Embed Size (px)
Citation preview

PT-INR延長時の対応 (非弁膜症性の心房細動でワーファリン内服中)
筑波大学附属病院 総合診療科 作成 大澤 亮 監修 五十野 博基
Clinical question 2015年5月8日
JHOSPITALIST network
分野:循環器
テーマ:治療
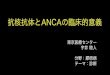
症例 88歳女性【現病歴】特別養護老人ホーム入所中で、非弁膜症性の心房細動(Af)がありWarfarin(WF)投与されていた方。ADLは全介助で、意志の疎通は困難。今回、発熱と炎症反応高値を認め、尿路感染症が疑われ入院となった。入院時の血液検査でPT-INRが測定不能であった。
【既往歴】脳梗塞(左片麻痺),尿路感染症,誤嚥性肺炎, 急性心不全
【内服歴】WF 2.5mg(最終確認半年前:INR2.75), フロセミド20mg, スピロノラクトン25mg, カルベジロール2.5mg
【身体所見】146cm, 33kg,BMI 15.5,JCS Ⅱ-2,認知症FAST:7d
体温 37.3℃,血圧 117/89mmHg,脈拍 89/min 不整,呼吸数 16/min
呼吸音:異常なし,腹部:平坦 軟 圧痛なし 腸蠕動音はやや低下,四肢に浮腫なし
【検査所見】Hb 10.9 g/dL, Plt 18万/μL, PT-INR/APTT:測定不能(日本ではINR≧10で測定不能となる事が多い) , eCCr 40ml/min(Cockcroft-Gault), CRP:14mg/dL
(認知症患者の医療倫理についても、検討を要する症例であるが、今回は医原性のINR過延長に焦点をしぼった)
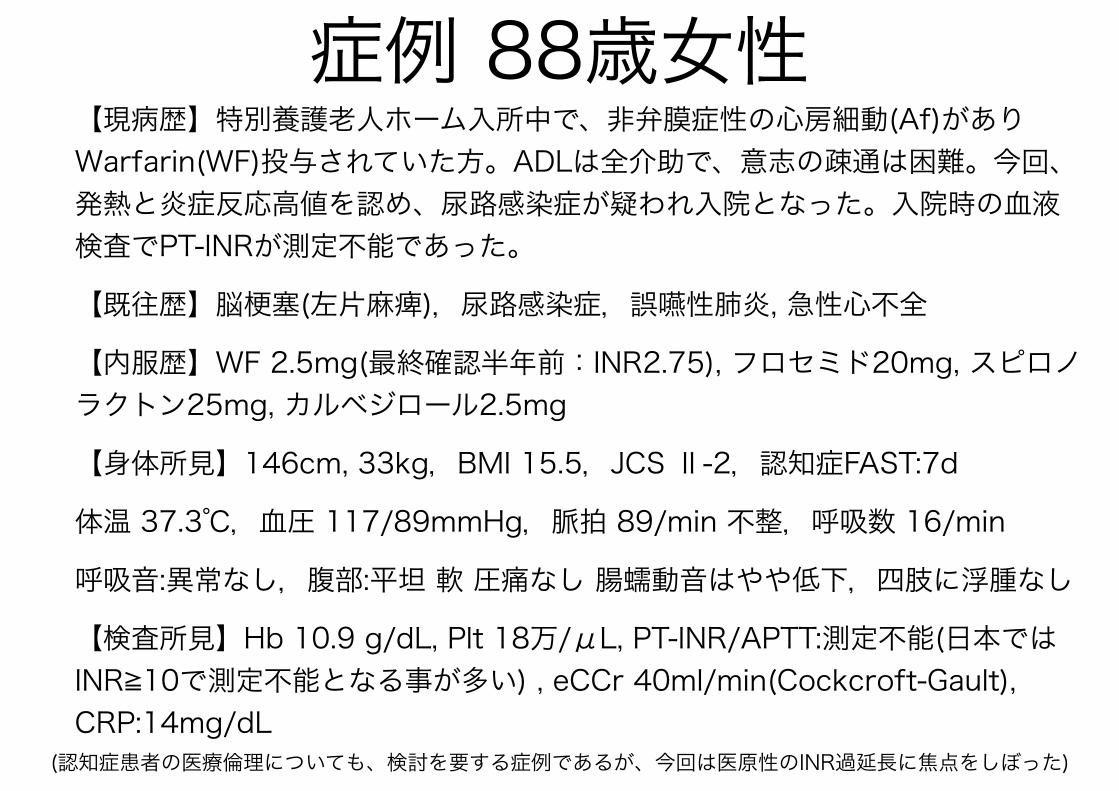
Clinical QuestionPT-INRが過延長したWF内服患者に対して
• Vit Kをつかう? • 使うならDiv or 内服? • どの位の量のVit KやFFPを使う? • follow upはどのタイミング?

BMJ 2015⑴出血(消化管出血や頭部外傷の既往)の有無を確認
⑵内服しているWF量の確認
⑶INR延長/出血リスク要因を分析:肝疾患、癌、食生活の変化、飲酒、薬物の相互作用をチェックする
Table
Table 1| Summary of the management of supra-therapeutic warfarin levels3 4
Bleeding*Not bleedingINR
Minor: stop warfarin and apply first aid measures; give1-3 mg intravenous vitamin K if bleeding does not stop
with such measures
Reduce warfarin dose; re-check INR in 48 hours†3.0-5.0
Omit warfarin until INR <5.0, then start reduced dose; re-checkINR in 48 hours†
5.0-8.0
Limb or life threatening: refer to secondary care forwarfarin reversal
Omit warfarin, give 1-5 mg oral vitamin K; re-check INR in 24hours†
>8.0
*The management of all types of bleeding applies to all INR categories.†Advice on when to recheck INR values is based on the authors’ experience and the half life of warfarin and vitamin K.INR=international normalised ratio.
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2015;350:h1282 doi: 10.1136/bmj.h1282 (Published 9 April 2015) Page 3 of 3
PRACTICE
<INR値とBleedingの有無を指標として対応>
BMJ 2015;350:h1282
Circulation 2012degrees of INR correction.7 Subcuta-neous vitamin K should not be usedbecause it is less effective than oral orintravenous vitamin K; at 24 hoursafter treatment with low-dose subcuta-neous vitamin K, fewer than 50% ofpatients will achieve an INR between1.8 and 4.0.6,8 We suggest 2 optionsfor administering oral vitamin K: Ei-ther give one quarter to one half of a5-mg tablet or add 1 to 2 mg of theintravenous preparation to a cup oforange juice. There is high-quality ev-idence that either method is effectivefor INR correction.1,9
An 86-year-old man is hospitalizedwith choledocholithiasis and biliaryobstruction. He is scheduled to un-dergo endoscopic retrograde cholan-giopancreatography with attemptedstone retrieval in !24 hours. He takeswarfarin for atrial fibrillation. His INRis currently 2.3, and his hepatic syn-thetic function appears to be normal.What is the optimal strategy to nor-malize his INR?
For warfarin-treated patients whoneed to undergo a semiurgent (within24–36 hours) procedure, low-dose oralvitamin K, given the day before theintervention, will often achieve suffi-cient INR correction and avoid theneed for transfusion. In a study of 2parallel cohorts of patients assessed ina perioperative anticoagulation man-agement clinic, all patients had theirwarfarin held 5 days before surgery.For patients whose INR was 1.4 to 1.9the day before surgery, 1 mg of oralvitamin K was given. Thirty-nine(90.7%) of the 43 individuals in thiscohort had an INR "1.5 the next day,and there was no difficulty reestab-lishing anticoagulation with warfarinafter the procedure.10 A study ofanticoagulated patients who wereplanning to discontinue warfarinyielded similar findings. One milli-gram of oral vitamin K, given on theday of discontinuation, produced anINR "1.4 in 10 of 15 patients 24hours later.11 Thus, if the endoscopicretrograde cholangiopancreatogra-phy can be safely performed the nextday, this patient should receive 1 to
2.5 mg of oral vitamin K as soon aspossible, with plans to administerfresh frozen plasma at the time of theprocedure only if the INR has notcorrected. However, low-dose vita-min K should not be used as asubstitute for careful perioperativemanagement. A recent small trialfound that low-dose oral vitamin K,when given at noon on the day beforesurgery, failed to achieve adequateINR correction in #60% of patientswho had discontinued their vitaminK antagonist 2 days before electivesurgery; most of these patients wereusing fluindione or acenocoumarol (vi-tamin K antagonists not available in theUnited States).5
A 52-year-old woman with a me-chanical mitral valve presents withminor epistaxis. Her INR is 15.7. Sheis otherwise stable; the epistaxis re-solves quickly with direct pressure,and a thorough review of systems andphysical examination reveal no otherevidence of bleeding.
The American College of ChestPhysicians Evidence-Based ClinicalPractice Guidelines state, “For patientswith INRs #9.0 and no significantbleeding, we recommend holding war-farin therapy and administering ahigher dose of vitamin K (2.5 to 5 mg)orally, with the expectation that theINR will be reduced substantially in 24to 48 h. Clinicians should monitorthe INR more frequently, administeradditional vitamin K if necessary,and resume therapy at an appropri-ately adjusted dose when the INR
reaches the therapeutic range.”12
There is moderate-quality evidence tosupport this recommendation; severalstudies indicate that a large proportionof patients with extreme INR elevation(eg, #10) will have their INR return toa safer range within 24 hours after 2 to5 mg of oral vitamin K is adminis-tered.13,14 Although some cliniciansexpress concern that active anticoagu-lant reversal may place a patient with aprosthetic heart valve at high risk forthrombotic complications, we haveconducted a small study that suggestslow-dose oral vitamin K can be used insuch patients without a high risk ofovercorrection.15 Additionally, throm-botic events have been very uncom-mon in the studies of low-dose oralvitamin that have been presented todate. We recommend that all non-bleeding patients with an INR #10should receive 2.5 to 5 mg of oralvitamin K. The INR should be mea-sured 24 to 48 hours later to guide theuse of additional therapy. Any sign ofbleeding should prompt a thoroughclinical evaluation with admission andconsideration of transfusion therapy(Figure).
A 37-year-old man receiving warfa-rin for secondary prevention of venousthromboembolism presents to theemergency department with a 2-dayhistory of melena and new massivehematemesis. His INR is 7.3.
Up to 10% of patients with warfarin-associated major bleeding will diewithin 30 days. The most lethal formof warfarin-associated bleeding is in-
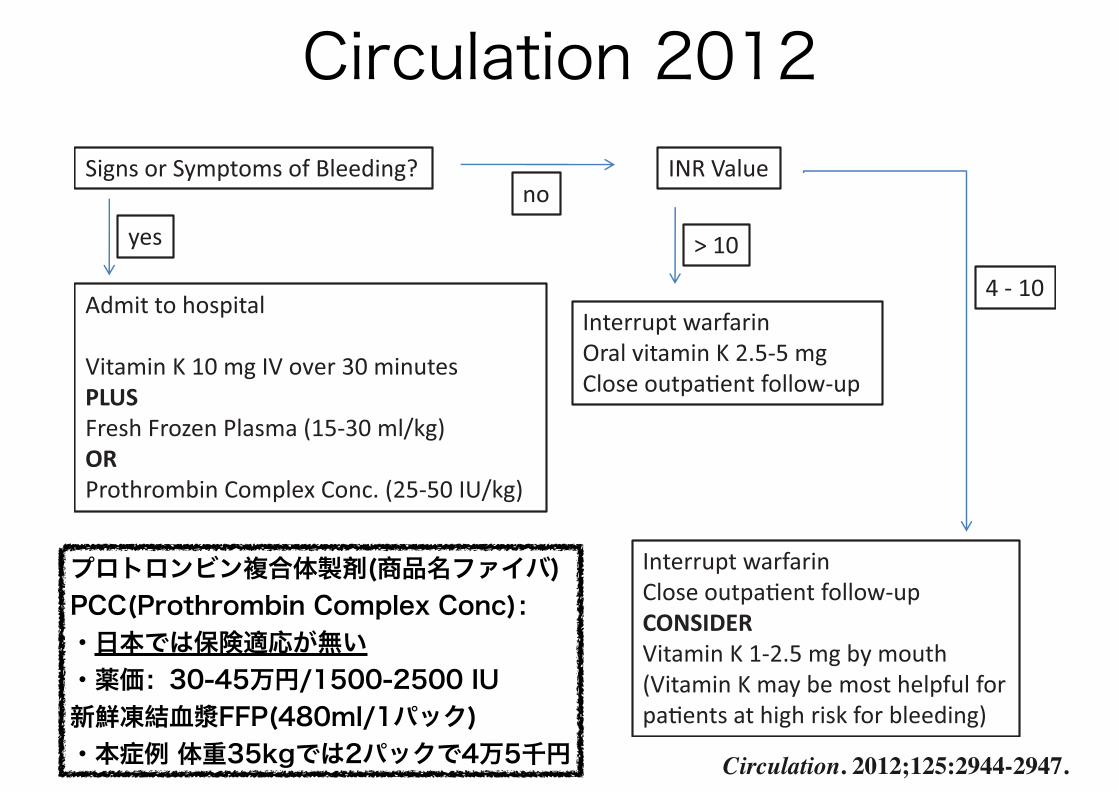
Signs or Symptoms of Bleeding?
yes
Admit to hospital Vitamin K 10 mg IV over 30 minutes PLUS Fresh Frozen Plasma (15-30 ml/kg) OR Prothrombin Complex Conc. (25-50 IU/kg)
no INR Value
> 10
Interrupt warfarin Oral vitamin K 2.5-5 mg Close outpa!ent follow-up
4 - 10
Interrupt warfarin Close outpa!ent follow-up CONSIDER Vitamin K 1-2.5 mg by mouth (Vitamin K may be most helpful for pa!ents at high risk for bleeding)
Figure. A suggested algorithm for the management of a warfarin-treated patient whoseinternational normalized ratio (INR) exceeds 4. IV indicates intravenously; Conc, concentrate.
Garcia and Crowther Warfarin Reversal 2945
at University of Tsukuba on April 20, 2015http://circ.ahajournals.org/Downloaded from
Circulation. 2012;125:2944-2947.
プロトロンビン複合体製剤(商品名ファイバ) PCC(Prothrombin Complex Conc): ·日本では保険適応が無い ·薬価:30-45万円/1500-2500 IU 新鮮凍結血漿FFP(480ml/1パック) ·本症例 体重35kgでは2パックで4万5千円

ACCP 2012
INR<4.5 WF量の減量
4.5≦INR≦9 ビタミンKの経口投与を検討。 WFを中止し、その後減量
INR>9 ビタミンKを経口投与する。 WFを中止し、その後減量
⑴major bleedingがない時
⑵major bleedingがある時、以下を行う•WF中止 •PCCまたはFFPを投与(但しPCC>FFPで推奨) •Vit K 5-10mg ivを併用 CHEST / 141 / 2 / FEBRUARY, 2012
ガイドラインをまとめると…
• 出血の有無を評価する • PT-INRが過延長した要因を検索する
• Vit Kの投与を判断する
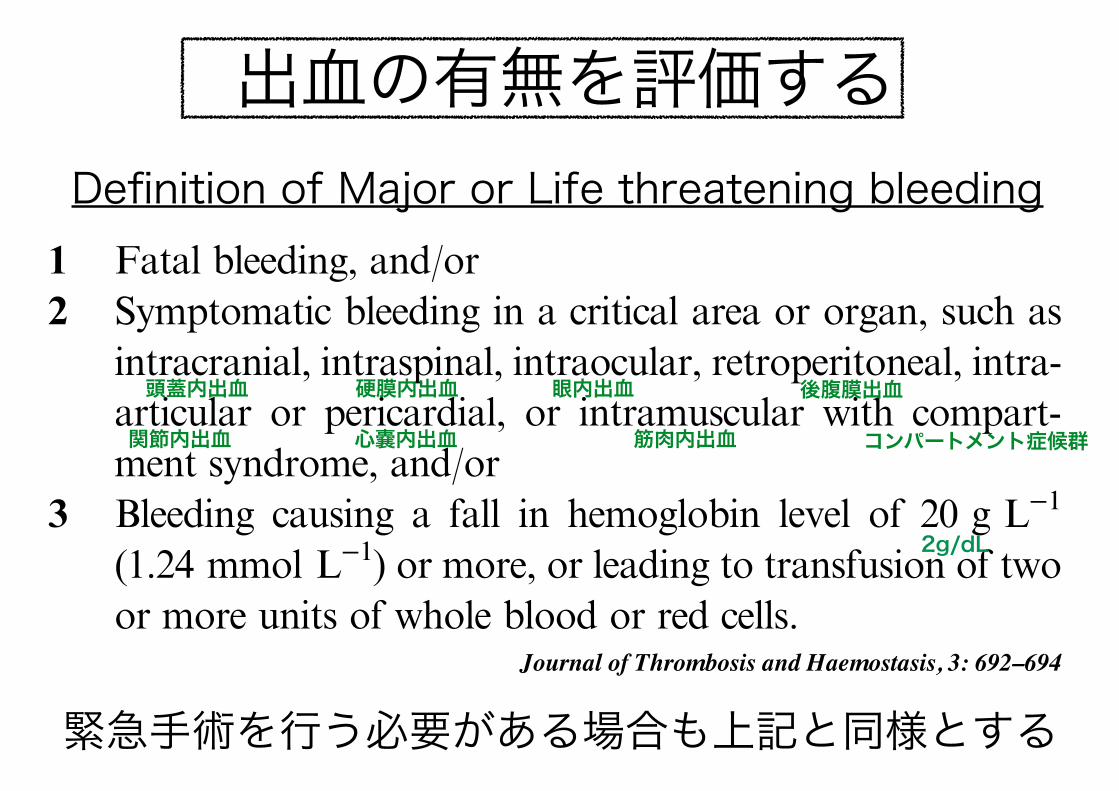
Definition of Major or Life threatening bleeding
hemorrhage between trials is evident (Table 1) [4]. Althoughthis variability is explained partly by different patient popula-tions, intensities of treatment, lack of validation of claimedinternational normalized ratio (INR), timing of anticoagulanttherapy in relationship to cardiac surgery and combinations ofantihemostatic agents, inconsistency in the definition of majorbleeding adds to these differences.
Methods
The objective of this ISTH SSC statement is to provide auniform definition of major bleeding in the evaluation ofantihemostatic agents, including inhibitors of coagulation,inhibitors of platelet function and fibrinolytic agents, for acutetreatment of thromboembolism or for long-term prophylaxisagainst thromboembolism. Long-term prophylaxis may beprimary, such as in patients with prosthetic heart valves andatrial fibrillation, or secondary, such as after systemic arterialembolism, myocardial infarction or venous thromboembo-lism. This definition is not intended to include postoperativebleeding in association with prophylaxis against venousthromboembolism, because that requires a definition of majorbleeding at the surgical site. A working group is currentlyvalidating surgical site hemorrhage and specific guidelines onthis topic are anticipated. Furthermore, we have not attemp-ted to define non-major bleeding in this statement. Anotherworking group will evaluate clinically significant non-majorbleeding in four ongoing trials with the long-acting pentasac-charide, idraparinux. That program will include about 12 000patients, many of whom will be treated with vitamin Kantagonists, and approximately 1200 of bleeds of this type areanticipated.
The following definition is based on a discussion held at themeeting of the subcommittee of Control of Anticoagulation atthe 50th Scientific and Standardization Committee Meeting ofthe ISTH in Venice, 18 June 2004. Presenters at this sessionincluded R. Beyth, C. Francis, C. Kearon, L. Linkins,M. Prinsand S. Schulman (C. Kearon and S. Schulman were cochairs).Attendees also contributed comments, and a general principlereached received wide acceptance. A draft definition was thensent to the cochairmen of the subcommittee, who wererequested to review and comment on the text within 1 month.
Responses were obtained from six cochairpersons and the texthas been revised by taking this input into account.
It is intended that these guidelines will be presented to theEuropean Agency for the Evaluation of Medicinal Prod-ucts (EMEA) and the United States Food and Drugs Admin-istration (FDA), and it is hoped that their widespread use infuture clinical trials will facilitate comparisons between trialsand the performance of systematic reviews of the literature.
Definition of major bleeding
As general principles, a definition of major bleeding needs to bebased on objective criteria, and major bleeds are those thatresult in death, are life-threatening, cause chronic sequelae orconsume major health-care resources. With this in mind, theControl of Anticoagulation Subcommittee recommends thefollowing criteria for major bleeding in non-surgical patients:1 Fatal bleeding, and/or2 Symptomatic bleeding in a critical area or organ, such as
intracranial, intraspinal, intraocular, retroperitoneal, intra-articular or pericardial, or intramuscular with compart-ment syndrome, and/or
3 Bleeding causing a fall in hemoglobin level of 20 g L)1
(1.24 mmol L)1) or more, or leading to transfusion of twoor more units of whole blood or red cells.
Discussion
The following comments should be made in relationship to theabove definition.
Fatal bleeding has not always been counted among majorbleeds in previous trials [5,6]; instead, these bleeds havesometimes been included among reported deaths withoutidentifying that bleeding was the cause of death. Similarly,intracranial bleeding has not always been counted amongmajor bleeds; instead, these bleeds have sometimes beenincluded as strokes without identifying that bleeding hadoccurred. The practice of including such bleeds as part ofcomposite outcomes without also identifying that bleeding isthe cause of these outcomes should be avoided.
All major bleeds should be described in a trial report. If thisis not feasible, as a minimum requirement authors shouldspecify the number of fatal bleeds and intracranial bleeds thatare included among the total number of major bleeds.
In order for bleeding in a critical area or organ to beclassified as a major bleed it must be associated with asymptomatic clinical presentation. For example, it is notuncommon that patients with venous thromboembolism havecomputed tomography scanning to detect a malignancy. If, inthe absence of symptoms to suggest bleeding, a smallretroperitoneal bleed was found on such an examination itwould not be classified as a major bleed.
In addition, in patients with symptoms and bleeding [e.g.present on a computerized tomography (CT) scan], it isrecognized that bleeding may not be the cause of thesymptoms (e.g. symptoms may be due to known cancer). If
Table 1 Range of rates of major hemorrhage on anticoagulanttherapy (vitamin K antagonists or heparins) in percentage per year inrandomized clinical trials according to indication [4]
Indication for anticoagulant therapyRates of majorhemorrhage
Prosthetic heart valves 1.0–19.2Atrial fibrillation 0–7Acute ischemic coronary syndrome 0–6.8Ischemic heart disease, long-term 0.6–14.5Venous thromboembolism, initial treatment 0–7.0Venous thromboembolism, long-term 0–16.7*
*Studies comparing low-molecular-weight with unfractionatedheparin, rate in percentage per 3 months.
Definitions of major bleeding in clinical studies 693
! 2005 International Society on Thrombosis and Haemostasis
緊急手術を行う必要がある場合も上記と同様とする
出血の有無を評価する
Journal of Thrombosis and Haemostasis, 3: 692–694
頭蓋内出血 硬膜内出血 眼内出血 後腹膜出血
関節内出血 心嚢内出血 筋肉内出血 コンパートメント症候群
2g/dL
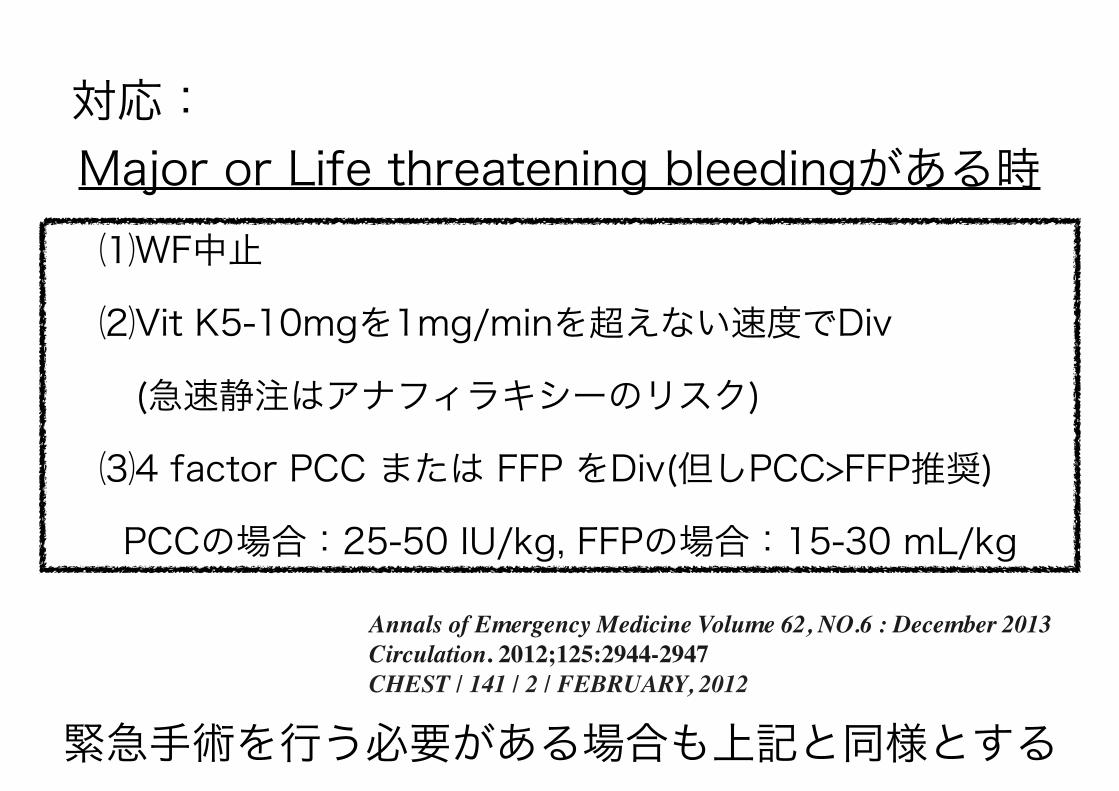
対応: Major or Life threatening bleedingがある時⑴WF中止
⑵Vit K5-10mgを1mg/minを超えない速度でDiv
(急速静注はアナフィラキシーのリスク)
⑶4 factor PCC または FFP をDiv(但しPCC>FFP推奨)
PCCの場合:25-50 IU/kg, FFPの場合:15-30 mL/kg
Annals of Emergency Medicine Volume 62, NO.6 : December 2013Circulation. 2012;125:2944-2947CHEST / 141 / 2 / FEBRUARY, 2012
緊急手術を行う必要がある場合も上記と同様とする
対応: Minor bleedingがある時
⑴WFを中止
⑵WF中止で止血しない場合には、Vit K1-3mg ivする
Minor bleeding:Major bleeding以外の出血
BMJ 2015;350:h1282

WFがVit Kを阻害することで、Vit K依存性であるⅡ, Ⅶ, Ⅸ, X凝固因子の産生が阻害される
http://kusuri-jouhou.com/medi/thrombosis/warfarin.html
warfarinの作用機序

PCC、FFPの作用機序• PCC:Ⅱ, Ⅶ, Ⅸ, X凝固因子の濃縮液 ただし、4 factor PCCと3 factor PCCがあるので注意が必要。4 factor PCCを使う(3 factor PCCはⅦ因子が入っていない)。
• FFP:新鮮凍結血漿なので、すべての凝固因子とフィブリノゲンが入っているPCC賛成 J Thromb Haemost 8: 2589-2591, 2010. FFP250ml輸注しても、凝固因⼦子活性は2~3%上昇する程度だが, プロトロンビン複合体製剤(PCC)であれば3,000IU(120ml)で, VII, IX, X, II因⼦子を40~80%上昇させることが可能
PCC反対 J Thromb Haemost 8: 2592-2595, 2010. ビタミンK依存性凝固因⼦子のみ含有されており, たとえばフィブリノゲンや第XIII因⼦子などの他の凝固因⼦子は含まれない(FFPには全て含まれる). PCCには未分画ヘパリンが含有されています(0.2~15 IU/mL)ので、⽌止⾎血能や凝固検査に影響する懸念がある.
ガイドラインではFFPよりも4 factor PCCを推奨
対応: Major or Life threatening bleedingがない場合
現病歴/既往歴:肝疾患、癌、下痢、心不全の増悪、発熱、閉塞性黄疸など
内服歴:WFと相互作用する薬がないかチェックする
生活習慣:食生活の変化、飲酒
PT-INRが過延長した要因を検索する
UPTODATEBMJ2015
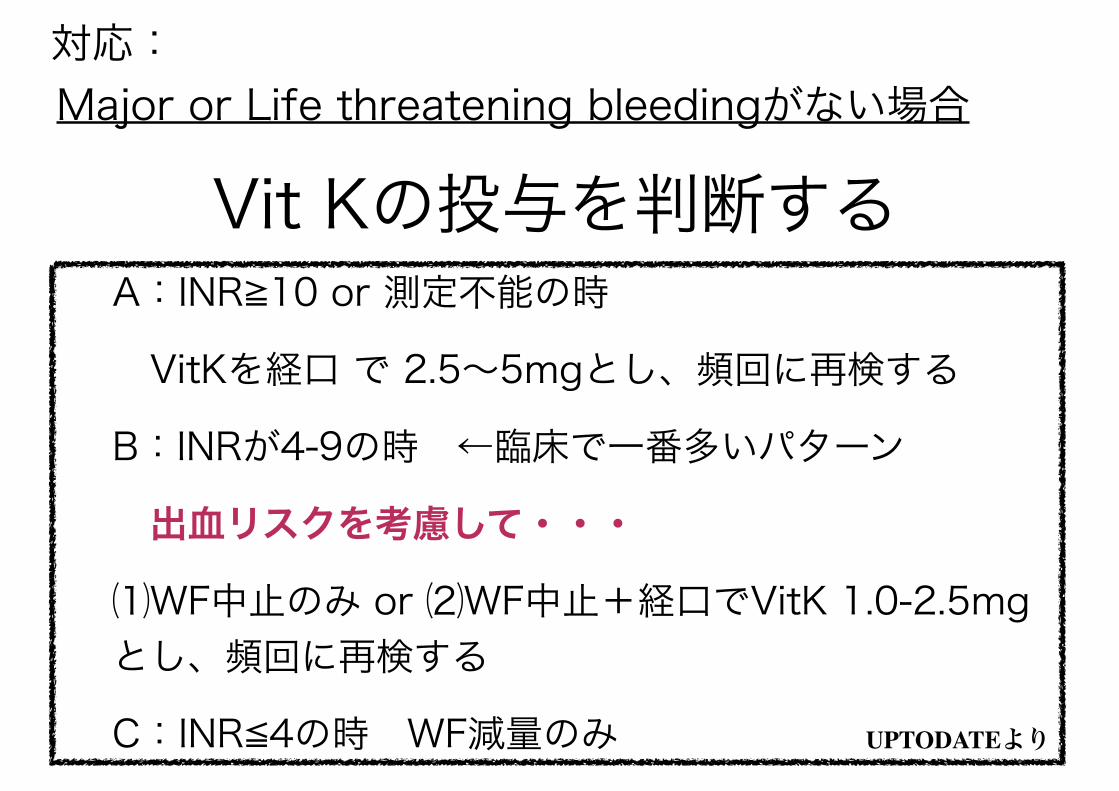
対応: Major or Life threatening bleedingがない場合
A:INR≧10 or 測定不能の時
VitKを経口 で 2.5~5mgとし、頻回に再検する
B:INRが4-9の時 ←臨床で一番多いパターン
出血リスクを考慮して・・・
⑴WF中止のみ or ⑵WF中止+経口でVitK 1.0-2.5mgとし、頻回に再検する
C:INR≦4の時 WF減量のみ
Vit Kの投与を判断する
UPTODATEより
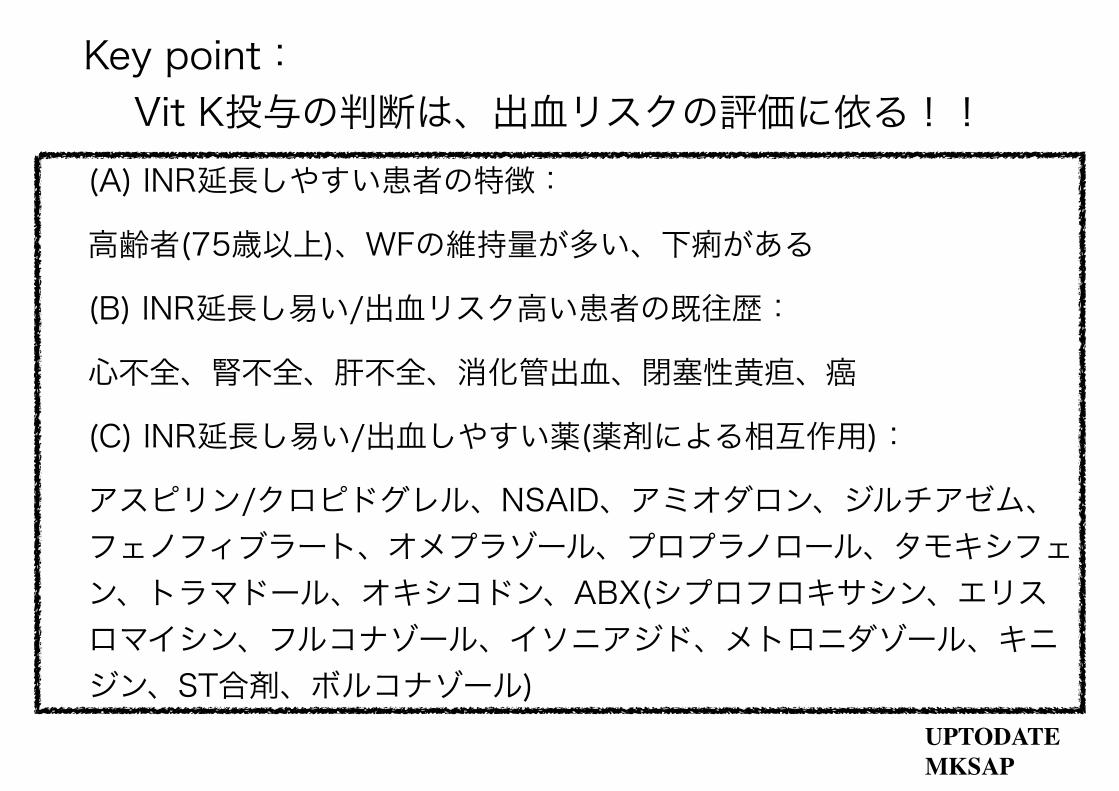
Key point: Vit K投与の判断は、出血リスクの評価に依る!!
(A) INR延長しやすい患者の特徴:
高齢者(75歳以上)、WFの維持量が多い、下痢がある
(B) INR延長し易い/出血リスク高い患者の既往歴:
心不全、腎不全、肝不全、消化管出血、閉塞性黄疸、癌
(C) INR延長し易い/出血しやすい薬(薬剤による相互作用):
アスピリン/クロピドグレル、NSAID、アミオダロン、ジルチアゼム、フェノフィブラート、オメプラゾール、プロプラノロール、タモキシフェン、トラマドール、オキシコドン、ABX(シプロフロキサシン、エリスロマイシン、フルコナゾール、イソニアジド、メトロニダゾール、キニジン、ST合剤、ボルコナゾール)
UPTODATEMKSAP
出血リスクの評価方法 - QBleed score - Outpatient bleeding risk index (OBRI) - HEMORR2HAGES risk index - HAS-BLED bleeding risk score - ATRIA risk score
抗凝固薬の開始や継続の判断、INR過延長時の対応に、使用できるかもしれない。
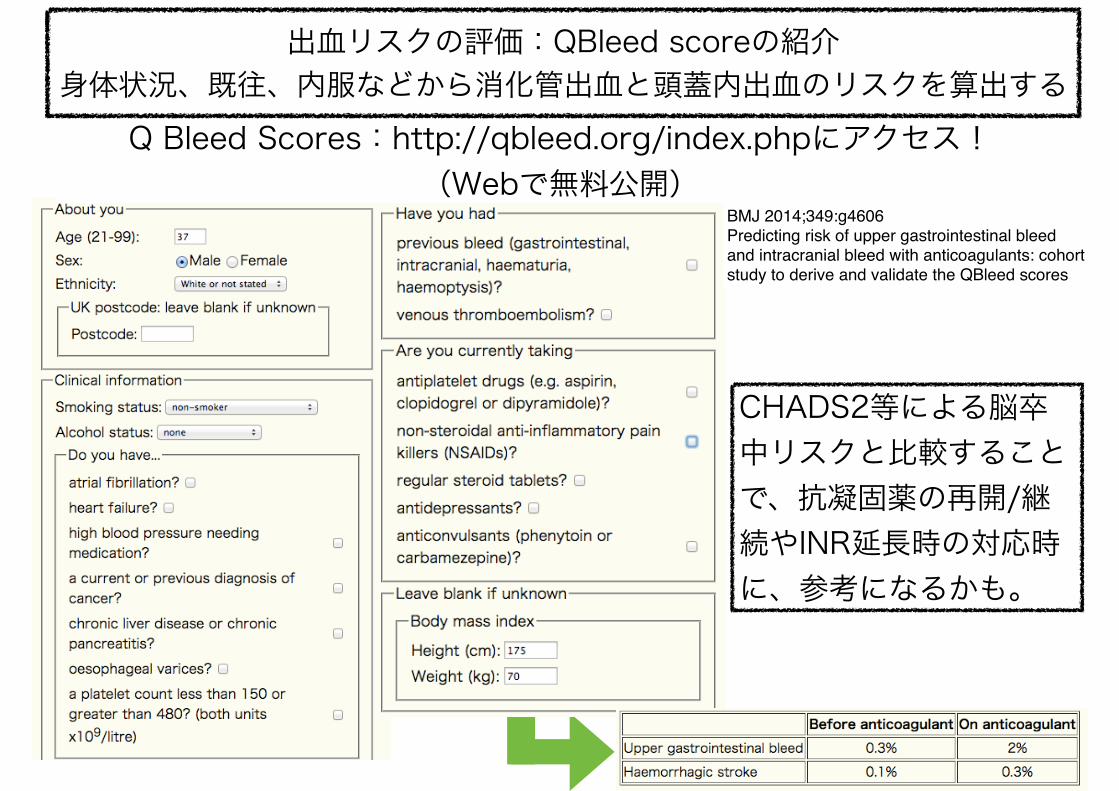
BMJ 2014;349:g4606 Predicting risk of upper gastrointestinal bleed and intracranial bleed with anticoagulants: cohort study to derive and validate the QBleed scores
Q Bleed Scores:http://qbleed.org/index.phpにアクセス! (Webで無料公開)
CHADS2等による脳卒中リスクと比較することで、抗凝固薬の再開/継続やINR延長時の対応時に、参考になるかも。
出血リスクの評価:QBleed scoreの紹介 身体状況、既往、内服などから消化管出血と頭蓋内出血のリスクを算出する
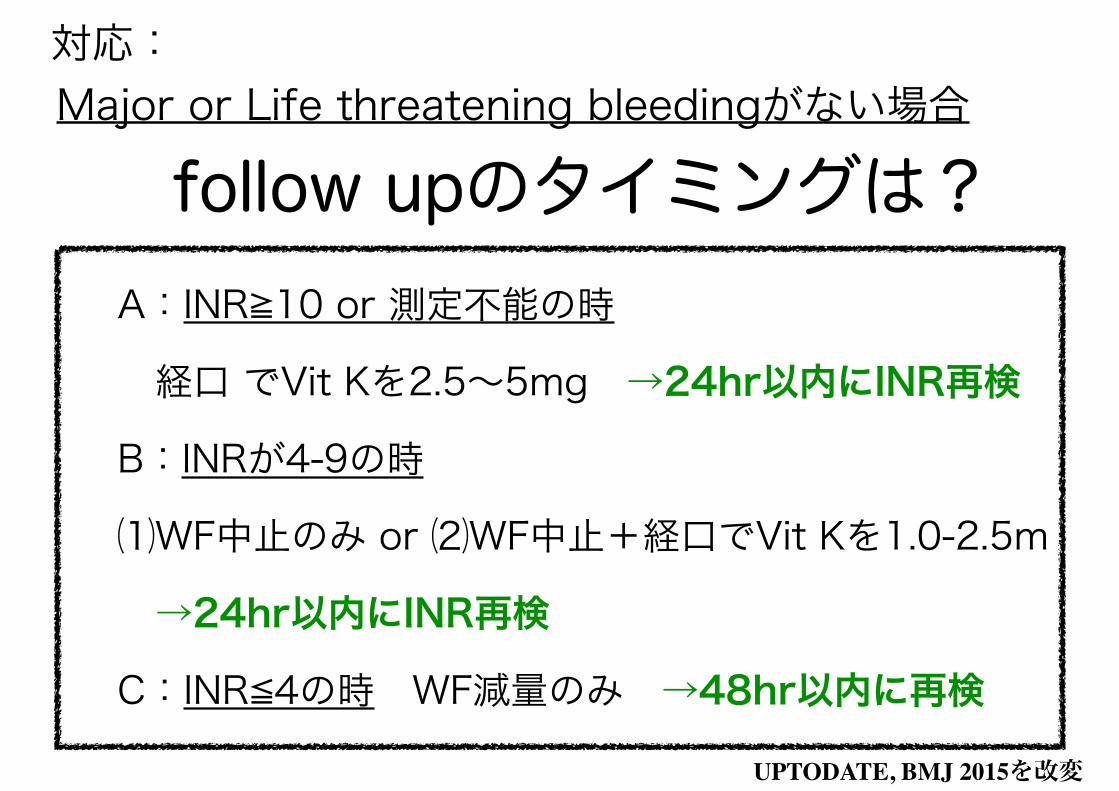
対応: Major or Life threatening bleedingがない場合
A:INR≧10 or 測定不能の時
経口 でVit Kを2.5~5mg →24hr以内にINR再検
B:INRが4-9の時
⑴WF中止のみ or ⑵WF中止+経口でVit Kを1.0-2.5m
→24hr以内にINR再検
C:INR≦4の時 WF減量のみ →48hr以内に再検
follow upのタイミングは?
UPTODATE, BMJ 2015を改変
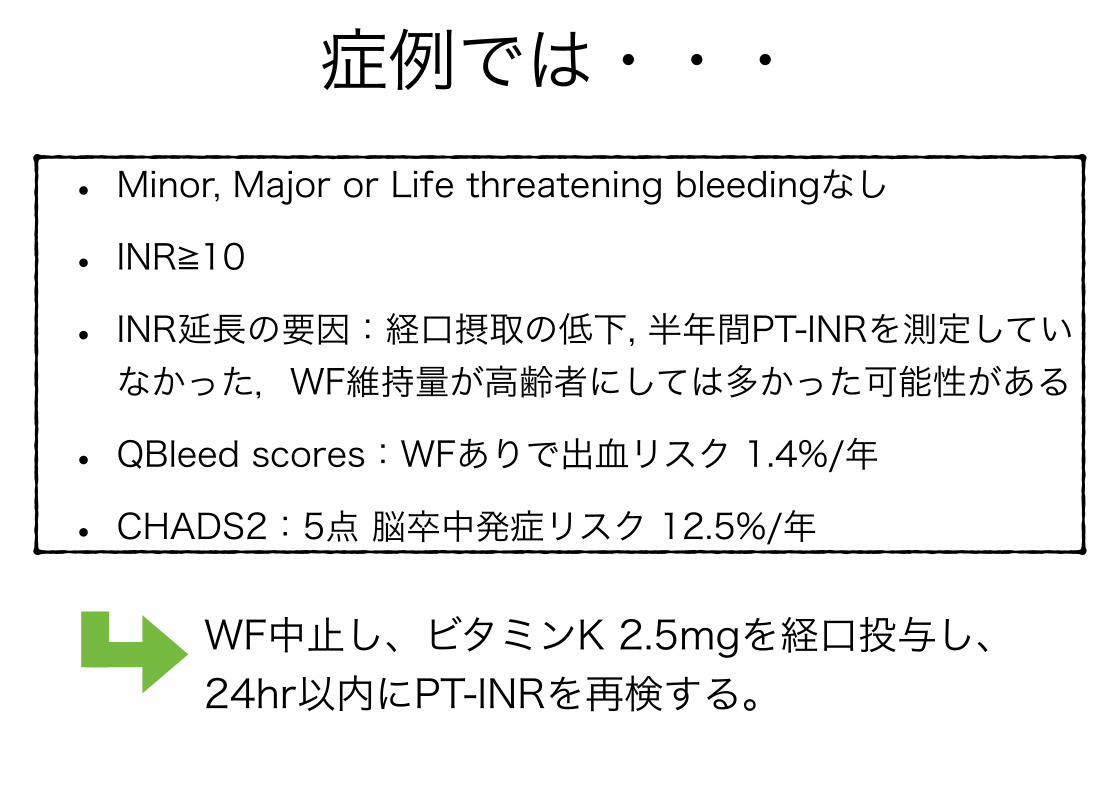
症例では・・・
WF中止し、ビタミンK 2.5mgを経口投与し、24hr以内にPT-INRを再検する。
• Minor, Major or Life threatening bleedingなし • INR≧10 • INR延長の要因:経口摂取の低下, 半年間PT-INRを測定していなかった,WF維持量が高齢者にしては多かった可能性がある
• QBleed scores:WFありで出血リスク 1.4%/年 • CHADS2:5点 脳卒中発症リスク 12.5%/年
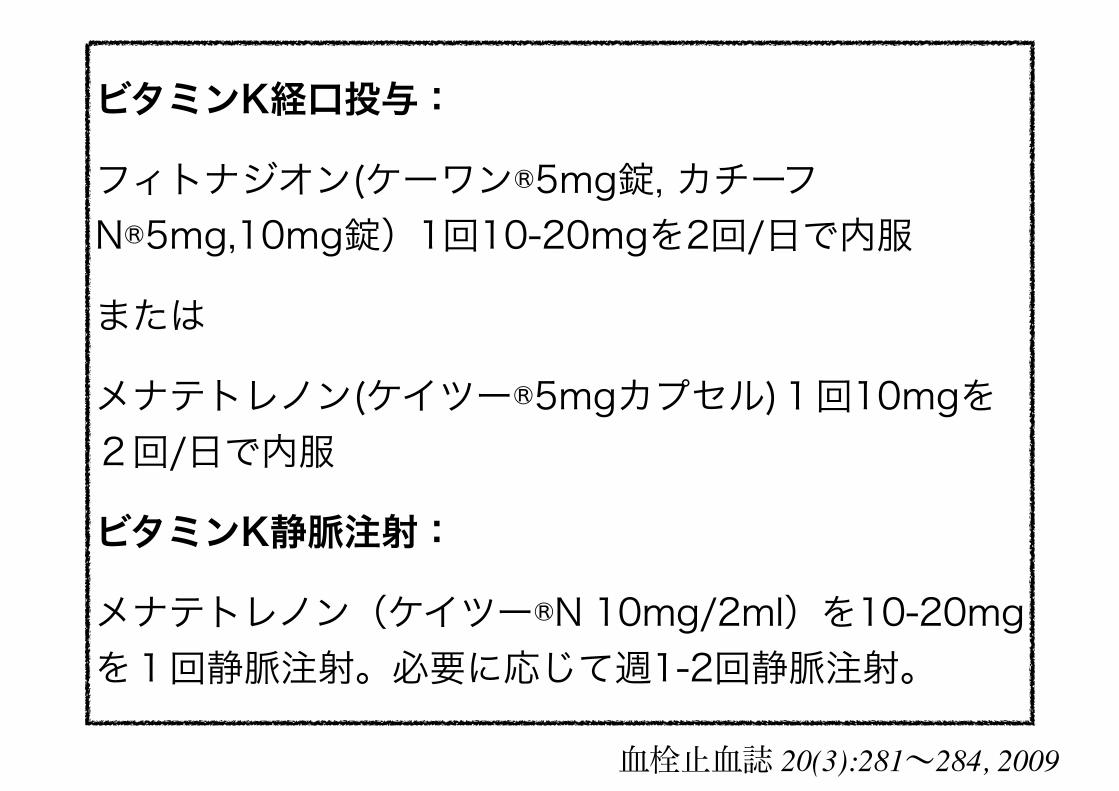
ビタミンK経口投与:
フィトナジオン(ケーワン®5mg錠, カチーフN®5mg,10mg錠)1回10-20mgを2回/日で内服
または
メナテトレノン(ケイツー®5mgカプセル)1回10mgを2回/日で内服
ビタミンK静脈注射:
メナテトレノン(ケイツー®N 10mg/2ml)を10-20mgを1回静脈注射。必要に応じて週1-2回静脈注射。
血栓止血誌 20(3):281~284, 2009
Take home message:INR延長時の対応
• Major bleeding あれば、緊急対応! • Major bleeding なければ、INR延長の要因を検索する • 出血リスクと脳卒中リスクを評価し、Vit K p.o.を検討 ➡出血リスクの評価に QBleed scoresがある
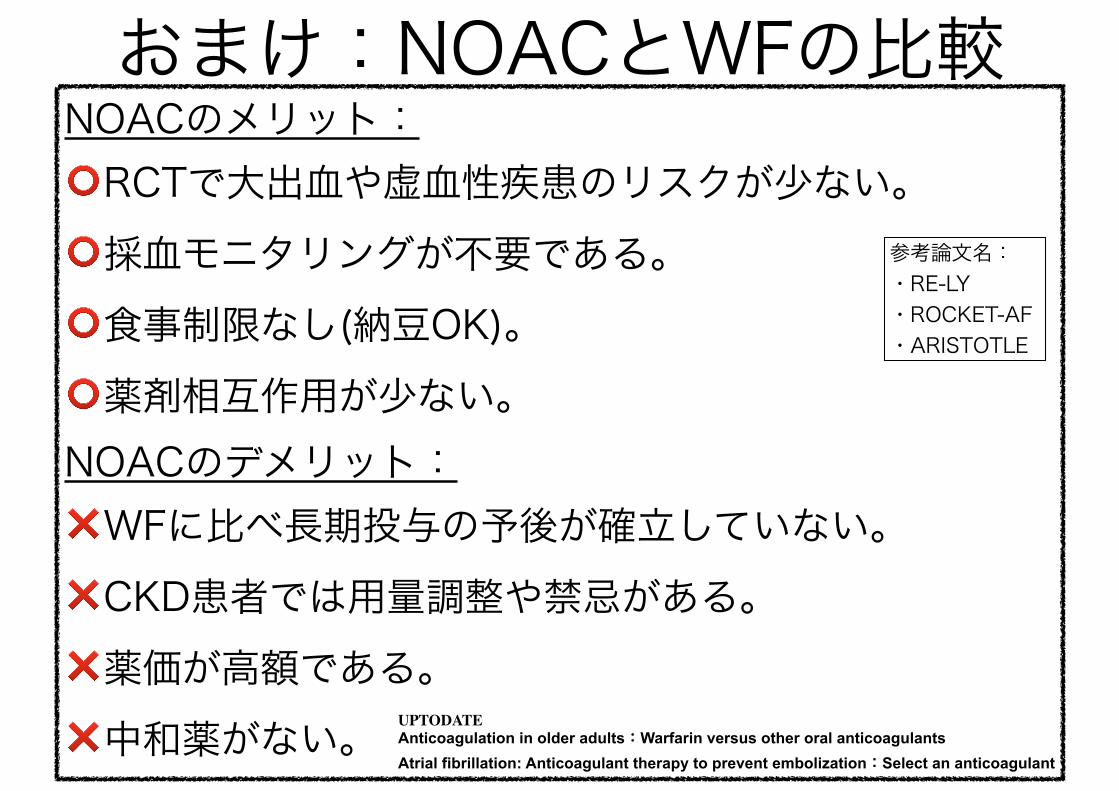
おまけ:NOACとWFの比較NOACのメリット: ⭕RCTで大出血や虚血性疾患のリスクが少ない。 ⭕採血モニタリングが不要である。 ⭕食事制限なし(納豆OK)。 ⭕薬剤相互作用が少ない。 NOACのデメリット: ❌WFに比べ長期投与の予後が確立していない。 ❌CKD患者では用量調整や禁忌がある。 ❌薬価が高額である。 ❌中和薬がない。
参考論文名: ・RE-LY ・ROCKET-AF ・ARISTOTLE
UPTODATEAnticoagulation in older adults:Warfarin versus other oral anticoagulants Atrial fibrillation: Anticoagulant therapy to prevent embolization:Select an anticoagulant