Embed Size (px)
Citation preview

COMMUNICATIONS
Clinical and Molecular Diagnostic Criteria of CongenitalAtrichia with Papular Lesions
Abraham Zlotogorski, Andrei A. Panteleyev,* Vincent M. Aita,* and Angela M. Christiano*Department of Dermatology, Hadassah Medical Center, Jerusalem, Israel; *Departments of Dermatology and Genetics & Development, Columbia
University, New York, New York, U.S.A.
Congenital atrichia with papular lesions is a rare,autosomal recessive form of total alopecia and muta-tions in the hairless (hir) gene have been implicated inthis disorder. Published estimates of the prevalenceof this disorder remain surprisingly low consideringpathogenetic mutations in hir have been found indistinct ethnicities around the world. Therefore, it islikely that congenital atrichia with papular lesions isfar more common than previously thought and isoften mistaken for its phenocopy, the putative auto-immune form of alopecia universalis. To clarify thisdiscrepancy, we propose criteria for the clinical diag-nosis of congenital atrichia with papular lesions.
Among these is the novel report of the consistentobservation of hypopigmented whitish streaks on thescalp surface of affected individuals. Additionally, wereport the identi®cation of a novel missense muta-tion in hir from a family of Arab Palestinian originthat exhibits the pathognomonic features of atrichiawith papular lesions. Collectively, we anticipate thatan increased recognition of this disorder will resultin more accurate diagnosis and the sparing ofunnecessarily treatment to patients. Key words: alope-cia/atrichia with papular lesions/diagnosis/hairless/muta-tion. J Invest Dermatol 117:1662±1665, 2001
Atrichia with papular lesions (APL) (OMIM#209500) isa rare form of irreversible alopecia that is inherited inan autosomal recessive pattern (Fredrich, 1950;Damste and Prakken, 1954; Loewenthal and Prakken,1961). In individuals affected with this form of hair loss,
hairs are typically absent from the scalp, axilla, and body. Patients arealmost completely devoid of eyebrows and eyelashes. Histologicexamination of affected scalp skin shows the absence of mature hairfollicle structures. Although alopecia may accompany severaldifferent forms of congenital ectodermal dysplasias, APL patientsare unique in that, along with total atrichia, papules and follicularcysts ®lled with corni®ed material represent a unique cutaneousabnormality among inherited alopecias. Apparently normal hairs arepresent at birth in most APL patients, but these neonatal hairs areusually shed within the ®rst months of life and are never replaced. Inindividual cases, the shedding of the hair occurs during the ®rst 2±3 yof life. At approximately 2 y of age, affected patients begin to developmultiple follicular papules, and variations in the structure andmorphology of the hair follicle remnants have been reported.
Recently, we and others reported linkage of this form of atrichiato chromosome 8p12 (Ahmad et al, 1998a; Cichon et al, 1998;Sprecher et al, 1998), and subsequently, a large number ofmutations have been identi®ed in families from around the worldshowing a similar phenotype, thereby establishing the molecularbasis of this disorder (Ahmad et al, 1998a, 1999a, b; Cichon et al,1998; Zlotogorski et al, 1998; Kruse et al, 1999; Sprecher et al,1999a, b; Aita et al 2000). Yet despite its unique and homogenous
clinical picture, APL remains frequently misdiagnosed as itsphenocopy, the putative autoimmune disorder alopecia universalis.This may be due to several factors, including the perceived rarity ofthis disease, an incomplete clinical and/or histopathologic descrip-tion, and the lack of de®nitive criteria for diagnosis.
Here, we attempt to clarify the clinical picture and thenomenclature of this disease based on our personal observation ofnine Arab families and retrospective analysis of other familiesdescribed in the literature. Additionally, we report a novel missensemutation in an Arab Palestinian patient. These ®ndings extend thebody of evidence implicating mutations in the hairless gene as anunderlying cause of APL. Furthermore, we propose an algorithmthat easily differentiates this disorder from AU and other forms oftotal alopecia by the implementation of a set of de®nitive criteriafor the diagnosis of APL.
MATERIALS AND METHODS
Family history We studied an Arab Palestinian family originatingfrom a village near Jerusalem with a single female affected withcongenital atrichia (Fig 1A). The family history was signi®cant forparental consanguinity and consistent with autosomal recessiveinheritance. The proband was a 6-y-old-girl who was born with normalscalp hair, which began to shed during the second to third month(Fig 2). It progressed to complete and permanent hairlessness at the ageof 1 y. The patient did not respond to standard topical steriod therapyused for treatment of alopecia universalis.
Clinical material Blood samples were collected from the family anda scalp biopsy was performed in the proband to con®rm the diagnosis.Speci®cally, a punch biopsy was taken from the left parietal region of thescalp under local anesthesia. The sample was ®xed in 4%paraformaldehyde and embedded in paraf®n. Four micrometer sectionswere processed and stained with hematoxylin and eosin according tostandard protocols. All procedures were performed in accordance withthe guidelines of the local Institutional Review Board.
0022-202X/01/$15.00 ´ Copyright # 2001 by The Society for Investigative Dermatology, Inc.
1662
Manuscript received October 19, 2000; revised February 13, 2001;accepted for publication April 27, 2001.
Reprint requests to: Dr. Angela M. Christiano, Department ofDermatology, Columbia University, College of Physicians & Surgeons,630 West 168th Street VC15-1526, New York, NY, 10032. Email:[email protected]

Mutation detection To screen for a mutation in the hairless gene,PCR ampli®cation of all exons of the human hairless gene wereperformed as described previously (Ahmad et al, 1999a). PCR productswere sequenced directly in an ABI Prism 310 Automated Sequencer,using the ABI Prism Rhodamine Terminator Cycle Sequencing ReadyReaction Sequencing Kit (Applied Biosystems, Foster City, CA),following puri®cation in a Centri¯ex Gel Filtration Cartridges (EdgeBiosystems, Gaithersburg, MD). The mutation was veri®ed in thepatient, the parents, and unaffected, unrelated control individuals usingrestriction enzyme digestion with PmlI (New England Biolabs, Beverly,MA).
RESULTS
Clinical ®ndings consistent with papular atrichia At thetime of examination, very few hairs remained on the scalp of theproband (Fig 2A). Careful examination of this patient led to anovel clinical observation that has not been described earlier incongenital atrichia, namely, hypopigmented whitish streaks on thescalp surface (Fig 2A). Hair was absent from the axillae and otherparts of the body, and the eyebrows and eyelashes were sparse(Fig 2B). She had the additional characteristic feature of groupeddiffuse papular eruption of approximately 100 papules, which beganto appear at age 2, on the scalp, cheeks, arm, elbows, thighs, andknees (Fig 2C). The patient showed no growth or developmentaldelay, normal teeth and nails, and no abnormalities in sweating.
Histopathology of the scalp Histologic studies revealed anormal but slightly hyperkeratotic epidermis, normal sweat (swg)and sebaceous (sg) glands, and the absence of any signs ofin¯amation. Only small fragments of hair follicle epithelia(Fig 2D, arrowheads), however, were found on serial sections ofskin sample. Two remnants of the upper hair follicle portion(Figs 2D, 1 and 2) reminiscent of utriculi in hairless mouse skinwere found in the upper dermis. Both these remnants did notcontain hair shafts and instead were ®lled with amorphous corni®edmaterial.
Identi®cation of a mutation in the hairless gene Weidenti®ed a homozygous G-to-A transition at nucleotide 3166 inthe hairless gene leading to the conversion of a valine residue(GTG) to a methionine residue (ATG) (Fig 1B). This mutation,designated V1056M, abolishes a restriction endonuclease site forthe enzyme PmlI, which was used as a screening assay in 40Caucasian control individuals, and 98 Arab Palestinian controlindividuals, to rule out the possibility that this mutation is apolymorphism (Fig 1C). Furthermore, the mutation V1056Mresides in a region of the hairless protein (amino acids 946±1157)recently shown to have homology to the cupin family ofmetalloenzymes, which are candidates for enzymes that regulatechromatin remodeling and the integrity of chromatin structure(Clissold and Ponting, 2001). The absence of this mutation in 276alleles, the conservation of this amino acid across all species wherehairless has been cloned, and its location within a domain ofpotential important function, supports that it is the pathogeneticmutation in this family.
DISCUSSION
Establishing the diagnosis of a disease requires rigid criteria, andbased on the large number of families we have personally examinedand on the reported literature, we propose an algorithm ofdiagnostic criteria for congenital APL (Table I). The ®rst of theseis the importance of family history, including the pattern ofinheritance established as autosomal recessive, with careful ques-tioning for consanguinity. Another important hallmark of theclinical history is that patients were born either without hair or withnormal hair that is shed during the ®rst several months and neverregrew, and that papules started to appear during the ®rst years oflife. The examination should reveal the complete lack or nearcomplete lack of scalp hair, sparse eyebrows and eyelashes, and lackof secondary axillary, pubic, or body hair. In addition, small to largenumbers of papules should be found distributed over some or all ofthe following areas: scalp, cheeks, arms, elbows, buttocks, thighs,and knees, and of particular note, under the midline of the eye.Whitish hypopigmentary ®ne marks or streaks may be present on
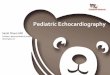
Figure 1. Genetic analysis of an Arab family with APL. (A) A pedigree representing a family with a single member affected with APL. Circlesand squares represent females and males, respectively. (B) Automated DNA sequence analysis of the hairless gene. DNA sequence of exon 16 fromcontrol, heterozygous carrier, and homozygous affected individuals. Note the arrow denoting the mutation at nucleotide position 3166 of the hairlesscDNA. (C) Restriction endonuclease analysis of the hairless gene with the enzyme Pml I. Note the mutation prevents cleavage by Pml I, resulting in a293 bp fragment. Wild-type alleles are cleaved into products of 122 bp and 171 bp.
VOL. 117, NO. 6 DECEMBER 2001 DIAGNOSTIC CRITERIA FOR CONGENITAL ATRICHIA 1663

the scalp, and patients should have normal nails, teeth, andsweating, and no major growth or developmental de®ciencies.Finally, two de®nitive laboratory tests include (i) a scalp biopsy toreveal the absence of hair follicles and the presence of cysts ®lledwith corni®ed material upon histologic examination, and (ii) themolecular diagnosis of mutations in the h gene.
We utilized these criteria in the identi®cation of a novel missensemutation in an Arab Palestinian patient now de®nitively diagnosedwith congential APL. The patient presented here exhibits thepathognomonic features of congenital APL. These include the
absence of scalp hair, following its shedding within the ®rst monthsof life, the persistence of papular lesions, and the histologydemonstrating the absence of mature hair follicles (Fig 2). Inaddition to the atrichia, the most characteristic feature of affectedindividuals with APL is the development of the corni®ed cysts,usually appearing by age 5 (Fig 2D). In our patient, the papulareruption started by age 2, and following repeated questioning ofother patients with APL, we discovered that papules may appeareven earlier, with a range between 1 and 10 y of age. In some cases,the lesions are few in number, and therefore are initially ignored by
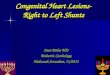
Figure 2. Clinical and histopathologic presentation of APL. (A) The scalp is almost completely devoid of hair, with few papules andhypopigmented whitish streaks. (B) Papules on the cheek. Note the common infra orbital location of papules. Sparse eyebrows and eyelashes are alsovisible. (C) Diffuse papular eruption on the upper arm. (D) Histologic examination reveals the complete absence of normal hair follicle structures. Notethe sebaceous glands (sg) and sweat glands (swg) appear normal.
Table I. Diagnostic criteria for APL
I. FAMILY HISTORY*Family history, pattern of inheritance established as autosomal recessive, possible history of consanguinity.*Patients are sometimes born without hair and none ever grows. More typically, patients are born with normal hair that shed after several months andnever regrow.*Papules that start to appear during the ®rst year of life, particularly under the midline of the eye, on the face, extremities.
II. EXAMINATION*Complete lack or almost complete lack of scalp hair.*Sparse eyebrows and eyelashes.*Lack of secondary axillary, pubic, or body hair.*Papules ± few to many distributed over some or all of the following areas: scalp, cheecks, arms, elbows, thighs, and knees.*Normal nails and teeth, normal sweating, and no growth or developmental problems.*Whitish hypopigmented streaks on the scalp.
III. LABORATORY TESTS*Lack of response to any treatment modality.*Biopsy ± absence of mature hair follicle structures, cysts ®lled with corni®ed material.*Mutation in the h gene.
1664 ZLOTOGORSKI ET AL THE JOURNAL OF INVESTIGATIVE DERMATOLOGY

the patients, the parents, and the clinician. In general, there is anincrease in the number of papules in the individual patient withage; however, there is a wide inter- and intrafamilial variability inthe number and distribution of papules on the body, which is notage related. Papules are observed mainly on the scalp, arms, elbows,thighs, knees, cheeks, and under the midline of the eye (Fig 2B,C).
Following examination of this patient, we noticed a clinical signthat was not described in earlier reports of APL, speci®cally,hypopigmented whitish streaks on the scalp surface (Fig 2A).These marks are also found in the other affected members of APLfamilies of Arab origin, as well as in the patients from previousreports of APL (Table I) and therefore we believe it is not anincidental ®nding. Hypopigmentation could develop as a secondarylesion (e.g., a post-in¯ammatory response), but none of our patientsadmitted scratching or in¯ammation. It is also noteworthy thatthese streaks are persistent and become a permanent feature of thescalp. In the future, it will be interesting to note whether atrichiapatients of non-Arab origin share these whitish streaks.
The mutation identi®ed in this study extends our knowledge ofmutations in the hairless gene which de®ne the pathogenetic basisof this disease. It is noteworthy that the clinical picture is identicalin patients carrying all types and combinations of mutations,including deletion, missense, splice site, and nonsense mutations(Ahmad et al, 1998a, b, 1999a, b; Cichon et al, 1998; Zlotogorski etal, 1998; Kruse et al, 1999; Sprecher et al, 1999a, b; Aita et al 2000).Speci®cally, based on examination of 10 Arab families, includingthe family in this report, we ®nd that the clinical phenotype ofcomplete scalp atrichia manifesting during the ®rst months, sparseeyebrows and eyelashes and papular eruption, is remarkablyconsistent irrespective of the type of mutation, and in contrast toprevious reports we observed no clinical evidence that wouldwarrant splitting the disease into subphenotypes on the basis of thetype of mutation and the number and distribution of papules(Zlotogorski et al, 1998; Ahmad et al, 1999a; Sprecher et al, 1999a,b). Unlike the paradigm in the mouse, where a splicing defectleading to reduction of hairless mRNA levels results in the hairlessmouse phenotype (Cachon-Gonzalez et al, 1994, 1999) andcomplete null mutations result in the more severe rhino phenotype(Ahmad et al, 1998c, d; Panteleyev et al, 1998c), such genotype-phenotype correlations have not yet emerged in human APL.
We have noticed two clinical features that display minorinterfamilial variation. These include (i) the amount of hair onthe scalp, ranging from complete absence to a few grouped hairsremaining on the vertex; and (ii) variability in the number anddistribution of the papules. Importantly, these variations do notdiffer from the intrafamilial variation, e.g., two affected members inthe same family may have 50 or 500 papules. Understanding thisvariation and taking into consideration the sometimes incompleteclinical phenotype description is crucial.
Furthermore, we have encountered several patients (A.Z.,A.M.C.) who have been mistakenly diagnosed as alopeciauniversalis, and treated accordingly. In fact, APL could easily bedismissed by the clinician as a case of AT/AU and the associatedpapular rash could be attributed to a form of keratosis pilaris as anexplanation for the papular lesions. We strongly urge thoseexamining these patients to use the guidelines we propose formaking the important distinction between APL and AT/AU. Webelieve that the phenotype of atrichia with papular lesion may bemore common than was earlier believed, and that in the nearfuture, clinicians will discover some APL patients that were labeledand treated accordingly as AU. Therefore, we propose the criteriaoutlined above so that patients with this disorder may be diagnosedaccurately and spared the battery of treatments that are destined tofail.
We thank HaMut Lam for expert technical assistance. We very much appreciate the
participation of the patient and family members in this study. We are grateful to Dr.
Benjamin Glaser, Jerusalem, Israel, for the generous gift of unrelated, unaffected
Arab control DNA. This work was supported in part by the National Alopecia
Areata Foundation (A.Z., A.M.C.), the Dermatology Foundation, and the NIH
Skin Disease Research Center Grant P30-44535 at Columbia University.
REFERENCES
Ahmad W, ul Haque MF, Brancolini V, et al. Alopecia universalis associated with amutation in the human hairless gene. Science 279:720±724, 1998a
Ahmad W, Irvine AD, Lam H, et al: A missense mutation in the zinc-®nger domainof the human hairless gene underlies congenital atrichia in a family of Irishtravelers. Am J Hum Genet 63:984±991, 1998b
Ahmad W, Panteleyev A, Sundberg JP, Christiano AM: Molecular basis for the rhino(hr rh8J) phenotype: a nonsense mutation in the mouse hairless gene. Genomics53:383±386, 1998c
Ahmad W, Panteleyev A, Henson-Apollonio V, Sundberg JP, Christiano AM:Molecular basis of a novel rhino (hr rhChr) phenotype: a nonsense mutation inthe mouse hairless gene. Exp Dermatol 7:281±288, 1998d
Ahmad W, Zlotogorski A, Panteleyev A, et al: Genomic organization of the humanhairless gene and identi®cation of a mutation underlying congenital atrichia inan Arab Palestinian family. Genomics 56:141±148, 1999a
Ahmad W, Nomura K, McGrath JA, Hashimoto I, Christiano AM: A homozygousnonsense mutation in the zinc-®nger domain of the human hairless geneunderlies congenital atrichia. J Invest Dermatol 113:281±283, 1999b
Aita VM, Ahmad W, Panteleyev AA, et al: A novel missense mutation (C622G) inthe zinc-®nger domain of the human hairless gene associated with congenitalatrichia with papular lesions. Exp Dermatol 9:157±162, 2000
Cachon-Gonzalez MB, Fenner S, Cof®n JM, Moran C, Best S, Stoye JP: Structureand expression of the hairless gene of mice. Proc Natl Acad Sci USA 91:7717±7721, 1994
Cachon-Gonzalez MB, San-Jose I, Cano A, et al: The hairless gene of the mouse:relationship of phenotypic effects with expression pro®le and genotype. DevDyn 216:113±126, 1999
Cichon S, Anker M, Vogt IR, et al: Cloning, genomic organization, alternativetranscripts and mutational analysis of the gene responsible for autosomalrecessive universal congenital alopecia. Hum Mol Genet 7:1671±1679, 1998
Clissold PM, Ponting CP: JmjC. cupin metalloenzyme-like domains in jumonji,hairless and phospholipase A2b. Trends Biochem Sci 26:7±9, 2001
Damste J, Prakken JR: Atrichia with papular lesions. a variant of congenitalectodermal dysplasias. Dermatologica 108:114±117, 1954
Fredrich HC: Zur Kenntnis der Kongenitale Hypotrichosis. Dermatol Wochenschr121:408±410, 1950
Kruse R, Cichon S, Anker M, et al: Novel hairless mutations in two kindreds withautosomal recessive papular atrichia. J Invest Dermatol 113:954±959, 1999
Lowenthal LJA, Prakken JR: Atrichia with papular lesions. Dermatologica 122:85±87,1961
Panteleyev AA, Paus R, Ahmad W, Sundberg JP, Christiano AM: Molecular andfunctional aspects of the hairless (hr) gene in laboratory rodents and humans.Exp Dermatol 7:249±267, 1998a
Panteleyev AA, van der Veen C, Rosenbach T, Muller-Rover S, Sokolov VE, PausR: Towards de®ning the pathogenesis of the hairless phenotype. J InvestDermatol 110:903±907, 1998b
Panteleyev AA, Ahmad W, Malashenko AM, Ignatieva EL, Paus R, Sundberg JP,Christiano AM: Molecular basis for the rhino Yurlovo (hr rhY) phenotype:severe skin abnormalities and female reproductive defects associated with aninsertion in the hairless gene. Exp Dermatol 7:281±288, 1998c
Sprecher E, Bergman R, Szargel R, et al: Atrichia with papular lesions maps to 8p inthe region containing the human hairless gene. Am J Med Genet 80:546±545,1998
Sprecher E, Bergman R, Szargel R, Friedman-Birnbaum R, Cohen N: Identi®cationof a genetic defect in the hairless gene in atrichia with papular lesions: evidencefor phenotypic heterogeneity among inherited atrichias. Am J Hum Genet64:1323±1329, 1999a
Sprecher E, Lestringant GG, Szargel R, et al: Atrichia with papular lesions resultingfrom a nonsense mutation within the human hairless gene. J Invest Dermatol113:687±690, 1999b
Sprecher E, Lestringant GG, Szargel R, et al: Reply to ``Settling the score onhairless''. J Invest Dermatol 115:762±763, 2000
Sundberg JP, Dunstan RW, Compton JG: Hairless mouse, HRS/J hr/hr. In: TCJones, U Mohr, RD Hunt, eds. Monographs on Pathology of Laboratory Animals.Integument and Mammary Glands. Heidelberg: Springer-Verlag, 1989, pp 192±197
Zlotogorski A, Ahmad W, Christiano AM: Congenital atrichia in ®ve ArabPalestinian families resulting from a deletion mutation in the human hairlessgene. Hum Genet 103:400±404, 1998
VOL. 117, NO. 6 DECEMBER 2001 DIAGNOSTIC CRITERIA FOR CONGENITAL ATRICHIA 1665