Embed Size (px)
Citation preview

부산대병원학술지 통권 제37호, 2015
- 261 -
부산대학교 어린이병원 소아청소년과
이 연 주
Lee Yeoun joo
Department of Pediatrics, Pusan National University Children’s Hospital
Chronic abdominal pain is a common symptom in children and adolescents. Among
children and adolescents who have abdominal pain, only 9-19% reveal an organic
cause and remaining patients show functional abdominal pain. Red flag signs are very
helpful to identify organic cause of chronic abdominal pain. Physicians always remind
of red flag signs, in doing history taking and physical examination. Patients who do
not reveal red flag signs are tend to have functional abdominal pain. Functional
abdominal pain is reinforced by ‘Brain-Gut axis’. After diagnosing functional
abdominal pain, diagnostic test should not be done frequently. In functional
*본 연구는 2014년도 양산부산대학교병원 임상연구비 지원으로 이루어졌음.

이 연 주
- 262 -
abdominal pain, education and reassurance of patients and their parents is the most
important treatment.
Key words: Abdominal pain; child
복통은 소아청소년과 진료실에서 흔히 만날
수 있다. 주로 5세 이상의 소아에서 지속적이
거나 간헐적으로 3개월 이상 나타나는 경우
만성 복통으로 칭한다. (Table 1) 만성 재발
성 복통은 어린이의 9-15%, 중학생의 13%,
고등학생의 17%가 경험하는 흔한 증세이다.
만성 복통을 경험하는 소아는 건강한 소아에
비해 신체적, 정신적, 사회적, 학교생활에서
현저한 불편을 경험하는 것으로 나타나는데,1
이는 경제적인 비용부담과 함께 부모의 직장
생활에도 영향을 끼쳐 궁극적으로 가족 구성
원 전체의 삶의 질에도 영향을 미친다.2 하지
만, 기질적 원인을 나타내는 만성 복통은 병·
의원을 방문하는 만성 복통 환자의 15% 안팎
에 지나지 않으며,3 80~90%를 차지하는 대다
수의 환자는 만성 비기질성 복통을 보인다.
최근의 미국 대규모 연구에 따르면, 기능성
복통 환자군이 기질적인 원인을 가지는 복통
환자군보다 오히려 삶의 질이 현저히 떨어지
는 것으로 나타났으며, 보호자의 사회생활에
끼치는 영향도 더 큰 것으로 나타났다.2
따라서, 소아의 만성 복통의 기질적, 비기질
적 원인에 대해 적절히 감별할 수 있어야 하
고, 비기질적 원인에 대하여서도 그 기전과
예후에 대해 이해함으로써 환자와 보호자에게
적절한 상담을 하는 것은 매우 중요한 일이라
하겠다. 본 원고에서는 만성 복통 환자에서
기질적 원인을 감별점과 기능성 복통의 기전
및 치료에 대하여 기술하고자 한다.
1. 만성 복통의 감별진단
만성 복통과 관련하여 다양한 용어가 혼용되
어 사용되고 있지만 교과서적으로 Table 1에
기술된 용어들이 대표적으로 사용된다. 이 중
기능성 위장관 질환은 Rome III criteria에서
더 세분화하여 나누어 정리하고 있다.(Table
2, 3) 기질적 질환이 있는 경우는 복통을 유
발하는 상황에 따라 위장관 질환과 관련된 복
통, 간·담·췌 관련 통증, 비뇨생식계 질환 관
련 통증 및 기타 전신적인 원인 관련 복통으
로 나누어 생각할 수 있다.(Table 4)
환자가 복통을 주소로 진료실에 내원한 경우
첫째, 복통이 발생한 시점을 통해 급성인지
만성인지를 구분한다. 만성 복통일 경우 둘째,
문진과 진찰을 통해 Table 5, 6에 나타난 적
색 신호 소견이 나타나는지 확인한다. 셋째,
적색 신호가 나타나는 경우 Table 4에서 특
정 질환을 시사하지 않는지를 고려하여 의심
되는 질환에 따라 추가적인 경험적 치료나 진
단적 접근을 고려한다. 넷째, 적색 신호가 나
타나지 않는 경우 증상에 대한 구체적인 문진
을 통해 Table 2, 3에 해당하는 기능성 복통
의 가지를 분유한다. 다섯 째, 적색 신호가 나

만성 복통을 호소하는 소아 청소년 환자의 임상적 접근법
- 263 -
타나지 않더라도 환자의 증세가심하거나 점점
악화되는 양상의 경우 추가적인 검사를 고려
할 수 있고, 시간을 갖고 주의 깊게 추적 관
찰한다.
간혹 특정 검사에서 이상 소견이 발견될 경
우 발견된 소견이 복통의 원인이라 단정해 버
리는 경우가 있을 수 있다. 예로 복통이 있는
환자에서 복부 초음파를 시행하여 담석을 발
견한 경우, 담석이 복통의 원인이라 단정 짓
기 쉽다. 하지만 담낭염이나 췌장염이 동반되
지 않은 담석은 복통을 일으킬 가능성이 떨어
지며, 황달, 식후 악화되는 통증, 우상복부 압
통이나 Murphy’s sign 등의 진찰 소견이 동
반되지 않으면 담석은 단지 우연히 발견된 소
견일 확률이 높다. 기질적 질환이 있더라도
기능성 복통이 함께 있는 경우는 흔하기 때문
에, 검사에서 나타난 소견과 복통의 양상을
면밀히 관찰하여 연관성을 확인하는 것은 굉
장히 중요한 사항이다.
소아·청소년기에 만성 복통으로 나타날 수
있는 대표적인 질환인 크론병의 경우, 복통과
함께 빈혈, 혈변과체중감소가 가장 주된 적색
신호이며,4 항문 주위의 수술력이나 크론병의
가족력은 크론병의 가능성을 강력히 시사하는
소견이므로 적절한 검사를 통해 꼭 감별진단
하여야 한다.
2. 기능성 복통
복통 환자에서 기질적 원인을 찾을 수 없는
경우, 비 기질적 복통으로 생각되는데, 재발성
복통, 만성 복통, 기능성 복통, 비기질성 복통
또는 심리적 원인의 복통이라는 다양한 표현
이 사용되어 왔다. Rome III로 대변되는 기
능성 위장관 질환에서는 소아와 청소년과 관
련된 기능성 질환을 H 항목에서 기술을 하고
있고, 특히 복통과 관련하여 H2로 기술하고
있다.(Table 2, 3) 구조적인 이상이 있는 질
환이나 염증과 같은 질환은 병리나 진단검사
를 통해서 이름 붙일만한 탄탄한 근거가 있지
만, 이런 기능성 질환은 수많은 연구에도 불
구하고 여전히 애매하고 설명하기 힘든 질환
군이다.
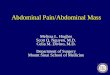
기능성 위장관 질환은 유전적 환경적 요인
위에 심리사회적 요인과 물리적 요인이 합쳐
져 발생한다고 생각된다.(Fig. 1) 유아기에 겪
었던 경험은 이후 심리사회적으로 발달하는데
큰 영향을 미친다. 질병에 걸렸을 때 가족의
과도한 반응, 큰 상실감, 약물의 남용, 감염에
의 노출은 커가면서 스트레스나 심리사회적
상태에 대해 예민해지게끔 만든다. 또한 장관
의 움직임, 점막의 면역성, 내장 과민성에도영
향을 끼쳐 더 민감하게끔 만든다. 게다가 뇌
에서 장으로 연결되는 ‘뇌-장 축’ 통로는 그러
한 표현을 상호적으로 강화시켜서 정착되게끔
만든다.5 그러므로 기능성 위장관 질환은 심리
사회적인 요인과 이것으로 인해 예민해진 장
관의 생리가 뇌-장 축을 통해서 계속 강화되
는 쪽으로 학습되는 것으로 설명할 수 있다.
원인 병원체가 확인된 감염성 장염 이후 과민
성 대장 증후군 환자의 빈도가 현저히 올라갔
다는 보고들이 이를 뒷받침해 준다.6
기질적 원인이 배제된 뒤 기능성 복통으로
진단을 한 이후에는 환자를 자주 방문시키거
나 검사를 하지 않도록 하여야 한다. 잦은 병
원 방문과 검사는 환자로 하여금 자신의 증세
에 집중하고, 증상을 크게 느끼고, 의료진이
진단에 대하여 자신이 없어한다고 생각하게
만든다.
기능성 복통을 완치시킬 수 있는 간단한 방
법은 없다. 기능성 복통 환자와는 신뢰와 공

이 연 주
- 264 -
감의 바탕에서 적절한 상담이 이루어져야 한
다. 환자로 하여금 자신의 증상이 위험하지
않으므로 안심하도록 하고, 증세를 악화시킬
만한 특정한 문제를 해소시키는 것에 중점을
두어야 한다. 통증이 어떻게 발생되며 환자가
어떻게 이를 인지하는지를 설명하여 주고, 만
성 복통으로 인해 발생할 수 있는 학업의 중
단, 사회 활동의 단절이 일어나지 않도록 하
는 것이 좋다. 일상생활의 모든 활동에 참여
하고 빠지지 않으면서 자신의 증상을 조절하
고 인내할 수 있도록 한다. 이러한 치료적 전
략은 Table 7에 기술되어 있다.
진통제, 위산 분비 억제제나 항 우울제와 같
은 약물이 때로 효과적일 수도 있으나, 환자
로 하여금 질환에 대해 집중하게 만들 수 있
으므로 주의하여야 한다. 증세가 지속적이고,
우울감이 동반되어 있거나 가족이나 학교생활
에 현저한 장애가 있는 경우는 정산건강의학
과에 의뢰하여 추가적인 진찰과 치료를 받게
유도할 수 있다. 7학교에서 담임선생님이나
보건실 담당자에게 환자의 상태를 공유하여
협조를 구하는 것도 환자, 보호자와 함께 상
의해 볼 수 있다.
만성 복통은 흔한 증세이나 실제로 기질적인
질환을 가지고 있을 확률은 9~19% 이다. 적
색 깃발신호는 기질적 질환의 가능성을 구분
해 내는 데 유용한 지표이므로 항상 염두에
두어야 한다. 기질적 질환이 의심되면 적절한
진단과 치료를 받을 수 있도록 방향을 제시하
여 주어야 하며, 기능성 복통이 의심되는 환
자에게도 질환의 기전에 대해 설명하여 환자
가 불안해하지 않도록 충분한 설명과 교육이
필요하다.
만성 복통은 소아청소년에서 흔하게 나타나
는 질환이다. 만성 복통 중 기질적 원인을 가
지는 복통은 전체의 9-19% 에 지나지 않고,
대부분은 기능성 복통이다. 기질적 원인을 가
지는 환자를 감별하기 위하여서는 적색깃발
신호를 염두에 두고 병력청취와 신체검사를
시행하여야 한다. 적색깃발 신호가 없는 경우
는 기능성 복통의 가능성이 높다. 기능성 복
통은 ‘뇌-장 축’을 따라 점차 강화되는 경향을
가지므로 기능성 복통으로 진단하면 가능한
한 진단적인 검사를 자주하지 않고 환자와 보
호자에게 질환의 경과에 대해 교육하고 안심
시켜 주는 것이 필요하다.
1. Petersen S, Hagglof BL, Bergstrom EI.
Impaired health-related quality of life in
children with recurrent pain. Pediatrics
2009; 124(4): e759-67.
2. Varni JW, Bendo CB, Nurko S et al.
Health-related quality of life in pediatric
patients with functional and organic
gastrointestinal diseases. J Pediatr 2015;
166(1): 85-90.
3. Han JJ YH, Ko JS, Seo JK. Chronic
Abdominal Pain-related Childhood Functional
Gastrointestinal Disorders Based on the

만성 복통을 호소하는 소아 청소년 환자의 임상적 접근법
- 265 -
Rome III Criteria in Korea. Korean J
Pediatr Gastroenterol Nutr 2009; 12(2): 111
∼9.
4. El-Chammas K, Majeskie A, Simpson P,
Sood M, Miranda A. Red flags in children
with chronic abdominal pain and Crohn's
disease-a single center experience. J Pediatr
2013; 162(4): 783-7.
5. Mayer EA, Tillisch K. The brain-gut axis in
abdominal pain syndromes. Annu Rev Med
2011; 62: 381-96.
6. Spiller R. Postinfectious functional dyspepsia
and postinfectious irritable bowel syndrome:
different symptoms but similar risk factors.
Gastroenterology 2010; 138(5): 1660-3.
7. Eccleston C, Palermo TM, Williams AC et al.
Psychological therapies for the management
of chronic and recurrent pain in children
and adolescents. Cochrane Database Syst
Rev 2014; 5: CD003968.
8. Di Lorenzo C, Colletti RB, Lehmann HP et
al. Chronic abdominal pain in children: a
clinical report of the American Academy of
Pediatrics and the North American Society
for Pediatric Gastroenterology, Hepatology
and Nutrition. J Pediatr Gastroenterol Nutr
2005; 40(3): 245-8.
9. Drossman DA. The functional gastrointestinal
disorders and the Rome III process.
Gastroenterology 2006; 130(5): 1377-90.
10. Kliegman RM SB, St. Geme JW, Schor
NF. Nelson textboom of Pediatrics, 19th
Edition, Philadelphia; Elsevier Saunders.
2011; 1247-8.
11. Taminiau J, Benninga M. Pediatric clinical
research will benefit from Rome III. J
Pediatr Gastroenterol Nutr 2005; 41 Suppl
1: S30-1.

이 연 주
- 266 -
Table 1. Recommended Clinical Definitions of Long-Lasting Intermittent or Constant
Abdominal Pain in Children.8
Chronic abdominal pain
Long-lasting intermittent or constant abdominal pain that is functional or organic (disease-based).
Functional abdominal pain
Abdominal pain without demonstrable evidence of a pathologic condition, such as an anatomic, metabolic, infectious, inflammatory or neoplastic disorder. Functional abdominal pain may present with symptoms typical of functional dyspepsia, irritable bowel syndrome, abdominal migraine, or functional abdominal pain syndrome.
Functional dyspepsia Functional abdominal pain or discomfort in the upper abdomen.
Irritable bowel syndrome
Functional abdominal pain associated with alteration in bowel movements.
Abdominal migraine Functional abdominal pain with features of migraine (paroxysmal abdominal pain associated with anorexia, nausea, vomiting or pallor as well as a maternal history of migraine headaches).
Functional abdominal pain syndrome
Functional abdominal pain without the characteristics of dyspepsia, irritable bowel syndrome, or abdominal migraine.
Table 2. Rome III Functional Gastrointestinal Disorders in Children and Adolescents9
H. Functional disroders: children and adolescents
H1. Vomiting and aerophagia
H1a. Adolescent rumination syndrome
H1b. Cyclic vomiting syndrome
H1c. Aerophagia
H2. Abdominal pain-related FGIDs
H2a. Functional dyspepsia
H2b. Irritable bowel syndrome
H2c. Abdominal migraine
H2d. Childhood functional abdominal pain
H2d1. Childhood functional abdominal pain syndrome
H3. Constipation and incontinence
H3a. Functional constipation
H3b. Nonretentive fecal incontinence

만성 복통을 호소하는 소아 청소년 환자의 임상적 접근법
- 267 -
Table 3. Rome III Criteria for Childhood Functional Abdominal Pain H2d and
Childhood Functional Abdominal Pain Syndrome H2d19
H2d. CHILDHOOD FUNCTIONAL ABDOMINAL PAIN
Diagnostic criteria must include all of the following;
∙ Episodic or continuous abdominal pain ∙ Insufficient criteria for other FGIDs ∙ No evidence of an inflammatory, anatomic, metabolic or neoplastic process that
explains the subject’s symptom
H2d1. CHILDHOOD FUNCTIONAL ABDOMINAL PAIN SYNDROME
Diagnostic criteria must satisfy criteria for childhood functional abdominal pain
and have at least 25% of the time one or more of the following:
∙ Some loss of daily function ∙ Additional somatic symptoms such as headache, limb pain, or difficulty sleeping

이 연 주
- 268 -
Table 4. Physiologic Causes of Chronic Abdominal Pain10
DISORDER CHARACTERISTICS
NONORGANIC
Functional abdominal pain Nonspecific pain, often periumbilicalIrritable bowel syndrome Intermittent cramps, diarrhea, and constipationNon-ulcer dyspepsia Peptic ulcer–like symptoms without abnormalities on evaluation
of the upper GI tract
GASTROINTESTINAL TRACT
Chronic constipation Hx of stool retention, evidence of constipation on examinationLactose intolerance Symptoms may be associated with lactose ingestion; bloating,
gas, cramps, and diarrheaParasite infection (especially Giardia)
Bloating, gas, cramps, and diarrhea
Excess fructose or sorbitol ingestion
Nonspecific abdominal pain, bloating, gas, and diarrhea
Crohn disease Anemia, hematochezia, diarrhea, weight loss, perianal diseasePeptic ulcer Burning or gnawing epigastric pain; worse on awakening or
before meals; relieved with antacidsEsophagitis Epigastric pain with substernal burningMeckel’s diverticulum Periumbilical or lower abdominal pain; may have blood in stoolRecurrent intussusception Paroxysmal severe cramping abdominal pain; blood may be
present in stool with episodeInternal, inguinal, or abdominal wall hernia
Dull abdomen or abdominal wall pain
Chronic appendicitis or appendiceal mucocele
Recurrent RLQ pain; often incorrectly diagnosed, may be rare cause of abdominal pain
GALLBLADDER AND PANCREAS
Cholelithiasis RUQ pain, might worsen with mealsCholedochal cyst RUQ pain, mass ± elevated bilirubinRecurrent pancreatitis Persistent boring pain, might radiate to back, vomiting
GENITOURINARY TRACT
Urinary tract infection Dull suprapubic pain, flank painHydronephrosis Unilateral abdominal or flank painUrolithiasis Progressive, severe pain; flank to inguinal region to testicleOther genitourinary disorders
Suprapubic or lower abdominal pain; genitourinary symptoms
MISCELLANEOUS CAUSESAbdominal migraine Nnausea, family History of migraineAbdominal epilepsy Might have seizure prodromeLead poisoning Vague abdominal pain ± constipationHenoch-Schönlein purpura Recurrent, severe crampy abdominal pain, occult blood in stool,
characteristic rash, arthritis

만성 복통을 호소하는 소아 청소년 환자의 임상적 접근법
- 269 -
Table 5. Alarm Symptoms Usually Needing Further Investigations10
Painthat wakes up the child from sleep
Persistent right upper or right lower quadrantpain
Significant vomiting (bilious vomiting, protracted vomiting, cyclical vomiting or
worrisome pattern to the physician)
Unexplained fever
Genitourinary tract symptoms
Dysphagia
Chronic severe diarrhea or nocturnal diarrhea
Gastrointestinal blood loss
Involuntary weight loss
Deceleration of linear growth
Delayed puberty
Family history of inflammatory bowel disease, celiac disease, and peptic ulcer disease
Table 6. Alarm Signs Usually Needing Further Investigations10
Localized tenderness in the right upper quadrant
Localized tenderness in the right lower quadrant
Localized fullness or mass
Hepatomegaly
Splenomegaly
Jaundice
Costovertebral angle tenderness
Arthritis
Spinal tenderness
Perianal disease
Abnormal or unexplained physical findings

이 연 주
- 270 -
Table 7. Guidelines to Establish a Therapeutic Physician-Patient Relationship9
1. Obtain the history through a nondirective, nonjudgmental, patient-centered interview.
2. Conduct a careful examination and cost-efficient investigation.
3. Determine how much the patient understands about the illness and his or her concerns
("What do you think is causing your symptoms?"
4. Provide a thorough explanation of the disorder that takes into consideration the patient’s
beliefs.
5. Identify and respond realistically to the patient’s expectations for improvement ("How do
you feel I can be helpful to you?").
6. When possible, provide a link between stressors and symptoms that are consistent with
the patient’s beliefs ("I understand you don’t think stress is causing your pain, but the
pain itself is so severe and disabling that it’s causing you a great deal of distress.").
7. Set consistent limits ("I appreciate how bad the pain must be, but narcotic medication is
not indicated.").
8. Involve the patient in the treatment ("Let me suggest some treatments for you to
consider.").
9. Make recommendations consistent with patient interests ("Antidepressants can be used for
depression, but they are also used to "turn down"the pain and in doses lower than that
used for depression.").
10. Establish a long-term relationship with a primary care provider.

만성 복통을 호소하는 소아 청소년 환자의 임상적 접근법
- 271 -
Figure 1. This biopsychosocial conceptualization of the pathogenesis and clinical
expression of the functional GI disorders (FGID) shows the relationships
between psychosocial and physiological factors, functional GI symptoms, and
clinical outcomes.11