Embed Size (px)
Citation preview

Clinical Pharmacy Practice-Pediatrics
Sun (Coco) Yang, BsPharm, MSc., Ph.D, BCPPS, APhChapman School of Pharmacy
June 2021

Pediatric conditions
I. Respiratory Distress Syndrome (RDS) in neonatesII. Respiratory Syncytial virus (RSV)III. Patent ductus arteriosus (PDA)

I. Respiratory Distress Syndrome (RDS) in neonates

Objectives
• Explain the pathophysiology and clinical presentation of respiratory distress syndrome (RDS);
• Discuss the pharmacologic agents for the prevention and treatment of RDS.

Respiratory Distress Syndrome (RDS)
• Premature newborns commonly have complications with respiratory development and function
• RDS is a respiratory disorder caused by surfactant deficiency due to prematurity
• Pulmonary surfactant prevents alveolar collapse to allow for optimal gas exchange and prevent respiratory failure
• Infants with RDS have immature lungs that often require oxygen supplementation or mechanical ventilation which both can lead to bronchopulmonary dysplasia (BPD), a chronic lung disorder.

Epidemiology
• RDS was a common cause of morbidity and mortality in neonates prior to the discovery of exogenous pulmonary surfactant
• ~Premature birth occurs in about 11% to 13% of pregnancies in the US.• The risk of RDS increases with decreasing gestational age (GA) and birth
weight• ~93% of preterm newborns (<28 weeks)• ~30% of preterm born at 30-31 GA
• Maternal steroid use before delivery promotes maturation of the surfactant system in the neonate
• With steroid use, 50% of infants born before 30 weeks’ GA and 25% of infants born after 30 weeks’ GA will develop RDS
• Despite recent declines in the incidence of RDS, the condition remains a significant cause of morbidity and mortality.

Pathophysiology• Surfactant acts to lower surface tension at the air-liquid interface in
the alveoli to prevent alveolar collapse• A sufficient amount of surfactant is needed to maintain normal lung
function however is not needed until the saccular phase which is around 36 weeks’ GA
• The inadequate production or impaired release of pulmonary surfactant in premature neonates can lead to RDS at birthSurfactant consists of lipids and surfactant proteinsEach protein has a unique functionThe proteins required for normal lung function are
• Phosphatidylcholine• Surfactant protein B• Surfactant protein C


Clinical Presentation
• Neonates with RDS usually present shortly after birth with signs of respiratory distress
• Grunting• Tachypnea• Retractions• Cyanosis• Nasal flaring• Oxygen requirements• Tachycardia

Diagnosis
Based on• Infants clinical picture at birth• Chest x-ray findings• Rule out of other neonatal
disorders such as• Early-onset sepsis;• Transient tachypnea of the
newborn; • Spontaneous pneumothorax

Non-pharmacologic options
• It is critical to establish oxygenation and ventilation promptly after birthto prevent pulmonary vasoconstriction and subsequent atelectasis
• Options include• Oxygen• Continuous positive airway pressure
(CPAP)• Mechanical ventilation

Therapeutic Goals• Primary goal
• Rapidly replace pulmonary surfactant, minimize potential lung injury and reduce duration of supplemental oxygen or mechanical ventilation with continued efforts to prevent BPD
Pharmacologic Options


Types of Surfactants
Surfactant (cost per dose
in pt)
Source Conc. Of phosph.(mg of
phosph./kg)
Initial Dose (mg of
phospholipids/kg)
MaintenanceDose ( mg of
phospholipids/kg)
Dosing interval
MAX Total doses
Beractant($664)
Bovine 25 100 mg/kg 100 mg/kg 6 4
Calfactant($343)
Bovine 35 105 mg/kg 105 mg/kg 12 4
Poractant alfa($570)
Porcine 80 200 mg/kg 100 mg/kg 12 3

Question
• Anaphylaxis reaction may worsen the difficulty of breathing or even cause patient’s death.
• Do we concern about the risk of anaphylaxis reaction when giving bovine/porcine surfactant to a newborn directly?
Hypersensitivity reactions are very common in childhood, but they are very rare in the neonatal period due to the immaturity of the immunological system.

Endotracheal tube The neonates may be placed in serval positions to facilitate surfactant distribution• Left and Right• https://www.youtube.com/wat
ch?v=1tic3rMVBMs• @11’45’’

SurfactantAdministration
• Instill the solution through a catheter into the endotracheal tube• The volume and the number of aliquots depends on the type of surfactant being
used• Position
Repeat dosing• May be repeated according to the recommended maximum• Infants with lung injury from mechanical ventilation or supp. Oxygen can benefit
from a repeat dose because pulmonary inflammation can inhibit surfactant function
Allergy potential is Low• allowing the use of bovine and porcine products• Immature newborn immunity
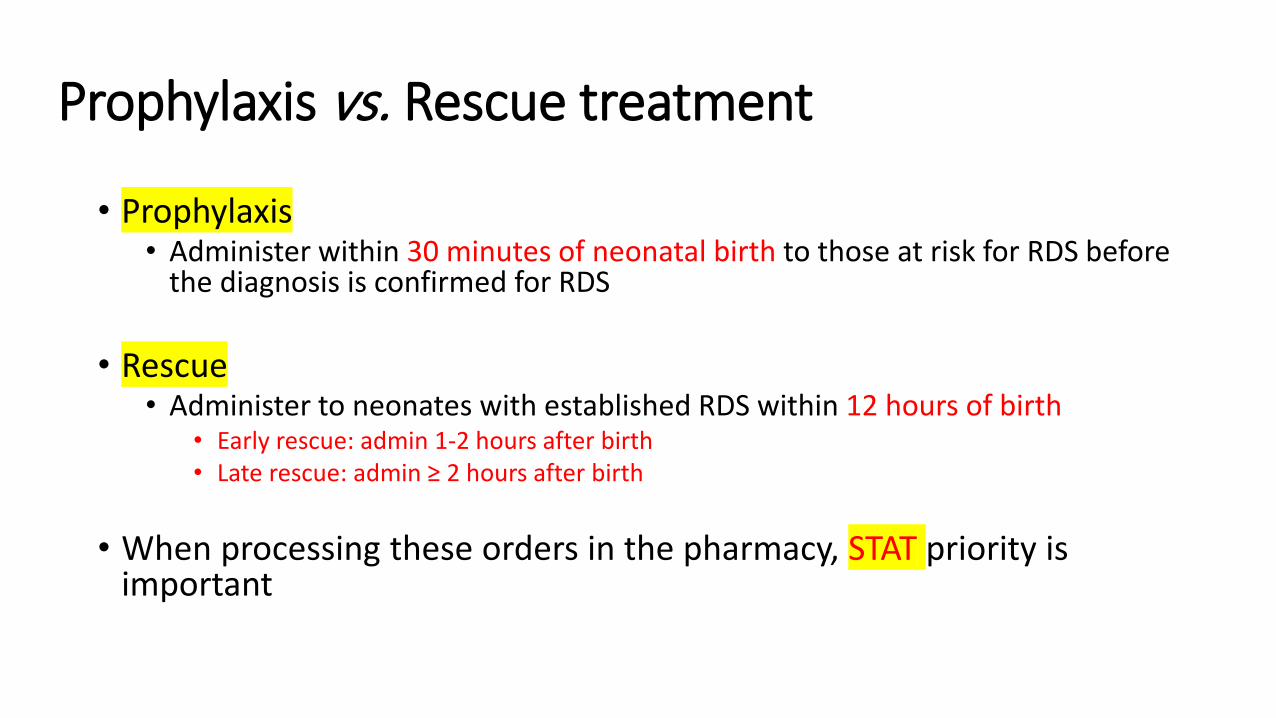
Prophylaxis vs. Rescue treatment
• Prophylaxis• Administer within 30 minutes of neonatal birth to those at risk for RDS before
the diagnosis is confirmed for RDS
• Rescue• Administer to neonates with established RDS within 12 hours of birth
• Early rescue: admin 1-2 hours after birth• Late rescue: admin ≥ 2 hours after birth
• When processing these orders in the pharmacy, STAT priority is important

Surfactant Replacement Therapy
• Standard of Care in RDS prophylaxis and treatment• Premature born <35 weeks gestation
• Allows for decreased ventilation requirements• Reduces incidence of mortality, pneumothorax, and pulmonary
interstitial emphysema• Infants < 30 weeks GA or with a birth weight < 1250g have the
greatest reduction in mortality

Patient Case - MT
MT is a (1.2 kg) female infant born via emergency C-section at 28-weeks gestation to a G2P2 mother who did not receive maternal steroids but did have prenatal care. Within 3 hours of birth, MT was noted to have substantial nasal flaring, grunting and was requiring oxygen. Her chest x-ray revealed a bell-shaped thorax.
1. What factor(s) are indicative of possible RDS in MT?2. Name 2 treatment options MT may require at this stage? How will
these be administered?

Summary
• RDS is a respiratory disorder caused by surfactant deficiency• Pulmonary surfactant prevents alveolar collapse to allow for optimal
gas exchange and prevent respiratory failure• The risk of RDS increases with decreasing gestational age and birth
weight < 1250 grams• Signs and symptoms present shortly after birth• Non-pharmacologic and pharmacologic options are available• Exogenous surfactant is the standard of care for prophylaxis and
rescue therapy

1. Define Respiratory Distress Syndrome (RDS)2. Who is categorized as increased risk of development? What factors are
considered?3. Clinical Presentation4. What are the therapeutic goals?5. Define RDS Standard of Care
a. Administrationb. Repeat dosingc. Allergy potentiald. Define Prophylaxis therapy approache. Define Rescue therapy approach
II. Respiratory syncytial virus (RSV)

Bronchiolitis• Bronchiolitis is the most common lower respiratory tract infection (LRTI) in
infants younger than 12 months. • Inflammation of the bronchioles and is often associated with wheezing• Associated with airway edema, epithelial lining necrosis, mucous production, and
bronchospasm.
• Usually as the result of a viral infection• Occurs during winter months (November through April). • Respiratory syncytial virus (RSV) has been most closely associated and is the
causative organism in 80% to 100% of cases occurring during the winter months.
• Infection occurs after exposure to infected respiratory droplets. The incubation period is generally 2–8 days, but it may last up to 4 weeks in young infants.
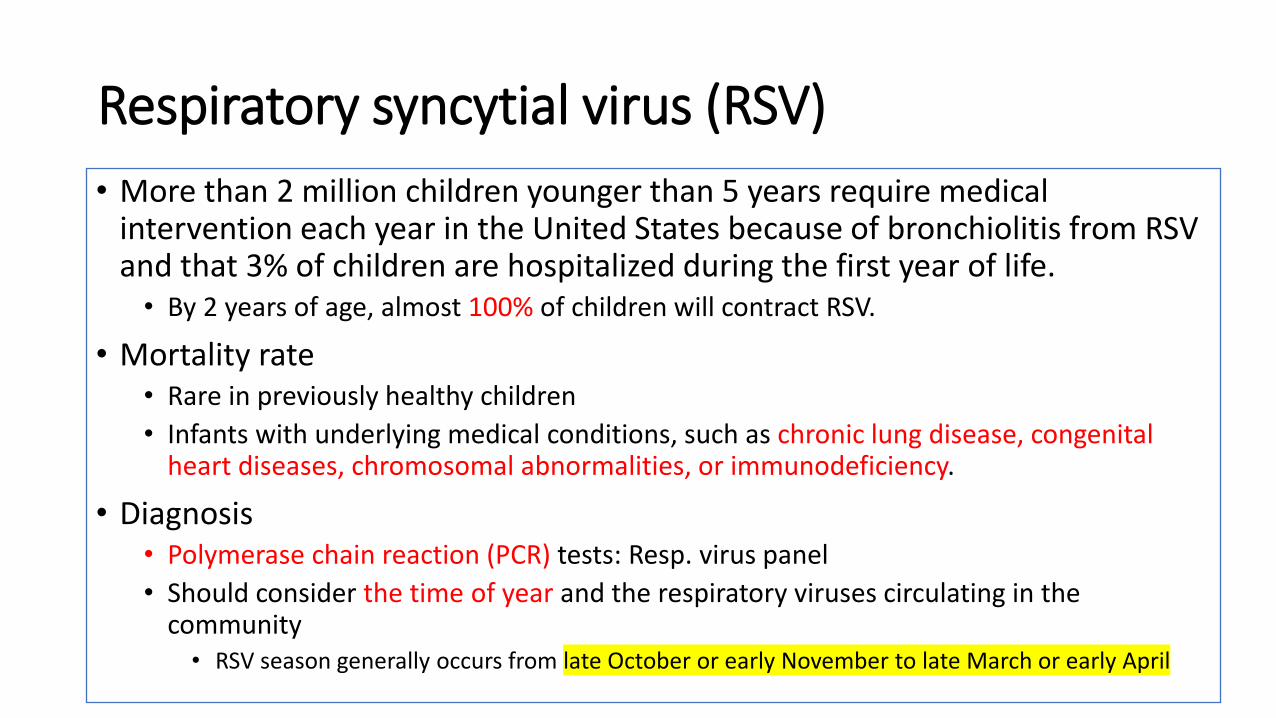
Respiratory syncytial virus (RSV)• More than 2 million children younger than 5 years require medical
intervention each year in the United States because of bronchiolitis from RSV and that 3% of children are hospitalized during the first year of life.
• By 2 years of age, almost 100% of children will contract RSV.
• Mortality rate• Rare in previously healthy children• Infants with underlying medical conditions, such as chronic lung disease, congenital
heart diseases, chromosomal abnormalities, or immunodeficiency.
• Diagnosis• Polymerase chain reaction (PCR) tests: Resp. virus panel• Should consider the time of year and the respiratory viruses circulating in the
community• RSV season generally occurs from late October or early November to late March or early April

RSV-caused bronchiolitis• Most children experience complete resolution of their symptoms
within 8–15 days without needing medical intervention.• Patients who experience more severe disease might present with the
additional symptoms of hypoxia, cyanosis, apnea, and respiratory distresshospitalized.
• Risk factors of severe disease• History of premature birth• Younger than 12 weeks• Chronic lung disease• Congenital heart defect• Immunodeficiency

RSV Prophylaxis
• Infection with RSV does not confer lifelong immunity.• Reinfection with RSV can occur throughout a person’s lifetime.• No vaccine is available
• Palivizumab (Synagis)• Humanized monoclonal antibody for prevention of LRTIs from RSV in high-risk
pediatric populations• Administered at a dose of 15 mg/kg intramuscularly every month during the RSV
season• Neonates/infants: Anterolateral thigh muscle• Older children: deltoid
• No more than 5 monthly doses during the RSV season• If the baby becomes infected with RSV, no further doses of palivizumab should be
given.

Who should receive RSV prophylaxis treatment?
Who should receive Synagis prophylaxis during the RSV season?In the first year of life• Premature infants born at <29 weeks gestation;• Premature infants born <32 weeks gestation with chronic lung
disease who are <12 months of age;• Infants < 12 months of age with a “hemodynamically
significant” congenital heart defect


Treatment• Primarily supportive care
• To maintain oxygenation, maintain adequate hydration, and reduce fever. • Non-pharmacologic treatment
• Supplemental oxygen once their O2 saturations decrease below 90%.• Pharmacologic treatments
• Nebulized hypertonic saline (3% to 12%)• Bronchodilators:
• AAP does not recommend the routine use of bronchodilators for children with bronchiolitis unless patient p/w asthma
• Corticosteroids• AAP does not recommend the routine use of corticosteroids in children with bronchiolitis
• Inhaled ribavirin• ??Efficacy; does not improve clinical outcomes• Requires administration by a special nebulizer (SPAG-2 [small-particle aerosol generator]) for a
minimum of 12–18 hours;• Teratogenic potential and is a pregnancy risk category X






PDA in term infants is reported to be 1 in 2000 live births and around 5%-10% of all CHDs. 1 in 500 live births if asymptomatic.▪ “silent” PDA
Female: male=2:1 Much higher rate in pre-term neonates▪ 1 in 125 live births

Ductus arteriosus Fetus: allows blood bypass lungs▪ Oxygen exchange through placenta
After birth:▪ In response to increased O2 and removal of
placental prostaglandins, the newborn ductus will functionally close during the first few days after delivery.▪ Closed about 96 hours after birth with permanent
destruction at about two weeks
▪ Pulmonary vascular resistance drops

Lung alveolus
What if DA is not closed? PDA▪ Acyanotic Left-to-right Shunt▪ Aorta PA and lungs pulmonary over-circulation
▪ Increasing pulmonary blood flow▪ Pulmonary hypertension/edema and CHF

Why PDA is not closed? Premature infants▪ Ductal tissue does not respond to high levels of circulating
oxygen postpartum like term newborn does.
Genomic/family history??▪ Family history is a predictor of current preterm birth▪ Spontaneous preterm birth in the current pregnancy was
significantly associated with a maternal family history of preterm birth among female relatives within 3 generations and notably sisters. Am J Obstet Gynecol MFM, 2021
▪ No consistent conclusions
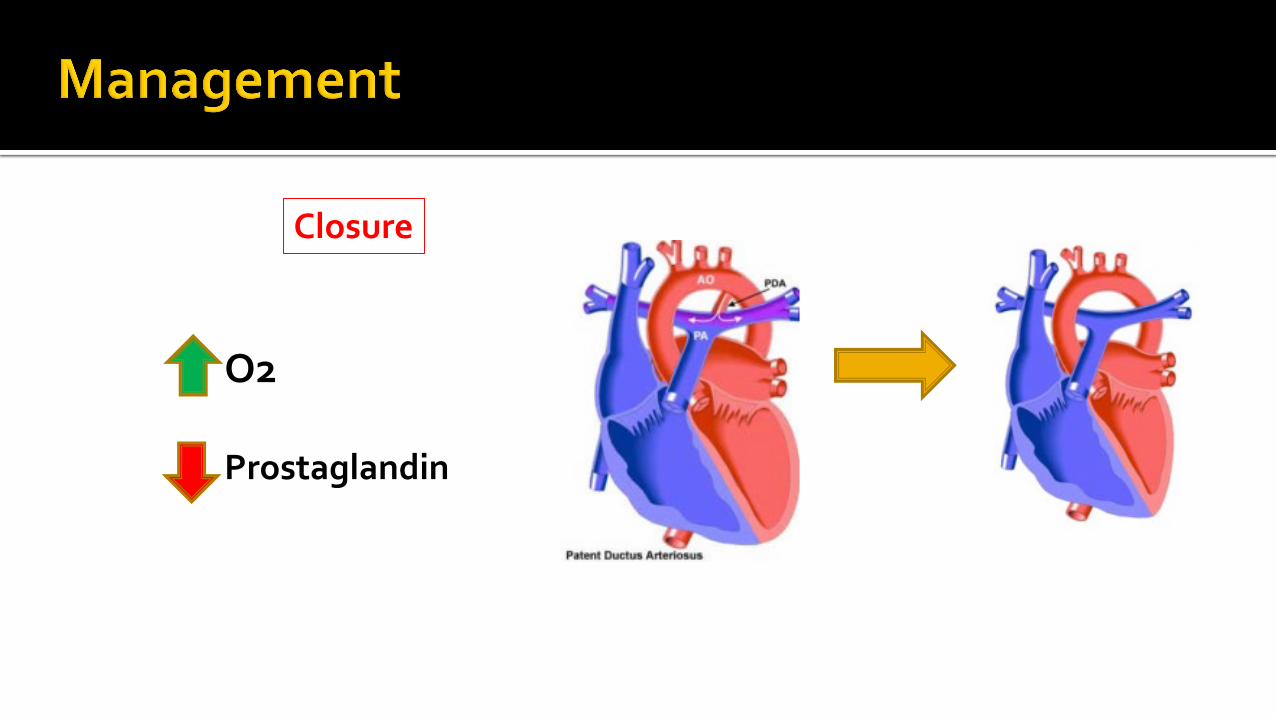
Closure
O2
Prostaglandin
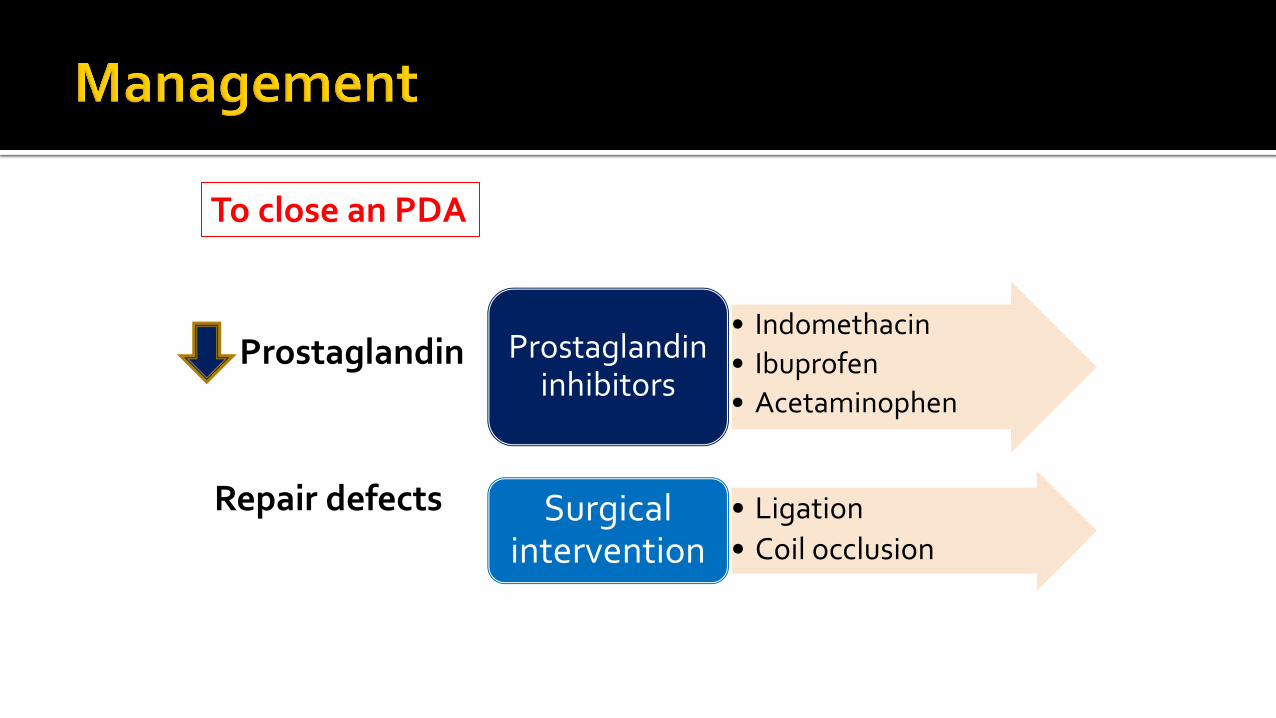
To close an PDA
Prostaglandin• Indomethacin• Ibuprofen• Acetaminophen
Prostaglandin inhibitors
Repair defects • Ligation• Coil occlusion
Surgical intervention

Landmark clinical study The National Collaborative Study on
PDA in Premature Infants More than 400 infants less than 1,750 g Receiving three dosages as an
intermittent infusion every 12 hours 79% of patients achieved ductal
closure. Patients receiving indomethacin
experienced significantly more bleeding episodes and elevation of serum creatinine.
MOA Decrease prostaglandins through
reversible inhibition of COX-1 and COX-2 enzymes
Dose Based on postnatal age at time of first
dose and urine output (UOP) after first dose.▪ UOP ≥ 1ml/kg/hour after first dose: q12hr▪ UOP 0.6-1 ml/kg/hour after first dose:
q24hr▪ Postnatal age >7 days:
▪ 1st: 0.2 mg/kg IV▪ 2nd: 0.25 mg/kg IV▪ 3rd: 0.25 mg/kg IV

Drug of choice for closure of PDA As effective as indomethacin Reduced risk of necrotizing enterocolitis and
transient renal insufficiency
MOA Decrease prostaglandins through reversible
inhibition of COX-1 and COX-2 enzymes
Dose Based on birth weight
▪ Gestational age ≤ 32 weeks (500g -1500g at birth)▪ 10 mg/kg/dose IV, followed by 5mg/kg/dose IV 24hrs
and 48hrs after the first dose
Dosage forms Oral solution: 20 mg/ml; IV solution: 10mg/ml
Special considerations Do not initiate ibuprofen for ductal closure
with renal impairment If DA does not close or reopen after initial
course, a second course may be considered versus indomethacin or surgical closure.
Enteral ibuprofen: at least as effective as IV administration
Data inadequate to determine if high-dose is superior to standard dose.

Same MOA
FDA approves IV formulation of acetaminophen in 2010 Reduced GI bleeding risk
▪ Ok for renal insufficient patients
Expensive▪ Ofirmev
Several case series and two small clinical trials Suggest that acetaminophen is an alternative to ibuprofen or indomethacin.
▪ Not FDA-approved indication for usage
Data are insufficient to recommend the routine use for ductal closure.

J Pediatr Pharmcol Ther 2017 Nov-Dec; 22(6): 461–466. 41 pre-term neonates, Missouri, U.S.
▪ Median gestational age: 25 weeks▪ Median birth weight: 760 g
Initial dosing: 15 mg/kg q6 hrs (88% via IV).
Median treatment duration: 7 days Outcomes
▪ Twenty-seven neonates (66%) required no further PDA treatment
▪ 10 neonates (24%) with Echocardiographic PDA closure documented
▪ 15 neonates (37%) reduced ductal size▪ No significant ADRs
Ann Pediatr Cardiol. 2019 May-Aug; 12(2): 97–102. A first dose of 25 mg/kg and maintenance
doses of 30 mg/kg/day, for 3 to 7 days. 87 preterm newborns
▪ Gestational age: 27.2 +/- 1.9 weeks▪ Birth weight: 889 g +/- 241 g
Outcomes▪ The ductus closure rate, after one or two cycles,
was 74.7% Acetaminophen in low doses showed to be
an effective alternative for the closure of the PDA for preterm newborns in whom treatment with indomethacin or ibuprofen failed or was contraindicated.

Patient case
C.P. is a 28-weeks post-conceptional age baby boy (current body weight=992 g) who remains ventilator-dependent. He was born at 26 weeks gestational age with a birth weight of 720 g. He has a continuous murmur and bounding peripheral pulse, and his chest radiography shows evidence of pulmonary over-circulation with mild cardiomegaly consistent with patent ductus arteriosus (PDA). He has no evidence of intraventricular hemorrhage on cranial ultrasonography.
Hgb 8 g/dLBlood urea nitrogen (BUN)
15 mg/dL
Serum creatinine (Scr)
0.9 mg/dL(baseline: 0.9 ml/dL)
Hematocrit (Hct) 40%Platelet count 160,000/mm3
Total bilirubin 1.4 mg/dLDirect bilirubin 0.4 mg/dL

B is the correct answer due to severe clinical symptoms

A is the correct answer as patient is on ventilatorso the PO is not an option for now.
Ibuprofen is the DOC for PDA, so indomethacin is NOT the best option due to its severe toxicities.

Patient case
C.P. is a 28-weeks post-conceptional age baby boy (current body weight=992 g) who remains ventilator-dependent. He was born at 26 weeks gestational age with a birth weight of 720 g. He has a continuous murmur and bounding peripheral pulse, and his chest radiography shows evidence of pulmonary over-circulation with mild cardiomegaly consistent with patent ductus arteriosus (PDA). He has no evidence of intraventricular hemorrhage on cranial ultrasonography.
Hgb 10 g/dLBlood urea nitrogen (BUN)
15 mg/dL
Serum creatinine (Scr)
0.9 mg/dL(baseline: 0.9 ml/dL)
Hematocrit (Hct) 40%Platelet count 160,000/mm3
Total bilirubin 2.4 mg/dLDirect bilirubin 0.4 mg/dL

B should be the best answer. Since patient's UOPreduced significantly, the second/third dose ofibuprofen should be dependent on the UOP afterthe first dose. If getting worse, need to switch toacetaminophen; if remaining the same or evengetting better, continue ibuprofen.

Rx pearls
• Ibuprofen is the DOC; less renal toxicity compared to indomethacin;• If anuria or marked oliguria (urinary output <0.6 ml/kg/hr) is evident
at the scheduled time of the second or third dose, hold dose until renal function returns to normal.
• Use is contraindicated in preterm infants with significant renal impairment.
This applies to both indomethacin and ibuprofendue to their potential renal toxicities.

Patient case
• UOP continue to drop to 0.5 ml/kg/hr.
• SCr: increased to 1.3 mg/dL.• Total bilirubin: increased from
2.4 mg/dL to 5.4 mg/dL• Direct bilirubin: increased from
0.4 mg/dL to 1.5 mg/dL.
Hgb 10 g/dLBlood urea nitrogen (BUN)
15 mg/dL
Serum creatinine (Scr)
1.3 mg/dL(baseline: 0.9 ml/dL)
Hematocrit (Hct) 40%Platelet count 160,000/mm3
Total bilirubin 5.4 mg/dLDirect bilirubin 1.5 mg/dL
This indicates patient's severerenal impairment.
Increasing bilirubin requires furtherworkup to roll out potential liver inpairment

Both D and E are accepted as an option. But personally I would prefer E as the best option.If patient hosptialized, a STAT lab order for liverenzymes can be completed within hours to roll outsevere hepatic impairment.