Embed Size (px)
Citation preview

Clinical characteristics of patients that experiencedifferent rates of exodrift after strabismus surgeryfor intermittent exotropia and the effect of the rateof exodrift on final ocular alignmentKa Hee Park, MD, and So Young Kim, MD
PURPOSE To evaluate the ocular motility factors associated with the rate of exodrift after surgical cor-
Author affiliations: DepartmentUniversity, Cheonan, KoreaThis work was supported in paSubmitted April 27, 2012.Revision accepted October 11,Correspondence: So Young Kim
330-930, Korea (email: ophdrkiCopyright � 2013 by the Am
Strabismus.1091-8531/$36.00http://dx.doi.org/10.1016/j.ja
54
rection of intermittent exotropia and to determine whether the rate had an effect on thesubsequent postoperative ocular alignment.
METHODS Consecutive patients who underwent surgical correction of intermittent exotropia
between 2009 and 2010 were observed for 12 months. Patients were divided intotwo groups, according to the averaged value of the rate of exodrift (fast vs slow).The ocular motility characteristics of the patients in each group were compared withidentify factors that correlated with the speed of postoperative exodrift and to deter-mine whether the rate had an effect on the final ocular alignment at 12 months aftersurgery.RESULTS A total of 159 patients underwent strabismus surgery during the study period. Of these, 130
experienced postoperative drift. The preoperative deviation at near and distance differedsignificantly between the fast and slow groups (P\ 0.05) and was correlated to the rateof exodrift (near r 5 0.427, distance r 5 0.378): fast group, 32.09D � 10.07D,27.60D � 6.65D; slow group, 31.74D �10.34D, 27.21D � 6.03D. The deviation at the firstday after the surgery differed significantly between groups (P\ 0.05) and was correlatedto the rate of drift (r 5 0.381): fast group, 4.72D � 5.46D esotropia; slow group,1.87D� 4.40D esotropia. The two groups did not differ significantly in other factors. Therewere no differences in ocular alignment at 12 months’ follow-up.CONCLUSIONS The rate of exodrift correlated with the size of the preoperative deviation and the amount of
the initial postoperative overcorrection. It had no affect on the ocular alignment at 12months after surgery. ( J AAPOS 2013;17:54-58)Intermittent exotropia is themost prevalent formof exo-tropia, probably resulting from a combination of inner-vational imbalance that upsets the reciprocal
relationship between active convergence and divergencemechanisms, mechanical factors, anatomical deformities,and hereditary factors.1,2 Patients with intermittentexotropia who are treated surgically tend to experiencepostoperative exodrift over time, and many authors havesuggested that an initial overcorrection is necessary toachieve satisfactory ocular alignment. However, it isdifficult to achieve a precise amount of overcorrectionwithout adjustable sutures. Currently there is no consensusas to the ideal amount of overcorrection.
of Ophthalmology, College of Medicine, Soonchunhyang
rt by the Soonchunhyang University Research Fund
2012., MD, 23-20 Bongmeong-dong Dongnam-gu, Cheonan,
[email protected]).erican Association for Pediatric Ophthalmology and
apos.2012.10.014
An awareness of postoperative drift patterns is impor-tant for establishing goals for the postoperative alignment.However, in most studies authors have addressed the de-sirable amounts of initial overcorrection to improve thelong-term ocular alignment after surgery, with no reporton the rate of postoperative exodrift in the intermittentexotropia. The purpose of this study was to evaluate thefactors associated with the rate of postoperative exodriftand to evaluate the relationship between the rate of exo-drift and subsequent postoperative ocular alignment in pa-tients who underwent surgical correction of intermittentexotropia.
Subjects and Methods
The medical records of consecutive patients who underwent sur-
gery for intermittent exotropia at Soonchunhyang University
Medical Center between 2009 and 2010 and who had follow-up
of at least 12 months were retrospectively reviewed. The rates
of exodrift were analyzed in patients who showed an exodrift at
12 months after surgery compared with deviation at 1 week after
surgery. The following patients were excluded: patients with high
Journal of AAPOS

Table 1. Demographics and operative characteristics of thesubjects with postoperative exotropic drift
Characteristic Subjects (N 5 130)
Age at surgery, years (range) 6.49 � 3.05 (2-19)SexMale, n (%) 66 (50.77)Female, n (%) 64 (49.23)
Type of surgeryBilateral lateral rectusmuscle recession, n (%)
104 (80.00)
Unilateral lateral rectusrecession and medial rectusmuscle resection, n (%)
26 (20.00)
Preoperative deviation, PDDistance 28.82 � 7.91 XTNear 28.97 � 8.25 XT
Postoperative deviation at distance, PD1 day 2.82 � 4.94 ET1 week 1.38 � 5.51 ET3 weeks 2.74 � 5.28 XT6 weeks 3.85 � 5.28 XT3 months 4.53 � 5.83 XT6 months 5.08 � 6.17 XT12 months 5.96 � 6.58 XT
ET, esotropia; PD, prism diopter; XT, exotropia.
Table 2. The rate of exodrift from postoperative 1 week to 12months in patients with exotropic drift
DurationRate of exodrift,
PD/month
Pearsoncorrelationcoefficient ra P valuea
1 week-3 weeks 8.25 � 9.74 0.712 0.0003 weeks-6 weeks 1.48 � 3.18 0.441 0.0006 weeks-3 months 0.46 � 1.25 0.399 0.0003 months-6 months 0.18 � 0.44 0.271 0.0026 months-12 months 0.15 � 0.30 0.318 0.0001 week-12 months 0.61 � 0.52
PD, prism diopters.aP\ 0.05 was considered to be significant.
Volume 17 Number 1 / February 2013 Park and Kim 55
ratio of accommodative convergence to accommodation (assessed
by the gradient method with 13.0 D lens at near); patients with
lateral incomitance of more than 10D; patients who received com-
bined recession and vertical transposition for an A- or a V-pattern
deviation without inferior oblique overaction; and patients who
underwent intraoperative or postoperative adjustable suture
technique.
The following information was taken at the preoperative exam-
ination: age of onset, past treatment, and family history of strabis-
mus. Visual acuity was measured through the full cycloplegic
refractive error after instillation of 1% cyclopentolate, 0.5% tro-
picamide, 0.5% phenylephrine eye drops. Dilated fundus exami-
nation was performed, and all patients were tested for near
(33 cm) and distance (5 m) fixation by alternative prism and cover
testing. Over- and underaction of the oblique muscle were
checked by duction and version tests. Sensory status was evaluated
for the cooperative patients using the Worth 4-dot test, and ster-
eoacuity was measured with the Titmus and Lang tests. Fusion
status was categorized into good, fair, or poor. Good control
was defined as a deviation that was broken only during the cover
test; fair control, as a deviation that was controlled by using a blink
or change in fixation after disruption with cover testing; and poor
control, as a deviation that was broken spontaneously without any
disruption of fusion.
Surgery was performed under general anesthesia by the same
surgeon (SYK), who chose the surgical technique on the basis of
experience. The primary surgical techniques included bilateral
lateral rectus recession, unilateral medial rectus resection, and
lateral rectus recession. Surgical dosages were applied using stan-
dard tables.
Alternative prism and cover testing was performed at postoper-
ative day 1; weeks 1, 3, and 6; and months 3, 6, and 12. We mea-
sured the rate of exodrift at each postoperative visit by dividing
prism diopter changes from the last visit with interval between
postoperative visit (prism diopter/month). The average monthly
drift rate for the entire study period was calculated as the change
in deviation from 1 week to 12 months after surgery divided by
12 months. The correlation between drift rate for each postoper-
ative visit and the total average drift rate was analyzed, and the
postoperative visit at which the exodrift rate most closely corre-
lated with the overall average drift was identified. This informa-
tion allowed classification of patients into two exodrift groups:
fast, with a rate greater than that for the best-correlated visit;
and slow, with a rate less than that for the best-correlated visit.
Ocular alignment of the groups was assessed at 12 months’
follow-up. Motor success was defined as alignment from 10D exo-
deviation to 5D esodeviation at distance. Recurrence was defined
as .10D of exodeviation, and overcorrection was defined as .5D
of esodeviation. Reoperation was performed if exotropia exceeded
20D at distance after primary surgery.
Statistical analysis was performed using SPSS for Windows
version 14.0 (SPSS Inc, Chicago, IL). Pearson correlation anal-
ysis was used to investigate the rate of exodrift between each
postoperative visit and total period. The t test and c2 test
were used to compare factors related to exodrift and ocular
alignment between two groups. P\ 0.05 was considered statis-
tically significant.
Journal of AAPOS
Results
Of the 159 patients with intermittent exotropia, 130(81.76%) exhibited postoperative exodrift at 12 months’follow-up and were included in this study. Of the 130patients (mean age, 6.49 � 3.05 years; 66 males), 104underwent a bilateral lateral rectus recession, 26 under-went a unilateral lateral rectus recession and medial rec-tus resection, and 4 patients had combined operation,with bilateral lateral rectus recession and oblique mus-cle–weakening procedure. Mean deviation at distancewas 28.82D � 7.91D exotropia preoperatively and5.96D � 6.58D exotropia 12 months postoperatively(Table 1).
The monthly rate of postoperative exodrift was 8.25D
� 9.74D at 1-3 weeks, 1.48D � 3.18D at 3-6 weeks, 0.46 D
� 1.25D at 6 weeks-3 months, 0.18D � 0.44D at 3-6months, and 0.15D � 0.30D at 6-12 months. The overall12-month drift rate of total period was 0.61D � 0.54D

Table 3. Dermographics, preoprerative data, and operative data of patients with exotropic drift
Trait
Group
P valueFast (n 5 43) Slow (n 5 87)
Mean alignment velocity, PD/month 17.90 � 1.71 3.47 � 0.35 0.027a
Past history, n (%) 2 (4.65) 4 (4.60) 0.649b
Family history, n (%) 1 (2.33) 2 (2.30) 0.704b
Mean age of onset, years 5.77 � 3.48 6.97 � 5.98 0.227c
Mean age at surgery, years 6.09 � 3.52 7.25 � 5.88 0.236c
Sex, n 0.950b
Male 22 44Female 21 43
Refractive error (SE)Right eye �0.07 � 3.00 �0.14 � 1.70 0.895c
Left eye �0.04 � 3.00 �0.16 � 1.61 0.817c
Amblyopia, n (%) 5 (11.63) 2 (2.30) 0.039a
Type of surgery 0.512Bilateral LR recess 33 71LR recess and MR resect 10 16
Preoperative deviationDistance,PD 32.09 � 10.01 XT 27.21 � 6.04 XT 0.015a
Near, PD 31.74 � 10.34 XT 27.60 � 6.65 XT 0.007a
Deviation at POD 1,PD 4.72 � 5.46 ET 1.87 � 4.40 ET 0.023a
Fusion good:fair:poor, n 2:7:34 6:17:64 0.188b
Cyclotorsion, n (%) 1 (2.33) 3 (3.45) 0.342b
Stereopsis, arcsec 132.65 � 135.72 122.53 � 171.07 0.762c
Arcsec, arcsecond; ET, esotropia; LR, lateral rectus muscle; MR, medial rectus muscle; PD, prism diopters; POD, postoperative day; SE, sphericalequivalent; XT, exotropia.aP\ 0.05 considered significant.bc2 test.ct test.
56 Park and Kim Volume 17 Number 1 / February 2013
and was significantly correlated with drift rates of allpostoperative visits (P\ 0.05). The drift rate of postop-erative 1-3 weeks (8.25D/month) showed the strongestcorrelation with the overall drift rate (Pearson correla-tion coefficient r 5 0.712, P \ 0.05), and based onthis, patients were divided into slow and fast groups(Table 2).
In the fast group, there were 43 patients with themonthly rate of exodrift 17.90D� 1.71D; in the slow group,87 patients with the rate of exodrift 3.47D � 0.35D. Meanage of onset was 5.77 � 3.48 years in the fast group and6.97 � 5.98 years in the slow group. Mean age at surgerywas 6.09 � 3.52 years in the fast group and 7.25 � 5.88years in the slow group. The fast group comprised 22malesand 21 females; the slow group, 44 males and 43 females.No statistically significant differences were noted betweenthe 2 groups with respect to mean age of onset (P5 0.227),mean age at surgery (P 5 0.236), type of surgery(P5 0.512), and sex (P5 0.950). No statistically significantdifferences were noted with respect to past treatment his-tory of strabismus (P5 0.649) and family history of strabis-mus (P 5 0.704) between the 2 groups. For sphericalequivalents of both eyes (P 5 0.895/0.817), fusion status(P5 0.188), presence of cyclotorsion (P5 0.342), and ster-eoacuity (P 5 0.762), there was no statistically differencebetween the two groups. The fast group did include signif-icantly more amblyopic patients than the slow group (5 vs2; P 5 0.039).
The preoperative deviation measured at distance dif-fered significantly between groups (32.09D �10.07D exo-tropia [fast group] vs 27.21D � 6.04D exotropia [slowgroup]; P 5 0.015), as did the deviation measured at near(P 5 0.007). The deviation at postoperative 1 day also dif-fered significantly (4.72D � 5.46D esotropia [fast group] vs1.87D � 4.40D esotropia [slow group]; P5 0.023; Table 3).
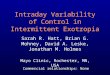
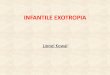
The preoperative deviation and the postoperative 1 daydeviation were correlated to the rate of exodrift (Pearsoncorrelation r 5 0.427/0.378, and 0.381, respectively;Figure 1). There were no statistically significant differencein ocular alignment at 12 months (P 5 0.130). In the fastgroup, 31 patients (72.09%) showed motor success, pa-tients were overcorrected, and 12 patients (27.91%) had re-currence. In the slow group, 73 patients (84.88%) showedmotor success, 1 patient (1.16%) was overcorrected, and12 patients (13.95%) had recurrence (Figure 2). Concern-ing long-term results, 2 patients (4.65%) in the fast groupand 4 patients (4.60%) in the slow group underwent reop-eration, and the period between the primary operation andthe reoperation was 15.50 months in the fast group and26.25 months in the slow group (Table 4).
Discussion
Previous investigators have reported postoperative successrates for intermittent exotropia from 50% to 79%.3 Factorssuch as magnitude of preoperative deviation, distance–near
Journal of AAPOS

FIG 1. Correlation of preoperative deviation (A), deviation at postop-erative day 1 (B) and the rate of exotropic drift. PD, prism diopters.
FIG 2. Ocular alignment of the fast and slow exodrift groups assessedat 12 months after surgery (P 5 0.130). PD, prism diopters.
Table 4. Distribution of ocular alignment at 12 months aftersurgery
Alignment
Group, number (%)
Fast (n 5 43) Slow (n 5 87)
Overcorrectiona 0 (0) 1 (1.16)Successb 31 (72.09) 73 (84.88)Recurrencec 12 (27.91) 12 (13.95)
aAlignment excess 5D for exotropia.bAlignment within 10D of exotropia and within 5D of esotropia andorthotropia.cAlignment excess 10D for exotropia (c2 test, P 5 0.130).
Volume 17 Number 1 / February 2013 Park and Kim 57
disparity, age at surgery, refractive error, and type of sur-gery have been reported as predictive of outcome.4-8
Postoperative exodrift is largely responsible for the lowsuccess rates but has not previously been evaluated ina large study. There is widespread agreement that in thesurgical management of intermittent exotropia, an initialovercorrection is required because of the tendencytoward postoperative exodrift.9-12 However, a few studieshave reported that an initial overcorrection ismeaningless.13 Ruttum14 reported a tendency towardmore postoperative exodrift with larger initial overcorrec-tion and less exodrift with smaller overcorrection and withundercorrection.
Journal of AAPOS
In the present study, preoperative deviation and initialpostoperative overcorrection were the most importantfactors relating to the rate of postoperative exodrift. Pa-tients with larger preoperative deviations or with largerinitial postoperative overcorrection had more posopera-tive exodrift, whereas those with less preoperative devi-ations or less initial postoperative overcorrection hadless.
The presence of amblyopia was significant in determin-ing the rate of exodrift after surgery. Amblyopic patientsseemed to tend toward exodrift faster. Jampolsky and col-leagues15 emphasized that anisomyopia and anisoastigma-tism bear distinct relationships to exodeviation, andunequal clarity retinal images may present an obstacle tofusion that may facilitate suppression and contribute tothe pathogenesis of exotropia. Accordingly, amblyopiawas considered as a factor affecting the exodrift; however,there were too few amblyopic subjects in the present studyto draw firm conclusions.
The present study had several limitations, including thesmall number of subjects, which did not permit us to cate-gorize patients by type, and a relatively short follow-up pe-riod which precludes determining the long-term stabilityof the surgical correction. Nevertheless, we were able todemonstrate the association of larger preoperative devia-tion and initial overcorrection with the rate of

58 Park and Kim Volume 17 Number 1 / February 2013
postoperative exodrift after surgery for intermittent exo-tropia and that the rate of exodrift had no influence onthe postoperative ocular alignment at 12 months aftersurgery.
References
1. Bielschowsky A. Divergence excess. Arch Ophthalmol 1934;12:157-66.
2. Matsuo T, Hayashi M, Fujiwara H, Yamane T, Ohtsuki H. Concor-dance of strabismic phenotypes in monozygotic versus multizygotictwins and other multiple births. Jpn J Ophthalmol 2002;46:59-64.
3. Ekdawi NS, Nusz KJ, Diehl NN, Mohney BG. Postoperative out-comes in children with intermittent exotropia from a population-based cohort. J APPOS 2009;13:4-7.
4. Scott AB, Mash AJ, Jampolsky A. Quantitative guidelines for exotro-pia. Invest Ophthalmol 1975;14:428-36.
5. Richard JM, Parks MM. Intermittent exotropia: Surgical results indifferent age groups. Ophthalmology 1983;90:1172-7.
6. Stoller SH, Simon JW, Lininger LL. Bilateral lateral rectus recessionfor exotropia: A survival analysis. J AAPOS 1994;31:89-92.
7. Gezer A, Sezen F,NasriN,GozumN. Factors influencing the outcomeof strabismus surgery in patient with exotropia. J AAPOS 2004;8:57-60.
8. Chia A, Seenyen L, Long QB. Surgical experience with two-musclesurgery for the treatment of intermittent exotropia. JAAPOS 2006;10:206-11.
9. Oh JY, Hwang JM. Survival analysis of 365 patients with exotropia af-ter surgery. Eye 2006;20:1268-72.
10. ScottWE, Keech R,Mash J. The postoperative results and stability ofexodeviation. Arch Ophthalmol 1981;99:1814-8.
11. Knapp P. Transactions of the NewOrleans Academy of Ophthalmol-ogy. Symposium on Strabismus. St Louis: C.V. Mosby; 1971:233–41.
12. Kim TW, Kim JH, Hwang JM. Long-term outcome of patients withlarge overcorrection following surgery for exotropia. Ophthalmolog-ica 2005;219:237-42.
13. Choi J, Kim SJ, Yu YS. Initial postoperative deviation as a predictor oflong-term outcome after surgery for intermittent exotropia. J AAPOS2011;15:224-9.
14. RuttumMS. Initial versus subsequent postoperative motor alignmentin intermittent exotropia. J AAPOS 1997;1:88-91.
15. Jampolsky A, Flom BC, Weymouth FS, Moster LE. Unequal cor-rected visual acuity as related to anisometropia. Arch Ophthalmol1955;54:893-905.
Journal of AAPOS