Embed Size (px)
Citation preview
CLINICAL PHARMACOLOGY OF
ROCURONIUM BROMIDEJerrold H. Levy, MD
Professor of AnesthesiologyEmory University School of Medicine
Division of Cardiothoracic Anesthesiology and Critical CareEmory HealthcareAtlanta, Georgia
CLINICAL PHARMACOLOGY OF
ROCURONIUM BROMIDEJerrold H. Levy, MD
Professor of AnesthesiologyEmory University School of Medicine
Division of Cardiothoracic Anesthesiology and Critical CareEmory HealthcareAtlanta, Georgia
HISTORICAL PERSPECTIVES OF NEUROMUSCULAR BLOCKING
AGENTS
HISTORICAL PERSPECTIVES OF NEUROMUSCULAR BLOCKING
AGENTS
INTRODUCTION OF NEW DRUGS1494 - 1942 Curare1947 - 1951 Succinylcholine chloride, Gallamine,
Metocurine, Decamethonium1960’s Alcuronium1970’s Pancuronium bromide, Fazadinium1980’s Vecuronium bromide, Atracurium besylate1990 Pipecuronium bromide1991 Doxacurium chloride1992 Mivacurium chloride1994 Rocuronium bromide1999 Rapacuronium bromide
INTRODUCTION OF NEW DRUGS
Succinylcholine chloride, Gallamine, Metocurine, Decamethonium
Pancuronium bromide, FazadiniumVecuronium bromide, Atracurium besylatePipecuronium bromideDoxacurium chlorideMivacurium chlorideRocuronium bromideRapacuronium bromide
STRUCTURAL CLASSES OF NONDEPOL.ARIZING RELAXANTS
• Steroids: Rocuronium bromide, Vecuronium bromide, Pancuronium bromide, Pipecuronium bromide
• Naturally occurring benzylisoquinolones: curare, metocurine
• Benzylisoquinoliniums: Atracurium besylate, Mivacurium chloride, Doxacurium chloride
STRUCTURAL CLASSES OF NONDEPOL.ARIZING RELAXANTS
Steroids: Rocuronium bromide, Vecuronium bromide, Pancuronium bromide, Pipecuronium bromide
Naturally occurring benzylisoquinolones: curare,
Benzylisoquinoliniums: Atracurium besylate, Mivacurium chloride, Doxacurium chloride
THE IDEAL RELAXANT
• Nondepolarizing• Rapid onset• Dose-dependent duration• No side-effects• Elimination independent of organ function• No active or toxic metabolites
THE IDEAL RELAXANT
dependent duration
Elimination independent of organ functionNo active or toxic metabolites
ONSET OF PARALYSIS IS AFFECTED BY:
• Dose (relative to ED• Potency (number of molecules)• Keo (chemistry/blood flow)• Clearance• Age
ONSET OF PARALYSIS IS AFFECTED BY:
Dose (relative to ED95)Potency (number of molecules)
(chemistry/blood flow)
PHARMACODYNAMICS OF ROCURONIUM BROMIDE
PHARMACODYNAMICS OF ROCURONIUM BROMIDE
ONSET OF ROCURONIUM BROMIDE
Onset: rapid to intermediate(dose dependent)
ONSET OF ROCURONIUM BROMIDE
Onset: rapid to intermediate(dose dependent)
TRACHEAL INTUBATION
Pre-Medication MeperidineAtropine
Induction Propofol toAlfentanil to
Rocuronium bromide 0.6 mg/kg Succinylcholine chloride 1 mg/kgIntubation 60 sec. later
TRACHEAL INTUBATION
Meperidine 1 mg/kgAtropine 0.01 mg/kgPropofol to 2.5 mg/kgAlfentanil to 0.25 mg/kg
Rocuronium bromide 0.6 mg/kg ORSuccinylcholine chloride 1 mg/kg
60 sec. later
ROCURONIUM BROMIDE:TRACHEAL INTUBATION
• Median time to 80% block with 0.6 mg/kg is 60 seconds (0.4
• Median onset time with 0.6 mg/kg is 1.8 minutes (0.6-13 minutes)
ROCURONIUM BROMIDE:TRACHEAL INTUBATION
80% block with 0.6 mg/kg is 60 seconds (0.4-6.0 minutes)Median onset time with 0.6 mg/kg is
13 minutes)
ROCURONIUM BROMIDE:TRACHEAL INTUBATION
• Median time to 80% blockade with 0.45 mg/kg is 78 seconds (0.8minutes)
• Median onset time with 0.45 mg/kg is 3.0 minutes (1.3-8.2 minutes)
ROCURONIUM BROMIDE:TRACHEAL INTUBATION
80% blockade with 0.45 mg/kg is 78 seconds (0.8-6.2
Median onset time with 0.45 mg/kg is 8.2 minutes)
LOW DOSE PHARMACODYNAMICS:CLINICAL PARAMETERS
Mean maximum blockade
Mean time to 80% blockade
Mean time to maximum blockade
Mean time to completion of intubation
LOW DOSE PHARMACODYNAMICS:CLINICAL PARAMETERS
Rocuronium bromideDose: .45 mg/kg (n = 14)
96 ± 5%
117 ± 24 seconds
214 ± 25 seconds
159 ± 25 seconds
ROCURONIUM BROMIDE:TRACHEAL INTUBATION
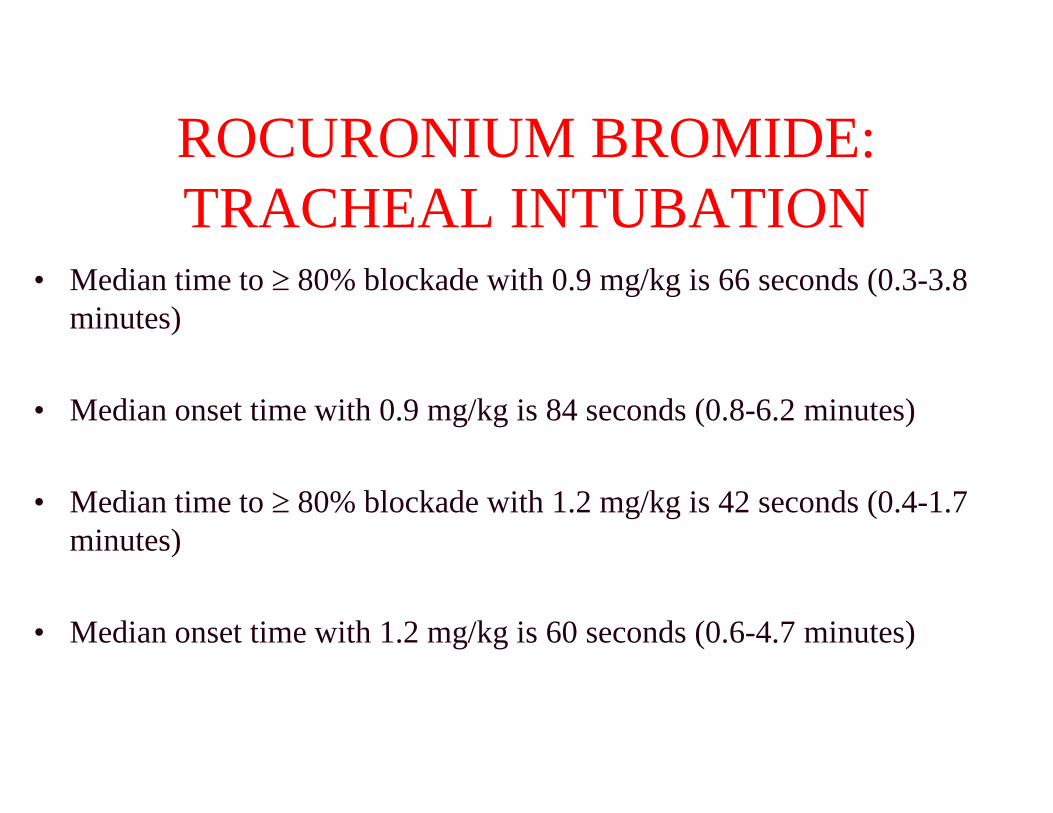
• Median time to 80% blockade with 0.9 mg/kg is 66 seconds (0.3minutes)
• Median onset time with 0.9 mg/kg is 84 seconds (0.8
• Median time to 80% blockade with 1.2 mg/kg is 42 seconds (0.4minutes)
• Median onset time with 1.2 mg/kg is 60 seconds (0.6
ROCURONIUM BROMIDE:TRACHEAL INTUBATION
80% blockade with 0.9 mg/kg is 66 seconds (0.3-3.8
Median onset time with 0.9 mg/kg is 84 seconds (0.8-6.2 minutes)
80% blockade with 1.2 mg/kg is 42 seconds (0.4-1.7
Median onset time with 1.2 mg/kg is 60 seconds (0.6-4.7 minutes)
ROCURONIUM BROMIDERAPID SEQUENCE
INTUBATION
ROCURONIUM BROMIDERAPID SEQUENCE
INTUBATION
ROCURONIUM BROMIDE RAPID SEQUENCE INTUBATION
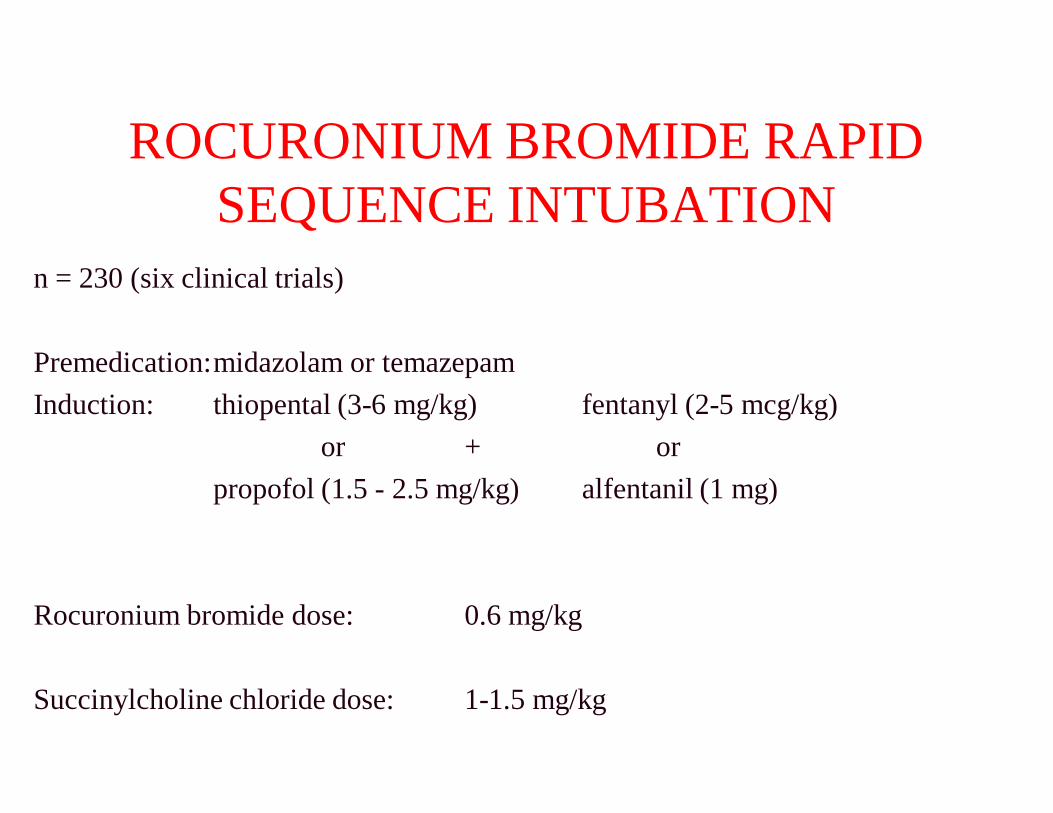
n = 230 (six clinical trials)
Premedication:midazolam or temazepamInduction: thiopental (3-6 mg/kg)
or +propofol (1.5 - 2.5 mg/kg)
Rocuronium bromide dose: 0.6 mg/kg
Succinylcholine chloride dose: 1-1.5 mg/kg
ROCURONIUM BROMIDE RAPID SEQUENCE INTUBATION
fentanyl (2-5 mcg/kg) or
alfentanil (1 mg)
0.6 mg/kg
1.5 mg/kg
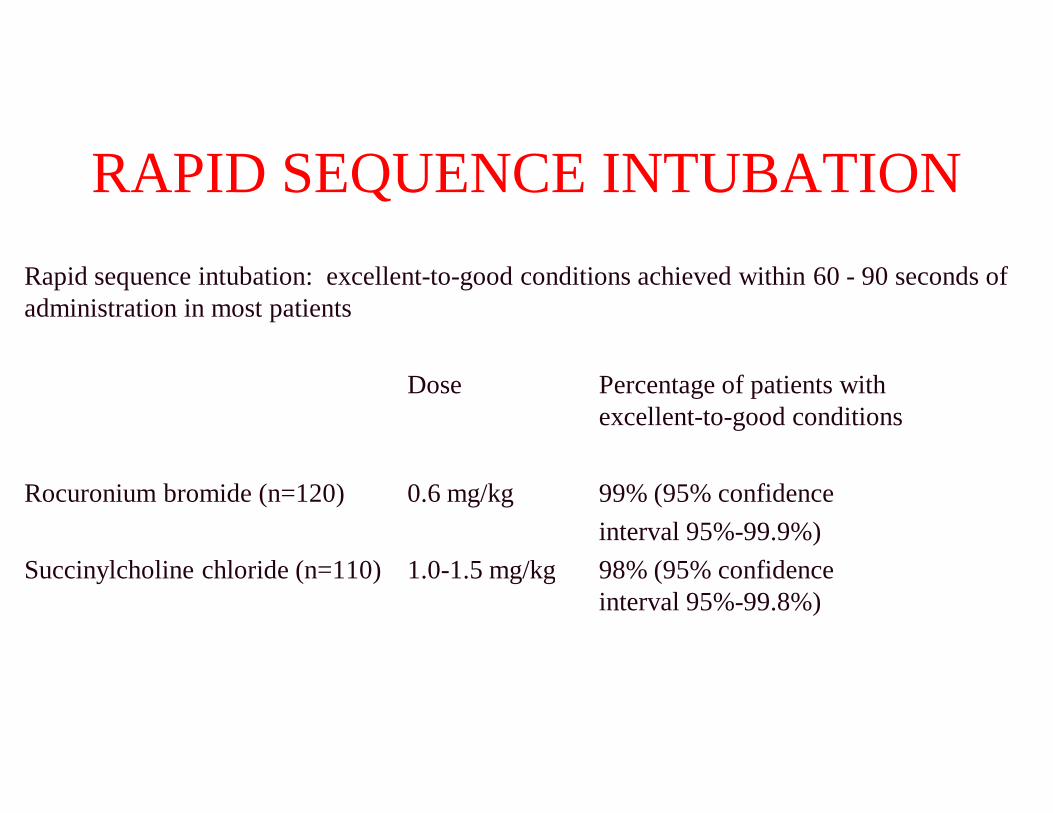
RAPID SEQUENCE INTUBATIONRapid sequence intubation: excellent-to-good conditions achieved within 60 administration in most patients
Dose
Rocuronium bromide (n=120) 0.6 mg/kg
Succinylcholine chloride (n=110) 1.0-1.5 mg/kg
RAPID SEQUENCE INTUBATIONgood conditions achieved within 60 - 90 seconds of
Percentage of patients with excellent-to-good conditions
99% (95% confidence interval 95%-99.9%)
1.5 mg/kg 98% (95% confidence interval 95%-99.8%)
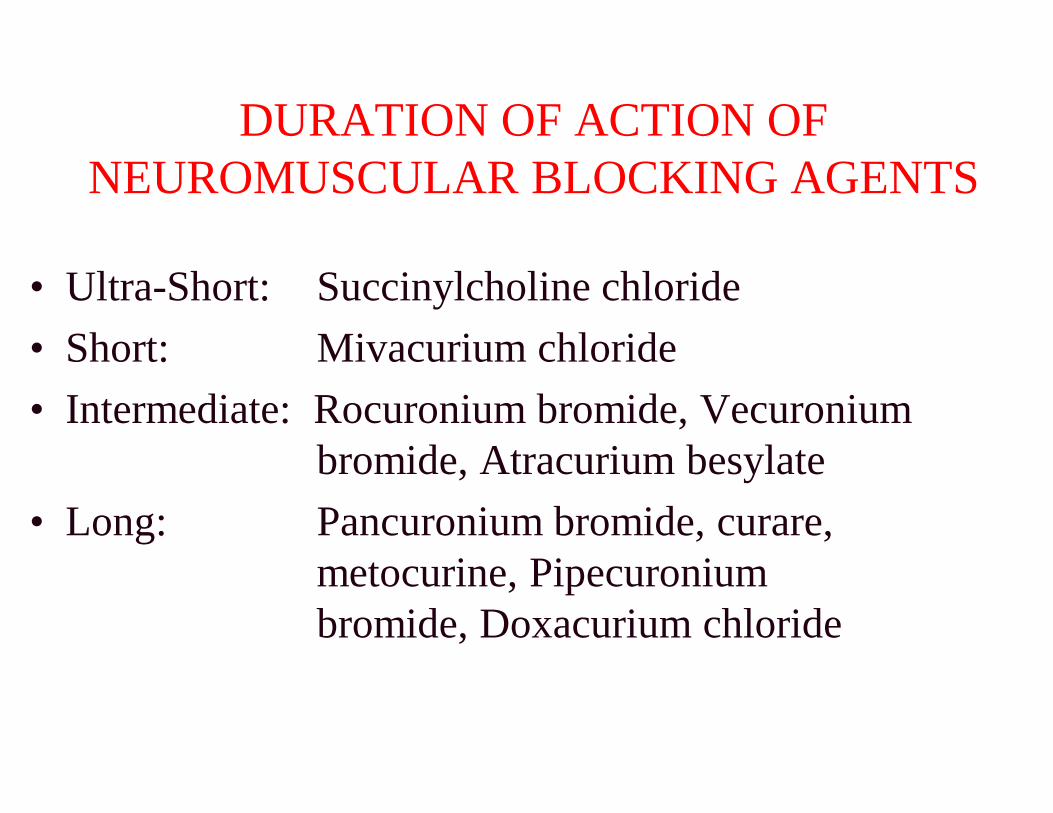
DURATION OF ACTION OF NEUROMUSCULAR BLOCKING AGENTS
• Ultra-Short: Succinylcholine chloride• Short: Mivacurium chloride• Intermediate: Rocuronium bromide, Vecuronium
bromide, Atracurium besylate• Long: Pancuronium bromide, curare,
metocurine, Pipecuronium bromide, Doxacurium chloride
DURATION OF ACTION OF NEUROMUSCULAR BLOCKING AGENTS
Succinylcholine chlorideMivacurium chloride
Intermediate: Rocuronium bromide, Vecuronium bromide, Atracurium besylatePancuronium bromide, curare, metocurine, Pipecuronium bromide, Doxacurium chloride
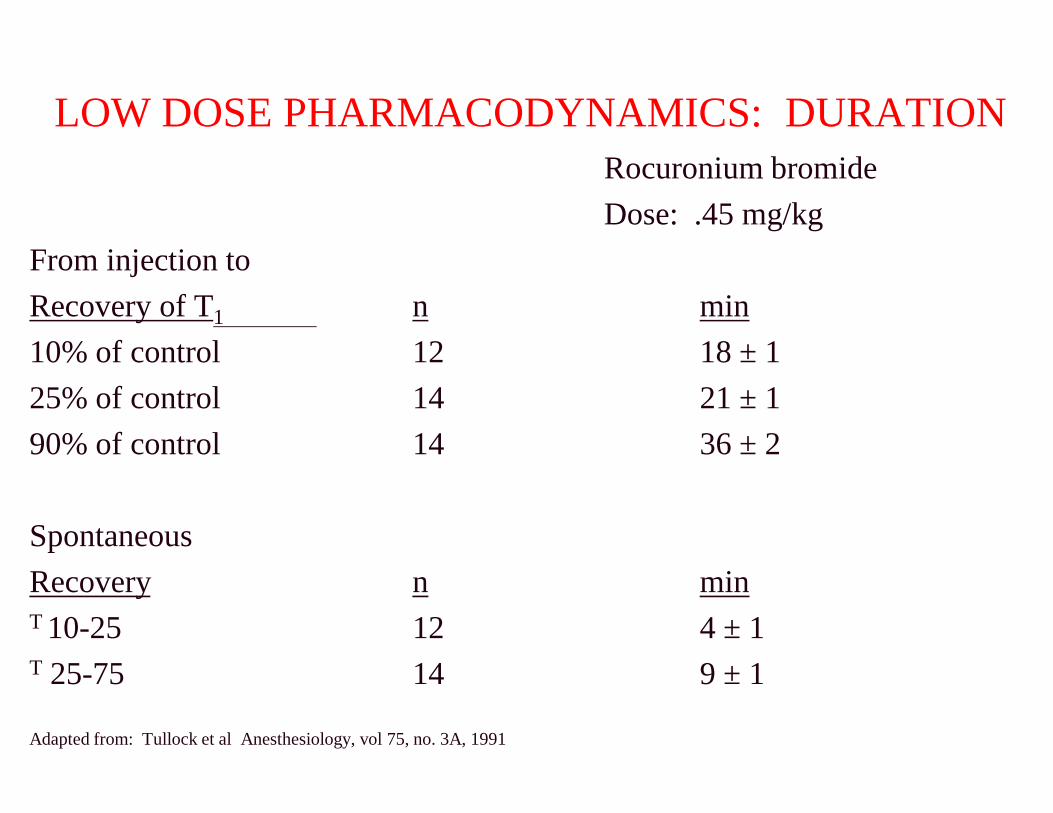
LOW DOSE PHARMACODYNAMICS: DURATION
From injection to Recovery of T1 n10% of control 1225% of control 1490% of control 14
SpontaneousRecovery nT 10-25 12T 25-75 14
Adapted from: Tullock et al Anesthesiology, vol 75, no. 3A, 1991
LOW DOSE PHARMACODYNAMICS: DURATIONRocuronium bromideDose: .45 mg/kg
min18 ± 121 ± 136 ± 2
min4 ± 19 ± 1
CARDIOVASCULAR PROFILE OF ROCURONIUM BROMIDE
AND OTHER NEUROMUSCULAR BLOCKING AGENTS
CARDIOVASCULAR PROFILE OF ROCURONIUM BROMIDE
AND OTHER NEUROMUSCULAR BLOCKING AGENTS
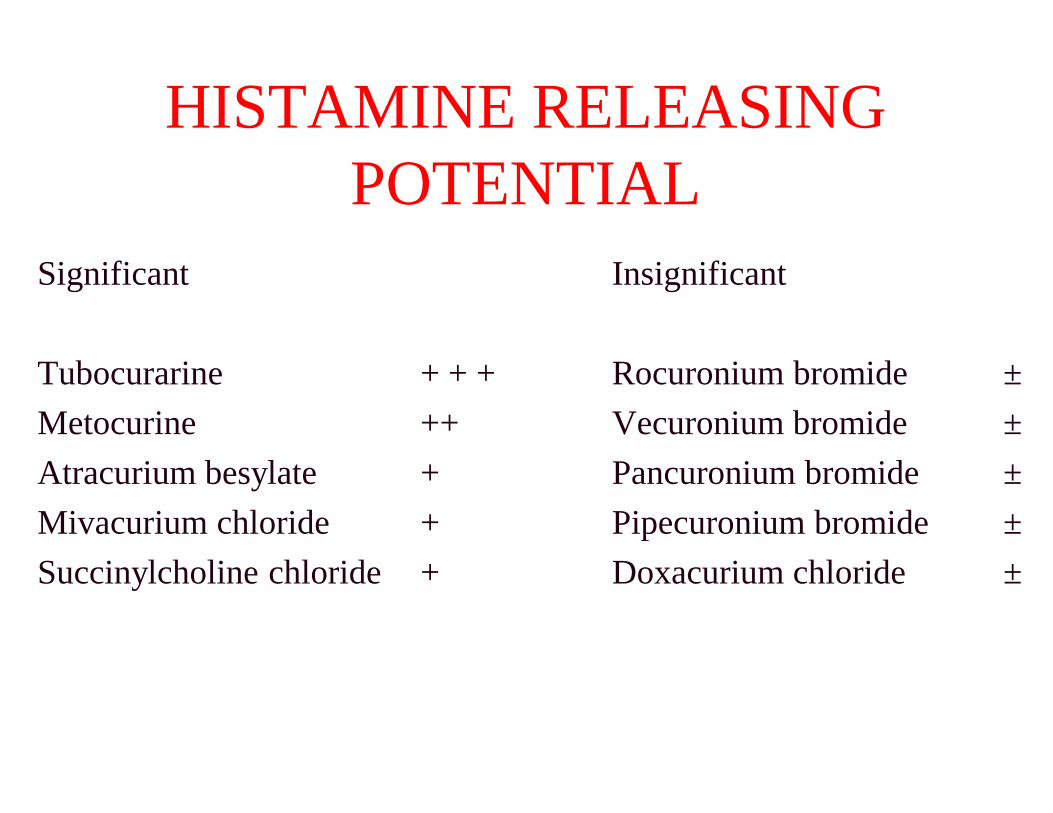
HISTAMINE RELEASING POTENTIAL
Significant
Tubocurarine + + +Metocurine ++Atracurium besylate +Mivacurium chloride +Succinylcholine chloride +
HISTAMINE RELEASING POTENTIAL
Insignificant
Rocuronium bromide ±Vecuronium bromide ±Pancuronium bromide ±Pipecuronium bromide ±Doxacurium chloride ±
Muscle Relaxants
Pancuronium• Vagolytic: increases heart rate,
may require beta blockade• Easy to use• Intermediate duration of action• Slower onset• Not reversed at end of case
Muscle Relaxants
Vagolytic: increases heart rate, may require beta blockade
Intermediate duration of action
Not reversed at end of case
Muscle Relaxants
Vecuronium• No effects on HR, BP
• Requires reconstitution
• Reliable and controllable duration of action
• Slower onset
• Stable hemodynamics/no histamine release
Muscle Relaxants
No effects on HR, BP
Requires reconstitution
Reliable and controllable duration of action
Stable hemodynamics/no histamine release
Muscle Relaxants
Rapacuronium• Minimal effects on HR, BP
• Controllable duration of action
• Fast onset
• Stable hemodynamics/minimal histamine release
• Potential for bronchospasm led to its removal in 2001
Muscle Relaxants
Minimal effects on HR, BP
Controllable duration of action
Stable hemodynamics/minimal histamine release
Potential for bronchospasm led to its removal in
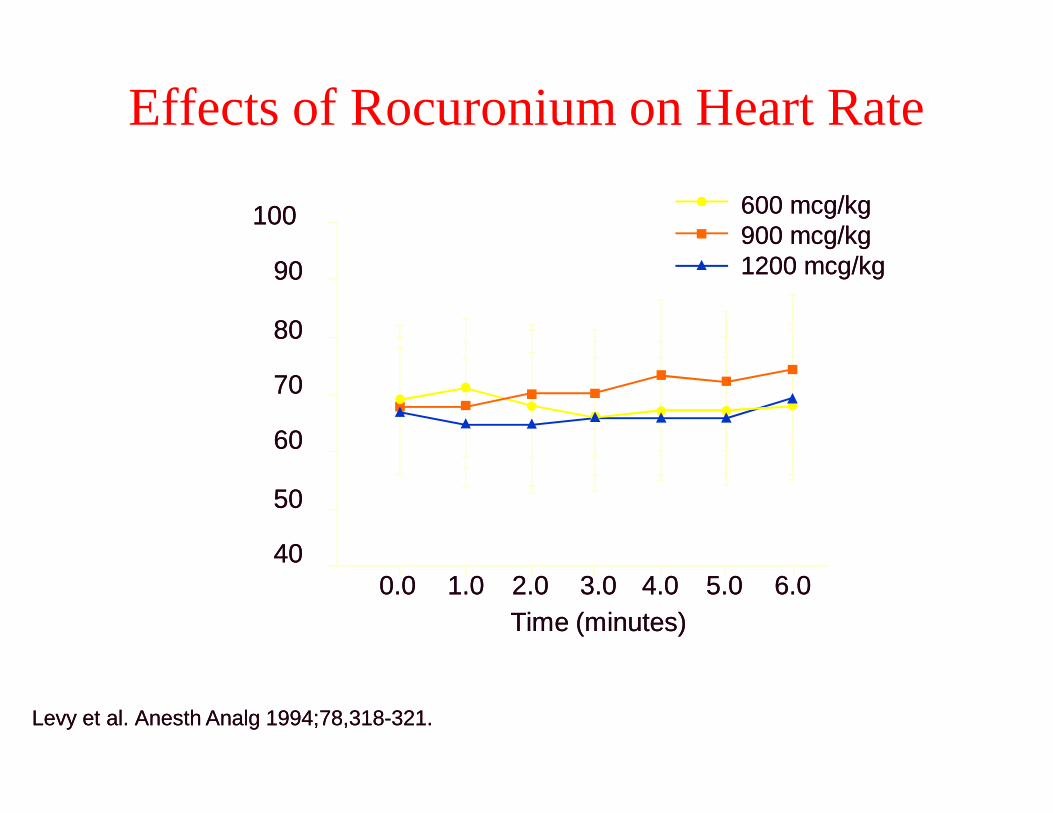
Effects of Rocuronium on Heart Rate
Time (minutes)Time (minutes)
100100
9090
8080
7070
6060
5050
40400.00.0 1.01.0 2.02.0
H
eart R
ate (beats/m
in)
H
eart R
ate (beats/m
in)
Levy et al. Levy et al. Anesth AnalgAnesth Analg 1994;78,3181994;78,318--321.321.
Effects of Rocuronium on Heart Rate
Time (minutes)Time (minutes)2.02.0 3.03.0 4.04.0 5.05.0 6.06.0
600 mcg/kg600 mcg/kg900 mcg/kg900 mcg/kg1200 mcg/kg1200 mcg/kg
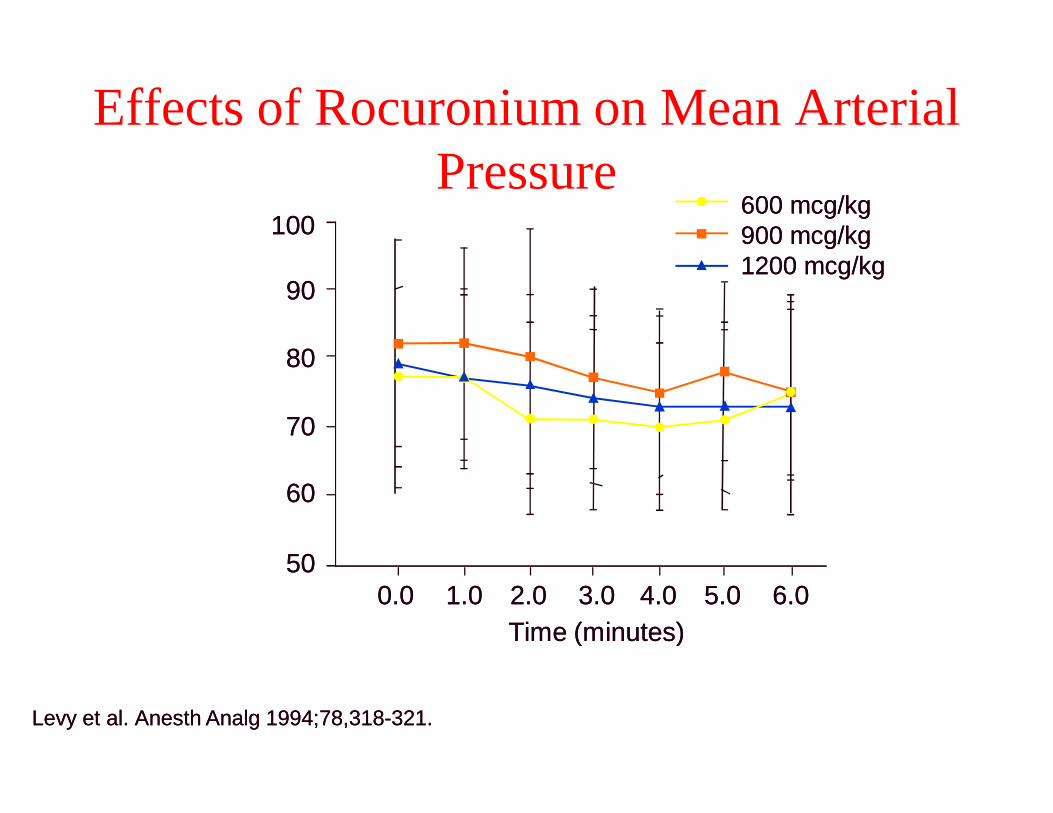
Effects of Rocuronium on Mean Arterial Pressure
Time (minutes)Time (minutes)
100100
9090
8080
7070
6060
50500.00.0 1.01.0 2.02.0M
ean Arterial Pressure (m
m
H
g)
M
ean Arterial Pressure (m
m
H
g)
Levy et al. Levy et al. Anesth AnalgAnesth Analg 1994;78,3181994;78,318--321.321.
Effects of Rocuronium on Mean Arterial Pressure
Time (minutes)Time (minutes)2.02.0 3.03.0 4.04.0 5.05.0 6.06.0
600 mcg/kg600 mcg/kg900 mcg/kg900 mcg/kg1200 mcg/kg1200 mcg/kg
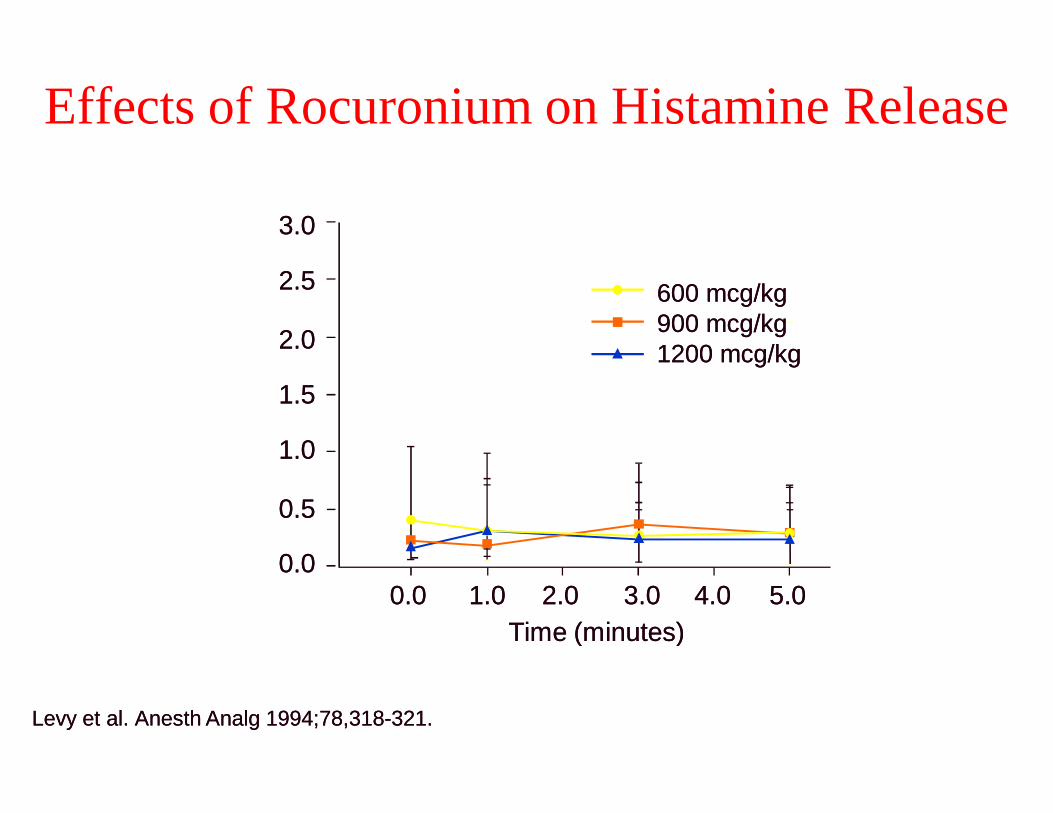
Effects of Rocuronium on Histamine Release
Time (minutes)Time (minutes)0.00.0 1.01.0
Plasm
a H
istam
ine (ng/m
l)
Plasm
a H
istam
ine (ng/m
l)
Levy et al. Levy et al. Anesth AnalgAnesth Analg 1994;78,3181994;78,318--321.321.
3.03.0
2.52.5
2.02.0
1.51.5
1.01.0
0.50.5
0.00.0
Effects of Rocuronium on Histamine Release
Time (minutes)Time (minutes)2.02.0 3.03.0 4.04.0 5.05.0
600 mcg/kg600 mcg/kg900 mcg/kg900 mcg/kg1200 mcg/kg1200 mcg/kg
ROCURONIUM BROMIDE:CARDIOVASCULAR PROFILE
• Favorable cardiovascular profile• Histamine release unlikely• Mild vagolytic activity
ROCURONIUM BROMIDE:CARDIOVASCULAR PROFILE
Favorable cardiovascular profileHistamine release unlikelyMild vagolytic activity
PHARMACODYNAMICS OF ROCURONIUM
BROMIDE IN PEDIATRICS
PHARMACODYNAMICS OF ROCURONIUM
BROMIDE IN PEDIATRICS
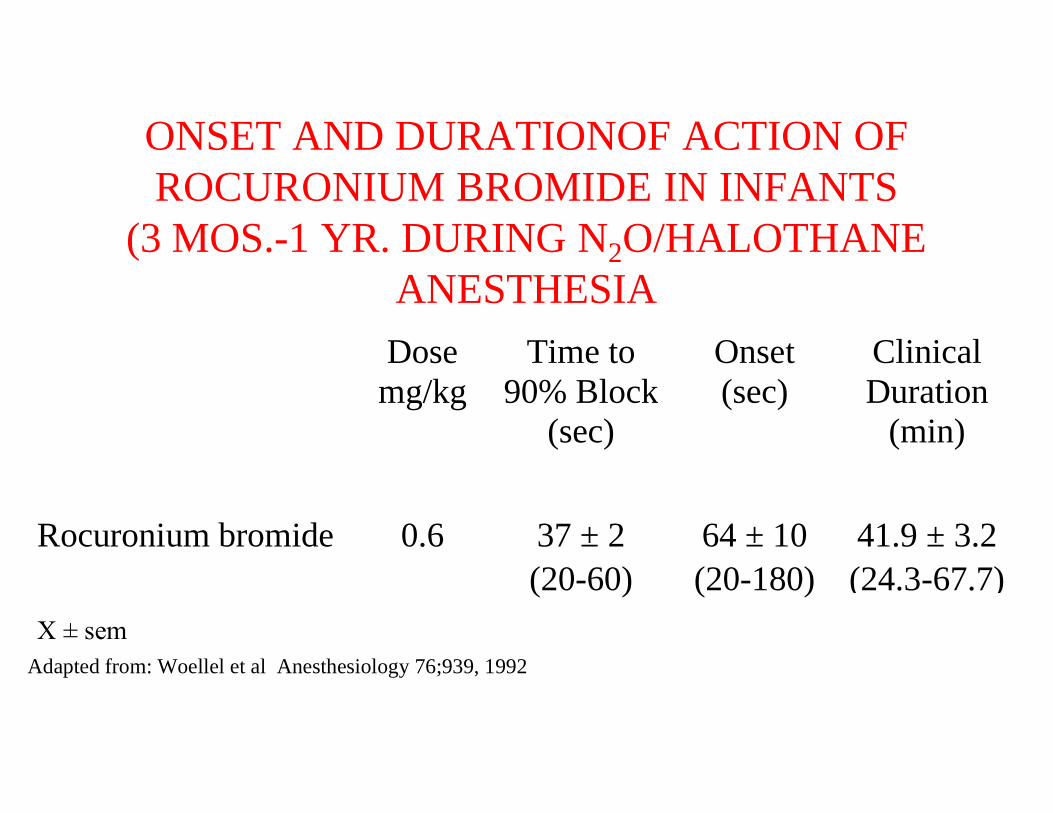
ONSET AND DURATIONOF ACTION OF ROCURONIUM BROMIDE IN INFANTS
(3 MOS.-1 YR. DURING NANESTHESIADosemg/kg 90% Block
Rocuronium bromide 0.6
Χ ± semAdapted from: Woellel et al Anesthesiology 76;939, 1992
ONSET AND DURATIONOF ACTION OF ROCURONIUM BROMIDE IN INFANTS
1 YR. DURING N2O/HALOTHANE ANESTHESIA
Time to90% Block
(sec)
Onset(sec)
ClinicalDuration
(min)
37 ± 2 64 ± 10 41.9 ± 3.2(20-60) (20-180) (24.3-67.7)
al Anesthesiology 76;939, 1992
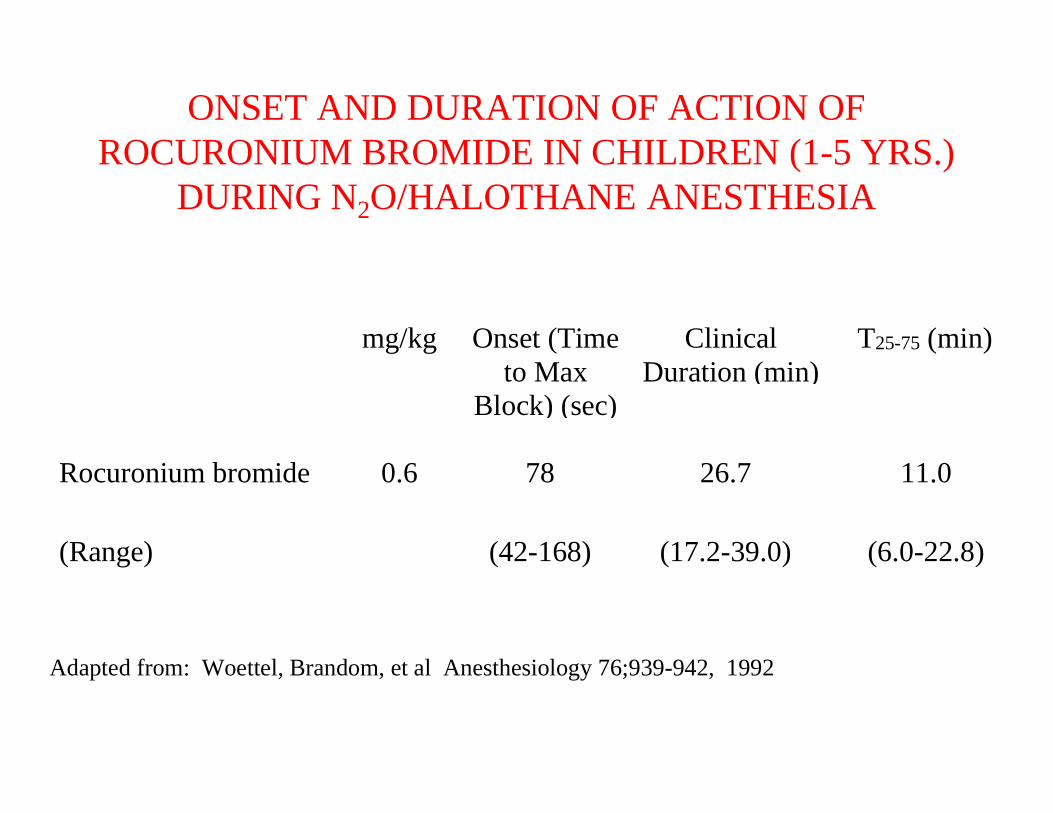
ONSET AND DURATION OF ACTION OF ROCURONIUM BROMIDE IN CHILDREN (1
DURING N2O/HALOTHANE ANESTHESIA
mg/kg Onset (Timeto Max
Block) (sec)
Rocuronium bromide 0.6 78
(Range) (42-168)
Adapted from: Woettel, Brandom, et al Anesthesiology 76;939-942, 1992
ONSET AND DURATION OF ACTION OF ROCURONIUM BROMIDE IN CHILDREN (1-5 YRS.)
O/HALOTHANE ANESTHESIA
Onset (Timeto Max
Block) (sec)
ClinicalDuration (min)
T25-75 (min)
78 26.7 11.0
(42-168) (17.2-39.0) (6.0-22.8)
Brandom, et al Anesthesiology 76;939-942, 1992
PHARMACODYNAMICS OF ROCURONIUM
BROMIDE IN GERIATRICS
PHARMACODYNAMICS OF ROCURONIUM
BROMIDE IN GERIATRICS
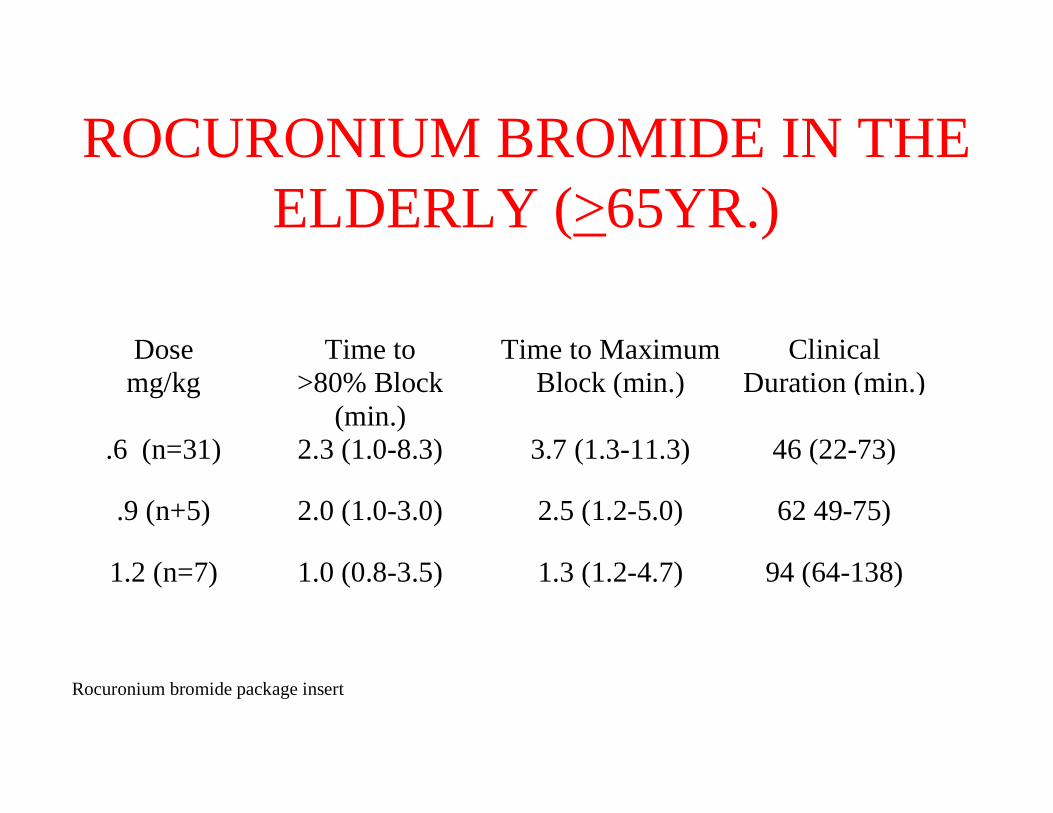
ROCURONIUM BROMIDE IN THE ELDERLY (
Dosemg/kg
Time to>80% Block
(min.)
Time to Maximum
.6 (n=31) 2.3 (1.0-8.3)
.9 (n+5) 2.0 (1.0-3.0)
1.2 (n=7) 1.0 (0.8-3.5)
Rocuronium bromide package insert
ROCURONIUM BROMIDE IN THE ELDERLY (>65YR.)
Time to MaximumBlock (min.)
ClinicalDuration (min.)
3.7 (1.3-11.3) 46 (22-73)
2.5 (1.2-5.0) 62 49-75)
1.3 (1.2-4.7) 94 (64-138)
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
Pediatrics (3 mos. - 1 yr):0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 1 minute, with 41 minutes of clinical relaxation (median)
Rocuronium bromide package insert
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 1 minute, with 41 minutes of clinical relaxation
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
Pediatrics (1 yr - 12 yrs): 0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 1 minute, with 27 minutes of clinical relaxation (median)
Rocuronium bromide package insert
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 1 minute, with 27 minutes of clinical relaxation
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
Adults (18 - 64 yrs): 0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 60 seconds, with 31 minutes of clinical relaxation (median)
Rocuronium bromide package insert
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 60 seconds, with 31 minutes of clinical relaxation
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
Geriatric ( 65 yrs): 0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 2.3 minutes, with 46 minutes of clinical relaxation (median)
Rocuronium bromide package insert
ROCURONIUM BROMIDE: INFLUENCE OF AGESummary
0.6 mg/kg Rocuronium bromide produces excellent to good intubating conditions within 2.3 minutes, with 46 minutes of clinical relaxation
CLINICAL PHARMACOLOGY OF ROCURONIUM BROMIDE
IN RENAL FAILURE
CLINICAL PHARMACOLOGY OF ROCURONIUM BROMIDE
IN RENAL FAILURE
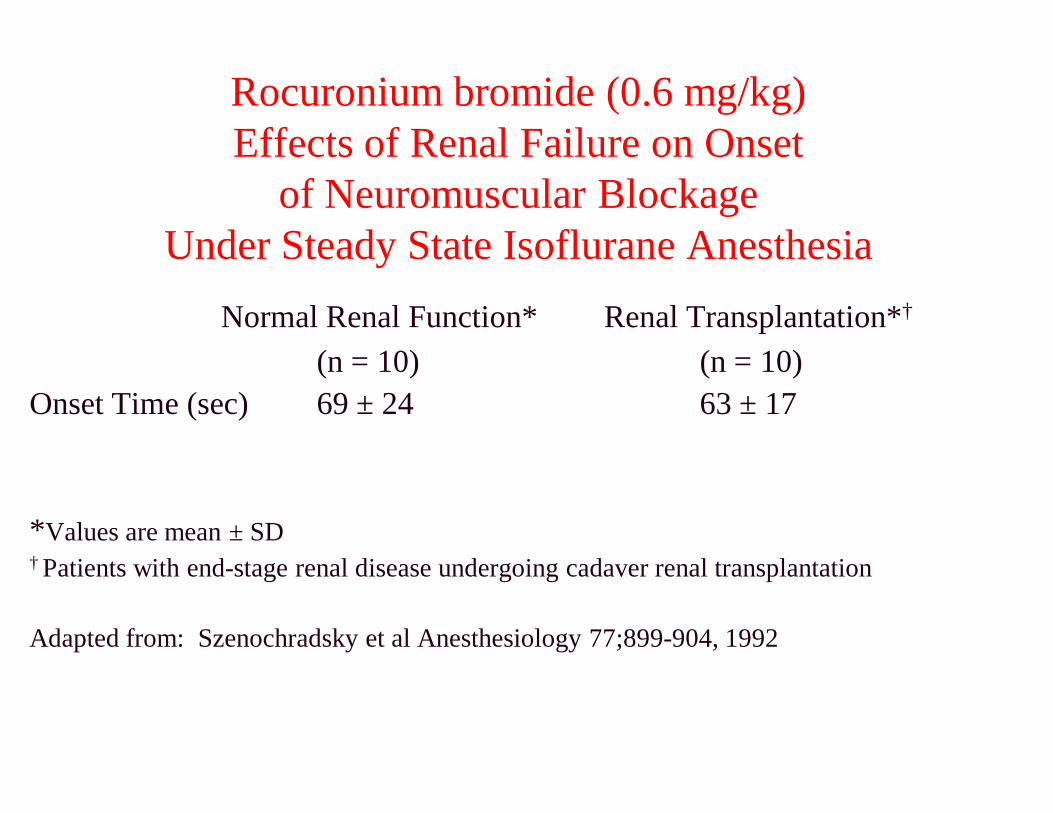
Rocuronium bromide (0.6 mg/kg)Effects of Renal Failure on Onset
of Neuromuscular BlockageUnder Steady State Isoflurane Anesthesia
Normal Renal Function*(n = 10)
Onset Time (sec) 69 ± 24
*Values are mean ± SD† Patients with end-stage renal disease undergoing cadaver renal transplantation
Adapted from: Szenochradsky et al Anesthesiology 77;899
Rocuronium bromide (0.6 mg/kg)Effects of Renal Failure on Onset
of Neuromuscular BlockageUnder Steady State Isoflurane Anesthesia
Normal Renal Function* Renal Transplantation*†
(n = 10)63 ± 17
stage renal disease undergoing cadaver renal transplantation
Adapted from: Szenochradsky et al Anesthesiology 77;899-904, 1992
CLINICAL PHARMACOLOGY OF ROCURONIUM BROMIDE
IN HEPATIC DISEASE
CLINICAL PHARMACOLOGY OF ROCURONIUM BROMIDE
IN HEPATIC DISEASE
ROCURONIUM BROMIDEEffects of Hepatic Disease Under Steady State
Isoflurane Anesthesia
Neuromuscular Effects• Onset unchanged• Recovery increased• Larger or repeat doses may have prolonged effect
Rocuronium bromide package insert
ROCURONIUM BROMIDEEffects of Hepatic Disease Under Steady State
Isoflurane Anesthesia
Larger or repeat doses may have prolonged effect
ROCURONIUM BROMIDEEffects of Hepatic Disease Under Steady State
Isoflurane Anesthesia
Pharmacokinetics• Clearance unchanged• Central and steady state distribution volumes and
elimination half-life increased
Rocuronium bromide package insert
ROCURONIUM BROMIDEEffects of Hepatic Disease Under Steady State
Isoflurane Anesthesia
Central and steady state distribution volumes and life increased
THE PHARMACODYNAMICS OF ROCURONIUM BROMIDE IN THE
OBESE
THE PHARMACODYNAMICS OF ROCURONIUM BROMIDE IN THE
OBESE
Obesity defined as 30% of Ideal Body Weight
• Dose can be based on patient’s actual body weight
Rocuronium bromide package insert
30% of Ideal Body Weight
Dose can be based on patient’s actual body weight
ROCURONIUM BROMIDE IN CONTINUOUS INFUSION
ROCURONIUM BROMIDE IN CONTINUOUS INFUSION

ROCURONIUM BROMIDEContinuous Infusion
Recommended Initial Infusion Rate (Adult):• 0.01-0.012 mg/kg/min. initiated only after
spontaneous recovery from an intubating doseUpon reaching the desired level of neuromuscular block, the infusion of Rocuronium bromide must be individualized for each patient
Rocuronium bromide package insert
ROCURONIUM BROMIDEContinuous Infusion
Recommended Initial Infusion Rate (Adult):0.012 mg/kg/min. initiated only after
spontaneous recovery from an intubating doseUpon reaching the desired level of neuromuscular block, the infusion of Rocuronium bromide must be individualized for each patient
ROCURONIUM BROMIDEContinuous Infusion
Recommended Initial Infusion Rate (Pediatric):• 0.012 mg/kg/min. initiated only after spontaneous
recovery from an intubating dose (under Halothane)Upon reaching the desired level of neuromuscular block, the infusion of Rocuronium bromide must be individualized for each patient
Rocuronium bromide package insert
ROCURONIUM BROMIDEContinuous Infusion
Recommended Initial Infusion Rate (Pediatric):0.012 mg/kg/min. initiated only after spontaneous recovery from an intubating dose (under Halothane)Upon reaching the desired level of neuromuscular block, the infusion of Rocuronium bromide must be individualized for each patient

ROCURONIUM BROMIDE DRUG INTERACTIONS
ROCURONIUM BROMIDE DRUG INTERACTIONS
ROCURONIUM BROMIDE: DRUG INTERACTIONS
Intravenous Anesthetics: The use of propofol for Induction and maintenance of anesthesia does not alter clinical duration of recovery
Rocuronium bromide package insert
ROCURONIUM BROMIDE: DRUG INTERACTIONS
The use of propofol for Induction and maintenance of anesthesia does not alter clinical
ROCURONIUM BROMIDE: DRUG INTERACTIONS
Volatile Anesthetics: Rocuronium bromide requirements are reduced by approximately 10-25% when used with enflurane or isoflurane, but little change when used with halothane
Rocuronium bromide package insert
ROCURONIUM BROMIDE: DRUG INTERACTIONS
Rocuronium bromide requirements are reduced by 25% when used with enflurane
or isoflurane, but little change when used with
ROCURONIUM BROMIDE: DRUG INTERACTIONS
Antibiotics:Drugs which may enhance the neuromuscular blocking action of nondepolarizing agents such as Rocuronium bromide include certain antibiotics (i.e., aminoglycosides; vancomycin; tetracyclines; bacitracin; polymyzins; collistin; and sodium colistimethate)
Rocuronium bromide package insert
ROCURONIUM BROMIDE: DRUG INTERACTIONS
Drugs which may enhance the neuromuscular blocking action of nondepolarizing agents such as Rocuronium bromide include certain antibiotics (i.e., aminoglycosides; vancomycin; tetracyclines; bacitracin; polymyzins; collistin; and sodium
ROCURONIUM BROMIDE: DRUG INTERACTIONS
Anticonvulsants:shorter durations of neuromuscular block may occur and infusion rates may be higher
Rocuronium bromide package insert
ROCURONIUM BROMIDE: DRUG INTERACTIONS
shorter durations of neuromuscular block may occur and infusion rates may be higher
ROCURONIUM BROMIDECONCLUSIONS
• Mono-quaternary steroidal drug• Structural relative of Vecuronium bromide• Rapid to intermediate onset of action. Significantly more
rapid than Vecuronium bromide or Atracurium besylate• For use in outpatient or inpatient procedures of varying
lengths• suitable for rapid sequence intubation• Favorable cardiovascular profiles• Eliminated mainly by liver: minimally by the kidneys
ROCURONIUM BROMIDECONCLUSIONS
quaternary steroidal drugStructural relative of Vecuronium bromideRapid to intermediate onset of action. Significantly more rapid than Vecuronium bromide or Atracurium besylateFor use in outpatient or inpatient procedures of varying
suitable for rapid sequence intubationFavorable cardiovascular profilesEliminated mainly by liver: minimally by the kidneys
Current Conceptsin
Neuromuscular Blockade
7776
Current Conceptsin
Neuromuscular Blockade
Neuromuscular Agents: Costs of Care• Cost of care acquisition cost
• The real, substantial savings accrue from use of intermediateshort-acting drugs because:• Inexpensive, long-acting drugs are associated with prolonged
postoperative recovery 1
• Fast recovery means shorter risk periods of residual blockade. This translates into fewer postoperative complications, as shown in the Berg study2
• Postoperative complications are Avoiding these is where the real cost savings accrue
1Ballantyne JC, et al. Anesth Analg. 1997; 85:4762Berg H, et al. Acta Anaesthesiol Scand. 1997;41:1095
Neuromuscular Agents: Costs of Care
The real, substantial savings accrue from use of intermediate- and
acting drugs are associated with prolonged
Fast recovery means shorter risk periods of residual blockade. This translates into fewer postoperative complications, as shown in the
Postoperative complications are very expensiveAvoiding these is where the real cost savings accrue
Ballantyne JC, et al. Anesth Analg. 1997; 85:476Berg H, et al. Acta Anaesthesiol Scand. 1997;41:1095
• Cardiovascular stability• Nondepolarizing vs depolarizing • Organ-independent elimination• Clinically significant active or toxic metabolites• Predictability of duration• Cumulative effects• Reversibility• Time to onset• Stability of solution• Cost
Rationale for Selection of NMBs:Rationale for Selection of NMBs:
Nondepolarizing vs depolarizing independent elimination
Clinically significant active or toxic metabolites
Rationale for Selection of NMBs:Rationale for Selection of NMBs:





























