Embed Size (px)
Citation preview
Clinical Anatomy of Pelvic
Peritoneum and Fascia Associate Professor
Dr. A. Podcheko2015
2
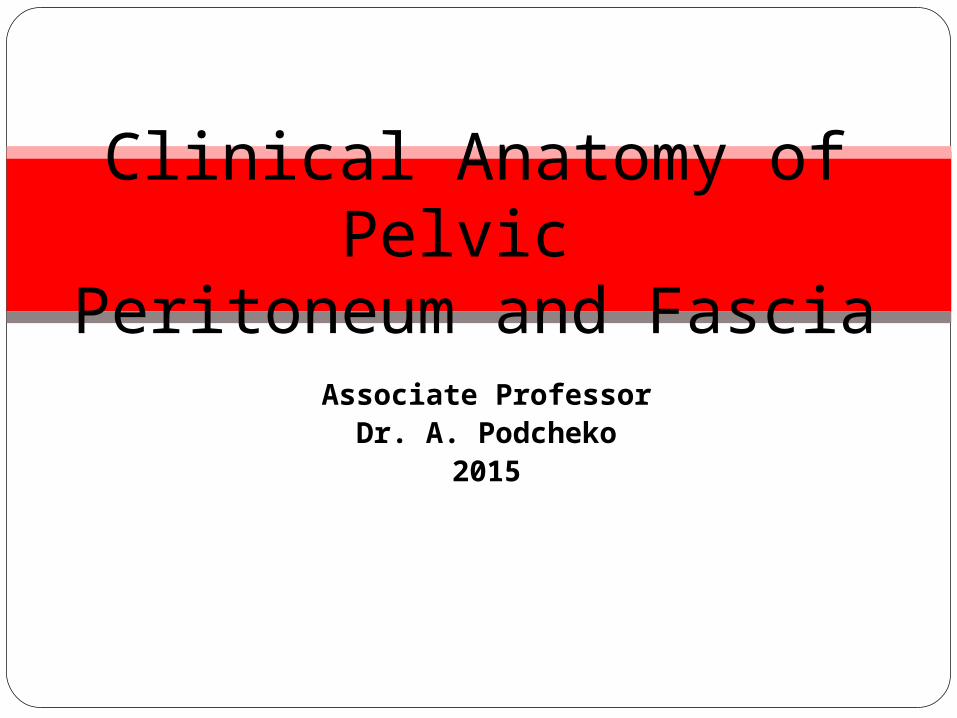
1 . Iliac crest
2. Gas bubble in colon
3. Ala of ilium
4. Lateral part of sacrum
5. Sacroiliac joint
6. Posterior inferior iliac spine
7. Anterior superior iliac spine
8. Anterior inferior iliac spine
9. Lunate surface of acetabulum
10. Spine of ischium
14. Ischial tuberosity
15. Superior ramus of pubis
16. Symphysis pubis
17. Inferior ramus of pubis
18. Obturator foramen
Review- Pelvis
24. 25. 26. 27.
1 .
2.
3.
4.
5.
6.
7.
8.
9.
10.
14.
15.
16.
17.
18. 24. Greater sciatic notch25. Transverse process, L5
Vertebra26. Gas bubble in colon27. Urinary bladder
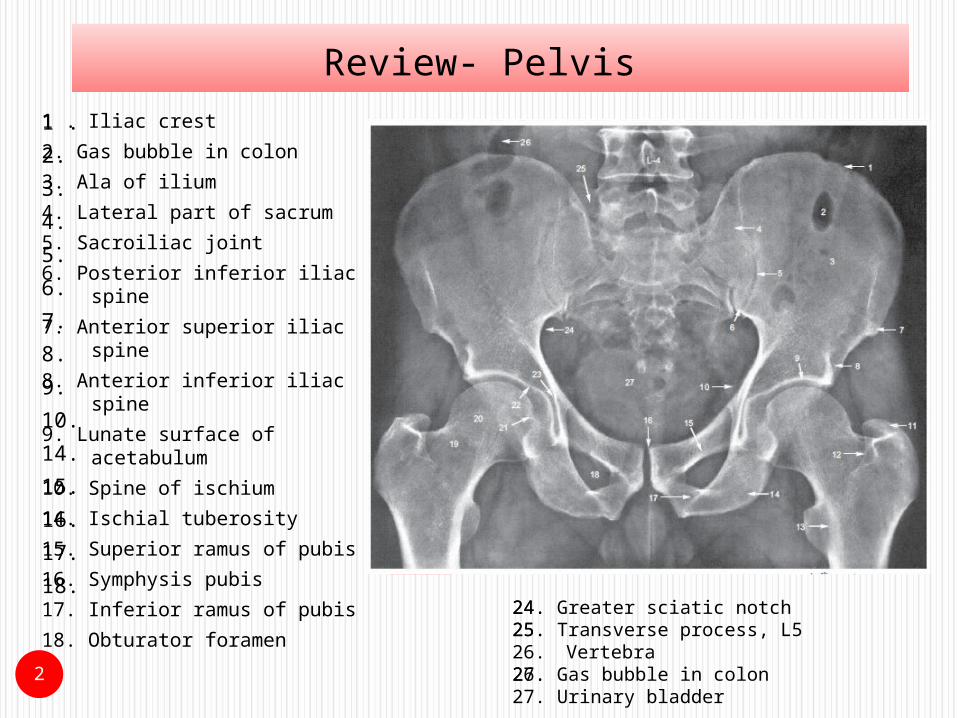
Pelvic Cavity The pelvic cavity contains
the terminal parts of the ureters and the urinary bladder,
rectum, pelvic genital organs, blood vessels, lymphatics,
and nerves. loops of small intestine
(mainly ileum) frequently, large intestine
(appendix and transverse and/or sigmoid colon).
3
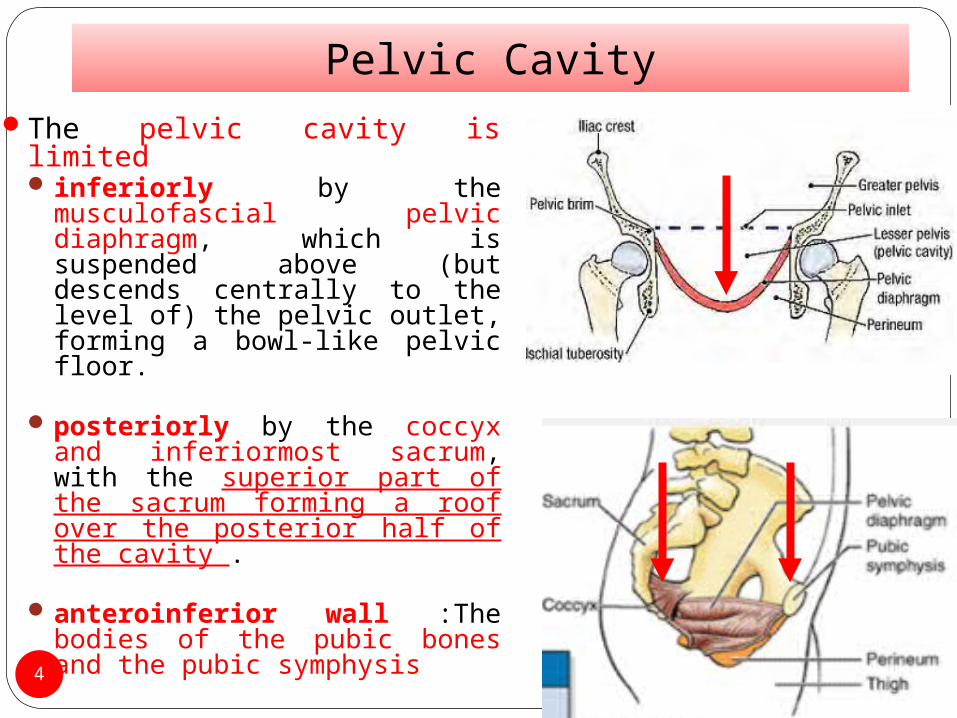
Pelvic CavityThe pelvic cavity is limited
inferiorly by the musculofascial pelvic diaphragm, which is suspended above (but descends centrally to the level of) the pelvic outlet, forming a bowl-like pelvic floor.
posteriorly by the coccyx and inferiormost sacrum, with the superior part of the sacrum forming a roof over the posterior half of the cavity .
anteroinferior wall :The bodies of the pubic bones and the pubic symphysis4
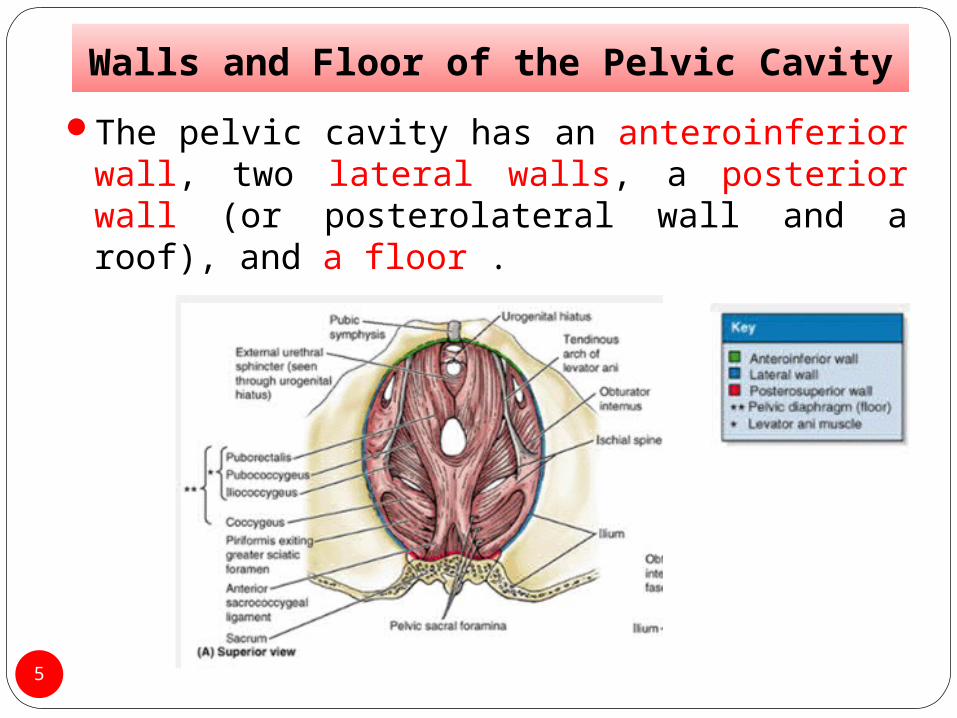
Walls and Floor of the Pelvic Cavity
The pelvic cavity has an anteroinferior wall, two lateral walls, a posterior wall (or posterolateral wall and a roof), and a floor .
5
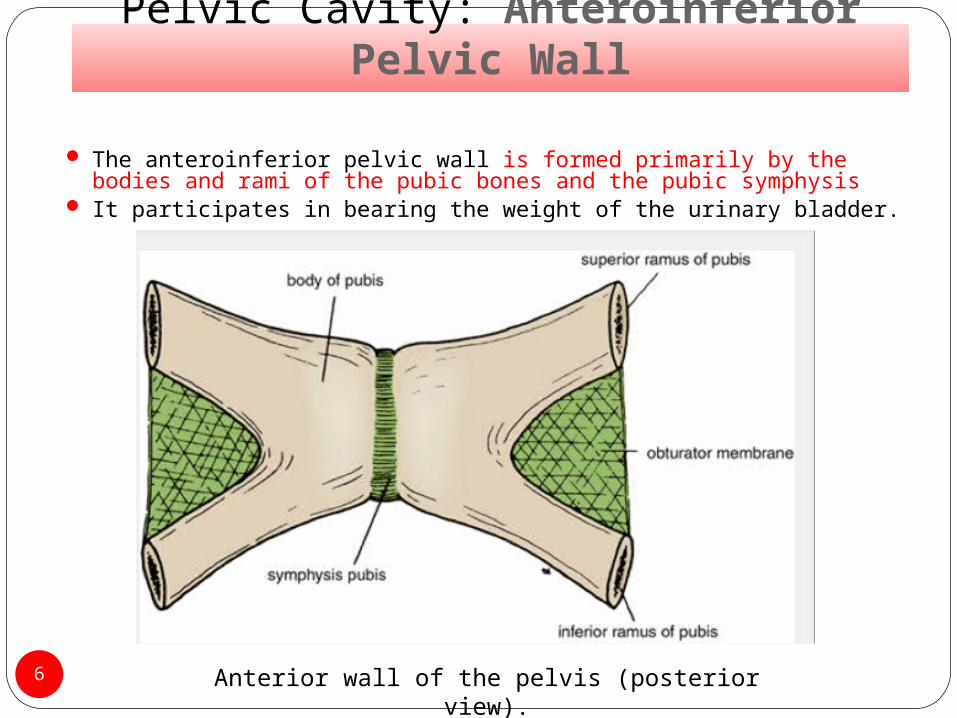
Pelvic Cavity: Anteroinferior Pelvic Wall
The anteroinferior pelvic wall is formed primarily by the bodies and rami of the pubic bones and the pubic symphysis
It participates in bearing the weight of the urinary bladder.
6 Anterior wall of the pelvis (posterior view).
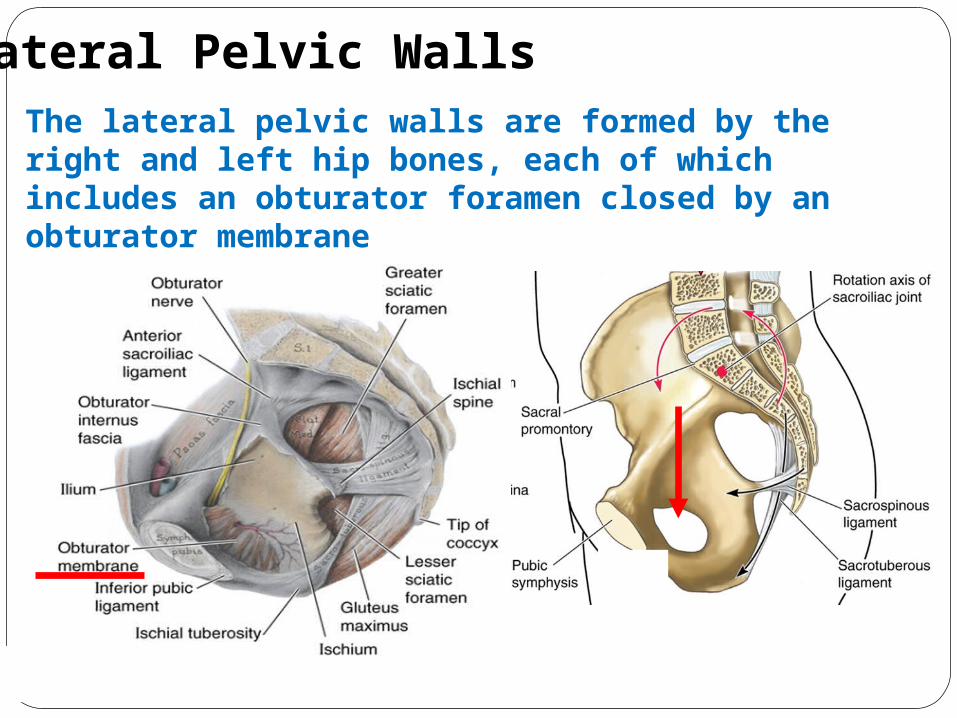
Lateral Pelvic WallsThe lateral pelvic walls are formed by the right and left hip bones, each of which includes an obturator foramen closed by an obturator membrane
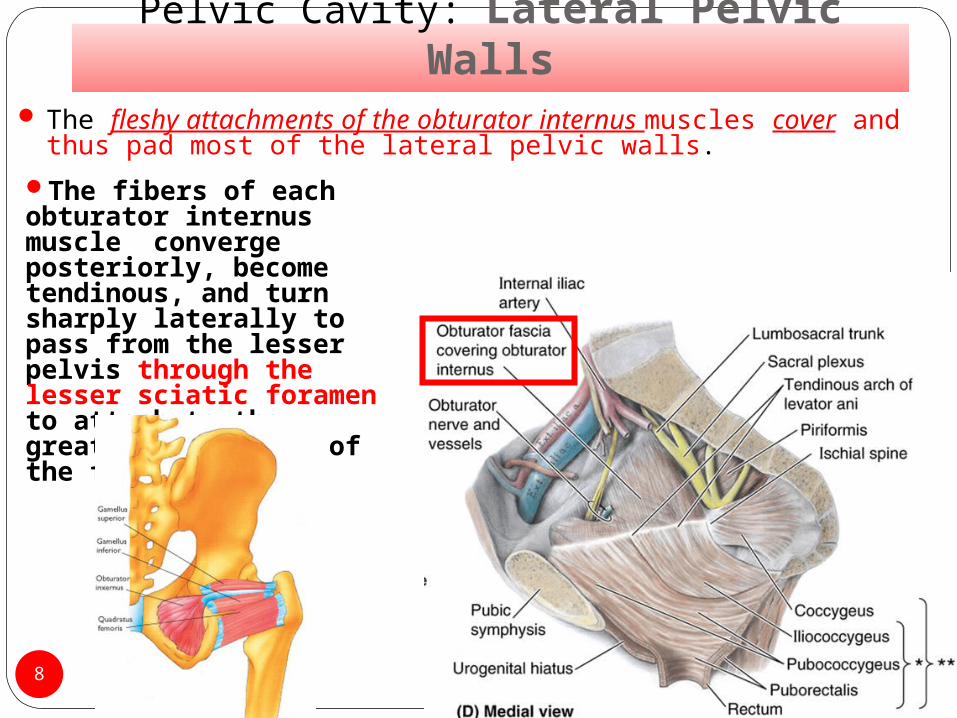
Pelvic Cavity: Lateral Pelvic Walls The fleshy attachments of the obturator internus muscles
cover and thus pad most of the lateral pelvic walls.
8
The fibers of each obturator internus muscle converge posteriorly, become tendinous, and turn sharply laterally to pass from the lesser pelvis through the lesser sciatic foramen to attach to the greater trochanter of the femur
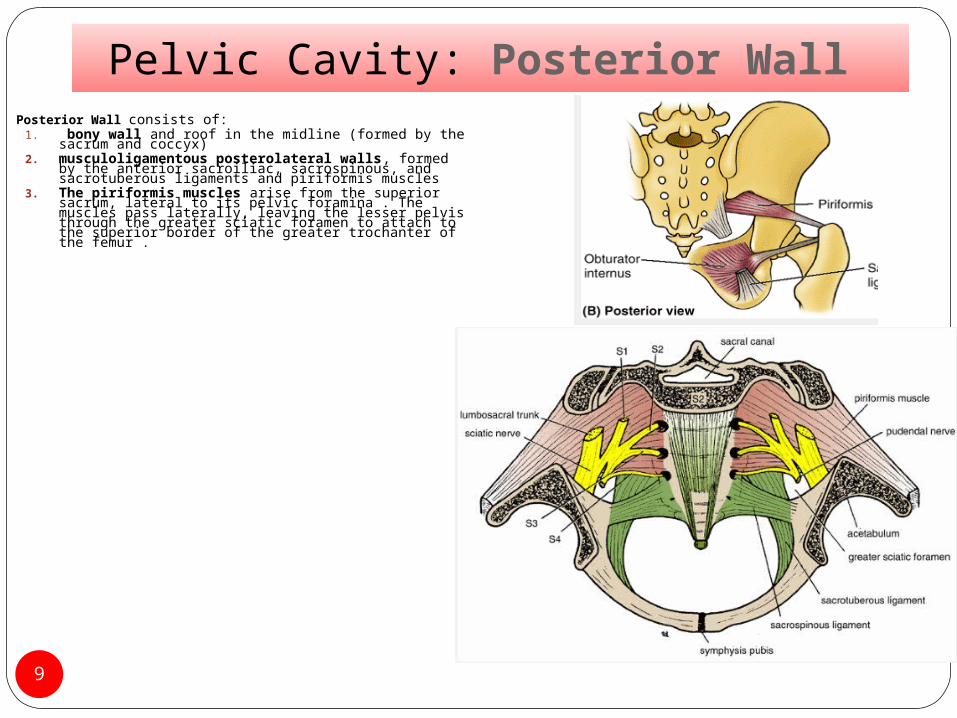
Pelvic Cavity: Posterior Wall Posterior Wall consists of:
1. bony wall and roof in the midline (formed by the sacrum and coccyx)
2. musculoligamentous posterolateral walls, formed by the anterior sacroiliac, sacrospinous, and sacrotuberous ligaments and piriformis muscles
3. The piriformis muscles arise from the superior sacrum, lateral to its pelvic foramina . The muscles pass laterally, leaving the lesser pelvis through the greater sciatic foramen to attach to the superior border of the greater trochanter of the femur .
9
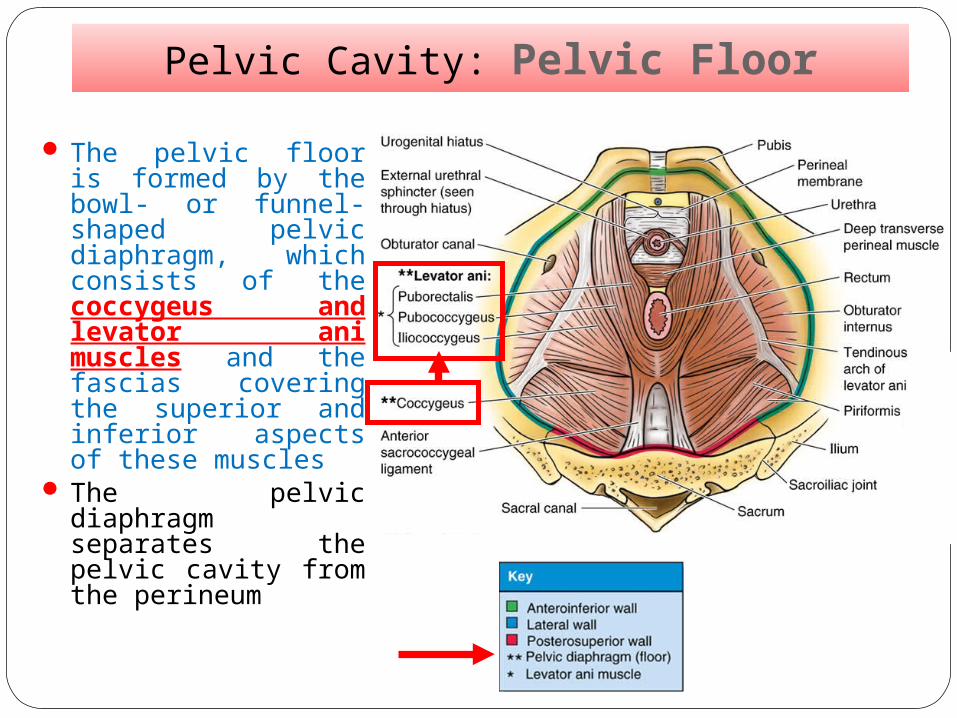
Pelvic Cavity: Pelvic Floor
The pelvic floor is formed by the bowl- or funnel-shaped pelvic diaphragm, which consists of the coccygeus and levator ani muscles and the fascias covering the superior and inferior aspects of these muscles
The pelvic diaphragm separates the pelvic cavity from the perineum
Relationships between Peritoneum and Peritoneal Cavity of the Pelvis
11
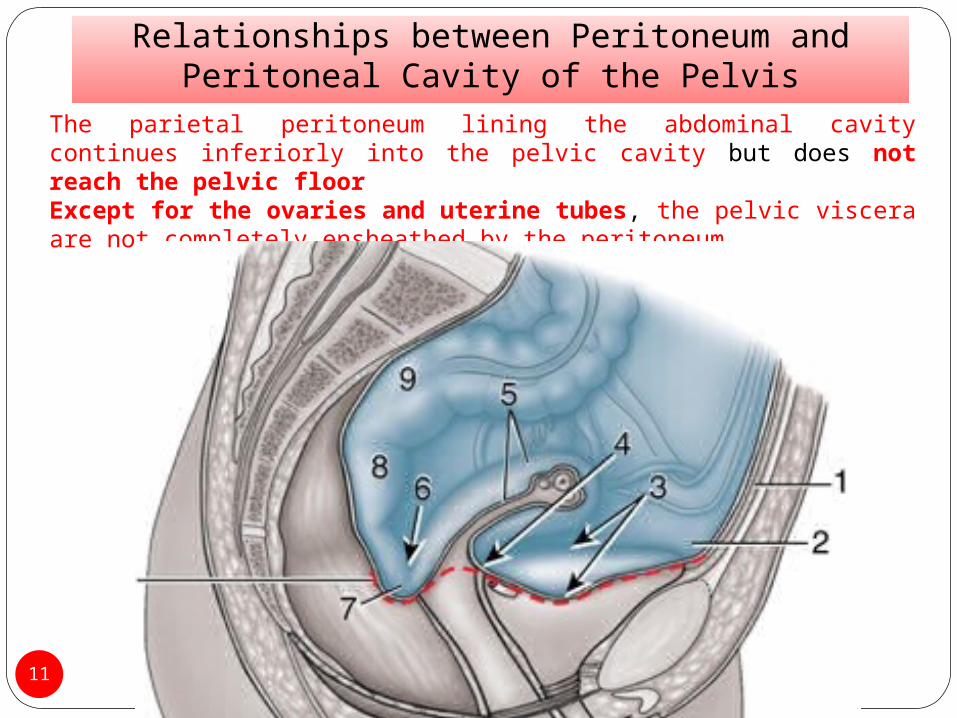
The parietal peritoneum lining the abdominal cavity continues inferiorly into the pelvic cavity but does not reach the pelvic floorExcept for the ovaries and uterine tubes, the pelvic viscera are not completely ensheathed by the peritoneum.
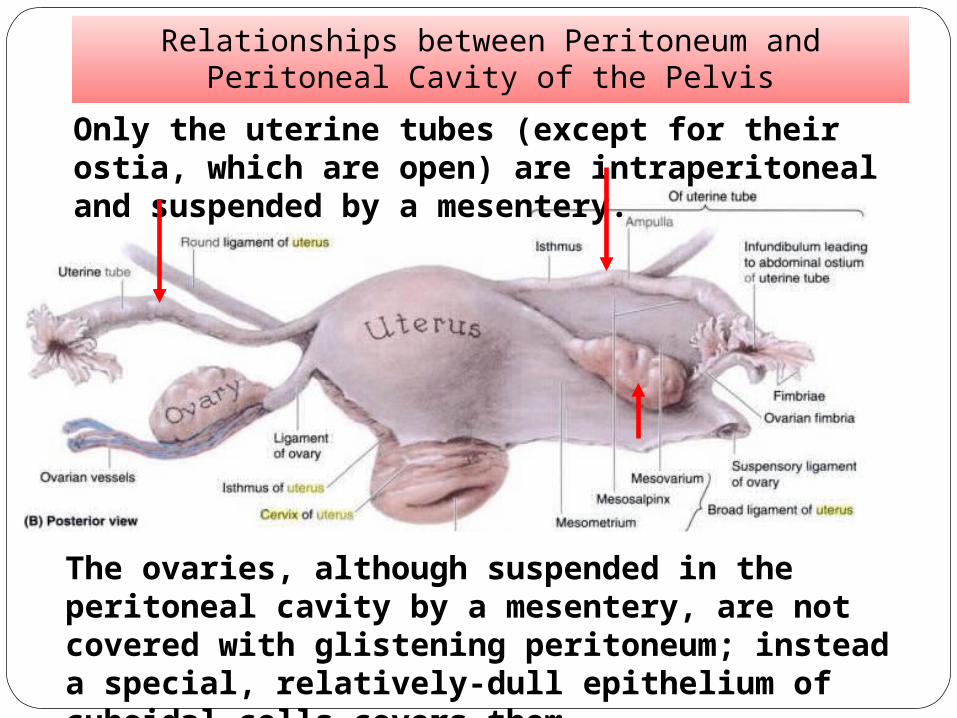
Only the uterine tubes (except for their ostia, which are open) are intraperitoneal and suspended by a mesentery.
The ovaries, although suspended in the peritoneal cavity by a mesentery, are not covered with glistening peritoneum; instead a special, relatively-dull epithelium of cuboidal cells covers them.
Relationships between Peritoneum and Peritoneal Cavity of the Pelvis
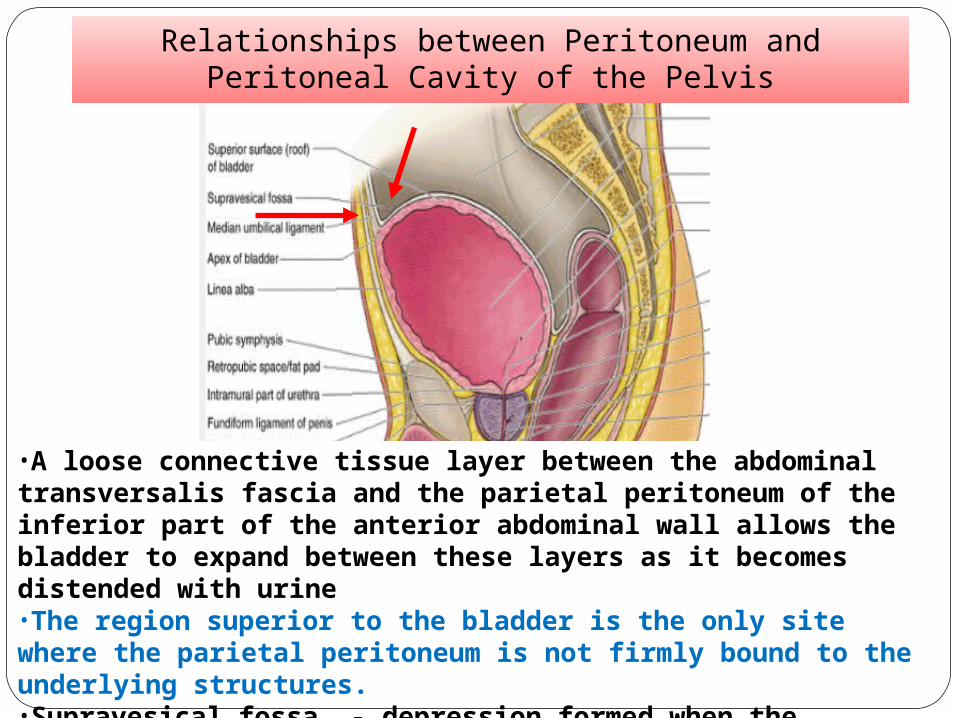
•A loose connective tissue layer between the abdominal transversalis fascia and the parietal peritoneum of the inferior part of the anterior abdominal wall allows the bladder to expand between these layers as it becomes distended with urine•The region superior to the bladder is the only site where the parietal peritoneum is not firmly bound to the underlying structures. •Supravesical fossa - depression formed when the peritoneum reflects onto the superior surface of the bladder
Relationships between Peritoneum and Peritoneal Cavity of the Pelvis
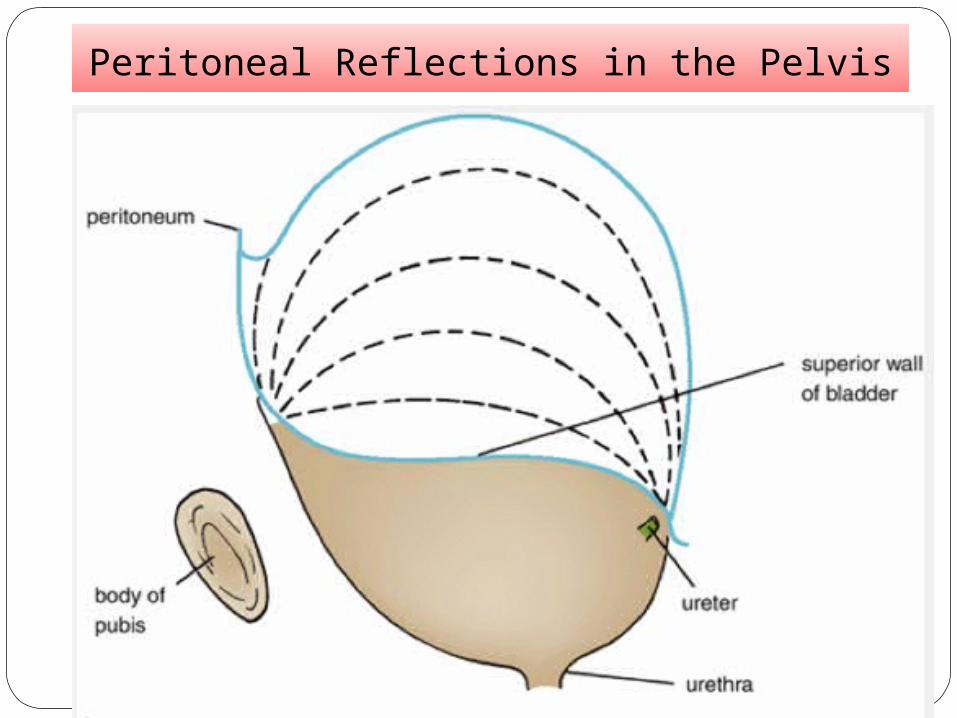
Peritoneal Reflections in the Pelvis
Peritoneal Reflections in the Pelvis:Female
15
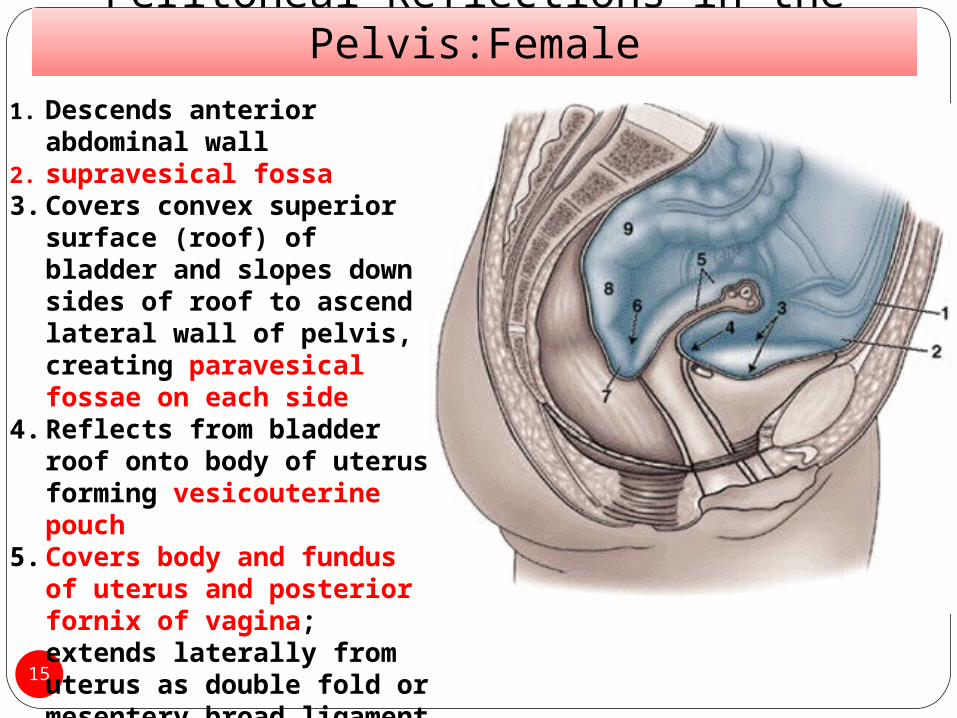
1. Descends anterior abdominal wall
2. supravesical fossa3. Covers convex superior
surface (roof) of bladder and slopes down sides of roof to ascend lateral wall of pelvis, creating paravesical fossae on each side
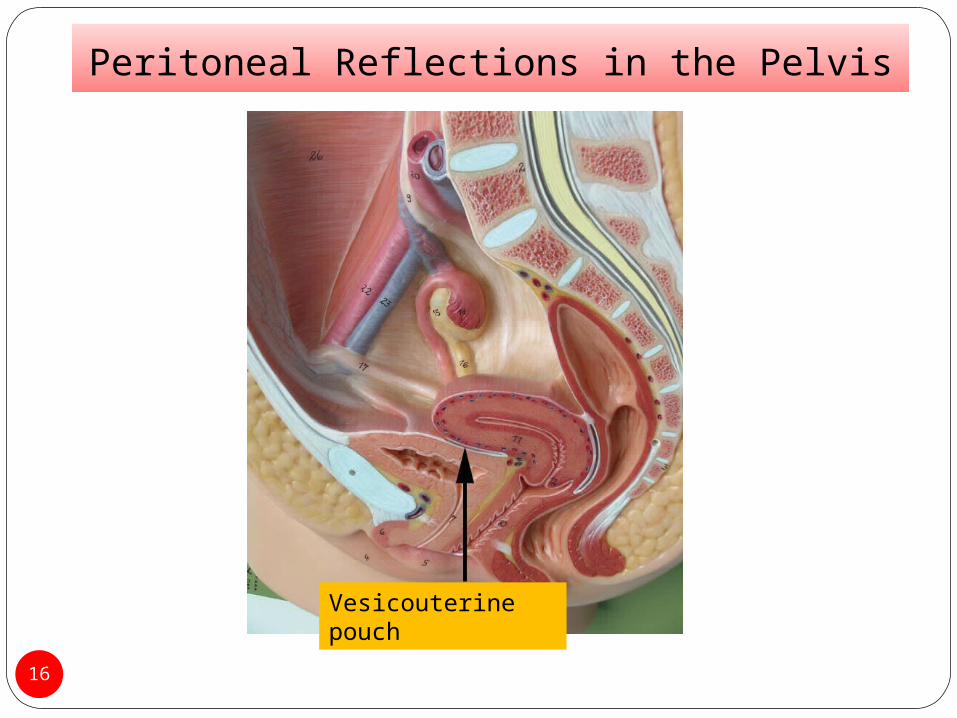
4. Reflects from bladder roof onto body of uterus forming vesicouterine pouch
5. Covers body and fundus of uterus and posterior fornix of vagina; extends laterally from uterus as double fold or mesentery broad ligament that engulfs uterine tubes, ovaries, and round ligaments of uterus
16
Peritoneal Reflections in the Pelvis
Vesicouterine pouch
Peritoneal Reflections in the Pelvis:Female
17
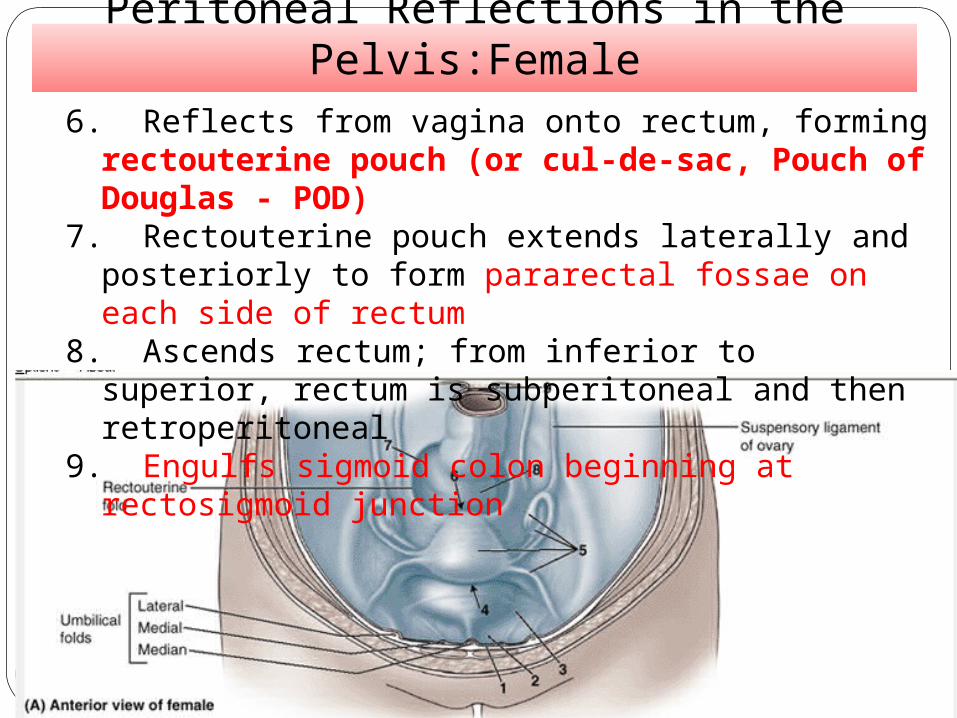
6. Reflects from vagina onto rectum, forming rectouterine pouch (or cul-de-sac, Pouch of Douglas - POD)
7. Rectouterine pouch extends laterally and posteriorly to form pararectal fossae on each side of rectum
8. Ascends rectum; from inferior to superior, rectum is subperitoneal and then retroperitoneal
9. Engulfs sigmoid colon beginning at rectosigmoid junction
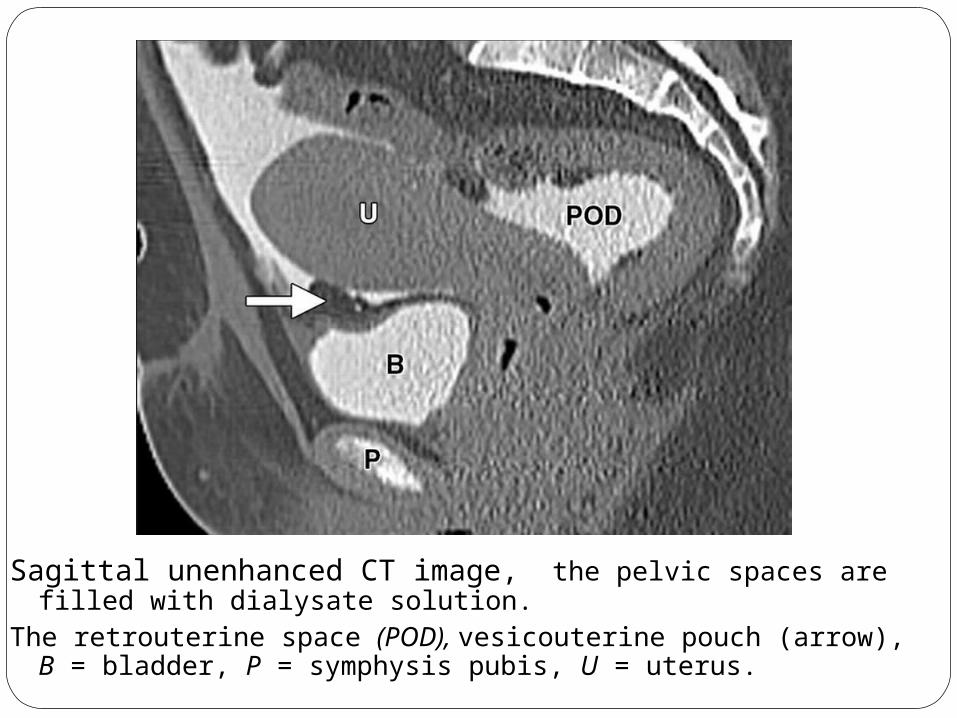
Sagittal unenhanced CT image, the pelvic spaces are filled with dialysate solution.
The retrouterine space (POD), vesicouterine pouch (arrow), B = bladder, P = symphysis pubis, U = uterus.
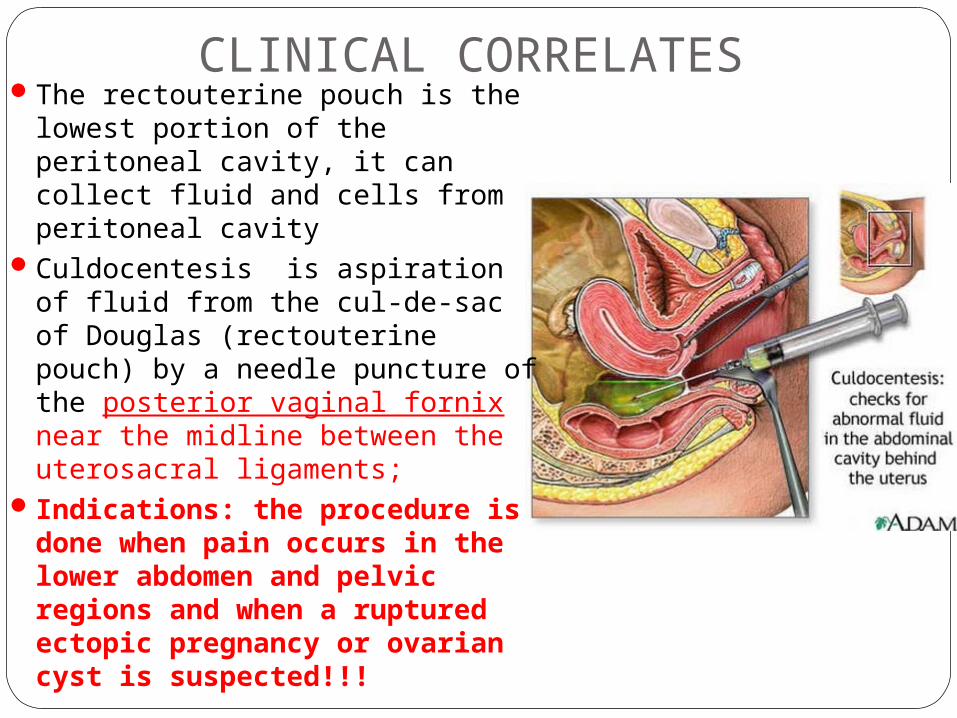
CLINICAL CORRELATESThe rectouterine pouch is the
lowest portion of the peritoneal cavity, it can collect fluid and cells from peritoneal cavity
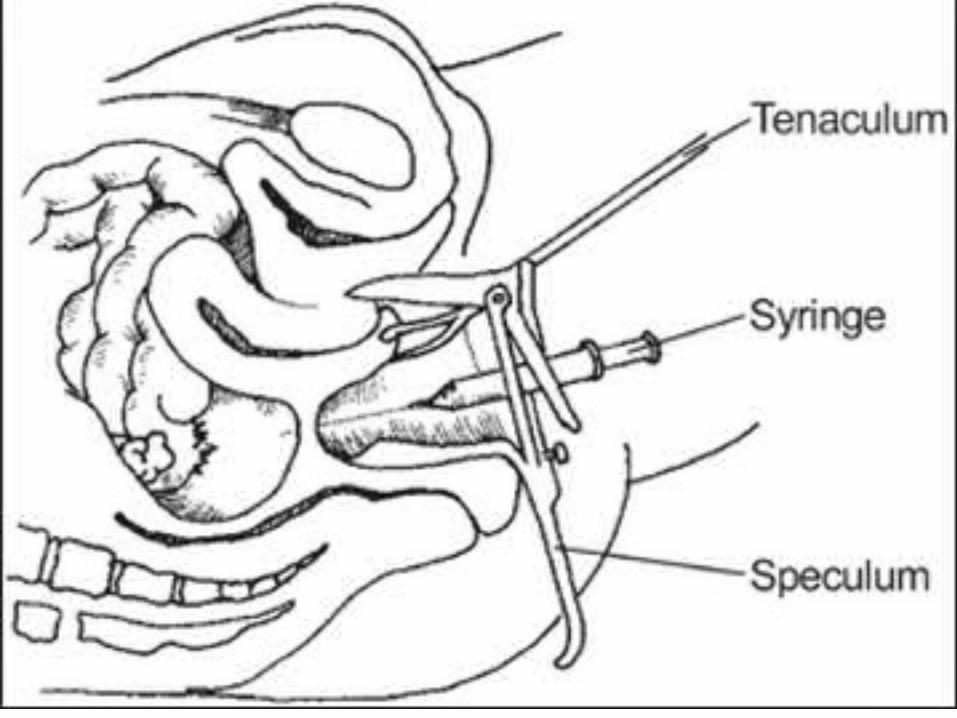
Culdocentesis is aspiration of fluid from the cul-de-sac of Douglas (rectouterine pouch) by a needle puncture of the posterior vaginal fornix near the midline between the uterosacral ligaments;
Indications: the procedure is done when pain occurs in the lower abdomen and pelvic regions and when a ruptured ectopic pregnancy or ovarian cyst is suspected!!!
A 29-year-old woman with a ruptured ectopic pregnancy is admitted to a hospital for culdocentesis. A long needle on the syringe is most efficiently inserted through which of the following structures?(A) Anterior fornix of the vagina(B) Posterior fornix of the vagina(C) Anterior wall of the rectum(D) Posterior wall of the uterine body(E) Posterior wall of the bladder
Peritoneal Reflections in the Pelvis: Female
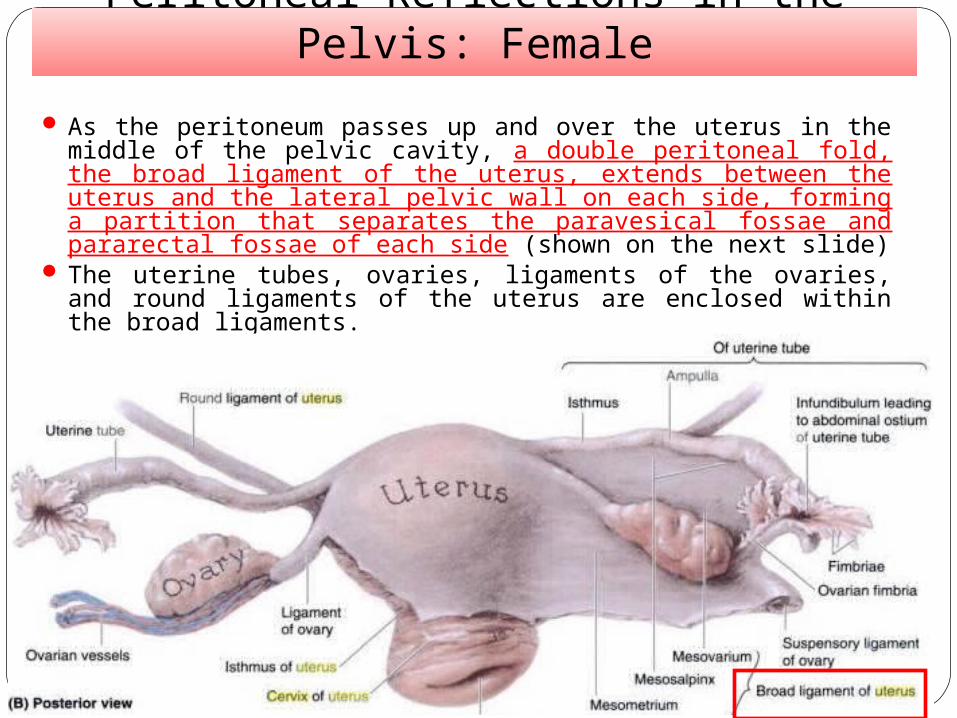
As the peritoneum passes up and over the uterus in the middle of the pelvic cavity, a double peritoneal fold, the broad ligament of the uterus, extends between the uterus and the lateral pelvic wall on each side, forming a partition that separates the paravesical fossae and pararectal fossae of each side (shown on the next slide)
The uterine tubes, ovaries, ligaments of the ovaries, and round ligaments of the uterus are enclosed within the broad ligaments.
BROAD LIGAMENT CONTENTB Bundle (ovarian neurovascular bundle)R Round ligamentO Ovarian ligamentA Artefacts (Vestigial Structures)Duct (Oviduct – Uterine tube)
A 53-year-old bank teller is admitted to alocal hospital for surgical removal of abenign pelvic tumor confined within thebroad ligament. There is a risk of injuringwhich of the following structures that lies inthis ligament?(A) Ovary(B) Proximal part of the pelvic ureter(C) Terminal part of the round ligament ofthe uterus(D) Uterine tube(E) Suspensory ligament of the ovary
The answer is D. The uterine tubes lie in the broad ligament.
The anterior surface of the ovary is attached to the posterior surface of the broad ligament of the uterus. The ureter descends retroperitoneally on the lateral pelvic wall but is crossed by the uterine artery in
the base (in the inferomedial part) of the broad ligament.
The terminal part of the round ligament of the uterus becomes lost in the subcutaneous tissue of the labium majora.
The suspensory ligament of the ovary is a band of peritoneum that extends superiorly from the
ovary to the pelvic wall.
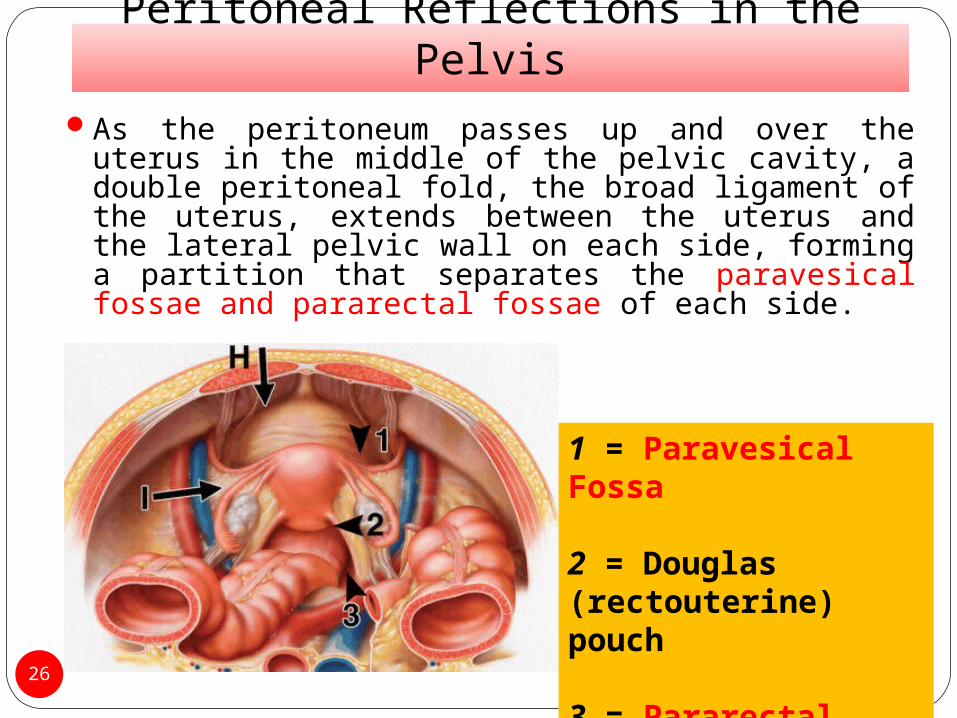
Peritoneal Reflections in the PelvisAs the peritoneum passes up and over the uterus
in the middle of the pelvic cavity, a double peritoneal fold, the broad ligament of the uterus, extends between the uterus and the lateral pelvic wall on each side, forming a partition that separates the paravesical fossae and pararectal fossae of each side.
26
1 = Paravesical Fossa
2 = Douglas (rectouterine) pouch
3 = Pararectal fossa
Peritoneal Reflections in the Pelvis: Males
27
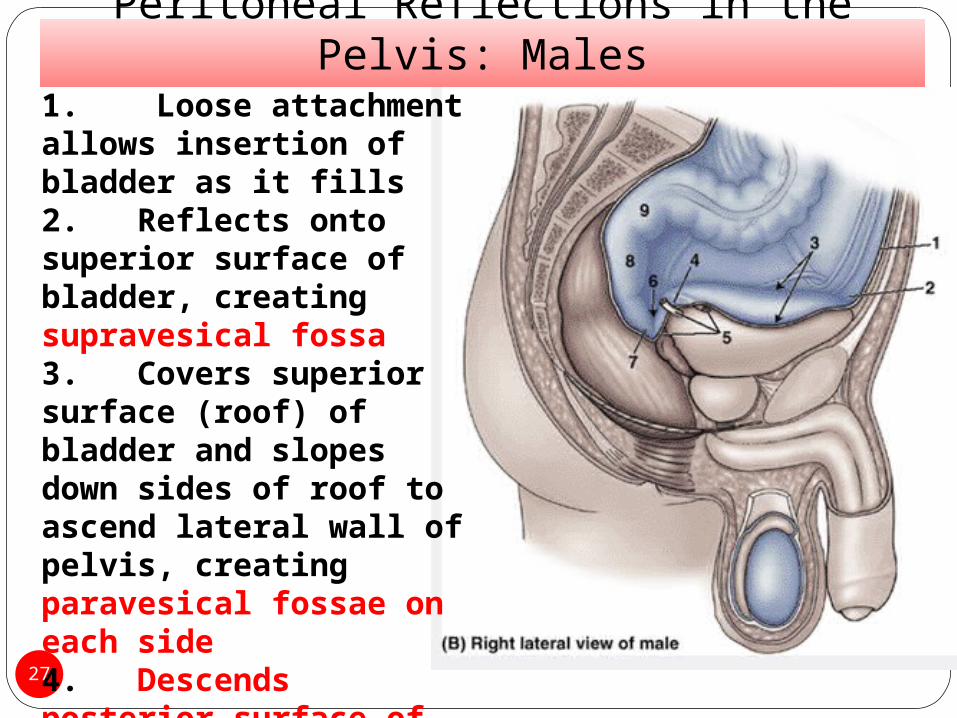
1. Loose attachment allows insertion of bladder as it fills2.Reflects onto superior surface of bladder, creating supravesical fossa3.Covers superior surface (roof) of bladder and slopes down sides of roof to ascend lateral wall of pelvis, creating paravesical fossae on each side4.Descends posterior surface of bladder as much as 2 cm
Peritoneal Reflections in the Pelvis: Males
28
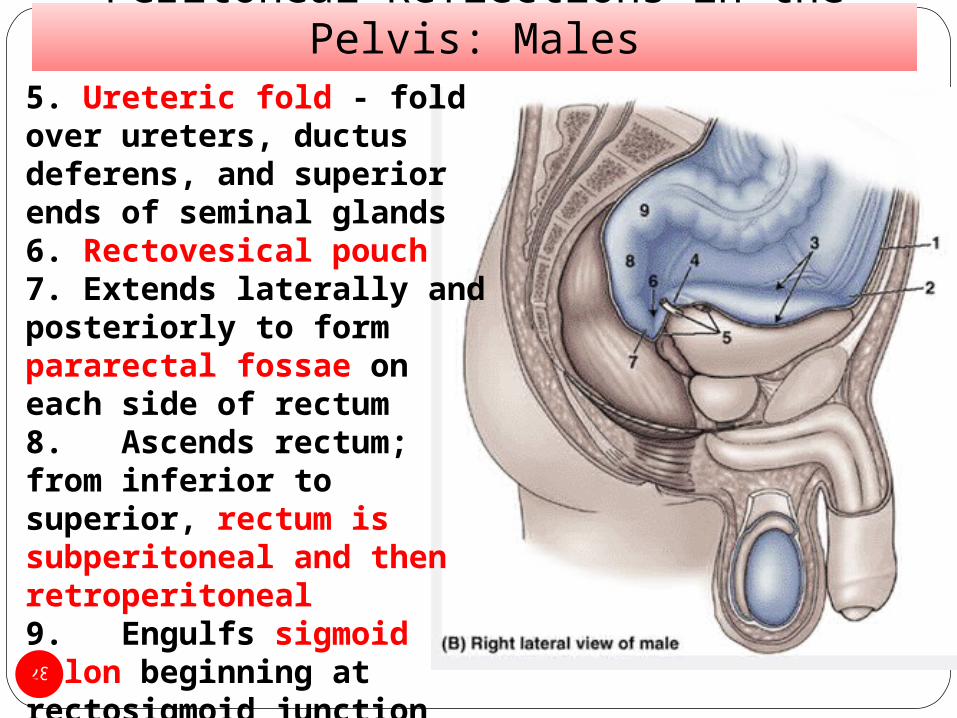
5. Ureteric fold - fold over ureters, ductus deferens, and superior ends of seminal glands6. Rectovesical pouch7. Extends laterally and posteriorly to form pararectal fossae on each side of rectum8.Ascends rectum; from inferior to superior, rectum is subperitoneal and then retroperitoneal9.Engulfs sigmoid colon beginning at rectosigmoid junction
Peritoneal Reflections in the Pelvis:Male
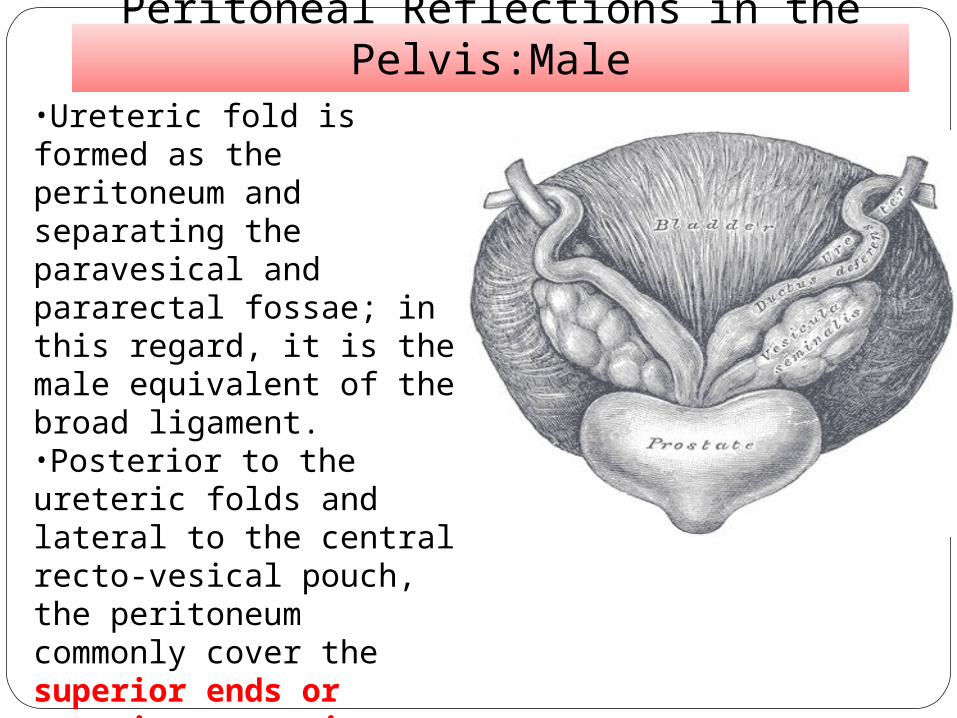
•Ureteric fold is formed as the peritoneum and separating the paravesical and pararectal fossae; in this regard, it is the male equivalent of the broad ligament. •Posterior to the ureteric folds and lateral to the central recto-vesical pouch, the peritoneum commonly cover the superior ends or superior posterior surfaces of the seminal glands (vesicles) and ampullae of the ductus deferens
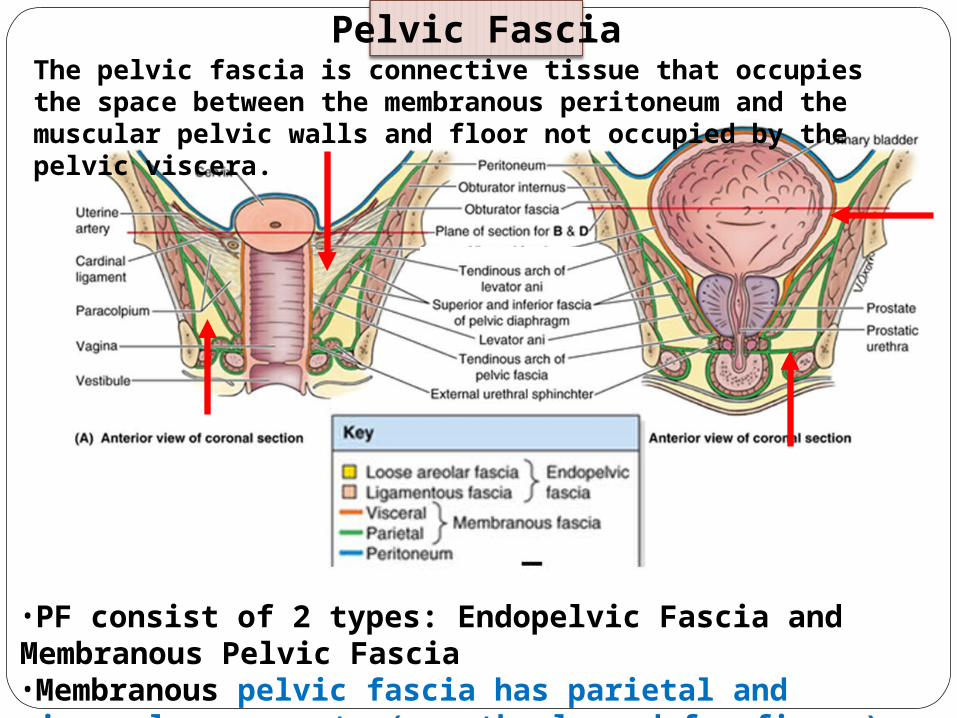
•PF consist of 2 types: Endopelvic Fascia and Membranous Pelvic Fascia •Membranous pelvic fascia has parietal and visceral components (see the legend for figure).
Pelvic FasciaThe pelvic fascia is connective tissue that occupies the space between the membranous peritoneum and the muscular pelvic walls and floor not occupied by the pelvic viscera.
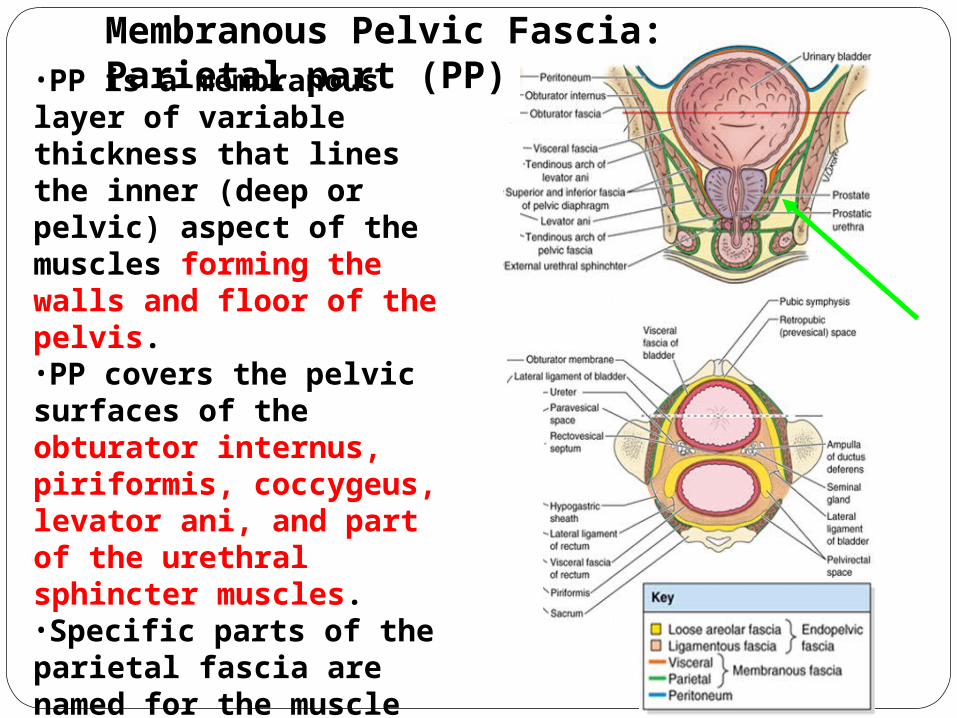
•PP is a membranous layer of variable thickness that lines the inner (deep or pelvic) aspect of the muscles forming the walls and floor of the pelvis.•PP covers the pelvic surfaces of the obturator internus, piriformis, coccygeus, levator ani, and part of the urethral sphincter muscles. •Specific parts of the parietal fascia are named for the muscle they cover (e.g., obturator fascia)
Membranous Pelvic Fascia: Parietal part (PP)
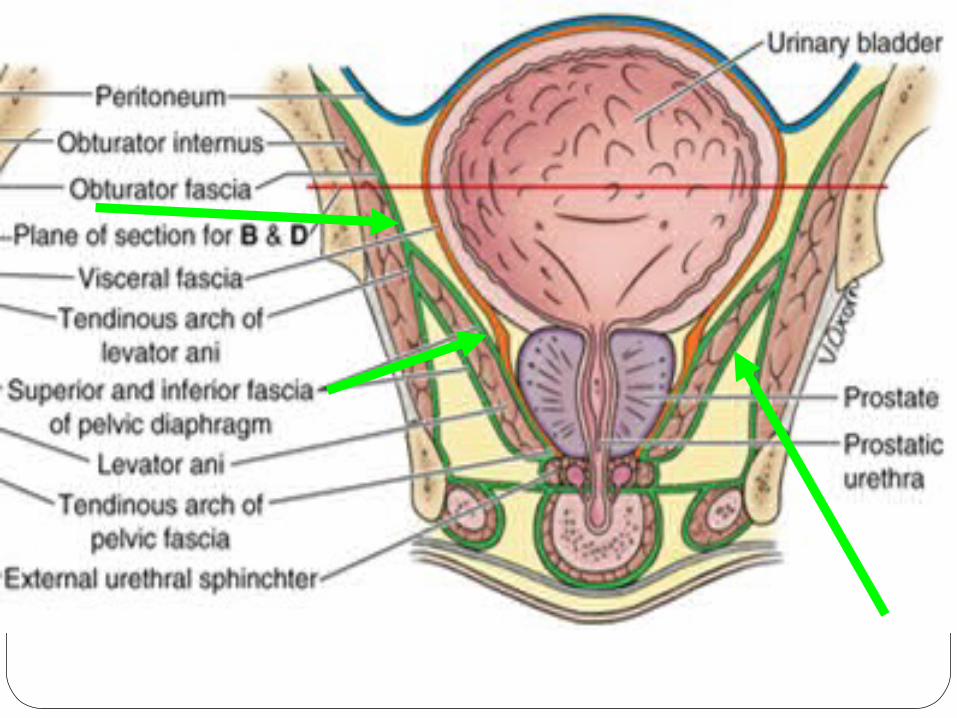
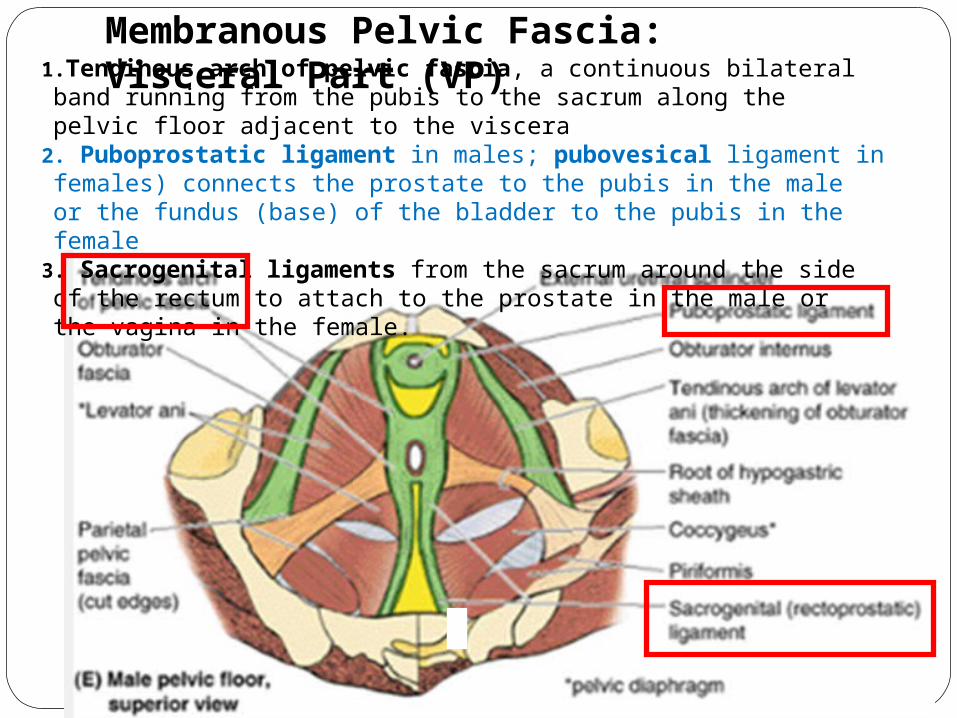
1.Tendinous arch of pelvic fascia, a continuous bilateral band running from the pubis to the sacrum along the pelvic floor adjacent to the viscera
2. Puboprostatic ligament in males; pubovesical ligament in females) connects the prostate to the pubis in the male or the fundus (base) of the bladder to the pubis in the female
3. Sacrogenital ligaments from the sacrum around the side of the rectum to attach to the prostate in the male or the vagina in the female.
Membranous Pelvic Fascia: Visceral Part (VP)
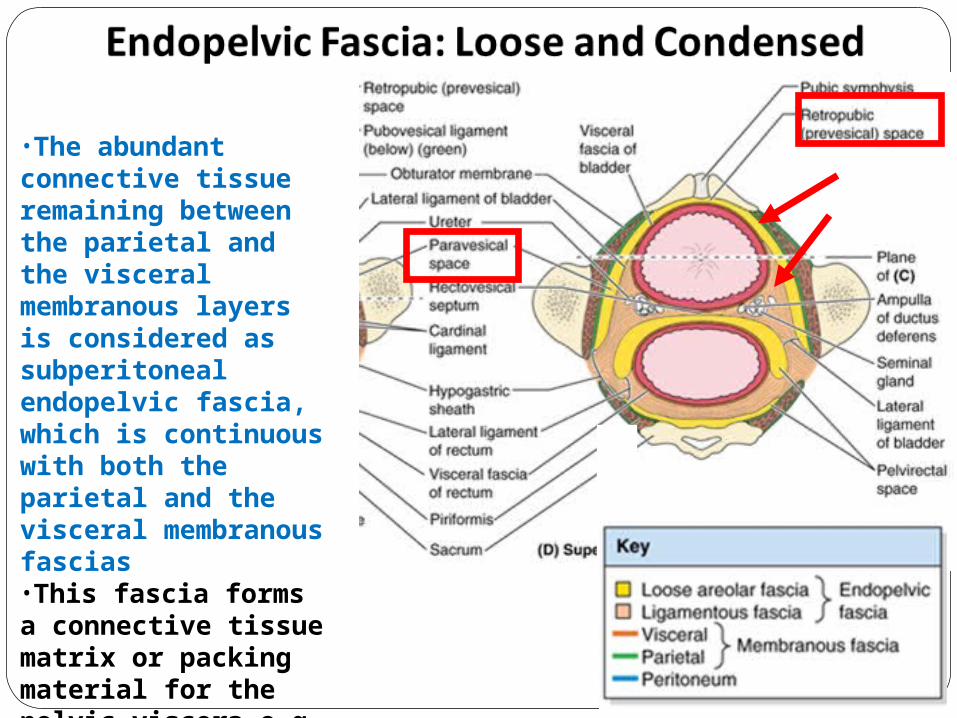
•The abundant connective tissue remaining between the parietal and the visceral membranous layers is considered as subperitoneal endopelvic fascia, which is continuous with both the parietal and the visceral membranous fascias•This fascia forms a connective tissue matrix or packing material for the pelvic viscera e.g paravesical space, retropubic space
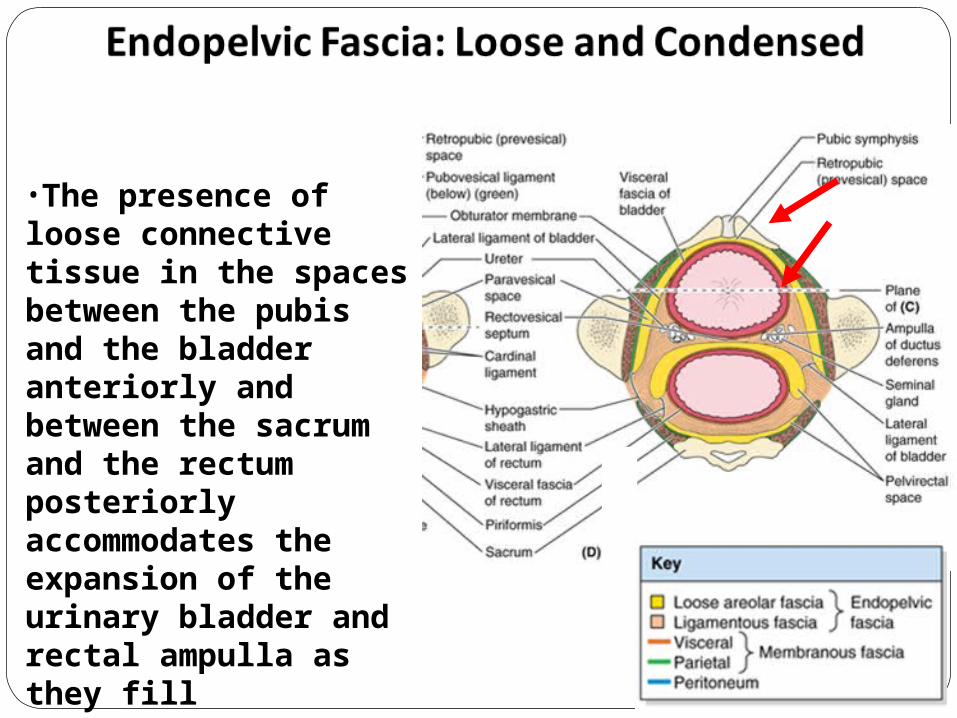
•The presence of loose connective tissue in the spaces between the pubis and the bladder anteriorly and between the sacrum and the rectum posteriorly accommodates the expansion of the urinary bladder and rectal ampulla as they fill
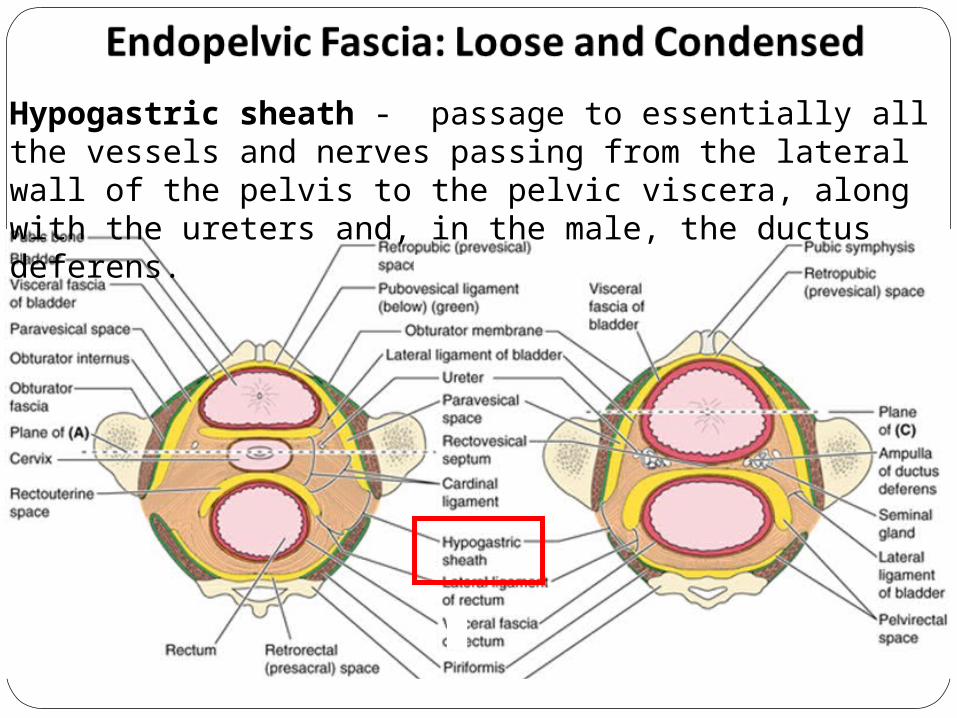
Hypogastric sheath - passage to essentially all the vessels and nerves passing from the lateral wall of the pelvis to the pelvic viscera, along with the ureters and, in the male, the ductus deferens.
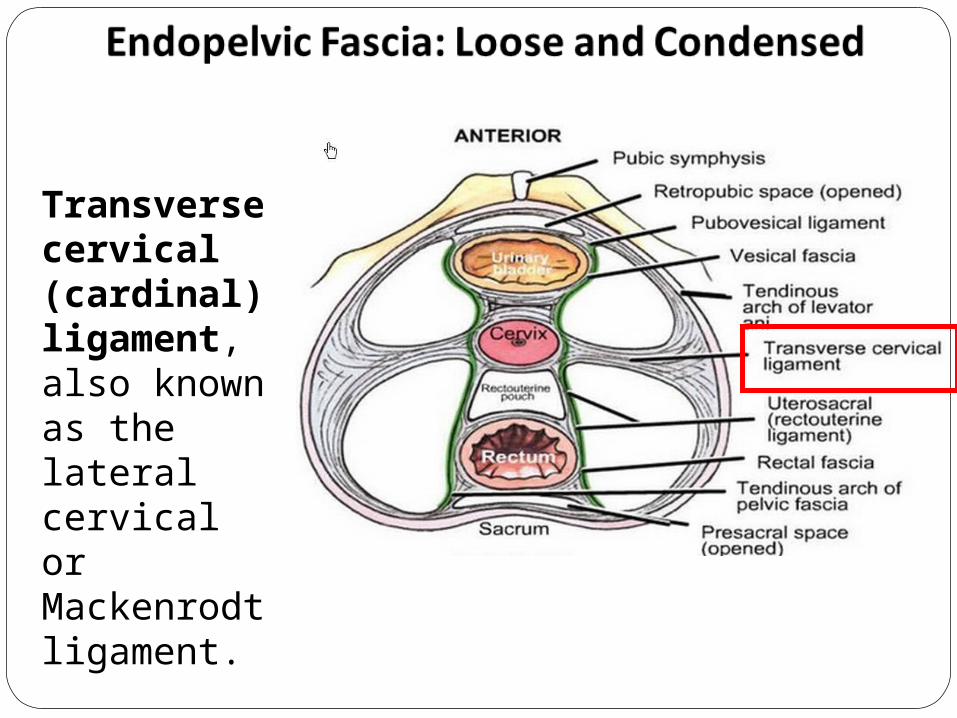
Transverse cervical (cardinal) ligament, also known as the lateral cervical or Mackenrodt ligament.
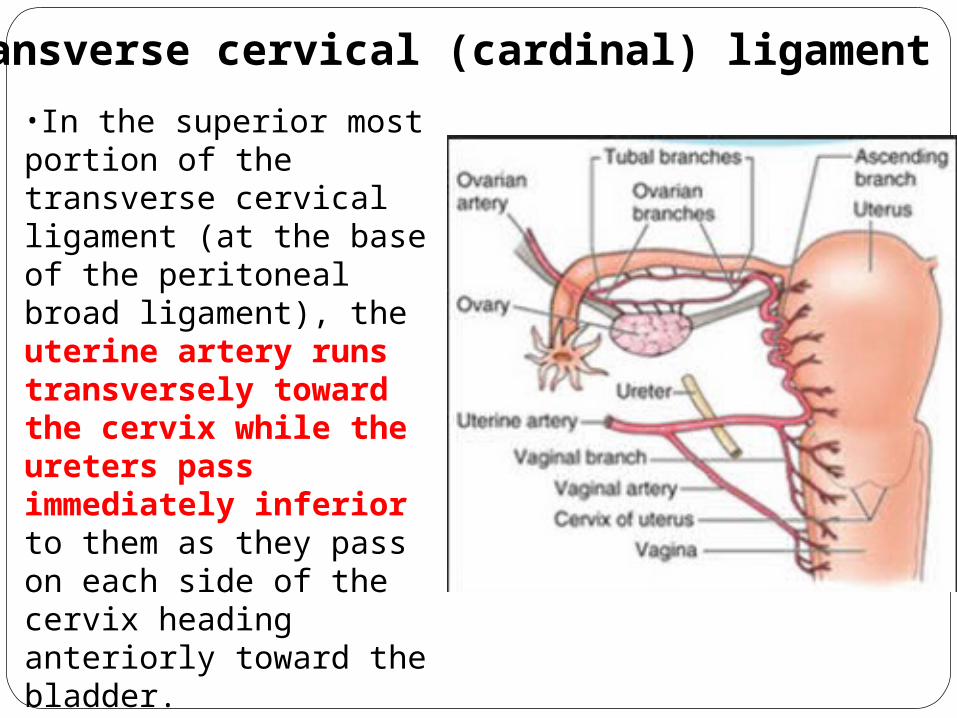
•In the superior most portion of the transverse cervical ligament (at the base of the peritoneal broad ligament), the uterine artery runs transversely toward the cervix while the ureters pass immediately inferior to them as they pass on each side of the cervix heading anteriorly toward the bladder. •This relationship is particularly important in surgery (injury of the ureters during ligation of ovarian artery).
Transverse cervical (cardinal) ligament
A 59-year-old woman comes to a local hos-pital for uterine cancer surgery. As the uterine artery passes from the internal iliac artery to the uterus, it crosses superior to which of the following structures that is sometimes mistak-enly ligated during such surgery?(A) Ovarian artery(B) Ovarian ligament(C) Uterine tube(D) Ureter(E) Round ligament of the uterus
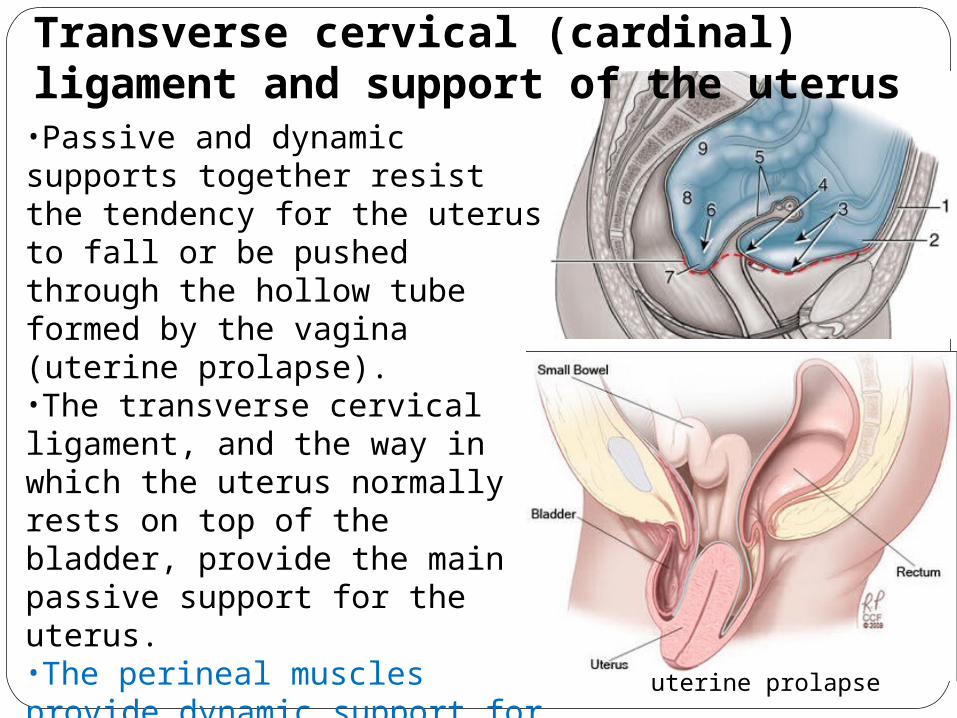
•Passive and dynamic supports together resist the tendency for the uterus to fall or be pushed through the hollow tube formed by the vagina (uterine prolapse). •The transverse cervical ligament, and the way in which the uterus normally rests on top of the bladder, provide the main passive support for the uterus. •The perineal muscles provide dynamic support for the uterus by contracting during moments of increased intra-abdominal pressure (sneezing, coughing, etc.).
Transverse cervical (cardinal) ligament and support of the uterus
uterine prolapse
Uterine Prolapse:
• Most common cause is childbirth
Signs & Symptoms:
• Vaginal pressure sensation
• Vaginal fullness
• Low back pain
Degrees of prolapse:
1 st degree - prolapse is above introitus
2 nd degree - goes to the introitus
3 rd degree - goes past introitus