Embed Size (px)
DESCRIPTION
Clinical, clinicopathologic, and radiographic findings in dogs with aspiration pneumonia_88 cases
Citation preview

1742 ScientificReports JAVMA,Vol233,No.11,December1,2008
SM
ALL
AN
IMA
LS
Aspiration pneumonia is a serious and potentially life-threatening inflammatory lung process. Patho-
logic damage to the lungs results from insults to the al-veolar capillary membranes, and loss of surface area for gas exchange leads to ventilation-perfusion mismatch and hypoxemia. Gastric acid aspiration directly causes alterations in surfactant function that result in loss of surface tension and atelectasis.1 Subsequent broncho-constriction increases airway resistance and the effort required for breathing. Acid injury adversely impacts pulmonary resistance to infection,2 and the presence of oral or gastrointestinal bacteria in aspirated fluid can result in development of severe bacterial pneumonia.3
Although aspiration pneumonia is encountered commonly in humans and other animals, definitive di-agnosis of the disorder is challenging. In people, aspira-tion events are categorized as aspiration pneumonitis or aspiration pneumonia depending on whether injury
Clinical, clinicopathologic, and radiographic findings in dogs with aspiration pneumonia:
88 cases (2004–2006)
David A. Kogan, bs; Lynelle R. Johnson, dvm, phd, dacvim; Karl E. Jandrey, dvm, dacvecc; Rachel E. Pollard, dvm, phd, dacvr
Objective—Toevaluateclinical,clinicopathologic,andradiographicfindingsindogswithas-pirationpneumonia.Design—Retrospectivecaseseries.Animals—88dogswithaspirationpneumonia.Procedures—History,physicalexaminationfindings,andclinicopathologicdatawereob-tainedfrommedicalrecordsandanalyzedforall88dogs.Thoracicradiographicfindingsforalldogswerereviewedtodeterminethetypeandlocationofpulmonaryinfiltrates.Results—Aspirationpneumoniawasevidentatadmissiontothehospitalin65(74%)dogsanddevelopedduringhospitalization in23 (26%)dogs.Less thanhalfof theseaffecteddogshadhighvaluesforrectaltemperature,heartrate,orrespiratoryrate;however,most(68%)affecteddogshadincreased,decreased,oradventitiouslungsounds.Neutrophiliawithaleftshiftwasacommonfinding.Hypoalbuminemiawasdetectedin31of58(53%)dogs.Hypoxemiaandahighalveolar-arterialgradientinpartialpressureofoxygenwerede-tectedin22of28(79%)dogsand27of28(96%)dogs,respectively.Amongthe88dogs,thoracicradiographyrevealedapredominantlyalveolar infiltrate in65(74%)dogsandaninterstitialpatternin23(26%)dogs;asinglelunglobewasaffectedin46(52%)dogs,mostcommonlytherightmiddlelunglobe(21/46[46%]dogs).Conclusions and Clinical Relevance—Indogs,aspirationpneumoniawasoftenassoci-ated with abnormalities in pulmonary auscultation in the absence of objective changesinphysicalexaminationfindings.However,neutrophilia,hypoalbuminemia,andhypoxemiawerefrequentlydetected,andradiographicevidenceofinfiltratesintherightmiddlelunglobewascommon.(J Am Vet Med Assoc2008;233:1742–1747)
is related to aspiration of sterile gastric contents that results in acid-induced damage or related to pulmonary inflammation that develops in response to infectious organisms contained within the aspirant.4,5 Definitive diagnosis of aspiration pneumonia is difficult to obtain because of the lack of specific identifying features.5–9 In humans, aspiration pneumonia is a clinical diagnosis based on the presence of respiratory tract signs and radiographic evidence of a newly developed pulmonary infiltrate in a patient at risk. Similar criteria appear to be applied in veterinary medicine, although identifica-tion of respiratory tract signs, risk factors, and newly developed lung infiltrates in a patient is often problem-atic. Various underlying disorders associated with as-piration have been identified in humans and other ani-mals, including dysphagia, laryngeal disease, decreased consciousness, and neurologic disease.5,7,10–13
Although aspiration pneumonia appears to devel-op quite commonly in dogs, little information is avail-able on specific features of the disease, hematologic changes, or the specific radiographic changes seen in dogs with naturally occurring disease. The purpose of
From the Veterinary Medical Teaching Hospital (Kogan), and the Departments of Veterinary Medicine and Epidemiology (Johnson) and Surgical and Radiological Sciences (Jandrey, Pollard), School of Veterinary Medicine, University of California, Davis, CA 95616. Dr. Kogan’s present address is Veterinary Medical and Surgical Group, 2199 Sperry Ave, Ventura, CA 93003.
Supported in part by the S.T.A.R. (Students Training in Advanced Re-search) program, School of Veterinary Medicine, University of Cali-fornia, Davis, and the Bailey Wrigley Fund.
Address correspondence to Dr. Johnson.
Abbreviations
Fio2 Fractionofinspiredoxygen
Pao2-Pao
2 Alveolar-to-arterialgradientinpartialpressureofoxygen

JAVMA,Vol233,No.11,December1,2008 ScientificReports 1743
SM
ALL A
NIM
ALS
the study reported here was to evaluate clinical, clini-copathologic, and radiographic findings in dogs with aspiration pneumonia. In addition, specific features in dogs that had aspiration pneumonia at the time of ad-mission to the hospital (ie, unknown duration) and in dogs that developed aspiration pneumonia during hos-pitalization were compared to elucidate discriminatory findings in dogs during the acute stages of the disorder (ie, signs within 12 hours of aspiration).
Materials and Methods
Case selection—The electronic medical database at the Veterinary Medical Teaching Hospital of the Uni-versity of California, Davis, was searched for the terms aspiration pneumonia and canine in records dated Jan-uary 1, 2004, to January 1, 2006, to identify all dogs with this clinical diagnosis. This time frame was chosen to generate a sufficient number of cases for evaluation from the period prior to transition from conventional film screen radiography to digital radiography. This was specifically done to eliminate the confounding variabil-ity caused by differing imaging techniques. Dogs were included in the study if aspiration pneumonia was listed in the medical record under the record field for the final clinical diagnoses. Dogs were included whether the di-agnosis was made at the time of admission to the hospi-tal or during hospitalization. Dogs were excluded from the study if radiographic images illustrating pulmonary infiltrates were not available for review. Records of dogs with forms of pneumonia other than aspiration pneu-monia were not evaluated.
Medical records review—Medical records were ex-amined by one of the authors (LRJ) to verify the clini-cal diagnosis of aspiration pneumonia by use of criteria (variably documented in individual records) as follows: witnessed or suspected regurgitation or vomiting epi-sodes followed by acute onset of respiratory difficulty, cough, or tachypnea; physical examination findings consistent with lower respiratory tract disease or radio-graphic detection of pulmonary infiltrates in a dog at risk for aspiration; and identification of systemic disorders or interventions potentially associated with aspiration, in-cluding anesthesia, esophageal dysfunction, laryngeal disease, gastrointestinal tract disease, and decreased con-sciousness in dogs with clinical or radiographic evidence of pneumonia. Medical records and radiographic reports were also scrutinized for comments that reflected clinical suspicion of an aspiration event and clinical or clinico-pathologic evidence of hypoxemia. Cases were excluded if supportive information for an aspiration event was not found or if an alternate cause for lower respiratory tract signs or radiographic changes supported diagnoses such as primary infectious pneumonia, pulmonary emboliza-tion, or neoplasia.
Information on age, breed, weight, and reproduc-tive status was abstracted from the records. These data were compared with data from the total hospital popula-tion of dogs during the study period. Reasons for initial evaluation at the hospital, physical examination findings (including rectal temperature, pulse rate, respiratory rate and effort, presence of cough, and detection of adventi-tious lung sounds), results of clinicopathologic testing
(ie, results of a CBC, serum biochemical and arterial blood gas analyses, and urinalysis), and radiographic findings were also obtained. Physical examination find-ings and clinical data obtained soon after the aspiration event were collated, although it was not possible to de-termine specifically the number of hours between the aspiration event and diagnostic testing. Complete blood cell count results were evaluated for responses compat-ible with pneumonia, including abnormally high or low Hct values or WBC counts, detection of a neutrophil band response, and presence of nucleated RBCs. Arterial blood gas data (room air conditions) were evaluated for evidence of hypoxemia via assessment of Pao
2 and calcu-
lation of the Pao2 - Pao
2 by use of a formula as follows:
Pao2 - Pao
2 = Fio
2 (PB – PH
2O) – (Paco
2•R−1) – Pao
2
where Pao2 is the partial pressure of oxygen, alveolar,
Fio2 is 0.21 in room air, PB is the barometric pressure (in
mm Hg), PH2O is the water vapor pressure (47 mm Hg at 37oC), and R is the respiratory quotient (0.9).
A value of Pao2 - Pao
2 > 15 mm Hg was considered
indicative of lung dysfunction.14 In dogs receiving supple-mental oxygen, the oxygenation ratio (fraction of Pao
2 to
Fio2) was estimated as the measured Pao
2 (mm Hg) di-
vided by Fio2.
The value used for Fio2 (range, 0.3 to 0.6) was es-timated from the oxygen flow rate used when admin-istering mask oxygen or from the value displayed on the oxygen cage in which 4 of the dogs were placed; Fio2 was considered 100% in 5 dogs that were intubated and ventilated. Direct measurement of tracheal oxygen concentration was not performed in any dog. An oxy-genation ratio > 400 was considered normal.15
Thoracic radiographs (2-, 3-, and 4-view sets) for each dog were reviewed by a board-certified radiologist (REP), who was unaware of the clinical course of disease. Radiographic views were assessed for the primary type of infiltrate (designated as interstitial, alveolar [includ-ing lobar consolidation], or bronchial); a mixed pattern was categorized on the basis of the predominant type of infiltrate detected. Location of the primary infiltrate was defined by the lobar branching pattern of the airways in dogs as described by Amis and McKiernan.16 The left cra-nial lung lobe in dogs is comprised of cranial and caudal segments; for the purposes of this study, each segment was considered independently. Therefore, the location of infiltrates was described as left cranial-cranial segment, left cranial-caudal segment, or left caudal, right cranial, right middle, accessory, or right caudal lobe. The number of affected lobar segments was identified for each dog.
For comparison of selected clinical variables, dogs were allocated to 1 of 2 groups. Group 1 dogs were those that had aspiration pneumonia at the time of ad-mission to the hospital. Group 2 dogs were those that developed aspiration pneumonia during hospitaliza-tion. Causes and clinical outcome among these dogs are reported elsewhere.17
Statistical analysis—Data are presented as mean ± SD, and ranges are provided where appropriate; characteristics are reported for all dogs. Hematologic and serum biochemi-cal values in groups 1 and 2 were compared by use of an unpaired t test. A Fisher exact test was used to detect dif-

1744 ScientificReports JAVMA,Vol233,No.11,December1,2008
SM
ALL
AN
IMA
LS
ferences between groups on the basis of the frequency of abnormal findings. Signalment characteristics for dogs with aspiration pneumonia were compared with those of dogs in the general hospital population by use of χ2 analysis. Statistical analyses were performed by use of commercial software,a and significance was set at a value of P < 0.05.
Results
Search of the electronic medical database yielded medical records of 105 dogs for which aspiration pneu-monia was listed as a final clinical diagnosis. Two cases were excluded because review of the medical records failed to identify supportive clinical evidence for aspira-tion pneumonia, and 15 cases were excluded because of the lack of radiographs for review. Medical records for the remaining 88 dogs were comprehensively reviewed.
Among the 88 dogs, there were 20 mixed-breed dogs and 68 purebred dogs. Sixteen (18%) dogs were consid-ered small-breed dogs (< 10 kg [22 lb]), 18 (21%) dogs were medium-sized breeds (10 to 20 kg [22 to 44 lb]), and 54 (61%) dogs were large-breed dogs (> 20 kg [44 lb]). This breed distribution contrasted somewhat with that of the general hospital population of 8,053 dogs, of which 27% were small-breed dogs, 17% were medium-sized breeds, and 56% were large-breed dogs. However, the sizes of affected study dogs did not differ significantly from sizes of dogs in the hospital population. Breeds that were represented more than twice among the study dogs included Golden Retriever (n = 10), Labrador Retriever (9), and English Springer Spaniel, German Shepherd Dog, Rottweiler, Pug, and Cocker Spaniel (3 of each breed). The percentages of Labrador Retrievers, German Shepherd Dogs, and Rottweilers with aspiration pneumonia (13.2%, 4.4%, and 4.4%, respectively) were similar to the percent-ages of those breeds in the hospital population (14.2%, 4.5%, and 3.5%, respectively). However, compared with the breed percentages in the hospital population, there were more Golden Retrievers (15% vs 6%), Cocker Span-iels (4.4% vs 2.5%), English Springer Spaniels (4.4% vs 0.6%), and Pugs (4.4% vs 1.6%) with aspiration pneumo-nia. Mean ± SD weight of dogs with aspiration pneumonia was 26.7 ± 17.2 kg (58.7 ± 37.8 lb; range, 2.6 to 91 kg [5.72 to 200.2 lb]). There were slightly more male (50/88 [57%])
than female (38/88 [43%]) dogs. Among the male dogs, 6 were sexually intact and 44 were castrated; among the fe-male dogs, 5 were sexually intact and 33 were spayed. The age of the dogs ranged from 4 months to 16 years (mean age, 8.4 ± 4.3 years). Eight (9%) dogs were < 1 year old, and 45 (51%) were > 8 years old. In comparison, 11% of dogs were < 1 year old and 41% were > 8 years old in the general hospital population of dogs.
Among the dogs with aspiration pneumonia, 34 of 80 (42%) had a high respiratory rate (ie, > 30 breaths/min), 26 of 83 (31%) had high rectal temperature (ie, > 39.2°C [102.5°F]), and 10 of 82 (12%) had a high heart rate (ie, > 160 beats/min). Most dogs (65/88 [74%]) had evidence of aspiration pneumonia at the time of admission to the hos-pital (group 1); the others (23/88 [26%]) developed aspira-tion pneumonia during hospitalization (group 2). General physical examination characteristics (including rectal tem-perature, pulse rate, and respiration rate) did not differ (P > 0.05) between dogs in groups 1 and 2. Compared with dogs in group 1, proportionally more dogs in group 2 had a high rectal temperature (10/20 [50%] dogs vs 16/63 [25%] dogs), although this difference was not significant (P = 0.053).
In the records of group 1, cough was reported for 37 of 65 (57%) dogs and increased respiratory effort was reported for 36 of 65 (55%) dogs. Lung sounds were considered normal or clear in 21 (32%) dogs and harsh or loud in 20 (31%) dogs. In the 65 dogs, adventitious lung sounds (crackles or wheezes) were detected in 16 (25%), whereas lung sounds were quieter than expected in 8 (12%). Fifteen of 65 (23%) dogs had a combina-tion of cough, increased respiratory effort, and abnormal lung sounds. Eight (12%) dogs had no clinical evidence of respiratory tract disease. Lung sounds were described for 15 of the 23 dogs in group 2 and were considered normal or clear in 5 of those dogs. For the remaining 10 of the 15 dogs, louder than expected or adventitious lung sounds were reported. Among 80 dogs with aspira-tion pneumonia for which lung sounds were described, abnormal lung sounds were reported for 55 (69%).
Hematologic values were available for 77 of 88 dogs; data from 1 dog with immune-mediated hemolytic ane-mia were excluded from analysis. Dogs in group 2 had significantly (P = 0.033) lower Hct than dogs in group 1 (mean values, 36.5 ± 2.0% vs 40.8 ± 7%; Table 1).
Group 1 Group 2
No. of dogs No. of dogs No. of dogs No. of dogs Reference with a with a with a with a Variable range Mean SD high value low value Mean SD high value low value
Hct (%) 40–55 40.8 7 2 21 35.7 9.5 0 10*Reticulocytes† (cells/µL) 7–65,000 39,781 55,361 1 NA 43,650 41,798 3 NANucleated RBCs (cells/µL) 0 1 1 6 NA 7 6 3 NAWBCs (cells/µL) 6–13,000 14,960 6,300 35 4 19,460 12,809 14‡ 3 Neutrophils (cells/µL) 3–10,500 11,910 5,724 30 0 15,390 10,437 13 2Band neutrophils (bands/µL) 100 2,050 1,768 30 NA 1,757 1,546 14 NALymphocytes (cells/µL) 1–4,000 1,385 1,001 2 25 1,316 981 1 12Monocytes (cells/µL) 0.15–1,200 991 627 16 0 1,402 1,902 9 2Eosinophils (cells/µL) 0–1,500 348 273 0 NA 228 174 0 NABasophils (cells/µL) 0–50 39 25 6 NA 28 18 0 NA
*Number of dogs in this category was significantly (P = 0.033) different from that of group 1. †For this variable, data were available from 11 dogs in group 1 and 10 dogs in group 2. ‡Number of dogs in this category was significantly (P = 0.047) different from that of group 1.
NA = Not applicable.
Table1—Valuesofhematologicvariablesin76of88dogswithaspirationpneumonia.Dogswereallocatedto1of2groupsonthebasisofwhethertheyhadaspirationpneumoniaatthetimeofadmissiontothehospital(group1;n=56)ordevelopedaspirationpneumoniaduringhospitalization(group2;20).Meanvaluesofeachvariabledidnotdiffer(P0.05)betweengroups.
JAVMA,Vol233,No.11,December1,2008 ScientificReports 1745
SM
ALL A
NIM
ALS
The mean WBC count in group 2 dogs was significantly (P = 0.047) higher than that in group 1 dogs (19,763 ± 12,809 cells/µL vs 14,962 ± 6,300 cells/µL).
Serum biochemical analyses were performed in 58 of 77 dogs. High liver enzyme activity was detected in 35 of those 58 dogs. Serum alkaline phosphatase activ-ity ranged from 16 to 6,182 U/L (mean, 590 ± 1,242 U/L) and was high (reference range, 15 to 127 U/L) in 35 of 58 (60%) dogs. Serum alanine transaminase activity ranged from 9 to 531 U/L (mean, 132 ± 345 U/L) and was high (reference range, 19 to 67 U/L) in 21 (36%) dogs. Serum albumin concentration ranged from 1.1 to 3.6 g/dL (mean, 2.8 ± 0.6 g/dL) and was low (reference range, 2.9 to 4.2 g/dL) in 31 (53%) dogs. There were no significant differences in serum liver enzyme activities or albumin concentration between groups 1 and 2.
Results of arterial blood gas analyses obtained in room air (Fio
2, 0.21) within 48 hours of the aspiration
event were available for 28 dogs. Among these dogs, mean Pao
2 was 68.5 ± 14.6 mm Hg (range, 39.2 to 93.7 mm
Hg). Hypoxemia (Pao2 < 80 mm Hg) was detected in 22
of 28 (79%) dogs (range, 39.2 to 77.7 mm Hg). Partial pressure of carbon dioxide ranged from 20.8 to 52.5 mm Hg (reference range, 35 to 45 mm Hg); hypercapnia was detected in 2 (7%) dogs, and hypocapnia was detected in 14 (50%) dogs. Mean Pao
2 - Pao
2 was 43.5 ± 17.0 mm Hg
(range, 12.8 to 82.8 mm Hg), and the Pao2 - Pao
2 value
was within the reference range (< 15 mm Hg) in only 1 dog. In 9 dogs, arterial blood gas analysis was repeated during administration of supplemental oxygen (ranging from 30% to 100%); the oxygenation ratio ranged from 93 to 532 mm Hg (mean, 277 mm Hg; median, 225 mm Hg), and values in 6 of 9 dogs were < 200 mm Hg.
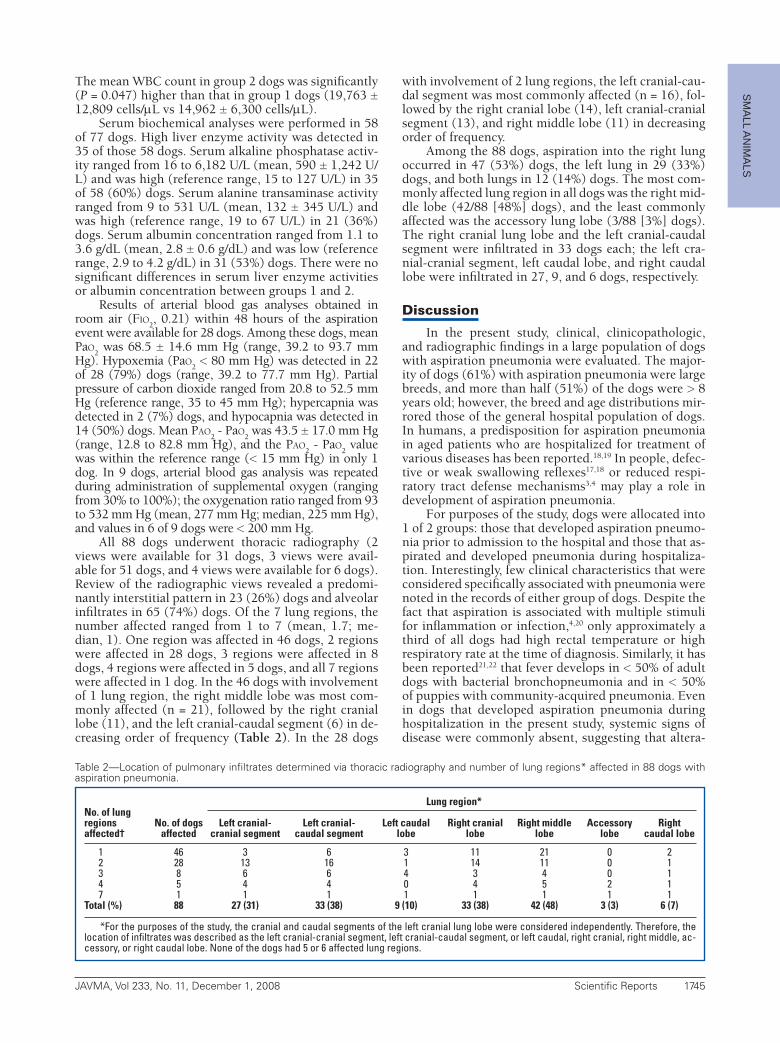
All 88 dogs underwent thoracic radiography (2 views were available for 31 dogs, 3 views were avail-able for 51 dogs, and 4 views were available for 6 dogs). Review of the radiographic views revealed a predomi-nantly interstitial pattern in 23 (26%) dogs and alveolar infiltrates in 65 (74%) dogs. Of the 7 lung regions, the number affected ranged from 1 to 7 (mean, 1.7; me-dian, 1). One region was affected in 46 dogs, 2 regions were affected in 28 dogs, 3 regions were affected in 8 dogs, 4 regions were affected in 5 dogs, and all 7 regions were affected in 1 dog. In the 46 dogs with involvement of 1 lung region, the right middle lobe was most com-monly affected (n = 21), followed by the right cranial lobe (11), and the left cranial-caudal segment (6) in de-creasing order of frequency (Table 2). In the 28 dogs
with involvement of 2 lung regions, the left cranial-cau-dal segment was most commonly affected (n = 16), fol-lowed by the right cranial lobe (14), left cranial-cranial segment (13), and right middle lobe (11) in decreasing order of frequency.
Among the 88 dogs, aspiration into the right lung occurred in 47 (53%) dogs, the left lung in 29 (33%) dogs, and both lungs in 12 (14%) dogs. The most com-monly affected lung region in all dogs was the right mid-dle lobe (42/88 [48%] dogs), and the least commonly affected was the accessory lung lobe (3/88 [3%] dogs). The right cranial lung lobe and the left cranial-caudal segment were infiltrated in 33 dogs each; the left cra-nial-cranial segment, left caudal lobe, and right caudal lobe were infiltrated in 27, 9, and 6 dogs, respectively.
Discussion
In the present study, clinical, clinicopathologic, and radiographic findings in a large population of dogs with aspiration pneumonia were evaluated. The major-ity of dogs (61%) with aspiration pneumonia were large breeds, and more than half (51%) of the dogs were > 8 years old; however, the breed and age distributions mir-rored those of the general hospital population of dogs. In humans, a predisposition for aspiration pneumonia in aged patients who are hospitalized for treatment of various diseases has been reported.18,19 In people, defec-tive or weak swallowing reflexes17,18 or reduced respi-ratory tract defense mechanisms3,4 may play a role in development of aspiration pneumonia.
For purposes of the study, dogs were allocated into 1 of 2 groups: those that developed aspiration pneumo-nia prior to admission to the hospital and those that as-pirated and developed pneumonia during hospitaliza-tion. Interestingly, few clinical characteristics that were considered specifically associated with pneumonia were noted in the records of either group of dogs. Despite the fact that aspiration is associated with multiple stimuli for inflammation or infection,4,20 only approximately a third of all dogs had high rectal temperature or high respiratory rate at the time of diagnosis. Similarly, it has been reported21,22 that fever develops in < 50% of adult dogs with bacterial bronchopneumonia and in < 50% of puppies with community-acquired pneumonia. Even in dogs that developed aspiration pneumonia during hospitalization in the present study, systemic signs of disease were commonly absent, suggesting that altera-
Lung region*No. of lung regions No. of dogs Left cranial- Left cranial- Left caudal Right cranial Right middle Accessory Rightaffected† affected cranial segment caudal segment lobe lobe lobe lobe caudal lobe
1 46 3 6 3 11 21 0 2 2 28 13 16 1 14 11 0 1 3 8 6 6 4 3 4 0 1 4 5 4 4 0 4 5 2 1 7 1 1 1 1 1 1 1 1Total (%) 88 27 (31) 33 (38) 9 (10) 33 (38) 42 (48) 3 (3) 6 (7)
*For the purposes of the study, the cranial and caudal segments of the left cranial lung lobe were considered independently. Therefore, the location of infiltrates was described as the left cranial-cranial segment, left cranial-caudal segment, or left caudal, right cranial, right middle, ac-cessory, or right caudal lobe. None of the dogs had 5 or 6 affected lung regions.
Table2—Locationofpulmonaryinfiltratesdeterminedviathoracicradiographyandnumberoflungregions*affectedin88dogswithaspirationpneumonia.

1746 ScientificReports JAVMA,Vol233,No.11,December1,2008
SM
ALL
AN
IMA
LS
tions in rectal temperature, pulse rate, and respiratory rate are not always reliable indicators of respiratory tract dysfunction.
Importantly, cough and respiratory difficulty were noted historically or detected during physical exami-nation in over half of the affected dogs in the present study. Abnormal lung sounds were reported in most dogs (68%), indicating the importance of a thorough physical examination (particularly thoracic auscultation) in local-ization of diseases of the lower respiratory tract. Crackles and louder than expected breath sounds were the most consistent finding in dogs with bacterial bronchopneu-monia also.21 Proficiency in thoracic auscultation is one of the more difficult skills to learn; however, it was clear-ly of importance in leading to the clinical diagnosis of pneumonia in dogs of the present study. However, spe-cific adventitious lung sounds were reported less often than harsh or loud lung sounds, which suggests physical signs of pathologic changes in the lungs of dogs with as-piration pneumonia may be subtle.
In the group of dogs included in the present study, neutrophilia with a left shift was common as one would expect in animals with inflammation or infection asso-ciated with pneumonia. Dogs that developed aspiration pneumonia during hospitalization had lower Hct val-ues, higher WBC counts, and higher (albeit not signifi-cantly) neutrophil counts than dogs that had aspiration pneumonia at the time of admission. The lower Hct in the former group may have resulted from IV administra-tion of fluids to hospitalized patients. The significantly higher WBC count in dogs that developed aspiration pneumonia during hospitalization could be evidence of a more acute inflammatory response. Among all of the affected dogs, hypoalbuminemia was detected in slightly more than half of the dogs for which data were available, although serum globulin concentration was not high. This could be suggestive of lung inflamma-tion and vasculitis that resulted in leakage of albumin into the alveolar space. Conversely, it may have been associated with concurrent systemic disease. High liver enzyme activities were also common, and a limitation of the study is that it did not evaluate the effect of co-morbid conditions on clinicopathologic variables.
Hypoxemia was detected in 79% of 28 dogs for which arterial blood gas data were available. Such dec-rements in Pao
2 values are indicative of variable dys-
function in pulmonary gas exchange. It is possible that hypoxemia was common among the dogs in the present study because this test is perhaps more typically per-formed in dogs that appear to be more severely affected. Interestingly, 50% of the 28 dogs were hypocapnic. Low Paco
2 values in dogs with pulmonary thromboembo-
lism have also been reported23; in that study, hypocap-nia was thought to represent altered control of ventila-tion. In dogs with aspiration injury, low values of Paco2 could be attributable to a similar mechanism or could result from compensatory hyperventilation induced by hypoxemia associated with ventilation-perfusion mismatch. In the present study, only 2 of the evalu-ated dogs were hypercapnic, indicating that alveolar hypoventilation was not a common problem. In stud-ies23–25 of pulmonary thromboembolism in dogs and humans, high Pao
2 - Pao
2 was more common than was
hypoxemia, suggesting that calculation of this variable results in improved detection of abnormalities in gas exchange. Calculation of the Pao
2 - Pao
2 is also useful
because it can be used to follow response to treatment, although this was not performed in the study of this report. Arterial blood gas analyses in dogs treated with supplemental oxygen revealed poor oxygen responsive-ness, thereby confirming that aspiration pneumonia can cause severe lung damage.
Among the dogs of the present study, the most common thoracic radiographic pattern was an alveo-lar infiltrate (detected in 65/88 [74%] dogs). Slightly more than 50% of dogs had involvement of a single lung region, most commonly the right middle lobe. In-volvement of this lung lobe in an aspiration event is most likely a consequence of the ventral orientation of the bronchus to this lobe from the right mainstem bronchus.16 Mucus pooling from ventral dependence might also increase the likelihood that this lung lobe will be affected. Overall, aspiration into the right lung occurred more commonly than aspiration into the left lung in dogs of the present study. In an investigation26 of dogs with experimentally induced lung aspiration, the right lung was involved more commonly than the left lung when dogs were maintained in dorsoventral or ventrodorsal positioning. The straighter angle of the right principal bronchus at the carina (compared with the angle of the left principal bronchus) was considered likely to contribute to this phenomenon. This is partic-ularly important to consider when performing thoracic radiography on a dog that is suspected of having aspi-ration pneumonia. The left lateral radiographic view is not routinely acquired but yields the best depiction of the right lung. Therefore, 3 radiographic views of the thorax should be obtained in dogs suspected of hav-ing aspiration pneumonia, particularly because if the infiltrates are distributed ventrally, the left lateral view may be the only one in which right cranial or middle lung lobe infiltrates are seen. Of equal importance is the fact that 26% of dogs in the present study had a pre-dominantly interstitial pattern of infiltrates identified radiographically. Aspiration pneumonia traditionally has been described as resulting in ventrally distributed alveolar infiltrates; however, that radiographic appear-ance was not evident in a subset of dogs in our study. Given the retrospective nature of the study, it was not possible to determine whether this lack of ventrally dis-tributed alveolar infiltrates in some dogs was related to the timing of thoracic radiography in relationship to the aspiration event; however, it is of clinical importance that identification of an interstitial pattern in thoracic radiographic views could be consistent with aspiration pneumonia.
In dogs that had involvement of 2 lung regions, the left and right cranial lung lobes and right middle lung lobes were most commonly affected. Radiographic pat-tern recognition is considered highly important in the diagnosis and characterization of pneumonia in hu-mans; aspiration pneumonia is characterized by multi-centric opacities in the lower rather than upper lobes.8 In dogs, a similar distribution of lesions should raise the suspicion for pneumonia. Nevertheless, the presence of infiltrates in atypical lung regions should not rule out

JAVMA,Vol233,No.11,December1,2008 ScientificReports 1747
SM
ALL A
NIM
ALS
consideration of aspiration pneumonia because 20% of dogs in the present study had involvement of the caudal and accessory lung lobes. Positioning during an aspira-tion event plays a role in the location of radiographically detectable infiltrates5; in a study26 in which contrast me-dium was infused into the trachea of anesthetized dogs, dogs placed in ventrodorsal recumbency were more like-ly to aspirate into the right caudal lung lobe.
Some limitations of the present study should be men-tioned. Diagnosis of aspiration pneumonia was based on clinical information obtained through retrospective analy-sis of medical record data. Various clinicians were involved in planning the diagnostic assessments, and various tests were performed for individual cases. Definitive diagnosis of aspiration pneumonia is challenging. In people with aspiration pneumonia, a high proportion of lipid-laden macrophages is found in bronchoalveolar lavage fluid,27 although this finding has relatively low specificity for dis-crimination of aspiration pneumonia from other chronic pulmonary conditions.6 Also, dogs have a high propor-tion of lipid-laden macrophages, compared with other species, and experimental induction of gastroesophageal reflux did not increase this index value.28,29 Detection of pepsin in bronchoalveolar lavage fluid can be used to di-agnose aspiration injury in children with gastroesophageal reflux.30 Unfortunately, collection of airway samples was rarely performed in the dogs of the present study, thereby precluding assessment of lipid-laden macrophages or pep-sin concentration. Thus, it was not possible to differenti-ate aspiration pneumonia from pneumonitis or to describe either the pulmonary inflammatory responses or the bac-teria involved in the aspiration injury. Prospective studies would be useful in providing additional information on the relative roles of acid injury and bacteria-induced dam-age in dogs with aspiration pneumonia.
a. GraphPad Prism, version 5.0, GraphPad Software Inc, San Diego, Calif.
References1. Schmidt R, Markart P, Ruppert C, et al. Time-dependent chang-
es in pulmonary surfactant function and composition in acute respiratory distress syndrome due to pneumonia or aspiration. Respir Res [serial online]. 2007;8:55. Available at: respiratory-research.com/content/pdf/rr86.pdf. Accessed Nov 1, 2007.
2. Mitsushima H, Oishi K, Nagao T, et al. Acid aspiration induces bacterial pneumonia by enhanced bacterial adherence in mice. Microb Pathog 2002;33:203–210.
3. Genné D, Sommer R, Kaiser L, et al. Analysis of factors that con-tribute to treatment failure in patients with community-acquired pneumonia. Eur J Clin Microbiol Infect Dis 2006;25:159–166.
4. van Westerloo DJ, Knapp S, van’t Veer C, et al. Aspiration pneumonitis primes the host for an exaggerated inflammatory response during pneumonia. Crit Care Med 2005;33:1770–1778.
5. Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med 2001;344:665–671.
6. Furuya ME, Moreno-Córdova V, Ramírez-Figueroa JL, et al. Cutoff value of lipid-laden alveolar macrophages for diagnosing aspira-tion in infants and children. Pediatr Pulmonol 2007;42:452–457.
7. Mukhopadhyay S, Katzenstein AL. Pulmonary disease due to
aspiration of food and other particulate matter: a clinicopatho-logic study of 59 cases diagnosed on biopsy or resection speci-mens. Am J Surg Pathol 2007;31:752–759.
8. Sharma S, Maycher B, Eschun G. Radiological imaging in pneumo-nia: recent innovations. Curr Opin Pulm Med 2007;13:159–169.
9. Shigemitsu H, Afshar K. Aspiration pneumonia: under-diagnosed and under-treated. Curr Opin Pulm Med 2007;13:192–198.
10. King LG, Vite CH. Acute fulminating myasthenia gravis in five dogs. J Am Vet Med Assoc 1998;212:830–834.
11. MacPhail CM, Monnet E. Outcome of and postoperative complica-tions in dogs undergoing surgical treatment of laryngeal paralysis: 140 cases (1985–1998). J Am Vet Med Assoc 2001;218:1949–1956.
12. Kane-Gill SL, Olsen KM, Rebuck JA, et al. Multicenter treat-ment and outcome evaluation of aspiration syndromes in criti-cally ill patients. Ann Pharmacother 2007;41:549–555.
13. Poncet CM, Dupre GM, Freiche VG, et al. Long-term results of upper respiratory syndrome surgery and gastrointestinal tract medical treatment in 51 brachycephalic dogs. J Small Anim Pract 2006;47:137–142.
14. King LG, Anderson JG, Rhodes WH, et al. Arterial blood gas ten-sions in healthy aged dogs. Am J Vet Res 1992;53:1744–1748.
15. Bernard GR, Artigas A, Brigham KL, et al. The American-Eu-ropean Consensus Conference on ARDS. Definitions, mecha-nisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994;149:818–824.
16. Amis TC, McKiernan BC. Systematic identification of endobron-chial anatomy during bronchoscopy in the dog. Am J Vet Res 1986;47:2649–2657.
17. Kogan DA, Johnson LR, Sturges BK, et al. Etiology and clinical outcome in dogs with aspiration pneumonia: 88 cases (2004–2006). J Am Vet Med Assoc 2008;233:1748–1755.
18. Reza Shariatzadeh M, Huang JQ, Marrie TJ. Differences in the features of aspiration pneumonia according to site of acquisition: community or continuing care facility. J Am Geriatr Soc 2006;54:296–302.
19. Carratalà J, Mykietiuk A, Fernández-Sabé N, et al. Health care-associated pneumonia requiring hospital admission: epidemiol-ogy, antibiotic therapy, and clinical outcomes. Arch Intern Med 2007;167:1393–1399.
20. Fraisse A, Bregeon F, Delpierre S, et al. Hemodynamics in exper-imental gastric juice induced aspiration pneumonitis. Intensive Care Med 2007;33:300–307.
21. Thayer GW, Robinson SK. Bacterial bronchopneumonia in the dog: a review of 42 cases. J Am Anim Hosp Assoc 1984;20:731–735.
22. Radhakrishnan A, Drobatz KJ, Culp WT, et al. Community-ac-quired infectious pneumonia in puppies: 65 cases (1993–2002). J Am Vet Med Assoc 2007;230:1493–1497.
23. Johnson LR, Lappin MR, Baker DC. Pulmonary thromboembo-lism in 29 dogs (1985–1995). J Vet Intern Med 1999;13:338–345.
24. Cvitanic O, Marino PL. Improved use of arterial blood gas anal-ysis in suspected pulmonary embolism. Chest 1989;95:48–51.
25. Schneider RF, Ntimba FD, Hourizadeh A, et al. Massive pulmo-nary embolism: a comparison of radiological and clinical char-acteristics and outcomes. Emerg Radiol 2002;9:79–81.
26. Eom K, Seong Y, Park H, et al. Radiographic and computed to-mographic evaluation of experimentally induced lung aspira-tion sites in dogs. J Vet Sci 2006;7:397–399.
27. Adams R, Ruffin R, Campbell D. The value of the lipid-laden macrophage index in the assessment of aspiration pneumonia. Aust N Z J Med 1997;27:550–553.
28. Savchenko O, Dhadwal AK, Pagala M, et al. Lipid-laden macrophage index in healthy canines. Eur J Clin Invest 2006;36:419–422.
29. Savchenko O, Vastola P, Pagala M, et al. Lipid laden macrophage indices and reflux finding score in canine gastroesophageal re-flux model. Pediatr Pulmonol 2007;42:1181–1186.
30. Farrell S, McMaster C, Gibson D, et al. Pepsin in bronchoalveolar lavage fluid: a specific and sensitive method of diagnosing gastro-oesophageal reflux-related pulmonary aspiration. J Pediatr Surg 2006;41:289–293.