Embed Size (px)
Citation preview

Clinical Diagnosis of Neurodegenerative Diseases by (CSF) Cerebro Spinal Fluid Labelling
Neuropeptide/Neurotransmitter Mapping & Oxidative Stress during
Parkinson’s Disease On / Off states
Parvez, S. H., Collin, C., Qureshi, G.A. & Parvez, S.
CNRS: Neuroendocrine Unit
Institut Alfred Fessard of Neurosciences, French National Research Center,
Bât 5, 91190 Gif Sur Yvette, FranceEmail: [email protected] & [email protected]
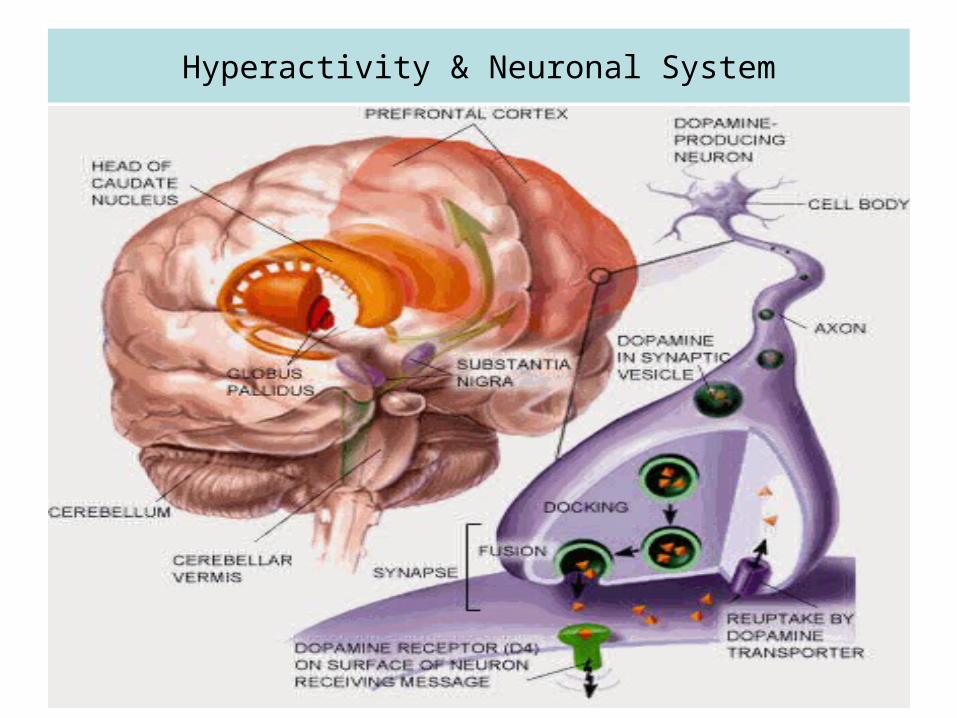
Hyperactivity & Neuronal System

Human Brain & Specific Functions
Parkinson’s Disease
1) Classical Clinical Features• Resting Tremor :Cogwheel Rigidity Bradykinesia :
Postural Instability
2)Associated Clinical Features• Micrographia : Hypophonia : Hypomimia• Shuffling Gate/Festination : Drooling• Dysphagia : Autonomic Dysfunction• Depression : Dementia
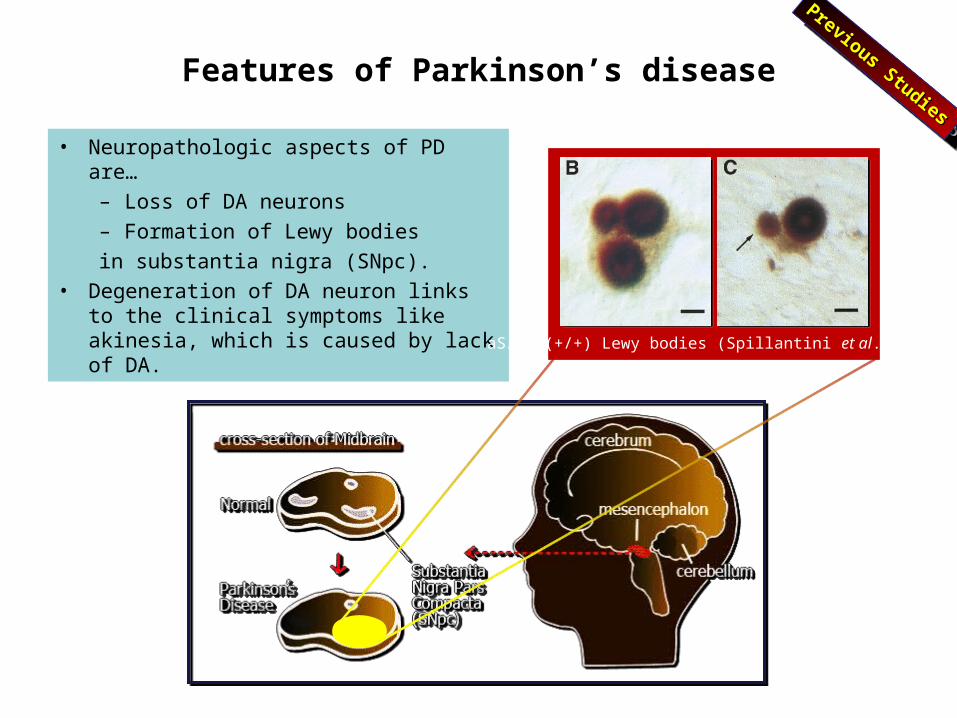
Features of Parkinson’s disease
• Neuropathologic aspects of PD are…– Loss of DA neurons– Formation of Lewy bodiesin substantia nigra (SNpc).
• Degeneration of DA neuron links to the clinical symptoms like akinesia, which is caused by lack of DA. aS/ubi(+/+) Lewy bodies (Spillantini et al., 1998)
Previous Studies
Previous Studies
Previous Studies
Previous Studies
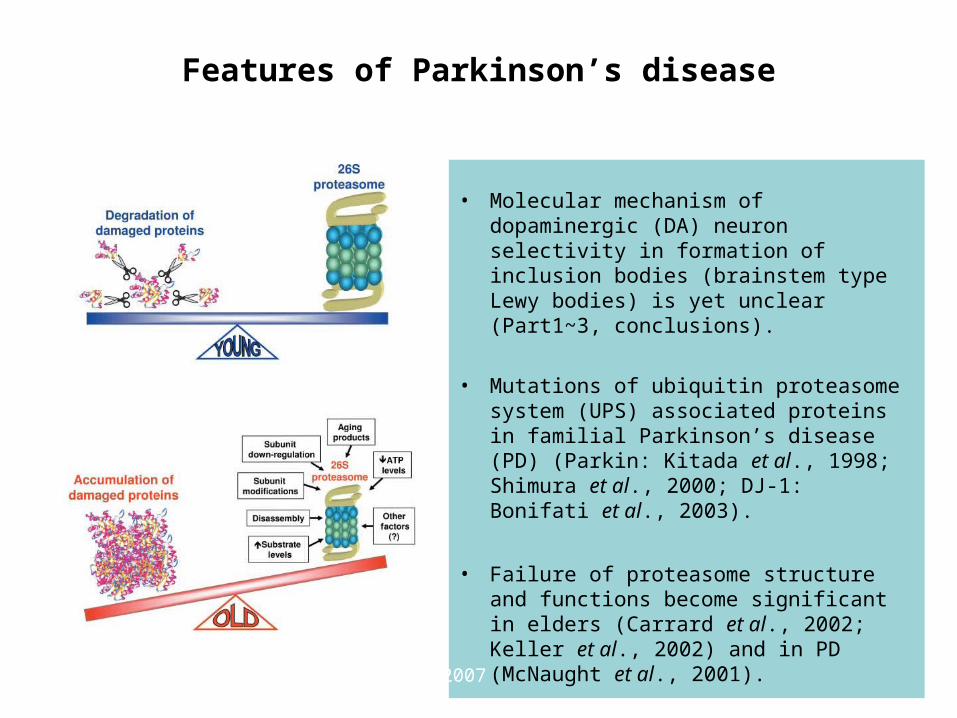
Features of Parkinson’s disease
• Molecular mechanism of dopaminergic (DA) neuron selectivity in formation of inclusion bodies (brainstem type Lewy bodies) is yet unclear (Part1~3, conclusions).
• Mutations of ubiquitin proteasome system (UPS) associated proteins in familial Parkinson’s disease (PD) (Parkin: Kitada et al., 1998; Shimura et al., 2000; DJ-1: Bonifati et al., 2003).
• Failure of proteasome structure and functions become significant in elders (Carrard et al., 2002; Keller et al., 2002) and in PD (McNaught et al., 2001).
modified from Vernace et al., 2007

Lewy bodies in human brainstem were TH positive
Lewy bodies (arrows in A and D) and a Pale body (arrowhead in D) had strong TH immunoreactivity. In the high power images in B, C and E, typical halo and Lewy neurites were shown and all of them were TH immunopositive. Scale bars indicate 20 μm in A, D and 8 μm in B, C, E.
nucleus
Lewy body
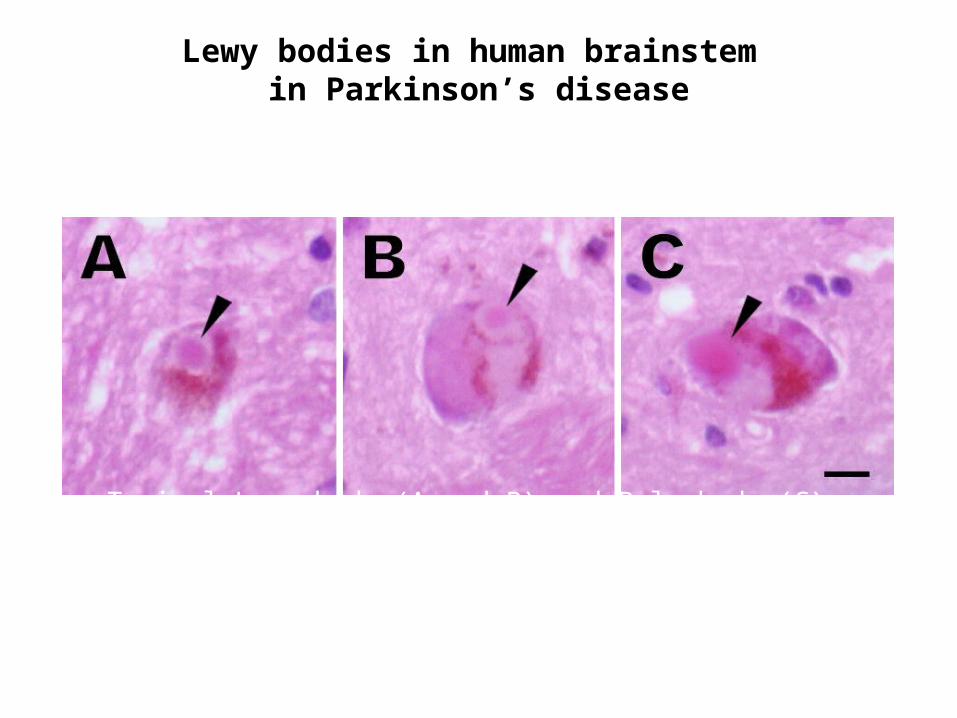
Lewy bodies in human brainstem in Parkinson’s disease
Typical Lewy body (A and B) and Pale body (C).Scale bar indicates 8 μm and all the images are same scale.
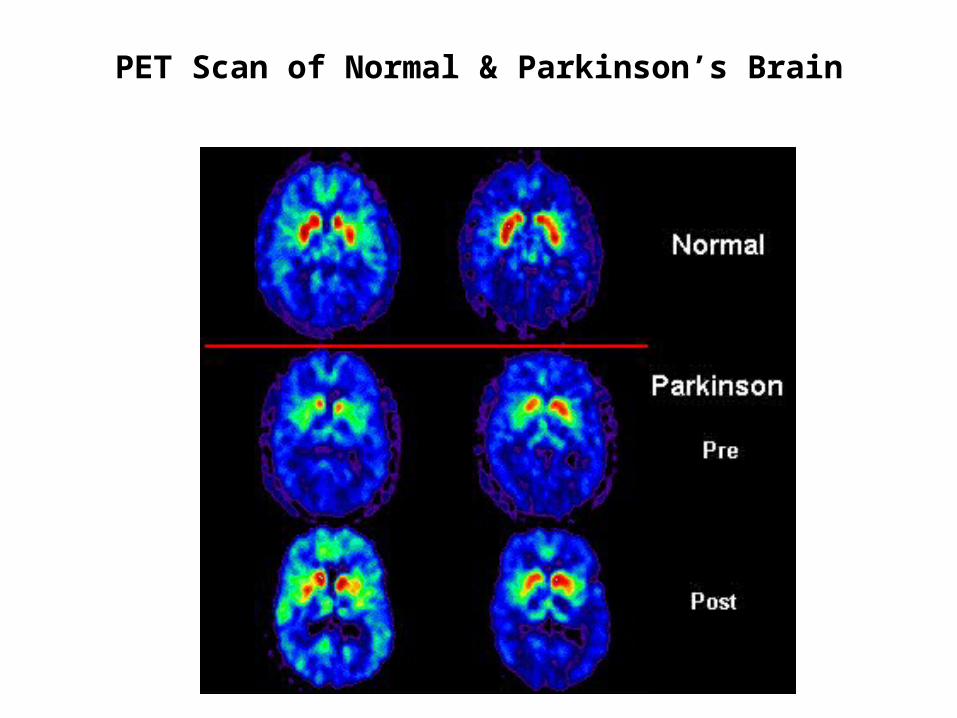
PET Scan of Normal & Parkinson’s Brain
Blood Brain Barrier
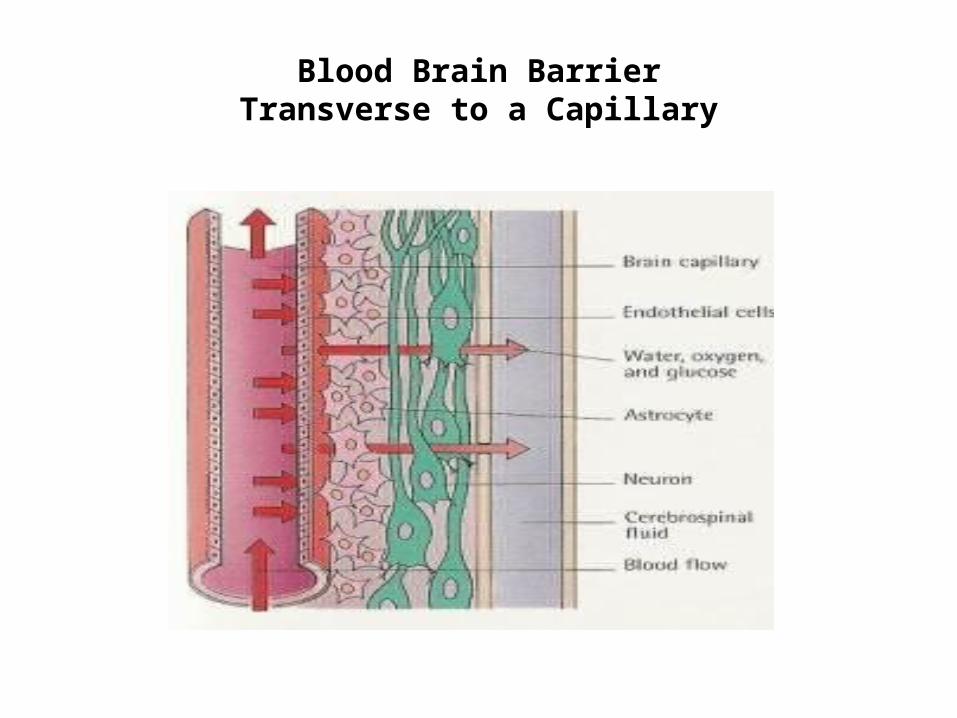
Blood Brain BarrierTransverse to a Capillary
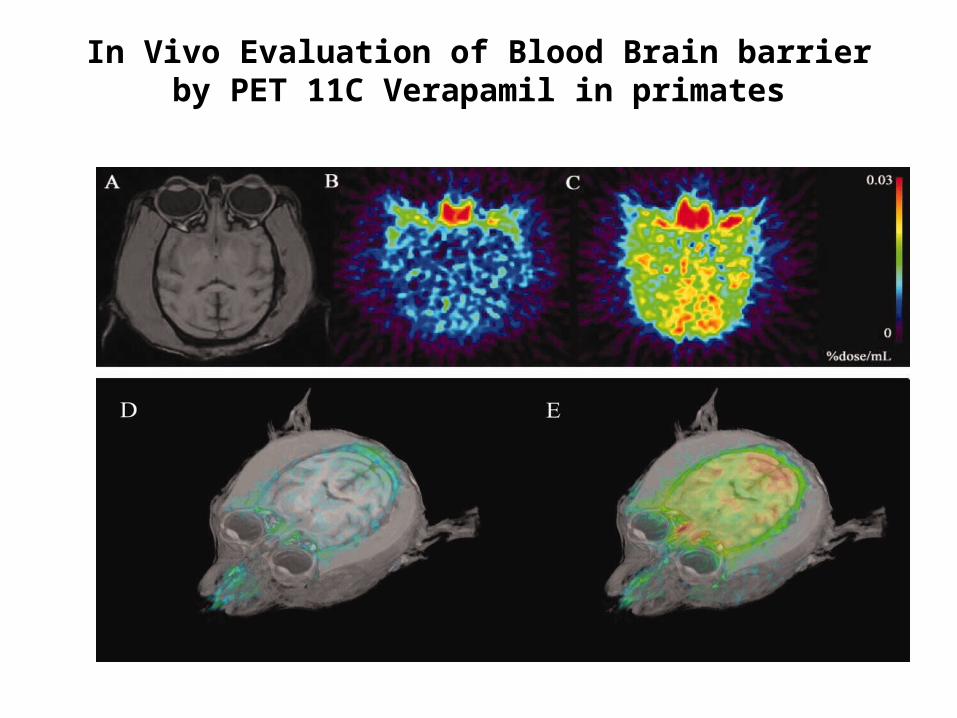
In Vivo Evaluation of Blood Brain barrierby PET 11C Verapamil in primates
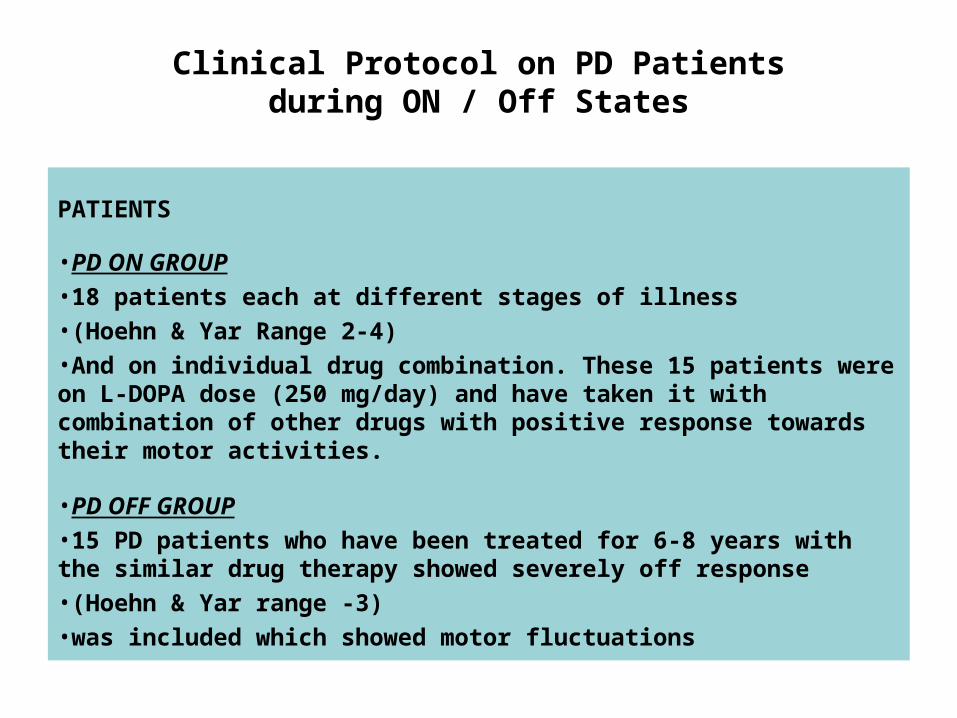
Clinical Protocol on PD Patientsduring ON / Off States
PATIENTS
•PD ON GROUP
•18 patients each at different stages of illness
•(Hoehn & Yar Range 2-4)
•And on individual drug combination. These 15 patients were on L-DOPA dose (250 mg/day) and have taken it with combination of other drugs with positive response towards their motor activities.
•PD OFF GROUP
•15 PD patients who have been treated for 6-8 years with the similar drug therapy showed severely off response
•(Hoehn & Yar range -3)
•was included which showed motor fluctuations
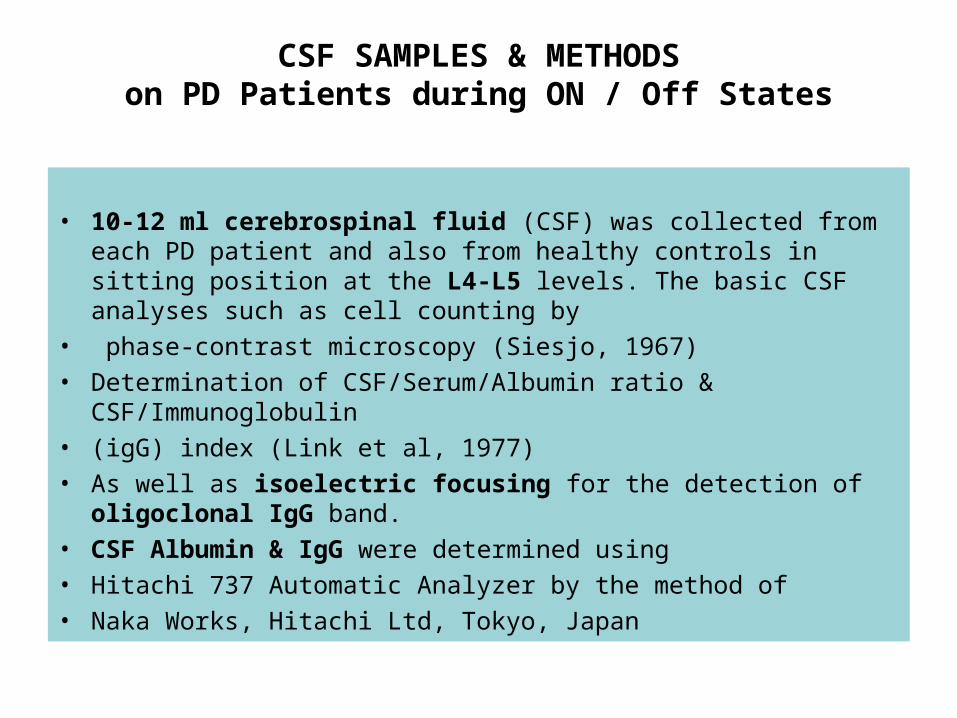
CSF SAMPLES & METHODSon PD Patients during ON / Off States
• 10-12 ml cerebrospinal fluid (CSF) was collected from each PD patient and also from healthy controls in sitting position at the L4-L5 levels. The basic CSF analyses such as cell counting by
• phase-contrast microscopy (Siesjo, 1967)• Determination of CSF/Serum/Albumin ratio & CSF/Immunoglobulin• (igG) index (Link et al, 1977)• As well as isoelectric focusing for the detection of oligoclonal IgG
band.• CSF Albumin & IgG were determined using• Hitachi 737 Automatic Analyzer by the method of• Naka Works, Hitachi Ltd, Tokyo, Japan
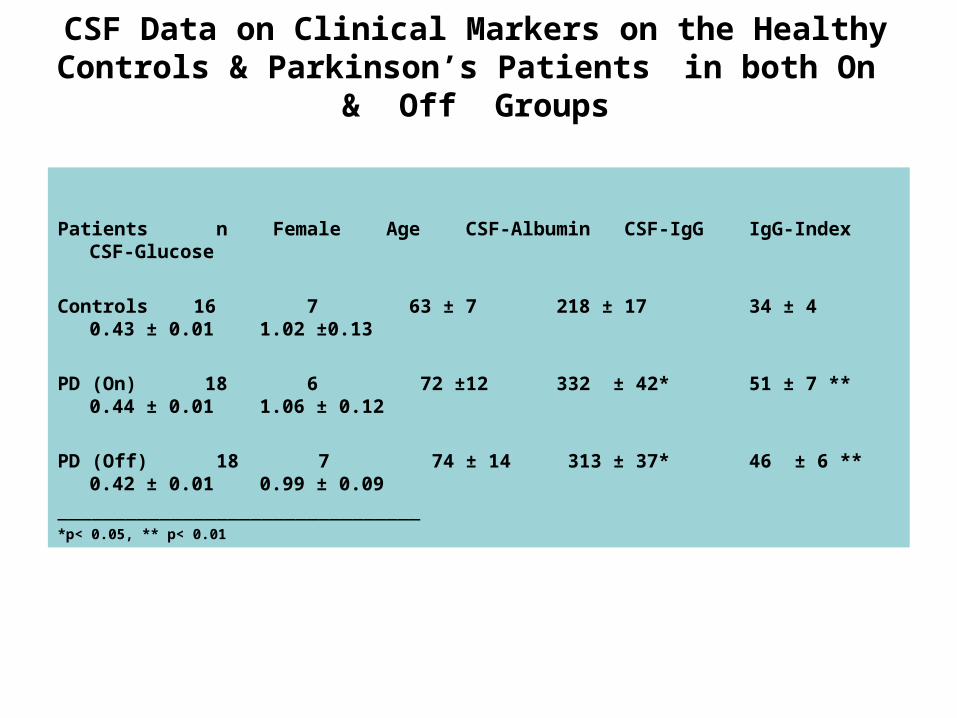
Patients n Female Age CSF-Albumin CSF-IgG IgG-Index CSF-Glucose
Controls 16 7 63 ± 7 218 ± 17 34 ± 4 0.43 ± 0.01 1.02 ±0.13
PD (On) 18 6 72 ±12 332 ± 42* 51 ± 7 ** 0.44 ± 0.01 1.06 ± 0.12
PD (Off) 18 7 74 ± 14 313 ± 37* 46 ± 6 ** 0.42 ± 0.01 0.99 ± 0.09
________________________________*p< 0.05, ** p< 0.01
CSF Data on Clinical Markers on the Healthy Controls & Parkinson’s Patients in both On & Off Groups
Direct and Indirect Pathways in Basal Ganglia
• GABA • Glutamate• Dopamine• Acetylcholine• Adenosine• Neuropeptide
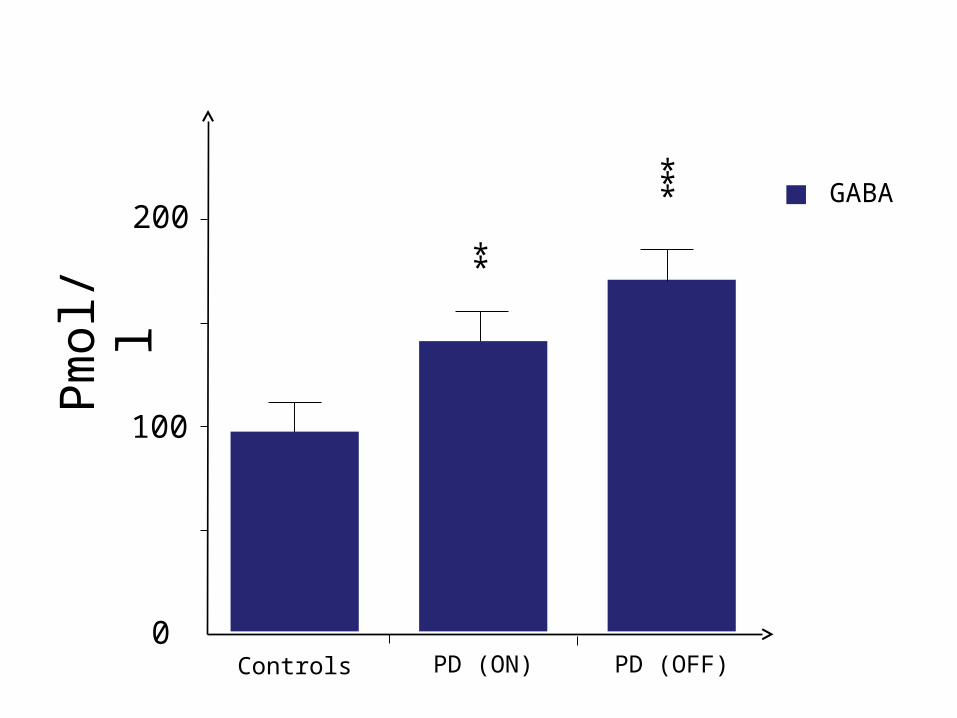
Controls PD (ON) PD (OFF)
**
***
100
200
0
Pm
ol/l
GABA
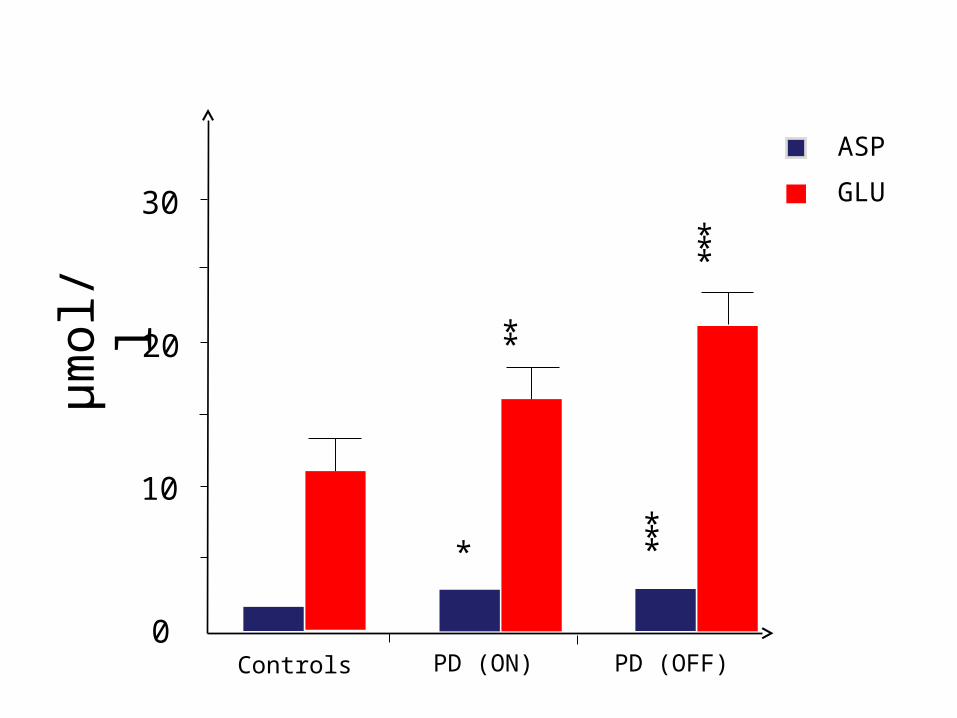
Controls PD (ON) PD (OFF)
**
***
10
20
0
µm
ol/l
GLU
****
30
ASP

Controls PD (ON) PD (OFF)
**
100
200
0
Pm
ol/l
DOPACHVA
DA
300
***
*
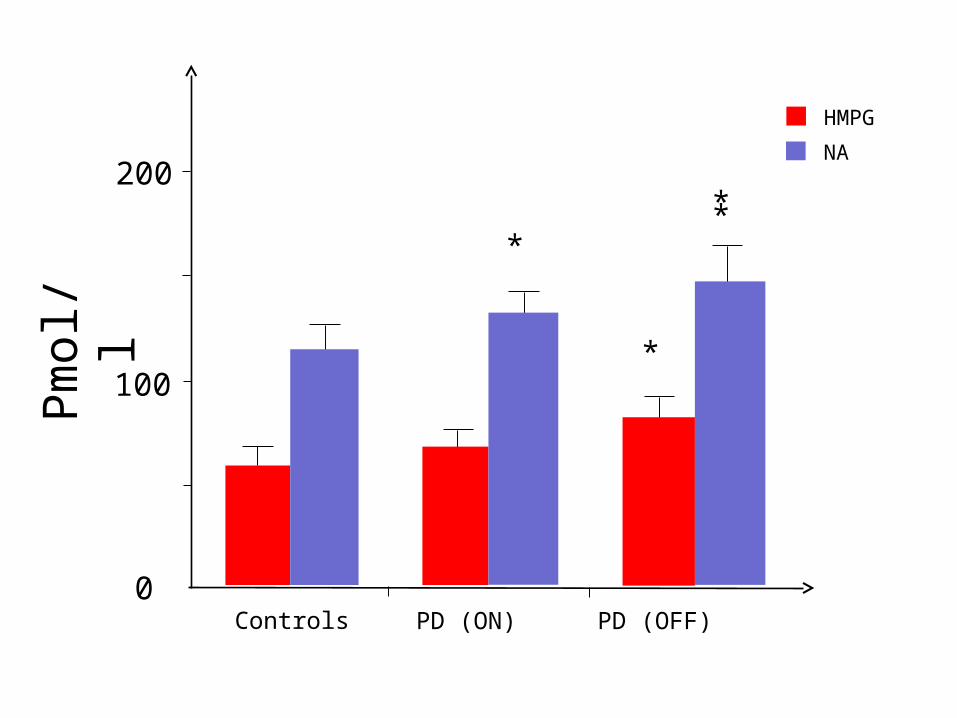
Controls PD (ON) PD (OFF)
**
100
200
0
Pm
ol/l
HMPG
NA
*
*
Controls PD (ON) PD (OFF)
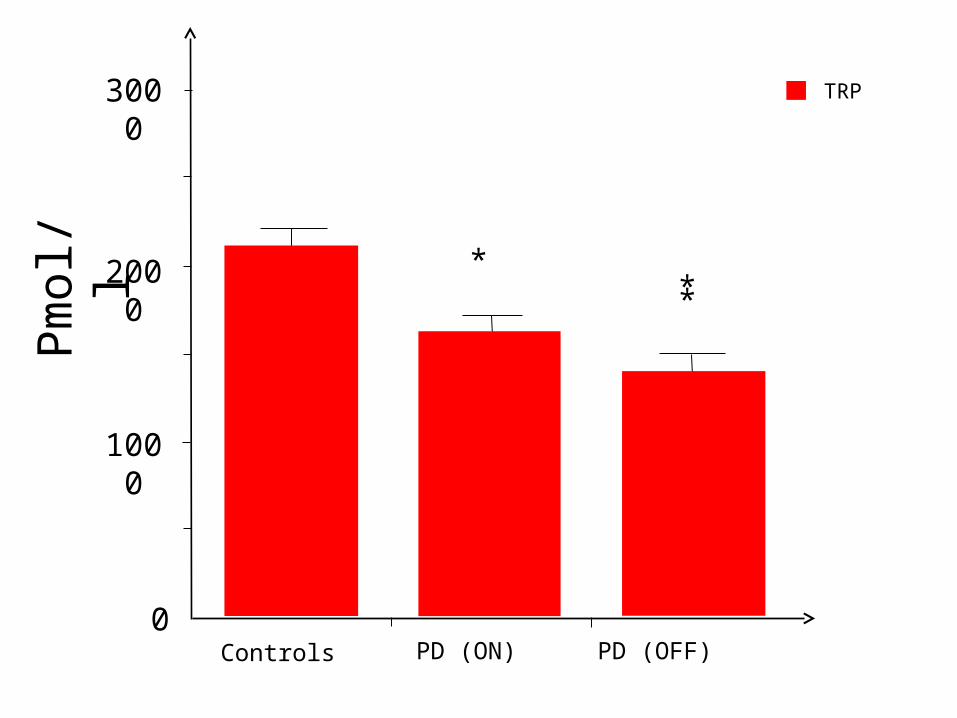
**
1000
2000
0
Pm
ol/l
TRP3000
*
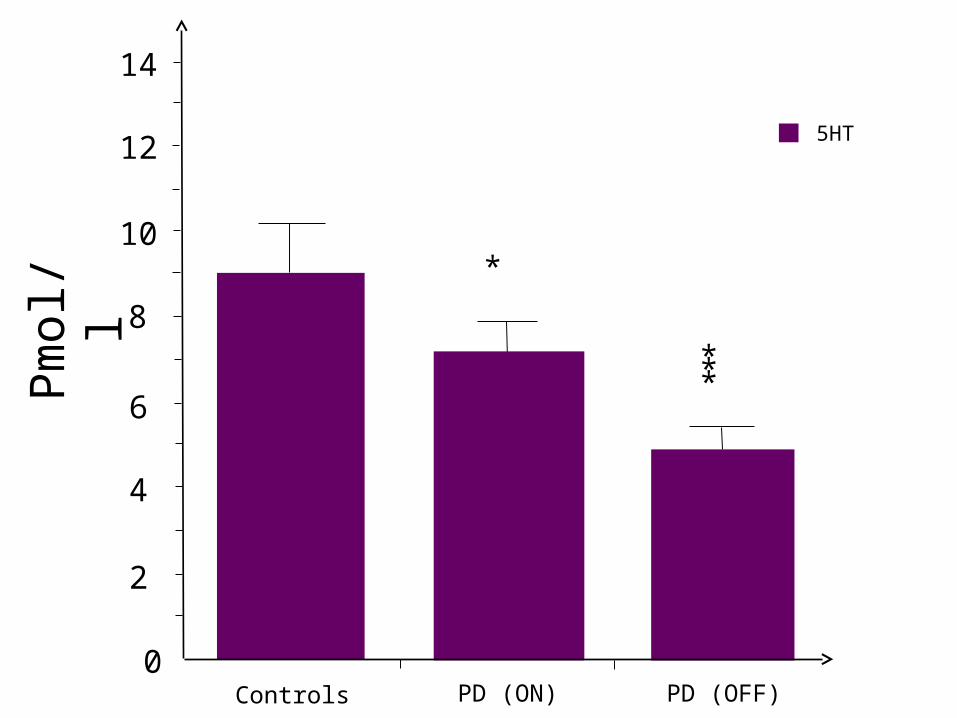
Controls PD (ON) PD (OFF)
***
2
8
0
Pm
ol/l
5HT
*
4
6
10
12
14
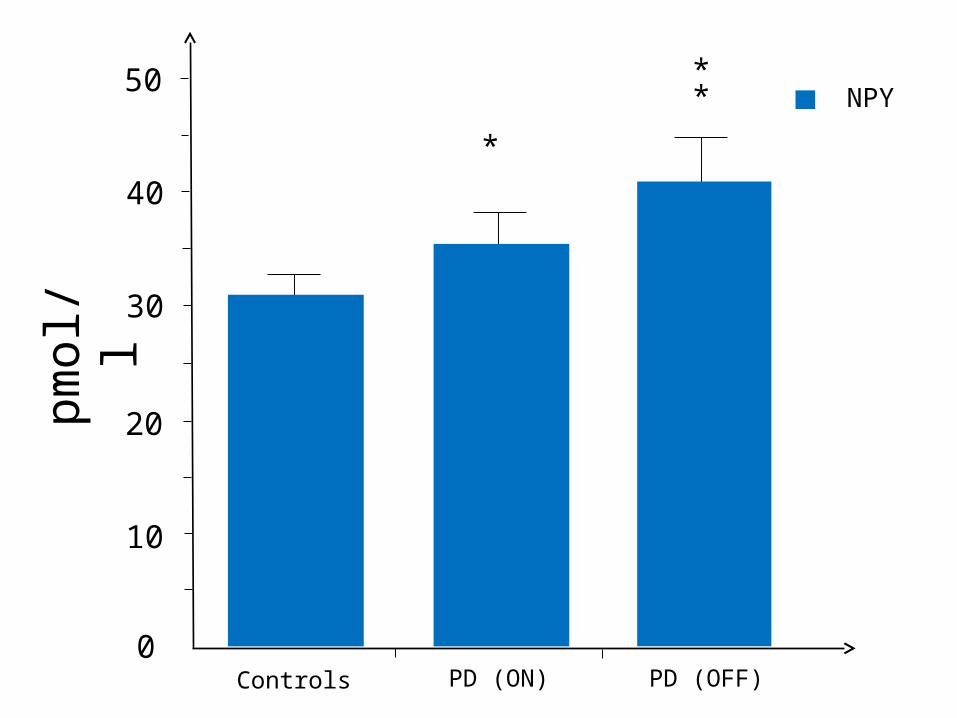
Controls PD (ON) PD (OFF)
*
**
10
0
pmol
/lNPY
20
30
50
40
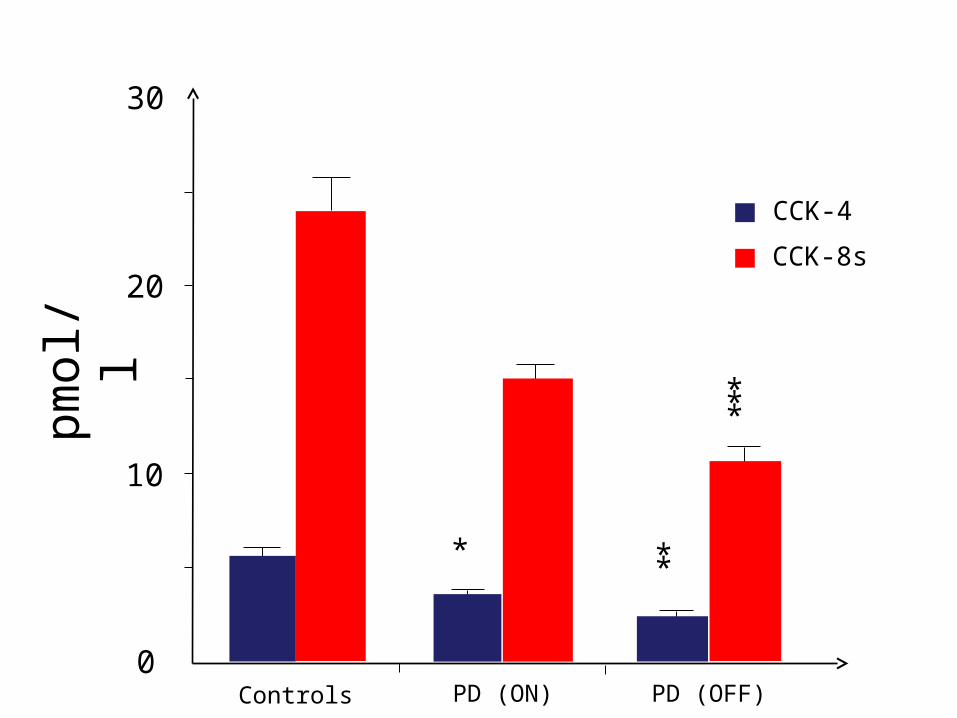
Controls PD (ON) PD (OFF)
**
10
20
0
pmol
/l
CCK-8s
*
***
30
CCK-4

CSF NeuropeptidesSubstance-P during PD-on & PD-off
pmol
/l
0
1
2
3
4
5
Controls PD (ON) PD (OFF)
Substance P***
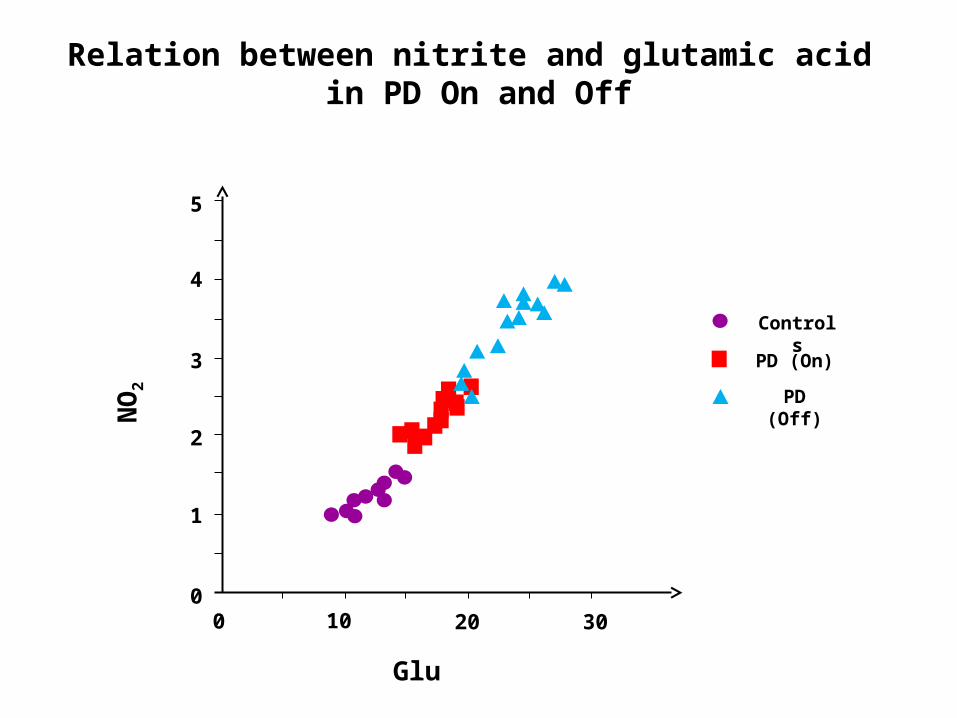
NO
2
Glu
1
2
3
4
5
00 10 20 30
Relation between nitrite and glutamic acid in PD On and Off
PD (Off)
PD (On)
Controls
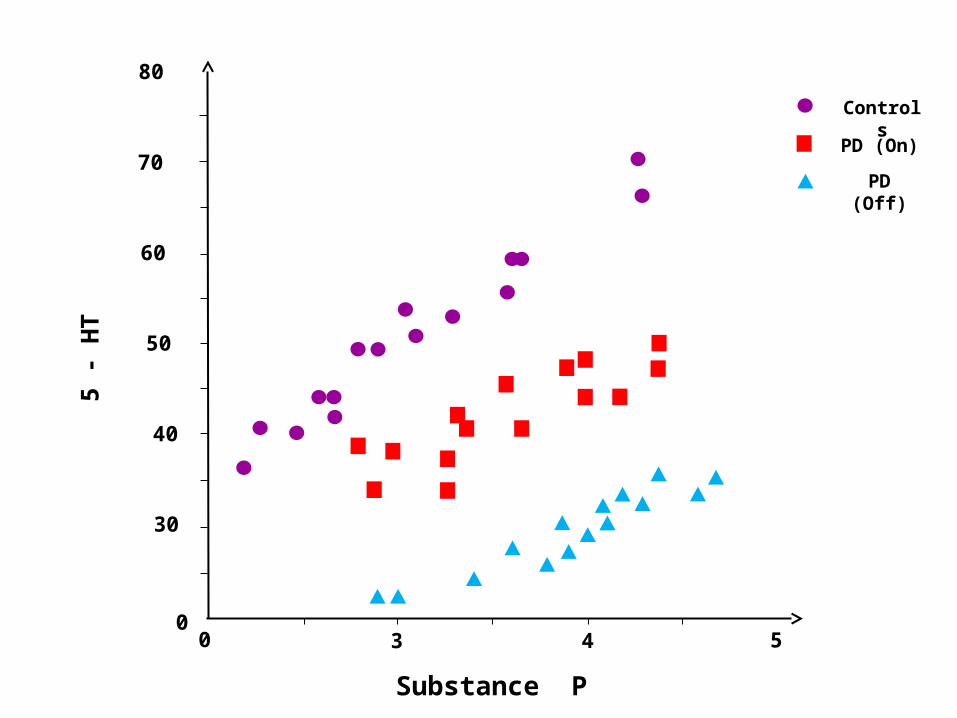
5 -
HT
30
40
50
60
70
00 3 4
PD (Off)
PD (On)
Controls
Substance P
5
80
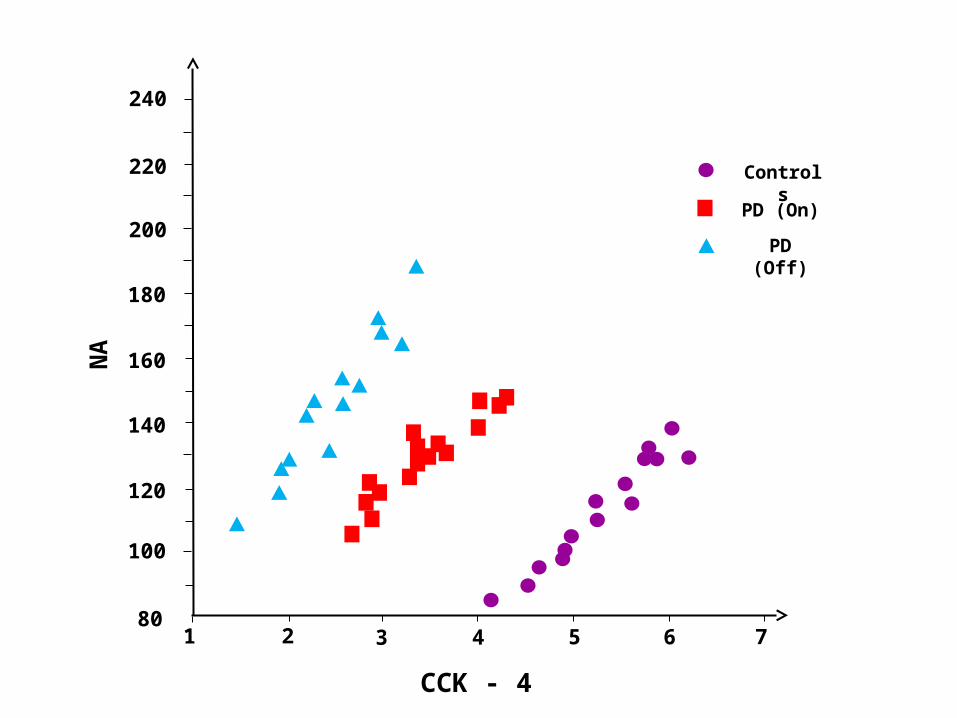
NA
100
180
801 3 4
PD (Off)
PD (On)
Controls
CCK - 4
72 5 6
120
140
160
200
220
240

HC
1
2
00 1
Cobalamin deficiency and its dynamic impact on neurotoxicity and oxidative stress
PD (Off)
PD (On)
Controls
2 3 4
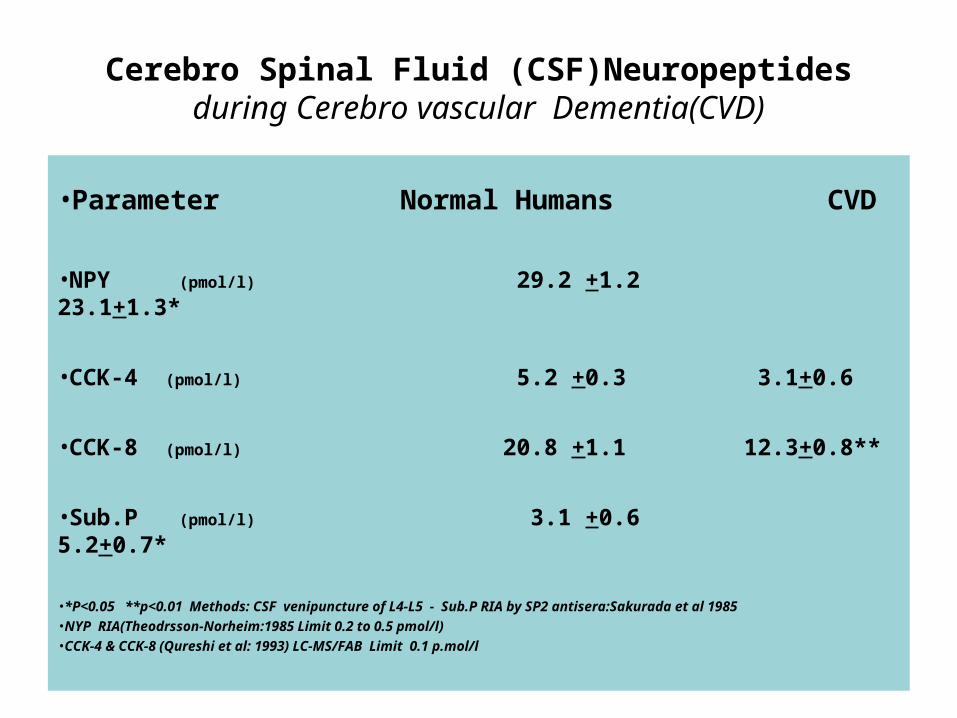
Cerebro Spinal Fluid (CSF)Neuropeptidesduring Cerebro vascular Dementia(CVD)
•Parameter Normal Humans CVD
•NPY (pmol/l) 29.2 +1.2 23.1+1.3*
•CCK-4 (pmol/l) 5.2 +0.3 3.1+0.6
•CCK-8 (pmol/l) 20.8 +1.1 12.3+0.8**
•Sub.P (pmol/l) 3.1 +0.6 5.2+0.7*
•*P<0.05 **p<0.01 Methods: CSF venipuncture of L4-L5 - Sub.P RIA by SP2 antisera:Sakurada et al 1985•NYP RIA(Theodrsson-Norheim:1985 Limit 0.2 to 0.5 pmol/l)•CCK-4 & CCK-8 (Qureshi et al: 1993) LC-MS/FAB Limit 0.1 p.mol/l
Synthesis of NO
Arginine NADPH NADP+
N-w-Hydroxyarginine
ARGININE SYTHASE
Citrulline + NO
Nitric acid

Free Radicals as Markers of Oxidative stress
a) Most of the free radicals are unstable species and can extract an electron from neighbouring molecuiles leading to oxidative stress
b) Oxygen-centered free radicals are the main radicals formed in cells such as OH; O2; H2O2, NO.
c) Free radical causes Protein, DNA, Lipid damage

Controls PD (ON) PD (OFF)
**
***
1
0
µm
ol/l
NO2
2
3
4

CSF Levels of Homocysteine & Vitamin B12in Controls, PD/ON & PD/OFF Stages
Patients Homocysteineµmol/l
Vitamin B12µmol/l
Controls 1.1 +0.1 0.08+0.006
PD (On) 1.56+0.130.06+0.005*
PD (Off) 1.89+0.210.041+0.003**
*P> 0.05 ** p>0.01
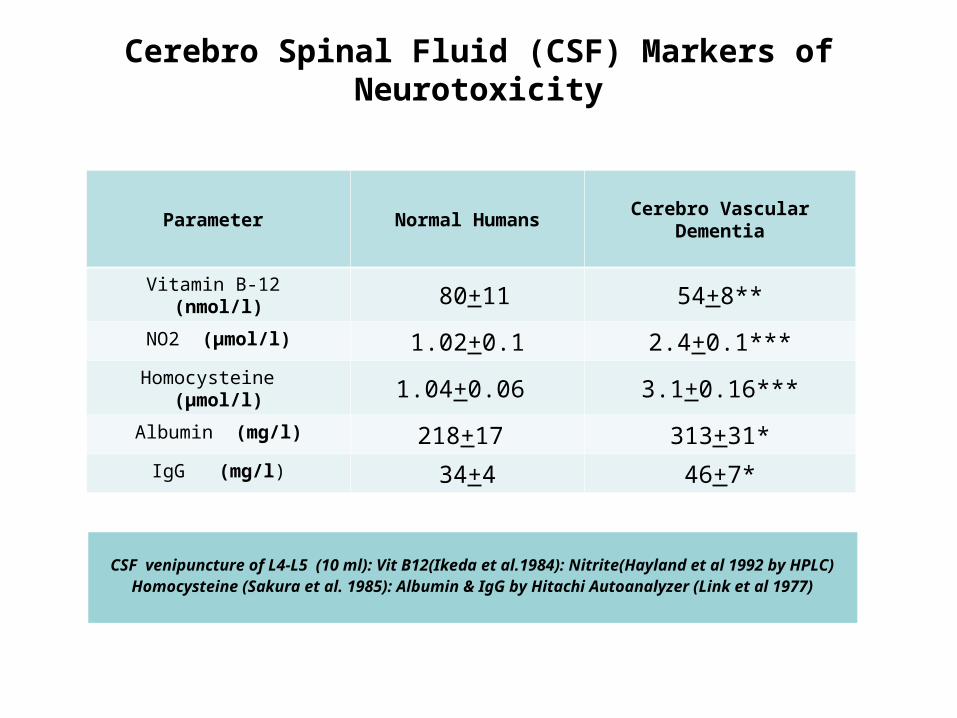
Cerebro Spinal Fluid (CSF) Markers of Neurotoxicity
CSF venipuncture of L4-L5 (10 ml): Vit B12(Ikeda et al.1984): Nitrite(Hayland et al 1992 by HPLC)Homocysteine (Sakura et al. 1985): Albumin & IgG by Hitachi Autoanalyzer (Link et al 1977)
Parameter Normal Humans Cerebro Vascular Dementia
Vitamin B-12 (nmol/l) 80+11 54+8**
NO2 (µmol/l) 1.02+0.1 2.4+0.1***Homocysteine (µmol/l) 1.04+0.06 3.1+0.16***
Albumin (mg/l) 218+17 313+31*
IgG (mg/l) 34+4 46+7*
Neuropeptides & Neuroprotective Role in Health & Disease
-Neuropeptides are mostly Neurohormonal secretions
-Neuropeptides triger & activate central/peripheral feedbacs
-Neuropeptide Concentration decreases significantly during diseases such as PD, AD, CVD but in
-Autoimmune diseases such as MS Neuropeprtide Concentration rises
-Such a discrimination shows that the patients of established Autoimmune Diseases try to activate their Immune response by producing higher levels of Neuropeptides for better resistance to neuropathologies.
-Neuropeptide activation of Adrenal Cortex produces Hyperglycaemic Pool of Epinephrine, Norepinephrine & also Cortisol etc which is ready to mobilize energy reserves to confront and adjust againstNeuronal Injury & start of Neurological Disease.
Dynamic Levels of METAL IONS in Cerebrospinal Fluid (CSF) during Parkinson’s Disease : On/OFF Phenomena
• The Role of Iron
• Copper
• Zinc
• And their Effects
• In On/Off Parkinson’s Patients
• On l-dopa therapy
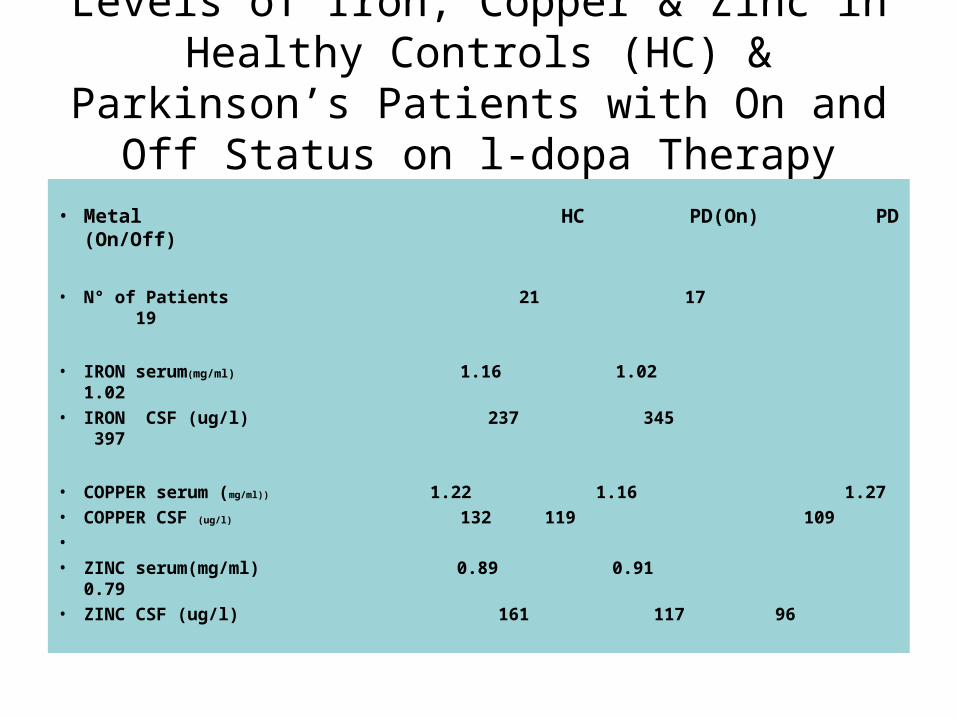
Levels of Iron, Copper & Zinc in Healthy Controls (HC) & Parkinson’s Patients with
On and Off Status on l-dopa Therapy
• Metal HC PD(On) PD (On/Off)
• N° of Patients 21 17 19
• IRON serum(mg/ml) 1.16 1.02 1.02
• IRON CSF (ug/l) 237 345 397
• COPPER serum (mg/ml)) 1.22 1.16 1.27
• COPPER CSF (ug/l) 132 119 109
•
• ZINC serum(mg/ml) 0.89 0.91 0.79
• ZINC CSF (ug/l) 161 117 96
Metal Ions & Neurodegeneration
B R A I NHigh Lipid Content Metal Ion Catalyzed
Formation of Reactive Oxygen Species & Oxidative Damage by H2O2
DNA adduct formation & Protein Damage or Transformation of PrP(sc) to Patho PrP27-30
Iron Induced overproduction of OH radical in Striatum & Brain Stem in Iron Loaded Mice
Iron Loaded Mice are highly prone to MPTP induced ParkinsonismIron induces Neuronal Apoptosis not directly but through its triggering action to
produce highly toxic free radicals : Any change in Iron homeostasis can lead to neurnal injury with a start of
neurodegenerative disease

a) Increase in Oxidative stress due to accumulation of free radicals
b) Increase neurotoxicity in the form of elevated Homocysteine and Glutamic acid
c) Deficiency of Vitamin B12
d) Change in enzyme activities
e) Decrease of number of receptors as can be seen in PD
Mechanism of Neurodegeneration
All these events one way or other contribute in degeneration of brain function

THANK YOU AGAIN
For your kind attention
Parvez, S. H., Collin, C., Qureshi, G.A. & Parvez, S.





























