Embed Size (px)
Citation preview

Neuro-Ophthalmology, 29:9–15, 2005Copyright ©c Taylor & Francis Inc.ISSN: 0165-8107DOI: 10.1080/01658100490900719
ORIGINAL PAPER
Clinical Heterogeneity of Hereditary OpticAtrophy in a Turkish Family
Golge AcarogluDepartment ofNeuro-Ophthalmology, SocialSecurity Eye Hospital, Ankara,Turkey
Yasemin AlanayDivision of Genetics,Department of Pediatrics,Hacettepe University Schoolof Medicine, Ankara, Turkey
Pascal Reynier andPatrizia Amati-BonneauINSERM E0018, Laboratoryof Biochemistry and MolecularBiology, CHU d’Angers,Angers, France
Gamze MenDepartment of Retina, SocialSecurity Eye Hospital, Ankara,Turkey
ABSTRACT Purpose: To present detailed clinical findings of a Turkish familyfrom central Anatolia with a hereditary form of optic atrophy. Design: Observa-tional case series. Material and methods: A detailed family history of a patient withoptic atrophy revealed similarly affected family members. Nine members of thisconsanguineous family were evaluated. The OPA1 gene of seven of the nine in-dividuals was screened for mutations using direct DNA sequencing. Results: Nomutation was found in the OPA1 gene. Four females were clinically affected,two of whom had previous diagnoses of glaucoma. Affected family membersdemonstrated abnormal findings in at least one of the following: optic disk, vi-sual field, or color vision. Myopia, oblique insertion of the optic nerve, marginalpigmentation of the optic nerve head, and entry and exit anomalies of centralretinal vessels were additional findings. Conclusion: This family demonstrates ahighly variable expression of a form of hereditary optic atrophy, ranging fromasymptomatic involvement to legal blindness. It is important for doctors tolook for subtle but typical optic disk, visual field, and color vision anomaliesin asymptomatic members when screening such families.
KEYWORDS Hereditary optic neuropathy; autosomal dominant optic atrophy; autosomalrecessive optic atrophy; OPA1 gene
INTRODUCTIONWe present a consanguineous Turkish family with hereditary optic atrophy,
showing broad clinical heterogeneity and subtle clinical findings in asymp-tomatic members.
MATERIALS AND METHODSA 32-year-old woman with a previous diagnosis of normal tension glaucoma
(NTG) was referred because she continued to lose vision despite medical ther-apy. Her maternal grandfather had lost his vision in midlife. The woman wasrelated to her husband, whose mother had been known to have ‘glaucoma’.Her daughter was having visual difficulty. Her brother was also married to arelative who had had low vision since childhood. An illustrative pedigree isshown in Figure 1. The proband’s husband, daughter, son, brother, sister-in-law,niece, and nephew (Patients 2-8, respectively) were examined. Her mother-in-law
Accepted 8 October 2004.
Correspondence and reprint requeststo: Golge Acaroglu M.D., AngoraEvleri, Masal Sokak E 3/2, 06530,Beysukent, Ankara, Turkey.E-mail: [email protected]
9
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
11/0
1/14
For
pers
onal
use
onl
y.

FIGURE 1 The patients in the pedigree are numbered as they are in the text. The proband is marked with an X, the examined familymembers with an asterisk. Males are indicated by squares, females by circles. A deceased person is indicated by a slash. Affectedpersons are shaded; asymptomatic ones have white centers and symptomatic ones do not. The diamond box indicates there were fourmore children in this family, sex unspecified.
(Patient 9) refused to be brought to the clinic so a sum-mary of her chart was retrieved from another institution.Clinical findings are summarized in Table 1.
After obtaining informed consent, peripheral wholeblood samples were collected from seven of the fam-ily members (excluding mother-in law [Patient 9] andinfant [Patient 8]). The samples were stored at -20◦Cand genomic DNA was extracted from leukocytes ac-cording to the method described by Miller et al.1 Thirtyprimer couples were used in the polymerase chain reac-tion (PCR) to amplify the 30 encoding exons, includingthe intron-extron junctions of the OPA1 gene.2 Thepurified PCR products were directly sequenced usinga Ceq2000 DNA sequencer (CEQ DTCS-Quick StartKit, Beckman Coulter, Fullerton, CA, USA).
RESULTSAlthough the mode of inheritance could not be
clearly established (as is frequently the case in familieswith consanguinity), affected family members had someclinical features compatible with autosomal dominantoptic atrophy (ADOA). Genetic analysis, however, didnot show any mutations in the OPA1 gene.
Case ReportsPatient 1
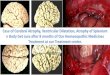
A 32-year-old woman presented with a progressivedecrease in vision. She had been previously diagnosedwith NTG and was started on Latanoprost 0.005%.Her visual acuities were 20/25 OD and 20/70 OS.Intraocular pressures were 10 mmHg OU. There wasno relative afferent pupillary defect. Cup-to-disk ra-tios were 0.5/0.7. Her left disk had a shallow temporal
cup with accompanying rim pallor and sharp bor-ders (Fig. 2). Automated perimetry showed bilateraldouble arcuate scotomas, sparing central vision. Sheidentified four of 12 Ishihara pseudoisochromatic (IP)plates. The Farnsworth-Munsell (F-M) 100 hue test re-vealed a blue-yellow (tritan) axis. A compressive or de-myelinating process was eliminated by normal mag-netic resonance imaging of the optic nerves. She deniedany systemic disease, toxic substance abuse, or hearingdifficulty.
Other Patients
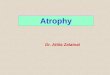
Patients 1, 3, 6, and 9 were symptomatic. Patient 3(daughter) had -3.5 D (OU) myopia. Asymmetrical cup-ping with temporal triangular pallor of the optic disks,visual field defects, and tritanopic axes of color visionloss were almost identical in the mother and daughter.Patient 6 had high myopia with astigmatism: −15.00(−1.50 × 38) OD and −15.75 (−1.75 × 117) OS. Dueto the severely tilted disks, it was difficult to define thecup borders. There were large areas of peripapillary at-rophy and one disk had a vein exiting at its edge (Fig. 3).This patient also had generalized color vision loss andconstricted visual fields. Patient 9 had ‘primary openangle glaucoma,’ as stated in her chart, and had under-gone trabeculectomies OU. Her intraocular pressureswere currently normal. Her optic disks were pale withcup-to-disk ratios of 0.8/0.8 and visual acuity levels ofcounting fingers OU.
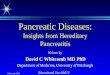
Patients 2, 4, 5, and 7 were asymptomatic. These pa-tients had excellent visual acuities and could identify allIP plates. All of them had wedge-shaped rim pallor of atleast one optic disk. Patients 2 and 4 (husband and son,respectively) had tritanopia when tested with the F-M100 hue test. The son also had paracentral scotomas
G. Acaroglu et al. 10
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
11/0
1/14
For
pers
onal
use
onl
y.

TAB
LE1
Su
mm
ary
of
Clin
ical
Fin
din
gs
Pati
ent
Ag
e(y
ears
)B
est-
corr
ecte
dvi
sual
acu
ity
Co
lor
VIs
hih
ara
Co
lor
VF-
M10
0V
isu
alfi
eld
s/fi
eld
def
ects
Op
tic
cup
c/d
Tem
po
ral
neu
rore
tin
alri
mar
eaan
dN
FLO
ther
ocu
lar
asso
ciat
ion
s
1Pr
ob
and
(Fem
ale)
3220
/25
20/7
04/
124/
12Tr
itan
OU
:Co
nst
rict
ed,d
ou
ble
arcu
ate
sco
tom
as0.
5D
eep
0.7
Shal
low
OU
:Dif
fuse
NFL
loss
Tem
po
ralp
allo
rO
S>
OD
NTG
2H
usb
and
4220
/20
20/2
012
/12
12/1
2M
ildtr
itan
OD
:BB
S,u
pp
erte
mp
ora
lsco
tom
as0.
3Sh
allo
w0.
5Sh
allo
wO
D:D
isc
edg
ear
tery
OS:
Wed
ge-
shap
edp
allo
r,o
bliq
ue
inse
rtio
n,
OD
:Dis
ced
ge
arte
ryO
S:O
bliq
ue
inse
rtio
n
per
ipap
illar
ycr
esce
nt
3D
aug
hte
r16
20/7
0(−
3.50
)20
/40
(−3.
50)
0/12
0/12
Trit
anO
U:C
on
stri
cted
OD
:Par
acen
tral
sco
tom
a
0.5
Shal
low
0.7
Shal
low
OU
:Lo
caliz
edN
FLlo
ssO
S:Pi
gm
ente
dri
mTe
mp
ora
lpal
lor
OS>
OD
Myo
pic
asti
gm
atis
m
4So
n14
20/2
020
/20
12/1
212
/12
Trit
anO
S:Pa
race
ntr
alsc
oto
ma
0.3
0.4
OS:
Wed
ge-
shap
edp
allo
ran
dp
igm
ente
dri
m5
Bro
ther
3020
/20
20/2
012
/12
12/1
2N
OS:
Sub
tle
par
acen
tral
sco
tom
a0.
40.
4O
S:W
edg
e-sh
aped
pal
lor
—
6Si
ster
-in
-law
3020
/200
(−12
.0)
20/1
00(−
12.0
)6/
126/
12G
ener
aliz
edlo
ss(U
nre
liab
le)
Co
nst
rict
edo
nco
nfr
on
tati
on
NA
OU
:Tilt
edd
iscs
,lar
ge
area
so
fp
erip
apill
ary
atro
ph
yan
dp
igm
ent
Hig
hm
yop
iaA
stig
mat
ism
Am
bly
op
iad
istu
rban
ce,d
iffu
seN
FLlo
ssO
D:P
igm
ente
dri
mO
S:D
isc
edg
eve
in
Tilt
edd
iscs
Dis
ced
ge
vein
7N
iece
720
/20
20/2
012
/12
12/1
2—
No
rmal
on
con
fro
nta
tio
n0.
5Sh
allo
w0.
6Sh
allo
wO
S:W
edg
e-sh
aped
pal
lor
OU
:Dis
ced
ge
vein
san
dar
teri
esD
isc
edg
ear
teri
esan
dve
ins
8N
eph
ew1
Fix-
follo
w(O
U)
NA
NA
NA
N,S
ymm
etri
c.N
(OU
)—
9M
oth
er-i
n-l
aw*
82C
FC
F—
——
0.8
0.8
Tota
lop
tic
atro
ph
yN
TG?
F-M
100,
Farn
swor
th-M
unse
ll10
0hu
ete
st;
NFL
,ne
rve
fiber
laye
r;O
U,
both
eyes
;O
D,
right
eye;
OS,
left
eye;
NTG
,no
rmal
tens
ion
glau
com
a;BB
S,bi
gbl
ind
spot
;N
A,
not
appl
icab
le;
N,
norm
al;
CF,
coun
ting
finge
rs.
11
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
11/0
1/14
For
pers
onal
use
onl
y.

FIGURE 2 Asymmetrical cupping and temporal triangular pallor of the optic disks in Patient 1 (proband).
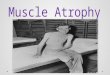
(Fig. 4) and there was dark pigmentation in the atrophicneuroretinal rim of his left eye. Patient 2 had a nasal diskedge artery in the right eye. His right visual field had abig blind spot and superotemporal isolated scotomas.An obliquely inserted left optic disk had wedge-shapedtemporal rim pallor and a peripapillary pigmented cres-cent. Patient 5 had the mildest clinical findings. A subtleleft paracentral scotoma could only be detected by staticthreshold perimetry. Patient 7 had big disks with wideshallow cups. There were major retinal vessels enteringand exiting at the disk margins (Fig. 5).
DISCUSSIONFamilies such as this are not rare in the rural parts
of Turkey since marriages between family members areusually arranged by the parents to prevent the split-ting up of their land. A hereditary disease, therefore,
FIGURE 3 Appearance of optic nerve heads in a myopic patient (Patient 6).
is very likely to present itself in the offspring of subse-quent generations. Inheritance may be autosomal dom-inant or recessive, becoming more prevalent as thecosanguineous marriages continue.
Recessive optic atrophies usually present early inlife with profound visual deficit and nystagmus. Thevast majority of these atrophies are seen in associa-tion with multisystem diseases.3,4 There are very fewreports of isolated primary recessive optic atrophy andsome authors believe that many of these cases arevariants of ADOA with partial penetrance.5 None ofour family members had ptosis, nystagmus, or oph-thalmoplegia. Moreover, none reported neurologicaldysfunction or hearing loss. The infant (Patient 8)was normal and there was no history of anyone af-fected in the first decade of life. However, both theproband’s marriage and that of her brother were con-sanguineous and had affected progeny, as is frequently
G. Acaroglu et al. 12
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
11/0
1/14
For
pers
onal
use
onl
y.

the case in families with recessive transmission andconsanguinity.
Some features of the clinical findings in this family,namely temporal disk pallor with a triangular area oftemporal excavation and the tritanopic axis on the F-M100 hue test, could be attributable to ADOA, whichis estimated to be the most common hereditary opticneuropathy.3,4,6−8 The ADOA gene (OPA1) has beenlocalized to the 3q28-qter region of chromosome 3.9,10
Despite its dominant mode of inheritance, it has vari-able expression within families and the detection rate
(A)
FIGURE 4 (A) Tritanopic color vision defect in an asymptomatic patient (Patient 4). (B) Paracentral scotomas in Patient 4. (Continued)
of OPA1 gene mutations by direct sequencing is re-ported to be 47–89%.11,12 Previous studies have sug-gested no genetic heterogeneity.13 However, one pedi-gree has been reported that maps to the OPA4 locus onchromosome 18.14 There are also families showing noevidence of linkage to either of these chromosomes.9,12
Moreover, a Turkish ADOA family without OPA1-OPA2 mutations has been reported.15
Complete screening of OPA1 found no mutationsor base-pair changes in seven affected members. Thismay be caused by family mapping to another locus or
13 Hereditary Optic Atrophy
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
11/0
1/14
For
pers
onal
use
onl
y.

(B)
FIGURE 4 (Continued)
by a large deletion that could not be detected by ourPCR-based approach. It is also possible that the familyrepresents a new as yet unmapped genetic locus for arare form of isolated recessive optic atrophy.
Peripheral visual fields of our symptomatic patientswere more affected than their central visual fields. This
FIGURE 5 Non-glaucomatous cupping and disk margin vessels in Patient 7.
is interesting when previous glaucoma diagnoses areaddressed. Patients sharing phenotypic characteristicsof both ADOA and NTG have been reported.16 Re-cent genetic linkage analysis of patients with NTG hasshown an association with polymorphisms of the OPA1gene.17 The phenotypes of Patients 1 and 3 (mother
G. Acaroglu et al. 14
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
11/0
1/14
For
pers
onal
use
onl
y.

and daughter) are unique combinations of the two.The positive family history, early age at onset, and tri-tanopic color vision loss can be attributable to ADOA,while the preserved central visual fields and healthy-appearing nasal neuroretinal rim areas are features ofNTG.16
Disks with large non-glaucomatous cups may be con-genitally large or the loss of optic nerve axons may giverise to cupping.18 They may contain a number of diskedge vessels, which is helpful in the differentiation be-tween primary and secondary large cups.19 The cupsmay also seem larger in a myopic eye with oblique in-sertion, as the sloping margins of the disk make it diffi-cult to define the cup borders. Two of our patients hadmyopia and one of them also had tilted disks. One ofthe asymptomatic patients had oblique insertion of theoptic disk. Similar findings were recently reported in ayoung individual.20
One eye had a nasal disk edge artery. Three eyes withlarge cups had disk edge veins that did not have visibleconnections to main vessel trunks. One of these eyesalso had two disk edge arteries in conjunction with diskedge veins, a rarely reported finding.21
According to one study, an incomplete pigment cres-cent within the neuroretinal rim tissue is reported toexist in all ADOA patients.16 Another study foundthe pigment ring in 30% of the optic disks of ADOApatients.22 We also observed this finding in three eyes(30%). Pigmentation of the optic nerve head has beenoccasionally reported in normals, but its significance isunknown.23
CONCLUSIONWe share the common observation that disk pallor
is the most important clinical sign of hereditary opticneuropathies. Other factors of diagnostic importanceare the utilization of the F-M 100 hue test and staticthreshold perimetry to detect mild color vision defectsand define subtle scotomas. Assessment of the varia-tions in optic disk and cup appearance and vasculatureis essential in order to appreciate the non-glaucomatousnature of these disks; however, the possibility of NTGshould be kept in mind.
ACKNOWLEDGEMENTThe authors would like to acknowledge Dr. William
F. Hoyt for his continuous support and offer their grate-
ful thanks for his help during the preparation of themanuscript.
REFERENCES[1] Miller SA, Dykes DD, Polesky HF. A simple salting out procedure
for extracting DNA from human nucleated cells. Nucl Acids Res.1988;16:1215–1220.
[2] Baris O, Delettre C, Amati-Bonneau P, Surget MO, Charlin JF, CatierA, Derieux L, Guyomard JL, Dollfus H, Jonveaux P, Ayuso C, Maume-nee I, Lorenz B, Mohammed S, Tourmen Y, Bonneau D, Malthiery Y,Hamel C, Reynier P. Fourteen novel OPA1 mutations in autosomaldominant optic atrophy including two de novo mutations in sporadicoptic atrophy. Hum Mutat. 2003;21:656–660.
[3] Kerrison JB. Hereditary optic neuropathies. Ophthalmol Clin NorthAm. 2001;14:99–107.
[4] Votruba M, Aijaz S, Moore AT. A review of primary hereditary opticneuropathies. J Inherit Metab Dis. 2003;26:209–227.
[5] Moller HU. Recessively inherited, simple optic atrophy; does it reallyexist? Ophthalmic Pediatr Genet. 1992;13:31–32.
[6] Kjer P. Infantile optic atrophy with dominant mode of inheritance.A clinical and genetic study of 19 Danish families. Acta Ophthalmol.1959; 37(Suppl 54):1–146.
[7] Kline LB, Glaser JS. Dominant optic atrophy. The clinical profile. ArchOphthalmol. 1979;97:1680–1686.
[8] Hoyt CS. Autosomal dominant optic atrophy. A spectrum of disabil-ity. Ophthalmology. 1980;87:245–249.
[9] Eiberg H, Kjer B, Kjer P, et al. Dominant optic atrophy (OPA1) mappedto chromosome 3q region. I. Linkage analysis. Hum Mol Genet.1994;3:977–980.
[10] Kjer B, Eiberg H, Kjer P, Rosenberg T. Dominant optic atrophymapped to chromosome 3q. II. Clinical and epidemiological aspects.Acta Ophthalmol Scand. 1996;74:3–7.
[11] Delettre C, Griffoin JM, Kaplan J, et al. Mutation spectrum andsplicing variants in the OPA1 gene. Hum Genet. 2001;109:584–591.
[12] Thiselton DL, Alexander C, Taanman JW, et al. A comprehensivesurvey of mutations in the OPA1 gene in patients with autosomaldominant optic atrophy. Invest Ophthalmol Vis Sci. 2002;43:1715–1724.
[13] Bonneau D, Souied E, Gerbert S, et al. No evidence of genetic hetero-geneity in dominant optic atrophy. J Med Genet. 1995;32:951–953.
[14] Kerrison JB, Arnould VJ, Ferraz-Sallum JM. Genetic heterogeneity ofdominant optic atrophy, Kjer Type. Identification of a second locuson chromosome 18q12.2–12.3. Arch Ophthalmol. 1999;117:805–810.
[15] Ozden S, Duzcan F, Wollnik B, et al. Progressive autosomal optic at-rophy and sensorineural hearing loss in a Turkish family. OphthalmicGenet. 2002;23:29–36.
[16] Fournier AV, Damji KF, Epstein DL, et al. Disc excavation in domi-nant optic atrophy. Differentiation from normal tension glaucoma.Ophthalmology. 2001;108:1595–1602.
[17] Aung T, Ocaka L, Ebenezer ND, et al. A major marker for normal ten-sion glaucoma: association with polymorphisms in the OPA1 gene.Hum Genet. 2002;110:52–56.
[18] Ambati BK, Rizzo III JF. Nonglaucomatous cupping of the optic disc.Int Ophthalmol Clin. 2001;41:139–149.
[19] Jonas JB, Zach FM, Gusek GC, et al. Pseudoglaucomatous physio-logic large cups. Am J Ophthalmol. 1989;107:141–144.
[20] Buono LM, Foroozan R, Sergott RC. Unexplained visual loss. SurvOphthalmol. 2003;48:626–630.
[21] Barroso L, Hoyt WF, Narahara M. Disc edge veins of Kraupa. Rare exitanomalies of the retinal vein. Br J Ophthalmol. 1992;76:442–443.
[22] Votruba M, Thiselton D, Bhattacharya S. Optic disc morphology ofpatients with OPA1 autosomal dominant optic atrophy. Br J Oph-thalmol. 2003;87:48–53.
[23] Shields MB. Gray crescent in the optic nerve head. Am J Ophthalmol.1980;89:238–244.
15 Hereditary Optic Atrophy
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
11/0
1/14
For
pers
onal
use
onl
y.







![Review Historical overview of hereditary ataxias with an ... · paraplegia [HSP], olivopontocerebellar atrophy [OPCA], ... balance, but without actual loss of power, and apart from](https://img.pdfslide.net/doc/110x75/6086b7a47e0df8319547dcb6/review-historical-overview-of-hereditary-ataxias-with-an-paraplegia-hsp-olivopontocerebellar.jpg)