Embed Size (px)
Citation preview
Interpreting clinical laboratory data
Graeme Vernon
Austin Health Drug Information
Outline
• Clinical pharmacy perspective
• Most common tests
• Case summaries
• Reference
– Jeff Hughes (editor). Case studies in clinical
practice. Use of laboratory test data,
Pharmaceutical Society of Australia, 2004.
Clinical pharmacy approach
• Lab data mainly for diagnostic use
– pharmacists do not diagnose
• Focus on tests relevant to pharmaceutical care
– understanding a diagnosis
– avoiding adverse outcomes from drug therapy
– monitoring therapy
– recognising adverse drug reactions
Normal ranges
• Normal range assumes a Normal distribution of
results
– ‘abnormal’ if > 2 standard deviations from mean
• Reference range
– normal range from a defined population
»hospital population
»pregnant women
»Infants, children
Important tests
• Sodium
• Potassium
• Creatinine
• Liver function
• Blood counts
• Glucose
• Calcium
• Magnesium
Sodium
• Serum levels 135–145 mEq/L
• Extracellular cation
• Osmolality depends on sodium, urea and glucose
concentrations
• Renal excretion
– angiotensin, aldosterone, renin, vasopressin
Hyponatremia
• Mild (125–135 mEq/L)
• More likely to be symptomatic < 125 mEq/L
– headache, lethargy, nausea, dizziness, confusion,
agitation, muscle twitching or cramps, psychosis,
seizures
– cerebral edema, coma (severe hyponatremia only)
Causes of hyponatremia
• Increased extracellular fluid volume (ECF)
– renal failure
– edema treated with diuretics
• Normal ECF
– syndrome of inappropriate antidiuretic hormone (SIADH)
– serum osmolality, urine osmolality, urine sodium
• Reduced ECF
– excess diuresis (renal sodium loss)
– gastrointestinal loss (vomiting, diarrhea)
Drug causes of hyponatremia
• SIADH
– stimulate central ADH release
– e.g. carbamazepine, SSRIs, chlorpromazine
• Increased ADH activity (kidneys)
– NSAIDs, amiloride
• Sodium and water removal
– diuretics
Hypernatremia
• Less common drug-related problem
• Symptoms
– thirst (may dissipate)
– confusion, neuromuscular excitation, seizures,
coma
– depend on rate of sodium rise
Causes of hypernatremia
• Reduced ECF
– diarhea, vomiting, burns, diuretics (sodium loss)
• Normal ECF
– diabetes insipidus (renal water loss due to reduced
ADH release)
– nephrogenic diabetes insipidus
» induced by hypercalcemia or hypokalemia
• Increased ECF
– hypertonic sodium (IV infusions, TPN)
– mineralocorticoids, Cushing’s syndrome
Drug causes of hypernatremia
• Nephrogenic diabetes insipidus
– lithium, foscarnet, amphotericin, demeclocycline
• Renal water loss
– loop diuretics, mannitol, overuse of osmotic laxatives
• Increased renal sodium
– fludrocortisone, corticosteroids
• Inceased body sodium
– hypertonic saline, sodium bicarbonate, sodium salts,
hypertonic saline enemas
Potassium
• Serum levels 3.5–5.0 mEq/L
• Intracellular
– 50–60 mEq (~2%) extracellular
– acute regulation - intracellular flow
»alkalosis, insulin, beta-2 stimulants shilf K into cells
– chronic regulation - renal elimination
Hypokalemia
• Cramping, paralytic ileus, constipation, hypotension, arrhythmias, tetany, muscle paralysis, respiratory failure
• Apparent potassium loss
– metabolic alkalosis, insulin, beta stimulants
• True loss
– reduced intake, GI loss, fluid loss (burns)
– hyperaldosteronism, Cushing’s syndrome
– magnesium deficiency
Drug causes of hypokalemia
• Intracellular shift
– adrenaline, salbutamol
• Renal loss
– thiazide, loop diuretics
– fludrocortisone, carbenoxolone, high-dose glucocorticosteroids
– amphotericin, cisplatin
• GI loss
– laxative abuse
Hyperkalemia
• Signs/symptoms > 6 mEq/L
• Cardiovascular
– hypotension
– ECG changes, bradycardia
– increase risk of digoxin toxicity
• Neuromuscular
– weakness
Drug causes of hyperkalemia
• Increased load
– potassium supplements
• Cellular shift
– beta-blockers, digoxin toxicity
• Reduced renal elimination
– ACE inhibitors, ARAs
– lithium, NSAIDs, amiloride, trimethoprim
Creatinine
• Serum levels (adults)
– 0.3–1.2 mg/dL, 0.03–0.11 mmol/L
• Formed from creatine in the liver
– 98% of creatine present in muscle
• Eliminated mainly by renal filtration
• Serum levels reflect both muscle mass and kidney
function
Creatinine clearance
• Better indicator of renal function
• Calculated from urine creatinine/24 hours
• Estimated from Cockcroft and Gault method
– age, lean body weight, serum creatinine
– (140 - age) x IBW ‚ (72 x serum creatinine in mg/dL)
– valid only for steady state
• Degrees of renal impairment
– mild 50–75 mL/min
– moderate 20–50 mL/min
– severe < 20 mL/min
Liver function tests
• Bilirubin (total)
– < 1 mg/dL (< 20 micromol/L)
• Alkaline phosphatase (ALP) < 120 U/L
– bile duct cells, bone, intestine
• Aspartate aminotransferase (AST) < 45 U/L
– liver cells, heart, kidney, muscles
• Alanine aminotransferase (ALT) < 36 U/L
– mainly liver cells
• Gamma glutamyl transpeptidase (GGT) < 60 U/L
– liver cells (cholestasis, alcohol, drugs)
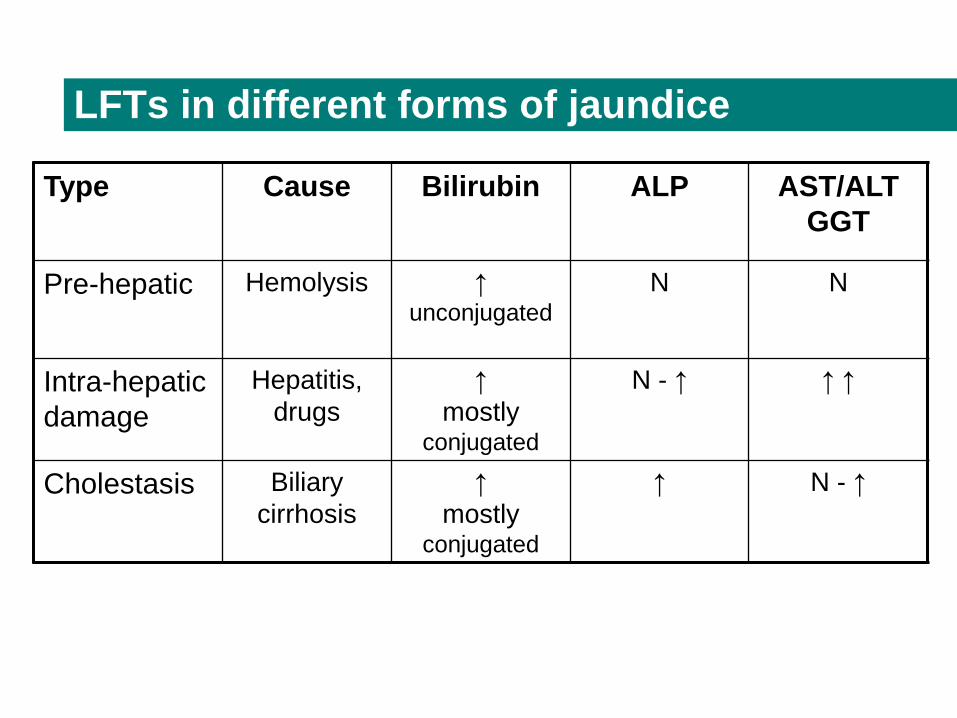
LFTs in different forms of jaundice
Type Cause Bilirubin ALP AST/ALT
GGT
Pre-hepatic Hemolysis ↑unconjugated
N N
Intra-hepatic
damage
Hepatitis,
drugs
↑
mostly conjugated
N - ↑ ↑ ↑
Cholestasis Biliary
cirrhosis
↑
mostly conjugated
↑ N - ↑
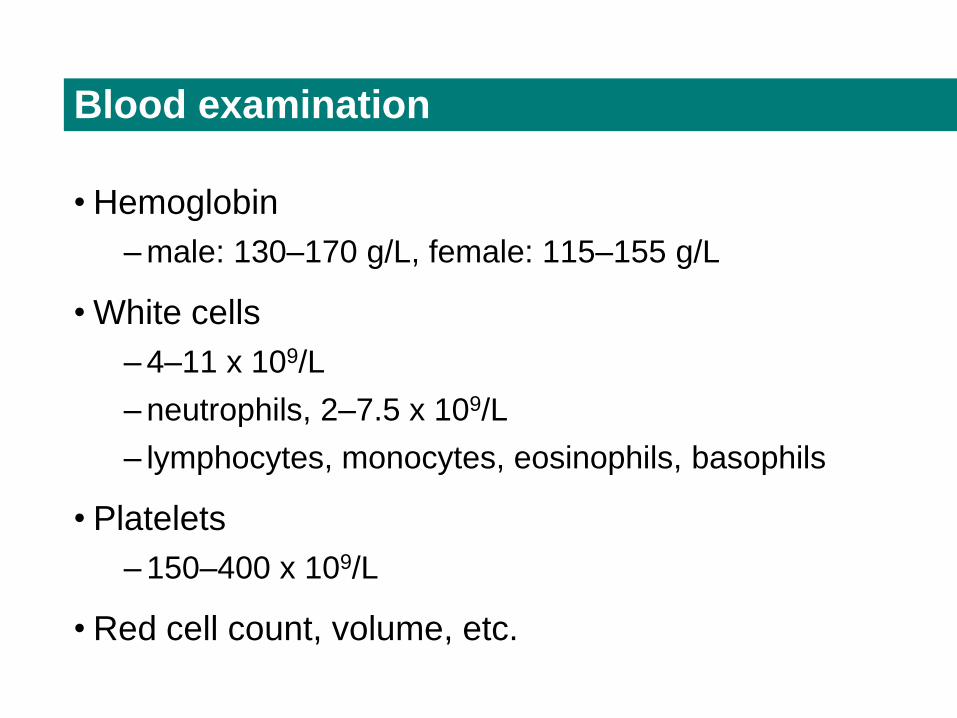
Blood examination
• Hemoglobin
– male: 130–170 g/L, female: 115–155 g/L
• White cells
– 4–11 x 109/L
– neutrophils, 2–7.5 x 109/L
– lymphocytes, monocytes, eosinophils, basophils
• Platelets
– 150–400 x 109/L
• Red cell count, volume, etc.
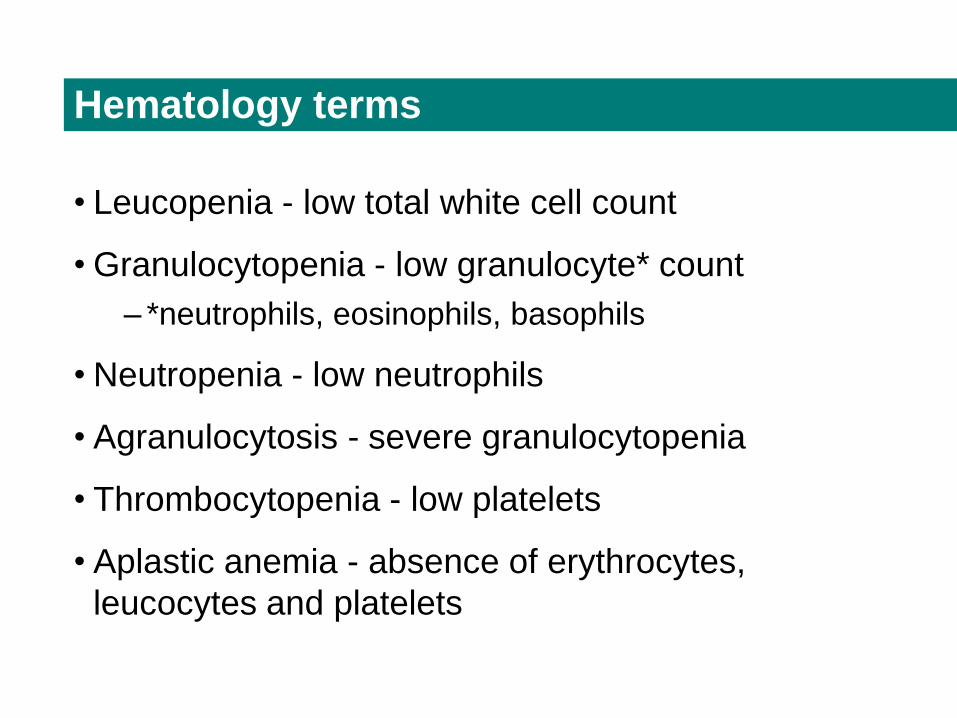
Hematology terms
• Leucopenia - low total white cell count
• Granulocytopenia - low granulocyte* count
– *neutrophils, eosinophils, basophils
• Neutropenia - low neutrophils
• Agranulocytosis - severe granulocytopenia
• Thrombocytopenia - low platelets
• Aplastic anemia - absence of erythrocytes,
leucocytes and platelets
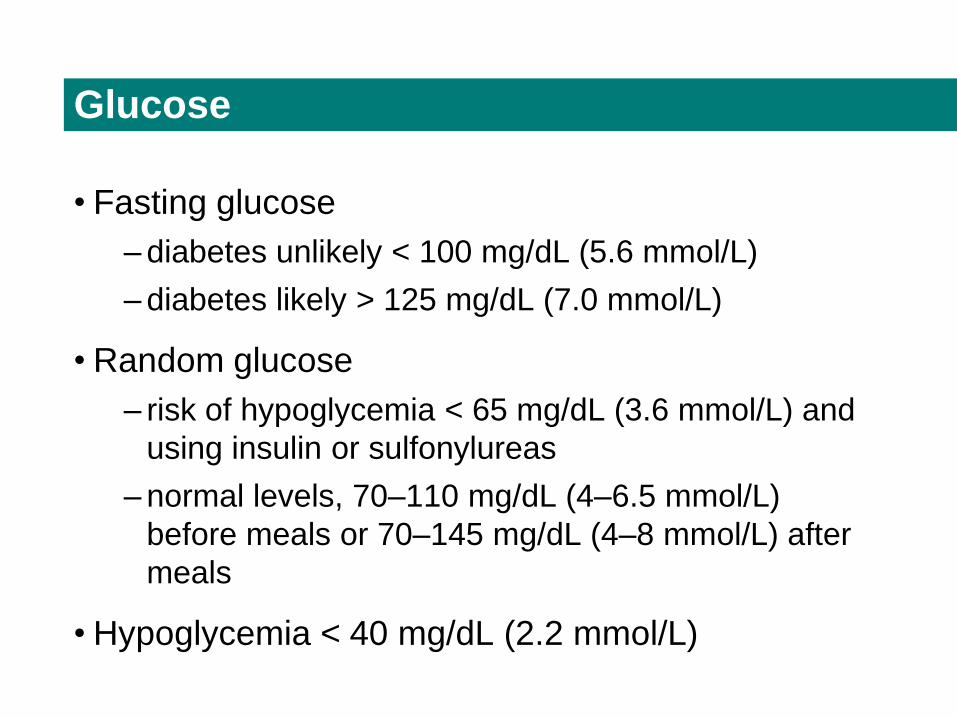
Glucose
• Fasting glucose
– diabetes unlikely < 100 mg/dL (5.6 mmol/L)
– diabetes likely > 125 mg/dL (7.0 mmol/L)
• Random glucose
– risk of hypoglycemia < 65 mg/dL (3.6 mmol/L) and
using insulin or sulfonylureas
– normal levels, 70–110 mg/dL (4–6.5 mmol/L)
before meals or 70–145 mg/dL (4–8 mmol/L) after
meals
• Hypoglycemia < 40 mg/dL (2.2 mmol/L)
Glycolated hemoglobin
• Glycolated = glycosylated hemoglobin (HbA1c)
• Glucose binds slowly to this type of hemoglobin in red blood cells.
• Steady state (formation, decomposition, destruction) with about 3.0 to 6.5% being HbA1c
• Diabetics have higher average blood glucose and therefore a higher proportion of HbA1c
• Indication of mean BGL over previous 4–8 weeks
– aim for 7% or less
Calcium
• Serum 8.4–10 mg/dL (2.1–2.6 mmol/L)
– adjust for calcium binding to albumin
» increased serum concentration of ionised (active) calcium
with low albumin levels
– Ca (corrected) =
Ca (measured) + [(4.0 - albumin) x 0.8]
where albumin concentration is in g/dL
Hypocalcemia
• Corrected serum calcium < 8.4 g/dL (2.1 mmol/L)
– Finger numbness, paresthesia, tetany and muscle
cramps
– CNS depression, confusion, hallucinations,
seizures
– ↓ myocardial contractility; arrhythmias,
bradycardia, hypotension
Hypercalcemia
• Corrected serum calcium > 10 g/dL (2.55 mmol/L)
– symptoms > 11 g/dL (2.85 mmol/L)
» life threatening > 14 g/dL (3.5 mmol/L)
– weight loss, vomiting
– muscle fatigue, lethargy, coma
– psychosis
– ↓ renal function
Magnesium
• Serum 1.4–2.0 mEq/L (0.7–1.0 mmol/L)
• Hypomagnesemia < 1.4 mEq/L (0.7 mmol/L)
– ↑ muscle reflexes, cramps
– disorientation, psychosis, seizures
– arrhythmias
Hypermagnesemia
• Serum magnesium > 2 mEq/L (1.0 mmol/L)
– 2–4 mEq/L (1–2 mmol/L)
»vomiting, skin flushing, weakness, ↓ consciousness
– 3.4–5.0 mEq/L (1.7–2.5 mmol/L)
» loss of tendon reflexes, muscle weakness
– 5.0–6.0 mEq/L (2.5–3.0 mmol/L)
»hypotension, vasodilation
– 8.0-10 mEq/L (4.0–5.0 mmol/L)
»arrhythmias (inc. AF)
– > 10 mEq/L (5.0 mmol/L)
»asytole, heart block, ventricular failure, coma, death
Case studies
• Acute renal failure
• Hyponatremia
• Jaundice
• Aplastic anemia
• DVT treatment





























