Embed Size (px)
Citation preview
CLINICAL FEATURES AND OUTCOME OF INFECTION IN SYSTEMIC LUPUS ERYTHEMATOSUS
Mary Kiernan and Barry Bresnihan
Department of Rheumatology, St. Vincent's Hospital, Elm Park, Dublin 4.
Summary INFECTION has now become the most
frequent cause of death in systemic lupus erythematosus. Seven patients were seen in a 4 year period who de- veloped infections requiring admission to hospital. Severe infections generally occurred early in the course, of the dis- ease. Despite intensive antibiotic ther- apy only 3 patients survived. Death was associated with corticosteroid dosage, azathioprine therapy, the severity of anaemia, and with the occurrence of septicaemia. In this study neither the occurrence of infection nor a fatal out- come were associated with features of active disease. It is concluded that pat- ients with systemic lupus need regular monitoring, even when disease is we.ll controlled, so as to minimise dosages of corticosteroids and immunosuppressive drugs and prevent the. occurrence of fatal infections.
Introduction Systemic lupus erythematous (SLE)
is an autoimmune disease of uncertain aetiology. The immunological abnormal- ities include defective cellular immunity (Horwitz and Cousar, 1975; Paty et al, 1975; Bresnihan and Jasin, 1977; Fauci et al, 1978). In addition, several disord- ers of polymorphonuclear leukocyte function have been described (Brandt and Hedberg, 1969; Slinger et ai, 1981). It has long been recognised that these abnormalities predispose patients to infection (Urowitz et al, 1976; Ginzler et al, 1978; Karsh et al, 1979). The require- ment for intensive immunosuppressive
382
therapy in some patients further in- creases the risk of infection (Lee et al, 1976; Urowitz et al, 1976; Ginzler et al, 1978; Karsh et al, 1979). Not surpris- ingly, therefore, sepsis has been re.por- ted as a major cause of death in several series (Dubois et al, 1974; Rosner et al, 1982). In recent years a relatively large number of patients with SLE have been referred to the rheumatology department at St. Vincent's Hospital, Dublin. The clinical features, treatment and outcome of those patients who developed life- threatening sepsis have been studied.
Methods Case notes of patients with SLE refer-
red to the rheumatology department, St. Vincent's Hospital, Dublin, since 1978 were examined and those who had major episodes of sepsis were identified. SLE was diagnosed according to the criteria of the American Rheumatism Associa- tion (Cohen eta / , 1971). Major sepsis was defined as a febrile illness charac- terised by clinical features of infection requiring admission to hospital. Some patients were under the direct care. of the rheumatology department and some were admitted to other specialist depart- ments. However, all had been seen and assessed by one of the authors (BB). Details of previous and current disease and treatment, and bacteriological feat- ures were noted.
Results Seven patients with episodes of sepsis
were identified. The clinical and labora- tory features which were noted at first
Vol. 152 Number 10
Systemic lup{ts erythematosus
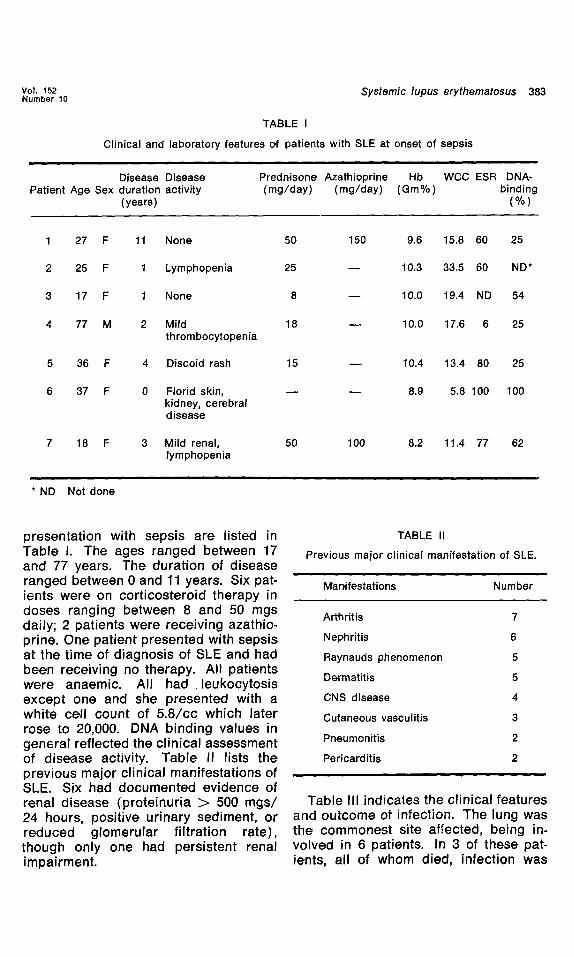
TABLE I
Clinical and laboratory features of patients with SLE at onset of sepsis
383
Disease Disease Patient Age Sex duration activity
(years)
Predn,isone Azathioprine Hb WCC ESR DNA- (mg/day) (mg/day) (Gin%) binding
(%)
1 27 F 11 None 50 150 9.6 15.8 60 25
2 25 F 1 Lymphopenia 25 - - 10.3 33.5 60 ND*
3 17 F 1 None 8 - - 10.0 19.4 ND 54
4 77 M 2 Mild 18 - - 10.0 17.6 6 25 thrombocytopenia
5 36 F 4 Discoid rash 15 - - 10.4 13.4 80 25
6 37 F 0 Florid skin, - - - - 8.9 5.8 100 100 kidney, cerebral disease
7 18 F 3 Mild renal, 50 100 8,2 11.4 77 62 lymphopenia
* ND Not done
presentation with sepsis are listed in Table I. The ages ranged between 17 and 77 years. The duration of disease ranged between 0 and 11 years. Six pat- ients were on corticosteroid therapy in doses ranging between 8 and 50 mgs daily; 2 patients were receiving azathio- prine. One patient presented with sepsis at the time of diagnosis of SLE and had been receiving no therapy. All patients were anaemic. All had leukocytosis except one and she presented with a white cell count of 5.8/cc which later rose to 20,000. DNA binding values in general reflected the clinical assessment of disease activity. Table II lists the previous major clinical manifestations of SLE. Six had documented evidence of renal disease (proteinuria > 500 mgs/ 24 hours, positive urinary sediment, or reduced glomerular filtration rate), though only one had persistent renal impairment.
TABLE II
Previous major clinical manifestation of SLE.
Man,ifestations Number
Arthritis 7
Nephritis 6
Raynauds phenomenon 5
Dermatitis 5
CNS disease 4
Cutaneous vasculitis 3
Pneumonitis 2
Pericarditis 2
Table III indicates the clinical features and outcome of infection. The lung was the commonest site affected, being in- volved in 6 patients. In 3 of these pat- ients, all of whom died, infection was
384 Kiernan and Bresn;han I.J.M.S. October, 1983
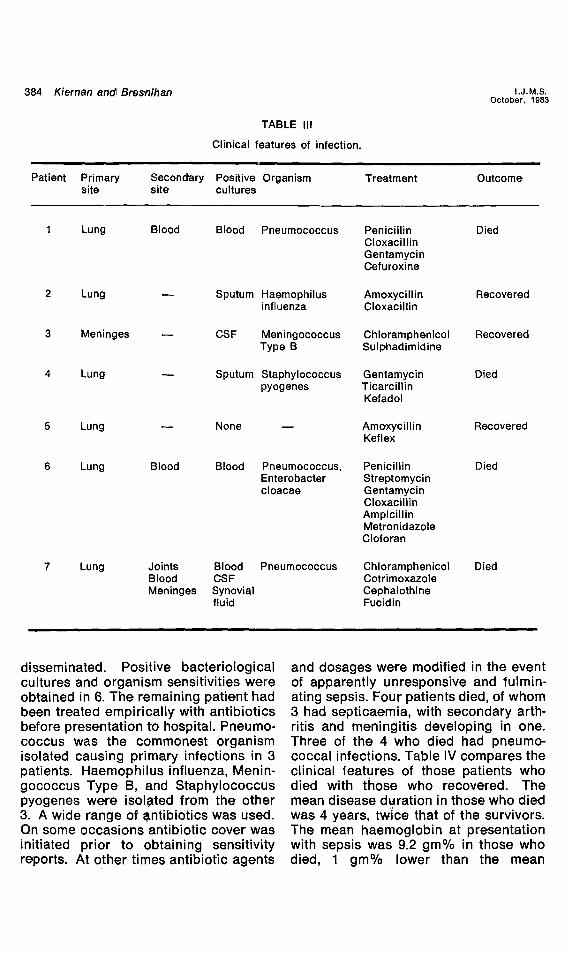
TABLE III
Clin,ical features of infection.
Patient Primary Secondary Positive Organism Treatment Outcome site site cultures
1 Lung Blood Blood Pneumococcus Penicillin Died Cloxacill in Gentamycin Cefuroxine
2 Lung - - Sputum Haemophilus Amoxycil l in Recovered influenza Cloxacill in
3 Meninges - - CSF Meningococcus Chloramphenicol Recovered Type B Sulphadimidine
4 Lung - - Sputum Staphylococcus Gentamycin Died pyogenes Ticarcillin,
Kefadol
5 Lung - - None - - Amoxycill in Recovered Keflex
6 Lung Blood Blood Pneumococcus, Penicillin Died Enterobacter Streptomycin cloacae Gentamycin
Cloxacill in Ampicil l in Metronidazole Cloforan
7 Lung Joints Blood Pneumococcus Chloramphenicol Died Blood CSF Cotrimoxazole Meninges Synovial Cephalothine
fluid Fucidin
disseminated. Positive bacteriological cultures and organism sensitivities were obtained in 6. The remaining patient had been treated empirically with antibiotics before presentation to hospital. Pneumo- coccus was the commonest organism isolated causing primary infections in 3 patients. Haemophilus influenza, Menin- gococcus Type B, and Staphylococcus pyogenes we,re isolated from the other 3. A wide range of ~ntibiotics was used. Qn some occasions antibiotic cover was initiated prior to obtaining sensitivity reports. At other times antibiotic agents
and dosages were modified in the event of apparently unresponsive and fulmin- ating sepsis. Four patients died, of whom 3 had septicae.mia, with secondary arth- ritis and meningitis developing in one. Three of the 4 who died had pneumo- coccal infections. Table IV compares the clinical features of those patients who died with those who recovered. The mean disease duration in those who died was 4 years, twice that of the survivors. The mean haemoglobin at presentation with sepsis was 9.2 gm% in those who died, 1 gm% lower than the mean
Vol. 152 Number 10 Systemic I~pus erythematosus 385
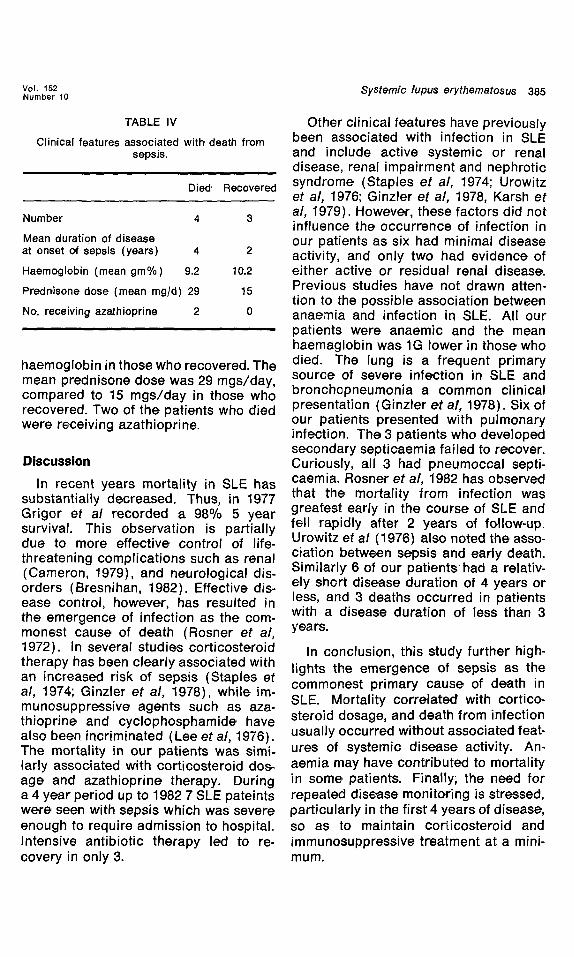
TABLE IV
Clin,ical features associated with death from sepsis.
Died' Recovered
Number 4 3
Mean duration of disease at onset of sepsis (years) 4 2
Haemoglobin (mean gm%) 9.2 10.2
Prednisone dose (mean rag/d) 29 15
No. receiving azathioprine 2 0
haemoglobin in those who recovered. The mean prednisone dose was 29 mgs/day, compared to 15 mgs/day in those who recovered. Two of the patients who died were receiving azathioprine.
Discussion
In recent years mortality in SLE has substantially decreased. Thus, in 1977 Grigor et al recorded a 98% 5 year survival. This observation is partially due to more effective control of life- threatening complications such as renal (Cameron, 1979), and neurological dis- orders (Bresnihan, 1982). Effective dis- ease control, however, has resulted in the emergence of infection as the com- monest cause of death (Rosner et al, 1972). In several studies corticosteroid therapy has been clearly associated with an increased risk of sepsis (Staples et al, 1974; Ginzler et al, 1978), while im- munosuppressive agents such as aza- thioprine and cyclophosphamide, have also been incriminated (Lee et al, 1976). The mortality in our patients was simi- larly associated with corticosteroid dos. age and azathioprine therapy. During a 4 year period up to 1982 7 SLE pateints were seen with sepsis which was severe enough to require admission to hospital. Intensive antibiotic therapy led to re- covery in only 3.
Other clinical features have previously been associated with infection in SLE and include active systemic or renal disease, renal impairment and nephrotic syndrome (Staples e t a / , 1974; Urowitz et al, 1976; Ginzler et al, 1978, Karsh et al, 1979). However, these factors did not influence the occurrence of infection in our patients as six had minimal disease activity, and only two had evidence of either active or residual renal disease. Previous studies have not drawn atten- tion to the possible association between anaemia and infection in SLE. All our patients were anaemic and the. mean haemaglobin was 1G lower in those who died. The lung is a frequent primary source of severe infection in SLE and bronchcpneumonia a common clinical presentation (Ginzler e t at, 1978). Six of our patients presented with pulmonary infection. The 3 patients who developed secondary septicaemia failed to recover. Curiously, all 3 had pneumoccal septi- caemia. Rosner et al, 1982 has observed that the mortality from infection was greatest early in the course of SLE and fell rapidly after 2 years of follow-up. Urowitz et al (1976) also noted the asso- ciation between sepsis and early death. Similarly 6 of our pat ients had a relativ- ely short disease duration of 4 years or less, and 3 deaths occurred in patients with a disease, duration of less than 3 yea rs.
In conclusion, this study further high- lights the emergence of sepsis as the commonest primary cause of death in SLE. Mortality correlated with cortico- steroid dosage, and death from infection usually occurred without associated feat- ures of systemic disease activity. An- aemia may have contributed to mortality in some patients. Finally; the need for repeated disease monitoring is stressed, particularly in the, first 4 years of disease, so as to maintain cori icosteroid and immunosuppressive treatment at a mini- mum.
386 Kiernan and Bresnihan I.J.M.S. October, 1983
References
Brandt, L., Hedberg, M. 1969. Impaired phagocy- cytosis by peripheral blood granulocytes in systemic lupus erythematosus. Scand. J. Haemat. 6, 348-353.
Bresnihan, B., Jasin, H. E. 1977. Suppressor func- tion of peripheral blood mononuclesr cells in normal individuals and in patients with syst- emic lupus erylhematosus. J. Clin. Invest. 59, 106-116.
Bresnihan, B. 1982. CNS lupus. Clin. Rheum. Dis. 8, 183-195.
Cameron, J. S. 1979. The nephritis of systemic lupus erythematosus. In Progress in Glomerul- onephritis. P. Kincaid-Smith, A. J. K. d"Apice, R. C. Atkins. 387-423. John Wiley, New York.
Cohen, A. S., Reyn.olds, W. E., Franklin, E. C., Ku.lka, J. P., Ropes, M. W., Shulman, L. E. and Wallace, S. L. 1971. Preliminary criteria for the classification of systemic lupus erythematosus. Bull. Rheum. Dis. 21, 643-648.
Dubois, E. L., Wierzchowiecki, M., Cox, M. and Weiner, J. M. 1974. Duration, and death in systemic lupus erythematosus. An analysis of 249 cases. J.A.M.A. 227, 1399-1402.
Fauci, A. S., Steinberg, A. D., Haynes, B. F. and Whalen, G. 1978. Immunoregulato,ry aberrations in systermic lupu6 erythematosus. J. Immunol. 121, 1473-1478.
Ginzler, E., Diamondl, H., Kaplan, D., Weiner, M., Schlesinger, M'. and, Selen,znick, M. 1978. Com- puter analysis of factors influencing frequency of infection, in systemic lupus erythematosus. Arthritis Rheum. 21, 37-44.
Ginzler, E., Diamond,, H., Weiner, M., Schlesinger, M., Fries, J. K., Washer, C., Medsger, T. A., Ziegler, G., Klippel, J. H., Had,ler, M'. N., Albert, D. A., Hess, E. V., Spencer-Green, G., Grayzel, A., Worth, D,., Hahr~, B. H. and Barnett, E. V. 1982. A Multi-Centre study of outcome in, sys- temic lupus erythematosis. 1. Entry variables
as predictors of prognosis. Arthritis Rheum. 25, 601-611.
Grigor, R., Edmonds, J., Leukonia, R., Bresnihan, B. and Hughes, G. R. V. 1978. Systemic lupus erythematosus. Am. J. Med. 58, 829-835.
Karsh, J. Klippel, J. H., Balow, J. E. and Decker, J. L. 1979. Mortality in lupus nephritis. Arthritis Rheum. 22, 764-769.
Lee, P., Urowitz, B. M., Bookman,, A. A. M., Koehler, B. E., Smythe, H. A., Gordon, D. A. and Ogryzlo, M. A. 1977. A review of 110 cases with reference to nephritis, the nervous system, infections, aseptic necrosis and prognosis. Quart. J. Med'. 46, 1-32.
Paty, J. G., Sien.knecht, C. W., Townes, A. S., Hanissuian, A. S., M'iller, J. B. and, Masi, T. 1975. impaired, cell-mediated' immunity in sys- temic lupus erythematosus. Am. J. Meal. 59, 769-778.
Rosner, S., Ginzler, E., Diamond, H. S., Weiner, M., Schlesinger, M., Fries, J. F., Wasner, C., Medsger, T. A., Ziegler, G., Klippel, J. H., Had; ler, A. M., Albert, D. A., Hess, E. V., Spencer- Green,, G., Grayzel, A., Worth, D., Hahn, B. H. and Barnett, E. V. 1982. A Multi-Centre study of outcome in' systemilc lupus erythematosus. I1. Causes of death. Arthritis Rheum. 25, 612- 617.
Shingu, M., Todoroki, T., Sakal, K. and Nobunaga, M. 1981. Suppression, of Fc receptor and C4.C3 receptors of the grar~ulocytes from patients with systemic lupus erythematosus. J. Rheum- atology. 8, 9,10-916.
Staples, P. H., Gerding, D. N., Decke, J. L. and Gordor~, R. S. 1974. Incidence of infection in systemic lupus erythematosus. Arthritis Rheum. 17, 1-10.
Urowitz, B. M., Bookman, A. A. M., Koehler, B. E., Gordon,, D. A., Smythe, H. A. and Ogryzlo, M. A. 1976. The bimodal mortality pattern of sys- temic lupus erythematosus. Am. J. Med. 60, 221-225.













