Embed Size (px)
Citation preview

22 Clin Pathol 1995;48:242-244
Apoptotic and mitotic indices in malignantmelanoma and basal cell carcinoma
E E Mooney, J M Ruis Peris, A O'Neill, E C Sweeney
AbstractAins-To assess the relative frequency ofmitotic and apoptotic cells in malignantmelanoma and basal cell carcinoma.Methods-Retrospective evaluation ofhaematoxylin and eosin stained slidesfrom 10 basal cell carcinomas, 10 nodularmelanomas, and 10 superficial spreadingmelanomas, with counting of apoptoticand mitotic cells per 1000 cells. Selectedcases were studied with in situ end-label-ling.Results-The ratio of apoptotic to mitoticcells was higher in basal cell carcinomathan in either form of melanoma becauseof the presence of a greater number ofapoptotic cells in basal cell carcinoma.Conclusion-The differing growth ratesand biological behaviour of these two tu-mours is reflected in the apoptotic:mitoticratio. Further assessment of this ratio iswarranted, both between tumour typesand between individual tumours of onetype, to determine its value as an indicatorof biological potential.(J Clin Pathol 1995;48:242-244)
Keywords: Apoptosis, mitosis, melanoma, basal cellcarcinoma.
Department ofHistopathology,St James's Hospital,Trinity College,Dublin, IrelandE E MooneyJ M Ruis PerisA O'NeillE C Sweeney
Correspondence to:Professor E C Sweeney,Department ofHistopathology,St James's Hospital,James's Street, Dublin 8,Ireland.
Accepted for publication25 August 1994
Amongst common malignant tumours of theskin, basal cell carcinoma and malignant mela-noma show a marked difference in growth rate,despite the fact that the mitotic rate in bothtumours is of near or equal value. As the rateof tumour growth depends primarily on thegrowth fraction of the cell population and thedegree of imbalance between cell productionand loss,' it is possible that the indolent growthof basal cell carcinoma might be due to greatercell loss than that in malignant melanoma. Totest this hypothesis we measured the mitoticand apoptotic rates of 10 basal cell carcinomasand compared them with the values obtained
Table 1 Characteristics of the malignant melanomas studied
SSMM NMM
Case No. Thickness (mm) Clark's level Thickness (mm) Clark's level
1 0-72 2 2-10 42 1-30 3 3 50 33 040 2 4-20 34 1-20 3 2-00 35 0-65 2 3.40 46 055 2 3-10 47 5 70 5 5-00 48 1-80 4 3-70 59 3 90 4 300 410 0-55 2 6-00 5
SSMM = superficial spreading malignant melanoma; NMM = nodular malignant melanoma.
in 10 superficial spreadingmalignant melanomas.
and 10 nodular
MethodsTen cases each of basal cell carcinoma, su-perficial spreading malignant melanoma andnodular malignant melanoma were randomlyselected from archive material. All neoplasmswere primary tumours of the skin. Standard4 ,um thick haemotoxylin and eosin stained sec-tions were reviewed. Using a grid, 1000 cellswere counted in each superficial spreadingmalignant melanoma. In each basal cell car-cinoma and nodular malignant melanoma 1000cells were counted in both superficial and deepareas of the tumour, and an average taken. Thenumber of apoptotic and mitotic cells per 1000cells was calculated. Only unequivocal mitoseswere counted and only viable areas of thetumour were chosen for assessment. Changesthat could clearly be identified as those ofapoptosis were (a) cells showing marked shrink-age of nucleus and cytoplasm or (b) fragmentsof cytoplasm containing dense chromatin frag-ments.2 Selected cases were studied using insitu end-labelling which identifies characteristicinternucleosomal double strandedDNA breaks(Oncor kit, Alpha Laboratories, Eastleigh,Hampshire, UK). Sections of testis, containingmeiosis induced double stranded DNA breaks,were used as positive controls.34 Bare fragmentsof chromatin, usually less than 3 gm, oramorphous fragments of debris, which couldnot confidently be judged to be apoptotic cells,were not counted. Other features noted werethe presence or absence of ulceration, Breslowtumour thickness,5 and Clarke's level.6Lymphocytic infiltration of tumour was as-sessed and graded from 0 (absent) to 3 (dense).Results were analysed using the Wilcoxon ranksum test.
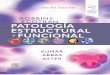
ResultsThe Clarke's level and Breslow thickness of themalignant melanomas are shown in table 1.Each category of malignant melanoma showsa range of lesions, with the average thicknessand level of invasion of the nodular malignantmelanomas being greater than in the superficialspreading malignant melanomas. The numbersof apoptotic and mitotic cells per 1000 cells(that is, the apoptotic and mitotic rates) areshown for each of the three tumour types intable 2. The number of mitoses did not exceedfive per 1000 in any of the tumours studied. Bycontrast, the number of apoptotic cells variedconsiderably, with basal cell carcinoma (fig 1)
242
on May 11, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.3.242 on 1 March 1995. D
ownloaded from

Apoptotic and mitotic indices in malignant melanoma and basal cell carcinoma 243
Table 2 Apoptotic (A) and mitotic (M) figures per 1000 cells in basal cell carcinomas (BCC), superficial spreading malignant melanomas (SSMM)and nodular malignant melanomas (NMM)
BCC SSMM NMM
Apoptosis: Apoptosis: Apoptosis:Case No. M A mitosis ratio M A mitosis ratio M A motosis ratio
1 3-0 20-0 6-7 0 2-0 ND 2-0 2-0 1-02 3-5 13-0 3-7 1.0 0 0 1-5 2-0 1-33 5-0 16-0 3-2 2-0 1.0 0-5 5-0 3-5 0-74 1-0 43-5 43-5 1-0 8-0 8-0 2-0 3-0 1-55 0-5 5-5 11*0 0 0 0 1-0 7-0 7-06 0-5 9-0 18-0 2-0 2-0 1-0 4-0 8-0 2-07 0 24-5 ND 1-0 4-0 4-0 2-5 3-0 1-28 0-5 5-0 10-0 0 1-0 ND 2-5 1-5 0-69 1-5 12-0 8-0 3-0 5-0 1-7 2-5 5-5 2-210 1-5 15-5 10-3 0 4-0 ND 4-5 2-0 0-4
Figure 1 Basal cell carcinoma showing numerous mitoticfigures (large amrowheads) and apoptotic figures (smallarrowheads).
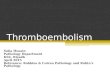
Figure 2 Melanoma showing mitotic figures(arrowheads), but no apoptotic figures.
showing a wide range of values compared withsuperficial spreading and nodular malignantmelanomas (fig 2). Expression of values as aratio (apoptosis:mitosis) is shown in table 2.The mean value of this ratio for basal cellcarcinoma was 13-9 (median 10-0); for su-perficial spreading malignant melanoma themean was 2-3 (median 1 3) and for nodularmalignant melanoma the mean was 1 8 (me-dian 1 3). The difference between the valuesfor basal cell carcinoma and malignant mela-noma is significant (p<005). Neither the de-gree of lymphocytic inflammatory response,nor tumour thickness/level, nor ulceration had asignificant effect on the apoptosis:mitosis ratio(data not shown).
Selected cases were studied using in situend-labelling. Cell fragments similar to thosemorphologically resembling apoptotic cellsstained with this technique, which does notstain mitotic cells (fig 3).
DiscussionBoth malignant melanoma and basal cell car-cinoma are tumours in which mitoses may beeasily identified on light microscopy, but whichdisplay a marked disparity in growth rate. Kerrand Searle referred to this as the "paradoxicallyslow growth rate" of basal cell carcinoma andsuggested that the high apoptotic rate, whichthey felt (without numerical quantification) tobe approximately equal to the mitotic rate,might account for this.7Our findings demonstrate that apoptotic cells
oumumber mitotic cells in basal cell carcinoma,with considerable variation in the absolutenumber of apoptotic cells and a cor-respondingly wide range of apoptosis:mitosisratios. By contrast, the melanomas had a similarnumber of mitoses to basal cell carcinoma, buta much smaller number of apoptotic cells andless of a ratio spread. As a simple index ofcell turnover, there is a significant differencebetween the indolent basal cell carcinoma andmore aggressive tumours. Whether there is asignificant difference between superficialspreading and nodular malignant melanomasand whether the apoptosis:mitosis ratio is ofprognostic significance will require assessmentof a larger number of cases and correlationwith clinical behaviour.
Assessment of mitotic figures has long beenused as a prognostic index in certain softtissue tumours, especially leiomyosarcoma.8
on May 11, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.3.242 on 1 March 1995. D
ownloaded from

Mooney, Ruis Peis, O'Neill, Sweeney
Figure 3 In situ end-labelling showing positive staining in an apoptotic cell (arrow) andno staining in an adjacent mitotic figure.
Traditionally, mitoses have been counted perhigh power field (hpf), which is inherently in-accurate being subject to variables such as sizedifference ofmicroscope fields.9 Assessment per
unit area or as a ratio of cells counted is moreaccurate and reproducible. As an index of cellproliferation, mitotic figure counting is perhapsthe easiest first line assessment. However, it isonly a crude reflection of growth fraction as
different tumours may have a delayed cell cycletime giving apparently more mitoses at any one
time. Despite this, mitotic rate alone is ofprognostic value in a certain subset of mela-nomas.'0 Coincident assessment of the numberof apoptotic cells and the formulation of theapoptosis:mitosis ratio provides a figure whichreflects tumour dynamics at the light micro-scopy level and may provide a numerical indexof biological behaviour.Although these cells demonstrate the mor-
phological features of apoptotic cells on lightmicroscopy and display breaks in inter-nucleosomal double stranded DNA with insitu end-labelling, they may not all be theproduct ofprogrammed cell death.4 This, how-ever, does not invalidate the difference notedbetween the two tumour types studied here.As with mitotic figure estimation, counting ofapoptotic bodies is subject to variables such as
rate of clearance and the indeterminate numberof nuclear or cytoplasmic fragments derivedfrom individual cells. As such, assessment ofmitotic and apoptotic indices can only be com-
parative, although proliferating cell nuclear an-
tigen (PCNA) or Ki67 staining should verifyany correlation between mitotic count andgrowth fraction.
It appears from the data that lymphocyticinfiltration (which theoretically might be as-
sociated with a high apoptotic rate) has littleeffect on the apoptosis:mitosis ratio. The dataalso demonstrate that lymphocytes infiltratingtumours were not mistaken for apoptotic cellsto any significant extent. Similarly, althoughulceration of malignant melanoma is an in-dependent prognostic variable," no correlationwith apoptotic cells was found. Assessmentof superficial areas of ulcerated tumours was
performed away from areas of necrotic debristo avoid a falsely high apoptotic count. A slighttrend towards a higher number of apoptoticcells and lower number of mitoses was seen inthe superficial compared with the deep portionof the nodular malignant melanomas, but thesmall number of cases precludes statistical as-sessment (data not shown). Many superficialspreading malignant melanomas were too thinfor superficial and deep areas to be demarcated.No difference was seen between superficial anddeep areas in basal cell carcinomas.
In conclusion, this preliminary study iden-tifies a significant difference in apoptotic:mi-totic ratios between two tumour types, adifference which reflects their clinical be-haviour. The apoptotic index correlates sig-nificantly with prognosis in non-Hodgkin'slymphomas.'2 Although basal cell carcinomamay show a significant variation in growthrate,"3 the principle application of a figure suchas the apoptosis:mitosis ratio would be in malig-nant melanoma, where in certain cases, use ofClark's level or Breslow thickness alone maybe misleading,'4 and where assessment of othervariables such as inflammatory response, re-gression or cell type has produced varying res-ults.15-18
The authors would like to thank J Walker for assistance withphotography.
1 Cotran RS, Kumar V, Robbins SL. Neoplasia. In: CotranRS, Kumar V, Robbins SL, eds. Robbins pathologic basisof disease. 4th edn. Philadelphia: WB Saunders, 1989:239-306.
2 Kerr JFR, Wyllie AH, Currie AR. Apoptosis: a basic bio-logical phenomenon with wide-ranging implications intissue kinetics. BrJ Cancer 1972;26:239-57.
3 Gaverieli Y, Sherman Y, Ben-Sasson SA. Identification ofprogrammed cell death in situ via specific labelling ofnuclear DNA fragmentation. J Cell Biol 1992;119:493-501.
4 Ansari B, Coates PJ, Greenstein BD, Hall PA. In situ end-labelling detects DNA strand breaks in apoptosis andother physiological and pathological states. J Pathol 1993;170:1-8.
5 Breslow A. Thickness, cross-sectional areas and depth ofinvasion in the prognosis of cutaneous melanoma. AnnSurg 1970;172:902-8.
6 Clark WH, From L, Bernardino EA, Mihm MC. Thehistogenesis and biologic behaviour of primary humanmalignant melanomas of the skin. Cancer Res 1969;29:705-26.
7 Kerr JFR, Searle J. A suggested explanation for the para-doxically slow growth rate of basal-cell carcinomas thatcontain numerous mitotic figures. JPathol 1972;107:41-4.
8 Enzinger FM, Weiss SW. Chapter 1. In: Soft tissue tumours.2nd edn. St Louis: CV Mosby Co., 1988:1-19.
9 Ellis PSJ, Whitehead R. Mitosis counting-a need forreappraisal. Hum Pathol 1981;12:3-4.
10 Schmoeckel C, Braun-Falco 0. Prognostic index in malig-nant melanoma. Arch Dermatol 1978;114:871-3.
11 Rosai J. Skin: Tumours and tumour-like conditions. In:Rosai J, ed. Ackerman's surgical pathology. 7th edn. StLouis: CV Mosby Co., 1989:88-172.
12 Leoncini L, Del Vecchio MT, Megha T, Barbini P, GalieniP, Pileri S, et al. Correlations between apoptotic andproliferative indices in malignant non-Hodgkin's lymph-omas. Am J Pathol 1993;142:755-63.
13 Jacobs GH, Rippey JJ, Altini M. Prediction of aggressivebehaviour in BCC. Cancer 1982;49:533-7.
14 Green MS, Ackerman AB. Thickness is not an accurategauge of prognosis of primary cutaneous melanoma. AmJ Dermatopathol 1993;15:461-73.
15 Van der Esch EP, Cascinelli N, Preda F, Morabito A,Bufalino R. Stage 1 melanoma of the skin: Evaluation ofprognosis according to histological characteristics. Cancer1981;48: 1668-73.
16 Clark WH, Elder DE, Guerry D, Braitman LE, Trock BJ,Schultz D, et al. Model predicting survival in stage 1melanoma based on tumour progression. 7 Natl CancerInst 1989;81:1893-904.
17 Gromet MA, Epstein WL, Blois MS. The regressing thinmalignant melanoma. A distinctive lesion with metastaticpotential. Cancer 1978;42:2282-92.
18 McGovern VJ, Shaw HM, Milton GW. Prognosis in patientswith thin malignant melanoma: influence of regression.Histopathology 1983;7:673-80.
244
on May 11, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.3.242 on 1 March 1995. D
ownloaded from



![Clinical Laboratory Technology - Central Georgia … · 2017-07-06 · CLINICAL LABORATORY TECHNOLOGY LIBRARY RESOURCES ... Atlas of Pathology, 2nd ed. [Robbins and Cotran] / E. Klatt](https://img.pdfslide.net/doc/110x75/5b1fa63e7f8b9a411d8b4a4e/clinical-laboratory-technology-central-georgia-2017-07-06-clinical-laboratory.jpg)