Embed Size (px)
Citation preview


• Age 18 -79 • Clinical diagnosis of ischemic stroke with measurable neurologic
deficit (NIHSS). • NINDS tPA NEJM 1995, Stroke 1996;27:1711-1718
• Reliably timed onset of symptoms of ischemic stroke within 3 hours of the time to initiation of treatment with intravenous tPA.
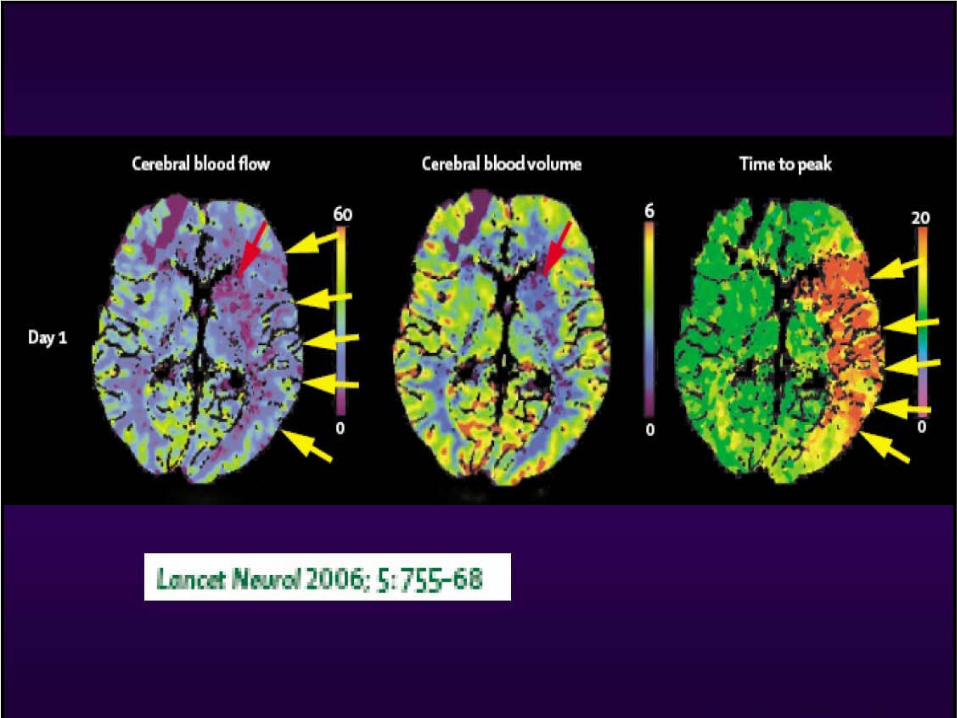
metaanalysis (Lancet 2004; 363 (9411): 768–774)
Inclusion criteria-NINDS

Contraindication to tPA• Minor / rapidly improving • ICH or mass on CT *• Seizure at stroke onset *• ICH ever • Stroke or serious head trauma < 3 months • GI or urinary tract haemorrhage in < 3 weeks • Major surgery/serious trauma in < 2 weeks • LP or Arterial puncture @ noncompressible site < 1 week • Current: symptoms of SAH,pericarditis or MI • Pregnant • SBP >185 mm of Hg or DBP> 110 mm of Hg (try ↓) *• Aggressive Rx to ↓ BP (>3doses of labetalol) *• Glucose <2.7 or >22 mmol/L *• Platelets <100 x 109/L • INR > 1.7, PTT >40
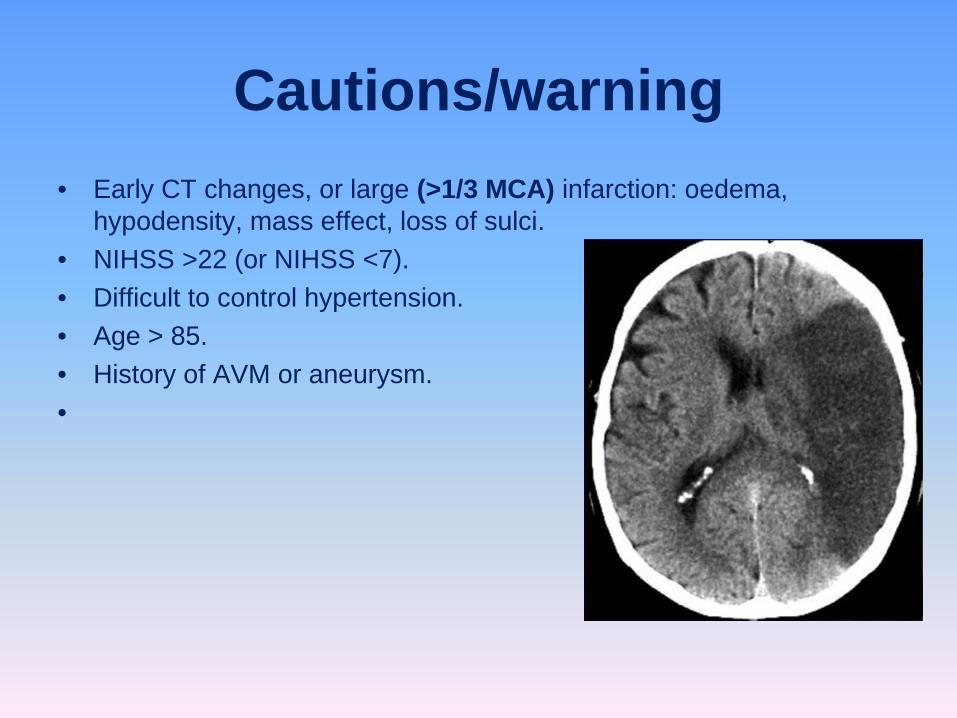
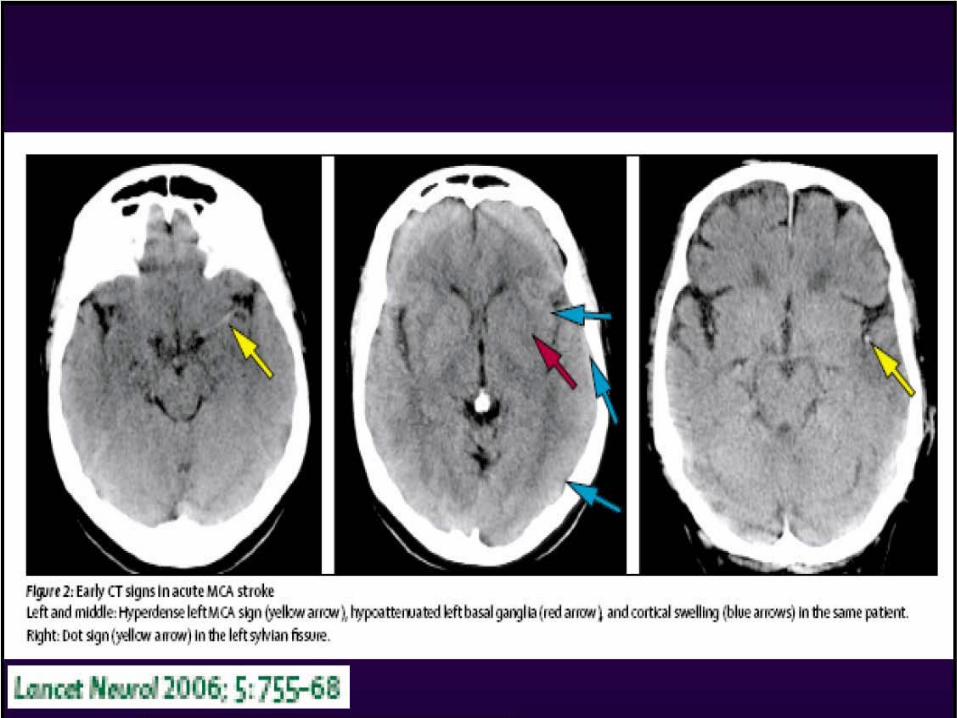
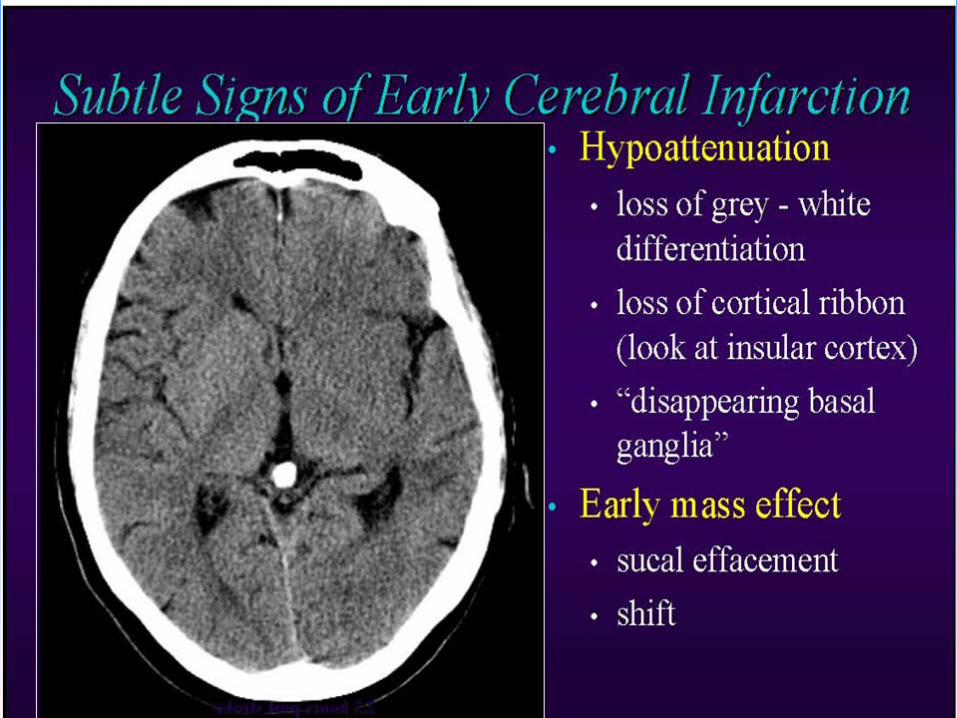
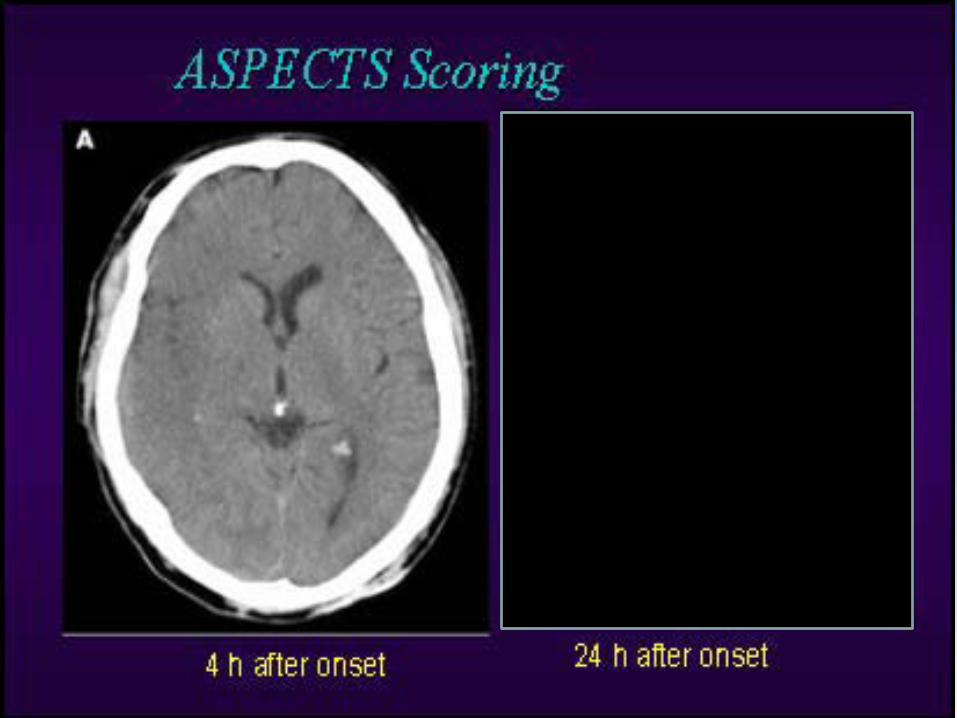
Cautions/warning• Early CT changes, or large (>1/3 MCA) infarction: oedema,
hypodensity, mass effect, loss of sulci. • NIHSS >22 (or NIHSS <7). • Difficult to control hypertension. • Age > 85. • History of AVM or aneurysm. •



• Benefits: • 42% vs. 26% regained independence at 3 months • NNT = 6 to have one additional patient recover to independence • NNT = 9 to have one additional patient achieve a full neurological
recovery • RISK: 6% overall risk of symptomatic brain hemorrhage (NNH: 18) •
• Dr. David Gladstone, 2004
ECASS-IIIECASS-III: Placebo controlled trial of alteplase (rt-PA) in acute
ischemic hemispheric stroke where thrombolytic is initiated between 3 and 4 hours after stroke onset
• To evaluate efficacy and safety of rt-PA between 3 and 4 hours after stroke onset in European setting.
• Multicenter, randomized, double blind, placebo controlled trial in 110 hospitals in 15 European countries.
• Inclusion CriteriaMale and female stroke patients, aged 18-80 years.
• Exclusion CriteriaNIHSS < 25 on admission, ordinary contraindications for thrombolysis, evidence of ICH on admission CT, prior clinical stroke or concomitant diabetes.

• Results:A total of 821 patients in the study and randomly assigned 418 to the alteplase group and 403 to the placebo group. The median time for the administration of alteplase was 3 hours 59 minutes. More patients had a favorable outcome with alteplase than with placebo (52.4% vs. 45.2%; odds ratio, 1.34; 95% confidence interval [CI], 1.02 to 1.76; P=0.04). In the global analysis, the outcome was also improved with alteplase as compared with placebo (odds ratio, 1.28; 95% CI, 1.00 to 1.65; P<0.05). The incidence of intracranial hemorrhage was higher with alteplase than with placebo (for any intracranial hemorrhage, 27.0% vs. 17.6%; P=0.001; for symptomatic intracranial hemorrhage, 2.4% vs. 0.2%; P=0.008). Mortality did not differ significantly between the alteplase and placebo groups (7.7% and 8.4%, respectively; P=0.68). There was no significant difference in the rate of other serious adverse events.
As compared with placebo, intravenous alteplase administered between 3 and 4.5 hours after the onset of symptoms significantly improved clinical outcomes in patients with acute ischemic stroke; alteplase was more
frequently associated with symptomatic intracranial hemorrhage.
• Patient Involvement:Patients will be randomized 1:1 to receive intravenous rt-PA (alteplase 0.9mg/kg bodyweight, maximally 90mg; 10% bolus plus one hour infusion) or placebo started between 3 and 4 hours from the onset of stroke.
• Primary Outcome:Primary efficacy endpoint is Modified Rankin Scale 0-1 at 90 days. Safety Endpoints: Survival at day 90, stroke related neurological deaths, symptomatic cerebral hemorrhage, cerebral herniation and symptomatic brain edema, vital signs, adverse events, laboratory parameters.
• Secondary Outcome:Secondary efficacy endpoint is Global Outcome (Modified Rankin Scale 0-1, Barthel Index 95-100, NIHSS 0-1, Glasgow Outcome Score 0-1) at 90 days. Further efficacy parameters are ordinary disability and functional scales, infarct size on CT at various time points after stroke onset, Modified Rankin Scale at 90 days stratified by admission NIHSS and length of in-hospital stay.


ECASS 3 is not clear yet
• Stroke+DM :exclude• >25 NIHSS: excluded• Early ischemic changes >1/3 MCA:excluded• NIHSS :0-1 in 90 days similar to NINDS-0 to 3
hrs• Bleeding rate 2.5% in tpa vs 0.2 in placebo
– European diff. of ICH !• Not enough studies
Nothing much but:
-recognition of stroke between heath employee since 2009-done-why worry?!
-no statistic, however I believe :2 acute stroke candidate arrive at ZMH per week3-5 not candidate >4-9 hours after event
-what about khalifa hospital? Almafraq,Alrhaba,Alain district-the same for Dubai-I guess?
At ZHM:
-all residents and doctors received a training sessions from sep.2009-Dec.2009 and still going
-Our parameds also received a training course regarding acute stroke protocol.(see UAE-paramed.protocol)
-ministry of interior parameds, training course (9-Jan.2011-April 4th 2011)
My/your job
-public education and stroke awareness
-stroke protocol :-EMS: ACT FASTO-20min.
-ER:ACT FASTO & NIHSS score -15-20 min.
-strokologist:ACT NIHSS score/CT Rx-10-25min.re do CT scan if >45min (ER doorRx)

A stroke, previously known medically as a cerebrovascular accident (CVA), is the rapidly developing loss of brain function's) due to disturbance in the blood supply to the brain. This can be due to ischemia 85% (lack of blood flow) caused by blockage (thrombosis, arterial embolism), or a hemorrhage 15% (leakage of blood).
Stroke definition?
Statistics:7/10 of residents and doctors can define stroke2/20 of parameds/nurse cant’
9/10 of doctors and resident can’t deal with acute stroke patients (lake of knolwedgefear?
20/20 of nurse and paramed cant’ deal with stroke patients
surprisely : strokologist/head of department able to manage stroke patients but want me to start the protocol? “discretions here”
Somewhat/somewhere-NO support enough!!
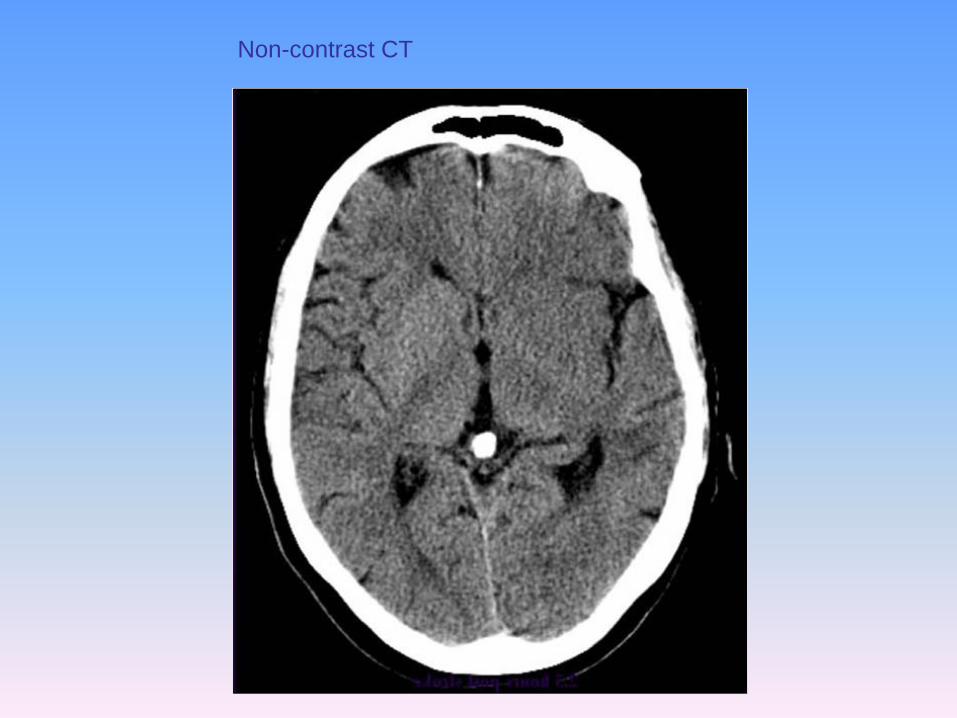
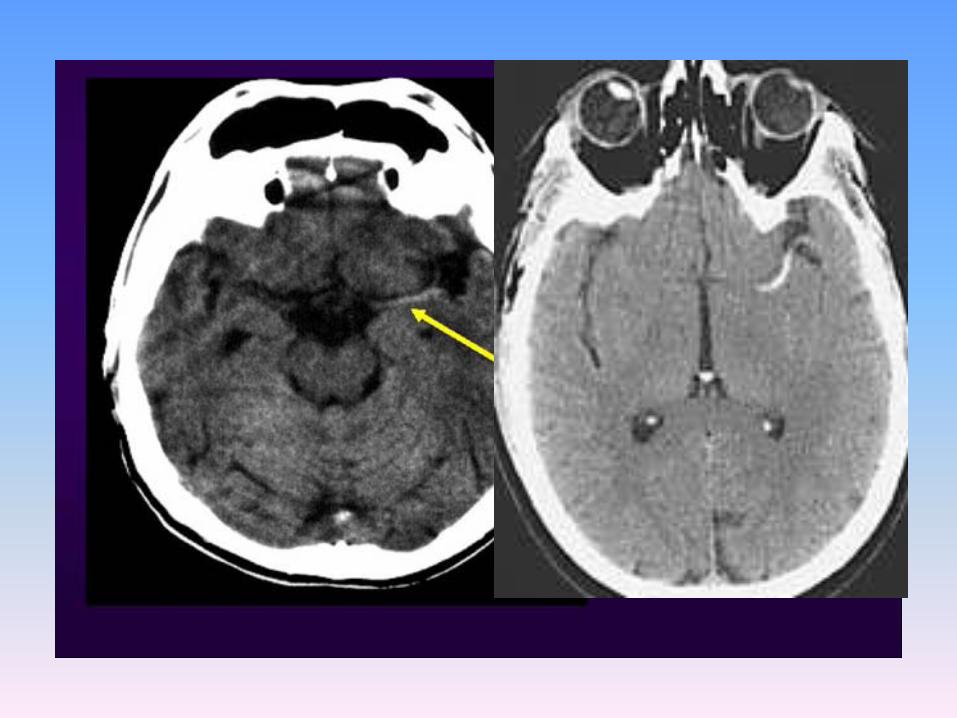
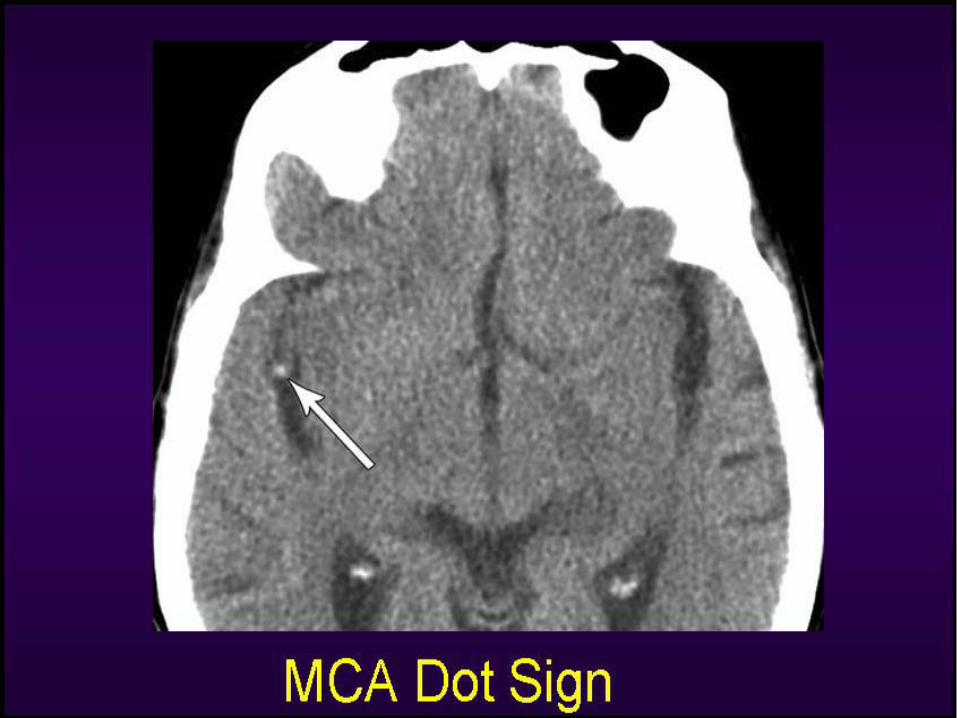
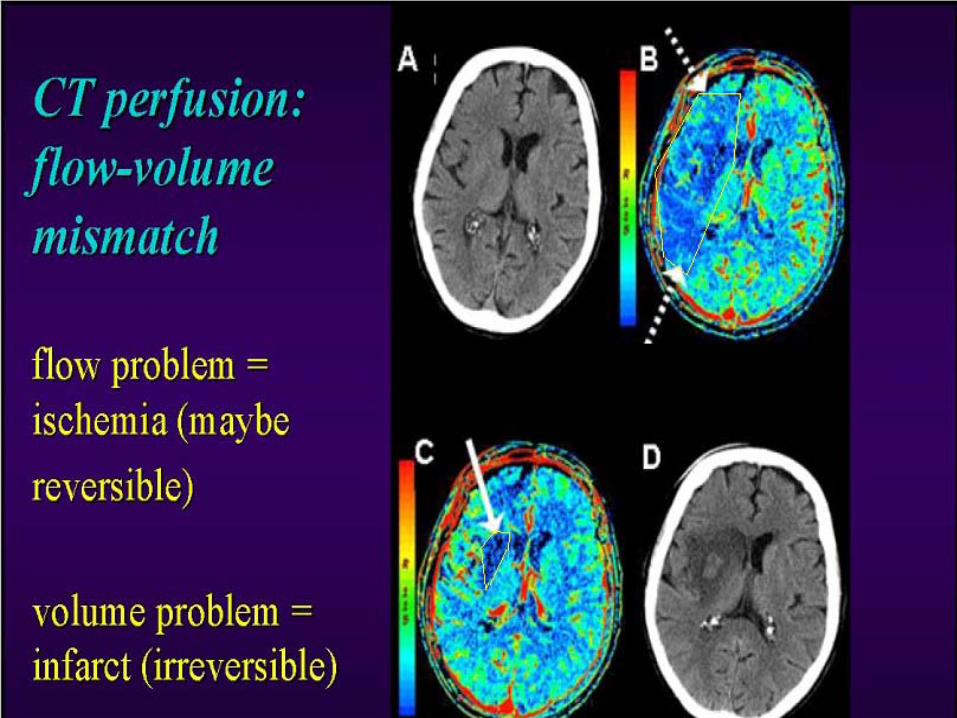
Non-contrast CT

With treatment
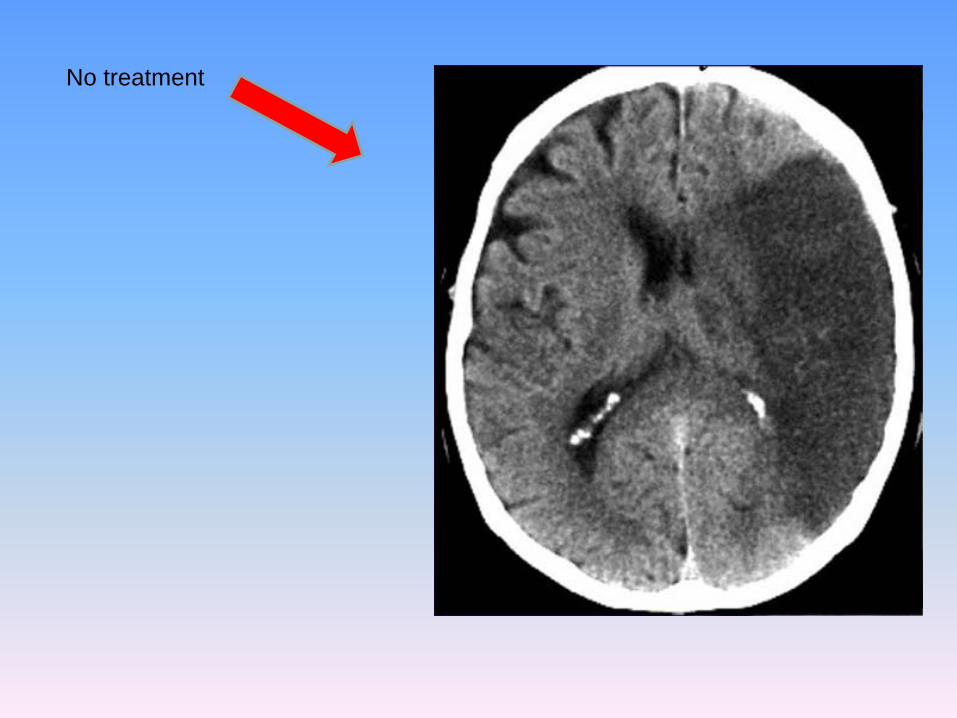
No treatment

Stroke impact on society?
-the 3rd leading cause of mortality worldwide and in UAE too?
-number of days admission +
-ICU admission+
-Cause effect++
-rehab. Cause
-family distress
-job loss
-number of working hours lost (pt./family/sponsor..)





prehospital• EMS Prompt cards: • NEW, unilateral
weakness, slurred speech/aphasia/mute &/or aphasia, facial droop
• Can GET to hospital w/in 2 hours of clearly defined onset (“last seen normal”)
• NOT TO BE BYPASS (should go to nearest ER-not applicable in UAE-we will accept in ZMH)


FAST-O
• Face• Arms• Speech• Time• Other:
– Double vision, sever headache, numbness of face; arms and legs, was and wean quadriparesis…

EMS Rx• Paramed.guidelines for acute stroke treatment • Manage ABC’s, get IV access, O2 • Assess glucose • NPO • Call ER & go fast • DON’T give excess sugar or fluids, or drop BP too much • Pre-hospital Identification –usually @ ER
• paramedic/ASA GUIDELINES – Early Management of Acute Ischemic Stroke In Adults

case1• 75 M• PMHx:
– HTN,DM, no recent (surgery, trauma, ICH )– Seizure disorder (no event for one year)-what Q would you ask here?
• Rx:– ASA 81mg,dilantin 300mg qhs,ACEI?
• HPI:– Sudden Rt sided weakness and aphasia @ 3PM
• O/E: time of arrival 3:15PM– VSS,ABCD normal, what test you want to do/what else?– FASTO:3/5 Rt sided weakness , non-fluance speak
• Discussion: is this stroke or mimickers?

case2• 102 F• PMHx:
– Dyslipedimic ,DM, no recent (surgery, trauma, ICH,old MI 2003 )– what other Qs would you ask here?
• Rx:– Lipitor 10mg od, ASA 81mg,thiazid I od, insulin sc 20/40u
• HPI:– Wakeup at 7 with Lt sided weakness and confused.
• O/E: time of arrival 7:20AM– VSS,ABCD normal, what test you want to do/what else?– FASTO:1/5 Lt sided weakness , denial being sick? Why?
• Discussion: is this stroke or mimickers?

case3• 35 M• PMHx:
– Newly Dx HTN, no Hx (DM, seizure, surgery, trauma, ICH )– what Q would you ask here?
• Rx:– none?
• HPI:– Lower limbs weakness and difficulty of swallowing @ 12 non– Symptoms resolved @ 12 :10 non– Similar symptoms @ 1:00 PM + double vision
• O/E: time of arrival 1:13PM– VSS,ABCD normal, what test you want to do/what else?– FASTO:x4 limbs 4/5, numb. Face trunk and limbs x4, skew eyes
• Discussion: is this stroke or mimickers? Where?

For residents and doctors
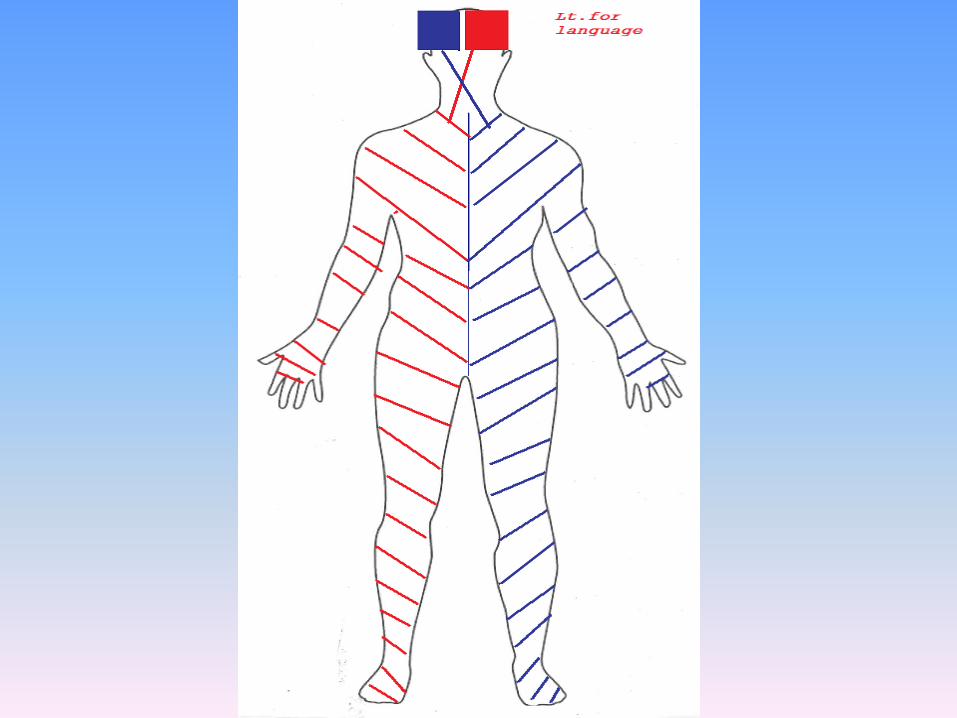
Yes< or = 4 hours for anterior circulation
limbs weaknessaphysiavisual field cut defectsensory lost
< or =6-12 hours for posterior circulation
limbs weakness, hemi./quadriplegia/paresisdysarthiadysphasiadysphagiadouble visionvisual field cut defect
“wax and wean symptoms” young patients
Above symptoms + autonomic feature may confuse the picture however stroke is NUMBER ONE to be considered
For ER Doc./Med. Oncall• Step 1: Is this a stroke? • What are common stroke syndromes? • What mimics a stroke – how do I rule those out? • Step 2: Is this a treatable stroke? • How bad is the stroke – NIHSS, CT / MRI, perfusion-diffusion -
specialist and consultant to decide for these studies • Indications / contraindications / side effects • Step 3: Can I maximize good outcomes?
ER assessment• Put down your reflex hammer!!! • Be quick (“Time is Brain”) • Full neuro exam can be done LATER!
• Is the patient a tPA candidate? • TIME OF ONSET: • When were they last at previous baseline or symptom-free? “when
were they last seen normal?” • What to do with “the waker-uppers?”
• Time of onset = last awake and normal • Be BRIEF! • Look for contra-indications / concerns.

Contraindication-do you remember!
• History:• When were they last seen normal? • How bad were they (rapidly improving? Sz?) • Ever had any bleeding (head, gut etc)? • On any medications (BP, warfarin, ASA, Insulin)? • Had any surgery or trauma recently? Been in a hospital for anything
in the last few months?



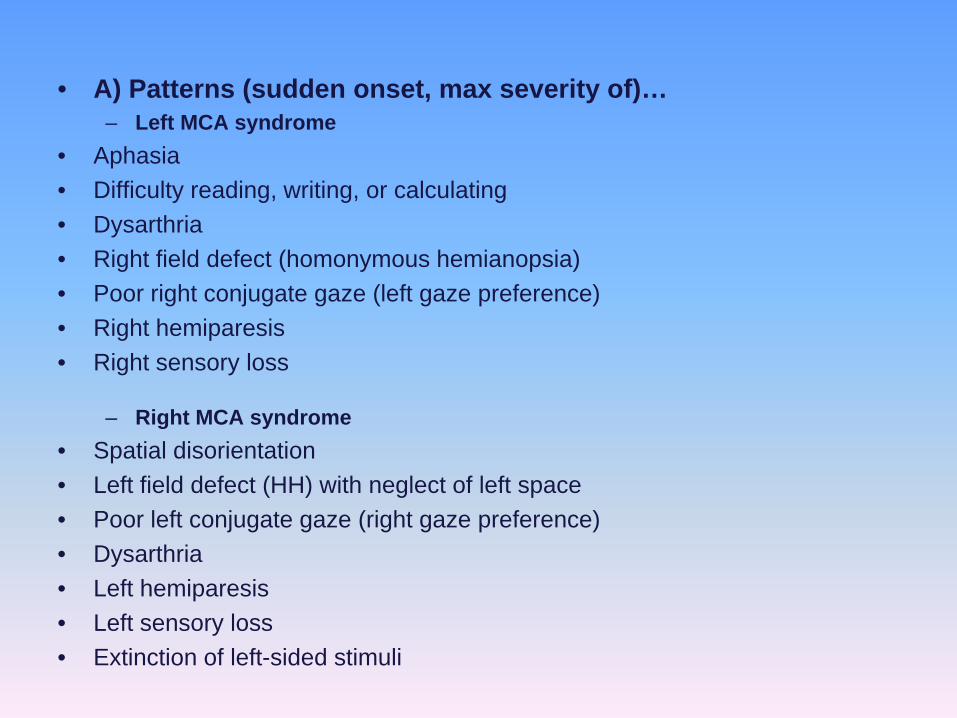
• A) Patterns (sudden onset, max severity of)… – Left MCA syndrome
• Aphasia • Difficulty reading, writing, or calculating • Dysarthria • Right field defect (homonymous hemianopsia) • Poor right conjugate gaze (left gaze preference) • Right hemiparesis • Right sensory loss
– Right MCA syndrome• Spatial disorientation • Left field defect (HH) with neglect of left space • Poor left conjugate gaze (right gaze preference) • Dysarthria • Left hemiparesis • Left sensory loss • Extinction of left-sided stimuli
– Vertebrobasilar syndrome • Vertigo, nausea, vomiting, cognitive (amnesia) • Bilateral visual field defects • Dysconjugate gaze (diplopia) • Nystagmus • Dysarthria • Motor or sensory loss in all four limbs • Crossed signs • Limb or gait ataxia
– Lacunar syndromes • Pure motor (corona radiata – IC – pons – medullary pyramids) • Pure sensory (cortex, Centrum semiovale, posterolateral thalamus /
posterior limb of IC) • Sensorimotor (large subcortical / thalamus) • Ataxic hemiparesis (corona radiata, anterior limb of internal capsule, upper
basis pontis, even lentiform) • Dysarthria-clumsy hand syndrome (see above)
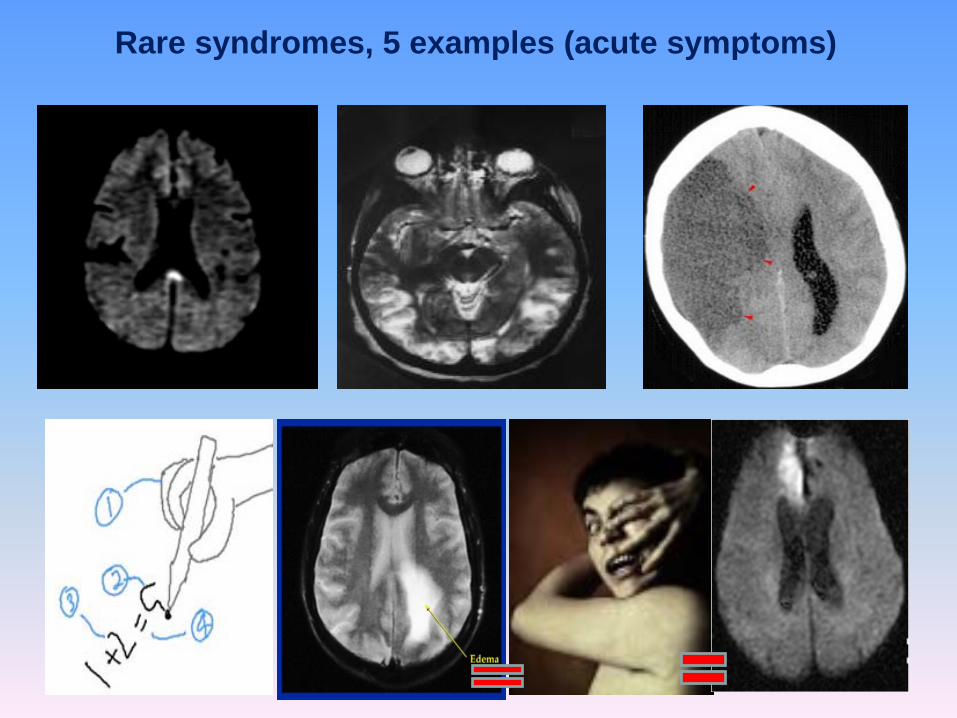
Rare syndromes, 5 examples (acute symptoms)

Is this a stroke?!• ~20% acute strokes are NOT strokes. • Common Stroke Mimics: • Hypoglycaemia • Hypertensive emergency (encephalopathy) • Migraine Aura • Seizure / post-ictal deficits • CNS pathology (infection, tumour) • Conversion disorder
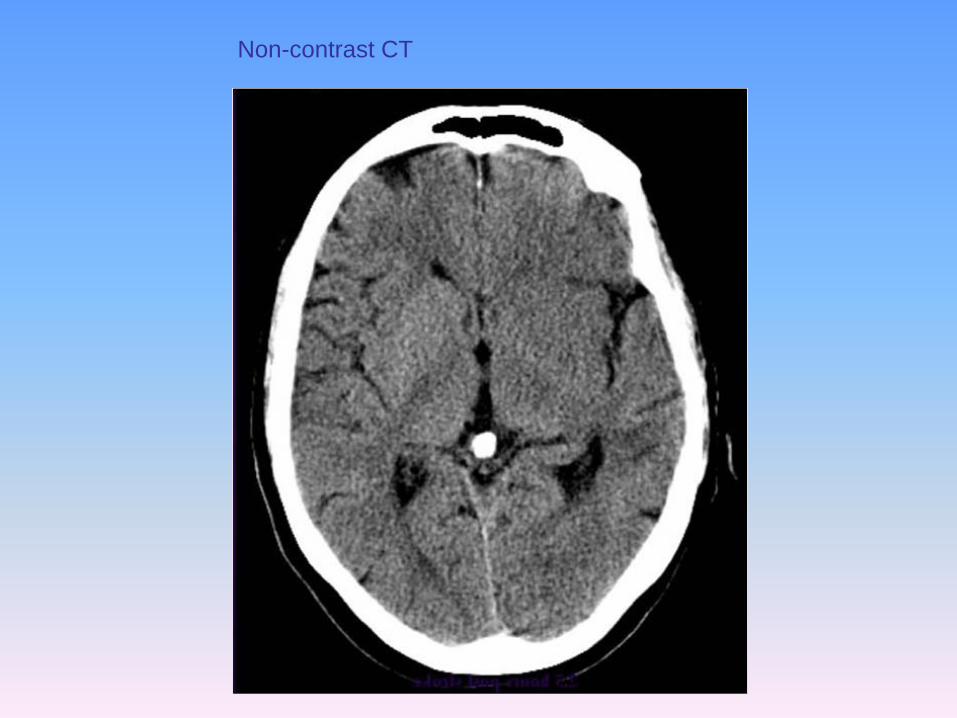
Non-contrast CT
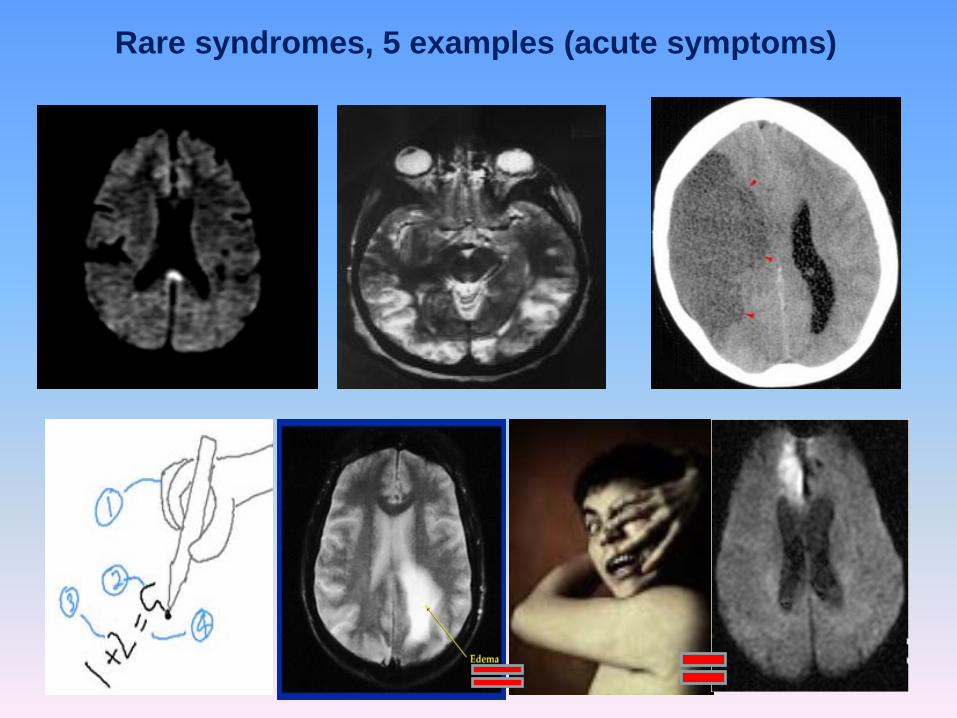
Rare syndromes, 5 examples (acute symptoms)

Stroke Mimickers







gradient echo-bad for a good tPAcandidates


What do I tell the family?• More patients treated with tPA have a better functional
neurological outcome than if left untreated • Risk of haemorrhage is (~5%) and can be fatal • NNT = 6 for one more independent, NNT = 9 for totally
normal • Better chance of doing well and not being dependent • OFF protocol should get (& document) consent

So you are giving the juice?• 0.9mg/kg total dose (e.g. 63 mg in a 70 kg person) • 10% of dose as bolus (e.g. 6.3 mg over 1 min); remainder in bag dripped
over 1 hour • Neuro vitals q15 min during infusion, q30 min x 6h and then q1h x16h (total
24h) (By RN, not you…) • BP: q 15 min x 2h, q 30m x 6 h, q 1h x 16h… • Delay placement of NG tubes, bladder catheters or arterial lines (ideally do
all of this BEFORE tPA) • CT scan @ 24h (BEFORE antiplatelet or anticoagulant) • Avoid antiplatelet for 24h • Avoid sc heparin for 3-4 days • Avoid placement of lines or bladder catheters • Monitor BP, Glucose and Temperature
– see order 1,2 & 3


Post tPA orders• NPO for all patients, frequent vitals and neurovitals for
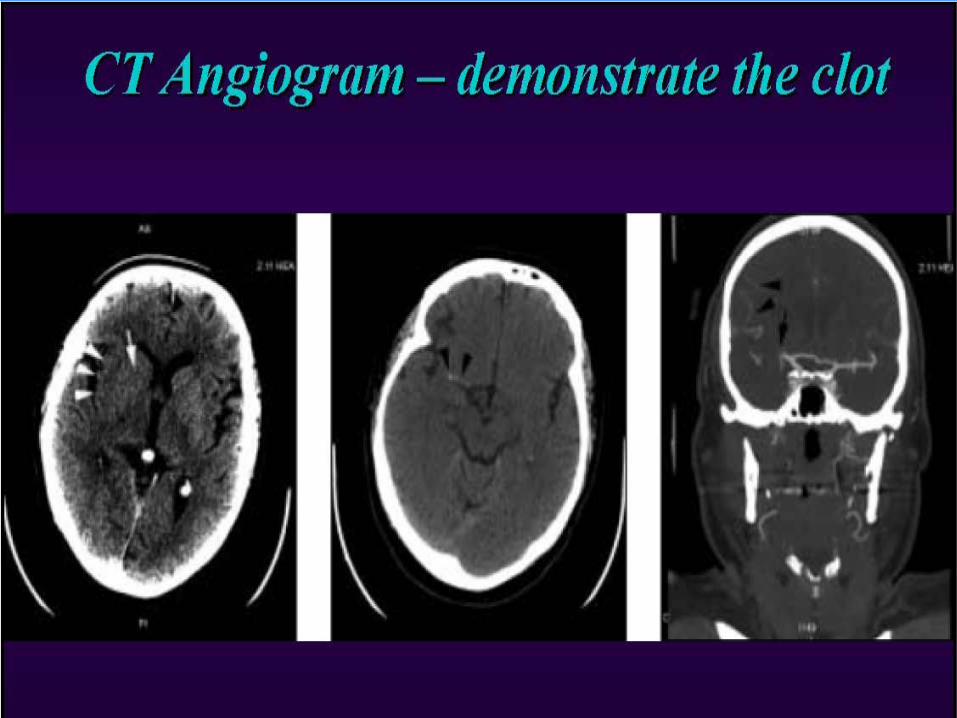
24h-ICU • Repeat CT head in 24 hours; MRI/MRA*/CTA*• Hold antiplatelet for 24 hrs, no place for
heparin/mechanical cardiac valve –risk vs. benefit)*• Source of stroke: TEE; U/S; Holter monit.TCD*• Secondary prevention (part 2 talk)• Coagulation profile workup & coagulopathy for
cryptogenic stroke*• FBS;Lipds profile• PT/SP/OT









![Medicine > Neurology > Stroke Stroke - Initial assessment ... · Stroke caused by intracerebral haemorrhage is defined as [1][L2]: ... and emboli may be generated. • The most common](https://img.pdfslide.net/doc/110x75/5c8ae1ae09d3f2fa728b79a9/medicine-neurology-stroke-stroke-initial-assessment-stroke-caused.jpg)