment study. Environ Int. 2012;49:100-109.
226. Lindsay G, Macmillan A, Woodward A. Movingurban trips from cars to bicycles: impact on healthand emissions. Aust N Z J Public Health. 2011;35(1):54-60.
227. Johan de Hartog J, Boogaard H, Nijland H,Hoek G. Do the health benefits of cycling outweighthe risks? Environ Health Perspect. 2010;118(8):1109-1116.
228. Andersen LB, Schnohr P, Schroll M, Hein HO.All-cause mortality associated with physical activityduring leisure time, work, sports, and cycling towork. Arch Intern Med. 2000;160(11):1621-1628.
229. Woodcock J, Edwards P, Tonne C, et al. Publichealth benefits of strategies to reducegreenhouse-gas emissions: urban land transport.Lancet. 2009;374(9705):1930-1943.
230. De Vries M, de Boer IJ. Comparingenvironmental impacts for livestock products:a review of life cycle assessments. Livest Sci. 2010;128(1-3):1-11. doi:10.1016/j.livsci.2009.11.007.
231. Westhoek H, Lesschen JP, Rood T, et al. Foodchoices, health and environment: effects of cuttingEurope’s meat and dairy intake. Glob Environ Change.2014;26:196-205. doi:10.1016/j.gloenvcha.2014.02.004.
232. Friel S, Dangour AD, Garnett T, et al. Publichealth benefits of strategies to reducegreenhouse-gas emissions: food and agriculture.Lancet. 2009;374(9706):2016-2025.
233. Scarborough P, Appleby PN, Mizdrak A, et al.Dietary greenhouse gas emissions of meat-eaters,fish-eaters, vegetarians and vegans in the UK. ClimChange. 2014;125(2):179-192. doi:10.1007/s10584-014-1169-1.
234. Diamond-Smith N, Potts M. A woman cannotdie from a pregnancy she does not have. IntPerspect Sex Reprod Health. 2011;37(3):155-158.
235. Nemet G, Holloway T, Meier P. Implications ofincorporating air-quality co-benefits into climatechange policymaking. Environ Res Lett. 2010;5(1):14-17.
236. Jensen H, Keogh-Brown M, Smith R, et al. Theimportance of health co-benefits in macroeconomicassessments of UK Greenhouse Gas emissionreduction strategies. Clim Change. 2013;121(2):223-237. doi:10.1007/s10584-013-0881-6.
Clinical Review & Education Special Communication Climate Change and Global Health Challenges
E16 JAMA Published online September 22, 2014 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 10/09/2014