Embed Size (px)
Citation preview

Pediatric Pulmonology 48:1112–1118 (2013)
Clinical and Epidemiologic Profile ofLower Respiratory Tract Infections Associated
With Human Bocavirus
Cristiano do Amaral de Leon, MD, Msc,1 Sergio Luis Amantea, MD, PhD,2*Diogo Andre Pilger, PhD,3 and Vlademir Cantarelli, PhD
4
Summary. Background: Acute viral bronchiolitis (AVB) remains the leading cause of lower
respiratory tract infection (LRTI) in infants under 2 years of age. Advances in molecular meth-
ods for virus detection have led to the identification of new infectious agents implicated in the
development of AVB, such as human bocavirus (HBoV). Objectives: To ascertain the frequen-
cy, seasonality, and clinical behavior of HBoV detection in a series of episodes of LRTI.
Study Design: The frequency of HBoV was assessed in children with LRTI episodes, aged
1–24 months, seen at the emergency department of Hospital da Crianca Santo Antonio, Porto
Alegre, Brazil, between May 2007 and July 2008. Virus-specific polymerase chain reaction
was used for detection. Results: A total of 455 nasal secretion samples were collected from
433 patients over a 14-month period. Of these, 60 were positive for HBoV (13.2%). Mean age
was 7.9 months and 55% of patients were male. Just over half of patients were under 6 months
of age (53.3%). Wheezing was the presenting respiratory complaint in 51.7%. Of the
60 patients, 80% were admitted to a pediatric ward. Diarrhea was present in nine patients
(18%). Co-detection was a frequent finding in our sample, occurring in 95% of cases. In our
series, the distribution of HBoV was clearly seasonal and was influenced by temperature, rela-
tive humidity, and precipitation. Conclusions: We conclude that HBoV detection in infants with
AVB and recurrent wheezing of viral etiology in Brazil is similar to that reported in other coun-
tries. The clinical course of HBoV detection is no different from that of other respiratory viruses
commonly found in this age range. Pediatr Pulmonol. 2013; 48:1112–1118.
� 2013 Wiley Periodicals, Inc.
Key words: child; bronchiolitis; wheezing; polymerase chain reaction.
Funding source: none reported.
INTRODUCTION
Acute viral bronchiolitis (AVB) remains the leadingcause of lower respiratory tract infection (LRTI) ininfants under 2 years of age, and the respiratory syncy-tial virus (RSV) has been the etiological agent most of-ten implicated in LRTI in this age bracket. However,advances in molecular methods for virus detection haveled to the identification of new infections agents impli-cated in the development of AVB.
Human bocavirus (HBoV) was first described in as-sociation with AVB in 2005, by Allander et al.1 Eversince, a number of studies and reports have soughtto characterize the behavior of this agent in LRTIs.HBoV is a member of the Parvoviridae family andwas initially isolated in Sweden, in nasopharyngealaspirates obtained from children hospitalized for LRTI.Later studies conducted in several countries havereported that HBoV is present in 1.5–19% childrenwith LRTI.2–8 In South and Central America, Salmon-Mulanovich et al.9 demonstrated the prevalence of
1Graduate Program in Medical Sciences, Universidade Federal de
Ciencias da Saude de Porto Alegre (UFCSPA), Porto Alegre, RS, Brazil.
2Pediatrics Department, UFCSPA, Porto Alegre, RS, Brazil.
3School of Pharmacy, Universidade Federal do Rio Grande do Sul
(UFRGS), Porto Alegre, RS, Brazil.
4Instituto de Ciencias da Saude (ICS), Universidade Feevale, Novo Ham-
burgo, RS, Brazil.
Conflict of interest: None.
*Correspondence to: Sergio Luis Amantea, MD, PhD, Pediatrics Depart-
ment, UFCSPA Rua Sarmento Leite, 245, Porto Alegre, RS, Brazil.
E-mail: [email protected]
Received 10 April 2012; Accepted 25 October 2012.
DOI 10.1002/ppul.22732
Published online 2 July 2013 in Wiley Online Library
(wileyonlinelibrary.com).
� 2013 Wiley Periodicals, Inc.

10.8% of HBoV in Argentina, 33.3% in Nicaragua,and 25.1% in Peru, in a series including 568 patients.Children are most often infected, with the highest fre-quency found in hospitalized infants.10,11 In adult popu-lations, HBoV is rarely isolated in association withLRTI.11,12 More recently, a study conducted in Asiasuggested a lower prevalence of HBoV in patientsyounger than 10 years, with rare cases of HBoV infec-tion detected in immunocompromised adults.13
Virtually all studies have shown a high rate of co-detection with other respiratory viruses.12,14–17 In addi-tion to its detection in respiratory tract secretions,HBoV has also been isolated in the feces, blood, andurine of pediatric patients.18–20
Few studies conducted in South America haveattempted to characterize the behavior of this virus,either as a causative agent of AVB or in recurrentLRTI-associated wheezing of early childhood.
The aim of this study was to ascertain the frequency,seasonality, and clinical behavior of HBoV detectionover a 14-month period in a series of episodes of LRTI.
MATERIALS AND METHODS
This was a cross-sectional study of infants aged1–24 months and treated at the pediatric emergency de-partment of Hospital da Crianca Santo Antonio(HCSA), Porto Alegre, in Rio Grande do Sul, the south-ernmost state of Brazil, over a 14-month period(May 2007 through July 2008).
Patients were considered eligible for inclusion if theyhad a clinical and radiological diagnosis of community-acquired LRTI (AVB or recurrent wheezing in earlychildhood).
Children with congenital heart disease, chronic lungdisease, or acute or chronic neuropathies were excludedfrom the sample. During the study period, all patientsin the target age range kept in for observation with apresumptive diagnosis of LRTI underwent plain chestradiography and polymerase chain reaction (PCR)-assisted detection of respiratory viruses as part of rou-tine management.
Diagnosis of AVB was considered in patients under24 months of age with a presenting complaint of new-onset obstructive respiratory disease (wheezing and/orrales with signs and symptoms of respiratory discom-fort).21 All patients were required to have had a prodro-mal illness (symptoms of upper airway infection) of nomore than 72 hr duration and have anteroposterior (AP)chest radiograph findings consistent with a diagnosis ofAVB, as established by a pediatric radiologist who wasnot involved in the study.
Patients were diagnosed with recurrent wheezingwhen they met all of the above criteria, but had experi-enced a similar episode before.
The decision to keep patients in the observationroom was always made by the attending staff of theemergency department, with no investigator input, aswere decisions to discharge patients or transfer them toinpatient units (pediatric wards or intensive care).
At HCSA, pediatric patients may remain in the ob-servation room for up to 24 hr, after which time theymust be discharged from the hospital or admitted to apediatric ward or intensive care depending on theircondition.
As part of routine care at HCSA, nasopharyngealaspirates are obtained from all patients referred to theobservation room with suspected LRTI, for isolation ofthe etiological agent involved. For the purposes of thisstudy, HBoV-specific real-time PCR was performed onall specimens.22
Relevant clinical data were obtained from standard-ized forms and through a review of patient charts. Thefollowing variables of interest were defined: gender, age(months) on admission, breastfeeding, premature birth,nature of the LRTI episode (first episode or recurrent),time elapsed between onset of symptoms and presenta-tion to the emergency department, axillary temperatureand oxygen saturation (on arrival), clinical severityscore,23 length of stay, presence of gastrointestinalcomplaints (vomiting, diarrhea), and presence of radio-graphic findings consistent with a presumptive diagno-sis of viral or bacterial infection. The clinical scoreused at HCSA is that developed by Cengizlier et al.,23
measured on a scale of 1–9 (1 being least severity and9 being most severity).
Samples and Nucleic Acid Extraction andcDNA Synthesis
Nasopharyngeal aspirates (NPA) samples that werekept frozen at—708C were used for total nucleicacids extraction, which were isolated from 200 ml ofeach buffered respiratory specimen using the QIAmpUltraSens Virus Kit (Qiagen, Hilden, Germany). To ensurethat negative results were not due to poor nucleic acidextraction or inhibition of PCR assay, amplification ofb-globin gene was applied for each sample.
Real-Time PCR
The HBoV was detected by a singleplex virus-specificPCR. Two microliter of DNA were assayed in a 20 mlreaction mixture containing 10.0 ml Platinum Syber Mix(SuperScript III Platinum Two-Step qRT-PCR kit withSyber Green, Invitrogen, Carlsbad, CA), 1.0 ml of bovineserum albumin, 1.0 ml (10 mM) of forward and reverseprimers. Glicosylase and dUTP were included in the PCRmaster mix to prevent false-positive reactions due toamplicon carry-over. All amplifications and detectionswere performed using the LightCycler instrument (Roche
LRTI Associated With HBoV 1113
Pediatric Pulmonology

Diagnostics, Mannheim, Germany) and identification ofvirus was assessed by melting curve analysis.
Primer Design and Preparation
Primers were especially designed from consensus ge-nome regions obtained from DNA Data Bank of Japan(DDBJ; http://blast.ddbj.nig.ac.jp/top-e.html). Typically,sequences of 50–100 representative strains of eachpathogen were downloaded and the sequences werealigned using Clustal W (http://clustalw.ddbj.nig.ac.jp/top-e.html). For hBoV, NP-1 gene was used and primerssequences were: HBOV-F1: GTCCAGAAAGAGGG-GAGAGG and HBOV-R1: GCTGATTGGGTGTTCCTGAT.22
The climate variables analyzed were: temperature(measured using a thermometer graduated in degreesCelsius, 8C), total monthly rainfall (measured using arain gauge graduated in millimeters, mm), and air hu-midity (measured by a psychrometer in percentage, %).The data were obtained from the National Instituteof Meteorology (INMET) recorded for the city ofPorto Alegre during the period of study, protocol no.067/2011.
A database was compiled in the SPSS v.15.0 softwareenvironment (SPSS Inc., Chicago, IL) and data wereanalyzed by means of descriptive statistics, using tablesof absolute and relative frequencies, measures of centraltendency and dispersion (means, medians, percentiles,interquartile ranges, standard deviations), and barand line graphs plotted in Microsoft Excel (Microsoft,Redmond, WA), depending on the nature of each vari-able (quantitative or categorical). The chi-squared testfor independence or Fisher’s exact test was used asnecessary to test for association between categoricalvariables. The nonparametric Mann–Whitney U andKruskal–Wallis tests were used to test for associationbetween quantitative variables. Spearman’s coefficientwas used to test for correlation between climate varia-bles and HBoV detection. The significance level wasset at 5% (a ¼ 0.05).
This project was approved by the UFCSPA ResearchEthics Committee with judgment no. 810/09.
RESULTS
A total of 455 nasopharyngeal aspirates were collect-ed from 433 patients over a 14-month period (22patients admitted for recurrent infection). Of these,60 were positive for HBoV (13.2%). Mean age was 7.9months (range, 1–24 months), and 55% of patientswere male. Just over half of patients were under6 months of age (53.3%). Wheezing was the presentingrespiratory complaint in 31 cases (51.7%). Of the 60patients, 48 (80%) were admitted to a pediatric ward,10 (16.7%) were discharged home, and two (3.3%)
were transferred from the emergency department direct-ly to the pediatric intensive care unit.
Thirty-two patients (53.3%) were being or had beenbreastfed and 21 (35%) had never been breastfed at all.Information on breastfeeding was unavailable for sevenpatients (11.7%). Of the 50 patients admitted for inpa-tient care, 43 (71.6%) had a median BronchiolitisSeverity Score of 4 (interquartile range [IQR], 1–7).Median oxygen saturation on arrival was 92% (IQR,77–100%). Diarrhea was present in nine patients (18%).On plain chest radiographs, 40 patients (66.7%) hadfindings consistent with a presumptive diagnosis of viralinfection. In 20 patients, findings were indicative ofbacterial co-detection (33.3%). Further radiographic ex-amination was ordered for three patients due to clinicaldeterioration during the hospital course; in all three,X-rays showed focal consolidation of presumablybacterial origin. No patients had pleural effusion or ra-diographic findings consistent with necrotizing lunginjury.
Of the 60 HBoV-positive patients, 10 (16.7%) did notrequire hospital admission and were discharged lessthan 24 hr after arrival. In those who did require hospi-talization (83%), the median length of stay was 7 days;44% of these patients remained in the hospital for lessthan 1 week.
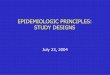
In our sample, HBoV detection clearly followed aseasonal distribution pattern (Fig. 1). Environmentalfactors such as temperature, relative humidity, and pre-cipitation influence the distribution of HBoV infectionover the course of the year. Monthly rainfall totals andincreased relative humidity contribute to a significantlyhigher frequency of HBoV infection, as shown inFigure 1.
Co-detection was a frequent finding in this series.HBoV was the only infectious agent isolated in onlythree of the 60 HBoV-positive samples (5%). Table 1shows the frequency of other viruses detected and astratification of cases by the number of viral pathogens.
Three patients (5%) in our sample required mechani-cal ventilation. RSV co-detection was present in allthree. There were no deaths during the study period.
Analysis of both study-eligible groups (AVB vs. re-current wheezing) showed similar patient profiles.There were no significant differences between AVB(54.3%) and recurrent wheezing (45.6%) patients interms of age, time elapsed between symptom onset andpresentation, oxygen saturation, body temperature,Bronchiolitis Severity Score, or hospital length of stay(Table 2).
DISCUSSION
The findings reported in this study corroboratethe hypothesis that HBoV is a prevalent pathogen of
1114 de Leon et al.
Pediatric Pulmonology

childhood respiratory disease. Our detection ratesare consistent with those of other published series,which have reported variable prevalence ranges of 1.5–19%.2,24 Methodological factors may also account forthese differences, as there are substantial discrepanciesin the criteria used for patient selection and in thechoice of method for detection of viral pathogens. Fur-thermore, this study was limited to patients with
relatively severe clinical manifestations, as only hospi-talized children were included, whereas other studiesused mixed samples (including outpatients as well).16
The possibility of including the same patient morethan once in our sample occurred 22 times. However,none of these patients had HBoV detected. In the agegroup we studied, recurrence of infections associatedwith different viral etiologies is a common event. Thus,
Fig. 1. Monthly frequency of HBoV detection according to different climate variables. A:
Average monthly temperature (8C); (B) Monthly total rainfall (mm); (C) Average monthly
relative humidity (%).
LRTI Associated With HBoV 1115
Pediatric Pulmonology

the frequency of HBoV should be cautiously inter-preted. In fact, the frequency of 13.2% refers to thepercentage of HBoV detected considering the numberof cases that met the inclusion criteria.
Analysis of the gender and age distribution of HBoVdetection in this sample revealed certain peculiarities.As in other studies,11,25–29 male patients were affectedslightly more often (55%), but the age distribution ofour series diverged from that usually described in theliterature.25 Over half of our patients were younger than6 months; in other series, patients have often beenolder.25
In the majority of patients in this sample, the present-ing clinical picture was minor and the later clinicalcourse during admission was uneventful. Cough wasthe leading symptom, followed by dyspnea/wheezingand fever.25 As described in other case series, gastroin-testinal manifestations were also present in our sample:diarrhea and vomiting occurred in 18 patients(36%).6,20,26,30
The objective of the exclusion of patients with under-lying diseases was to make the sample more homoge-neous regarding clinical manifestations associated onlywith viral etiology. However, such strategy might havecontributed to a lower severity of our cases when com-pared with other studies in which cases with underlyingdiseases were not excluded.31–33
HBoV detection followed a seasonal distribution,similar to that classically described for RSV.21,34 Con-versely, in other populations, occurrence of the virusdid not appear to be associated with any particular timeof year.26 Nevertheless, some reports have suggestedthat HBoV infection occurs more often in the wintermonths.1,27,35 This diversity in reported distributionssuggests that other factors may also influence develop-ment of HBoV infection.36
High co-detection rates have been reported in mostpublished case series (18–72%). In this sample, HBoVwas the sole detectable infectious agent in only threecases (5%). This phenomenon has been discussed byseveral authors. Kesebir et al.28 justified this differencein co-detection rates by testing patients with LRTI forHBoV infection whose specimens had already testednegative for other respiratory viruses. Esposito et al.37
suggest that the association between HBoV and otherrespiratory viruses may be of clinical importance, andthat infection with HBoV alone appears to produce nomajor symptoms in infants seen in emergency depart-ments. High rates of co-detection may also mean thatHBoV boosts the pathogenic potential of other viruses;even certain associated technical aspects (due to thehigh sensitivity of molecular methods) have beenreported.37
Some studies, such as the one by Flores et al.,38
showed a greater severity in some clinical parametersof HBoV co-infection, mainly in terms of respiratorysyncytial virus, when compared with simple HBoVinfection.
Several studies have pointed out differences betweenetiologic agents and associated clinical manifestations
TABLE 1— Frequency of Virus Detection in 60 ChildrenWith HBoV
N1 %
Number of infectious agents
Single detection (HBoV) 3 5.0
Co-detection (HBoV þ 1 virus) 32 53.3
Multiple co-detection (HBoV þ 2 or more viruses) 25 41.7
Agents present in co-detection
Respiratory syncytial virus 24 40.0
Rhinovirus 17 28.3
Influenza A 14 23.3
Metapneumovirus 12 20.0
Influenza B 7 11.7
Parainfluenza 3 6 10.0
Parainfluenza 1 3 5.0
Adenovirus 2 3.3
Parainfluenza 2 1 1.7
1Co-detection may involve more than one agent in addition to
HBoV.
TABLE 2— Association Between Demographic Variables and First Episode of Wheezing or Recurrent Wheezing
Variable1 patients
First episode of wheezing
Yes No
P-value2N ¼ 31 (IQR25–75) N ¼ 26 (IQR25–75)
Age (months) 5.5 (3.0–10.0) 5.0 (3.0–9.0) 0.903
Onset of symptoms (days) 4.5 (3.0–7.0) 5.0 (3.0–13.0) 0.866
SatO2 (%) 96.5 (93.0–99.0) 94.5 (89.0–97.0) 0.180
Axillary temperature (8C) 37.4 (36.8–38.0) 37.5 (36.7–38.1) 0.738
Bronchiolitis Severity Score 4.0 (4.0–5.0) 4.0 (3.0–4.0) 0.232
Length of stay (days) 7.5 (5.0–9.0) 6.0 (4.0–9.0) 0.408
1Median (IQR25–75).2Mann–Whitney U-test.
1116 de Leon et al.
Pediatric Pulmonology

considering recurrent wheezing and AVB.39,40 We wereunable to observe such differences in our series. Differ-ences in the characteristics of the studies, such as inclu-sion of patients without comorbidities and from ayounger age group, might have contributed to the clini-cal presentation of our findings.
Some limitations of this study should be noted.Although it was conducted over a 14-month period anddetected HBoV in a significant proportion of patients,sample size may still be a limiting factor for compari-son between certain subgroups of the study.
We conclude that there are cases of HBoV detectionin infants with AVB and recurrent wheezing with viraletiology in our region. Despite a relative dearth of com-parative data on the clinical behavior of HBoV inBrazil, the data presented herein suggest that it is simi-lar to that reported in other countries, and that the clini-cal course of HBoV detection is no different from thatof other respiratory viruses commonly found in this agerange.
REFERENCES
1. Allander T, Tammi MT, Eriksson M, Bjerkner A, Tiveljung-Lin-
dell A, Andersson B. Cloning of a human parvovirus by molec-
ular screening of respiratory tract samples. Proc Natl Acad Sci
USA 2005;102:12891–12896.
2. Allander T, Jartti T, Gupta S, Niesters HG, Lehtinen P, Oster-
back R, Vuorinen T, Waris M, Bjerkner A, Tiveljung-Lindell A,
et al. Human bocavirus and acute wheezing in children. Clin
Infect Dis 2007;44:904–910.
3. Chung JY, Han TH, Kim CK, Kim SW. Bocavirus infection in
hospitalized children, South Korea. Emerg Infect Dis 2006;
12:1254–1256.
4. Kaplan NM, Dove W, Abu-Zeid AF, Shamoon HE, Abd-
Eldayem SA, Hart CA. Human bocavirus infection among
children, Jordan. Emerg Infect Dis 2006;12:1418–1420.
5. Lau SK, Yip CC, Que TL, Lee RA, Au-Yeung RK, Zhou B, So
LY, Lau YL, Chan KH, Woo PC, et al. Clinical and molecular
epidemiology of human bocavirus in respiratory and fecal
samples from children in Hong Kong. J Infect Dis 2007;196:
986–993.
6. Monteny M, Niesters HG, Moll HA, Berger MY. Human boca-
virus in febrile children, The Netherlands. Emerg Infect Dis
2007;13:180–182.
7. Qu XW, Duan ZJ, Qi ZY, Xie ZP, Gao HC, Liu WP, Huang CP,
Peng FW, Zheng LS, Hou YD. Human bocavirus infection
people’s Republic of China. Emerg Infect Dis 2007;13:165–
168.
8. Redshaw N, Wood C, Rich F, Grimwood K, Kirman JR. Human
bocavirus in infants, New Zealand. Emerg Infect Dis 2007;13:
1797–1799.
9. Salmon-Mulanovich G, Sovero M, Laguna-Torres VA, Kochel
TJ, Lescano AG, Chauca G, Sanchez JF, Rodriguez F, Parrales
E, Ocana V, et al. Frequency of human bocavirus (HBoV) infec-
tion among children with febrile respiratory symptoms in
Argentina, Nicaragua and Peru. Influenza Other Respir Viruses
2011;5:1–5.
10. Fry AM, Lu X, Chittaganpitch M, Peret T, Fischer J, Dowell
SF, Anderson LJ, Erdman D, Olsen SJ. Human bocavirus: a
novel parvovirus epidemiologically associated with pneumonia
requiring hospitalization in Thailand. J Infect Dis 2007;195:
1038–1045.
11. Sloots TP, McErlean P, Speicher DJ, Arden KE, Nissen MD,
Mackay IM. Evidence of human coronavirus HKU1 and human
bocavirus in Australian children. J Clin Virol 2006;35:99–102.
12. Maggi F, Andreoli E, Pifferi M, Meschi S, Rocchi J, Bendinelli
M. Human bocavirus in Italian patients with respiratory dis-
eases. J Clin Virol 2007;38:321–325.
13. Kim JS, Lim CS, Kim YK, Lee KN, Lee CK. Human bocavirus
in patients with respiratory tract infection, Korean. J Lab Med
2011;31:179–184.
14. Arden KE, McErlean P, Nissen MD, Sloots TP, Mackay IM.
Frequent detection of human rhinoviruses, paramyxoviruses,
coronaviruses, and bocavirus during acute respiratory tract
infections. J Med Virol 2006;78:1232–1240.
15. Christensen A, Nordbo SA, Krokstad S, Rognlien AG, Dollner
H. Human bocavirus in children: mono-detection, high viral
load and viraemia are associated with respiratory tract infection.
J Clin Virol 2010;49:158–162.
16. Pozo F, Garcia-Garcia ML, Calvo C, Cuesta I, Perez-Brena P,
Casas I. High incidence of human bocavirus infection in chil-
dren in Spain. J Clin Virol 2007;40:224–228.
17. Regamey N, Frey U, Deffernez C, Latzin P, Kaiser L. Isolation
of human bocavirus from Swiss infants with respiratory infec-
tions. Pediatr Infect Dis J 2007;26:177–179.
18. Albuquerque MC, Rocha LN, Benati FJ, Soares CC, Maranhao
AG, Ramirez ML, Erdman D, Santos N. Human bocavirus in-
fection in children with gastroenteritis, Brazil. Emerg Infect Dis
2007;13:1756–1758.
19. Lee JI, Chung JY, Han TH, Song MO, Hwang ES. Detection of
human bocavirus in children hospitalized because of acute gas-
troenteritis. J Infect Dis 2007;196:994–997.
20. Vicente D, Cilla G, Montes M, Perez-Yarza EG, Perez-Trallero
E. Human bocavirus, a respiratory and enteric virus. Emerg In-
fect Dis 2007;13:636–637.
21. American Academy of Pediatrics Subcommittee on Diagnosis
and Management of Bronchiolitis. Diagnosis and management
of bronchiolitis. Pediatrics 2006;118:1774–1793.
22. Pilger DA, Cantarelli VV, Amantea SL, Leistner-Segal S. Detec-
tion of human bocavirus and human metapneumovirus by real-
time PCR from patients with respiratory symptoms in Southern
Brazil. Mem Inst Oswaldo Cruz 2011;106:56–60.
23. Cengizlier R, Saraclar Y, Adalioglu G, Tuncer A. Effect of oral
and inhaled salbutamol in infants with bronchiolitis. Acta
Pediatr Jpn 1997;39:61–63.
24. Ma X, Endo R, Ishiguro N, Ebihara T, Ishiko H, Ariga T,
Kikuta H. Detection of human bocavirus in Japanese children
with lower respiratory tract infections. J Clin Microbiol 2006;
44:1132–1134.
25. Al-Sonboli N, Hart CA, Al-Aeryani A, Banajeh SM, Al-
Aghbari N, Dove W, Cuevas LE. Respiratory syncytial
virus and human metapneumovirus in children with acute respi-
ratory infections in Yemen. Pediatr Infect Dis J 2005;24:734–
736.
26. Bastien N, Brandt K, Dust K, Ward D, Li Y. Human bocavirus
infection Canada. Emerg Infect Dis 2006;12:848–850.
27. Foulongne V, Rodiere M, Segondy M. Human bocavirus in
children. Emerg Infect Dis 2006;12:862–863.
28. Kesebir D, Vazquez M, Weibel C, Shapiro ED, Ferguson D,
Landry ML, Kahn JS. Human bocavirus infection in young chil-
dren in the United States: molecular epidemiological profile and
clinical characteristics of a newly emerging respiratory virus.
J Infect Dis 2006;194:1276–1282.
29. Weissbrich B, Neske F, Schubert J, Tollmann F, Blath K,
Blessing K, Kreth HW. Frequent detection of bocavirus DNA in
LRTI Associated With HBoV 1117
Pediatric Pulmonology

German children with respiratory tract infections. BMC Infect
Dis 2006;6:109.
30. Arnold JC, Singh KK, Spector SA, Sawyer MH. Human bocavi-
rus: prevalence and clinical spectrum at a children’s hospital.
Clin Infect Dis 2006;43:283–288.
31. Bastien N, Chui N, Robinson JL, Lee BE, Dust K, Hart L, Li Y.
Detection of human bocavirus in Canadian children in a 1-year
study. J Clin Microbiol 2007;45:610–613.
32. Jung JW. Respiratory syncytial virus infection in children with
congenital heart disease: global data and interim results of
Korean RSV-CHD survey. Korean J Pediatr 2011;54:192–196.
33. Wright M, Piedimonte G. Respiratory syncytial virus prevention
and therapy: past, present, and future. Pediatr Pulmonol 2011;
46:324–347.
34. Mullins JA, Lamonte AC, Bresee JS, Anderson LJ. Substantial
variability in community respiratory syncytial virus season tim-
ing. Pediatr Infect Dis J 2003;22:857–862.
35. Manning A, Russell V, Eastick K, Leadbetter GH, Hallam N,
Templeton K, Simmonds P. Epidemiological profile and clinical
associations of human bocavirus and other human parvoviruses.
J Infect Dis 2006;194:1283–1290.
36. Naghipour M, Hart CA, Cuevas L. Infections with the novel
human bocavirus. Rev Med Microbiol 2007;18:5–10.
37. Esposito S, Bosis S, Niesters HG, Tremolati E, Sabatini C, Porta
A, Fossali E, Osterhaus AD, Principi N. Impact of human boca-
virus on children and their families. J Clin Microbiol 2008;
46:1337–1342.
38. Flores CJ, Vizcaya AC, Araos BR, Montecinos PL, Godoy MP,
Valiente-Echeverria F, Perret PC, Valenzuela CP, Hirsch BT,
Ferres GM. Human bocavirus in Chile: clinical characteristics
and epidemiological profile in children with acute respiratory
tract infections. Rev Chilena Infectol 2011;28:504–511.
39. Maffey AF, Barrero PR, Venialgo C, Fernandez F, Fuse VA,
Saia M, Villalba A, Fermepin MR, Teper AM, Mistchenko
AS. Viruses and atypical bacteria associated with asthma exac-
erbations in hospitalized children. Pediatr Pulmonol 2010;
45:619–625.
40. Kusel MM, de Klerk NH, Kebadze T, Vohma V, Holt PG,
Johnston SL, Sly PD. Early-life respiratory viral infections,
atopic sensitization, and risk of subsequent development of
persistent asthma. J Allergy Clin Immunol 2007;119:1105–
1110.
1118 de Leon et al.
Pediatric Pulmonology