Embed Size (px)
DESCRIPTION
Citation preview

Journal of Veterinary Cardiology (2007) 9, 83e89
www.elsevier.com/locate/jvc
Clinical and echocardiographic findingsof pulmonary artery stenosis in seven cats
Donald P. Schrope, DVM, Dipl ACVIM a,*,William J. Kelch, DVM, PhD, Dipl ACVPM b
a Oradell Animal Hospital, 580 Winters Avenue, Paramus, NJ 07652, USAb Department of Comparative Medicine, College of Veterinary Medicine,University of Tennessee, Box 1071, Knoxville, TN 37901-1071, USA
Received 19 November 2006; received in revised form 19 November 2006; accepted 10 September 2007
KEYWORDSPulmonary artery;Stenosis;Feline;Congenital
Abstract Objectives: Describe the clinical, electrocardiographic (ECG), radio-graphic and echocardiographic findings in cats with isolated pulmonary artery ste-nosis. Assess the usefulness of systolic and diastolic Doppler measurements atpredicting stenosis severity.Background: Pulmonary artery stenosis is an infrequent congenital cardiac defect inhumans that has not been reported in cats. In humans, pulmonary artery stenosis isusually seen in conjunction with other cardiac defects and may lead to clinical signsif severe.Animals, materials and methods: Seven cats with pulmonary artery stenosis wereretrospectively evaluated. Medical records, radiographs, ECGs, echocardiogramsand angiocardiograms were reviewed. Severity of stenosis was assessed by two-dimensional and color Doppler echocardiographic evaluation and clinical findings.Peak systolic and diastolic gradients across the stenosis, and systolic and diastolicpressure decay half-times were graded using echocardiography. In addition, the du-ration of antegrade flow during diastole was subjectively assessed. Univariate anal-yses were performed to assess the best variable to predict stenosis severity.Results: Concurrent congenital defects were not identified. Only cats with severeobstruction showed clinical signs including exertional dyspnea and lethargy. Dia-stolic Doppler measurements were superior to systolic measurements at predictingseverity of stenosis. Antegrade flow throughout diastole and/or a diastolic pressurehalf-time of >100 ms indicated severe obstruction. The prognosis for pulmonaryartery stenosis appears to be good regardless of severity.
* Corresponding author.E-mail address: [email protected] (D.P. Schrope).
1760-2734/$ - see front matter ª 2007 Elsevier B.V. All rights reserved.doi:10.1016/j.jvc.2007.09.001

84 D.P. Schrope, W.J. Kelch
Conclusion: Among cats with pulmonary artery stenosis, clinical signs are uncom-mon and prognosis is good. Doppler assessment of diastolic flow appears to besuperior to systolic flow at predicting severity.ª 2007 Elsevier B.V. All rights reserved.
Congenital stenosis of the main and/orbranched pulmonary arteries has been identifiedin humans and is commonly identified with con-current lesions such as ventricular septal defect,pulmonic stenosis, patent ductus arteriosus, ortetralogy of Fallot.1e3 Congenital obstruction ofthe right ventricular outflow tract is uncommonin cats with an incidence of about 2e3% of congen-ital cardiac defects.4,5 To the authors’ knowledge,stenosis of the main or branched pulmonary ar-teries has not been reported in a cat.
Stenosis of the pulmonary artery is hemody-namically similar to coarctation of the aorta andwas referred to as coarctation of the pulmonaryartery in early human studies.1 As with other typesof stenotic lesions, Doppler echocardiography hasbeen used to assess the severity of aortic coarcta-tion using the modified Bernoulli’s equation to es-timate the systolic pressure gradient across theobstruction, however, this does not consistentlyreflect severity of the stenosis when compared togradients measured at cardiac catheterization.6,7
Further studies of aortic coarctation in humanshave identified variable degrees of diastolic flowacross the stenosis. Both subjective and objectiveassessment of this diastolic flow has been found tobe more accurate than systolic gradients at assess-ing severity of coarctation in many patients.6,8,9 Inhumans with pulmonary artery stenosis and in ex-perimental studies of pulmonary artery bandingin dogs, there are varying conclusions about howclosely the Doppler systolic and cardiac catheteri-zation-derived gradients correlated.10,11 In catswith pulmonary artery stenosis, it was hypothe-sized that diastolic Doppler evaluation would re-late better to severity than systolic evaluation.
Animals, materials and methods
Cats with an echocardiographic diagnosis of pul-monary artery stenosis were retrospectively re-viewed. The majority of these cats were identifiedthrough an animal shelter that receives animalsfrom multiple sites along the east coast of theUnited States. All of the cats were initially evalu-ated because a murmur had been ausculted onphysical exam.
The P-wave and QRS complex amplitude andduration, and the PR interval were measured onthree consecutive cardiac cycles and averaged onthe electrocardiograms that were available forreview. The mean QRS axis was also assessed.The vertebral heart scale (VHS) was measured onall lateral and ventrodorsal radiographs that wereavailable for review.12
Complete echocardiograms were performed us-ing standard echocardiographic views. Maximumpulmonary valve annulus diameter (PVD) andpulmonary artery stenosis diameter (PSD) wereobtained from right or left parasternal short-axistwo-dimensional (2D) images during systole. Pul-monary artery stenosis diameter was evaluatedwith the assistance of color-flow Doppler (CFD) toidentify the vena contracta in all cases. In catswith severe disease the stenotic orifice was oftenso small that it was not easily identified withoutCFD. The ratio of stenosis diameter to pulmonaryvalve annulus diameter (PSD/PVD) was calculated.Maximum right atrial diameter (RAD) and left atrialdiameter (LAD) were obtained from right para-sternal long-axis 2D images during diastole. Mea-surements of the RAD were performed usinga method similar to published methods of measur-ing the LAD in long-axis.13 The ratio of RAD to LADwas calculated and considered normal if <1.0.14
Right ventricular end-diastolic diameter (RVDd)and left ventricular end-diastolic diameter (LVDd)were obtained from M-mode tracings. The RVDdto LVDd ratio was generated and considered nor-mal if <0.33.14 The remainder of the left heartmeasurements was made from standard 2D andM-mode echocardiographic views. All 2D and M-mode measurements were made on three consec-utive cardiac cycles and averaged.
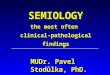
Peak systolic flow velocity through the stenosiswas measured in all cats after normal pulmonaryvalve flows were confirmed and a velocity step-upwas identified at the level of the stenosis. Estima-tion of the peak systolic pressure gradient (PaS)and peak diastolic pressure gradient (PaD) acrossthe stenosis was calculated using the modifiedBernoulli’s equation. Peak diastolic flow velocitywas measured at the onset of diastole identified bythe end of the T-wave on the electrocardiogram(Fig. 1).8 The systolic pressure decay half-time

Clinical and echocardiographic findings 85
(Spht) was measured from the peak systolic flow tothe onset of diastole (the end of the T-wave). Thediastolic pressure decay half-time (Dpht) was mea-sured from the onset of diastole to baseline or tothe onset of systole if antegrade flow was presentthroughout diastole. All measurements were per-formed on three consecutive waveforms and aver-aged. The presence or absence of diastolic flow(DFA) was also subjectively assessed from thespectral Doppler tracing and graded as; (0þ) no di-astolic flow, (1þ) flow through 50% or less of dias-tole, (2þ) flow through >50% but <100% ofdiastole, and (3þ) diastolic flow throughout dias-tole resulting in continuous flow across the stenosis(Fig. 1).
Angiocardiography was performed to bettercharacterize the lesion in the two initial cases.The ratio of minimal stenosis diameter to PVannulus diameter was obtained and averagedfrom at least two cardiac cycles during systole.
For statistical analysis, severity of stenosis wasassessed based on the echocardiographic PSD/PVDratio. The diastolic and systolic Doppler data werecompared to the PSD/PVD ratio. Univariate analy-ses were performed to assess the correlation withstenosis severity.c A p-value <0.05 was consideredsignificant; r refers to the coefficient of linear cor-relation between two variables; r-squared for con-tinuous variables refers to the coefficient of
Figure 1 Spectral Doppler findings in cats 3 (A) and 7(B) and technique used to identify diastolic Dopplermeasurements. The onset of diastole was identified atthe end of the T-wave and the peak diastolic gradientwas measured at this point. The systolic pressure decayhalf-time (Spht) was measured from the peak systolicflow to the onset of diastole. The diastolic pressuredecay half-time (Dpht) was measured from the onsetof diastole to the end of diastolic flow.
c JMP, Version 5.1 statistical software (SAS Institute Inc., SASCampus Dr, Cary, NC 27513, USA).
multiple determination which estimates the pro-portion of the response variation that can beexplained by the continuous independent variable;and r-squared for an ordinal variable refers to theuncertainty coefficient which, analogous to the co-efficient of multiple determination for continuousvariables, also explains the proportion of the re-sponse variation explained by the ordinal indepen-dent variable.
Results
The signalment, clinical signs, and findings ofcardiac auscultation are summarized in Table 1.None of the cats had evidence of jugular pulses,cyanosis, alterations in femoral pulse strength orquality, abnormalities in S1 or S2, or a galloprhythm during a resting examination.
Six of the cats were asymptomatic at the timeof presentation. One cat (diagnosed at 12 years ofage) was described as less active than expected allof her life by one of two owners. One cat, that hadinitially been asymptomatic, developed moderateexertional dyspnea soon after diagnosis. An arte-rial blood gas was performed after dyspnea wasinduced by exercise. The arterial blood gas wasassessed as a mixed metabolic and respiratoryacidosis with hypoxia (pH 7.1, pCO2 45.6, pO2
84.0, HCO3 14.0, BEe15, sO2 90%). The calculatedalveolar to arterial gradient was nine. The findingswere consistent with hypoperfusion from pulmo-nary artery stenosis. The clinical signs in cat 7did not progress over time, and no treatment wasinitiated.
Three cats had an ECG available for review. Noabnormalities were identified in two of the cats (#2and 6). The ECG of cat 5 revealed deep S-waves inleads I, II, III, aVF, a right mean electrical axis shift(170�e180�), and widening of the QRS complex(50 ms) suggestive of right ventricular enlargementor a partial right bundle branch block. Five cats(#3e7) had chest radiographs available for review.All five cats had normal VHS on lateral and ventro-dorsal views and one cat (#7) had subjective evi-dence of right ventricular enlargement anda small pulmonary artery bulge.
Echocardiography was performed in all sevencats and identified pulmonary artery stenosis withvariable degrees of main pulmonary artery dilationproximal to the stenotic lesion (Figs. 2 and 3).Color-flow Doppler confirmed turbulence duringsystole at the suspected stenosis in all cats and di-astolic flow at the level of the stenosis in cats 6and 7. No cat showed evidence of pulmonary valvedisease or left heart abnormalities. A summary of

86 D.P. Schrope, W.J. Kelch
Table 1 Signalment, initial auscultation findings, and clinical signs in seven cats with pulmonary artery stenosis
Cat Breed Sex Age atdiagnosis
Age as ofpublication (years)
Auscultation at initialexamination
Clinical signs
1 DSH F 2 months 6.8 2e3/6 left and right basilar SM None2 DSH F 8 months 7.4 2e3/6 right basilar SM None3 DSH F 9 months 9 3/6 left basilar SM None4 DSH M 3 years 9a 4/6 left basilar SM None5 Persian M 5 months 4.6 3/6 right basilar SM None6 DSH F 12.7 years 13.9b 4/6 left basilar SM Lethargy7 DSH M 15 months 9.6 2e3/6 left basilar SM and 1/6 DM Exertional dyspnea
DSH¼ domestic short hair, M¼male, F¼ female, SM¼ systolic murmur, and DM¼ diastolic murmur.a Lost to follow-up.b Euthanized.
the 2D echocardiographic findings of the rightheart and spectral Doppler data is presented in Ta-ble 2. Visualization of the pulmonary artery bifur-cation and branched pulmonary arteries from theright parasternal short-axis view was accomplishedin the majority of cats. In cat 6 the branched pul-monary arteries could only be visualized froma left parasternal short-axis view. In cats 4 and 7the branched pulmonary arteries could not be visu-alized well from the right or left side with 2D. TheCFD in both cats, though, did show flow conver-gence and turbulence at the bifurcation with split-ting of the color-flow pattern into the origins ofthe branched pulmonary arteries.
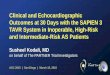
Angiocardiography confirmed in cats 4 and 7 anisolated lesion of the distal main pulmonary artery
just proximal to the bifurcation without involve-ment of the branched or peripheral segmentalpulmonary artery (Fig. 4). The average ratio ofPSD/PVD on the angiocardiograms was 0.50 in cat4 and 0.32 in cat 7.
Based on the univariate analyses, the Dpht(p¼ 0.002; r¼�0.94; r2¼ 0.88) was most closelyassociated with stenosis severity. The DFA(p¼ 0.025; r2¼ 0.94), PaD (p¼ 0.003; r¼�0.92;r2¼ 0.85) and PaS (p¼ 0.009; r¼�0.88; r2¼ 0.78)were also significantly associated with stenosis se-verity. Cats 6 and 7 had evidence of right atrialand ventricular dilation as well as clinical signs. Itwas felt that these two cats had severe disease.Both cats with severe stenosis had a DFA of 3þ dia-stolic flow and Dpht >100 ms (Table 2).
Figure 2 Two-dimensional (A) and color-flow Doppler (B) images of cat 1 with mild pulmonary artery stenosis. Im-ages were obtained during systole. Note the mild narrowing of the pulmonary artery just proximal to the bifurcation(A) and associated flow convergence using color-flow Doppler (B). (Ao¼ aorta, MPa¼main pulmonary artery, RPa¼right-branched pulmonary artery, LPa¼ left-branched pulmonary artery).

Clinical and echocardiographic findings 87
Figure 3 Two-dimensional (A) and color-flow Doppler (B) images of cat 6 with severe pulmonary artery stenosis. Im-ages were obtained during systole. Note the severe stenosis in the body of the pulmonary artery and severe dilation ofthe main pulmonary artery (A). The stenotic orifice was very difficult to identify using only 2D imaging in this cat.Color-flow Doppler identified the orifice of the stenotic lesion and confirmed flow convergence (B). (Ao¼ aorta,MPa¼main pulmonary artery, RPa¼ right-branched pulmonary artery, LPa¼ left-branched pulmonary artery).
All of the cats were alive well into maturity andonly cat 6 had died at the time of publication. Cat 6had been euthanized approximately 15 monthsafter diagnosis due to repeated signs of anorexia,depression, and sneezing, as well as a suspiciouspulmonary nodule on radiographs. A necropsy wasnot allowed. Cat 4 was lost to follow-up at approx-imately 8 years of age. At the time of publication,serial echocardiograms have been performed on theremaining five cats. No progression in the degree ofstenosis has been identified.
Discussion
Pulmonary artery stenosis is a well-known congen-ital anomaly in humans that most often occurs in
conjunction with other congenital cardiac anoma-lies. The cause of pulmonary artery stenosis isunclear. Postmortem studies in adults reveal intimalinvasion by smooth muscle, medial hyperplasia, andincreased and disorganized elastin fibers at the siteof stenosis. In contrast, postmortem studies ininfants reveal fibrous intimal proliferation, medialhypoplasia, and loss of elastin fibers.3 Postmortemsamples were not available from cats in this studyfor comparison with the findings in humans.
A classification scheme for pulmonary arterystenosis based on the stenosis location and numberof lesions has been developed in humans.1 Theclassification divides the pulmonary artery intofour segments; (1) main pulmonary artery, (2) bi-furcation, (3) left- and right-branched pulmonaryarteries, and (4) peripheral segmental pulmonary
Table 2 Echocardiographic findings at initial diagnosis
Cat Wt(kg)
RVDd/LVDd RAD/LAD PVD(cm)
PSD(cm)
PSD/PVD PaS(mmHg)
Spht(ms)
PaD(mmHg)
Dpht(ms)
DFA(þ)
1 0.8 0.19 0.92 0.50 0.30 0.60 13.0 37 0.00 0 02 2.5 0.31 0.85 0.90 0.45 0.50 16.2 47 5.86 30 13 2.8 0.20 1.10 0.90 0.45 0.50 21.5 33 4.67 43 24 2.3 0.13 0.98 0.85 0.36 0.42 37.7 43 13.69 30 25 2.3 0.27 0.83 0.74 0.31 0.41 21.2 58 4.75 50 26 3.7 0.40 1.15 0.75 0.22 0.29 59.9 61 20.61 132 37 4.3 0.46 1.18 1.04 0.27 0.26 45.2 50 28.94 130 3
The cats were ranked from least to most severe based on severity of the echocardiographic PSD/PVD ratio. RVDd/LVDd¼ ratio ofright ventricular to left ventricular end-diastolic dimensions, RAD/LAD¼ ratio of maximal right atrial diameter in long-axis to max-imal left atrial diameter in long-axis (diastole), PVD¼ pulmonary valve annulus diameter (systole), PSD¼ pulmonary artery steno-sis diameter (systole), PaS¼ pulmonary artery stenosis peak systolic gradient, Spht¼ pulmonary artery stenosis systolic pressurehalf-time, PaD¼ pulmonary artery stenosis peak diastolic gradient, Dpht¼ pulmonary artery stenosis diastolic pressure half-time,and DFA¼ subjective grading of diastolic flow (0þ to 3þ). Weight (Wt) listed is that recorded at the time of initial diagnosis.

88 D.P. Schrope, W.J. Kelch
arteries. Single lesions of the main pulmonary ar-tery or branched pulmonary arteries are classifiedas Type I pulmonary artery stenosis. Type I lesionsare further subclassified into Type Ia (isolated ste-nosis of the main pulmonary artery), Type Ib (iso-lated stenosis of the right-branched pulmonaryartery), and Type Ic (isolated stenosis of the left-branched pulmonary artery). Isolated lesions lo-cated at the bifurcation with extension into theproximal branched pulmonary arteries are classi-fied as Type II. Lesions involving the peripheralsegmental pulmonary arteries with no abnormali-ties of the main pulmonary artery, bifurcation, orleft- or right-branched pulmonary arteries areclassified as Type III. Lesions involving the periph-eral segmental pulmonary arteries with additionallesions in the main, left-branched, and/or right-branched pulmonary arteries are classified asType IV. Type Ia is one of the least common classesof pulmonary artery stenosis seen in humans.1 Incontrast, the cats in this study showed no evidenceof other concurrent cardiac defects and the lesionwas classified as Type Ia in all cats.
Figure 4 Selective right ventricular angiocardiogramfrom cat 4 with distal pulmonary artery stenosis. Opaci-fication of the right ventricle (RV), main pulmonary ar-tery (MPa), and right- (RPa) and left (LPa)-branchedpulmonary arteries is evident. Mild opacification of theright atrium and the caudal vena cava (CVC) is also pres-ent resulting from retrograde movement of the catheterback into the right atrium during injection. Note the ste-nosis of the main pulmonary artery just proximal to thebifurcation (black arrow) with normal branched pulmo-nary arteries.
Of the seven cats, six cats were mixed breed,and no sex predilection was suggested (Table 1).The age at the time of diagnosis for most of thesecats suggests a congenital lesion although a herita-ble basis could not be assessed since the majoritywere stray animals.
All seven cats presented with basilar systolicmurmurs although the point of maximal intensityvaried (Table 1). Only one cat with severe stenosisand visible Doppler flow throughout diastole hada diastolic murmur. In humans with pulmonary ar-tery stenosis the presence of a diastolic murmur isvariable.1,2
Exertional dyspnea was seen in one of the catswith severe stenosis. Exertional dyspnea is one ofthe most common clinical signs identified inhumans with pulmonary artery stenosis, and islikely related to hypoperfusion of the pulmonaryarterial tree.3 Based on the blood gas analysis, thiswas also the likely cause for exertional dyspnea inthis cat. It is also possible that certain lesionscould result in asymmetric blood flow to branchedpulmonary arteries further contributing to ventila-tioneperfusion mismatch.
The available radiographs and ECGs did notreveal specific findings that would differentiatepulmonary artery stenosis from other causes ofbasilar systolic murmurs. In fact, radiographic orelectrocardiographic abnormalities were limitedto cats with moderate to severe disease.
Although PaS and PaD were correlated to dis-ease severity, a ‘‘natural’’ cut-off between mod-erate and severe disease was not obvious to theauthors (Table 2). Studies in human aortic coarcta-tion support the value of evaluating other diastolicflow parameters.6,8,9 In this study, Dpht and DFAwere statistically significant and there appearedto be natural cut-offs between moderate and se-vere disease using Dpht and DFA. One human paperevaluating patients with aortic coarctation sug-gested that a Dpht of >100 ms was consistentwith severe stenosis.8 Findings in this study suggestthat a similar value may be appropriate in catswith pulmonary artery stenosis. Both cats witha Dpht >100 ms and a DFA of 3þ had the most se-vere stenosis when graded by 2D echocardiographyand clinical signs.
The discrepancy between systolic and diastolicDoppler findings and obstruction severity in hu-mans with aortic coarctation is not clear. Causesmay be related to changes in cardiac output,collateral blood flow, ductal flow, and the shapeand length of the stenosis.6e8 Except for the mor-phology of the stenosis, none of these would likelybe a cause for similar findings in the pulmonary ar-tery. It is possible that, with more severe stenosis,

Clinical and echocardiographic findings 89
the flexible walls of the main pulmonary arteryproximal to the obstruction absorb kinetic energyas the right ventricle contracts against the steno-sis. This could result in a lower peak systolic driv-ing force across the stenosis resulting in a lowerrelative gradient.
The greatest limitations to this study are thoseinherent to a retrospective study and the smallnumber of cats available. Furthermore, grading ofseverity was based on 2D echocardiographic find-ings and clinical signs. Ideally, disease severitywould have been graded by angiocardiographicand intra-cardiac pressure data but these invasivediagnostics were believed to not be in the bestinterest for the majority of these cats.
References
1. Gay BB, French RH, Shuford WH, Rogers Jr JV. The roent-genologic features of single and multiple coarctations ofthe pulmonary artery and branches. Am J Roentgenol Ra-dium Ther Nucl Med 1963;90:599e613.
2. D’Cruz IA, Agustsson MH, Bicoff JP, Weinberg M, Arcilla RA.Stenotic lesions of the pulmonary artery. Clinical and hemo-dynamic findings in 84 cases. Am J Cardiol 1964 April:441e50.
3. Kreutzer J, Landzberg MJ, Preminger TJ, Mandell VS,Treves ST, Reid LM, Lock JE. Isolated peripheral pulmonaryartery stenosis in the adult. Circulation 1996;93:1417e23.
4. Buchanan JW. Causes and prevalence of cardiovascular dis-ease. In: Kirk RW, Bonagura JD, editors. Kirk’s current veteri-nary therapy XI. Philadelphia: WB Saunders; 1992. p. 647e55.
Available online at ww
5. Liu SK. Pathology of feline heart disease. Vet Clin North Am1977;7:323e39.
6. Houston AB, Simpson IA, Pollock JC, Jamieson MP, Doig WB,Coleman EN. Doppler ultrasound in the assessment of sever-ity of coarctation of the aorta and interruption of the aorticarch. Br Heart J 1987;57:38e43.
7. Marx GR, Allen HD. Accuracy and pitfalls of Doppler evalu-ation of the pressure gradient in aortic coarctation. J AmColl Cardiol 1986;7:1379e85.
8. Carvalho JS, Redington AN, Shinebourne EA, Rigby ML,Gibson D. Continuous wave Doppler echocardiography andcoarctation of the aorta: gradients and flow patterns inthe assessment of severity. Br Heart J 1990;64:133e7.
9. Valdez-Cruz LM, Cayre RO. Coarctation of the aorta. In:Valdez-Cruz LM, Cayre RO, editors. Echocardiographicdiagnosis of congenital heart disease: an embryologic andanatomic approach. Philadelphia: Lippincott-Raven; 1999.p. 475e82.
10. Houston AB, Sheldon CD, Simpson IA, Doig WB, Coleman EN.The severity of pulmonary valve or artery obstruction inchildren estimated by Doppler ultrasound. Eur Heart J1985;6:786e90.
11. Valdes-Cruz LM, Horowitz S, Sahn DJ, Larson D, OliveriaLima C, Mesel E. Validation of a Doppler echocardiographicmethod for calculating severity of discrete stenotic obstruc-tions in a canine preparation with a pulmonary arterialband. Circulation 1984;69:1177e81.
12. Litster AL, Buchanan JW. Vertebral scale system to measureheart size in radiographs of cats. J Am Vet Med Assoc 2004;216:210e4.
13. Rishniw M, Erb HN. Evaluation of four 2-dimensional echo-cardiographic methods of assessing left atrial size in dogs.J Vet Intern Med 2000;14:429e35.
14. Boon JA. Acquired heart diseases. In: Boon JA, editor. Man-ual of veterinary echocardiography. Baltimore: Williams &Wilkins; 1998. p. 261e382.
w.sciencedirect.com