Embed Size (px)
Citation preview
Clinical Decision Making
for Oral Anticoagulation
Iain Speirits
Pharmacist Clinical Cardiology
Friday 08th September 2017
Overview
• Epidemiology
• ESC
• Mechanisms of Action
• Comparison with VKA
• Treatment Considerations
• Choice of DOAC
• Case Studies
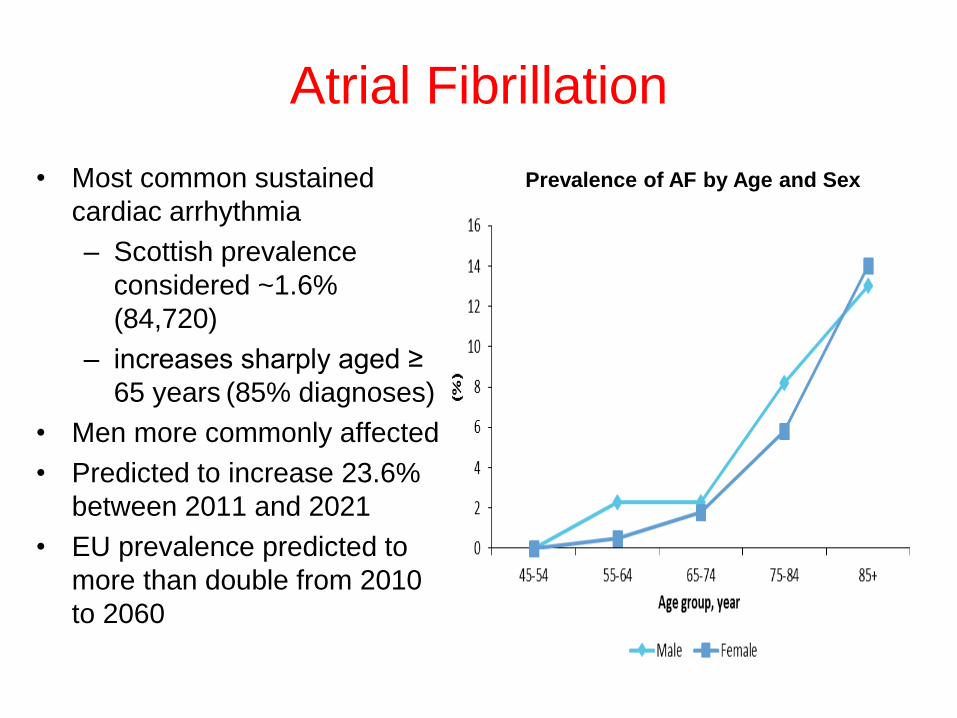
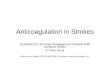
Atrial Fibrillation
• Most common sustained
cardiac arrhythmia
– Scottish prevalence
considered ~1.6%
(84,720)
– increases sharply aged ≥
65 years (85% diagnoses)
• Men more commonly affected
• Predicted to increase 23.6%
between 2011 and 2021
• EU prevalence predicted to
more than double from 2010
to 2060
Prevalence of AF by Age and Sex
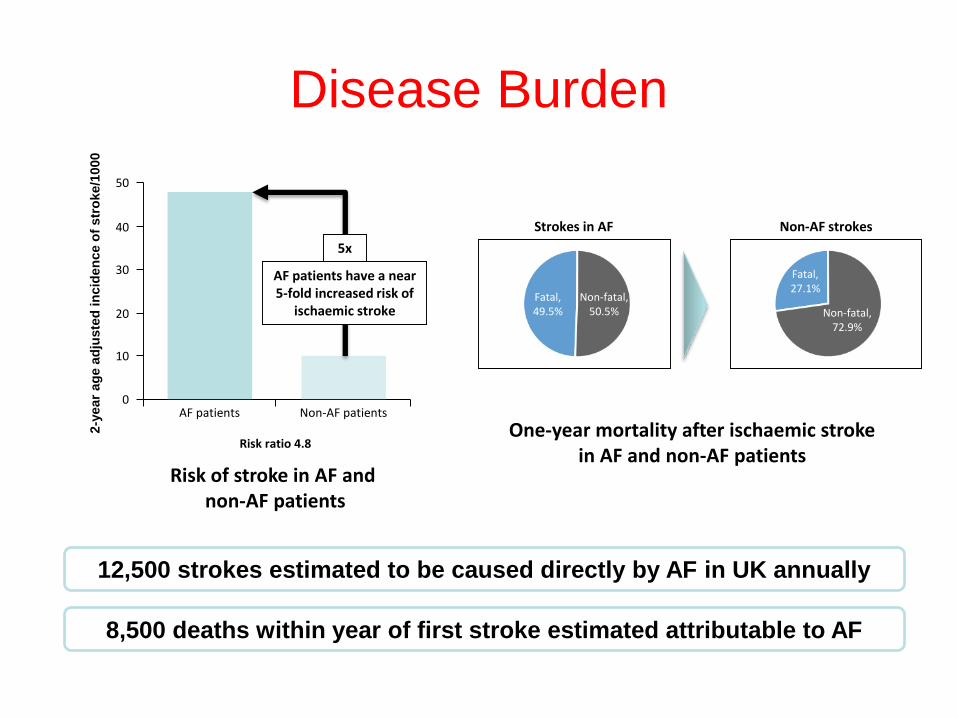
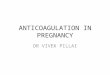
Disease Burden
Risk ratio 4.8
2-y
ear
ag
e a
dju
ste
d in
cid
en
ce o
f str
oke/1
000
Risk of stroke in AF andnon-AF patients
AF patients Non-AF patients
One-year mortality after ischaemic stroke in AF and non-AF patients
12,500 strokes estimated to be caused directly by AF in UK annually
8,500 deaths within year of first stroke estimated attributable to AF
10
0
20
30
40
50
AF patients have a near 5-fold increased risk of
ischaemic stroke
5x
Fatal,49.5%
Non-fatal,50.5%
Fatal,27.1%
Non-fatal,72.9%
Strokes in AF Non-AF strokes
Oral Anticoagulants Underused
• SSNAP (2014) highlights lack of effective
stroke prevention in UK
– 3,790 patients identified as being in AF prior to
admission
– 41.2% of AF patients admitted to hospital with
stroke on OAC prior to admission
– 15.1% of patients not on OAC had justifiable
reason not to be receiving one
– 34% taking only antiplatelet drugs, considered
ineffective for patients in AF
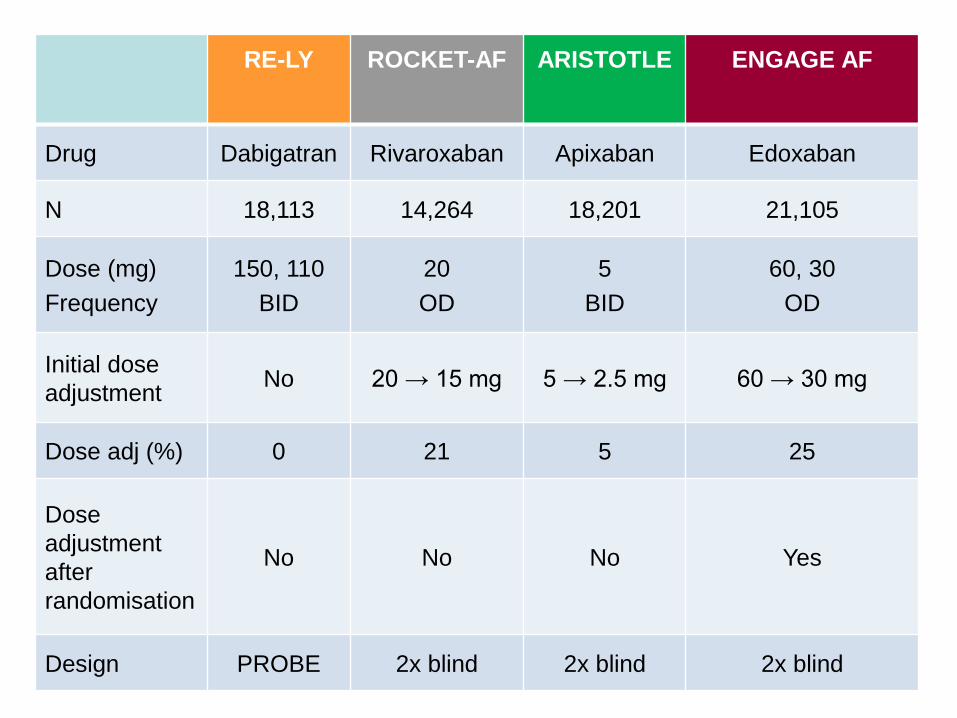
RE-LY ROCKET-AF ARISTOTLE ENGAGE AF
Drug Dabigatran Rivaroxaban Apixaban Edoxaban
N 18,113 14,264 18,201 21,105
Dose (mg)
Frequency
150, 110
BID
20
OD
5
BID
60, 30
OD
Initial dose
adjustmentNo 20 → 15 mg 5 → 2.5 mg 60 → 30 mg
Dose adj (%) 0 21 5 25
Dose
adjustment
after
randomisation
No No No Yes
Design PROBE 2x blind 2x blind 2x blind
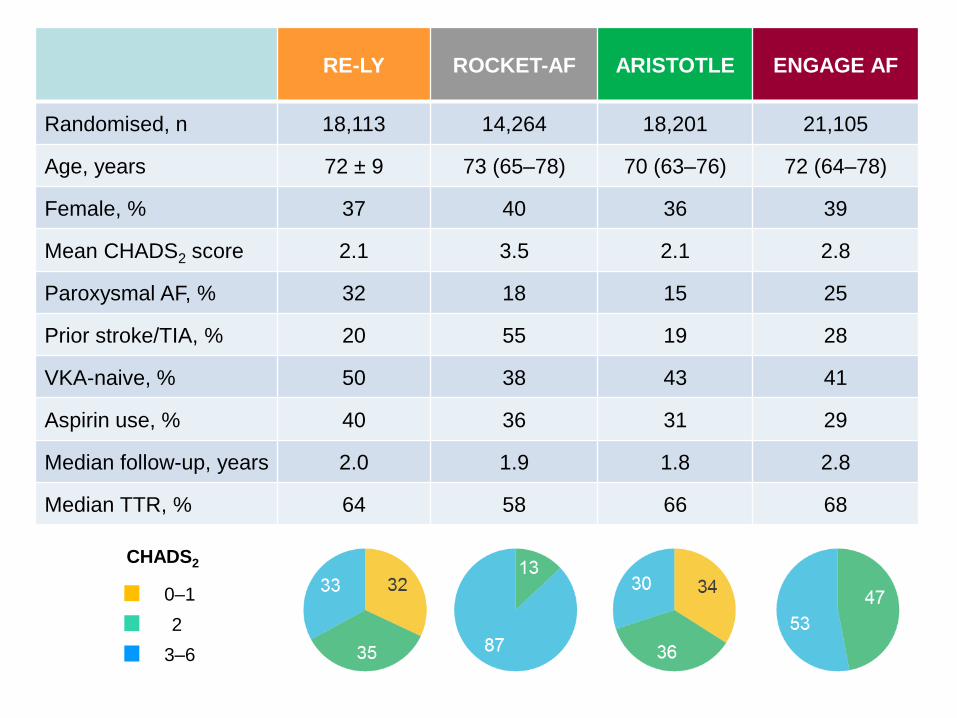
RE-LY ROCKET-AF ARISTOTLE ENGAGE AF
Randomised, n 18,113 14,264 18,201 21,105
Age, years 72 ± 9 73 (65–78) 70 (63–76) 72 (64–78)
Female, % 37 40 36 39
Mean CHADS2 score 2.1 3.5 2.1 2.8
Paroxysmal AF, % 32 18 15 25
Prior stroke/TIA, % 20 55 19 28
VKA-naive, % 50 38 43 41
Aspirin use, % 40 36 31 29
Median follow-up, years 2.0 1.9 1.8 2.8
Median TTR, % 64 58 66 68
CHADS2
2
3–6
0–1
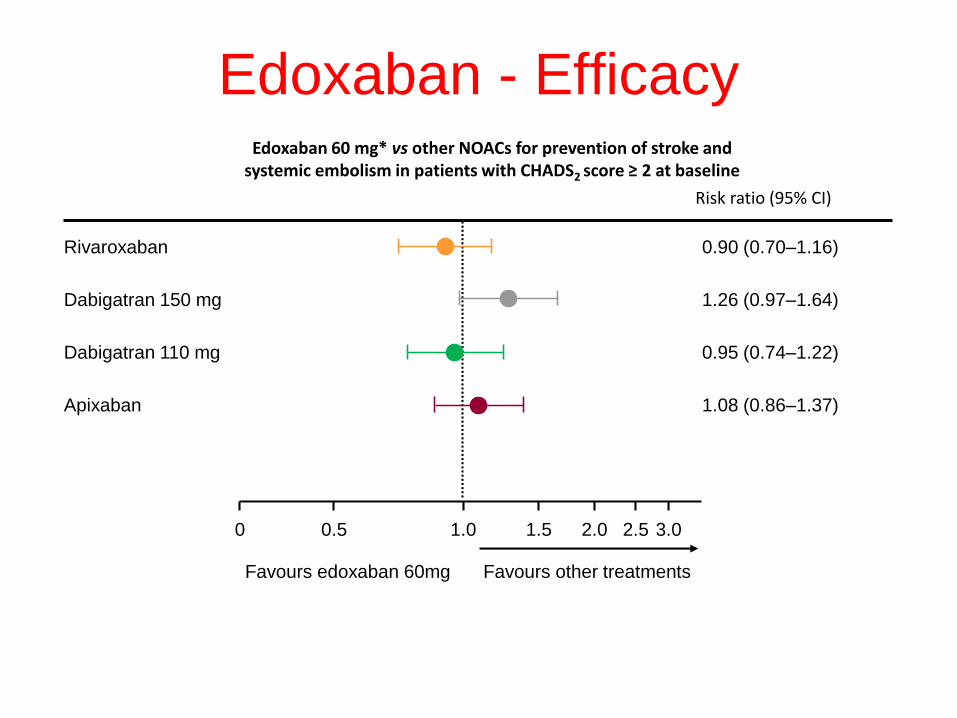
Edoxaban 60 mg* vs other NOACs for prevention of stroke and systemic embolism in patients with CHADS2 score ≥ 2 at baseline
Risk ratio (95% CI)
Rivaroxaban 0.90 (0.70–1.16)
Dabigatran 150 mg 1.26 (0.97–1.64)
Dabigatran 110 mg 0.95 (0.74–1.22)
Apixaban 1.08 (0.86–1.37)
0 1.0 3.00.5 1.5 2.0 2.5
Favours edoxaban 60mg Favours other treatments
Edoxaban - Efficacy
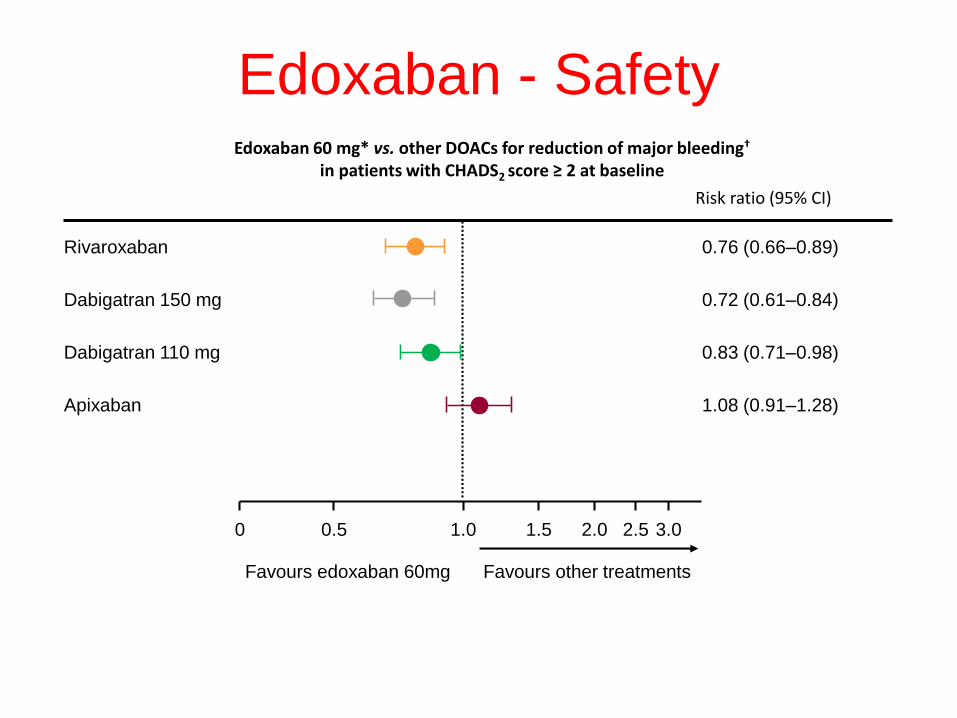
Risk ratio (95% CI)
Rivaroxaban 0.76 (0.66–0.89)
Dabigatran 150 mg 0.72 (0.61–0.84)
Dabigatran 110 mg 0.83 (0.71–0.98)
Apixaban 1.08 (0.91–1.28)
0 1.0 3.00.5 1.5 2.0 2.5
Favours edoxaban 60mg Favours other treatments
Edoxaban 60 mg* vs. other DOACs for reduction of major bleeding†
in patients with CHADS2 score ≥ 2 at baseline
Edoxaban - Safety
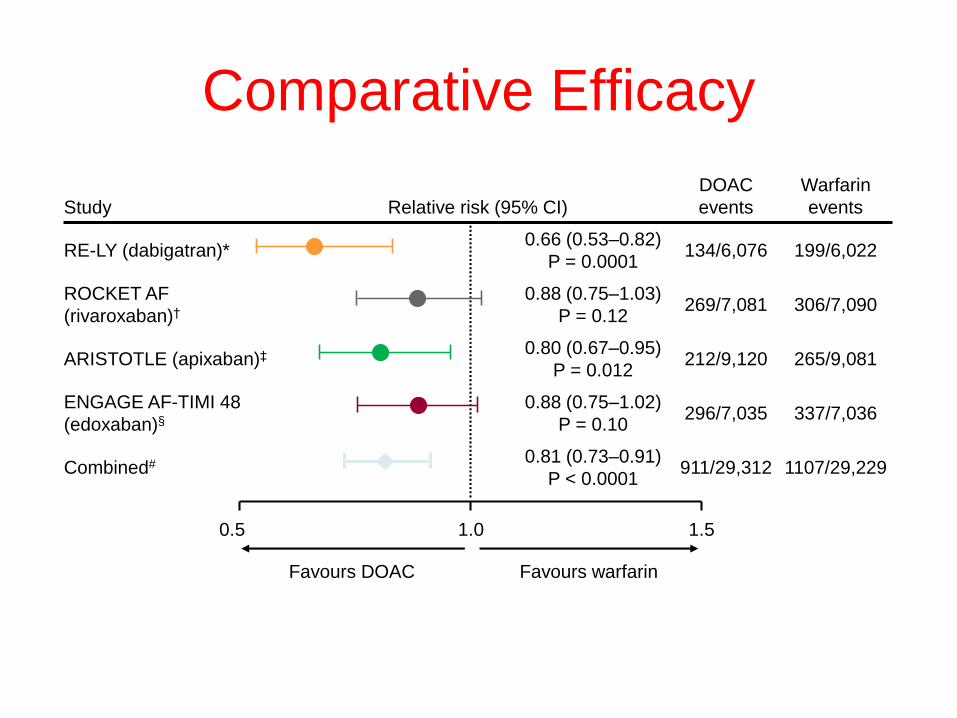
Study Relative risk (95% CI)
DOAC
events
Warfarin
events
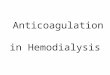
RE-LY (dabigatran)*0.66 (0.53–0.82)
P = 0.0001134/6,076 199/6,022
ROCKET AF
(rivaroxaban)†
0.88 (0.75–1.03)
P = 0.12269/7,081 306/7,090
ARISTOTLE (apixaban)‡ 0.80 (0.67–0.95)
P = 0.012212/9,120 265/9,081
ENGAGE AF-TIMI 48
(edoxaban)§
0.88 (0.75–1.02)
P = 0.10296/7,035 337/7,036
Combined# 0.81 (0.73–0.91)
P < 0.0001911/29,312 1107/29,229
Comparative Efficacy
0.5 1.0 1.5
Favours DOAC Favours warfarin
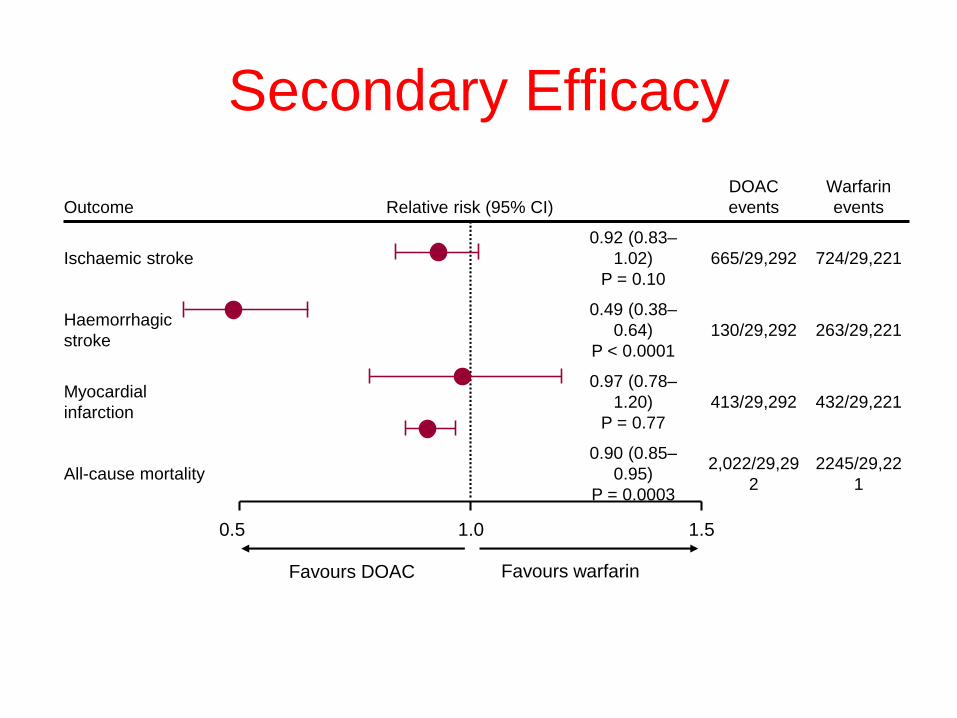
Secondary Efficacy
Outcome Relative risk (95% CI)
DOAC
events
Warfarin
events
Ischaemic stroke
0.92 (0.83–
1.02)
P = 0.10
665/29,292 724/29,221
Haemorrhagic
stroke
0.49 (0.38–
0.64)
P < 0.0001
130/29,292 263/29,221
Myocardial
infarction
0.97 (0.78–
1.20)
P = 0.77
413/29,292 432/29,221
All-cause mortality
0.90 (0.85–
0.95)
P = 0.0003
2,022/29,29
2
2245/29,22
1
0.5 1.0 1.5
Favours DOAC Favours warfarin
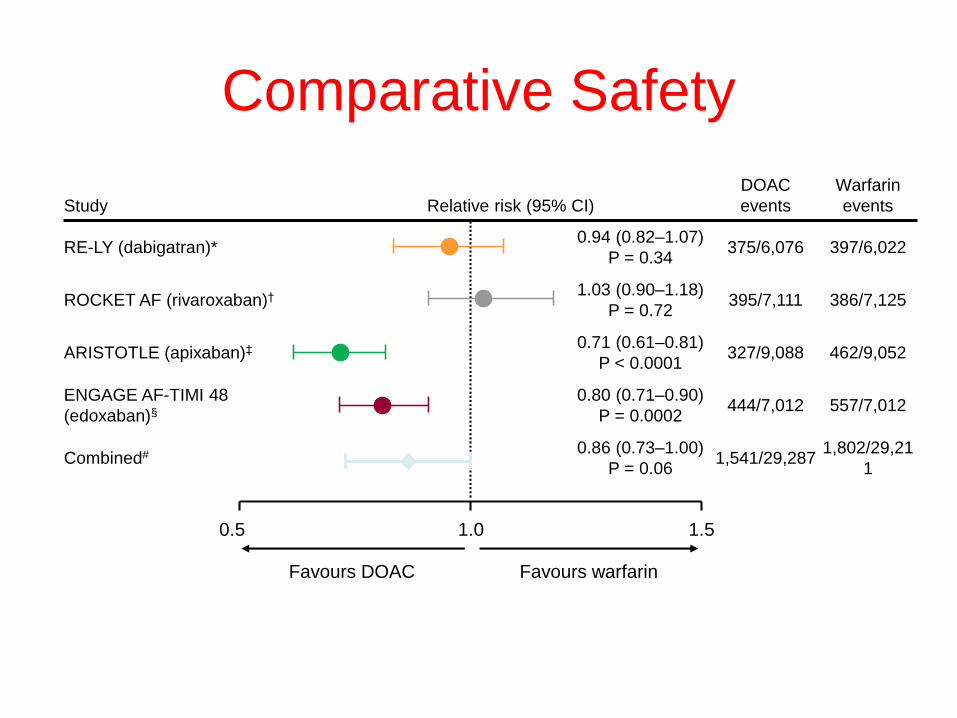
Comparative Safety
Study Relative risk (95% CI)
DOAC
events
Warfarin
events
RE-LY (dabigatran)*0.94 (0.82–1.07)
P = 0.34375/6,076 397/6,022
ROCKET AF (rivaroxaban)† 1.03 (0.90–1.18)
P = 0.72395/7,111 386/7,125
ARISTOTLE (apixaban)‡ 0.71 (0.61–0.81)
P < 0.0001327/9,088 462/9,052
ENGAGE AF-TIMI 48
(edoxaban)§
0.80 (0.71–0.90)
P = 0.0002444/7,012 557/7,012
Combined# 0.86 (0.73–1.00)
P = 0.061,541/29,287
1,802/29,21
1
0.5 1.0 1.5
Favours DOAC Favours warfarin
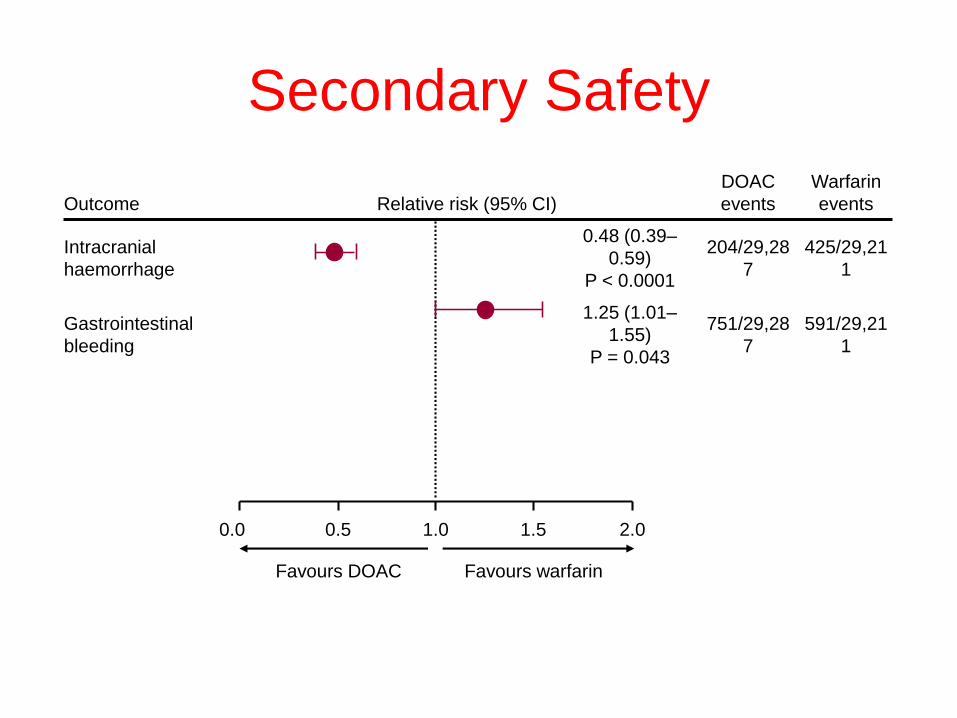
Outcome Relative risk (95% CI)
DOAC
events
Warfarin
events
Intracranial
haemorrhage
0.48 (0.39–
0.59)
P < 0.0001
204/29,28
7
425/29,21
1
Gastrointestinal
bleeding
1.25 (1.01–
1.55)
P = 0.043
751/29,28
7
591/29,21
1
Secondary Safety
0.0 1.0 2.01.50.5
Favours DOAC Favours warfarin
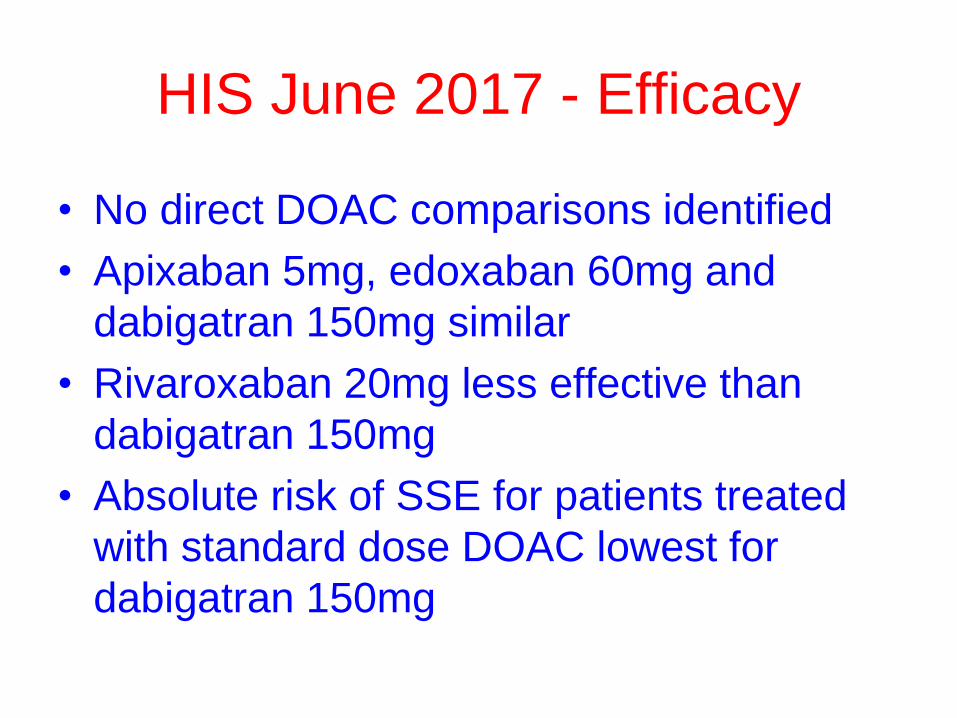
HIS June 2017 - Efficacy
• No direct DOAC comparisons identified
• Apixaban 5mg, edoxaban 60mg and
dabigatran 150mg similar
• Rivaroxaban 20mg less effective than
dabigatran 150mg
• Absolute risk of SSE for patients treated
with standard dose DOAC lowest for
dabigatran 150mg
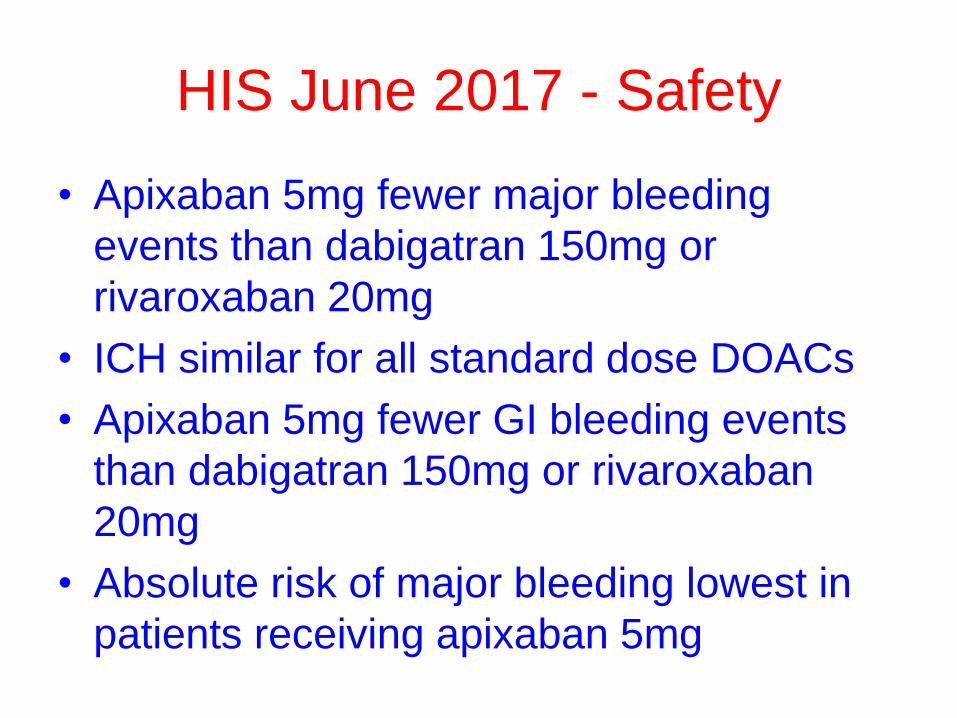
HIS June 2017 - Safety
• Apixaban 5mg fewer major bleeding
events than dabigatran 150mg or
rivaroxaban 20mg
• ICH similar for all standard dose DOACs
• Apixaban 5mg fewer GI bleeding events
than dabigatran 150mg or rivaroxaban
20mg
• Absolute risk of major bleeding lowest in
patients receiving apixaban 5mg
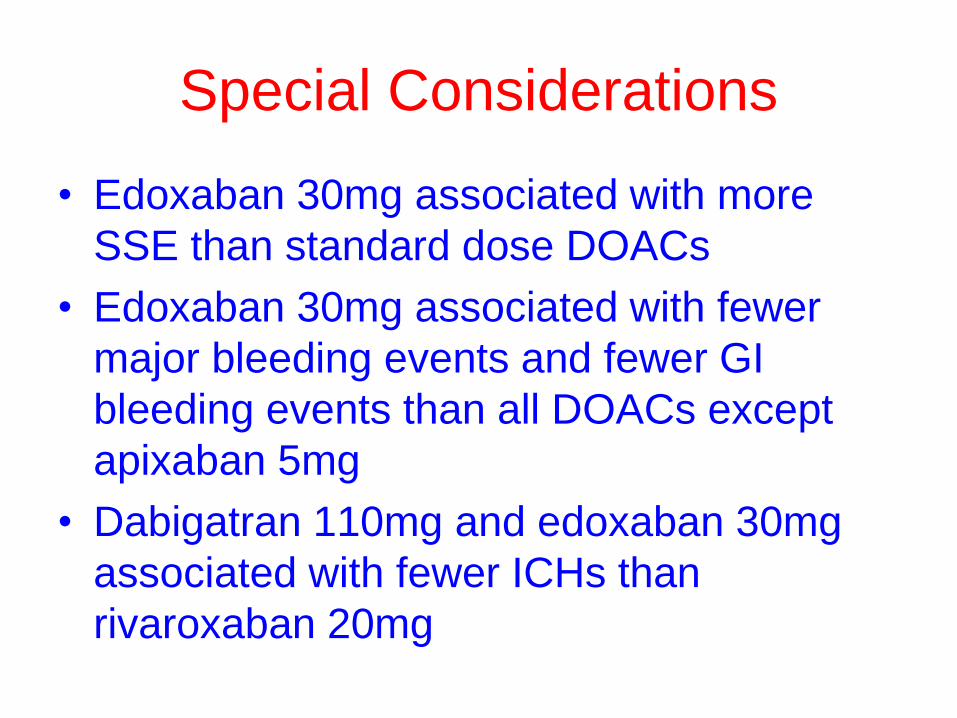
Special Considerations
• Edoxaban 30mg associated with more
SSE than standard dose DOACs
• Edoxaban 30mg associated with fewer
major bleeding events and fewer GI
bleeding events than all DOACs except
apixaban 5mg
• Dabigatran 110mg and edoxaban 30mg
associated with fewer ICHs than
rivaroxaban 20mg
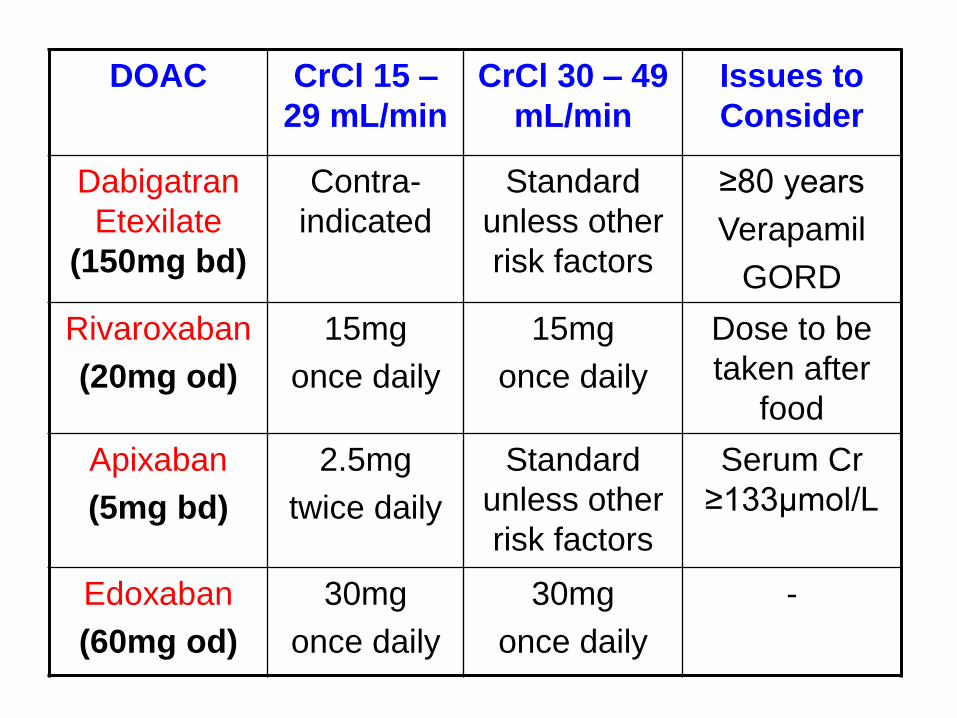
DOAC CrCl 15 –
29 mL/min
CrCl 30 – 49
mL/min
Issues to
Consider
Dabigatran
Etexilate
(150mg bd)
Contra-
indicated
Standard
unless other
risk factors
≥80 years
Verapamil
GORD
Rivaroxaban
(20mg od)
15mg
once daily
15mg
once daily
Dose to be
taken after
food
Apixaban
(5mg bd)
2.5mg
twice daily
Standard
unless other
risk factors
Serum Cr
≥133µmol/L
Edoxaban
(60mg od)
30mg
once daily
30mg
once daily
-
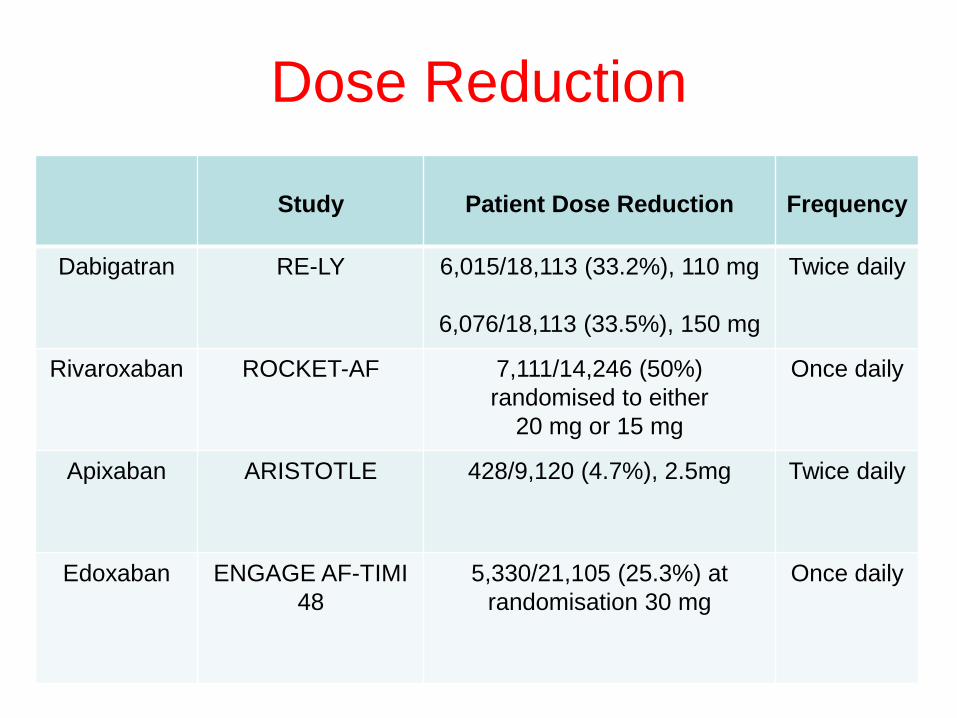
Dose Reduction
Study Patient Dose Reduction Frequency
Dabigatran RE-LY 6,015/18,113 (33.2%), 110 mg
6,076/18,113 (33.5%), 150 mg
Twice daily
Rivaroxaban ROCKET-AF 7,111/14,246 (50%)
randomised to either
20 mg or 15 mg
Once daily
Apixaban ARISTOTLE 428/9,120 (4.7%), 2.5mg Twice daily
Edoxaban ENGAGE AF-TIMI
48
5,330/21,105 (25.3%) at
randomisation 30 mg
Once daily
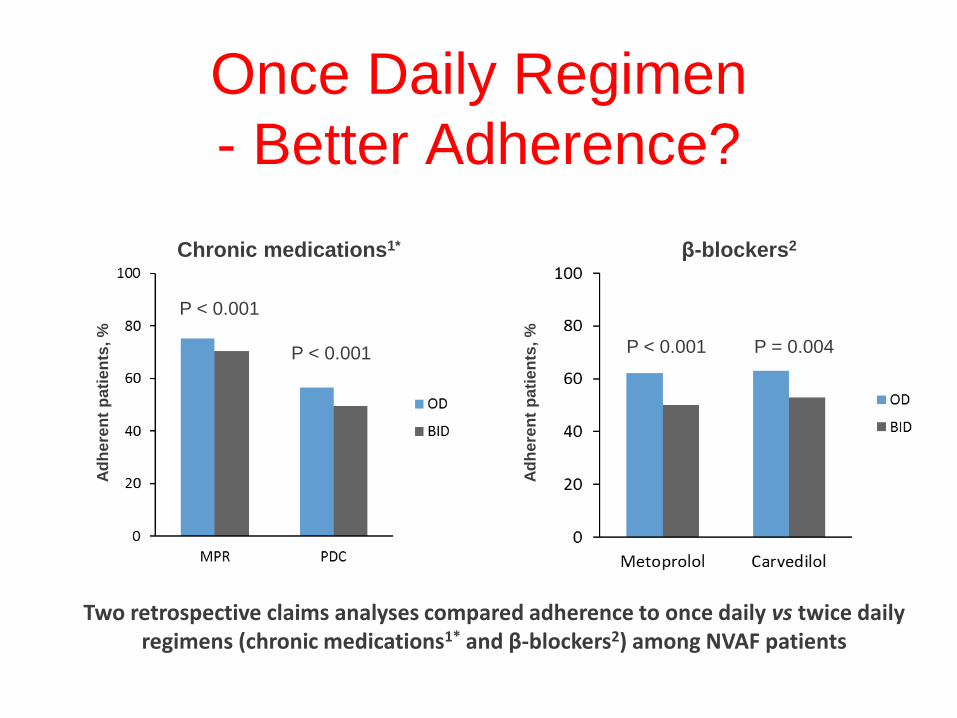
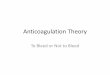
Once Daily Regimen
- Better Adherence?A
dh
ere
nt
pa
tie
nts
, %
P < 0.001
P < 0.001
Chronic medications1*
Ad
here
nt
pa
tie
nts
, %
β-blockers2
P < 0.001 P = 0.004
Two retrospective claims analyses compared adherence to once daily vs twice daily regimens (chronic medications1* and β-blockers2) among NVAF patients
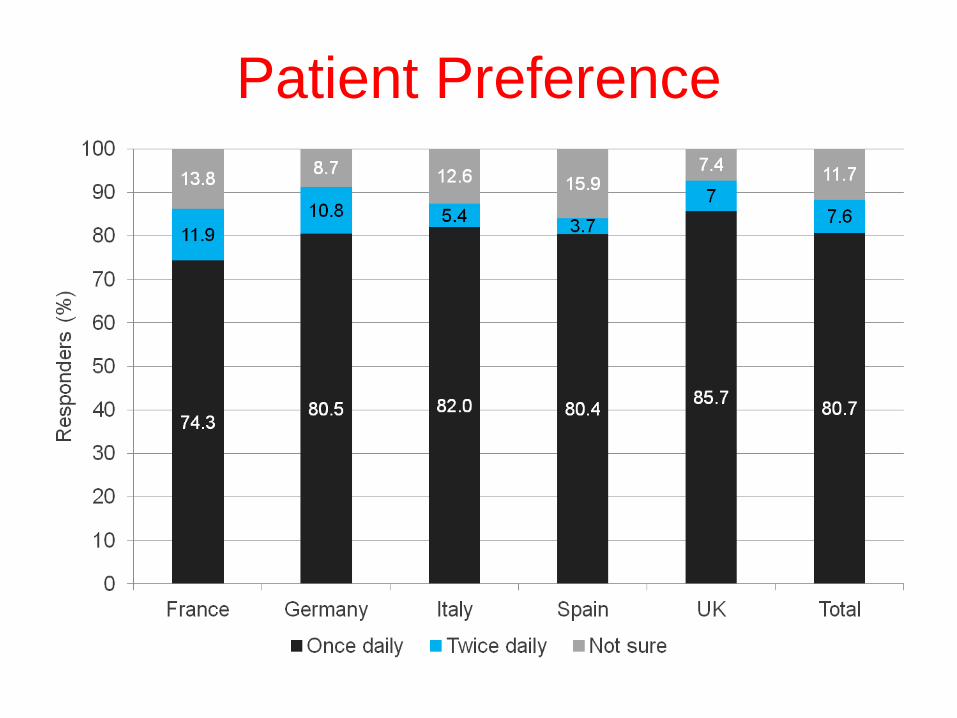
Patient Preference
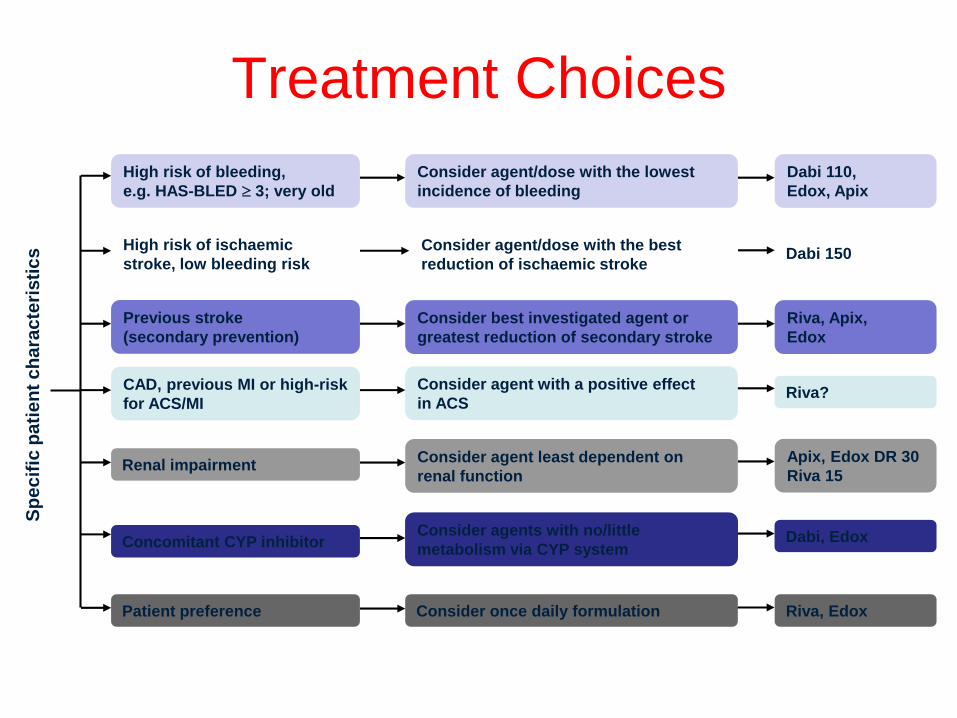
Patient preference Consider once daily formulation Riva, Edox
High risk of bleeding,
e.g. HAS-BLED 3; very old
Consider agent/dose with the lowest
incidence of bleeding
Dabi 110,
Edox, Apix
CAD, previous MI or high-risk
for ACS/MI
Consider agent with a positive effect
in ACS Riva?
High risk of ischaemic
stroke, low bleeding risk
Consider agent/dose with the best
reduction of ischaemic strokeDabi 150
Concomitant CYP inhibitorConsider agents with no/little
metabolism via CYP systemDabi, Edox
Renal impairmentConsider agent least dependent on
renal function
Apix, Edox DR 30
Riva 15
Sp
ec
ific
pa
tie
nt
ch
ara
cte
risti
cs
Previous stroke
(secondary prevention)
Consider best investigated agent or
greatest reduction of secondary stroke
Riva, Apix,
Edox
Treatment Choices
Thank you
Questions?
Case Study One
Female RW (85 years)
Relevant Medical History
• L breast CA (15.06.2015)
• pAF (30.03.2015); pre-op ECG 130bpm
• Rectal CA (12.03.2015)
• Osteoporosis (24.01.2014)
• Rheumatoid arthritis (07.08.2013)
• Hypothyroidism (06.02.2004)
Current Drug Therapy
Alendronic acid 70mg weekly, bisoprolol
1.25mg, fluoxetine 20mg, folic acid 5mg,
letrozole 2.5mg, levothyroxine 100µg,
methotrexate 20mg weekly, simvastatin
40mg and Theical-D3® daily
Condition and Treatment Considerations
• CHA2DS2-VASc = 3
– ≥75 years (2), female (1)
• Annual Risks:
– Stroke (3.2%) and SSE (4.6%)
Investigations
Occasional palpitations, exertional dyspnoea
BP 132/75mmHg, pulse 72bpm regular
Weight 62kg, serum Cr 77µmol/L
eGFR >60mL/min/1.73m2
Cockcroft-Gault CrCl 47mL/min
Treatment Outcomes
Commenced on apixaban 5mg twice daily
No effect on previous recurrent bleeding
(following surgery and radiotherapy)
Case Study Two
Male JT (87 years)
Relevant Medical History
• Asbestos-induced pleural plaque (14.10.2016)
• COPD - MRC 2 (20.05.2016)
• Pernicious anaemia (19.11.2014)
• pAF (11.04.2014)
• POCS (27.10.2013)
• Hypertension (03.02.2004)
Current Drug Therapy
Bisoprolol 2.5mg daily
Candesartan 16mg daily
Clopidogrel 75mg daily
Simvastatin 40mg daily
Condition and Treatment Considerations
• CHA2DS2-VASc = 5
– ≥75 years (2), hypertension (1), stroke (2)
• Annual Risks:
– Stroke (7.2%) and SSE (10%)
Investigations
No cardiovascular symptoms, though TATT
BP 177/73mmHg, pulse 44bpm regular
Weight 82kg, serum Cr 85µmol/L
eGFR >60mL/min/1.73m2
Cockcroft-Gault CrCl 63mL/min
Treatment Outcomes
Commenced on edoxaban▼ 60mg daily
Bisoprolol dose reduced to 1.25mg daily
Candesartan dose increased to 32mg daily
Follow-up (One)
• Renal function re-checked eight days after
review following candesartan dose increase:
U+Es N, K+ 4.8mmol/L
• BP 157/73mmHg, pulse 54bpm regular
Follow-up (Two)
Discussed tolerance to edoxaban at clinic
review; patient now feeling well, denies any
difficulties, bruising and bleeding
• BP 148/81mmHg, pulse 52bpm regular