Embed Size (px)
Citation preview

Clinical Breast Examination: PracticalRecommendations for OptimizingPerformance and ReportingDebbie Saslow, PhD; Judy Hannan, RN, MPH; Janet Osuch, MD, MS;Marianne H. Alciati, PhD; Cornelia Baines, MD; Mary Barton, MD; Janet Kay Bobo, PhD;Cathy Coleman, RN, OCN; Mary Dolan, MD, MPH; Ginny Gaumer, RN, MS;Daniel Kopans, MD; Susan Kutner, MD; Dorothy S. Lane, MD; Herschel Lawson, MD;Helen Meissner, PhD, ScM, MPH; Candace Moorman, MPH; Henry Pennypacker, PhD;Peggy Pierce, RN, MSN, MPH; Eva Sciandra; Robert Smith, PhD; Ralph Coates, PhD
ABSTRACT Clinical breast examination (CBE) seeks to detect breast abnormalities or evaluate
patient reports of symptoms to find palpable breast cancers at an earlier stage of progression.
Treatment options for earlier-stage cancers are generally more numerous, include less toxic alter-
natives, and are usually more effective than treatments for later-stage cancers. For average-risk
women aged 40 and younger, earlier detection of palpable tumors identified by CBE can lead to
earlier therapy. After age 40, when mammography is recommended, CBE is regarded as an adjunct
to mammography. Recent debate, however, has questioned the contributions of CBE to the de-
tection of breast cancer in asymptomatic women and particularly to improved survival and reduced
mortality rates. Clinicians remain widely divided about the level of evidence supporting CBE and their
confidence in the examination. Yet, CBE is practiced extensively in the United States and continues
to be recommended by many leading health organizations. It is in this context that this report
provides a brief review of evidence for CBE’s role in the earlier detection of breast cancer, highlights
current practice issues, and presents recommendations that, when implemented, could contribute
to greater standardization of the practice and reporting of CBE. These recommendations may also
lead to improved evidence of the nature and extent of CBE’s contribution to the earlier detection of
breast cancer. (CA Cancer J Clin 2004;54:327–344.) © American Cancer Society, Inc., 2004.
INTRODUCTION
The Clinical Breast Examination’s (CBE’s) Contributions to the Earlier Detection ofBreast Cancer
No clinical trial has compared CBE alone with a no-screening condition, andevidence demonstrating that mammography alone reduces breast cancer mortalitymakes it highly unlikely that a trial of CBE alone will ever be conducted.1
As discussed in the accompanying literature review,2 CBE detects some cancersnot found by mammography, although the magnitude of its contribution to theearly detection of breast cancers among asymptomatic women is relatively small.3–6
In addition, CBE may be important for women who do not receive regularmammograms, either because mammography is not recommended (ie, womenaged 40 and younger) or because some women do not receive screening mam-
Dr. Saslow is Director, Breast andGynecological Cancers, AmericanCancer Society, Atlanta, GA.
Ms. Hannan is Chief, Educationand Training Section, Program Ser-vices Branch, Division of CancerPrevention and Control, Centers forDisease Control and Prevention, At-lanta, GA.
Dr. Osuch is Professor of Surgeryand Epidemiology, Michigan StateUniversity, East Lansing, MI.
Dr. Alciati is President, Manage-ment Solutions for Health, Inc., Re-ston, VA.
Dr. Baines is Professor Emerita,Department of Health Sciences, Fac-ulty of Medicine, University of To-ronto, Toronto, Canada.
Dr. Barton is Assistant Professor,Department of Ambulatory Care andPrevention, Harvard Medical Schooland Harvard Pilgrim Health Care,Boston, MA.
Dr. Bobo is Health Research Leaderand Senior Epidemiologist, BattelleCenters for Public Health Researchand Evaluation, Seattle, WA.
Ms. Coleman is Consultant, BreastCenter Development, Tiburon, CA.
Dr. Dolan is Division Chief, Wom-en’s Primary Healthcare, Universityof North Carolina School of Medi-cine, Chapel Hill, NC.
Ms. Gaumer is Nurse Consultantfor Quality Assurance, Georgia De-partment of Human Resources, Sa-vannah, GA.
Dr. Kopans is Director, Breast Im-aging Division, Massachusetts Gen-eral Hospital, Boston, MA.
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 327

mography consistent with recom-mended guidelines.7–9 Furthermore,CBE’s contribution to women’shealth may extend beyond its abilityto identify previously undetected pal-pable masses. Specifically, CBE pre-sents an opportunity for health careproviders to educate women aboutbreast cancer, its symptoms, riskfactors, and advances in its early de-tection, as well as normal breast com-position and variability.7 It also letsclinicians discuss the benefits and lim-its of breast self-examination (BSE)and demonstrate BSE for womenwho elect to do it.
Recommendations byMajor Organizations
Organizations that provide clin-ical guidelines and practice policiesfor the early detection of breastcancer vary in their recommenda-tions for CBE. Variation is by age atinitiation, breast cancer risk status,frequency of CBE performance,and the strength of language used torecommend CBE. Some organiza-tions continue to recommend CBE,while others make no recommen-dation regarding CBE for breastcancer screening among asymptom-atic women (Table 1). For example,the revised 2003 guidelines of theAmerican Cancer Society recom-mend CBE as part of a periodichealth examination, preferably atleast every 3 years for women intheir 20s and 30s and annuallyamong asymptomatic women aged
40 years or older.7 The Susan G. Komen BreastCancer Foundation also recommends CBE atleast every 3 years among women aged 20 to 39and annually beginning at age 40.10 AnnualCBE beginning at age 40 also is recommendedby the American College of Obstetricians andGynecologists11 and the American College ofRadiology.12 The American Medical Associa-tion13 recommends CBE every 1 to 2 years for
women aged 40 to 49 years and annually be-ginning at 50 years of age.
Several international groups also recom-mend CBE. The Canadian Task Force on Pre-ventive Health Care recommends CBE every 1to 2 years among women aged 50 to 69.14 TheScottish Intercollegiate Guidelines Networkand the Royal New Zealand College of Gen-eral Practitioners15 recommend CBE amongspecific age and breast cancer risk groups. Someof these organizations also emphasize the roleof CBE in patient education and assistingwomen to become familiar with their ownbreasts.
Other US and international organizationsmake no specific recommendation either for oragainst CBE. The US Preventive Services TaskForce, for example, following a review of pub-lished literature on breast cancer screening,16,17
concluded that the evidence is insufficient torecommend for or against routine CBE aloneto screen for breast cancer. The American Col-lege of Preventive Medicine,18 the AmericanCollege of Physicians,19 and American Associ-ation of Family Practitioners20 do not addressCBE in their breast cancer screening state-ments.
Use of CBE in the United States
In practice, CBE is a common componentof current breast cancer screening and is per-formed extensively across the United States.Screening trends assessed by the NationalHealth Interview Survey found that, by 1992,90% of women aged 40 or older had everreceived a CBE (per the self-reported data),and 50% of women aged 40 or older had re-ceived a CBE in the previous year.21 Morerecent data (also from self-reports) from theBehavioral Risk Factor Surveillance System, astate survey system of health risk behaviors,suggest similar levels. Behavioral Risk FactorSurveillance System data from 2000 revealedthat an overall median across states of 91% ofwomen aged 40 years and older had a CBE atleast once.22 Additionally, the National Breastand Cervical Cancer Early Detection Program(NBCCEDP) is mandated under law to pro-vide both mammography and CBE screening
Dr. Kutner is Chair, Breast CancerTask Force of Northern CaliforniaKaiser Permanente, and Surgeon,Santa Teresa Medical Center, SanJose, CA.
Dr. Lane is Associate Dean, Continu-ing Medical Education, and Distin-guished Service Professor, Vice Chairand Residency Program Director, De-partment of Preventive Medicine,Stony Brook University School ofMedicine, Stony Brook, NY.
Dr. Lawson is Senior Medical Ad-visor, Program Services Branch, Di-vision of Cancer Prevention andControl, Centers for Disease Controland Prevention, Atlanta, GA.
Dr. Meissner is Chief, AppliedCancer Screening Research Branch,National Cancer Institute, Rock-ville, MD.
Ms. Moorman is Chief, ProfessionalEducation Unit, Cancer Detection Sec-tion, California Department of HealthServices, Sacramento, CA.
Dr. Pennypacker is Professor ofPsychology, University of Florida,and President, Mammatech Corpo-ration, Gainesville, FL.
Ms. Pierce is Assistant Professor,University of Tennessee College ofNursing, Knoxville, TN.
Ms. Sciandra is Director of BreastHealth, American Cancer Society,Eastern Division, Loudonville, NY.
Dr. Smith is Director, CancerScreening, American Cancer Soci-ety, Atlanta, GA.
Dr. Coates is Associate Director forScience, Division of Cancer Preven-tion and Control, Centers for Dis-ease Control and Prevention,Atlanta, GA.
This article is available online athttp://CAonline.AmCancerSoc.org
CBE Recommendations
328 CA A Cancer Journal for Clinicians

for the early detection of breast cancer. Now inits 12th year, the NBCCEDP has providedscreening services to uninsured women in all50 states, the District of Columbia, 6 US ter-ritories, and 15 American Indian/Alaska Nativeorganizations, including more than four mil-lion breast and cervical screening examinations,and has diagnosed more than 14,000 breastcancers.23 Taken together, these results showthat large numbers of US women have receivedat least one CBE and that many women receiveCBE on a periodic basis.
Studies of physicians vary in the proportionsreporting routine performance of CBE. Forexample, one study of family physicians andinternists in Long Island community hospitals
showed that only 56% regularly performedCBE on women aged 50 to 75 years,24 but ina study of preventive services delivery amongfamily practice physicians in Ohio, 85% ofwomen aged 50 to 69 years were observed toreceive a CBE during well visits.25 Severalstudies found that the proportion of physiciansreporting routine performance of CBE variedas a function of specialty.26,27
Barriers to High-quality Performance
Although CBE generally continues to be rec-ommended by many groups as a component ofcomprehensive breast cancer screening and is per-formed by large numbers of US physicians, the
TABLE 1 Recommendations by Major Health Organizations for the Performance of CBE AmongAsymptomatic Women
Organization
RecommendationsRole in Breast
Awareness andPatient/Provider
Interaction
Age (years)
20–39 40–49 50 and older
United StatesGovernment-convened panel
United States Preventive ServicesTask Force
No recommendation No recommendation No recommendation Not discussed
Professional associationsAmerican College of Obstetricians
and GynecologistsNo recommendation Annually Annually Not discussed
American College of Physicians No recommendation No recommendation No recommendation Not discussedAmerican College of Radiology No recommendation Annually Annually Not discussedAmerican Medical Association No recommendation Every 1–2 years Annually All medical care decisions
should involve patient/provider deliberation
American College of PreventiveMedicine
No recommendation No recommendation No recommendation Not discussed
American Association of FamilyPractitioners
No recommendation No recommendation No recommendation Not discussed
Voluntary health organizationsAmerican Cancer Society As part of a periodic
health examinationAs part of a periodic
health examinationAs part of a periodic health
examinationOpportunity for women and
providers to discuss breastPreferably at least
every 3 yearsPreferably annually Preferably annually changes
Susan G. Komen Breast CancerFoundation
At least every 3 years Annually Annually Opportunity for women andproviders to discuss breastchanges
InternationalGovernment agency
Canadian Task Force on PreventiveHealth Care
No recommendation No recommendation Every 1 to 2 years, womenaged 50 to 69 years
Not discussed
Scottish Intercollegiate GuidelinesNetwork
Annually among highrisk women
Annually among highrisk women
Continue more frequentscreening
Not discussed
Professional associationRoyal New Zealand College of
General PractitionersNo recommendation No recommendation In conjunction with biennial
mammography (aged 50to 74 years)
Not discussed
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 329

way in which it is performed varies consider-ably.2,28 In the NBCCEDP, reporting is stan-dardized, but the method of performing CBE isnot.3 The technique has also not been standard-ized in most screening trials.1,2 While the sensi-tivity and specificity of CBE were generallycomparable across the NBCCEDP and screeningtrials, these levels of performance are lower thanwhat could be achieved with standardization oftechnique and training to that standard.
Studies that used well-described, standardizedmethods for performing CBE provide some ev-idence of higher levels of sensitivity in clinicalexamination.1,9 Training studies using objective,structured clinical examination have observedimprovements in performance of CBE tech-niques and in patient interaction skills.29 Studiesusing silicone breast models show that both train-ing in CBE technique and experience in detect-ing breast lumps can increase sensitivity fordetecting lumps in the models,28,30,31 althoughspecificity in many studies declines at higher levelsof sensitivity.2 A study demonstrated that trainingwith silicone breast models increased detection ofknown benign lumps in women,32 providing ev-idence that detection skills learned using siliconemodels can be effectively applied to patients.
Despite the potential of training to enhanceperformance, studies of medical students andresidents reveal low performance scores on ob-jective examinations of CBE components, aswell as low sensitivity and specificity using sil-icone breast models.29,33 Medical students’perceptions of their own need for additionaltraining and the small number of CBEs theyhave actually performed illustrate the limits ofcurrent medical school training in the perfor-mance of CBE.2,29,31,32 Similarly, physiciansreport lack of confidence in their CBEskills34–36 and indicate high levels of interest inimproving them.36
Developing Recommendations for CBEPerformance and Reporting
CBE presents an interesting challenge for clin-ical practice and public health. It is widely prac-ticed, yet concern remains about its effectivenessin reducing breast cancer mortality. CBE appearsto find some cancers missed by mammography—
although a small proportion—and may be usefulin women for whom mammography is not rec-ommended or who do not receive screeningmammography consistent with recommendedguidelines. CBE is practiced with little standard-ization despite reasonable evidence that perfor-mance can be improved by training andexperience. Furthermore, the lack of standardizedperformance and reporting has limited the avail-ability of data to address questions about CBE’srole in breast cancer detection.
In this context, the American Cancer Soci-ety, in collaboration with the Centers for Dis-ease Control and Prevention, initiated aplanning process to develop recommendationsfor optimizing the performance and reportingof CBE. Providing standards that are based onexisting literature and expert opinion shouldlay the foundation for enhancing test sensitivityand specificity to the extent possible and pro-vide a valuable tool to assist providers in im-proving test performance and communicatingabout test findings within and across specialties.Such assistance is particularly important in thecase of breast cancer, where failure to diagnoseis the primary cause for malpractice claims inthe United States and the second-leading rea-son for subsequent payments to claimants.37
Furthermore, enhancing the standardization ofCBE performance, combined with more uni-form interpretation and reporting, will providea basis for gathering much-needed data aboutthe nature of CBE’s contribution to earlierdetection of breast cancer. Such data are essen-tial to resolving inconsistent practice guidelinesacross organizations and the resulting confusionfor women and their health care providers.
The process of developing recommenda-tions for CBE performance and reporting be-gan with a thorough review of the literature.2
This review covered numerous areas, includingtrials and case series reports; standards (or lackthereof) for performing CBE and reporting re-sults; factors influencing specificity and sensi-tivity; proficiency of providers in performingCBE; the effect of provider training, experi-ence, and specialty on proficiency; and barriersto performing CBE.
Additionally, to ensure that the full range ofclinical and public health issues related to CBE
CBE Recommendations
330 CA A Cancer Journal for Clinicians

performance and reporting were addressed, in-terviews were conducted with experts in theearly detection of breast cancer. These expertsidentified issues that needed to be addressed tounderstand the contribution of CBE to the de-tection of breast cancer and what would be re-quired to realize substantial improvements inperformance and reporting. The issues identifiedincluded the level of evidence supporting CBE asa screening examination, test characteristics, cur-rent practices, interpretation and reporting of re-sults, examiner training, and CBE’s relationshipto other screening tests for breast cancer.
Based on the research literature and expertguidance, a committee was formed of nationaland international experts well versed in CBE andits performance and reporting. This committeewas charged with developing recommendationsfor physicians and health organizations that wouldenhance CBE performance and reporting.
Members of the committee conferred inworking groups and as a full committee througha series of conference calls and a face-to-facemeeting held in Atlanta on October 10 and 11,2002. The committee also worked in concertwith a related American Cancer Society advisorygroup, the Breast Physical Examination WorkingGroup (one of five working groups within theBreast Cancer Early Detection Guideline Re-view).7 Early drafts of the committee’s reportwere disseminated to a broad range of profes-sional and public health organizations for reviewand comment. After comments were compiledand assessed, modifications were made to thereport.
The intent of this effort was to provide aframework for standardization, recognizingthat additional detail would be needed in someareas (eg, development of a lexicon for inter-preting and reporting that would be compatiblewith the Breast Imaging Reporting and DataSystem, development of a sample reportingform) and that implementation of some recom-mendations would require additional efforts in-volving collaboration among organizations andsupplemental funding. Identification of pro-cesses and funding for implementation werebeyond the scope of the committee’s work.The committee envisioned that the reportwould provide a tool for immediate action in
some areas and a stimulus for follow-up actionin others.
This report provides detailed descriptions ofeach recommendation, its components, thecommittee’s rationale for the recommendation,and responsibilities for implementation. Thebalance between support from research andfrom practical evidence varies across recom-mendations. In general, evidence about CBE,including its contributions to early detection ofbreast cancer and subsequent reduction in mor-tality as discussed above, as well as factors thatinfluence its performance, is limited. As a re-sult, several aspects of these recommendationsrely on clinical expertise and practical experi-ence. Not surprisingly, the committee’s finalrecommendation is a call for research into par-ticular questions that will provide a firmerfoundation for decisions about the practice ofCBE as a component of women’s health care.
RECOMMENDATIONS
Recommendations are presented in two areas,the clinical breast examination itself and over-coming barriers to performance. Some recom-mendations can be implemented immediatelywithin clinical settings, and clinicians are encour-aged to lead this effort (Table 2). Others willrequire partnerships between the clinical com-munity and health care organizations to establishsystems, increase awareness, and gather necessaryinformation to achieve outcomes.
BREAST EXAMINATION
The premise underlying CBE is that visuallyinspecting and palpating of the breast and sur-rounding tissue can detect breast abnormalities.CBE was considered by the committee to in-clude a continuum of integrally related com-ponents, from the examination itself, tointerpretation and reporting of findings, to pa-tient follow up. The recommendations for per-formance in this report represent generalstandards that can be immediately disseminatedand adopted based on current evidence. Al-though these recommendations reflect an im-
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 331

portant first step, the committee recognizes theneed for more detailed practice algorithms andfor reporting forms that have been tested. Ef-forts to develop these follow-up tools are cur-rently planned.
Neither CBE nor mammography is a substi-tute for the other as an independent examinationfor detecting breast abnormalities. When a suspi-cious mass is found on CBE, it must be evaluatedand explained even if mammography examina-tion does not show an abnormality.1. The Examination:
a. Adopt standards for CBE that include astepwise progression of elements con-
sisting of clinical history, visual inspec-tion, and palpation.Lead responsibility for implementation: cli-nicians.
b. Encourage widespread dissemination ofstandards for CBE.Lead responsibility for implementation: healthcare organizations.
Studies have assessed the influence of testcharacteristics (such as search pattern, palpa-tion, pressures, duration), patient characteristics(such as tissue density, and nodularity), andtumor characteristics (such as size, depth, mo-bility) on the CBE’s sensitivity and specificity.2
TABLE 2 Summary of CBE Recommendations and Lead Responsibility for Implementation
Lead Responsibility
CliniciansHealth care
organizations
Researchsponsoring
organizations
CBEThe examination
Adopt standards for CBE that include a stepwise progression of elements consisting ofclinical history, visual inspection, and palpation.
✓
Encourage widespread dissemination of standards for CBE. ✓Interpretation and reporting
Reporting should consist of a summary of relevant portions of a patient’s history and adescription of whether the CBE is interpreted as normal/negative or abnormal. Ifabnormal, include a description of the visual and palpable finding, including changesin the appearance of skin or nipples, the presence of nipple discharge, the presenceof breast masses or palpable asymmetries, and the presence of palpable lymphnodes.
✓ ✓
Develop a consistent, standardized lexicon and format for documenting the interpretationand reporting of specific CBE findings.
✓
Follow upAdopt a standardized approach to follow up that provides continuous care to the patient
until an appropriate resolution of findings is reached. This approach should make useof all appropriate follow-up options, ensure appropriate timing of subsequent actions,involve communication and coordination with other providers, and include properdocumentation and tracking.
✓
Overcoming barriers to the implementation of CBEExaminer training
Develop and promote training systems to improve and maintain the proficiency of thosewho perform CBE, and encourage the integration of such systems into basic andcontinuing education programs for health care professionals.
✓
Public educationPromote and encourage public education about CBE so that women know what to
expect in the performance of CBE and follow-up care, understand the benefits,limitations, and potential harms associated with CBE, and become familiar with theirown breast characteristics as well as health practices that might increase thelikelihood of identifying breast abnormalities.
✓
Research and quality improvementSupport and encourage research in key aspects of CBE, particularly questions related to
characteristics of abnormalities found by CBE, the timing of the examination, trainingof examiners (clinicians), reporting systems, and CBE’s contributions to earlydetection of breast cancer, and the reduction of morbidity and mortality from thisdisease.
✓ ✓
CBE Recommendations
332 CA A Cancer Journal for Clinicians

CBE techniques have been described and illus-trated in several recent reviews;1,2,38 figuresfrom one of these reviews are used to illustratethe recommendations presented here (Figures1–3).1 These studies provide some basis forrecommendations concerning the specific wayCBE is performed. Not all aspects of visualinspection and palpation have been studied incontrolled settings, however, and thus the fol-lowing recommendations rely in part on theclinical expertise of the committee and thepremise that visual inspection and palpation ofevery area of the breast and surrounding tissuewill lead to identification of more breast masses.
Clinicians are encouraged to adopt and imple-ment the following standards for performanceof the CBE examination. Efforts to encouragewidespread dissemination of these standards mustbe implemented as a partnership between clini-cians and health care organizations.
Clinical History
A clinical history that identifies the patient’spersonal and family health history is useful inassessing risk of breast cancer. Some womenwill not report symptoms until asked, and aclinical history provides an important opportu-nity to seek out this information. This healthhistory can direct attention to potentially rele-vant symptoms and provides important contextfor interpreting findings. The clinical guide-lines and policy statements of many organiza-tions concerning the performance of screeningCBE emphasize the importance of a woman’sindividual risk for breast cancer.15 Further-more, information on clinical history can helpguide follow up. The clinical history also pro-vides an opportunity for the provider to ex-plain the benefits and limitations of theexamination, its elements, the time involved,and the related events that occur after the ex-amination (interpretation, reporting, and fol-low up).
The clinical history should:Y Identify screening practices for breast
health, when they were performed, andresults. These practices include breast self-examination (BSE), prior CBE, and priorscreening and diagnostic mammograms.
Y Ask about any breast changes and howthey were identified. This includes changesin appearance of skin or nipples, presenceof lumps, pain (focal versus general andconstant versus cyclic), itching, or stainingof garments or bed sheets that would indi-cate spontaneous nipple discharge.
Y Assess risk by asking about age and per-sonal history, including benign breast dis-ease, biopsy, cancer, cosmetic or otherbreast surgery, history of hormonal ther-apy, and/or oral contraceptive use, obstet-ric history, family history, and healthpromotion habits (eg, exercise, nutrition).
Visual Inspection
Once the clinical history has been com-pleted, the patient’s breasts should be visuallyinspected. To minimize awkwardness and po-tential misunderstandings, providers should in-form women in advance that a visual inspectionwill be performed and describe what is beingassessed during this part of the examination.The patient should sit with her hands pushingtightly on her hips. This position contracts thepectoralis major muscles and enhances identi-fication of asymmetries. Although adding mul-tiple positions (eg, hands over head and handsat sides) may further assist identification ofasymmetries, it does not add substantively tothe single position recommended and may re-duce time devoted to palpation. When con-ducting the visual inspection, the providermust view the breasts from all sides and should:Y Assess symmetry in breast shape or contour
(subtle changes or differences),2,38,39 andY Assess skin changes, particularly any skin ery-
thema, retraction or dimpling, and nipplechanges.2,38,39 Physical signs associated withadvanced breast cancer have been summa-rized using the acronym BREAST, signify-ing Breast mass, Retraction, Edema, Axillarymass, Scaly nipple, and Tender breast.38
If the clinician is seeing the patient on aregular basis, visual inspection allows the mon-itoring of changes in appearance over timewhen observations are compared with previ-ously documented examination. Visual inspec-tion takes only a short amount of time, with the
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 333

remainder of the examination spent predomi-nately on palpation.
Palpation
Following the visual inspection, the exam-iner palpates each breast and nearby lymphnodes. To minimize awkwardness and the po-tential for misunderstanding, providers shouldinform women in advance that palpation willbe performed and describe what is being as-sessed during this part of the examination. Pal-pation provides an opportunity for discussionof the normal variability of breast characteristicsand the importance of women becoming fa-miliar with the characteristics of their ownbreasts. Thoroughness is essential; palpationmust examine all breast tissue as well as nearbylymph nodes. Appropriate palpation includesfive key characteristics:Y Position: Patients should be sitting for
palpation of the axillary, supraclavicular,and infraclavicular lymph nodes. Patientsshould be lying down for breast palpation,with their ipsilateral hand overhead to flat-
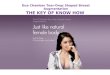
ten the breast tissue on the chest wall,thereby reducing the thickness of thebreast tissue being palpated (Figure 1). Ifthis maneuver does not result in a rela-tively even distribution of breast tissue, thebreast should be further centralized byplacing a small pillow under the shoulder/lower back on the side of the breast beingexamined. The tissue being examinedneeds to be as thin as possible over thechest wall. The examiner must be able tosee the full palpation area.
Y Perimeter: All breast tissue falls within apentagon shape (as opposed to the tradi-tional perception of the breast as a conicalstructure). The examiner should use thefollowing landmarks to cover all of thisarea: down the midaxillary line, across theinframammary ridge at the fifth/sixth rib,up the lateral edge of the sternum, acrossthe clavicle, and back to the midaxilla.
Y Pattern of search: The full extent ofbreast tissue should be searched using a“vertical strip” pattern (Figure 1).2,40 (Asystematic analysis demonstrated the supe-
FIGURE 1 Position of Patient and Direction of Palpation for the CBE.The top figure shows the lateral portion of the breast, and the bottom picture shows the medial portion of the breast. Arrowsindicate the vertical strip pattern of examination. (Reprinted with permission from Barton MB, Harris R, Fletcher SW.1)
CBE Recommendations
334 CA A Cancer Journal for Clinicians

riority of the vertical strip search patternover concentric circle and radial spoke pat-terns in thoroughness of coverage, as per-formed by women trained in BSE toexamine themselves.40) The search shouldbe initiated at the axilla. If a mastectomyhas been performed, the chest wall, skin,and incision should be included.
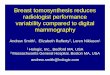
Y Palpation: The examiner should use thefinger pads of the middle three fingers to pal-pate one breast at a time (Figure2). Palpate with overlapping dime-sized cir-cular motions.2,30 Tissue at and beneath thenipple should be palpated, not squeezed.Squeezing often results in discharge as well asdiscomfort. Only spontaneous discharge war-rants further evaluation.41 Breast tissue in theupper outer quadrant and under the areolaand nipple should be thoroughly searched, asthese are the two most common sites forcancer to arise.42
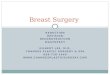
Y Pressure: As each area of tissue is exam-ined, three levels of pressure should be ap-plied in sequence: light, medium, anddeep, corresponding to subcutaneous, mid-level, and down to the chest wall (Figure3). Adapt the palpation to the size, shape,and consistency of tissue, and accommo-date pressure to other factors such as breastsize and the presence of breast implants.Providers sometimes lack confidence per-forming CBE in women with breast im-plants; implants correctly placed are locatedbehind the tissue of the breast. Therefore,the steps for CBE are exactly the same asin women without implants.The duration of the examination is intention-
ally not specified, for several reasons. First, whilethoroughness is related to time spent performingCBE, performance time can decrease with in-creased proficiency. Additionally, a variety of pa-tient factors, such as breast size, tenderness,
FIGURE 2 Palpation Technique.Pads of the index, third, and fourth fingers (inset) make small circular motions, as if tracking the outer edge of a dime.(Reprinted with permission from Barton MB, Harris R, Fletcher SW.1)
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 335

lumpiness, body weight, and risk factors, can in-fluence the time required to perform a proficientCBE. The committee determined that specifyinga uniform time frame would be misleading moreoften than not and would inappropriately shift thefocus of performance away from proficiency andthoroughness.2. Interpretation and Reporting:
a. Reporting should consist of a sum-mary of the relevant portions of a pa-tient’s history and a description ofwhether the CBE is interpreted asnormal/negative or abnormal. If ab-normal, include a description of the
visual and palpable findings, includingchanges in the appearance of skin ornipples, the presence of nipple dis-charge, the presence of breast massesor palpable asymmetries, and the pre-sence of palpable lymph nodes.Lead responsibility for implementation: cli-nicians and health care organizations.
b. Develop a consistent, standardized lexi-con of terms and format for document-ing the interpretation and reporting ofspecific CBE findings.Lead responsibility for implementation:health care organizations.
FIGURE 3 Levels of Pressure for Palpation of Breast Tissue Shown in a Cross-sectional View of the Right Breast.The examiner should make three circles with the finger pads, increasing the level of pressure (subcutaneous, mid-level,and down to the chest wall) with each circle. (Reprinted with permission from Barton MB, Harris R, Fletcher SW.1)
CBE Recommendations
336 CA A Cancer Journal for Clinicians

The primary function of CBE is to identifyabnormalities that warrant further evaluation;CBE alone is not capable of accurately distin-guishing benign from malignant status. Inter-preting the visual and tactile observations ofCBE is complex. A variety of patient charac-teristics can influence interpretation, includingage, parity, tissue density and nodularity,menopausal status, phase of the ovarian cycle,and health history.2 For example, bloody nip-ple discharge during the last trimester of preg-nancy or the first 3 months of lactation may beconsidered a normal physiologic change, but itwould be interpreted quite differently in awoman who was not pregnant or lactating.Similarly, skin erythema or lymphedemawould not necessarily be cause for further eval-uation in a woman having recently undergoneradiation therapy of the breast but would cer-tainly require follow up in a woman withoutsuch a history. A more common and difficultchallenge involves breast lumpiness or nodular-ity, which varies considerably among womenand over time for the same woman. For exam-ple, increased nodularity might be normal dur-ing the luteal phase of the menstrual cycle, butat other times it might be cause for furtherexamination.
As with the performance of CBE, no standardsystem exists for interpreting or reporting CBEfindings. No standardized terminology exists fordescribing findings such as degree of nodularity;thickening versus a mass; dimpling of skin; or thesize, mobility, shape, or consistency of an abnor-mality. Thus, even if CBE was performed uni-formly to its highest potential sensitivity andspecificity, differences in interpretation and howfindings are reported limit its potential benefits inguiding further evaluation and permitting earliertreatment of breast cancer. Efforts to improve theinterpretation of mammography reporting andsubsequent associated management recommen-dations have resulted in improvements in accu-racy and consistency in those areas, but severalstudies demonstrate the importance of continuedsystem refinement and training.43–45 Standardiza-tion of interpretation and reporting might yieldsimilar positive effects for CBE. Although devel-opment of a detailed lexicon for CBE was be-yond the scope of this initiative, the committee
recommends further development of a systemthat complements the Breast Imaging Reportingand Data System and its lexicon developed by theAmerican College of Radiology. The frameworkprovided below under Reporting represents aninitial step in this process and provides immediateguidance for practice.
Another important byproduct of standardiz-ing interpretation and reporting is the potentialto provide data for more accurate estimates ofsensitivity and specificity in clinical practicesettings. Estimates of false-positive and false-negative results based on reporting and medicalrecords data could be used to provide feedbackto health care professionals to improve theirproficiency.
Information about the number of cancers firstidentified by CBE, particularly as a function ofage and other population characteristics, couldhelp clarify the role of CBE as a component ofearly detection and the use of this examination inrelationship to other screening modalities.
Interpretation
Interpretation involves three elements: identi-fication of visual and palpable characteristics ofthe breasts and lymph nodes; accurate assignmentof specific, common, descriptive terminology toeach characteristic; and determination of appro-priate follow-up actions for identified findings.The interpretation and reporting elements de-scribed below provide a general framework foridentifying all relevant features of a proficientCBE, describing visual and physical findings, andreporting these findings and follow-up recom-mendations. This framework is general, repre-senting an important initial step in the process ofdeveloping a standardized lexicon and patient fol-low up, as well as a reporting format for CBE.Describing and interpreting findings can be chal-lenging, as when women have highly nodularbreasts, for example. The role of CBE, however,is to identify and appropriately describe visual andpalpable findings; determination of benign or ma-lignant status can be established only throughfurther evaluation. Clinicians are encouraged toadopt and begin implementing this frameworkfor CBE interpretation and reporting. Develop-ment and implementation of a detailed system, as
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 337

well as analysis of reporting data, must be under-taken as a partnership between clinicians andhealth care organizations.
In the most general form, the results of CBEcan be interpreted in two ways:Y Normal/Negative: No abnormalities on
visual inspection or palpation.Y Abnormal: Asymmetrical finding on either
visual inspection or palpation that warrantsfurther evaluation and possible referral. Find-ings will reflect a continuum of possible out-comes, from probably benign to highlysuspicious of cancer. Determination of be-nign or malignant status, however, can be es-tablished only through further evaluation.
Reporting
Reporting should include a description of allfindings in specific and precise language, re-gardless of interpretation. In the case of a neg-ative interpretation, description of findingsprovides a baseline for interpreting future re-sults from visual inspection and palpation. Inthe case of an abnormal interpretation, a de-scription provides an important guide forfollow-up examination.
Reporting should follow the same se-quence as the examination itself. The follow-ing outline directs providers’ attention tothose aspects of the exam that representunique patient characteristics or abnormali-ties. To the extent possible, electronic re-porting should be encouraged to providecompatibility with existing medical recordssystems and more efficient analysis of report-ing trends. Additional research assessing re-porting consistency, feasibility, and systems-related issues should be performed.
Normal/Negative CBE: NormalBreast Characteristics
Y Clinical history – describe:X Breast screening practices.X Breast changes.X Risk factors for breast cancer.X Hormonal factors at time of examination
(eg, time in menstrual cycle, pregnancy,breast feeding, hormonal contraceptives,hormone therapy).
Y Visual inspection – describe:X Scarring.X Symmetry of breast shape and appear-
ance of skin and nipple-areolar complex.Y Palpation of lymph node – describe results
with respect to:X Infra- and supraclavicular nodes.X Axillary nodes.
Y Breast palpation – describe results with re-spect to:X Nodularity.
� Normal nodularity should not be de-scribed as a fibrocystic condition.
� Normal cyclic breast tenderness shouldnot be described as a pathologiccondition.
X Symmetry.X Tenderness (focal versus generalized and
constant versus intermittent).Y Recommended follow up.
Abnormal CBE: AbnormalBreast Characteristics
Y Clinical history – describe:X Breast screening practices.X Breast changes.X Risk factors for breast cancer.X Hormonal factors at time of examination
(eg, time in menstrual cycle, pregnancy,breast feeding, hormonal contraceptives,hormone therapy).
Y Visual inspection – describe:X Contour (skin retraction, dimpling).X Color (erythema).X Texture (skin thickening or lymphed-
ema).X Skin retraction or dimpling.X Nipple scaling or retraction.X Nipple inversion (age of onset during
adulthood).X Location of abnormal findings or mass ac-
cording to a clock face as the examinerfaces the patient, clearly indicating whetherthe abnormality is in the right or leftbreast.
X Size/extent of abnormal finding or mass.Y Palpation – for each palpable abnormality
(including breast tissue and infraclavicular,
CBE Recommendations
338 CA A Cancer Journal for Clinicians

supraclavicular, and axillary lymph nodes),describe:X Three-dimensional dominant mass or
two-dimensional thickening.� Location in three dimensions (subcuta-
neous, midlevel, next to chest wall,and according to a clock face as theexaminer faces the patient).
� Size.� Shape (round, oblong, irregular, lobu-
lar �having one to four rounded orcurved extensions from a centralmass�).
� Mobility (mobile, fixed to skin orchest wall).
� Consistency (soft, similar to surround-ing breast tissue, hard).
� External texture (smooth, irregular�having bumps distributed over the ex-ternal surface of the mass�).
X Nipple discharge.� Spontaneous.� Color.� Number of involved ducts.� Right or left breast, or both.
Y Recommended follow up.3. Follow Up:
Adopt a standardized approach to followup that provides continuous care to thepatient until an appropriate resolution offindings is reached. This approach shouldmake use of all appropriate follow-up op-tions, ensure appropriate timing of subse-quent actions, involve communication andcoordination with other providers, and in-clude proper documentation and tracking.Lead responsibility for implementation: healthcare organizations.
The final but equally important componentof the CBE is follow up; different types offindings will require different follow-up ac-tions, but appropriate follow up is essential.The committee recommends the following ba-sic approach for follow up, supplemented bymore detailed follow-up algorithms appropri-ate to the provider’s profession and uniquehealth care system.
Follow Up for Normal/Negative CBE
In the case of a normal/negative CBE, arepeat CBE at the next screening interval orpreventive health examination is the appropri-ate follow up. Descriptive findings from thenormal/negative CBE should serve as the base-line for the next interval CBE.
Follow Up for Abnormal CBE
In the case of an abnormal CBE:Y The provider should not discount an ab-
normal CBE because of a negative mam-mogram or other imaging examination.
Y Providers must follow up all conflicting orabnormal findings to satisfactory resolutionusing the actions outlined below.
Y All referrals must ensure that a copy of theCBE report is provided to specialists per-forming follow-up imaging to assist in ex-amination and interpretation.One or more of the following follow-up
options are available:Y Repeat CBE.Y Medical management of probably benign
condition.Y Referral to a breast specialist.Y Imaging (ultrasound, mammography, mag-
netic resonance imaging).Y Aspiration.Y Biopsy (percutaneous or excisional).
Timing
The timing of follow-up actions must beappropriate to the findings and should be de-signed to minimize patient burden and psycho-logical stress. For women aged 40 and older, arepeat CBE in the case of negative findings willlikely occur as part of the woman’s regularpreventive health care. Among women aged 40and younger with a negative CBE, this intervalmay be longer. In the case of abnormal find-ings, follow up should take place at a shorterinterval, at least within 6 months and usuallywithin a shorter time frame.
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 339

Coordination
If follow up is necessary, examiners mayneed to work with other care providers, in-cluding radiologists, oncologists, surgeons,and other breast health specialists. Clearcommunication about follow up and effec-tive coordination of any follow-up actionsare essential.
Tracking to Ensure That Follow Up Has Occurred
Appropriate tracking must be in place toensure that follow up has occurred. This in-volves making adequate documentation, re-minders to resolve outstanding issues or patientquestions, having a system for patient callbackand reminders, and taking actions to obtainpatient feedback.
OVERCOMING BARRIERS TO THE PERFORMANCEOF CBE
The recommendations forwarded by thecommittee to address barriers to proficientCBE focus on examiner training, public edu-cation, and research and quality improvement.4. Examiner Training:
Develop and promote training systems toimprove and maintain the proficiency ofthose who perform CBE, and encouragethe integration of such systems into basicand continuing education programs healthcare professionals.Lead responsibility for implementation: healthcare organizations.
CBE training should build on existing trainingprograms designed to improve CBE proficiencyand include the components described below. Inaddition, training programs should be made moreavailable, and these programs integrated intomedical and nursing school curricula, programsfor residents and fellows, and continuing medicaland nursing education. Expanding the availabilityof training will require collaborative effortsamong clinicians, health organizations, and thecommunity.
Training Components
Didactic Presentation
Training should include a didactic presenta-tion that:Y Provides basic information on the anatomy
and physiology of the breast.Y Provides the rationale for performing CBE
through background information on breasthealth and disease.
Y Identifies and describes elements of standardCBE—clinical history, visual inspection, pal-pation, interpretation and reporting, andfollow-up of abnormal results to resolution.
Visual Presentation
Training also should include a visual, real-time CBE performance—either a video ordemonstration—so that trainees can see correctCBE techniques.
Practice and Feedback
Finally, and no doubt most important, traineesshould have an opportunity to practice CBE skillsand to obtain feedback from experienced exam-iners. This skills-building element should involvethe use of high-quality silicone models and, ifpossible, instructors posing as patients. Live mod-els provide a more realistic clinical experience,allow training in components of CBE beyondpalpation, provide palpation experience withbreast tissue, and can provide valuable feedbackabout provider-patient interactions. If instructorsare not available to pose as patients during theinitial training, training programs should developa plan for ensuring that trainees are given skillspractice on live models with feedback in the nearfuture. Training also must include measuring anddemonstrating adequate levels of sensitivity andspecificity of lump detection.
Training Characteristics
Training Should Be Flexible to AccommodateDiverse Settings and Trainee Needs
Training programs should be tailored to suita variety of settings, including basic medicaleducation, residency, fellowship, nursing edu-
CBE Recommendations
340 CA A Cancer Journal for Clinicians

cation, and continuing medical education.Training in all three components—the exami-nation, interpretation and reporting, and fol-low up—may not be possible to complete inone session or a brief series of sessions. It maybe more effective in some cases to divide train-ing into phases so that examiners can improvetheir skills in each component through succes-sive sessions.
Participation in Training Should BeIncentive Based
Training and retraining programs need toprovide incentives for health care professionalsto participate, such as continuing educationunits, information and skills for clinicians, andcertification that might reduce the clinician’srisk of successful malpractice claims.
Training Should Offer General Guidance onFollow Up That Focuses on Resolutionof Findings
The level of detail in instruction about appro-priate follow up may vary across the trainee’sprofession and the setting. The fundamentaltraining principle is that providers must follow thepatient to resolution or refer her to another healthcare professional, depending on the complexity ofthe problem. Within established standards of care,algorithms that are appropriate to the examiner’shealth care system/institution can direct specificactions.
Sponsoring Institutions Should DevelopStrategies to Increase the Number ofQualified Trainers
As the demand for CBE training grows, wemust ensure that a sufficient supply of qualifiedtrainers is available. Furthermore, because CBEis a tactile skill and didactic instruction alone isinsufficient, institutions will need to help po-tential instructors become skilled at behavioraland skill-based teaching techniques, includingproviding constructive and motivating feed-back.
Training of Trainers Should Have FourCore Elements
The four core elements of training shouldbe:Y Teaching all components of CBE.Y Encouraging consistent performance of a
standardized exam as necessary for provid-ing a quality CBE.
Y Providing the necessary information for in-terpreting CBE findings.
Y Teaching new skills and improving exist-ing skills.
5. Public EducationPromote and encourage public educationabout CBE so that women:a. Know what to expect in the perfor-
mance of CBE and follow-up care.b. Understand the benefits, limitations,
and potential harms associated withCBE.
c. Become familiar with their own breastcharacteristics as well as health practicesthat might increase the likelihood ofidentifying breast abnormalities.
Lead responsibility for implementation: healthcare organizations.Many women are not aware that many
health organizations recommend CBE in ad-dition to regular mammograms, and most donot know what to expect in a CBE. Beinginformed and educated will help women be-come active partners with their provider intheir own health care decisions. Professionalorganizations play a valuable role in influenc-ing their members to follow current guide-lines as a component of comprehensive breastcancer screening. Public education messagesabout CBE should be part of a wider effort topromote informed health care decision-making among women. Messages should besimple, clear, and tailored to different groups ofwomen, if possible. CBE is an opportunity fordialogue between women and their providers andshould parallel education about the importance ofwomen understanding their own normal breastcharacteristics.
Public education efforts should convey thefollowing messages:
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 341

Y Why CBE can be important.X It contributes to the detection of palpa-
ble breast cancers and other breast ab-normalities.
X It offers a test for detecting palpablebreast cancers at an earlier stage of pro-gression; it adds to, but does not replace,mammography.
X However, its contribution to the detec-tion of breast cancer among asymptom-atic women is relatively small. Not allorganizations recommend CBE.
Y What should be expected in a proficientCBE.X Components include careful visual in-
spection and palpation of the breast andlymph nodes.
X It provides a trained examination and anopportunity for patient/provider interac-tion about breast health.
Y What should happen if an abnormality isidentified.X Follow up should be conducted to an
appropriate resolution.X Follow up is required for an abnormal
CBE regardless of the results from themammogram.
Y What a woman can do to improve thequality of her CBE.X Provide a complete history.X Adhere to a schedule of appointments.
Y When screening CBE should be per-formed.X Premenopausal women.
� These women should be screened aspart of a periodic health examinationaccording to screening guidelines.
� If possible, screening should be a weekor two after a woman’s period toavoid breast tenderness and shortly be-fore her mammogram.
X Postmenopausal women.� These women should be screened
as part of a periodic health examina-tion according to screening guide-lines.
� If possible, screening should be shortlybefore a woman’s mammogram.
X Pregnant and breastfeeding women.
� These women should be screened aspart of a periodic health examinationaccording to screening guidelines.
� These women might expect increasedbreast tenderness and nodularity.
6. Research and Quality ImprovementSupport and encourage research in key as-pects of CBE, particularly questions re-lated to characteristics of abnormalitiesfound by CBE, the timing of the exam,training of examiners (clinicians), reportingsystems, and CBE’s contributions to earlydetection of breast cancer and the reduc-tion of morbidity and mortality from thedisease.Lead responsibility for implementation: healthcare organizations and research sponsoringorganizations.The evidence regarding many aspects of CBE
is insufficient. Standardized performance, report-ing, and follow up, combined with reporting andsurveillance systems, could provide the founda-tion for assessing the relative contributions ofCBE to the earlier detection of breast cancer.Such information may enable more accurate es-timates of sensitivity and specificity of CBE inclinical practice settings. Information about thenumber of cancers first identified by CBE, par-ticularly as a function of age and other populationcharacteristics, could help clarify the role of thisexamination as a component of early detectionand the most effective use of CBE relative toother screening modalities. Such data might alsobe used to assess the costs and benefits of CBE asan early detection test. This type of information isessential to resolving the confusion engenderedby having disparate practice guidelines across or-ganizations. Furthermore, such data could pro-vide the basis for further enhancements intraining providers to be proficient in CBE.
Research Needs:Y CBE characteristics.
X Sensitivity and specificity.� In clinical practice.� Among women at different ages (pre-
menopausal, perimenopausal, postmeno-pausal).
X Method of initial detection of abnormal-ities.
CBE Recommendations
342 CA A Cancer Journal for Clinicians

� CBE, mammography, BSE.� By woman, partner, provider.
X Characteristics of masses identified.� Size, shape, consistency, mobility, ex-
ternal texture.X Timing.
� Effect of examination performance atdifferent times of the menstrual cycleon sensitivity and specificity.
� Effect of dissociating CBE from otherscreening modalities for breast cancer.
Y CBE training.X Components of optimal training.X Optimal frequency.X Systems for integrating CBE training
with other medical/health care training.X Characteristics of effective trainers.X Measurement of training effectiveness.
Y CBE reporting systems.X Acceptability of using a uniform or stan-
dardized lexicon for reporting.X Feasibility of expanding medical records
or registry databases to include informa-tion about detection of breast abnormali-ties by CBE.
Y Contribution to the earlier detection ofbreast cancer and reductions in breastcancer mortality.
CONCLUSION
CBE can contribute to the ability of healthcare professionals and women to detect somebreast cancers and should lead to appropriatefollow-up care. The committee recognizes
that these recommendations are a first step inan incremental process of change and thatmany organizations and groups should beinvolved in defining and conducting such aprocess. Rather than develop a set of detailedalgorithms and recommended procedures,the members chose to articulate a smallergroup of general recommendations that em-body several key themes and principles. Inaddition to appearing in this publication,these recommendations and accompanyingtext have been distributed to a wide range ofstakeholders and interested parties to serve asa catalyst for further discussion and action.These recommendations provide a strongfoundation for informing clinical practice,professional training, public education, andresearch efforts.
ACKNOWLEDGEMENTS
The authors express their appreciation toAnne Rodgers, under contract to Manage-ment Solutions for Health, Inc, for technicalwriting prior to and during the CBE com-mittee meeting and to Connie Lim, Ameri-can Cancer Society, for administrativeassistance. Support for this project was pro-vided by the American Cancer Society andthe Centers for Disease Control and Preven-tion. Management Solutions for Health, Inc.provided facilitation and report developmentservices under contract to the AmericanCancer Society.
REFERENCES
1. Barton MB, Harris R, Fletcher SW. Does thispatient have breast cancer? The screening clinicalbreast examination: Should it be done? How?JAMA 1999;282:1270–1280.
2. McDonald S, Saslow D, Alciati MH. Perfor-mance and reporting of clinical breast examina-tion: A review of the literature. CA Cancer J Clin2004;54:345–361.
3. Bobo JK, Lee NC, Thames SF. Findingsfrom 752,081 clinical breast examinations re-ported to a national screening program from1995 through 1998. J Natl Cancer Inst 2000;92:971–976.
4. Oestreicher N, White E, Lehman CD, et al.Predictors of sensitivity of clinical breast examina-
tion (CBE). Breast Cancer Res Treat 2002;76: 73–81.
5. Newcomer LM, Newcomb PA, Trentham-Dietz A, et al. Detection method and breast car-cinoma histology. Cancer 2002;95:470–477.
6. Bancej C, Decker K, Chiarelli A, etal. Contribution of clinical breast examination tomammography screening in the early detection ofbreast cancer. J Med Screen 2003;10:16–21.
7. Smith RA, Saslow D, Sawyer KA, et al.American Cancer Society guidelines for breastcancer screening: Update 2003. CA Cancer J Clin2003;53:141–169.
8. Baines CJ. Physical examination of the breastsin screening for breast cancer. J Gerontol1992;47:63–67.
9. Baines CJ. Screening for breast cancer: howuseful are clinical breast examinations. J NatlCancer Inst 2000;92:958–959.
10. The Susan G. Komen Breast Cancer Foun-dation. Early Detection and Screening: ClinicalBreast Exam. Available at: www.komen.org/intradoc-cgi/idc_cgi_isapi.dll?IdcService�SS_GET_PAGE&ssDocName�EDS3-3-2. AccessedSeptember 7, 2004.
11. American College of Obstetricians and Gy-necologists. Primary and preventive care: periodicassessments. ACOG, 2000.
12. Feig SA, D’Orsi SJ, Hendrick RE, et al.American College of Radiology guidelines forbreast cancer screening. Am J Roentgenol1998;171:29–33.
CA Cancer J Clin 2004;54:327–344
Volume 54 Y Number 6 Y November/December 2004 343

13. American Medical Association. AMA Poli-cies on Breast Cancer. Available at: www.ama-assn.org/ama/pub/category/9060.html. AccessedSeptember 7, 2004.
14. Morrison BJ. Screening for Breast Cancer, inCanadian Task Force on the Periodic Health Ex-amination. Canadian Guide to Clinical Preven-tive Health Care. Ottawa: Health Canada;1994:788–795.
15. US Preventive Services Task Force. Screen-ing for breast cancer: recommendations and ra-tionale. Available at www.guideline.gov/compare/comparison.aspx?file�BRSCREEN8.inc#table2recommendations. Accessed Septem-ber 23, 2004.
16. Agency for Healthcare Research and Qual-ity. Screening for breast cancer. File Inventory,Systematic Evidence Review Number 15. Availableat: www.ahrq.gov/clinic/prev/brscrinv.htm. Ac-cessed September 7, 2004.
17. Humphrey LL, Helfand M, Chan BKS,Woolf SH. Breast cancer screening: A summaryof the evidence for the US Preventive ServicesTask Force. Ann Intern Med 2002;137:347–360.
18. Ferrini R, Mannino E, Ramsdell E, Hill L.Screening mammography for breast cancer: Amer-ican College of Preventive Medicine Practice PolicyStatement. Available at: www.acpm.org/breast.htm. Accessed September 7, 2004.
19. American College of Physicians. ACP ClinicalPractice Guidelines. Available at: www.acponline.org/sci-policy/guidelines/past.htm. Accessed Sep-tember 7, 2004.
20. American Association of Family Practitioners.Recommendations for Periodic Health Examina-tions—Breast Cancer. Available at: www.aafp.org/x24976.xml. Accessed September 7, 2004.
21. Breen N, Kessler L. Trends in cancer screen-ing - United States, 1987 and 1992. Oncology1996;10:328–330.
22. Centers for Disease Control and Prevention.2000 BRFSS summary prevalence report. Availableat: www.cdc.gov/brfss/pdf/2000prvrpt.pdf. Ac-cessed September 7, 2004.
23. Centers for Disease Control and Prevention.The National Breast and Cervical Cancer Early
Detection Program—reducing mortality throughscreening. Available at: www.cdc.gov/cancer/nbccedp/about.htm#facts. Accessed September 7,2004.
24. Lane DS, Messina CR. Current perspectiveson physician barriers to breast cancer screening.J Am Board Fam Pract 1999;12:8–15.
25. Stange KC, Flocke SA, Goodwin MA, et al.Direct observation of rates of preventive servicedelivery in community family practice. Prev Med2000;31:167–176.
26. Desnick L, Taplin S, Taylor V, et al. Clinicalbreast examination in primary care: perceptionsand predictors among three specialties. J WomensHealth 1999;8:389–397.
27. Frank E, Rimer BK, Brogan DJ, Elon L. USwomen physicians’ personal and clinical breastcancer screening practices. J Women HealthGend Based Med 2000;9:791–801.
28. Fletcher SW, O’Malley MS, Pilgrim CA,Gonzalez JJ. How do women compare with in-ternal medicine residents in breast lump detec-tion? J Gen Int Med 1989;4:277–283.
29. Chalabian J, Garman K, Wallace P, Dunning-ton G. Clinical breast evaluation skills of houseofficers and students. Am Surg 1996;62:840–845.
30. Pennypacker HS, Naylor L, Sander AA, Gold-stein MK. Why can’t we do better breast examina-tions? Nurse Pract Forum 1999;10:122–128.
31. Chalabian J, Dunnington G. Do our currentassessments assure competency in clinical breastevaluation skills? Am J Surg 1998;175:497–502.
32. Hall DC, Adams CK, Stein GH, et al. Im-proved detection of human breast lesions followingexperimental training. Cancer 1980;46:408–414.
33. Sloan DA, Donnelly MB, Schwartz RW, et al.Assessing medical students’ and surgery residents’clinical competence in problem solving in surgicaloncology. Ann Surg Oncol 1994;1:204–212.
34. Wiecha JM, Gann P. Provider confidencein breast examination. Fam Pract Res J 1993;13: 37–41.
35. Lane DS, Burg MA. Promoting physician pre-ventive practices: needs assessment for CME inbreast cancer detection. J Cont Ed 1989;9:245–256.
36. Warner SL, Worden JK, Solomon LJ, Wad-land WC. Physician interest in breast cancerscreening: a survey of Vermont family physicians.J Fam Pract 1989;29:281–285.
37. Physician Insurers Association of America.Breast cancer study - 2002. Physician InsurersAssociation of America, 2002.
38. Coleman EA, Heard JK. Clinical breastexamination: an illustrated educational reviewand update. Clin Excell Nurse Pract 2001;5:197–204.
39. Henderson MA, Cawson JM, Bilous M.Breast cancer: getting the diagnosis right. Med JAustralia 1995;163:494–499.
40. Saunders KJ, Pilgrim CA, Pennypacker HS.Increased proficiency of search in breast self-examination. Cancer 1986;58:2531–2537.
41. Dixon J, Ma B, Nigel J. Management ofDisorders of the Ductal System and Infections,in Harris JR (ed). Diseases of the Breast.Philadelphia: Lippincott Williams & Wilkins;2000:47–55.
42. Haagensen CD. Physician’s Role in theDetection and Diagnosis of Breast Cancer, inHaagensen CD (ed). Diseases of the Breast.3rd ed. Philadelphia: W.B. Saunders Co.;1986:636.
43. Berg WA, D’Orsi CJ, Jackson VP, et al. Doestraining in breast imaging reporting and data sys-tem (BI-RADS) improve biopsy recommenda-tions or feature analysis agreement withexperienced breast imagers and mammography?Radiology 2002;224:871–880.
44. Taplin SH, Ichikawa LE, Kerlikowske K, etal. Concordance of breast imaging reporting anddata system assessments and management recom-mendations in screening mammography. Radiol-ogy 2002;222:529–535.
45. Lehman CD, Holt S, Peacock S, et al. Use ofthe American College of Radiology BI-RADSguidelines by community radiologists: concor-dance of assessments and recommendations as-signed to screening mammograms. Am JRoentgenol 2002;179:15–20.
CBE Recommendations
344 CA A Cancer Journal for Clinicians
![InvestigationofClinicalCharacteristicsandEtiologicalFactor ... · enamelbreakdownandwidespreadcariesthatdetermine bothfunctionalandestheticcomplications)(Figures1–4) [6].Earlydetection,intervention,andappropriatetherapy](https://img.pdfslide.net/doc/110x75/61454f4b34130627ed50e527/investigationofclinicalcharacteristicsandetiologicalfactor-enamelbreakdownandwidespreadcariesthatdetermine.jpg)