Embed Size (px)
Citation preview
1
Clinical Approach to theClinical Approach to the Patient with Kidney Disease –
Hematuria, Proteinuria, Elevated Serum Creatinine and Diabetic Nephropathy
1 DOS CME Course 20111 Oxtober 20101Confidential
Presenter name: Marc A. Pohl, MD Presenter title: Ray W. Gifford Chair in Hypertension, and Head, Section of
Clinical Hypertension Department: Nephrology and Hypertension Institute Glickman Urological & Kidney Institute
© Cleveland Clinic 2011
THE FOUR QUESTIONS
1. Is there or is there not evidence of kidney (renal) parenchymal disease?parenchymal disease?
2. If kidney parenchymal disease is present, where within the kidney, is the primary pathology?
3. Is there evidence of reduced kidney function (i.e., reduction of glomerular filtration rate [GFR])?
2
( , g [ ])
4. Why is the detection of kidney disease and/or reduced kidney function important?
DOS CME Course 2011
2
3 DOS CME Course 2011
4 DOS CME Course 2011
3
5 DOS CME Course 2011
6 DOS CME Course 2011
4
HOW DO WE DETECT KIDNEY DISEASE AND/OR REDUCED KIDNEY FUNCTION?
• Urinalysis
• Presence or absence of proteinuria
• Assessment of the kidney’s filtering ability, i.e.,glomerular filtration rate (GFR)
– Serum creatinine
7
– BUN
– Mathematically estimated or measured GFR
DOS CME Course 2011
HEMATURIA
Every Life Deserves World Class CareEvery Life Deserves World Class Care
8 DOS CME Course 20118 DOS CME Course 2011
5
Hematuria: Definition
St i tl d fi d h t i i “bl d i th i ”• Strictly defined, hematuria is “blood in the urine.”
In conventional use, it means an abnormal
number of red blood cells in the urine.
9 DOS CME Course 2011
Hematuria: What is normal?
• <2 erythrocyte per high power field (? Higher in females) in a “urine sediment” re-suspended inin females) in a urine sediment re-suspended in a small volume (K0.5 mL) of an aliquot of a freshly-voided sample (10 mL) after light centrifugation (400G x 10 min) (Fogazzi, 1999)
10 DOS CME Course 2011
6
Hematuria: Caveats
• 2nd morning voided (mid-stream) specimens are best.
• Always examine urine fresh (within 1 2 hrs never stored• Always examine urine fresh (within 1-2 hrs., never stored in refrigerator).
• Avoid strenuous exercise before giving sample.
• Do not examine urine during menstruation in females.
• Catheterized samples of urine are unreliable.
11
Catheterized samples of urine are unreliable.
• Urine should be concentrated and acidic.
DOS CME Course 2011
Hematuria: “Dipstick”
• Commercial “dipsticks” detect 1-2 erythrocytes (in reality heme in erythrocytes) per HPF and are as sensitive as urinary sediment exams for detecting hematuria, BUT
• False negative for erythrocytes) may occur with:
– Consumption of large amounts of Vitamin C
• False positives (for erythrocytes) may occur with:– Semen contamination– Alkaline urine (pH >8.0)
12
(p )– Oxidizing agent contamination (cleansing agents)– Hemoglobinuria or myoglobinuria
DOS CME Course 2011
7
Pigmenturia
• Red or red-brown urine and negative dipstick may be seen inseen in:
–Porphyrinuria
–Rhubarb, senna or beetroot ingestion
–Aminopyrine, diphenylhydantoin, phenolsulfonpthathalein, metronidazole, nitrofurantoin
13
p p , ,phenacetin, phenothiazine, rifampicin, salazosulfapyridine administration
DOS CME Course 2011
Hemoglobinuria and Myoglobinuria:
Clinical Differentiation
HEMOGLOBINURIA
• Urine red (alkaline) or red-brown (acid), heme-positive (diffuse not kl d) th t i ispeckled); no erythrocytes in urine
• Plasma pink
• Serum haptoglobin levels decreased
• Serum creatine phosphokinase levels normal
MYOGLOBINURIA
• Urine red or reddish –brown; heme-positive (diffuse not speckled; no
14
erythrocytes in urine
• Plasma clear
• Serum haptoglobin levels normal
• Serum creatine phosphokinase levels increased.
DOS CME Course 2011
8
Hematuria: Sequencing of Tests
If dipstick is positive for blood, immediate microscopy of a p p , py
fresh urinary sediment (not stored for later examination) is
the most cost-effective approach.
(NHS-Office of Health Technology Assessment, 2006)
15 DOS CME Course 2011
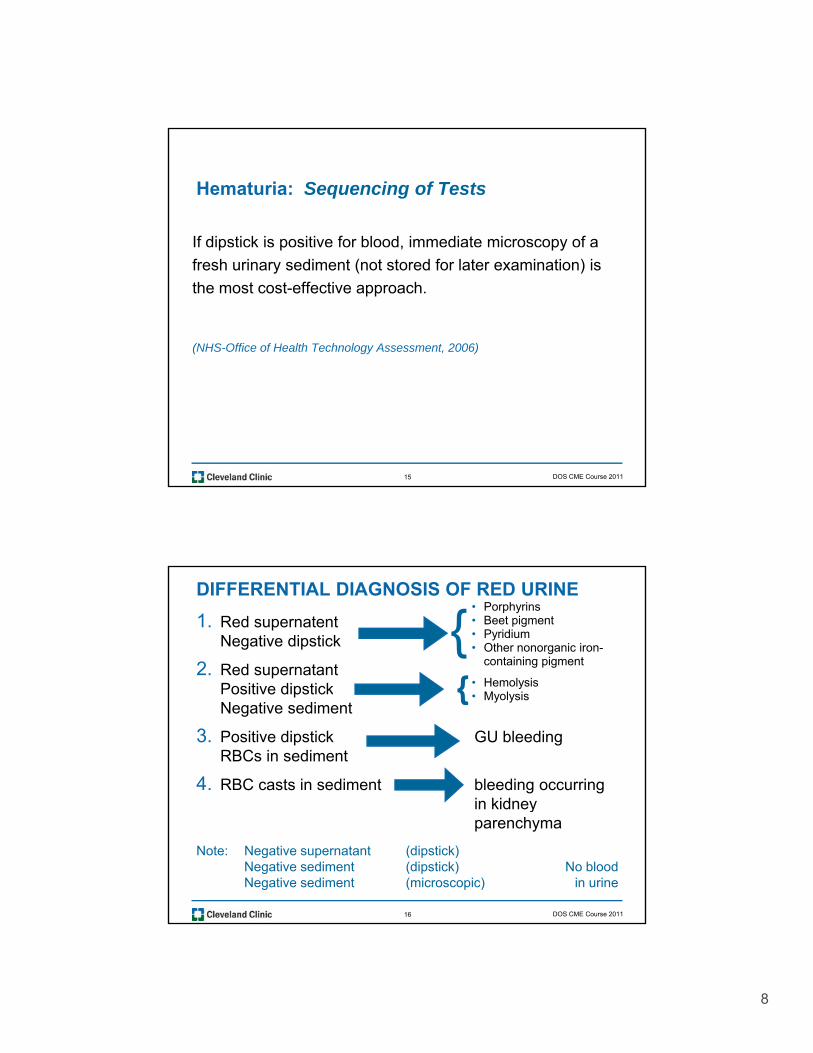
DIFFERENTIAL DIAGNOSIS OF RED URINE
1. Red supernatentNegative dipstick
2. Red supernatantP iti di ti k
• Porphyrins• Beet pigment• Pyridium• Other nonorganic iron-
containing pigment
• Hemolysis{
{Positive dipstickNegative sediment
3. Positive dipstick GU bleedingRBCs in sediment
4. RBC casts in sediment bleeding occurringin kidney
Hemolysis• Myolysis {
16
in kidney parenchyma
Note: Negative supernatant (dipstick)Negative sediment (dipstick) No bloodNegative sediment (microscopic) in urine
DOS CME Course 2011
9
Causes of Hematuria
• Infections– Pyelonephritis cystitis
• Glomerular
• Vascular– Renal vein thrombosis
– Atheroemboli
Malignant hypertension– Glomerulonephritis
– Hereditary glomerular diseases line think basement membrane and Alport’s disease
– Vasculitis
• Interstitial– AIN
– Malignant hypertension
• Malignancy– Renal cell carcinoma
– Transitional cell carcinoma
– Carcinoma of prostate
• Others– Calculi
17
– PKD
– Papillary necrosis
– Calculi– Hypercalcemia– Hypercalciuria– Hyperuricemia– Coagulopathy – Cytoxan
DOS CME Course 2011
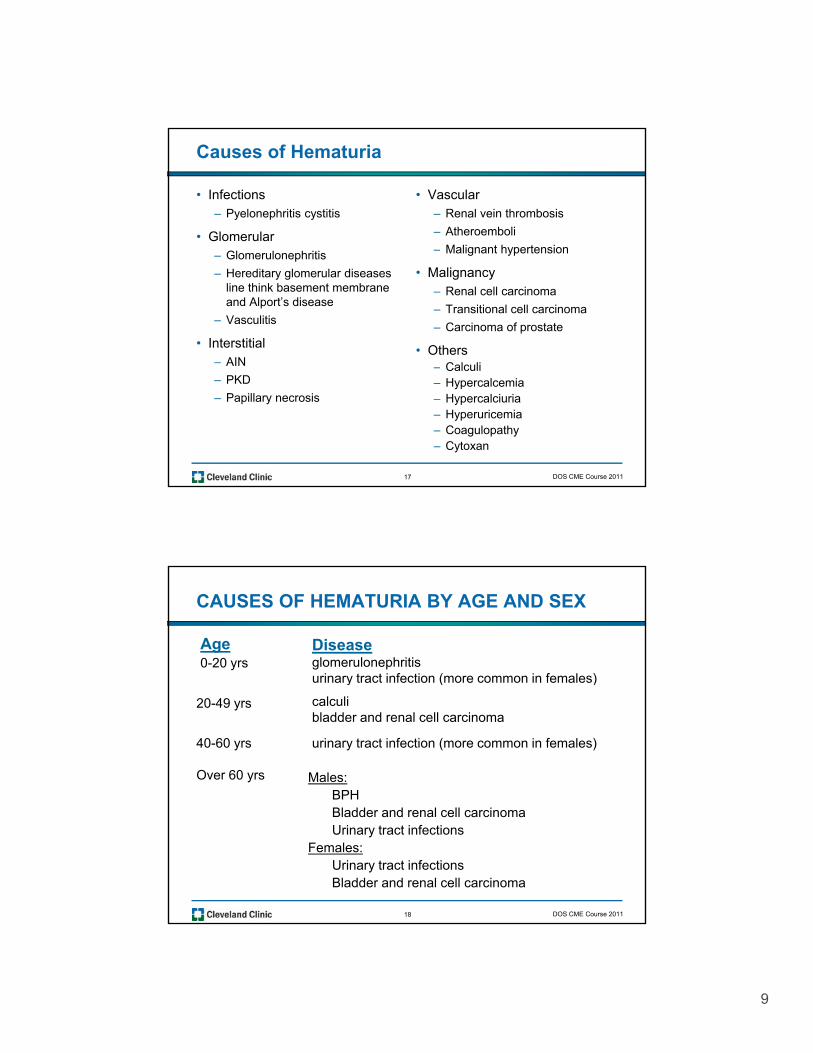
CAUSES OF HEMATURIA BY AGE AND SEX
Age0-20 yrs
Diseaseglomerulonephritisurinary tract infection (more common in females)y ( )
calculibladder and renal cell carcinoma
20-49 yrs
40-60 yrs urinary tract infection (more common in females)
Over 60 yrs Males:BPH
18
Bladder and renal cell carcinomaUrinary tract infections
Females:Urinary tract infectionsBladder and renal cell carcinoma
DOS CME Course 2011
10
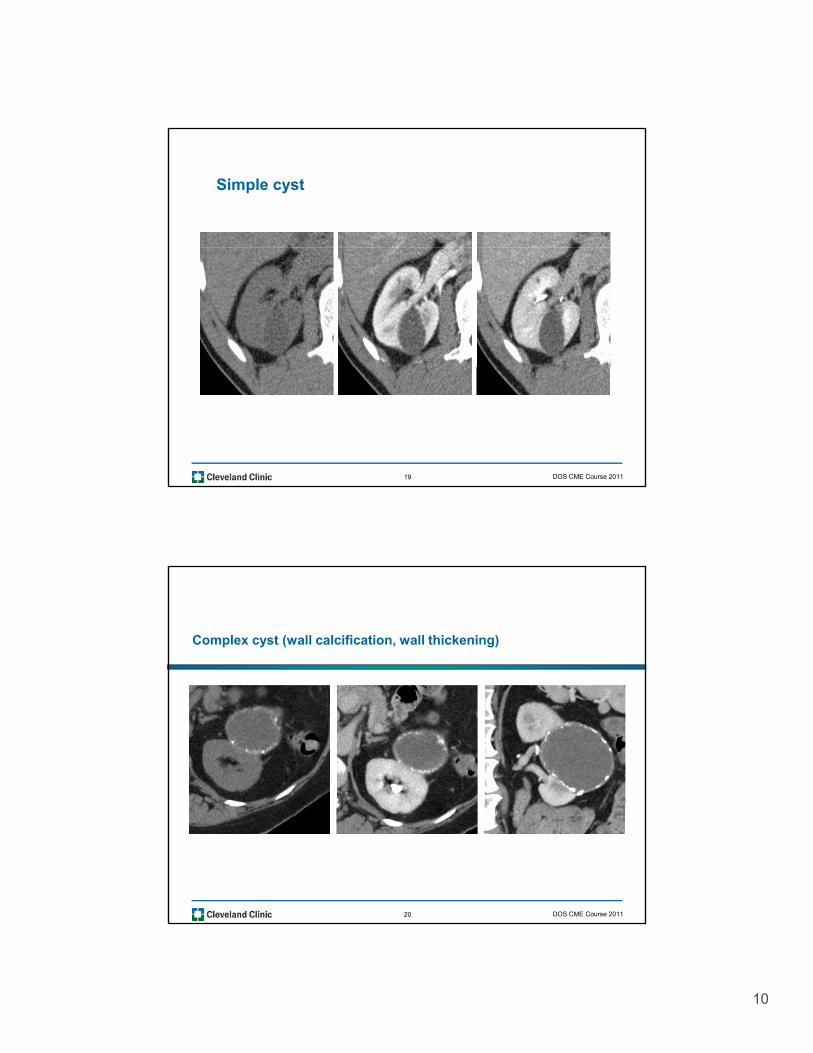
Simple cyst
19 DOS CME Course 2011
Complex cyst (wall calcification, wall thickening)
20 DOS CME Course 2011
11
21
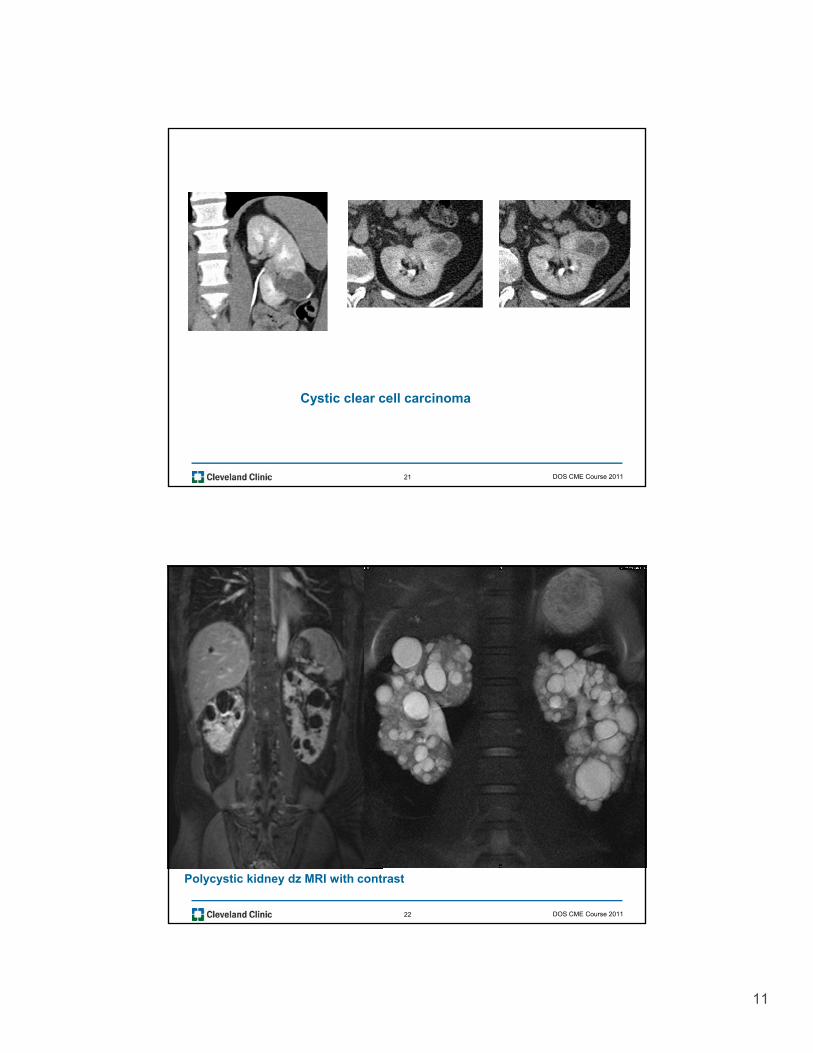
Cystic clear cell carcinoma
DOS CME Course 2011
22
Polycystic kidney dz MRI with contrast
DOS CME Course 2011
12
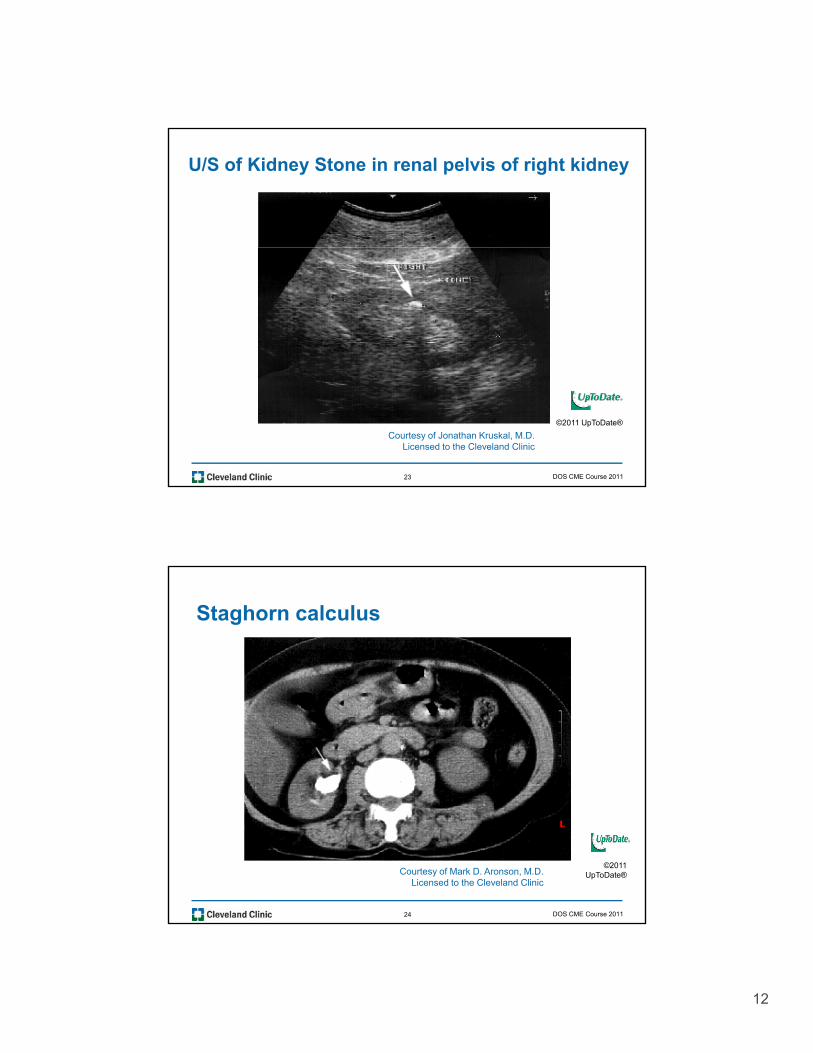
U/S of Kidney Stone in renal pelvis of right kidney
23
©2011 UpToDate®
Courtesy of Jonathan Kruskal, M.D.Licensed to the Cleveland Clinic
DOS CME Course 2011
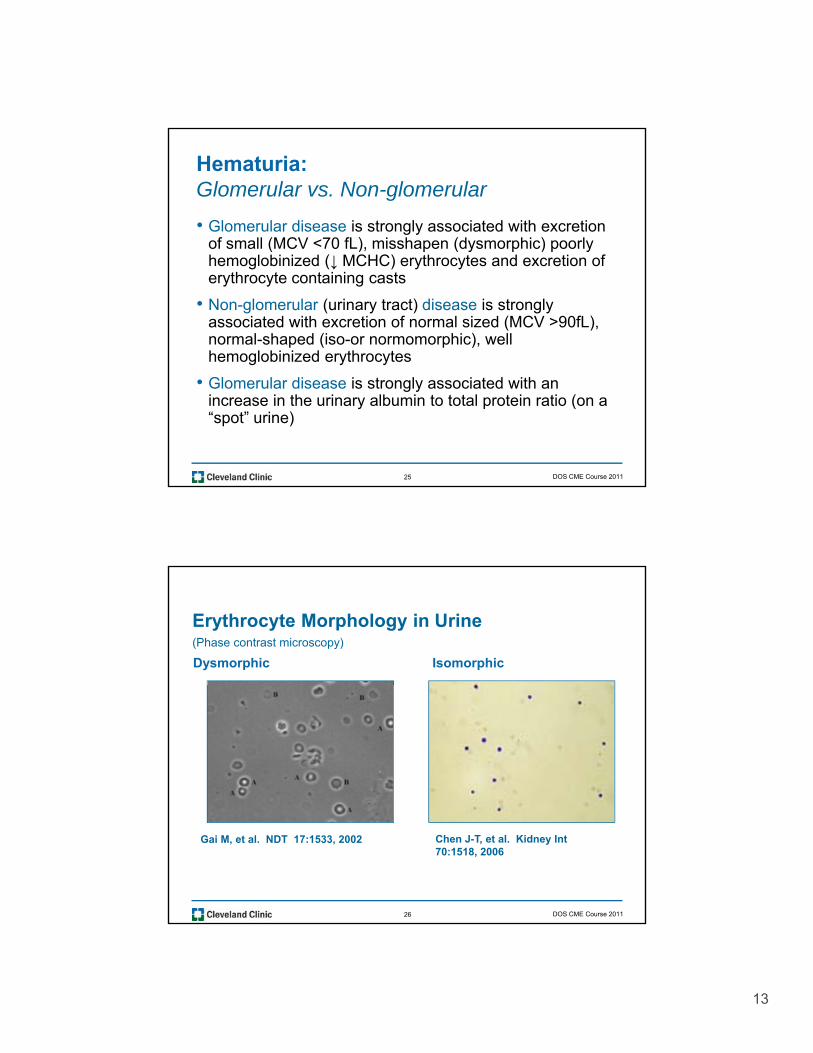
Staghorn calculus
24
©2011 UpToDate®Courtesy of Mark D. Aronson, M.D.
Licensed to the Cleveland Clinic
DOS CME Course 2011
13
Hematuria:Glomerular vs. Non-glomerular
• Glomerular disease is strongly associated with excretion of small (MCV <70 fL), misshapen (dysmorphic) poorlyof small (MCV 70 fL), misshapen (dysmorphic) poorly hemoglobinized (↓ MCHC) erythrocytes and excretion of erythrocyte containing casts
• Non-glomerular (urinary tract) disease is strongly associated with excretion of normal sized (MCV >90fL), normal-shaped (iso-or normomorphic), well hemoglobinized erythrocytes
25
• Glomerular disease is strongly associated with an increase in the urinary albumin to total protein ratio (on a “spot” urine)
DOS CME Course 2011
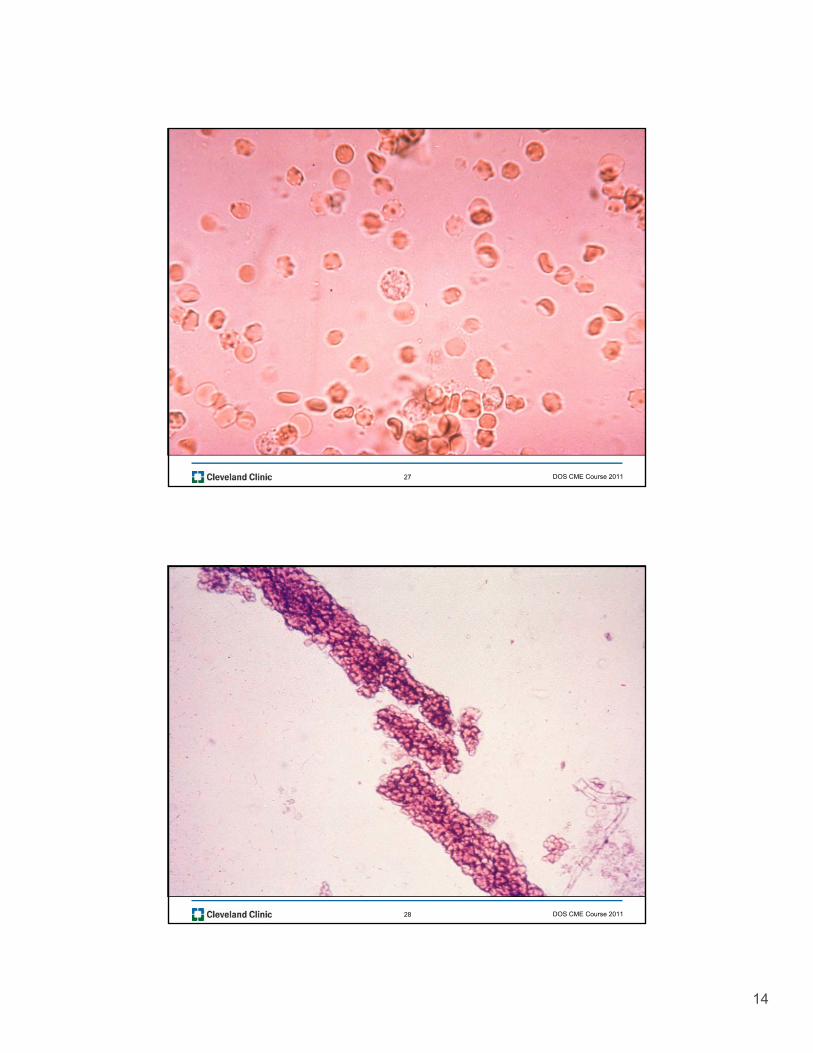
Erythrocyte Morphology in Urine (Phase contrast microscopy)
Dysmorphic Isomorphic
26
Gai M, et al. NDT 17:1533, 2002 Chen J-T, et al. Kidney Int 70:1518, 2006
DOS CME Course 2011
14
27 DOS CME Course 2011
28 DOS CME Course 2011
15
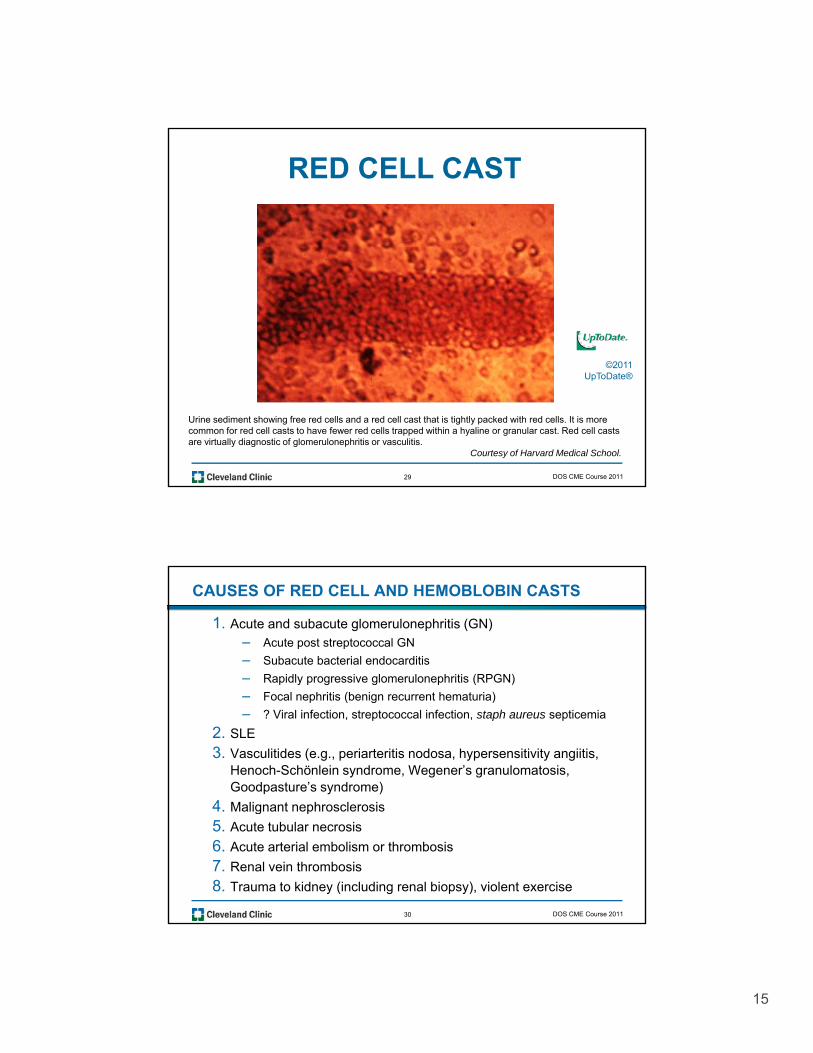
RED CELL CAST
©2011
29
©2011 UpToDate®
Urine sediment showing free red cells and a red cell cast that is tightly packed with red cells. It is more common for red cell casts to have fewer red cells trapped within a hyaline or granular cast. Red cell casts are virtually diagnostic of glomerulonephritis or vasculitis.
Courtesy of Harvard Medical School.
DOS CME Course 2011
CAUSES OF RED CELL AND HEMOBLOBIN CASTS
1. Acute and subacute glomerulonephritis (GN)– Acute post streptococcal GN
– Subacute bacterial endocarditis
– Rapidly progressive glomerulonephritis (RPGN)
– Focal nephritis (benign recurrent hematuria)
– ? Viral infection, streptococcal infection, staph aureus septicemia
2. SLE
3. Vasculitides (e.g., periarteritis nodosa, hypersensitivity angiitis, Henoch-Schönlein syndrome, Wegener’s granulomatosis, Goodpasture’s syndrome)
4 Malignant nephrosclerosis
30
4. Malignant nephrosclerosis
5. Acute tubular necrosis
6. Acute arterial embolism or thrombosis
7. Renal vein thrombosis
8. Trauma to kidney (including renal biopsy), violent exercise
DOS CME Course 2011
16
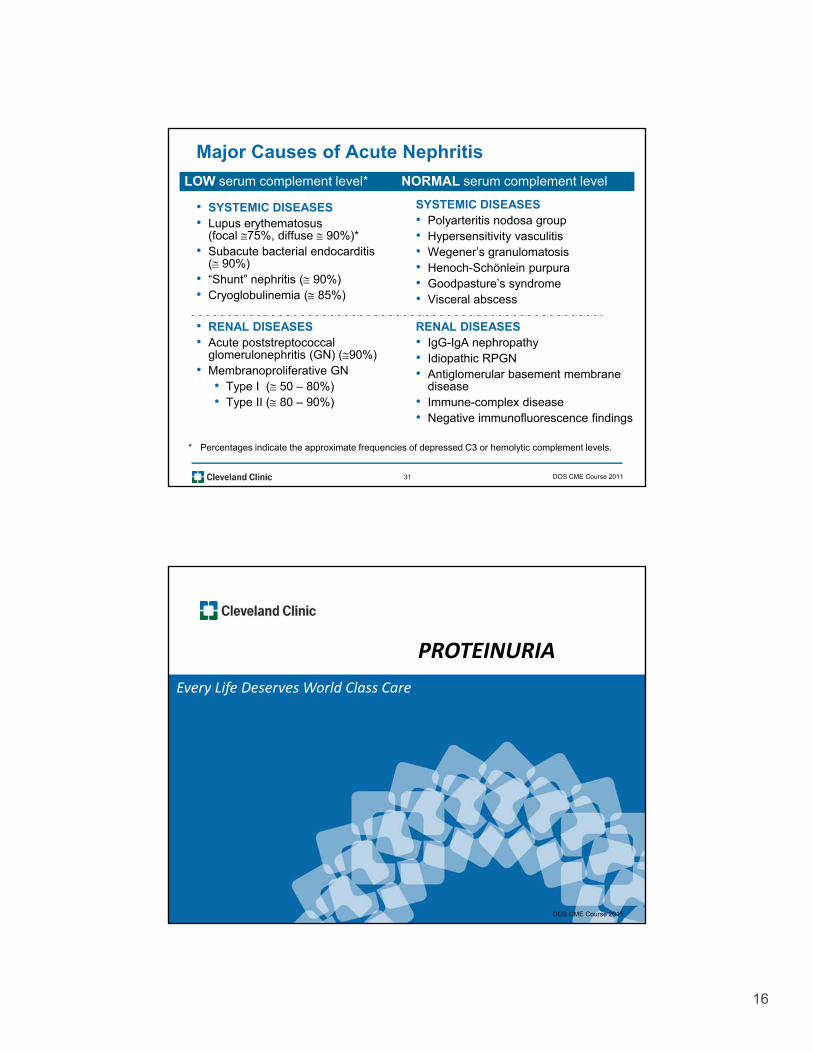
Major Causes of Acute Nephritis
• SYSTEMIC DISEASES• Lupus erythematosus
(focal 75%, diffuse 90%)*S b t b t i l d diti
SYSTEMIC DISEASES• Polyarteritis nodosa group• Hypersensitivity vasculitis
W ’ l t i
LOW serum complement level* NORMAL serum complement level
• Subacute bacterial endocarditis ( 90%)
• “Shunt” nephritis ( 90%)• Cryoglobulinemia ( 85%)
• RENAL DISEASES• Acute poststreptococcal
glomerulonephritis (GN) (90%)M b lif ti GN
• Wegener’s granulomatosis• Henoch-Schönlein purpura• Goodpasture’s syndrome• Visceral abscess
RENAL DISEASES• IgG-IgA nephropathy • Idiopathic RPGN
31
• Membranoproliferative GN• Type I ( 50 – 80%)• Type II ( 80 – 90%)
• Antiglomerular basement membrane disease
• Immune-complex disease• Negative immunofluorescence findings
* Percentages indicate the approximate frequencies of depressed C3 or hemolytic complement levels.
DOS CME Course 2011
PROTEINURIA
Every Life Deserves World Class CareEvery Life Deserves World Class Care
32 DOS CME Course 201132 DOS CME Course 2011
17
PROTEINURIA
VS. ALBUMINURIA
VS. MICROALBUMINURIA
33 DOS CME Course 2011
34 DOS CME Course 2011
18
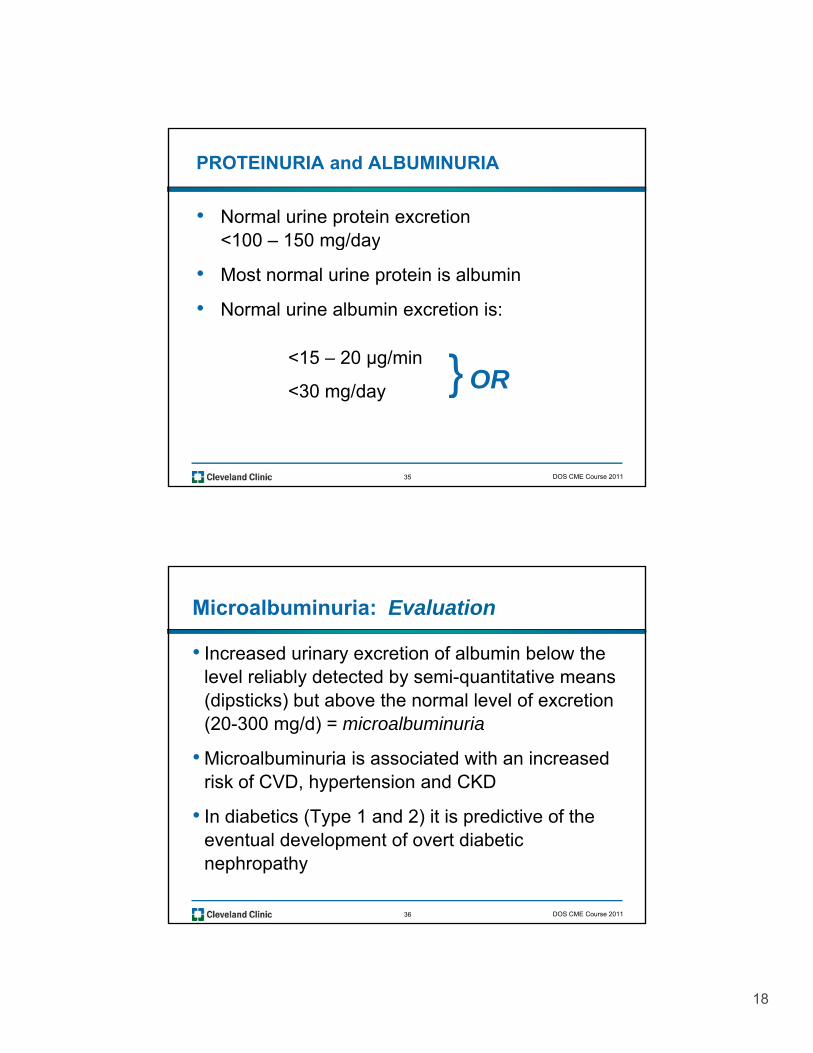
PROTEINURIA and ALBUMINURIA
• Normal urine protein excretion <100 – 150 mg/dayg y
• Most normal urine protein is albumin
• Normal urine albumin excretion is:
<15 – 20 µg/min }
35
µg
<30 mg/day } OR
DOS CME Course 2011
Microalbuminuria: Evaluation
• Increased urinary excretion of albumin below the level reliably detected by semi-quantitative means y y q(dipsticks) but above the normal level of excretion (20-300 mg/d) = microalbuminuria
• Microalbuminuria is associated with an increased risk of CVD, hypertension and CKD
36
• In diabetics (Type 1 and 2) it is predictive of the eventual development of overt diabetic nephropathy
DOS CME Course 2011
19
37 DOS CME Course 2011
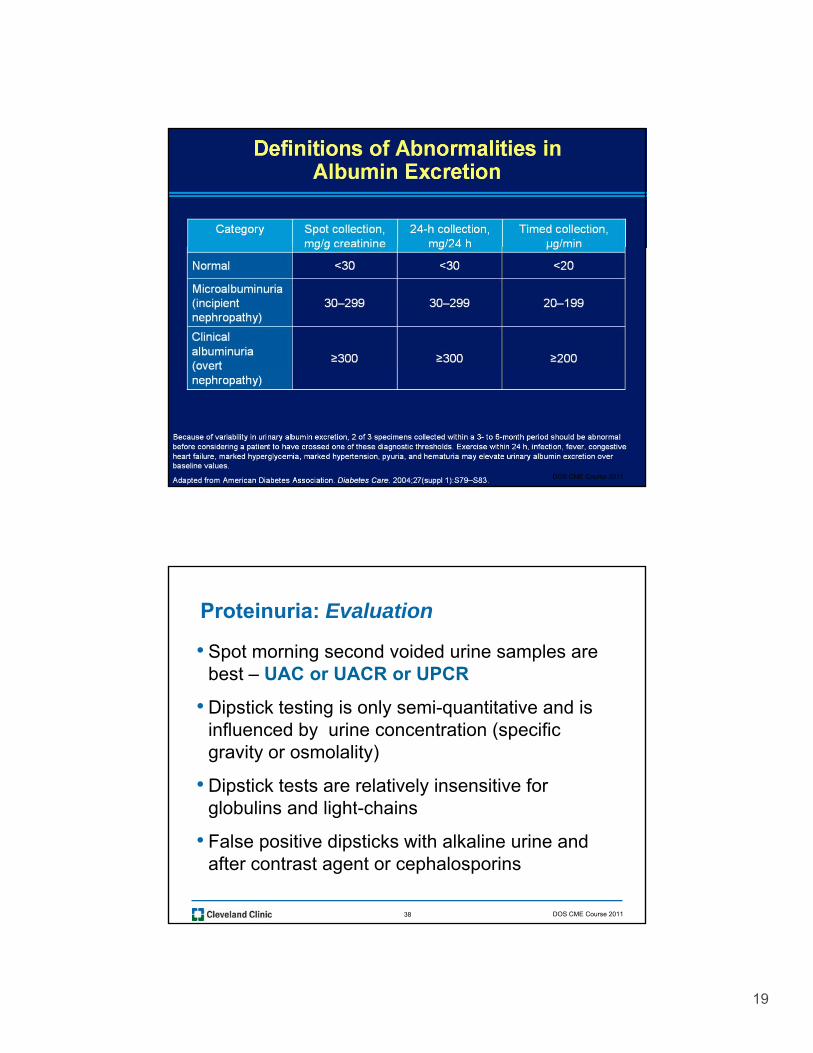
Proteinuria: Evaluation
• Spot morning second voided urine samples are best – UAC or UACR or UPCR
• Dipstick testing is only semi-quantitative and is influenced by urine concentration (specific gravity or osmolality)
• Dipstick tests are relatively insensitive for globulins and light chains
38
globulins and light-chains
• False positive dipsticks with alkaline urine and after contrast agent or cephalosporins
DOS CME Course 2011
20
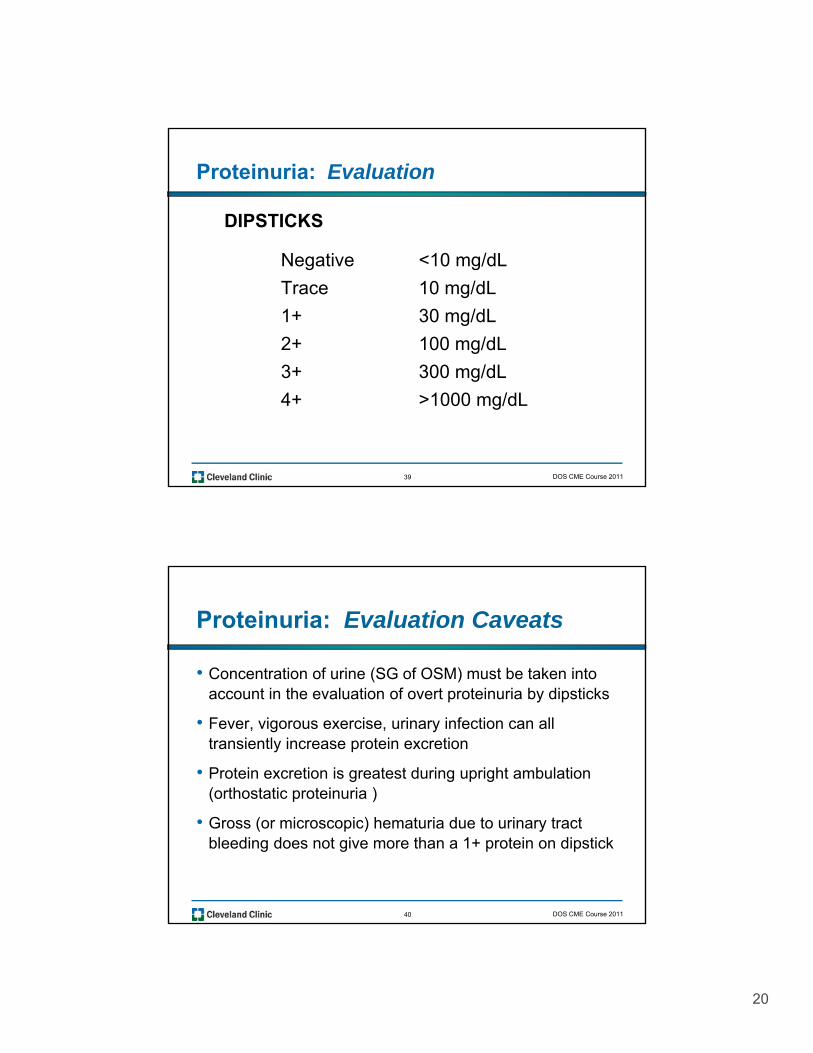
Proteinuria: Evaluation
DIPSTICKS
Negative <10 mg/dL
Trace 10 mg/dL
1+ 30 mg/dL
2+ 100 mg/dL
3+ 300 /dL
39
3+ 300 mg/dL
4+ >1000 mg/dL
DOS CME Course 2011
Proteinuria: Evaluation Caveats
• Concentration of urine (SG of OSM) must be taken into account in the evaluation of overt proteinuria by dipsticks
• Fever, vigorous exercise, urinary infection can all transiently increase protein excretion
• Protein excretion is greatest during upright ambulation (orthostatic proteinuria )
40
• Gross (or microscopic) hematuria due to urinary tract bleeding does not give more than a 1+ protein on dipstick
DOS CME Course 2011
21
BEWARE OF UACR
41 DOS CME Course 2011
Albuminuria (UACR) as a Prognostic Tool: Caveats
• Numerous cross-sectional studies have shown a strong association between UACR and subsequent all-cause mortality, CV events and progressive CKD (Lamers-Heerspink, et al: J Am Soc Nephrol 21:1355, 2010.)
• However, both albumin excretion (UA) and creatinine excretion (C) contribute to risk – in
42
creatinine excretion (C) contribute to risk – in opposite direction (similar to KT/V) (Kestenbaum B, de Boer J. J Am Soc Nephrol 21:1243, 2010.)
DOS CME Course 2011
22
• Since U Cr decreases with age, loss of muscle mass, vegetarian and low-protein diets – UACR may increase without any absolute increase inmay increase without any absolute increase in AER.
• Since U Cr increases with body building, high red-meat diets and acute muscle breakdown, UACR may not increase despite an increase in
43
absolute AER.
DOS CME Course 2011
PROTEINURIA
• Abnormal
• I di t kid di ( ti )• Indicates kidney disease (rare exceptions)
• Qualitatively detected by routine urinalysis-dipstick and several other methods.
• Quantitatively determined by:
–“spot” urine specimen (protein/creatinine ratio)
44
spot urine specimen (protein/creatinine ratio)
–24-hour urine collection
• 65% of total urine protein consists of albumin
DOS CME Course 2011
23
When bubbles settle on the surface of the
urine, they indicate disease of the kidneys
and that the complaint will be protracted.
— Hippocrates
45 DOS CME Course 2011
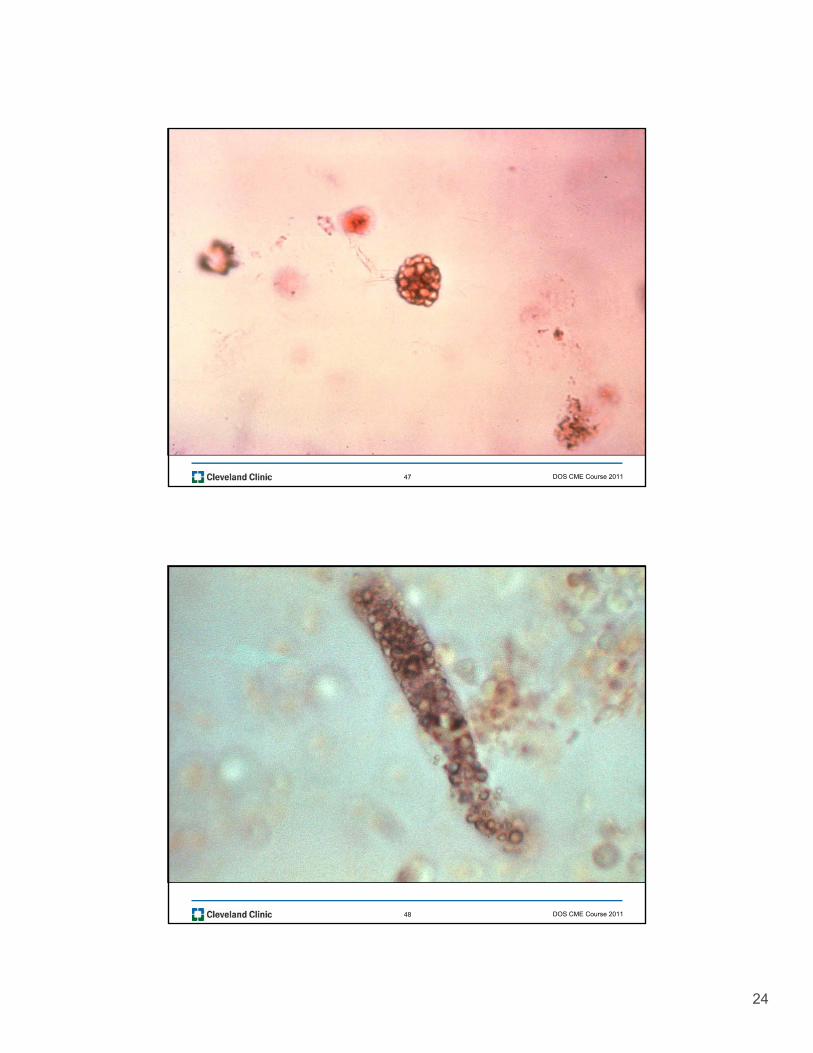
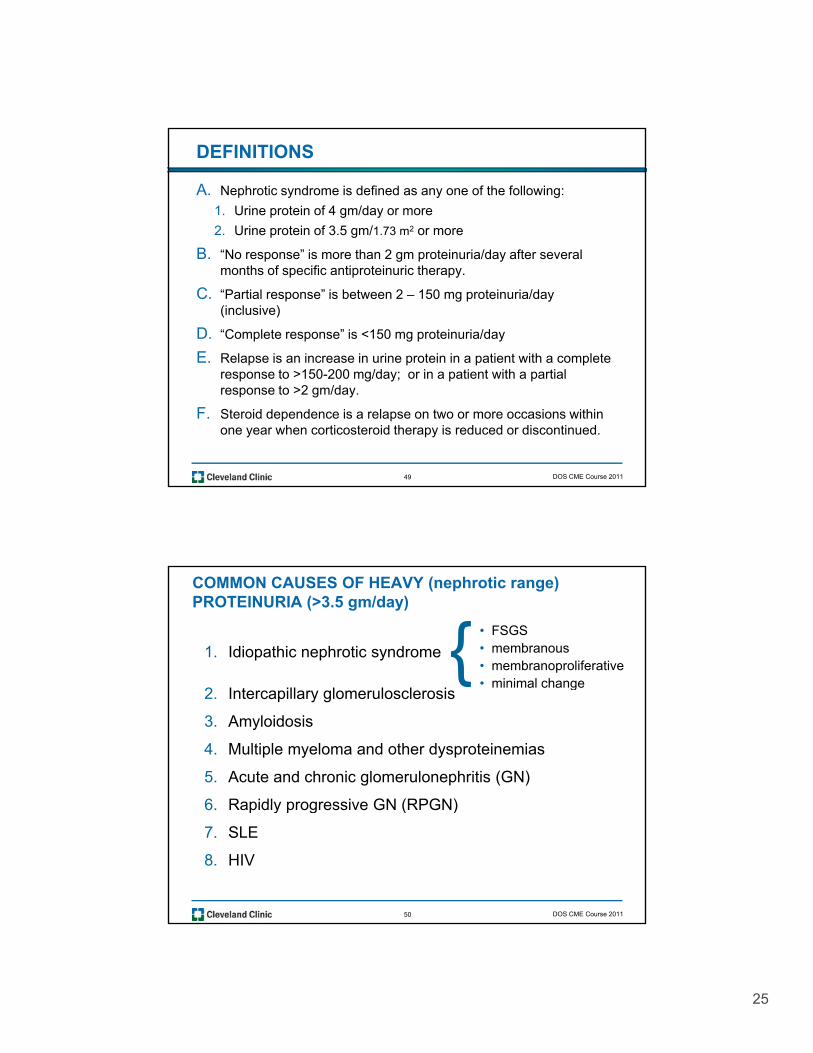
NEPHROTIC SYNDROME
Nephrotic syndrome is a clinical entity having many causes and characterized by increased glomerular membrane permeability manifested by massive proteinuria and excretion of fat bodies. There is variable edema, hypoproteinemia, and hyperlipdemia Protein excretion
46
and hyperlipdemia. Protein excretion usually greater than 3.5 gm/24 hrs/1.73 m2
of body surface if GFR is normal.
DOS CME Course 2011
24
47 DOS CME Course 2011
48 DOS CME Course 2011
25
DEFINITIONS
A. Nephrotic syndrome is defined as any one of the following:
1. Urine protein of 4 gm/day or more
2. Urine protein of 3.5 gm/1.73 m2 or more
BB. “No response” is more than 2 gm proteinuria/day after several months of specific antiproteinuric therapy.
C. “Partial response” is between 2 – 150 mg proteinuria/day (inclusive)
D. “Complete response” is <150 mg proteinuria/day
E. Relapse is an increase in urine protein in a patient with a complete
49
response to >150-200 mg/day; or in a patient with a partial response to >2 gm/day.
F. Steroid dependence is a relapse on two or more occasions within one year when corticosteroid therapy is reduced or discontinued.
DOS CME Course 2011
COMMON CAUSES OF HEAVY (nephrotic range) PROTEINURIA (>3.5 gm/day)
1. Idiopathic nephrotic syndrome• FSGS• membranous• membranoproliferative• minimal change
{2. Intercapillary glomerulosclerosis
3. Amyloidosis
4. Multiple myeloma and other dysproteinemias
5. Acute and chronic glomerulonephritis (GN)
6 Rapidly progressive GN (RPGN)
minimal change{
50
6. Rapidly progressive GN (RPGN)
7. SLE
8. HIV
DOS CME Course 2011
26
COMMON CAUSES OF HEAVY (nephrotic range)
PROTEINURIA (>3.5 gm/day), cont.
9. Hepatitis B + C
10. Vasculitides (e.g., periarteritis)
11. Malignant nephrosclerosis
12. Renal venous congestion
13. Drugs
• Renal vein thrombosis• Constrictive pericarditis• Severe CHF{
• VEGF inhibitors{• NSAIDs
i ill i
{
51
14. Morbid obesity
G b to s• anti-TNF agents• gamma interferon{ • penicillamine
• gold• pamdironmate
{
DOS CME Course 2011
Causes of Moderate Proteinuria (0.5 - 3.5 gm/day)
1. Any of the causes of “heavy proteinuria”
2. Latent or chronic glomerulonephritis
3. Nephrosclerosis and/or
52
4. Pyelonephritis/interstitial nephritis
DOS CME Course 2011
27
CAUSES OF MINIMAL OR INTERMITTENT PROTEINURIA(<0.5 gm/day)
1. Latent glomerulonephritis, healing APSGN or focal nephritis
2. Obstruction
3. Chronic pyelonephritis
4. Benign nephrosclerosis
5. Polycystic kidney disease
6. Hypercalcemia; potassium depletion
7. Tubular syndromes (Fanconi, TRA, etc.)
53
y ( )
8. Neoplasms, stones malformations
9. “Benign” proteinurias (often intermittent)a. Functional proteinuria
b. Postural (orthostatic) proteinuria
DOS CME Course 2011
ORTHOSTATIC PROTEINURIA
DEFINITION: protein excretion <150 mg/day when recumbent, but >150 mg/day when upright
1. “Persistent” proteinuria (5-10%*)
• Present during BOTH the recumbent and upright postures
2. “Transient” orthostatic proteinuria (75-80%*)
• Present inconstantly from day to day
54
3. “Fixed” orthostatic proteinuria (15%*)
• Present consistently on separate days
* Routine urinalysis in healthy young males → proteinuria
DOS CME Course 2011
28
1. Healthy adolescents and young adults (3-5%)2. Routine health examination
ORTHOSTATIC PROTEINURIA, continued
CLINICAL CHARACTERISTICS
3. Clinical and laboratory examination normal except for the proteinuria
4. Total daily protein excretion usually < 1.0 g/day5. Prognosis - good
RENAL HISTOLOGY (patients with “fixed” orthostatic proteinuria )
8% definite abnormalities
55
8% - definite abnormalities 45% - subtle alternations of glomerular structure47% - normal biopsy
• Clinical significance of abnormal biopsy not clear.• Little histological data for patients with “transient” orthostatic proteinuria
DOS CME Course 2011
FUNCTIONAL PROTEINURIA
1. Fever
2 E i ( thl ti ti )2. Exercise (e.g., athletic exertion)
3. Exposure to heat or cold
4. Emotional stress
5 C ti h t f il
56
5. Congestive heart failure
DOS CME Course 2011
29
RENAL DISEASE OCCURRING IN THE ABSENCE OF PROTEINURIA
1. Acute and chronic pyelonephritis
2. Obstructive nephropathy
3. Nephrolithiasis
4. Nephropathies of hypercalcemia and potassium depletion
5 Benign nephrosclerosis
57
5. Benign nephrosclerosis
6. Polycystic kidney disease (PKD)
7. Tumors, congenital malformations
DOS CME Course 2011
NEPHRITIC vs. NEPHROTIC
Proteinuria Variable amount “heavy” (>3.5 gm /day)
Urine RBCs + RBC Lipiduria (OFBs free fatUrine RBCs + RBC Lipiduria (OFBs, free fat, sediment casts fatty casts, Maltese
crosses
Hypoallbumi- Less common Commonnemia
Edema Acute ↓ GFR Consequence of hypo-
58
↓ q ypPreserved tubular albuminemia ↑ISF
function↑ reabsorption of ↑ reabsorption of
NA and H2O NA and H2O
DOS CME Course 2011
30
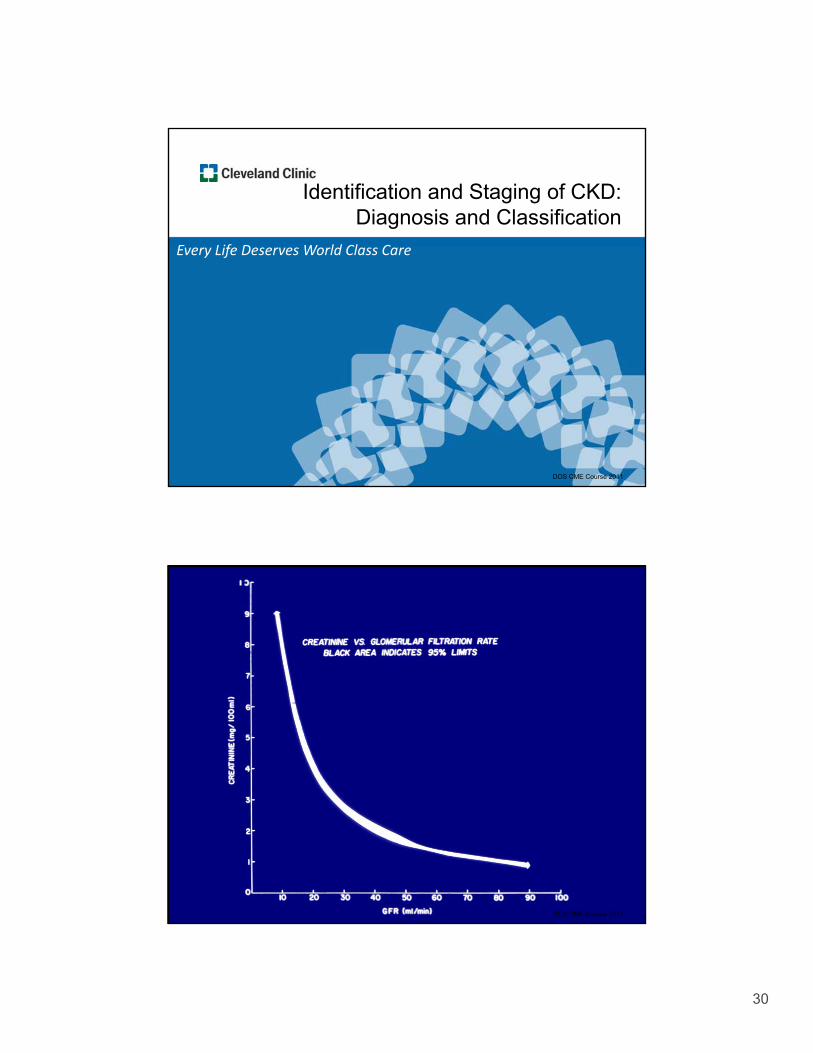
Every Life Deserves World Class Care
Identification and Staging of CKD: Diagnosis and Classification
Every Life Deserves World Class Care
59 DOS CME Course 201159 DOS CME Course 2011
60 DOS CME Course 2011
31
Glomerular Filtration Rate (GFR)
• GFR is the clearance by the kidney of a marker (either endogenous or exogenous) in plasma expressed asendogenous or exogenous) in plasma, expressed as the volume of plasma completely cleared of that marker per unit time:
C = UV/P
61
• Reported in ml/min/1.73 m2
DOS CME Course 2011
Filtration Markers
ExogenousEndogenous
• Inulin
• 51Cr-EDTA
• 99mTc-DTPA
125
• Creatinine
• Urea
• Cystatin C
62
• 125I-iothalamate
• “Cold” iothalamate
• Iohexol
DOS CME Course 2011
32
Why do we care about GFR?
• GFR is the best overall measure of kidney function
• Chronic kidney disease is a public health problem by 2030 more than 2 million people in USA will need dialysis or transplantation
• The definition and classification system for CKD is based on level of GFR accurate estimation of GFR
63
is central to the detection, evaluation and management of CKD
DOS CME Course 2011
Estimation of GFR – K/DOQI
• The level of GFR should be estimated from prediction equations that take into account the SCr concentration and some or all of the following variables: age, gender, race, g g , g , ,and body size:
–Cockcroft-Gault equation
–MDRD Study equation / re-expressed MDRD equation
• The GFR may be measured directly (e.g., iothalamate)
64
(e.g., iothalamate)
• The SCr concentration alone should not be used to assess the level of kidney function
K/DOQI Clinical Practice Guidelines, AJKD 2002;39(suppl 1)
DOS CME Course 2011
33
SUSPECT REDUCED KIDNEY FUNCTION,
(i.e., DECREASED GFR) IF…
•S Creat > 0.9 to 1.0 mg/dL (women)
•S Creat > 1.3 mg/dL (men)
65 DOS CME Course 2011
Definition of CKD – 3 Components
1. Anatomical or structural: with/out decreased GFR:
– pathologic abnormalities
– markers of kidney damage, including abnormalities in the composition of the blood or urine or abnormalities in imaging tests
2. Temporal component: > 3 months of abnormality
66
p p y
3. Functional component on its own: eGFR <60 ml/min/1.73 m2, with or without kidney damage
DOS CME Course 2011
34
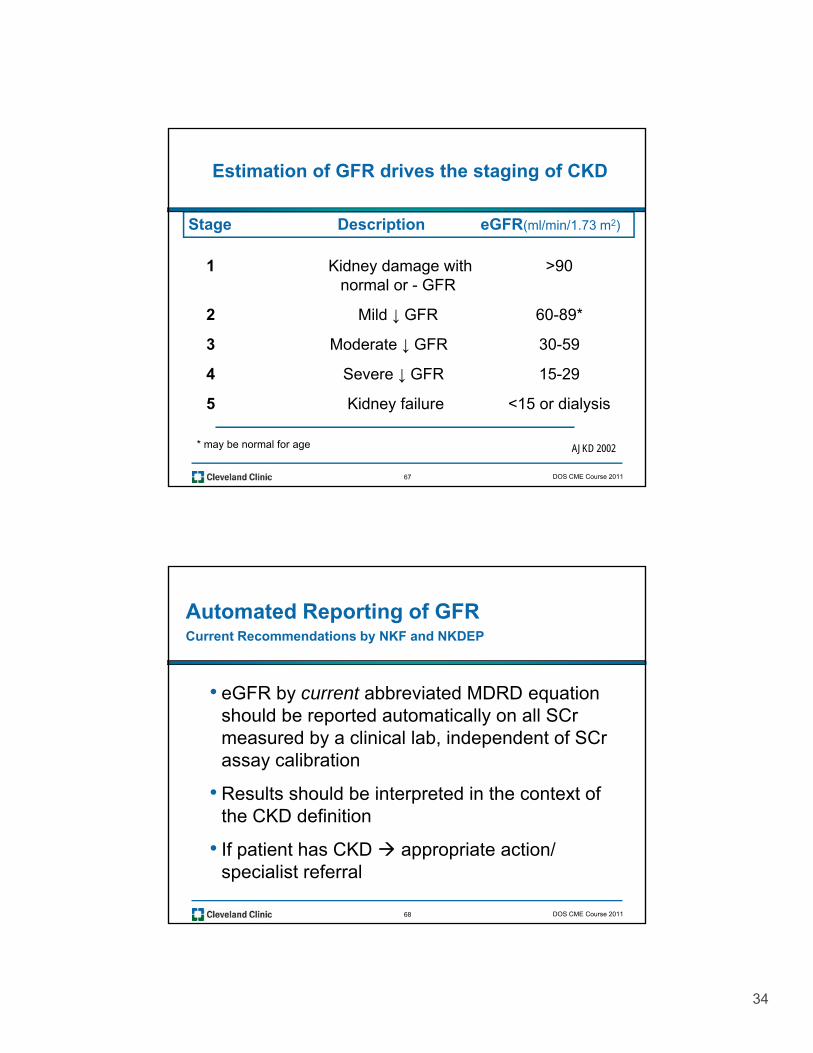
Estimation of GFR drives the staging of CKD
Stage Description eGFR(ml/min/1.73 m2)
1 Kidney damage with >90normal or - GFR
2 Mild ↓ GFR 60-89*
3 Moderate ↓ GFR 30-59
67
4 Severe ↓ GFR 15-29
5 Kidney failure <15 or dialysis
* may be normal for age AJKD 2002
DOS CME Course 2011
Automated Reporting of GFRCurrent Recommendations by NKF and NKDEP
• eGFR by current abbreviated MDRD equation should be reported automatically on all SCr measured by a clinical lab, independent of SCr assay calibration
• Results should be interpreted in the context of
68
the CKD definition
• If patient has CKD appropriate action/ specialist referral
DOS CME Course 2011
35
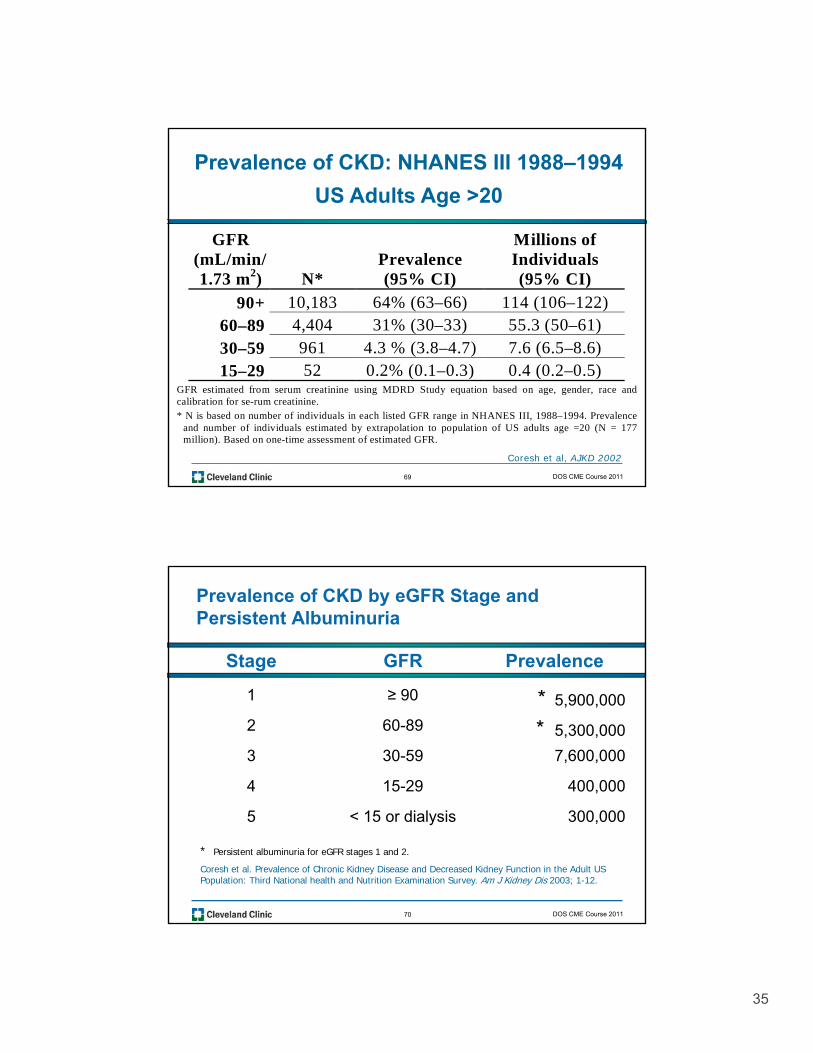
Prevalence of CKD: NHANES III 1988–1994
US Adults Age >20
GFR Millions of(mL/min/1.73 m2) N*
Prevalence(95% CI)
Individuals(95% CI)
90+ 10,183 64% (63–66) 114 (106–122)60–89 4,404 31% (30–33) 55.3 (50–61)30–59 961 4.3 % (3.8–4.7) 7.6 (6.5–8.6)15 29 52 0 2% (0 1 0 3) 0 4 (0 2 0 5)
69
15–29 52 0.2% (0.1–0.3) 0.4 (0.2–0.5)GFR estimated from serum creatinine using MDRD Study equation based on age, gender, race andcalibration for se-rum creatinine.* N is based on number of individuals in each listed GFR range in NHANES III, 1988–1994. Prevalence
and number of individuals estimated by extrapolation to population of US adults age =20 (N = 177million). Based on one-time assessment of estimated GFR.
Coresh et al, AJKD 2002
DOS CME Course 2011
Prevalence of CKD by eGFR Stage and Persistent Albuminuria
Stage GFR Prevalence
1 ≥ 90 * 5,900,000
2 60-89 * 5,300,000
3 30-59 7,600,000
4 15-29 400,000
70
5 < 15 or dialysis 300,000
* Persistent albuminuria for eGFR stages 1 and 2.
Coresh et al. Prevalence of Chronic Kidney Disease and Decreased Kidney Function in the Adult US Population: Third National health and Nutrition Examination Survey. Am J Kidney Dis 2003; 1-12.
DOS CME Course 2011
36
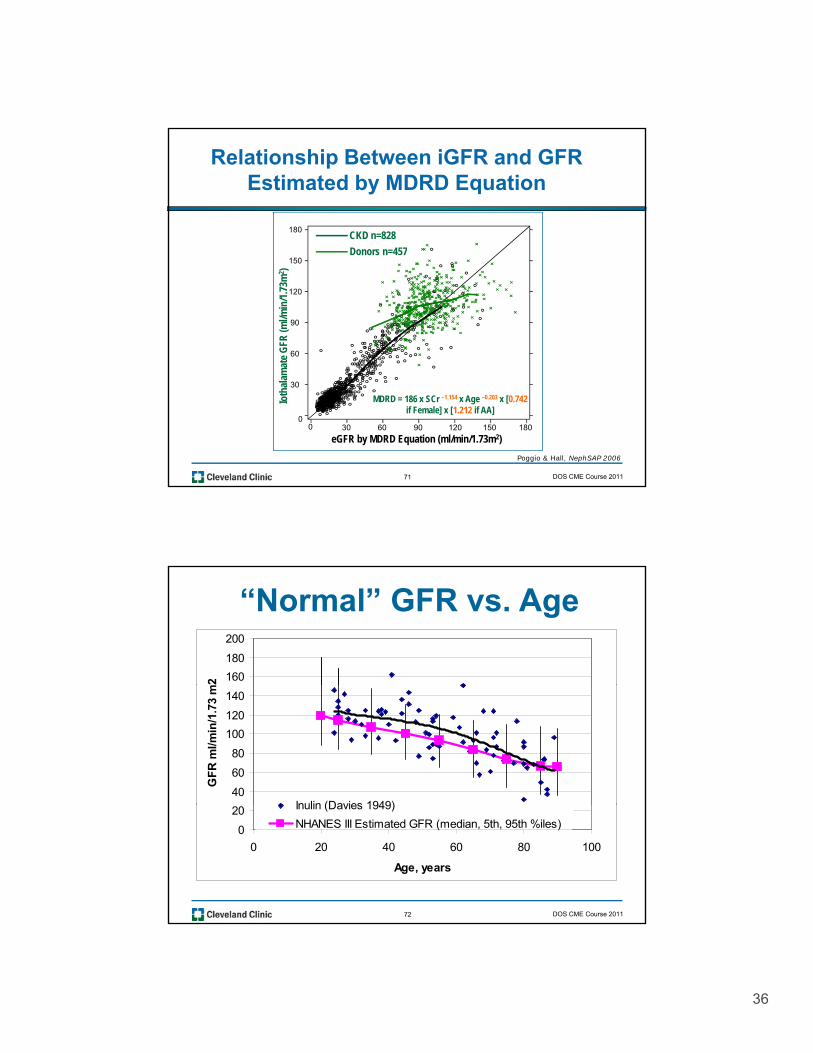
Relationship Between iGFR and GFR Estimated by MDRD Equation
180CKD n=828
D 457
60
90
120
150Donors n=457
ate
GFR
(ml/m
in/1
.73m
2 )
71
0
30
eGFR by MDRD Equation (ml/min/1.73m2)0 30 60 90 120 150 180
Ioth
alam
a
Poggio & Hall, NephSAP 2006
MDRD = 186 x SCr –1.154 x Age –0.203 x [0.742if Female] x [1.212 if AA]
DOS CME Course 2011
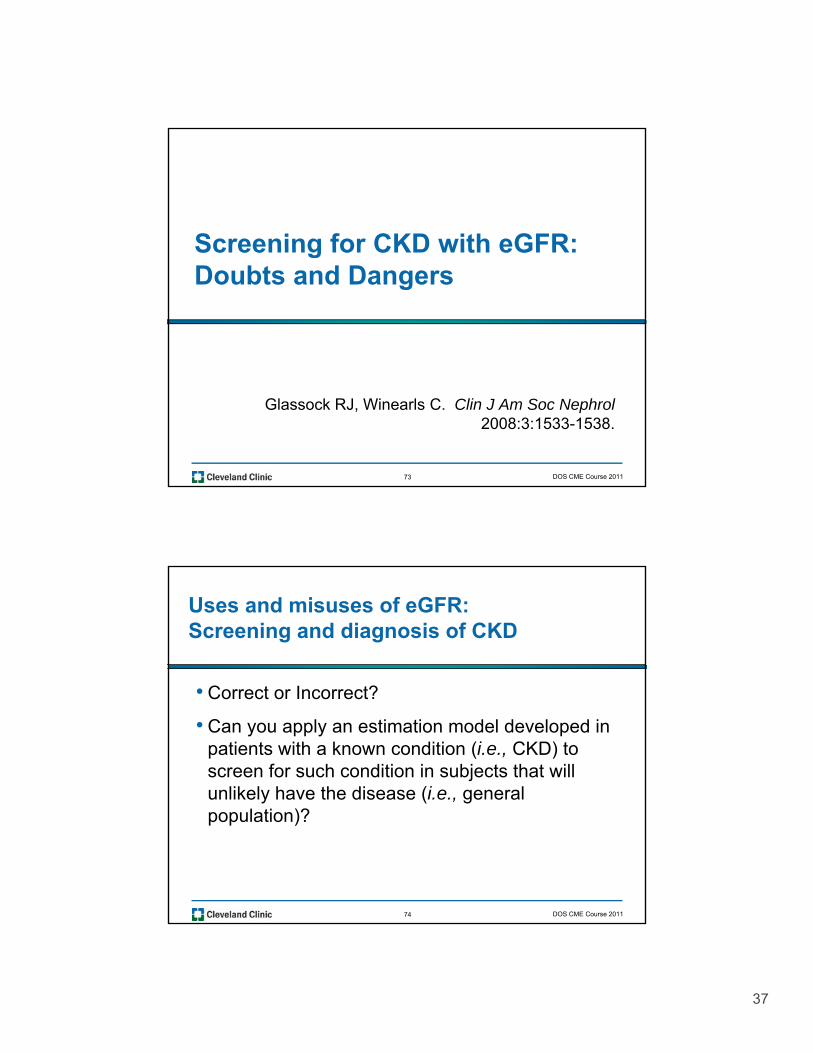
“Normal” GFR vs. Age
160
180
200
2
40
60
80
100
120
140
GF
R m
l/min
/1.7
3 m
Inulin (Davies 1949)
72
0
20
0 20 40 60 80 100
Age, years
Inulin (Davies 1949)
NHANES III Estimated GFR (median, 5th, 95th %iles)
DOS CME Course 2011
37
Screening for CKD with eGFR:Screening for CKD with eGFR: Doubts and Dangers
73
Glassock RJ, Winearls C. Clin J Am Soc Nephrol2008:3:1533-1538.
DOS CME Course 2011
Uses and misuses of eGFR:Screening and diagnosis of CKD
• Correct or Incorrect?
• Can you apply an estimation model developed in patients with a known condition (i.e., CKD) to screen for such condition in subjects that will unlikely have the disease (i.e., general
74
population)?
DOS CME Course 2011
38
Classifications of CKD (KDOQI) based on ( Q )
MDRD-eGFR will be WRONG when
compared to a gold-standard mGFR in
one of every three instances
75 DOS CME Course 2011
MDRD-eGFR: The Future ?
• Ancestry- and geography – specific coefficients –(a “universal MDRD equation is impossible)
• Adjustments for body habitus, customary dietary intake (meat/vegetable protein)
• Calibration to a universal (global) “gold standard” creatinine
• Repeated measurements (≥3 months apart) to define chronicity
76
chronicity
• Combination of eGFR (MDRD) and Cystatin C eGFR (?)
• Abandonment for diagnostic/epidemiologic purposes (?)
DOS CME Course 2011
39
Staging of CKD
• Subjects (of any age) with eGFR* <5th percentile for age/sex but without any corroborating evidence of kidneyage/sex but without any corroborating evidence of kidney damage (macroalbuminuria, glomerular hematuria, imaging or histology) would be labeled as:
“RedUced Renal Function of Uncertain Significance”(RUFUS) NOT Chronic Kidney Disease
77
(*Ancestry/Geography specific)
Winearls & Glassock, Kidney Int. Int 2009; 75(10):1009.
DOS CME Course 2011
Conclusions
• Global prevalence rates of CKD have been greatly overestimated due to inherent flaws in the K/DOQI construct and the eGFR (MDRD) formula
• Even with “bona-fide” Stage 3 CKD the risk of surviving and receiving ESRD treatment (in developed countries) is very low and inversely related to age (0.2-0.4% per year; greater in males than females), despite higher mortality in males from CVD
• The combination of reduced eGFR and dipstick
78
The combination of reduced eGFR and dipstick positive proteinuria greatly increases the risk of progression to ESRD (proteinuria more predictive than eGFR). eGFR and proteinuria are poorly correlated with each other
DOS CME Course 2011
40
When bubbles settle on the surface of the
urine, they indicate disease of the kidneys
and that the complaint will be protracted.
— Hippocrates
79 DOS CME Course 2011
DIABETIC NEPHROPATHY
Every Life Deserves World Class CareEvery Life Deserves World Class Care
80 DOS CME Course 201180 DOS CME Course 2011
41
81 DOS CME Course 2011
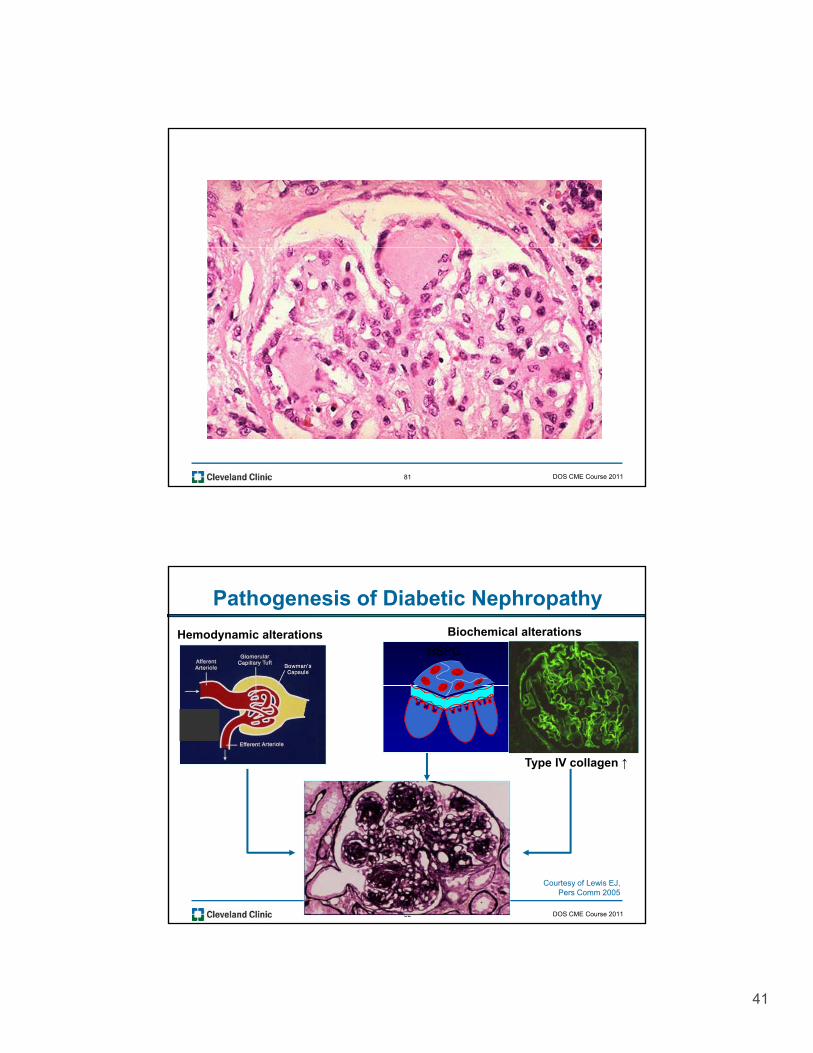
Pathogenesis of Diabetic Nephropathy
Biochemical alterationsHemodynamic alterationsHSPG ↓
Type IV collagen ↑
82
Courtesy of Lewis EJ, Pers Comm 2005
DOS CME Course 2011
42
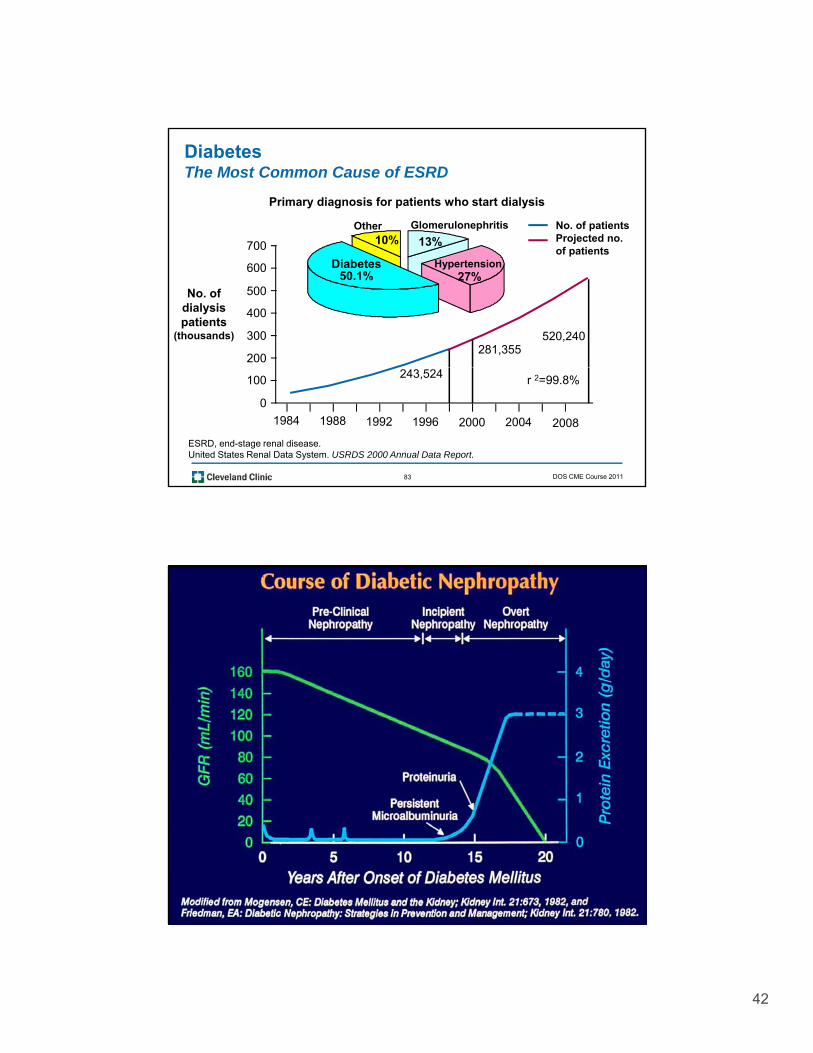
DiabetesThe Most Common Cause of ESRD
Primary diagnosis for patients who start dialysis
Glomerulonephritis
13%Other
10%No. of patientsProjected no.
f ti t700
Diabetes50.1%
Hypertension27%
of patients
200
300
400
500
600
700
281,355520,240
No. of dialysis patients
(thousands)
83
ESRD, end-stage renal disease.United States Renal Data System. USRDS 2000 Annual Data Report.
1984 1988 1992 1996 2000 2004 2008
0
100 r 2=99.8%243,524
DOS CME Course 2011
84
43
85 DOS CME Course 2011
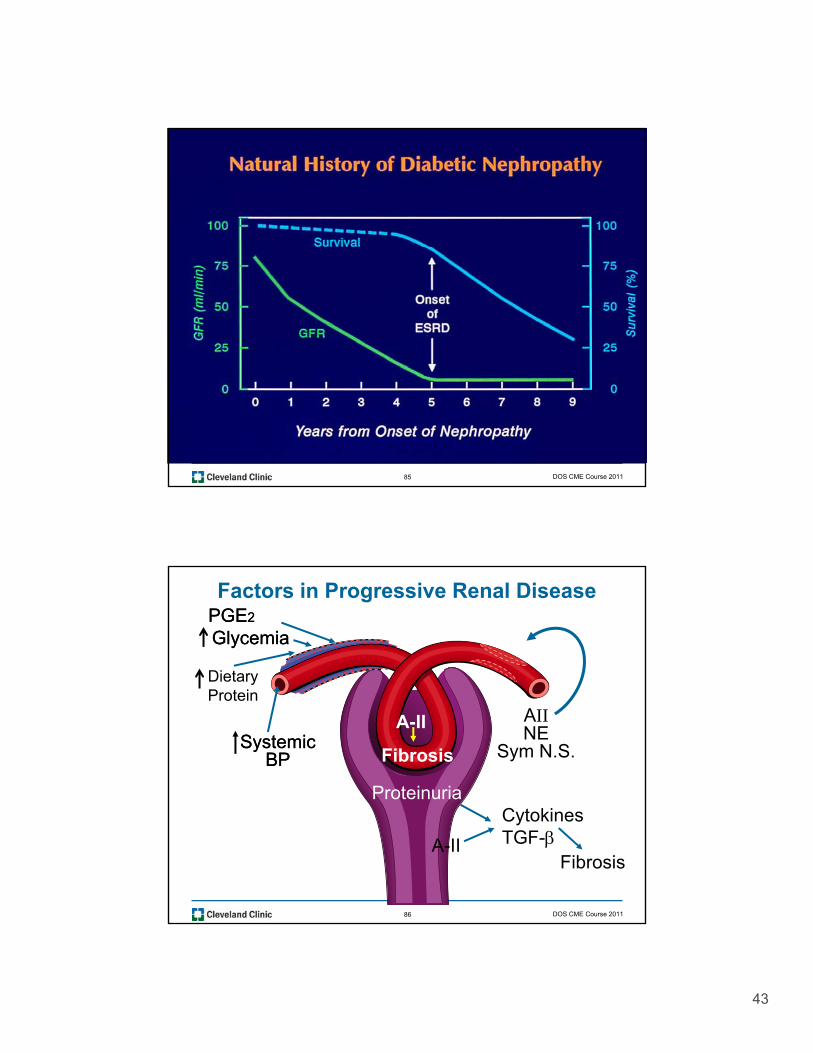
Factors in Progressive Renal DiseasePGEPGE22
GlycemiaGlycemia
Dietary
AIINE
Sym N.S.SystemicSystemicBPBP
Proteinuria
A-II
Fibrosis
Protein
86
CytokinesTGF-A-II
Fibrosis
DOS CME Course 2011
44
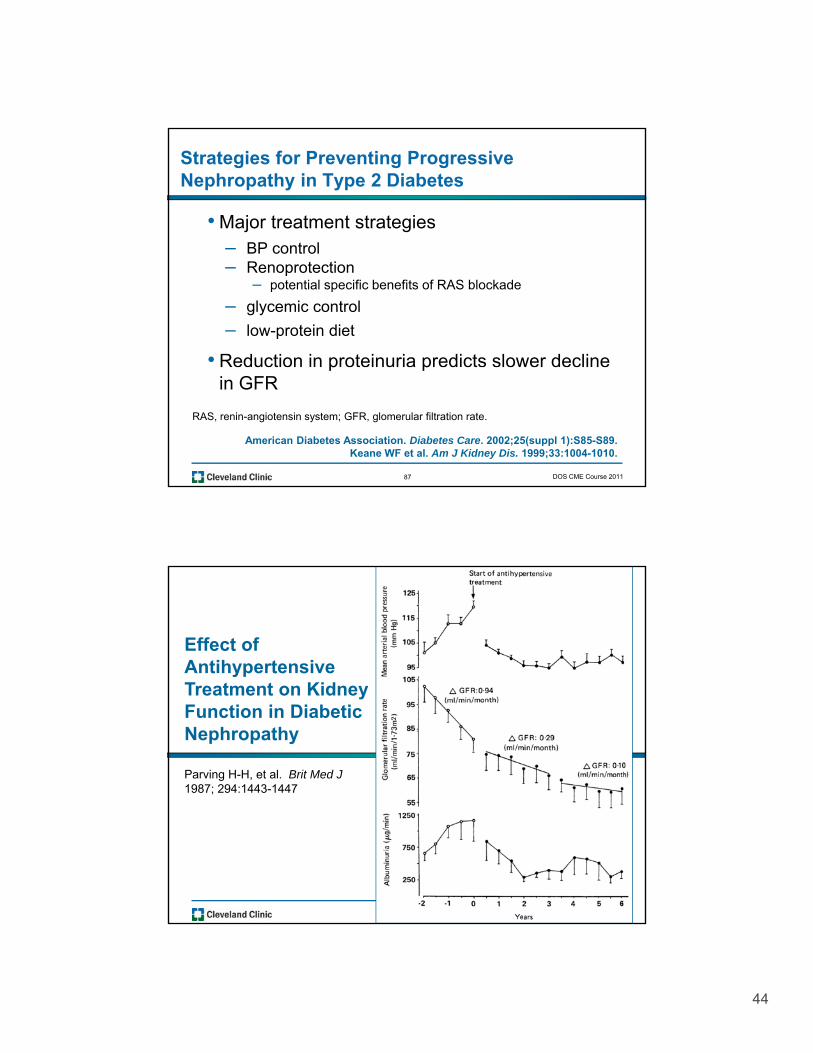
Strategies for Preventing Progressive Nephropathy in Type 2 Diabetes
• Major treatment strategiesBP control– BP control
– Renoprotection– potential specific benefits of RAS blockade
– glycemic control
– low-protein diet
• Reduction in proteinuria predicts slower decline
87
p pin GFR
RAS, renin-angiotensin system; GFR, glomerular filtration rate.
American Diabetes Association. Diabetes Care. 2002;25(suppl 1):S85-S89.Keane WF et al. Am J Kidney Dis. 1999;33:1004-1010.
DOS CME Course 2011
Effect of AntihypertensiveT t t KidTreatment on Kidney Function in Diabetic Nephropathy
Parving H-H, et al. Brit Med J1987; 294:1443-1447
88
45
Do Certain Antihypertensive
A H U i R lAgents Have Unique Renal
Effects in Diabetes?
89 DOS CME Course 2011
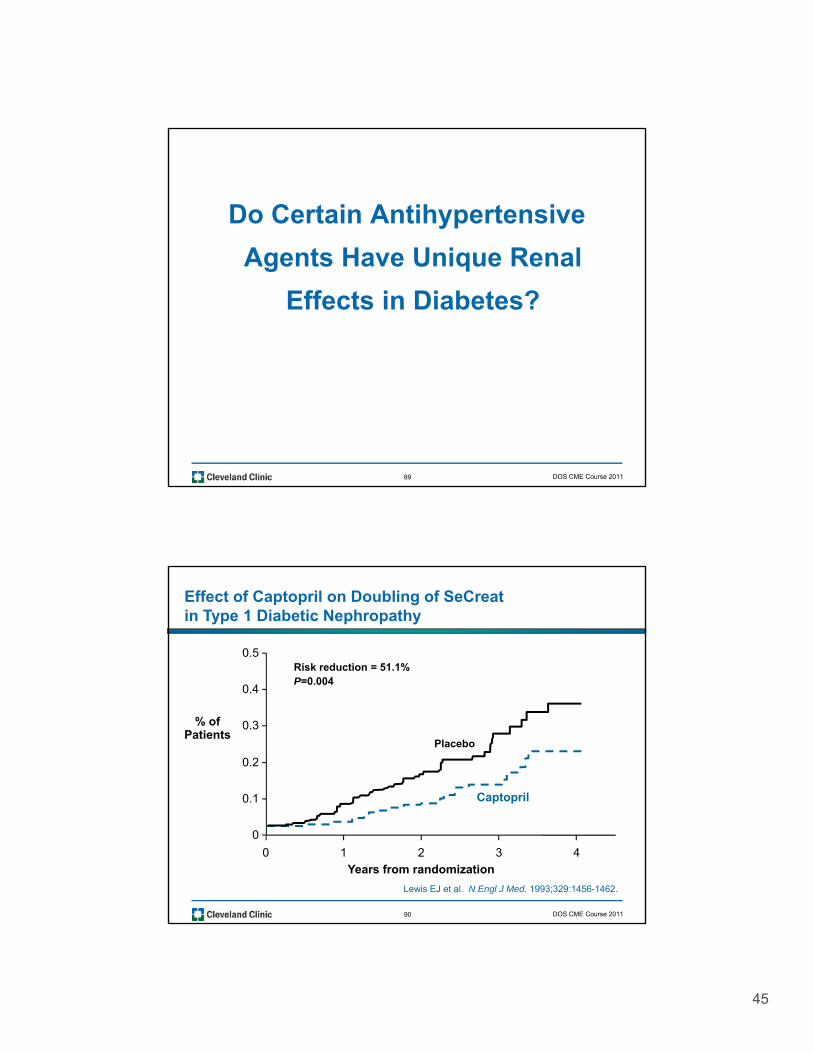
Effect of Captopril on Doubling of SeCreatin Type 1 Diabetic Nephropathy
0 4
0.5Risk reduction = 51.1%P=0.004
0.1
0.2
0.3
0.4
Placebo
Captopril
% ofPatients
90
0
0 1 2 3 4
Years from randomization
Lewis EJ et al. N Engl J Med. 1993;329:1456-1462.
DOS CME Course 2011
46
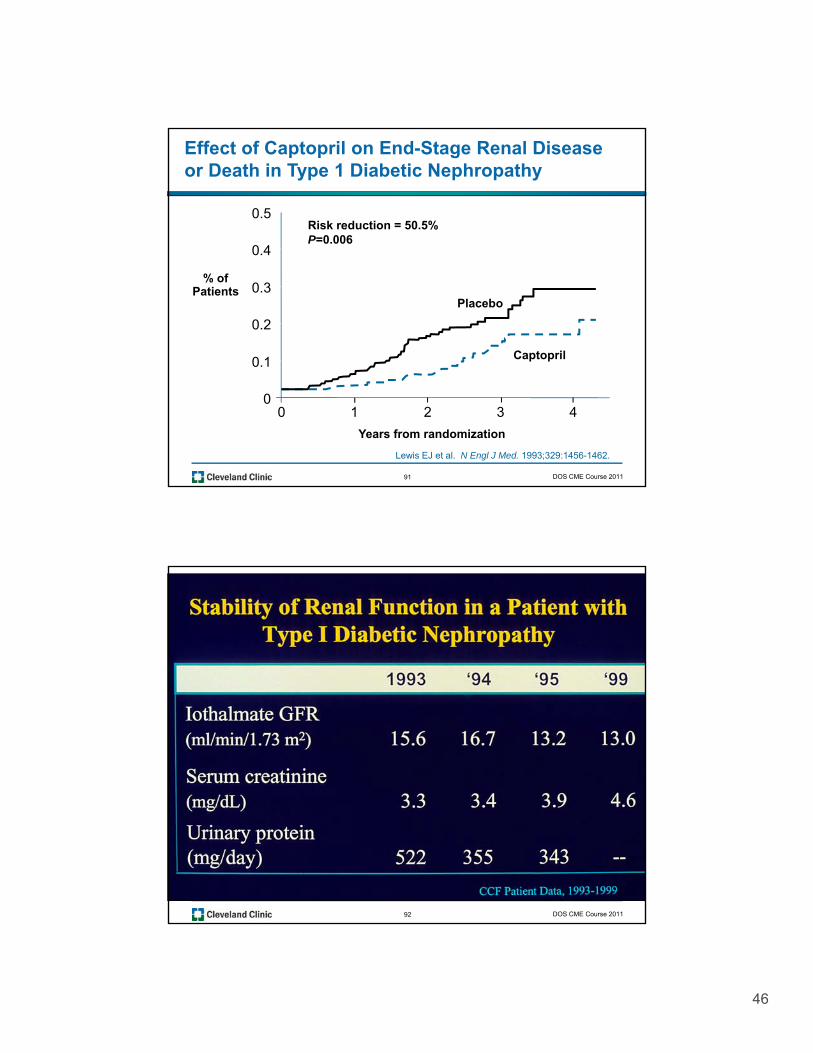
Risk reduction = 50.5%P=0.006
Effect of Captopril on End-Stage Renal Diseaseor Death in Type 1 Diabetic Nephropathy
0 4
0.5
Placebo
Captopril
% ofPatients
0.1
0.2
0.3
0.4
91
Years from randomization
Lewis EJ et al. N Engl J Med. 1993;329:1456-1462.
00 1 2 3 4
DOS CME Course 2011
92 DOS CME Course 2011
47
Angiotensin Converting Enzyme Inhibitors (ACEi) and Angiotensin II Receptor Blockers (ARBs)Lingering Questions
Have the intrarenal effects of ACE inhibitors been observed with the ARBs?
Which experimental models?
93
Which experimental models?
Which ARBs?
DOS CME Course 2011
Mechanisms of Protection: ACEI and AIIRA
• Effects on glomerular hemodynamics and• Effects on glomerular hemodynamics and permselectivity
• Effects on proteinuria, sclerosis, and structural injury
• Effects on pro-sclerosing mediators
94
p g
• Role of combined ACEI plus AIIRA
DOS CME Course 2011
48
Recent Nephrology Trials in Type 2 Diabetes
IRMA II/MARVAL RENAAL/IDNTMicroalbuminuria Proteinuria ESRD
Cardiovascular Morbidity and Mortality
Early Stage Late Stage End Stage
95
Early Stage Late Stage End Stage
Kidney Disease
DOS CME Course 2011
Double-blind treatmentScreening/enrollment
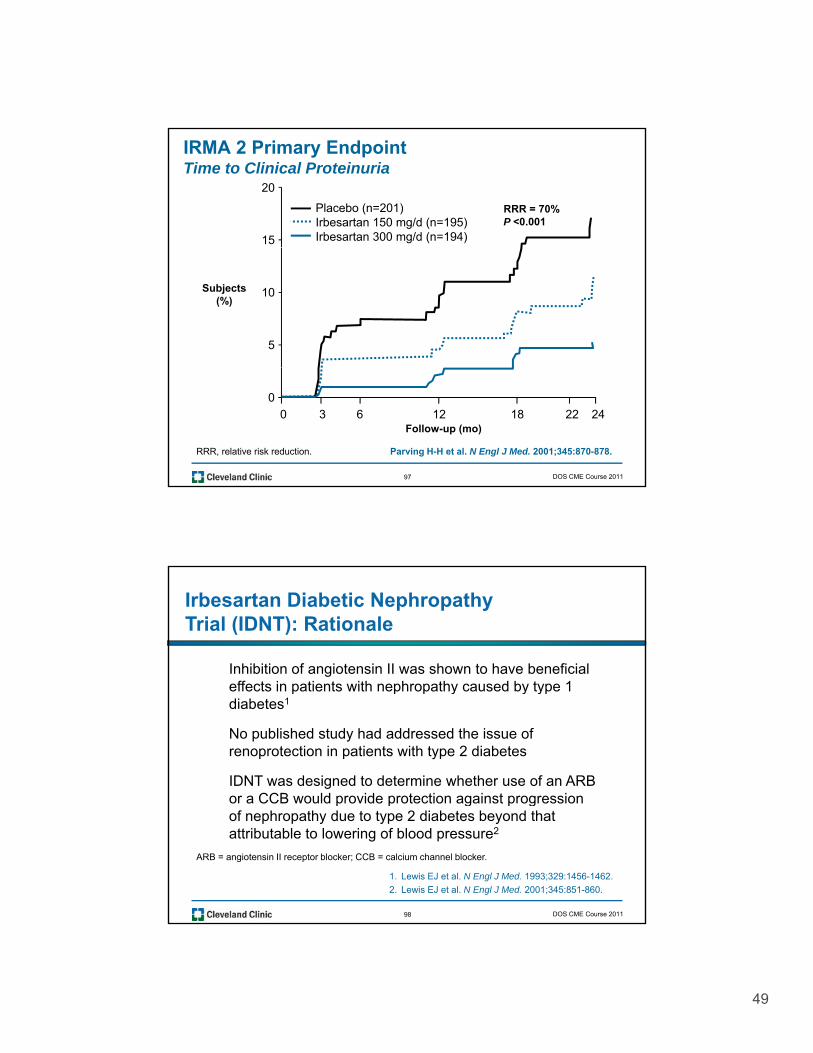
IRMA 2Study Design
• 590 subjects with hypertension, type 2 diabetes, microalbuminuria (albumin excretion rate 20–200 µg/min), and normal renal function
Screening/enrollment
Irbesartan 300 mg/d
Placebo
Irbesartan 150 mg/d
96
Up to 5 weeks Follow-up: 2 years
Adjunctive antihypertensive therapies (excluding ACE inhibitors, angiotensin II receptor blockers,and dihydropyridine calcium channel blockers) could be added to all groups to help achieve equal BP levels.
g
Parving H-H et al. N Engl J Med. 2001;345:870-878.
DOS CME Course 2011
49
15
20
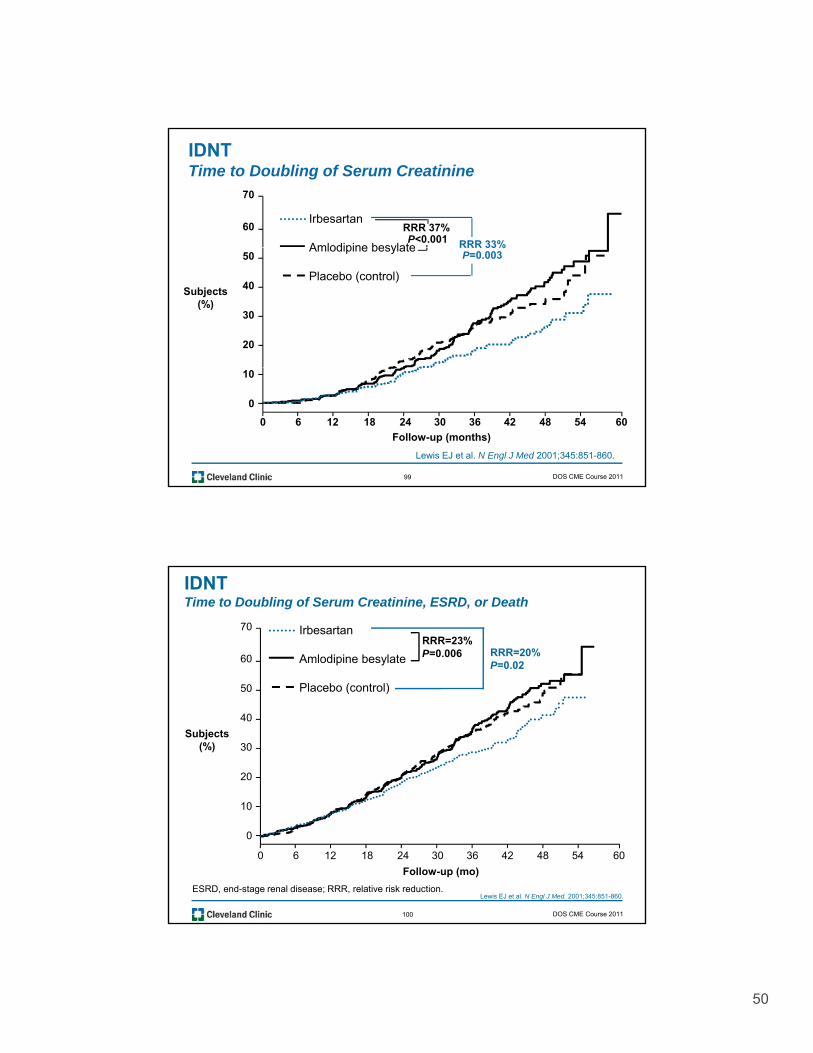
Placebo (n=201)Irbesartan 150 mg/d (n=195)Irbesartan 300 mg/d (n=194)
IRMA 2 Primary EndpointTime to Clinical Proteinuria
RRR = 70%P <0.001
5
10Subjects(%)
97
0
0 3 6 12 18 22 24Follow-up (mo)
RRR, relative risk reduction. Parving H-H et al. N Engl J Med. 2001;345:870-878.
DOS CME Course 2011
Irbesartan Diabetic Nephropathy Trial (IDNT): Rationale
Inhibition of angiotensin II was shown to have beneficial effects in patients with nephropathy caused by type 1effects in patients with nephropathy caused by type 1 diabetes1
No published study had addressed the issue of renoprotection in patients with type 2 diabetes
IDNT was designed to determine whether use of an ARB or a CCB would provide protection against progression
98
1. Lewis EJ et al. N Engl J Med. 1993;329:1456-1462.
2. Lewis EJ et al. N Engl J Med. 2001;345:851-860.
p p g p gof nephropathy due to type 2 diabetes beyond that attributable to lowering of blood pressure2
ARB = angiotensin II receptor blocker; CCB = calcium channel blocker.
DOS CME Course 2011
50
60
70
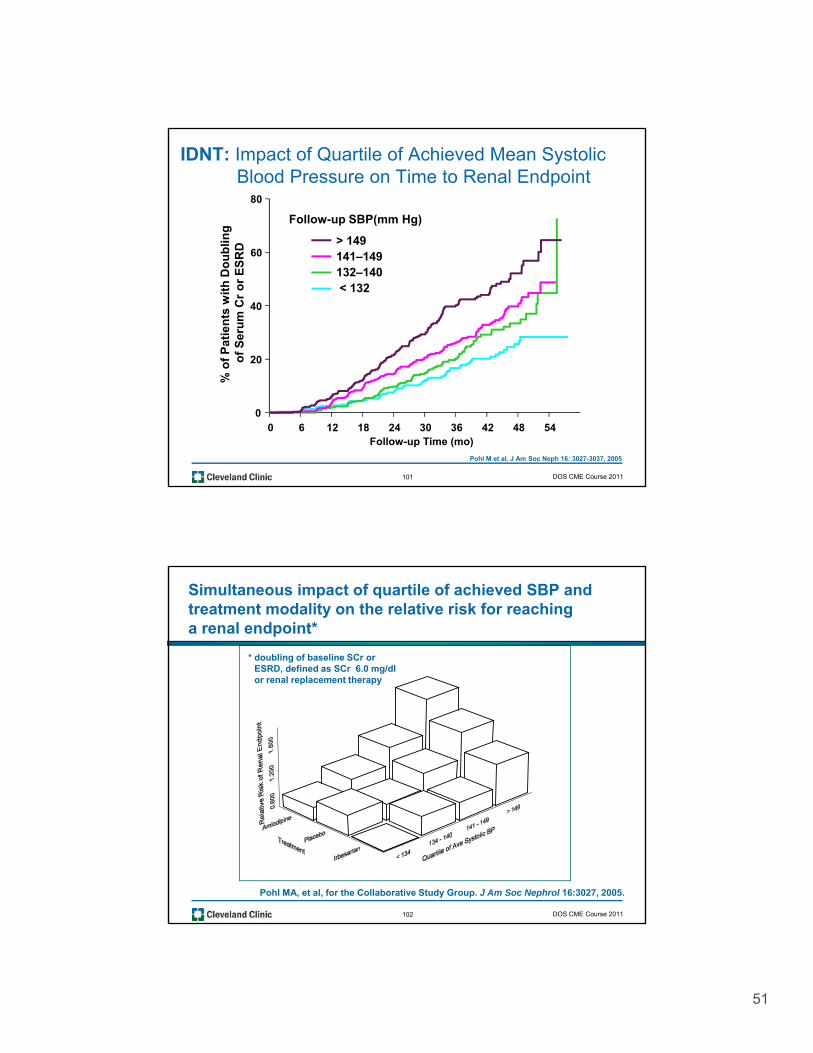
IDNTTime to Doubling of Serum Creatinine
Irbesartan
Amlodipine besylate
RRR 37%P<0.001 RRR 33%
Subjects (%)
20
30
40
50Amlodipine besylate
Placebo (control)
RRR 33%P=0.003
99
0 6 12 18 24 30 36 42 48 54
Follow-up (months)
60
0
10
Lewis EJ et al. N Engl J Med 2001;345:851-860.
DOS CME Course 2011
50
60
70
IDNTTime to Doubling of Serum Creatinine, ESRD, or Death
Irbesartan
Amlodipine besylate
Pl b ( t l)
RRR=20%P=0.02
RRR=23%P=0.006
Subjects (%)
10
20
30
40
50 Placebo (control)
100
0 6 12 18 24 30 36 42 48 54
Follow-up (mo)
60
0
10
ESRD, end-stage renal disease; RRR, relative risk reduction.Lewis EJ et al. N Engl J Med. 2001;345:851-860.
DOS CME Course 2011
51
IDNT: Impact of Quartile of Achieved Mean SystolicBlood Pressure on Time to Renal Endpoint
80
bli
ng
D > 149
Follow-up SBP(mm Hg)
20
40
60
of
Pat
ien
ts w
ith
Do
ub
of
Ser
um
Cr
or
ES
RD
141–149132–140< 132
101
0 6 12 18 24 30 36 42 48 54Follow-up Time (mo)
0
% o
Pohl M et al. J Am Soc Neph 16: 3027-3037, 2005
DOS CME Course 2011
Simultaneous impact of quartile of achieved SBP and treatment modality on the relative risk for reaching a renal endpoint*
* doubling of baseline SCr or ESRD, defined as SCr 6.0 mg/dl or renal replacement therapy
102
Pohl MA, et al, for the Collaborative Study Group. J Am Soc Nephrol 16:3027, 2005.
DOS CME Course 2011
52
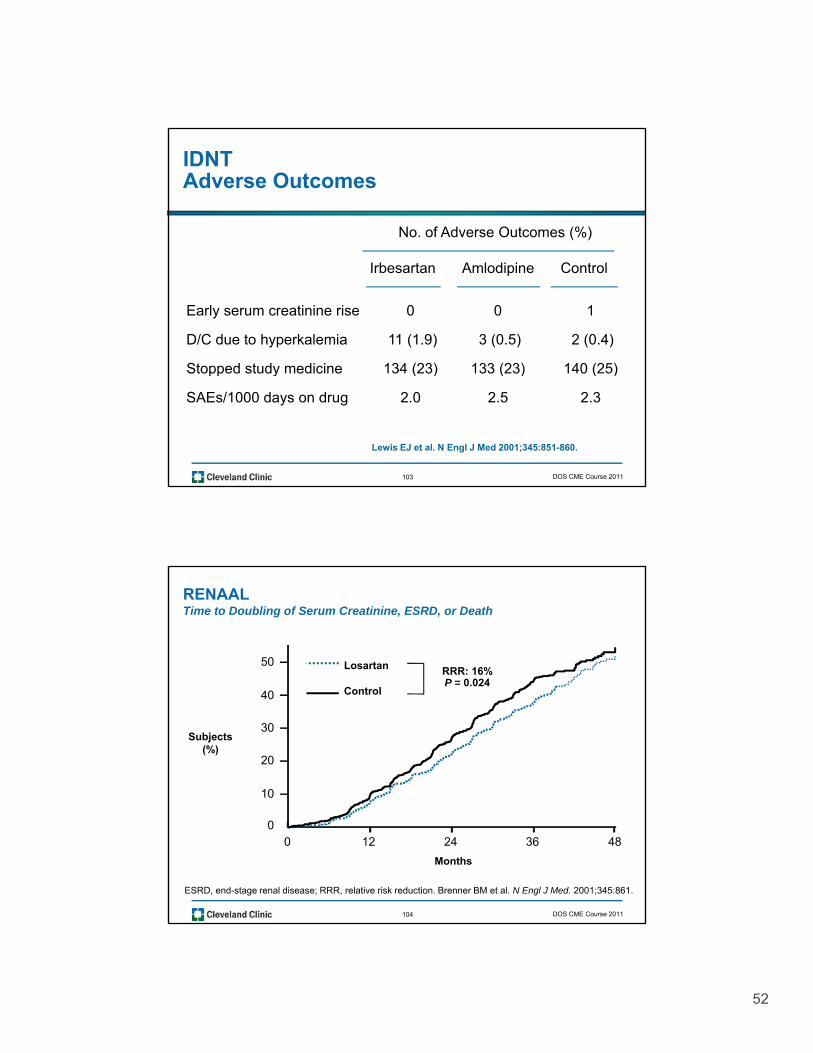
No. of Adverse Outcomes (%)
IDNTAdverse Outcomes
Early serum creatinine rise 0 0 1
D/C due to hyperkalemia 11 (1.9) 3 (0.5) 2 (0.4)
Stopped study medicine 134 (23) 133 (23) 140 (25)
Irbesartan Amlodipine Control
103
Stopped study medicine 134 (23) 133 (23) 140 (25)
SAEs/1000 days on drug 2.0 2.5 2.3
Lewis EJ et al. N Engl J Med 2001;345:851-860.
DOS CME Course 2011
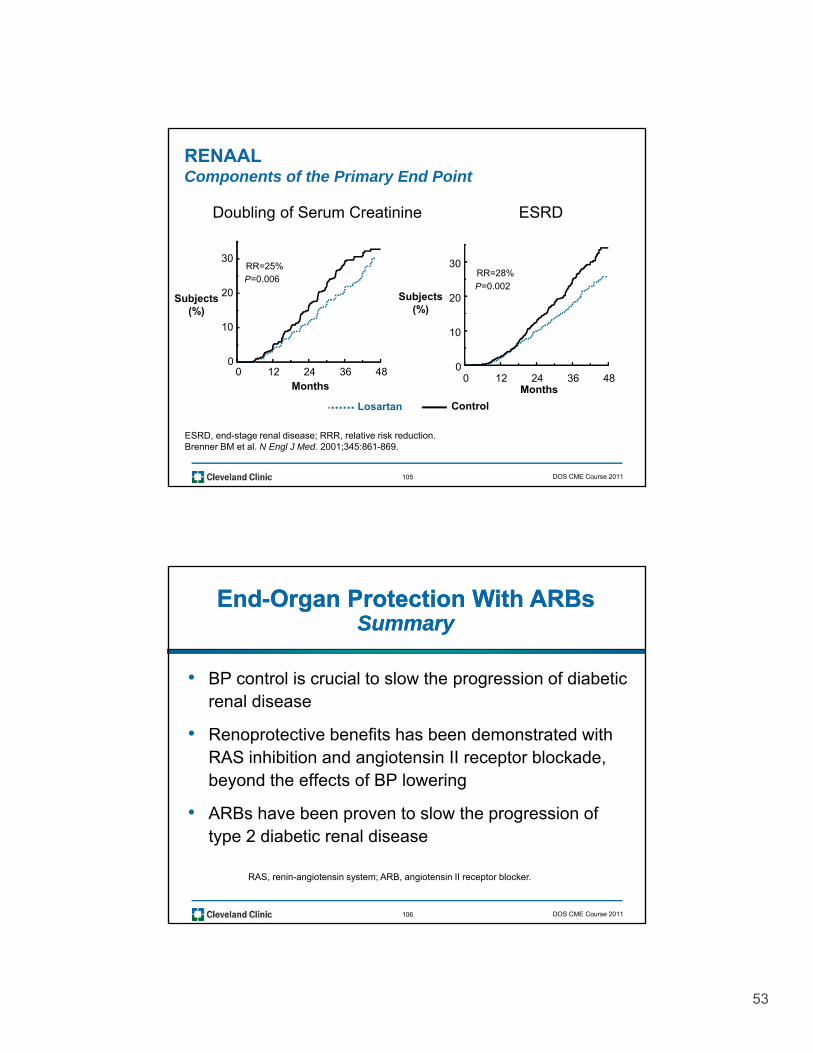
RENAALTime to Doubling of Serum Creatinine, ESRD, or Death
50 Losartan RRR: 16%P = 0.024
Subjects(%)
10
20
30
40 ControlP 0.024
104
ESRD, end-stage renal disease; RRR, relative risk reduction. Brenner BM et al. N Engl J Med. 2001;345:861.
Months
0 12 24 36 480
DOS CME Course 2011
53
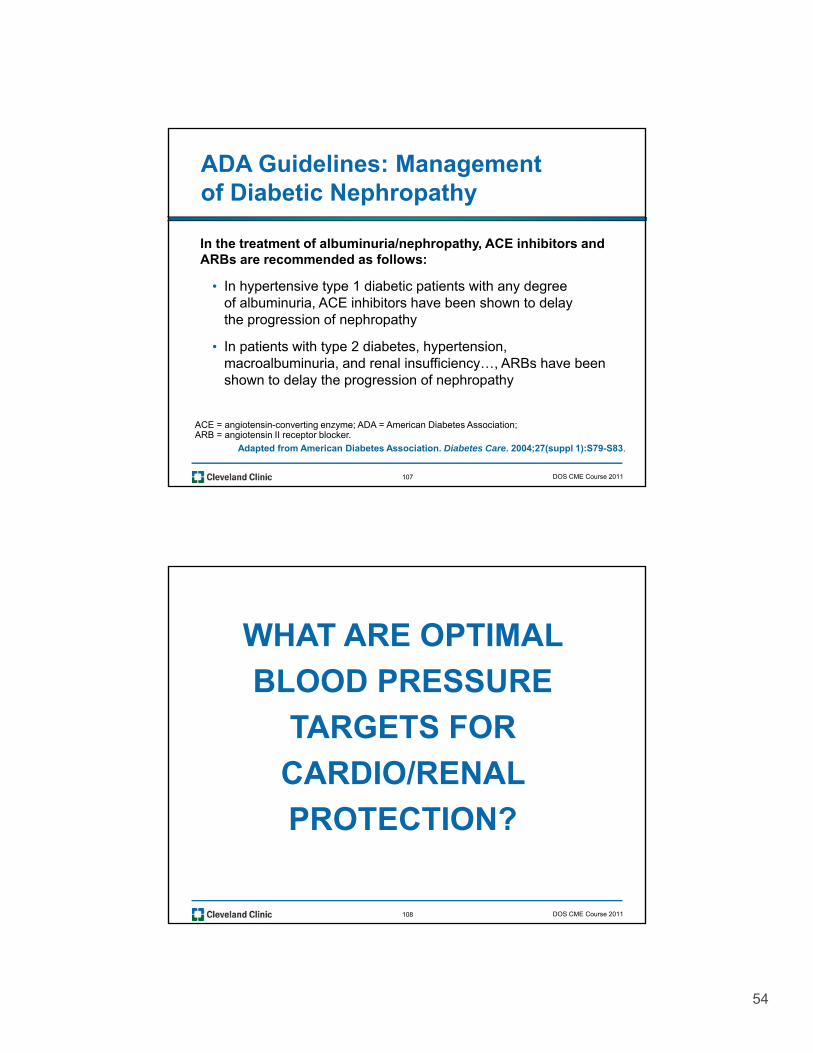
RENAALComponents of the Primary End Point
Doubling of Serum Creatinine ESRD
0
10
20
30
P=0.006RR=25%
0
10
20
30
P=0.002
RR=28%
Subjects(%)
Subjects(%)
105
0 12 24 36 48Months
0 12 24 36 48Months
0
ESRD, end-stage renal disease; RRR, relative risk reduction.Brenner BM et al. N Engl J Med. 2001;345:861-869.
Losartan Control
DOS CME Course 2011
• BP control is crucial to slow the progression of diabetic
EndEnd--Organ Protection With ARBsOrgan Protection With ARBsSummarySummary
p grenal disease
• Renoprotective benefits has been demonstrated with RAS inhibition and angiotensin II receptor blockade, beyond the effects of BP lowering
106
• ARBs have been proven to slow the progression of type 2 diabetic renal disease
RAS, renin-angiotensin system; ARB, angiotensin II receptor blocker.
DOS CME Course 2011
54
ADA Guidelines: Management of Diabetic Nephropathy
In the treatment of albuminuria/nephropathy, ACE inhibitors andIn the treatment of albuminuria/nephropathy, ACE inhibitors and ARBs are recommended as follows:
• In hypertensive type 1 diabetic patients with any degree of albuminuria, ACE inhibitors have been shown to delay the progression of nephropathy
• In patients with type 2 diabetes, hypertension, macroalbuminuria, and renal insufficiency…, ARBs have been
107
macroalbuminuria, and renal insufficiency…, ARBs have been shown to delay the progression of nephropathy
ACE = angiotensin-converting enzyme; ADA = American Diabetes Association; ARB = angiotensin II receptor blocker.
Adapted from American Diabetes Association. Diabetes Care. 2004;27(suppl 1):S79-S83.
DOS CME Course 2011
WHAT ARE OPTIMAL
BLOOD PRESSUREBLOOD PRESSURE
TARGETS FOR
CARDIO/RENAL
108
PROTECTION?
DOS CME Course 2011
55
Independent and Additive Impact of Blood Pressure Control and Angiotensin II Receptor Blockade on Renal Outcomes in the Irbesartan Diabetic Nephropathy Trial: Clinical Implications and Limitations
109
• Pohl MA, et al, for the Collaborative Study Group. J Am Soc Nephrol 16:3027, 2005.
DOS CME Course 2011
Impact of Achieved Blood Pressure on Cardiovascular Outcomes in the Irbesartan Diabetic Nephropathy TrialIrbesartan Diabetic Nephropathy Trial
• Berl T, et al., for the Collaborative Study Group.
110
, , y p
J Am Soc Nephrol 2005;16:2170.
DOS CME Course 2011
56
SUMMARY
•Lowering BP, particularly SBP, is clearly renal and cardio protective but belowrenal and cardio-protective, but below certain levels of SBP and DBP risk may occur in selected populations.
•BP of 120-125/80-85 appears to be ideal target
111
target.
• Inhibiting/blocking the RAS benefits both heart and kidney
DOS CME Course 2011
112 DOS CME Course 2011112 DOS CME Course 2011