Embed Size (px)
Citation preview

http://lup.sagepub.com/Lupus
http://lup.sagepub.com/content/22/7/690The online version of this article can be found at:
DOI: 10.1177/0961203313490240
2013 22: 690 originally published online 20 May 2013LupusBK Han, R Bhatia, P Traisak, K Hunter, B Milcarek, C Schorr, H Eid, D Feinstein, P Cronin and SL Kolasinski
to the intensive care unitClinical presentations and outcomes of systemic lupus erythematosus patients with infection admitted
Published by:
http://www.sagepublications.com
can be found at:LupusAdditional services and information for
http://lup.sagepub.com/cgi/alertsEmail Alerts:
http://lup.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- May 20, 2013OnlineFirst Version of Record
- Jun 10, 2013Version of Record >>
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from

Lupus (2013) 22, 690–696
http://lup.sagepub.com
PAPER
Clinical presentations and outcomes of systemic lupus
erythematosus patients with infection admitted to the intensive
care unit
BK Han1,*, R Bhatia1, P Traisak1, K Hunter2, B Milcarek2, C Schorr3, H Eid1, D Feinstein1,P Cronin1 and SL Kolasinski1
1Division of Rheumatology, 2Department of Biostatistics, 3Department of Internal Medicine, Cooper Medical School of Rowan University, USA
Objective: The objective of this article is to investigate clinical presentations and outcomes ofsystemic lupus erythematosus (SLE) patients with infection admitted to the intensive care unit(ICU). Methods: SLE patients with infection, SLE patients with noninfectious causes, andnon-SLE patients with infection were identified from the Cooper University Hospital ProjectIMPACT database between 2002 and 2010. We examined demographic data, APACHE IIscores, physiologic data, laboratory data, length of stay in the ICU and hospital, and mortalityof the three groups. Results: Twenty-five SLE patients with infection, 45 SLE patients withnoninfectious causes, and 1466 non-SLE patients with infection were included in the study.SLE patients with infection had higher APACHE II scores, higher maximum temperature,higher minimum and maximum heart rate (HR), lower minimum and maximum systolic bloodpressure (SBP), and longer ICU length of stay in comparison to SLE patients with noninfec-tious causes. There were no statistical differences in white blood cell (WBC) count. SLEpatients with infection had a higher mortality compared to SLE patients with noninfectiouscauses. There was no difference in mortality between SLE patients with infection and non-SLEpatients with infection. Conclusion: SLE patients with infection in the ICU had a highermortality and a higher APACHE II score compared to SLE patients with noninfectiouscauses in the ICU. Their physiologic signs including temperature, HR, and SBP were morereflective of infection than their WBC count. Lupus (2013) 22, 690–696.
Key words: Systemic lupus erythematosus; infection
Introduction
Systemic lupus erythematosus (SLE) is a multisys-tem disease caused by tissue damage resulting fromantibody and complement-fixing immune complexdeposition. There is a wide spectrum of clinicalpresentations that are characterized by remissionsand exacerbations.1
SLE patients are at an increased risk for infectiondue both to the disease and the use of immunosup-pressive agents. According to one study, 108 out of137 SLE patients (79%) had serious infections eventhough they took glucocorticoids and otherimmunosuppressive agents sparingly. Infectionsdocumented in this study were usually associated
with disease exacerbations.2 In a population-basedstudy, a significant increase in bacterial infectionswas observed in SLE patients as compared to anage- and gender-matched cohort of normal con-trols.3 Many immune abnormalities in SLE, includ-ing complement deficiency,4–6 defects inchemotaxis,7 and phagocytic activity,8,9 mayaccount for the susceptibility for infection.
Immunosuppressive agents such as glucocortic-oids are a risk factor for infection in SLE patients.A study showed that the infection rate in hospita-lized patients increased from 0.43 to 1.63 per 100hospital days with an increase in glucocorticoiddose from zero to more than 50mg/d.10 In anotherstudy, a fivefold increase in the frequency of allinfections was found as average prednisone doseincreased from zero to greater than 40mg/d.11
It is known that some SLE patients developsevere acute illnesses and require admission to theintensive care unit (ICU). Infection is one of themost common causes for admission to the ICU.
*B.K.H. and R.B. contributed equally to this paper.
Correspondence to: Bobby Kwanghoon Han, 900 Centennial Blvd.,
Bldg 2, Ste 201, Voorhees, NJ 08043, USA.
Email: [email protected]
Received 17 August 2012; accepted 20 April 2013
! The Author(s), 2013. Reprints and permissions: http://www.sagepub.co.uk/journalsPermissions.nav 10.1177/0961203313490240
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from

Patients with SLE may have vague clinical signsand symptoms due to their impaired immuneresponses to infection and this can delay interven-tions including treatment in the ICU. In this retro-spective study, we examined clinical presentationsand outcomes of patients with SLE who wereadmitted to the ICU for infection and comparedthem to SLE patients who were admitted for non-infectious causes and to non-SLE patients whowere admitted with infection.
Patients and methods
SLE patients with sepsis or respiratory infection(Group A), a comparison group of SLE patientswith noninfectious causes (Group B), and anothercomparison group of non-SLE patients with sepsisor respiratory infection (Group C) admitted toCooper University Hospital Medical ICU wereidentified from the Cooper University HospitalProject International Mission for Prognosis andAnalysis of Clinical Trials (IMPACT) databasebetween January 1, 2002, and December 31, 2010.Project IMPACT (Cerner Corporation, KansasCity, MO) is a nationally representative, voluntary,fee-based database system used to measure anddescribe the care of intensive care patients. It wasinitially developed by a multidisciplinary group ofcritical care expert members of the Society ofCritical Care Medicine. Participating institutionsupload data quarterly to a central repository.Data fields include hospital and ICU organiza-tional characteristics, admission source, demo-graphics, physiological data (includinghemodynamic indices and laboratory values), pro-cedures, complications, hospital and ICU length ofstay, and outcomes. All data are collected by dedi-cated onsite personnel who are trained and certifiedby Project IMPACT. Only those patients who ful-filled the American College of Rheumatology(ACR) criteria for classification of SLE12 afterchart review were included in Group A andGroup B of this study.
Data collection
The patients who met the following inclusion andexclusion criteria were included in this study.Group A inclusion criteria were: 1) age greaterthan 18 years old; 2) presence of clinical diagnosisof SLE (ICD9 CM 710.0) according to ACR cri-teria; and 3) admitted to ICU with sepsis or respira-tory infection. Group B inclusion criteria were: 1)age greater than 18 years old; 2) presence of clinical
diagnosis of SLE (ICD9 CM 710.0) according toACR criteria; and 3) admitted to ICU with nonin-fectious causes. Group C inclusion criteria were: 1)age greater than 18 years old; 2) no clinical diagno-sis of SLE (ICD9 CM 710.0), rheumatoid arthritis(RA) (714.0), psoriatic arthritis (696.0), ankylosingspondylitis (720.0), systemic sclerosis (710.1), poly-myositis (710.4), dermatomyositis (710.3), sarcoid-osis (135), vasculitis (446.29), Wegenersgranulomatosis (446.4), Churg Strauss syndrome(446.4), cryoglobulinemic vasculitis (273.2),Henoch-Schonlein purpura (287.0), polyarteritisnodosa (446.0), Kawasaki disease (446.1), primarycentral nervous system (CNS) angiitis, giant cellarteritis (446.5), and Takayasu’s arteritis (446.7);and 3) admitted to ICU with sepsis or respiratoryinfection.
Exclusion criteria for all groups were: 1) historyof malignancy within the past five years; 2) historyof viral hepatitis (ICD9 CM 070) such as hepatitisB or C; and 3) history of human immunodeficiencyvirus (HIV) (ICD9 CM 042).
The following information was abstracted fromthe Cooper University Hospital Project IMPACTdatabase: demographic data (age, gender), acutephysiology and chronic health evaluation II(APACHE II) scores, physiologic data (tempera-ture, heart rate (HR), systolic blood pressure(SBP)), laboratory data (white blood cell (WBC)count, hematocrit, creatinine (Cr)), comorbidities,length of stay in the ICU, length of stay in thehospital, and mortality. The Cooper UniversityHospital Project IMPACT data set included entryof the maximum and minimum value of all physio-logic and laboratory data within the first 24 hoursof ICU admission. APACHE II is a type of ICUscoring system applied within 24 hours of admis-sion of a patient to an ICU. A score from 0 to 71 iscomputed based on several measurements. The cal-culation of the APACHE II score was based on theworst physiological variables (furthest from themean) collected in the first 24 hours.
The following additional information on SLEpatients in both the infection and the noninfectiouscauses group was obtained from chart review: dis-ease duration, clinical manifestations of SLE, andtreatments prior to admission.
Statistical analysis
Mann Whitney U (median difference) Pearson chisquare and Fisher’s exact tests were used for allunivariate significance tests. Multivariable logisticregression was used to estimate unadjusted and
Clinical presentations and outcomes of SLEBK Han et al.
691
Lupus
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from

adjusted effects on odds of mortality betweenGroup A and Group C.
Results
Twenty-five SLE patients with infection (Group A)and 45 SLE patients with noninfectious causes(Group B) were admitted to the ICU at CooperUniversity Hospital from January 2002 toDecember 2010. The mean age of SLE patientswith infection was 49.2 (41.0–57.5) years withmean lupus disease duration of 95.7 (49.1–143.3)months. The mean age of SLE patients with nonin-fectious causes was 42.8 (37.5–48.1) years with meanlupus disease duration of 121.6 (80.8–162.4) months.The majority in both groups was female (Group A80.0% (61%–92.3%), Group B 88.9% (77%–95.8%)). The overall characteristics were similar inboth groups. For this study, active SLE was definedas either having active SLE symptoms or requiringprednisone greater than 7.5mg/d or immunosup-pressive agents based on chart review, and the pro-portion of patients with active SLE was similar inboth groups. The SLE group with infection receivedmore immunosuppressive treatments and hydroxy-chloroquine in comparison to the SLE group withnoninfectious causes but this was not statisticallysignificant. Additionally, there was a trend towardmore pleuritis in the SLE group with noninfectiouscauses admitted to the ICU (Table 1).
ICU admission diagnoses for the SLE groupwith infection were pneumonia 10, urosepsis four,sepsis four, colon perforation four, septic thrombo-phlebitis one, necrotizing fasciitis one, and sub-acute bacterial endocarditis one. Their causativeagents were E coli three, K. pneumoniae one, methi-cillin-resistant S aureus three, vancomycin-resistantenterococcus one, group A streptococcus one, Spneumoniae one, proteus one, acinetobacter one,and unidentified (culture negative or undocu-mented) 13 (Table 2).
ICU admission diagnoses for the SLE groupwith noninfectious causes were lupus nephritistwo, cerebral hemorrhage two, cerebral infarctionone, seizures three, pulmonary alveolar hemor-rhage two, pleural or pericardial effusion three,catastrophic antiphospholipid syndrome one,aortic dissection two, mitral regurgitation one, con-gestive heart failure one, asthma one, chronicobstructive pulmonary disease one, gastrointestinalbleeding two, hemoperitoneum two, uterine bleed-ing one, retroperitoneal hematoma one, pseudoa-neurysm one, Guillain Barre syndrome one,
angioedema one, epidural hematoma one, adrenalinsufficiency one, vertebral compression fractureone, opioid overdose two, altered mental statustwo, and post-operation care nine.
In the comparison to 1466 patients in the non-SLE with infection group (Group C), SLE patientswith infection (Group A) were younger (49.2 (41.0–57.5) years vs 62.6 (61.7–63.5) years, p< 0.01) andmore likely to be female (80.0% (61.1%–92.3%) vs
Table 1 Baseline characteristics of SLE-infected group and
SLE-noninfected group
SLE infected(n¼ 25)
SLE noninfected(n¼ 45) p value
Age, mean (SD) 49.2 (20.2) 42.8 (17.5) 0.18
Male sex, n (%) 5 (20.0) 5 (11.1) 0.48
SLE disease duration inmonths (SD)
95.7 (87.5) 121.6 (118.9) 0.44
SLE activea, n (%) 19 (76.0) 31(68.9) 0.52
SLE treatment prior toadmission, n (%)
Prednisone 17 (68.0) 23 (51.1) 0.17
Cyclophosphamide 2 (8.0) 4 (8.9) 1.00
Other immunosuppressivetreatments
7 (28.0) 8 (17.8) 0.32
Hydroxychloroquine 11 (44.0) 10 (22.2) 0.06
Rash, n (%) 8 (32.0) 18 (40.0) 0.51
Photosensitivity, n (%) 3 (12.0) 8 (17.8) 0.74
Oral sores, n (%) 4 (16.0) 7 (15.6) 1.00
Arthritis, n (%) 15 (60.0) 27 (60.0) 1.00
Lupus nephritis, n (%) 12 (48.0) 24 (53.3) 0.67
Pleurisy/serositis, n (%) 3 (12.0) 11(24.4) 0.21
Thrombocytopenia, n (%) 6 (24.0) 15 (33.3) 0.42
SLE: systemic lupus erythematosus; SD: standard deviation; for SLE
disease duration, n¼ 16 for SLE-infected group and n¼ 35 for SLE-
noninfected group. aActive SLE was defined as having active SLE
symptoms or requiring prednisone greater than 7.5mg/d or immuno-
suppressive treatments.
Table 2 Infectious agents and their source of infection in the
SLE patients with infection group
Infectious agents Source
E. coli Urosepsis
E. coli Urosepsis
E. coli Colon perforation
K. pneumoniae Colon perforation
Methicillin-resistant S. aureus Necrotizing fasciitis
Methicillin-resistant S. aureus Sepsis
Methicillin-resistant S. aureus Pneumonia
Vancomycin-resistant enterococcus Urosepsis
Group A streptococcus Thrombophlebitis
S. pneumoniae Sepsis
Proteus Pneumonia
Acinetobacter Sepsis
SLE: systemic lupus erythematosus.
Clinical presentations and outcomes of SLEBK Han et al.
692
Lupus
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from

48.2% (45.6%–50.7%), p< 0.01). The percentagesof co-morbidities were similar in the SLE groupwith infection and the non-SLE group with infec-tion; hypertension (48.0% (29.2%–67.2%) vs60.6% (58.1%–63.1%), p¼ 0.10), diabetes mellitus(28% (10.5%–45.5%) vs 40.1% (37.6%–42.6%),p¼ 0.17), congestive heart failure (32% (16.1%–51.9%) vs 23.1% (21%–25.3%), p¼ 0.73).
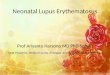
SLE patients with infection had significantlylonger ICU length of stay, higher APACHE IIscores, higher maximum temperature, higher min-imum and maximum HR and lower minimum andmaximum SBP in comparison to the SLE with non-infectious causes group. There was a trend towardhigher minimum and maximum WBC and higherminimum and maximum Cr in the SLE with infec-tion group in comparison to the SLE with nonin-fectious causes group. However, this was notstatistically significant (Table 3). The distributionof WBC count was generally less than 15,000/mlin the SLE group with infection (Figure 1).Among 24 SLE patients with infection, 63% (15/24) had a maximum WBC count less than 15,000/mland 38% (nine of 24) had a WBC count less than11,000/ml. The two patients who received cyclo-phosphamide in the SLE group with infection didnot have leukopenia. Among the four patients whoreceived cyclophosphamide in the SLE group withnoninfectious causes, one patient had leukopenia.A history of lupus nephritis was present in 89%(17/19) of SLE patients with noninfectious causes
who had a maximum Cr greater than 1.2mg/dl andin 55% (six of 11) of SLE patients with infectionwho had a maximum Cr greater than 1.2mg/dl.
Survivor and nonsurvivor data were evaluated inboth the SLE with infection and the SLE with non-infectious causes groups. Nonsurvivor patients fromthe SLE with infection group had higher APACHEII scores and lower minimum temperature.Nonsurvivor patients from the SLE with noninfec-tious causes group had higher APACHE II scoresand higher minimum and maximum Cr (Table 4).
Table 3 Physiologic data comparison between SLE-infected group and SLE-noninfected group
SLE infected (n¼ 25) SLE noninfected (n¼ 45)
p valueMedian IQR Median IQR
APACHE II 19.0 15.5–23.0 15.0 10.5–17.5 <0.01a
HR min 86.0 70.0–98.0 70.0 62.5–82.5 <0.01a
HR max 116.0 100.5–128.0 104.0 96.0–117.5 0.03a
SBP min 83.5 78.5–87.0 96.0 87.0–115.0 <0.01a
SBP max 138.0 122.5–156.0 155.0 137.5–164.5 0.02a
Temp min 36.5 36.1–36.8 36.4 36.2–36.8 0.71
Temp max 37.7 37.2–38.9 37.3 37.0–37.4 0.04a
WBC min 11.0 6.6–14.8 9.1 7.1–13.6 0.40
WBC max 13.7 8.2–18.4 11.1 8.5–15.5 0.37
HCT min 26.6 23.0–32.3 26.6 22.4–31.4 0.75
HCT max 31.0 26.3–34.8 28.5 25.8–32.2 0.23
CR min 1.2 0.8–2.7 0.9 0.6–3.5 0.54
CR max 1.5 0.9–3.9 1.0 0.7–3.6 0.44
ICU LOS 2.91 1.99–7.13 1.65 0.85–4.72 0.03a
HOSP LOS 10.0 5.0–29.5 15.0 8.0–22.5 0.55
SLE: systemic lupus erythematosus; APACHE II: acute physiology and chronic health evaluation II; HR: heart rate; SBP:
systolic blood pressure; Temp: temperature; WBC: white blood cell count; HCT: hematocrit, CR: creatinine; min: minimum,
max: maximum; ICU: intensive care unit; HOSP: hospital; LOS: length of stay. For APACHE II, n¼ 22 for SLE infected,
n¼ 37 for SLE noninfected. For temp, values are mean with standard deviation (SD) instead of median with interquartile
range (IQR). ap� 0.05.
Age (years)
WB
C (
103 /
ml)
0 20 40 60 80 1000
10
20
30
40
Figure 1 Distribution of maximum WBC count in SLEpatients admitted for infection.WBC: white blood cell; SLE: systemic lupus erythematosus.
Clinical presentations and outcomes of SLEBK Han et al.
693
Lupus
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from

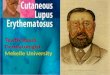
There were no statistically significant differencesin any of the parameters evaluated among the SLEgroup with infection and the non-SLE with infec-tion group. Mortality was 40.0% (22.4%–59.8%)in the SLE with infection group, 11.1% (4.2%–22.9%) in the SLE with noninfectious causesgroup and 31.8% (29.4%–34.2%) in the non-SLEwith infection group (Figure 2). There wasincreased risk of mortality in the SLE group withinfection relative to the SLE with noninfectiouscauses group that was statistically significant(p< 0.01). There was no difference in mortalityunadjusted for age and gender (p¼ 0.39, oddsratio (OR)¼ 1.43, 95% confidence interval(CI)¼ 0.64–3.21) and in mortality adjusted forage and gender (p¼ 0.27, OR¼ 1.67, 95%CI¼ 0.67–4.15) between the SLE with infectiongroup and the non-SLE with infection group.
Discussion
In this study, we examined clinical data of SLEpatients who were admitted to the ICU for infec-tion. Infection was one of the most common causesfor ICU admission. Among the 70 SLE patientshospitalized in the ICU and found in the CooperUniversity Hospital Project IMPACT databasebetween 2002 and 2010, 35.7% (25/70) wereadmitted with infection. The result was consistentwith several other studies that showed infection as a
main cause for ICU admission in patients withrheumatic diseases including SLE.13–16
In the comparison between SLE patientsadmitted to the ICU for infection and SLE patientsadmitted for noninfectious causes, we found thatthe overall baseline clinical characteristics weresimilar in both groups. SLE patients have anincreased risk for infection due to their inherentimmune system abnormalities; however, this does
Table 4 Survivor and nonsurvivor physiologic data comparison in SLE-infected group and SLE-noninfected group
SLE infected (n¼ 25)
p value
SLE noninfected (n¼ 45)
p valueSurvivor (n¼ 15) Nonsurvivor (n¼ 10) Survivor (n¼ 40) Nonsurvivor (n¼ 5)
APACHE II 17.0 (14.0–20.0) 23.0 (19.0–33.0) <0.01a 14.0 (10.0–16.0) 24.0 (17.5–31.0) <0.01a
HR min 90.0 (69.0–99.0) 82.0 (71.0–99.0) 1.00 71.5 (63.3–83.0) 68.0 (55.0–73.0) 0.13
HR max 118.0 (110.0–134.0) 112 (90.0–129.8) 0.43 104.5 (97.3–117.8) 96.0 (82.5–125.0) 0.31
SBP min 85.0 (80.0–87.0) 80.0 (77.5–90.0) 0.52 96.0 (87.8–116.8) 95.0 (81.5–115.5) 0.69
SBP max 134.0 (119.0–160.0) 138 (133.5–156.3) 0.50 154.5 (136.3–164.0) 161.0 (141.0–211.0) 0.45
Temp min 36.7 (36.3–36.9) 36.0 (34.7–36.5) <0.01a 36.5 (36.2–36.8) 35.9 (35.8–36.8) 0.26
Temp max 37.6 (37.1–39.0) 37.7 (37.2–38.6) 0.95 37.3 (37.0–37.7) 37.1 (36.8–38.3) 0.66
WBC min 12.9 (8.3–15.1) 8.5 (4.4–16.7) 0.48 9 (6.9–13.0) 13.7 (8.4–16.6) 0.15
WBC max 13.6 (8.3–15.6) 15.4 (6.9–19.3) 0.73 11 (8.2–15.3) 14.8 (9.4–20.1) 0.30
HCT min 26.3 (22.0–30.9) 28 (23.9–32.8) 0.48 26.5 (22.4–31.2) 29.1 (18.9–33.9) 0.56
HCT max 26.8 (25.4–34.8) 32.3 (30.5–35.2) 0.12 28.5 (25.6–32.3) 30.6 (23.9–37.5) 0.82
CR min 1.1 (0.9–2.5) 1.5 (0.6–3.5) 0.86 0.8 (0.5–2.0) 5.0 (2.2–10.4) 0.01a
CR max 1.4 (0.9–4.2) 1.8 (0.7–4.4) 0.91 0.9 (0.6–2.4) 5.1 (2.2–10.7) 0.02a
ICU LOS 3.0 (2.0–7.8) 2.9 (2.0–4.6) 0.64 1.7 (0.9–4.6) 4.32 (0.85–7.78) 0.84
HOSP LOS 24 .0 (9.0–31.0) 6.5 (3.5–14.5) 0.05a 13.5 (7.3–22.0) 20.0 (12.0–44.5) 0.28
SLE: systemic lupus erythematosus; APACHE II: acute physiology and chronic health evaluation II; HR: heart rate; SBP: systolic blood pressure;
Temp: temperature; WBC: white blood cell count; HCT: hematocrit; CR: creatinine; min: minimum; max: maximum; ICU: intensive care unit;
HOSP: hospital; LOS: length of stay. For APACHE II, n¼ 7 for SLE-infected nonsurvivor, n¼ 32 for SLE-noninfected survivor. For temp, values
are mean with standard deviation (SD) instead of median with interquartile range (IQR). ap� 0.05.
0
SLE infecte
d
SLE non-infecte
d
non-SLE infecte
d
10
20
30
40
50
Mo
rtal
ity
(%)
Figure 2 Mortality in SLE patients with infection, SLEpatients with no infection and non-SLE patients with infection.The p value was <0.01 for the SLE-infected versus SLE-non-infected group and 0.39 for the SLE-infected versus non-SLE-infected group.SLE: systemic lupus erythematosus.
Clinical presentations and outcomes of SLEBK Han et al.
694
Lupus
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from

not appear to be associated with any particularclinical features according to our data. Regardingtreatments, both groups had a similar percentage ofprednisone and cyclophosphamide treatments. Theuse of other immunosuppressive agents includingmethotrexate, azathioprine, and mycophenolatemofetil was numerically higher in SLE patientsadmitted for infection but it was not statisticallysignificant. The percentages of patients who weretaking hydroxychloroquine were low in bothgroups. We found that many patients who weretaking immunosuppressive agents did not takehydroxychloroquine (data not shown).
The study demonstrated that SLE patients wereable to have appropriate physiologic responses toinfection. SLE patients with infection had highermaximum temperature, higher minimum and max-imum HR, and lower minimum and maximum SBPcompared to SLE patients with noninfectiouscauses. However, their WBC count was not statis-tically different. In our analysis, many SLE patientsadmitted for infection had normal or mildly ele-vated WBC count. It is possible that SLE patientsdo not generate a robust increase in WBC countbecause of their preexisting leukopenia andimmunosuppressive treatments.
Neutropenia is common in SLE patients.17
Neutrophils undergo a process called NETosis,which is a specialized form of cell death character-ized by rupture of cellular membranes and expul-sion of a mesh-like structure termed a neutrophilextracellular trap (NET).18 A recent study demon-strated that increased NETosis of neutrophils wasobserved in lupus patients and that abundant auto-antigens including double-stranded DNA (dsDNA)present in the NET released from neutrophils arehypothesized to trigger autoimmunity.19 The asso-ciation between leukopenia and infection in SLE isnot well studied. In one study, a low WBC count inSLE patients at admission is a risk factor for a pooroutcome in the ICU.15 It is possible that a normalWBC count in SLE patients could delay the diag-nosis of an infection. Another recent study showedthat inadequate antimicrobial treatment is a riskfactor for mortality in SLE patients admitted tothe ICU.20
SLE patients with infection had a higherAPACHE II score and a higher mortality com-pared to SLE patients with noninfectious causes.Several studies have shown that infection is amain cause of death in the ICU.15,21 Among SLEpatients with infection, nonsurvivors had higherAPACHE II scores. Many previous studiesshowed that APACHE II scores were associatedwith mortality.16,21–25 Of note, serum Cr and SBP
were significantly higher in nonsurvivors amongSLE patients with noninfectious causes and thissuggests that lupus nephritis is a major risk factorfor mortality in this group. It was supported by thefact that most of patients with elevated Cr in theSLE group with noninfectious causes had a historyof lupus nephritis. Several other studies haveshowed renal involvement due to lupus predicts apoor outcome.14,15,26
In the comparison between SLE patientsadmitted for infection and non-SLE patientsadmitted for infection, SLE patients were signifi-cantly younger, with more females than the non-SLE patients who were admitted for infection.There was no difference in mortality between thetwo groups before and after adjustment for age andgender. Previous studies showed inconsistentresults. Patients with rheumatic diseases includingSLE had a similar mortality compared to nonse-lected patients in the ICU in several studies,13,15,27
whereas they had a higher mortality in one study.14
Age is one of the major prognostic factors in theICU.28 SLE patients with infection had a numeric-ally higher mortality compared to non-SLEpatients with infection even if they were younger.It is likely that an insufficient number of subjects inthe SLE group with infection led to the lack ofstatistical difference in the mortality between thetwo groups.
This study is the first to our knowledge thatexamined a subgroup of SLE patients who areadmitted to the ICU for infection. Our study hasseveral limitations. First, our data were retrievedfrom a single tertiary-care medical center. As aresult, it was difficult to obtain sufficient numbersof patients for analysis and the results may not beapplicable to hospitals in other areas. Secondly, ourstudy is a retrospective study that is subject to mul-tiple potential biases, including unavailability ofcertain data. In addition, we were unable toobtain the validated SLE activity scores, includingSystemic Lupus Erythematosus Disease ActivityIndex (SLEDAI) or European Consensus LupusActivity Measurement (ECLAM) for the patients.We noted many patients who were labeled ashaving SLE did not meet criteria and excludedthose patients from our study. Further prospectivestudies are warranted to examine risk factors aswell as long-term prognosis of SLE patients withserious infections.
In conclusion, this study showed that SLEpatients admitted to the ICU for infection had ahigher mortality and a higher APACHE II scorecompared to SLE patients with noninfectiouscauses in the ICU. SLE patients had appropriate
Clinical presentations and outcomes of SLEBK Han et al.
695
Lupus
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from

physiologic signs in response to infection, includingincreased temperature, increased HR, anddecreased SBP. However, WBC count was normalor mildly elevated in many patients. Our data raisethe possibility that WBC count is misleading indiagnosing infection in SLE patients admitted tothe ICU.
Funding
This research received no specific grant from anyfunding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.
References
1 Grossman JM, Kalunian KC. Definition, classification, activity anddamage indices. In: Wallace DJ, Hahn BH (eds), Dubois’ lupus ery-thematosus, 6th ed. Philadelphia, PA: Lippincott Williams&Wilkins, 2002. p. 19–31.
2 Ropes NW. Systemic lupus erythematosus. Cambridge, MA:Harvard University Press, 1976.
3 Nived O, Sturfelt G, Wolhein F. Systemic lupus erythematosus andinfection: A controlled and prospective study including an epidemio-logic group. Q J Med 1985; 218: 271–287.
4 Lee SL, Wallace SL, Barone R, Blum L, Chase PH. Familial defi-ciency of two subunits of the first component of complement. C1rand C1s associated with lupus erythematosus-like disease. ArthritisRheum 1978; 21: 958–967.
5 Hyatt AC, Altenburger KN, Johnston RB, Winkelstein JA.Increased susceptibility to severe pyogenic infections in patientswith an inherited deficiency of the second component of comple-ment. J Pediatr 1981; 98: 417–419.
6 Mascart-Lemone F, Hauptmann G, Goetz J, et al. Genetic defi-ciency of C4 presenting with recurrent infections and a SLE-likedisease. Am J Med 1983; 75: 295–304.
7 Perez HD, Andron RI, Goldstein IM. Infection in patients withsystemic lupus erythematosus. Association with a serum inhibitorof complement-derived chemotactic activity. Arthritis Rheum 1979;22: 1326–1333.
8 Martınez-Cairo Cueto S, Ramırez-Lacayo ML, Veladiz-Saint-Martin P, Lopez-Roman M. Deterioration of intracellulardestruction capacity of S. aureus in children with systemiclupus erythematosus [in English and Spanish]. Arch InvestMed (Mex) 1986; 17: 25–36.
9 Roberts PJ, Isenberg DA, Segal AW. Defective degradation of bac-terial DNA by phagocytes from patients with systemic and discoidlupus erythematosus. Clin Exp Immunol 1987; 69: 68–78.
10 Staples PJ, Gerding DN, Decker JL, Gordon Jr RS. Incidence ofinfection in systemic lupus erythematosus. Arthritis Rheum 1974;17: 110.
11 Ginzler E, Diamond H, Kaplan D, Weiner M, Schlesinger M,Seleznick M. Computer analysis of factors influencing frequencyof infection in systemic lupus erythematosus. Arthritis Rheum 1978;21: 37–44.
12 Tan EM, Cohen AS, Fries JF, et al. The 1982 revised criteria forthe classification of systemic lupus erythematosus. Arthritis Rheum1982; 25: 1271–1277.
13 Godeau B, Boudjadja A, Dhainaut JF, et al. Outcome of patientswith systemic rheumatic disease admitted to medical intensive careunits. Ann Rheum Dis 1992; 51: 627–631.
14 Janssen NM, Karnad DR, Guntupalli KK. Rheumatologic dis-eases in the intensive care unit: Epidemiology, clinical approach,management, and outcome. Crit Care Clin 2002; 18: 729–748.
15 Williams FM, Chinn S, Hughes GR, Leach RM. Critical illness insystemic lupus erythematosus and the antiphospholipid syndrome.Ann Rheum Dis 2002; 61: 414–421.
16 Namendys-Silva SA, Baltazar-Torres JA, Rivero-Sigarroa E,Fonseca-Lazcano JA, Montiel-Lopez L, Domınguez-Cherit G.Prognostic factors in patients with systemic lupus erythematosusadmitted to the intensive care unit. Lupus 2009; 18: 1252–1258.
17 Budman DR, Steinberg AD. Hematologic aspects of systemiclupus erythematosus. Current concepts. Ann Intern Med 1977; 86:220–229.
18 Kaplan MJ. Neutrophils in the pathogenesis and manifestations ofSLE. Nat Rev Rheumatol 2011; 7: 691–699.
19 Garcia-Romo GS, Caielli S, Vega B, et al. Netting neutrophils aremajor inducers of type I IFN production in pediatric systemiclupus erythematosus. Sci Transl Med 2011; 3: 73ra20.
20 Feng PH, Lin SM, Yu CT, et al. Inadequate antimicrobial treat-ment for nosocomial infection is a mortality risk factor for systemiclupus erythematous patients admitted to intensive care unit. Am JMed Sci 2010; 340: 64–68.
21 Moreels M, Melot C, Leeman M. Prognosis of patients with sys-temic rheumatic diseases admitted to the intensive care unit.Intensive Care Med 2005; 31: 591–593.
22 Kollef MH, Enzenauer RJ. Predicting outcome from intensive carefor patients with rheumatologic diseases. J Rheumatol 1992; 19:1260–1262.
23 Alzeer AH, Al-Arfaj A, Basha SJ, et al. Outcome of patients withsystemic lupus erythematosus in intensive care unit. Lupus 2004;13: 537–542.
24 Camargo JF, Tobon GJ, Fonseca N, et al. Autoimmune rheumaticdiseases in the intensive care unit: Experience from a tertiary refer-ral hospital and review of the literature. Lupus 2005; 14: 315–320.
25 Anton JM, Castro P, Espinosa G, et al. Mortality and long termsurvival prognostic factors of patients with systemic autoimmunediseases admitted to an intensive care unit: A retrospective study.Clin Exp Rheumatol 2012; 30: 338–344.
26 Ansell SM, Bedhesi S, Ruff B, et al. Study of critically ill patientswith systemic lupus erythematosus. Crit Care Med 1996; 24:981–984.
27 Ozbalkan Z, Topeli A, Kiraz S, Ozturk MA, Ertenli I, CalguneriM. The contribution of underlying systemic rheumatic diseases tothe mortality in patients admitted for intensive care: A matchedcohort study. Clin Exp Rheumatol 2004; 22: 223–226.
28 The French Multicenter Group for ICU Research. The Inserm unit169 of statistical and epidemiological studies: Factors related tooutcome in intensive care: French multicenter study. Crit CareMed 1989; 17: 305–308.
Clinical presentations and outcomes of SLEBK Han et al.
696
Lupus
at UNIV OF CONNECTICUT on January 6, 2014lup.sagepub.comDownloaded from