Embed Size (px)
Citation preview
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
Clinical Research Billing Basics &
How to Develop a Coverage Analysis
Julie Colasacco & Michael C. Roach Presented at
Virginia Commonwealth University August 29, 2013

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
Goals • Raise Awareness
• Teach – knowledge transfer
2
©2013 Aegis Compliance & Ethics Center, LLP
Important Terms & Acronyms • Clinical Research Billing – CRB
• Medicare Clinical Trial Policy – CTP
• Qualifying Clinical Trial – QCT
• Centers for Medicare & Medicaid Services – CMS
3

©2013 Aegis Compliance & Ethics Center, LLP
Overview 1. Regulatory risks of clinical research billing non-compliance 2. The importance of a Coverage Analysis (CA) for compliance 3. An overview of Medicare rules for billing during clinical research studies 4. The “basics” of billing for research team members 5. How the budget structure influences what can be billed to insurance 6. How the language of the Informed Consent Form influences what can be
billed to insurance 7. What does Medicare mean by a “qualifying clinical trial”? 8. What does Medicare mean by “routine costs”? 9. The importance of the research coordinator in ensuring clinical research
billing is compliant 10. Tips on protocol design for investigator-initiated studies to improve
budgeting and billing 11. The role of the study calendar in clinical research billing 12. Improving communications during the research study
4

©2013 Aegis Compliance & Ethics Center, LLP
Overview 13. Pause for Questions 14. Introduction to the Coverage Analysis: Purposes 15. Review of forms needed 16. Development of a Coverage Analysis
• Step 1: Draft a grid • Step 2: Review ICF • Step 3: Review CTA/Budget • Step 4: QCT Analysis • Step 5: Which are “routine costs”? • Step 6: How to document reasoning • Step 7: Coding the CA
5

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
1. Regulatory risks of clinical
research billing non-compliance
6

©2013 Aegis Compliance & Ethics Center, LLP
Risks Associated With Non-Compliance • CRB risks can be grouped:
1. Billing for services that are already paid by the sponsor (double billing)
2. Billing for services promised free in the informed consent 3. Billing for services that are for research-purposes only 4. Billing for services that are part of a non-qualifying clinical trial 5. Billing Medicare Advantage Plan when claim should be directed
to Medicare Administrative Contractor (“MAC”)
7

©2013 Aegis Compliance & Ethics Center, LLP
Challenges Cause of most research billing non-compliance:
• Breakdown in coordination
Important information to coordinate • What research studies are being conducted at the facility? • Which patients are enrolled in a research study? • Which services should be charged to payors
and which charged to study account? • Sponsor, grant, internal account
• Informed consent language • Clinical trial agreement language • Protocol Language
8
©2013 Aegis Compliance & Ethics Center, LLP
Coordination • Who impacts research billing?
• Principal Investigator • Clinical Research Coordinator – vital communication coordinator • IRB process • Budget negotiators • Clinical Trial Agreement negotiators • Grant administration • Information Technology • Health Information Management • Registration/Scheduling • Medical center billing and coding • Physician professional fee billing and coding • Study fund managers • Managed care contract negotiators • ….and others!
9

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
2. The importance of a
Coverage Analysis (CA) for compliance
10
©2013 Aegis Compliance & Ethics Center, LLP
What is a Coverage Analysis? • Systematic review of research related documents to
determine the Medicare billing status of both the study itself and the items and services provided to the research subjects that are required by the study
• A tool to coordinate information for purposes of: • Budgeting • Billing • Auditing
11

©2013 Aegis Compliance & Ethics Center, LLP
What a Coverage Analysis is not • Guarantee of coverage in all cases
• Substitute for the pre-authorization process
• Based on individual investigators’ decisions or billing practices
• Substitute for the practice of medicine or physician judgment
• Treatment plan
• “Black and white” or “perfect translation”
12
©2013 Aegis Compliance & Ethics Center, LLP
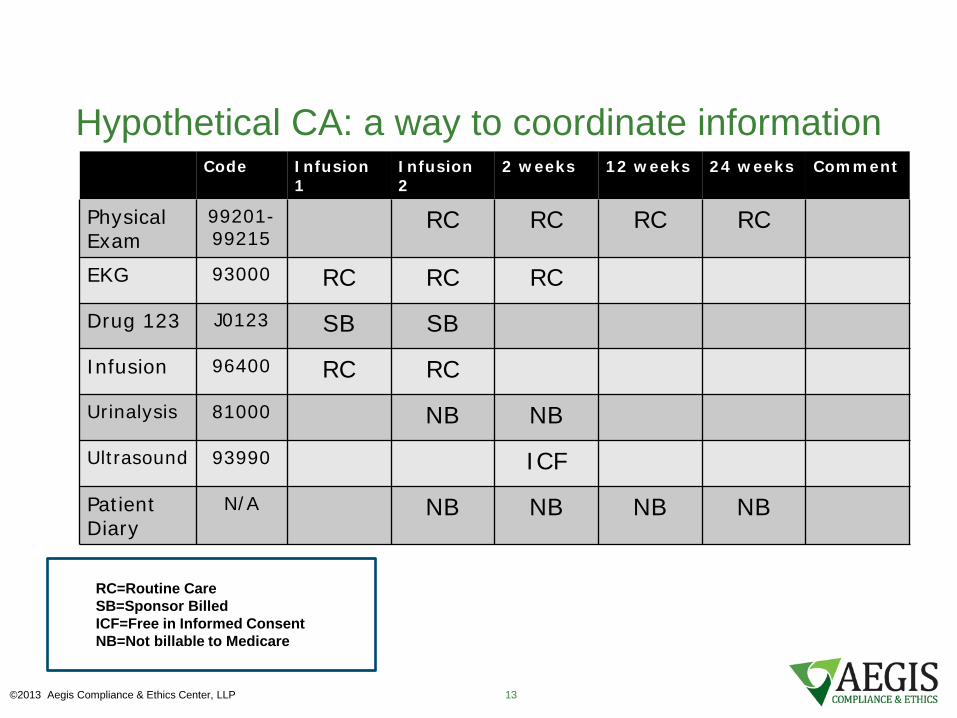
Hypothetical CA: a way to coordinate information Code Infusion
1 Infusion 2
2 weeks 12 weeks 24 weeks Comment
Physical Exam
99201-99215
RC RC RC RC
EKG 93000 RC RC RC
Drug 123 J0123 SB SB
Infusion 96400 RC RC
Urinalysis 81000 NB NB
Ultrasound 93990 ICF
Patient Diary
N/A NB NB NB NB
RC=Routine Care SB=Sponsor Billed ICF=Free in Informed Consent NB=Not billable to Medicare
©2013 Aegis Compliance & Ethics Center, LLP 13

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
3. An overview of Medicare rules
for billing during clinical research studies
14
©2013 Aegis Compliance & Ethics Center, LLP
True or False? • Medicare pays for standard of care during
research studies.
• False: Medicare pays for “routine costs” during “qualifying clinical trials”
15
©2013 Aegis Compliance & Ethics Center, LLP
True or False? “My friend in California says this service is covered when she provides it, so it’s covered for us, too.” Maybe: Medicare Administrative Contractors (“MACs”) can issue local coverage determinations (“LCDs”) that limit coverage in their area.
If your friend has a different MAC, you may not be able to bill a service that she can.
Possible for your friend to have a different MAC even if she works at a facility down the street from you
16
©2013 Aegis Compliance & Ethics Center, LLP
True or False? “We have billed for this service hundreds of times and the claim is always paid by Medicare, so it must be covered.” False: You cannot assume that just because Medicare has been paying for a service that it is a covered service
17
©2013 Aegis Compliance & Ethics Center, LLP
True or False? “You are making clinical decisions when you decide something is not billable to Medicare.” False. Decisions about whether a service is covered is not a clinical decision. It is a decision based on an analysis of the billing rules and coverage determinations made by CMS and Medical Directors at MACs.
18
©2013 Aegis Compliance & Ethics Center, LLP
Medicare’s CRB Framework Medicare requires a five-part process for clinical research services coverage:
1. Does the study “qualify” for coverage?
2. What items and services are “routine costs”?
3. Do Medicare rules allow coverage of specific “routine costs” within a research study?
4. What is paid for by the sponsor?
5. What is promised free in the informed consent?
19
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
4. The “basics” of billing
for research team members
©2013 Aegis Compliance & Ethics Center, LLP 20

©2013 Aegis Compliance & Ethics Center, LLP
Billing Basics • Before getting into the details of CRB, it is
important to step back and understand: • The billing system in the U.S. • The structure of the Medicare Program
• Medicare is a driver of reimbursement across many payors, particularly for CRB
• Understanding some of the basics helps with budgeting,
putting the CRB rules in context, and improves claims management
21

©2013 Aegis Compliance & Ethics Center, LLP
Structure of Medicare reimbursement for an outpatient service
Service
Technical component
Professional component
Medicare pays a technical component and professional component for all Part B services. Who receives which component depends upon the
place of service.

©2013 Aegis Compliance & Ethics Center, LLP
Service provided in a physician office setting
Service
Technical component
Professional component
Medicare pays physician both components in one payment

©2013 Aegis Compliance & Ethics Center, LLP
Service provided in a hospital outpatient setting
Service
Technical component
Professional component
Medicare pays hospital
Medicare pays physician

©2013 Aegis Compliance & Ethics Center, LLP
The Legal Structure of Medicare • To understand Medicare research billing rules,
it is important to step back and understand the legal structure of Medicare
• Statutory basis for Medicare coverage follows this principle:
• Medicare covers items and services that are “reasonable and necessary to diagnose or treat illness or injury”
• Known as the “Reasonable & Necessary Rule”
25
©2013 Aegis Compliance & Ethics Center, LLP
The Hierarchy of Medicare Rules The Statute
National – CMS • National Coverage Determinations (“NCDs”)
• www.cms.gov/medicare-coverage-database/overview-and-quick-search.aspx
• Manuals (e.g., Medicare Benefit Policy Manual, Medicare Claims Processing Manual)
Local - MACs • Local Coverage Determinations (“LCDs”) • Medical Director “articles” • Medical Director “rulings”
“Reasonable & Necessary Rule” • Document medical necessity when no coverage rule
26
©2013 Aegis Compliance & Ethics Center, LLP
Medicare Contractors Have Wide Discretion Example: CyberKnife
No national uniform policy; regional decision “Geography Has Role in Medicare Cancer Coverage,” NYT December 16, 2008
“[G]eography may play as big a role as medicine in determining which men diagnosed with prostate cancer are eligible for CyberKnife. As it turns out, Medicare pays for the treatments in 33 states — but not in 17 others.”
“Our guidance to them is that if there’s no evidence it works, they shouldn’t pay for it,” said Dr. Steve Phurrough, Medicare’s coverage director in Washington. “The CyberKnife is a good example of a technology where you can review the evidence and come to different conclusions.”
27

©2013 Aegis Compliance & Ethics Center, LLP
Implications of hospital vs. physician billing in CRB process • The “answer” in the CA will be the same for hospital billing
and physician billing – but how the charges are presented on the claim forms will look very differently
• Hospital billing and physician billing should usually match during a research study – with respect to when services are charged to the study account and when the item or service is billed normally
• Payment for hospital services versus physician services varies immensely
• Budgeting must take into account both the hospital charge and the physician charge (if the service is hospital-based)
28
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
5. How the budget
structure influences what can be billed to insurance
29
©2013 Aegis Compliance & Ethics Center, LLP
Medicare’s CRB Framework
Medicare requires a five-part process for clinical research services coverage:
1. Does the study “qualify” for coverage?
2. What items and services are “routine costs”?
3. Do Medicare rules allow coverage of specific “routine costs” within a research study?
4. What is paid for by the sponsor?
5. What is promised free in the informed consent?
30

©2013 Aegis Compliance & Ethics Center, LLP
First things first: What is a clinical trial agreement? A clinical trial agreement (CTA) sets out the obligations of parties involved in a research study The CTA sets out: what services are to be performed “who does what” “who owns what” how much money will be paid for which services “extra” regulatory obligations the parties will take on the “rules of the road” between the parties
31
©2013 Aegis Compliance & Ethics Center, LLP
Why is the CTA important for the research billing process? • Whatever is paid for by the sponsor in the CTA cannot
be billed to the subject or the subject’s insurer
• If the CTA is not clear on what is being paid for by the sponsor, the document may be misinterpreted both by the sponsor and by regulators in the event of an audit
• The information in the CTA on what the sponsor is paying for must be communicated to the billing process
• Institutions may suffer unintended consequences based on what is written in the CTA
32
©2013 Aegis Compliance & Ethics Center, LLP
Non-industry contracts • The concepts in this presentation apply equally to contracts
for funding support with non-industry sponsors
• Most CRB compliance risks can occur without respect to whether the sponsor is industry, government, or a private foundation
• Negotiators of government contracts should coordinate with the individuals who negotiate the budget and be cognizant of their impact on the CRB process
• Offices within organizations that deal with government contracts should be brought into the CRB process training
33

©2013 Aegis Compliance & Ethics Center, LLP
What and where is the “study budget”? • The study budget for industry-sponsored studies is
typically an appendix or exhibit to the CTA and serves as the compensation detail
• The study budget and the main body of the contract are part of the same document – they will be interpreted together
34

©2013 Aegis Compliance & Ethics Center, LLP
Operational issues that could impact the CRB process Many clinical trial agreements have been negotiated in “parts”
• One person negotiates the main body • Another person negotiates the “budget”/compensation • Protocol is incorporated but may not be reviewed carefully by
either person, particularly if there is no formal MCA process in place
Fundamental principle of Clinical Trial Agreements – Singularity:
• A CTA is one contract with many parts • Interpreted as a single legal document
35
©2013 Aegis Compliance & Ethics Center, LLP
Bringing a CRB perspective early to a CTA • Best practice CRB processes analyze both the main body of the
CTA and the “study budget” exhibit from a billing perspective • Goal: Clarity in the final documents
• If sponsor is paying for all services, then the CTA and study budget should be clear and that should be reflected in a Medicare Coverage Analysis (MCA) or other communication tool to inform the CRB process
• If sponsor is only paying for some of the protocol services, then the
study budget should be clear as to which services are being paid for so there is no confusion in developing the MCA
• Ambiguities in the CTA and study budget will usually be interpreted by
insurers to their benefit (i.e., no billing)
36

©2013 Aegis Compliance & Ethics Center, LLP
Main body of the CTA: Case studies of language Examples of clauses (risky language): • “Payment for Study services are set out in Exhibit B. Such
compensation constitutes payment for all of the Institution’s costs for conducting Study services.”
• “Sponsor agrees to pay Institution in accordance with Exhibit B. Institution agrees not to bill any third-party payer for services required by the Study.”
• “Exhibit A sets out the payment schedule to Institution for Study services. Unscheduled imaging services shall be invoiced to sponsor at $350 per service.”
37

©2013 Aegis Compliance & Ethics Center, LLP
Main body of the CTA: Case studies of language Examples of clauses (neutral language): • “During the term of the Study, Sponsor agrees to provide financial support
for the Study in accordance with the budget set out in Exhibit A.”
• “Payment to Institution for items provided and services performed by Institution during the Study are set out in Exhibit A.”
• Negotiations will not always be able to produce completely neutral language in the main body of the CTA; if the main body contains discussion of specifics of the financials, then be precise and ensure that the main body of the CTA and the study budget language do not contradict each other
38

©2013 Aegis Compliance & Ethics Center, LLP
Structure of Financial Provisions: Compensation Exhibit/“Study Budget” There is no standard approach to the Compensation Exhibit – each sponsor tends to have its own format
Some structures utilized:
• Payments for “research service” at milestones • Note: Is “research service” defined? Be clear which services are
considered research services
• Spreadsheet with payments based on schedule of events • Note: Best practice
39

©2013 Aegis Compliance & Ethics Center, LLP
Structure of Financial Provisions: Compensation Exhibit/“Study Budget”
• Consider adopting a consistent approach for the compensation exhibits: the more detail on which services are being paid for, the better
• The MCA can serve as a tool for budgeting and lends itself to be used as the compensation exhibit
• Negotiating Suggestion: Watch out for footnotes! Avoid footnotes in the study budget, if possible
40
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
6. How the language of the
Informed Consent Form influences what can be
billed to insurance
©2013 Aegis Compliance & Ethics Center, LLP 41
©2013 Aegis Compliance & Ethics Center, LLP
Medicare’s CRB Framework
Medicare requires a five-part process for clinical research services coverage:
1. Does the study “qualify” for coverage?
2. What items and services are “routine costs”?
3. Do Medicare rules allow coverage of specific “routine costs” within a research study?
4. What is paid for by the sponsor?
5. What is promised free in the informed consent?
42
©2013 Aegis Compliance & Ethics Center, LLP
Role of the Informed Consent Form Interpreting the ICF • ICF interpreted for MCA from the perspective of the subject • Plain meaning of the words used in the informed consent
• Promises made to subject regarding what is free must be kept
• If two sentences in Costs section could reasonably be
interpreted in a way that they contradict each other, then re-word
43
©2013 Aegis Compliance & Ethics Center, LLP
Research Informed Consent: Context OHRP & FDA Rules:
45 CFR 46.116 & 21 CFR 50.20: “The information that is given to the subject or the representative shall be in language understandable to the subject or the representative.”
Goal: Language in 6th to 8th grade reading level
Government reviews and audits of ICF: Interpreted from the perspective of the subject The ICF means what it says: assumes plain meaning of the terms
44

©2013 Aegis Compliance & Ethics Center, LLP
ICF & Added Costs Section Regulation:
45 CFR 46.116(b)(3) & 21 CFR 50.25(b)(3) require the ICF include, when appropriate, “any additional costs to the subject that may result from participation in the research”
If the “added costs” section of the informed consent form states that an item or service will not be charged to the patient, then the provider cannot bill for that service Note: The regulation does not require that the ICF list the services that are or are not charged, rather it requires the ICF to list the “additional costs” the patient will incur as a result of participating in the study (many routine costs are not costs resulting from participation)
45

©2013 Aegis Compliance & Ethics Center, LLP
Problematic Added Costs Language “You or your insurer will have no costs for participating in this research study.”
(Subject/insurer may not be billed for any protocol-required items or services, nor for complications/injuries or other costs associated with participation)
“Your routine medical care will be billed in the usual way. However, you will not be charged for any study visits or services.”
(Inconsistent terms within the same document) “You will be responsible for the costs of any services you would have received if you did not enroll in this research study. However, you will not be billed for any lab services or imaging services.”
(Inconsistent terms within the same document) 46

©2013 Aegis Compliance & Ethics Center, LLP
Added Costs Section Contemplating the CRB Process Language which keeps the ICF “neutral”:
“You will be responsible for the costs of services required by the research study that are routine to treat your condition. You will not be responsible for the costs of services that are required only because you are enrolled in the research study.”
Language which specifically identifies services that will not be billed (if IRB desires specifics)
“You will be responsible for costs for care you would have received if you were not enrolled in this research. However, you will not be responsible for the costs of the CT scan conducted at the start of each drug cycle.”
47

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP 48
Medicare CRB Rules: The Regulatory Specifics
©2013 Aegis Compliance & Ethics Center, LLP
In a Nutshell Medicare covers “routine costs” in a “qualifying clinical trial” but note that all other Medicare rules still apply.
49

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
7. What does Medicare mean by a “qualifying
clinical trial”?
©2013 Aegis Compliance & Ethics Center, LLP 50
©2013 Aegis Compliance & Ethics Center, LLP
“Qualifying” Status Research study must meet CMS’ “qualifying clinical trial”
criteria for any items and services in the study to be confidently covered.
• Government and Drug Trials: CMS Clinical Trial Policy (NCD
310.1)
• Device Studies: Device study coverage rules from regulations and Medicare Benefit Policy Manual • 42 CFR Part 405, Subpart B (42 CFR 405.201 et seq.) • Ch. 14 of the Medicare Benefit Policy Manual
51
©2013 Aegis Compliance & Ethics Center, LLP
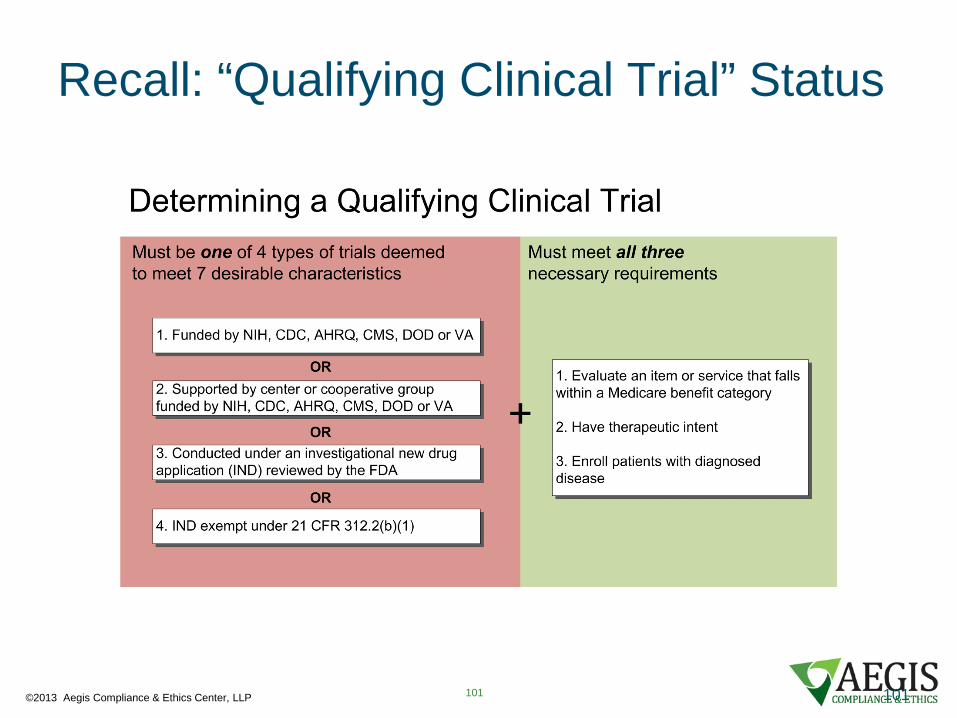
Qualifying Clinical Trials ("QCTs") Part 1 – “Deemed Studies” These studies are “deemed” to have 7 characteristics CMS wants
to see in a study it will cover
1. Studies funded by NIH, CDC, AHRQ, CMS, DOD, and VA
2. Studies supported by centers or cooperative groups funded by NIH, CDC, AHRQ, CMS, DOD, and VA;
3. Studies being conducted under an IND application; or
4. IND exempt studies under 21 CFR 312.2(b)(1)
52

©2013 Aegis Compliance & Ethics Center, LLP
Qualifying Clinical Trials (“QCTs”) Part 2 – “Necessary Requirements”
1. The study must investigate an item or service that Medicare pays for (falls in a benefit category)
2. The study must enroll patients with diagnosed disease
3. The study must have therapeutic intent
53
©2013 Aegis Compliance & Ethics Center, LLP
Benefit Category Test • NCD 310.1 lists 72 benefit categories
• Drug studies: “Drugs and biologicals”
54

©2013 Aegis Compliance & Ethics Center, LLP
Diseased Subjects Test Medicare only covers items and services that are reasonable and necessary to “diagnose or treat” illness or injury (with limited exceptions)
• Requirement comes from Medicare statutory principles
CA documents the subjects’ diagnosis
CTP: “Trials of diagnostic interventions may enroll healthy patients in order to have a proper control group.”
55

©2013 Aegis Compliance & Ethics Center, LLP
Therapeutic Intent Test
For the time being, application of therapeutic intent criterion is deferred to local Medicare Contractors
Principally an issue for Phase I drug studies
• Can be vast differences from one Medicare contractor to another
56

©2013 Aegis Compliance & Ethics Center, LLP
Therapeutic Intent There are two discussions of therapeutic intent in the CTP:
• “The trial must not be designed exclusively to test toxicity or disease pathophysiology. It must have therapeutic intent.”
• “The principal purpose of the trial is to test whether the intervention potentially improves the participants' health outcomes.”
57

©2013 Aegis Compliance & Ethics Center, LLP
Qualifying Clinical Trial Test - Recap It is really a four part test:
• Is the trial one of the “deemed” studies?
• Does the trial assess something in a Medicare Benefit Category?
• Does the trial enroll people with diagnosed disease?
• Does the trial have therapeutic intent?
If “no” to any one of these, it is not a QCT
58

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP 59
“Qualifying”/Approved Device Trials

©2013 Aegis Compliance & Ethics Center, LLP 60
Device Trials Always check with your Medicare
Administrative Contractor is Palmetto for the Richmond Virginia area for their specific requirements

©2013 Aegis Compliance & Ethics Center, LLP
Category A Experimental Devices
Generally not covered
• However, Medicare may cover routine costs, if the device is used for a life-threatening condition.
• Medicare contractor decides
• Device itself must be provided free
61

©2013 Aegis Compliance & Ethics Center, LLP
Category B Non-Experimental Devices
These devices can be covered under Medicare. • FDA approved IDE study protocols restrict
investigational devices shipment to a limited number of clinical sites for testing on a specific number of patients.
• Medicare coverage is based on the device continuing to meet criteria that led to the FDA category designation
62

©2013 Aegis Compliance & Ethics Center, LLP
Clinical Trials Billing
Medicare may cover procedures using devices with an IDE that have been categorized as non-experimental /investigational (Category B) Medicare only covers those procedures if:
• They involve a device the FDA has determined is non-experimental/investigational (Category B), and
• The device is furnished in accordance with FDA-approved protocols governing clinical trials
63
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
8. What does Medicare
mean by “routine costs”?
©2013 Aegis Compliance & Ethics Center, LLP 64

©2013 Aegis Compliance & Ethics Center, LLP
“Routine Costs” from the Medicare CTP
“Items or services that are typically provided absent a clinical trial (e.g., conventional care);
[Note: Not the same as “standard of care”]
“Items or services required solely for the provision of the investigational item or service (e.g., administration of a noncovered chemotherapeutic agent), the clinically appropriate monitoring of the effects of the item or service, or the prevention of complications; and
“Items or services needed for reasonable and necessary care arising from the provision of an investigational item or service--in particular, for the diagnosis or treatment of complications.”
65
©2013 Aegis Compliance & Ethics Center, LLP
Routine Costs – Short Version
1. Detection, prevention, or monitoring of complications;
2. Administration of investigational item; or
3. Conventional care
66

©2013 Aegis Compliance & Ethics Center, LLP
Detecting, preventing, or monitoring complications
Identify nexus between the item or service and a known potential side effect of the item or service
• What are the potential side effects of the drug? • What are the potential complications of use of the device?
67

©2013 Aegis Compliance & Ethics Center, LLP
Detecting, preventing, or monitoring complications
Places in which CAs identify potential side effects • Protocol • Informed Consent • Product Label • Drug compendium discussion
• AHFS-DI– American Hospital Formulary Service Drug Information • NCCN – National Comprehensive Cancer Network Drugs & Biologics
Compendium • Thompson Micromedex DrugDex • Clinical Pharmacology
68
©2013 Aegis Compliance & Ethics Center, LLP
Administration of Investigational Item
What is required to administer the investigational item?
• Surgery? • Infusion?
Note: must be something that would be covered outside of study if similar therapy or procedure occurs.
69
©2013 Aegis Compliance & Ethics Center, LLP
Conventional Care
CAs should identify objective practice guidelines
1. Professional association guidelines (e.g., National Comprehensive Cancer Network/NCCN)
2. Peer-reviewed literature 3. Significant textbooks 4. Disease-based associations 5. NIH recommendations 6. Guidelines.gov
70

©2013 Aegis Compliance & Ethics Center, LLP
Conventional Care: Example NCCN Practice Guidelines for Cancer of the Oropharynx: follow-up
Physical exam – Year 1: every 1-3 months Year 2: every 2-4 months Years 3-5: every 4-6 months > 5 Years: every 6-12 months
71

©2013 Aegis Compliance & Ethics Center, LLP
Additional Note: “All Other Medicare Rules Apply”
Coverage is available if Medicare covers the “routine cost” outside of clinical trial MCA applies normal Medicare rules on top of any item or service identified as a “routine cost”
72
©2013 Aegis Compliance & Ethics Center, LLP
Other Medicare Rules
Example: Rule against coverage of self-administered drugs (Medicare Benefits Policy Manual, Ch. 15, Sec. 50.5)
• Exception examples: • anti-emetics; • oral anti-cancer drugs
73

©2013 Aegis Compliance & Ethics Center, LLP
Routine Costs vs. Standard of Care
Just because the physician normally performs a service at a given frequency for similar patients not on trial does not mean the service qualifies as a routine cost
E.g., PSA exams for prostate cancer patients
• Study calls for monthly PSA • Physician typically does monthly PSA and argues they are
therefore “conventional care” and consequently “routine costs” • NCCN guidelines call for every 3 months • No other objective evidence produced by physician to support
medical necessity of monthly PSAs
74
©2013 Aegis Compliance & Ethics Center, LLP
Routine Costs vs. Standard of Care
EKG performed 3 days after each infusion of cardio-toxic drug during trial
• Routine cost: detecting and monitoring known side effects
Also performed at annual follow-up visits for life Is EKG at follow-up a routine cost?
75

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
9. The importance of the research coordinator in
ensuring clinical research billing is
compliant
©2013 Aegis Compliance & Ethics Center, LLP 76

©2013 Aegis Compliance & Ethics Center, LLP 77
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
10. Tips on protocol
design for investigator-initiated studies to
improve budgeting and billing
©2013 Aegis Compliance & Ethics Center, LLP 78
©2013 Aegis Compliance & Ethics Center, LLP
The design of the study impacts billing
3 Items to think about in protocols:
1. Loose use of the term “research” • If the service is being used for research purposed
and clinical care, then discuss the clinical care • When a protocol only talks about the research
aspects of a service, an auditor could ignore the clinical usefulness of the services
79

©2013 Aegis Compliance & Ethics Center, LLP
The design of the study impacts billing
3 Items to think about in protocols:
2. Stating a potential benefit • If protocol or informed consent form states that the
subject will receive no benefit from the study, then no services will be billable
• Describe in the protocol and the informed consent any potential benefit (though do not guarantee benefit)
80
©2013 Aegis Compliance & Ethics Center, LLP
The design of the study impacts billing
3 Items to think about in protocols:
3. What are the objectives in a Phase 1 study? • Is it necessary in the study to state principal and
secondary objectives of the study? Or can all objectives be stated without rank?
• Some Medicare Contractors and auditors have denied coverage to Phase 1 studies when measurement of therapeutic outcome is not a primary objective or a clearly articulated objective
81
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
11. The role of the study
calendar in clinical research billing
©2013 Aegis Compliance & Ethics Center, LLP 82

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
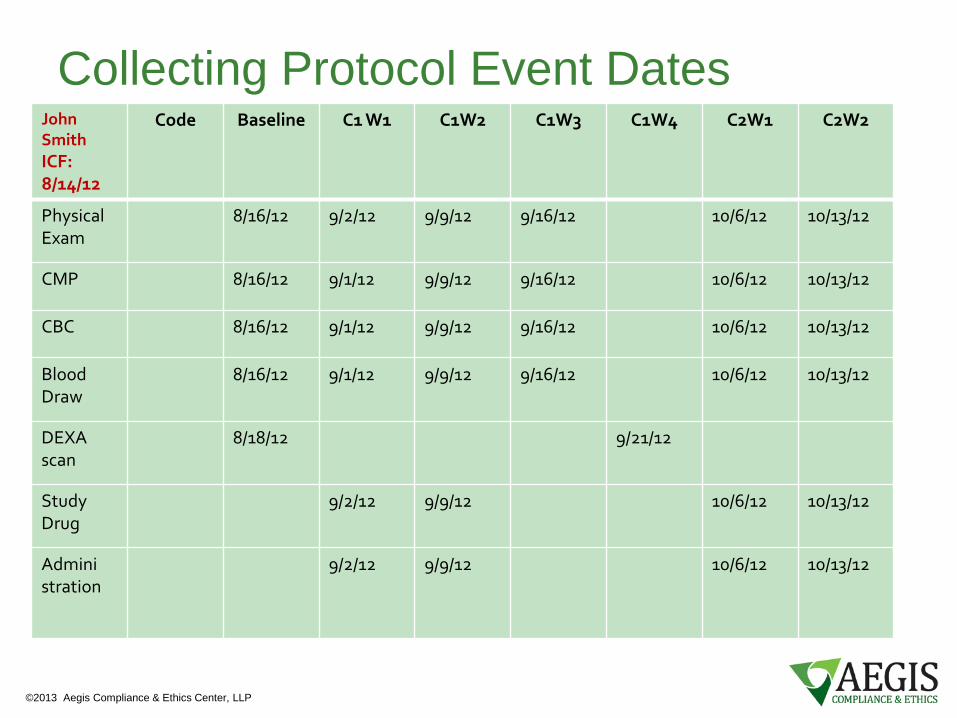
Study Calendars
• Study calendars help orient reviewers to where the subject is in the study
• The study calendar helps to sync the schedule of events with the CA
• Example: A charge for a CBC on 9/16/12 – which CBC is it?
83
©2013 Aegis Compliance & Ethics Center, LLP
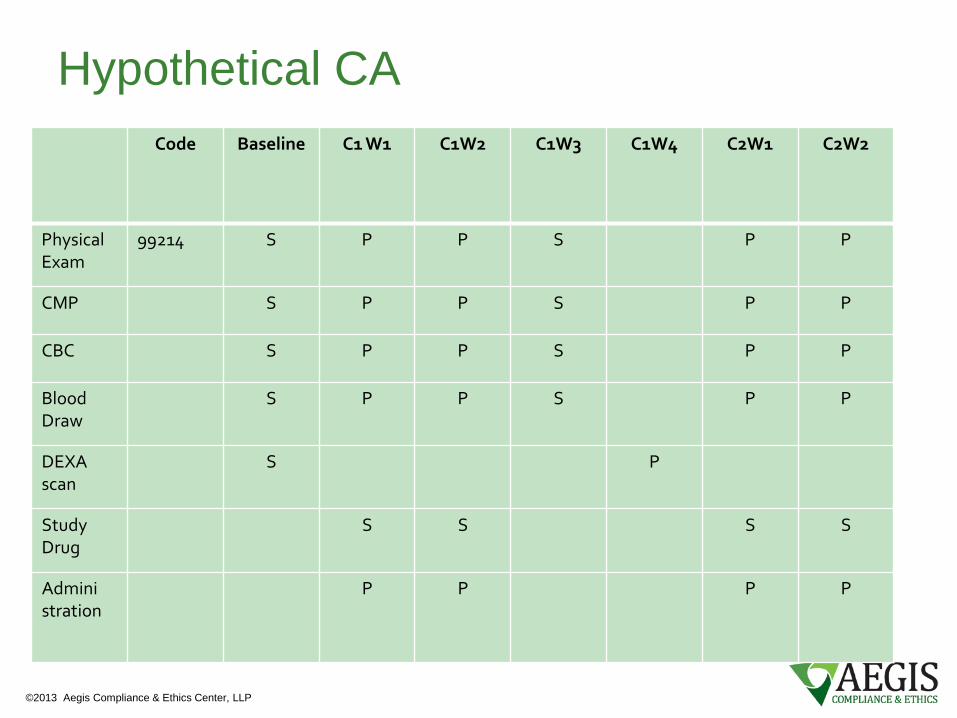
Hypothetical CA Code Baseline C1 W1 C1W2 C1W3 C1W4 C2W1 C2W2
Physical Exam
99214
S P P S P P
CMP S P P S P P
CBC S P P S P P
Blood Draw
S P P S P P
DEXA scan
S P
Study Drug
S S S S
Admini stration
P P P P
©2013 Aegis Compliance & Ethics Center, LLP
Collecting Protocol Event Dates John Smith ICF: 8/14/12
Code Baseline C1 W1 C1W2 C1W3 C1W4 C2W1 C2W2
Physical Exam
8/16/12 9/2/12 9/9/12 9/16/12 10/6/12 10/13/12
CMP 8/16/12 9/1/12 9/9/12 9/16/12 10/6/12 10/13/12
CBC 8/16/12 9/1/12 9/9/12 9/16/12 10/6/12 10/13/12
Blood Draw
8/16/12 9/1/12 9/9/12 9/16/12 10/6/12 10/13/12
DEXA scan
8/18/12 9/21/12
Study Drug
9/2/12 9/9/12 10/6/12 10/13/12
Admini stration
9/2/12 9/9/12 10/6/12 10/13/12
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
12. Improving
communications during the research study
©2013 Aegis Compliance & Ethics Center, LLP 86
©2013 Aegis Compliance & Ethics Center, LLP
Reality…
• This isn’t going to happen overnight
• Try piloting ideas for CRB claims management
• Do not be afraid to re-think plan after results of piloting
• Personal Observation: We have yet to see a CRB process which after 1 year looks the same as its roll-out
87
©2013 Aegis Compliance & Ethics Center, LLP
The importance of databases
• Sharing information and communication is a
critical feature of managing clinical research billing
• Databases and an information platform are the most common solutions
88

©2013 Aegis Compliance & Ethics Center, LLP
The importance of databases
What information to collect? • Study identification • IRB status • Subject enrollment • Study calendars • Coverage Analyses • Study document housing
89
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
13. Pause for Questions
©2013 Aegis Compliance & Ethics Center, LLP 90
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
Workshop Discussion
91
4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
14. Introduction to the
Coverage Analysis: Purposes
©2013 Aegis Compliance & Ethics Center, LLP 92

©2013 Aegis Compliance & Ethics Center, LLP
Screening C1W1 C1W2 C1W3 C1W4 C2 W1
C2 W2
C2 W3
C2 W4
After Discontinuation
Phys Exam
99201-99215
X X X X X X X X X X
ECG 93000 X X
Echo cardiogram
93000-93014
X X X
Chest CT or MRI
71250-71270, 71550-71552
X X X
Abdominal CT or MRI
74150-74170, 74181-74183
X X
Pelvis CT or MRI
72192-72194, 72195-72197
X X
Bone Scan 78300-78306
X X
CBC w/diff 85025 X X X X X X X X X X
Comprehensive Metabolic Panel
80053 X X X X X X X X X X
Study Drug J9999 X X X X
©2013 Aegis Compliance & Ethics Center, LLP
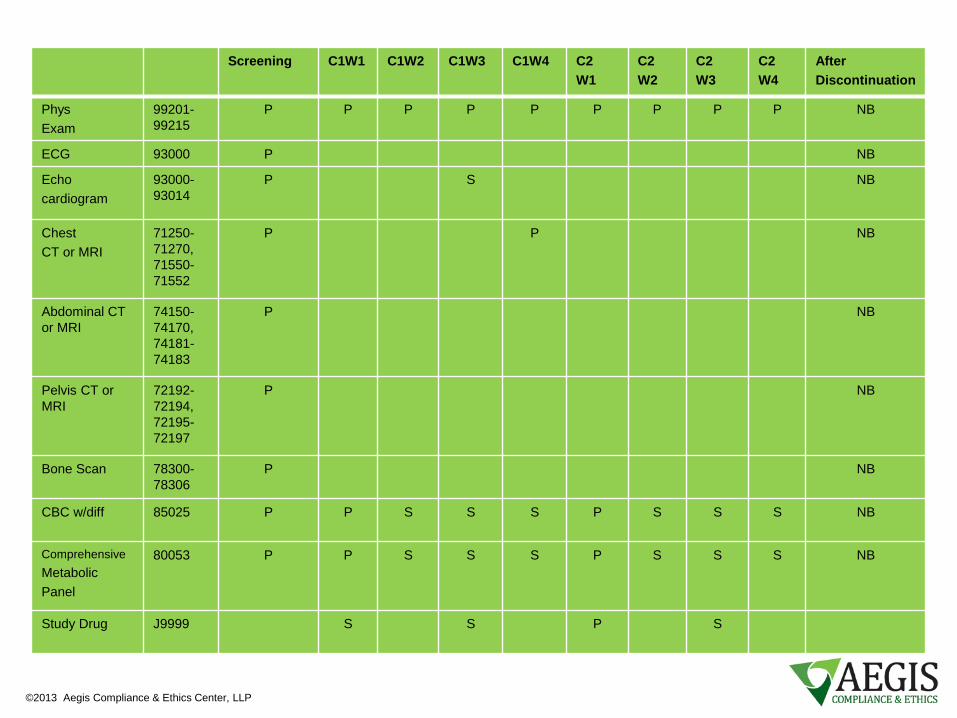
Screening C1W1 C1W2 C1W3 C1W4 C2 W1
C2 W2
C2 W3
C2 W4
After Discontinuation
Phys Exam
99201-99215
P P P P P P P P P NB
ECG 93000 P NB
Echo cardiogram
93000-93014
P S NB
Chest CT or MRI
71250-71270, 71550-71552
P P NB
Abdominal CT or MRI
74150-74170, 74181-74183
P NB
Pelvis CT or MRI
72192-72194, 72195-72197
P NB
Bone Scan 78300-78306
P NB
CBC w/diff 85025 P P S S S P S S S NB
Comprehensive Metabolic Panel
80053 P P S S S P S S S NB
Study Drug J9999 S S P S

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
15. Review of forms
needed
©2013 Aegis Compliance & Ethics Center, LLP 95
©2013 Aegis Compliance & Ethics Center, LLP
First Question
Is the study a new study or a active study?
96
©2013 Aegis Compliance & Ethics Center, LLP
Basic Documents Needed
• Protocol • CTA/Budget – Funding Document • Informed Consent Form • IND Status – drug study • FDA IDE Letter – device study
97

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
Sections 16
Development of a Coverage Analysis Step 1: Draft a grid Step 2: Review ICF Step 3: Review CTA/Budget Step 4: QCT Analysis Step 5: Which are “routine costs”? Step 6: Document reasoning Step 7: Coding the CA
©2013 Aegis Compliance & Ethics Center, LLP 98

©2013 Aegis Compliance & Ethics Center, LLP
General Order of Steps for Developing an CA: Active Study 1. Develop grid
2. What items and services are promised free in the informed consent?
3. What items and services are paid for by the sponsor?
4. Qualifying clinical trial (QCT) analysis
5. Determine items and services that are routine costs
6. Determine if routine costs are covered by Medicare
7. Apply Medicare rules to the routine costs
8. Finalize grid
99
©2013 Aegis Compliance & Ethics Center, LLP
General Order of Steps for Developing an CA: Proposed Study : 1. Develop grid 2. Perform QCT analysis 3. Identify items and services “hard-wired” free into protocol 4. Determine items and services that are routine costs 5. Determine if routine costs are covered by Medicare 6. Check proposed contract to determine if offered budget covers items and
services that are not billable 7. Negotiate contract/budget 8. Finalize “added costs” section of informed consent
9. Finalize grid once study approved
100
©2013 Aegis Compliance & Ethics Center, LLP
Recall: “Qualifying Clinical Trial” Status
101 101
©2013 Aegis Compliance & Ethics Center, LLP
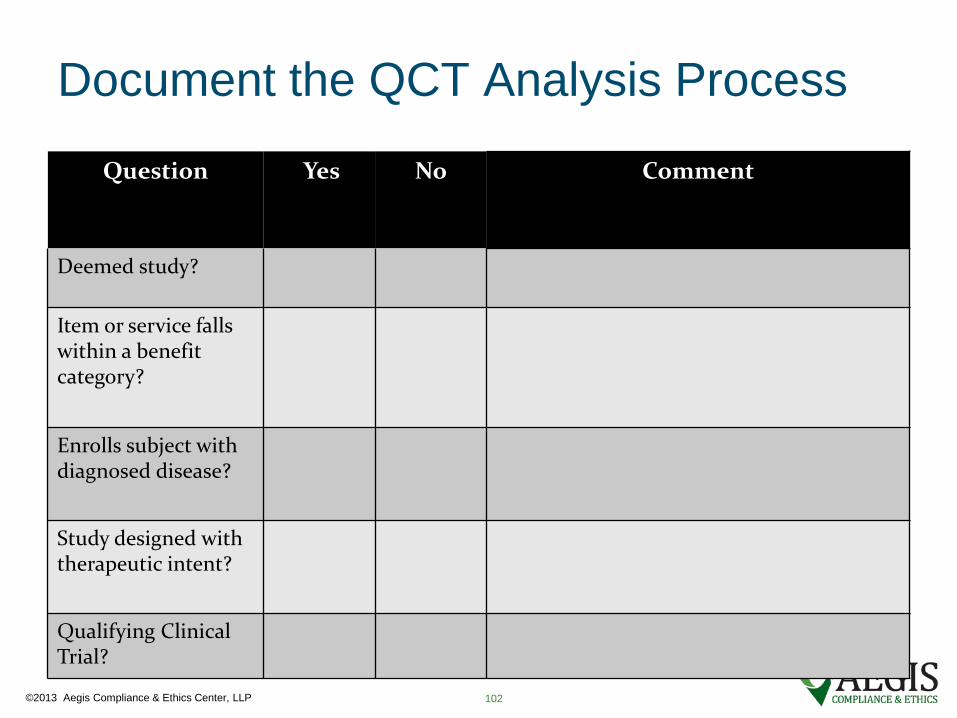
Document the QCT Analysis Process
Question Yes No Comment
Deemed study?
Item or service falls within a benefit category?
Enrolls subject with diagnosed disease?
Study designed with therapeutic intent?
Qualifying Clinical Trial?
102

©2013 Aegis Compliance & Ethics Center, LLP
Document the QCT Analysis Process
Question Yes No Comment
Deemed study? X IND # 55,512
Item or service falls within a benefit category?
X Drugs & Biologicals
Enrolls subject with diagnosed disease?
X Crohn’s Disease – Include direct quote from protocol and reference page number
Study designed with therapeutic intent?
X “To determine the efficacy of [study drug] in minimizing occurrences of abdominal pain over 24 week period.”
Qualifying Clinical Trial?
X
103
©2013 Aegis Compliance & Ethics Center, LLP
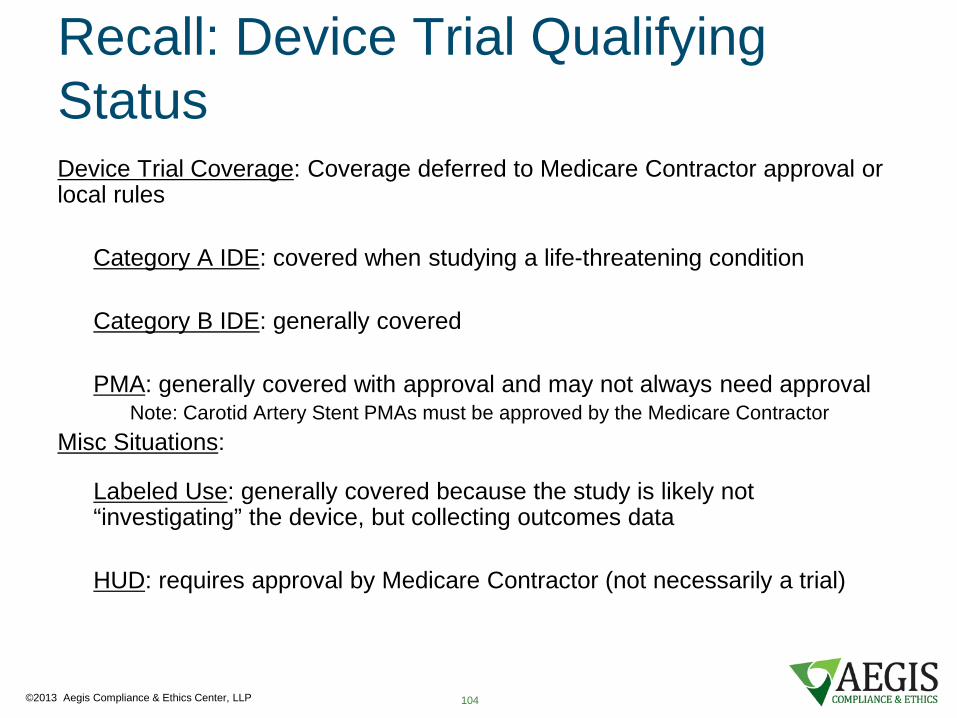
Recall: Device Trial Qualifying Status Device Trial Coverage: Coverage deferred to Medicare Contractor approval or local rules
Category A IDE: covered when studying a life-threatening condition
Category B IDE: generally covered
PMA: generally covered with approval and may not always need approval Note: Carotid Artery Stent PMAs must be approved by the Medicare Contractor
Misc Situations:
Labeled Use: generally covered because the study is likely not “investigating” the device, but collecting outcomes data HUD: requires approval by Medicare Contractor (not necessarily a trial)
104

©2013 Aegis Compliance & Ethics Center, LLP
Document Device Trial Qualifying
Question If the device has an IDE what category is it? Comments
Does the device have an IDE?
Yes Category A
Category B
No
Question If the device is FDA approved is it being studies on-label or off-label?
Comments
Is the device approved by the FDA?
Yes On-Label
Off-Label
No
Coverage Eligibility Summary
Question Yes No Supporting Explanation
Is the study eligible for coverage?
105

©2013 Aegis Compliance & Ethics Center, LLP
“Routine Cost”
Short version approach to “routine costs” used in MCAs:
1. Detection or prevention of complications 2. Conventional care 3. Administration of investigational item If study documents are not clear: will each subject enrolled
in the study need the item or service for the patient’s clinical management?
106

©2013 Aegis Compliance & Ethics Center, LLP
Which of the events are justified for billing under the coverage rules as “routine costs”?
Code Infusion 1 Infusion 2 2 weeks 12 weeks 24 weeks
Physical Exam
99201-99215
RC RC RC RC
EKG 93000 RC RC RC
Drug 123 J9999 SB SB
Infusion 96400 RC RC
Urinalysis 81000 NB NB
Ultrasound 93990 ICF
Patient Diary N/A NB NB NB NB
RC=Routine Care SB=Sponsor Billed ICF=Free in Informed Consent NB=Not billable to Medicare
©2013 Aegis Compliance & Ethics Center, LLP
Document Reasoning
EKG: “The EKG in this study is conventional care. Practice Guidelines for treatment of XYZ Condition recommend EKG at this frequency. [Cite Guidelines].”
108
©2013 Aegis Compliance & Ethics Center, LLP
Document Reasoning
EKG: “The EKG in this study is to detect complications. The study drug has known cardiotoxic effects. Protocol, p. 65.”
109

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
Research Codes
110

©2013 Aegis Compliance & Ethics Center, LLP
Research Coding Principal matters:
• V70.7 diagnosis code
• Q0/Q1 modifiers
• Condition Code 30 (research setting)
• ClinicalTrials.gov number
111
©2013 Aegis Compliance & Ethics Center, LLP
Where to find the rules Medicare Claims Processing Manual Chapter 32, Section 69.6
“Requirements for Billing Routine Costs in Clinical
Trials” Note: references to these research coding rules are scattered throughout Medicare rules and commentary, but the Claims Processing Manual provides the most concise resource and reference.
112

©2013 Aegis Compliance & Ethics Center, LLP
ClinicalTrials.gov number When a study is registered with clinicaltrials.gov (a website managed by the NIH), it is assigned an 8 digit number Providers may report the clinicaltrials.gov number on the claim form, but this is strictly voluntary today. New guidelines go into effect January 1, 2014 CMS conducts monthly aggregations of claims using the clinicaltrials.gov code
113

©2013 Aegis Compliance & Ethics Center, LLP
V70.7
“Examination of participant in clinical trial.” Used as the secondary diagnosis for all claims with research-related items and services.
Note: If used as the primary diagnosis, then the claim will be rejected.
Used for inpatient and hospital outpatient claims and physician billing.
114
©2013 Aegis Compliance & Ethics Center, LLP
Q0/Q1
Modifiers placed after CPT code on: Hospital outpatient claims Physician billing claims
Not used in inpatient hospital claims Not used for services on claims which are not related to the research study Line item by line item use
115
©2013 Aegis Compliance & Ethics Center, LLP
Q0/Q1
Q0 – “Investigational clinical service provided in a clinical research study that is in an approved clinical research study.” Q1 - “Routine clinical service provided in a clinical research study that is in an approved clinical research study.”
116

©2013 Aegis Compliance & Ethics Center, LLP
Q0
“Investigational clinical services are defined as those items and services that are being investigated as an objective within the study. Investigational clinical services may include items or services that are approved, unapproved, or otherwise covered (or not covered) under Medicare.” Examples:
• Study drugs that are billable • Category B devices • Investigational devices with Medicare approval • Laboratory tests which are identified in the objectives as
instrumental to the hypothesis
117

©2013 Aegis Compliance & Ethics Center, LLP
Q1
“Routine clinical services are defined as those items and services that are covered for Medicare beneficiaries outside of the clinical research study; are used for the direct patient management within the study; and, do not meet the definition of investigational clinical services. Routine clinical services may include items or services required solely for the provision of the investigational clinical services (e.g., administration of a chemotherapeutic agent); clinically appropriate monitoring, whether or not required by the investigational clinical service (e.g., blood tests to measure tumor markers); and items or services required for the prevention, diagnosis, or treatment of research related adverse events (e.g., blood levels of various parameters to measure kidney function).” (emphasis added)
118
©2013 Aegis Compliance & Ethics Center, LLP
Condition Code 30
• Used on the claim form whenever a V70.7 is used
• One-for-one use
119
©2013 Aegis Compliance & Ethics Center, LLP
A note on the medical record
Section 69.3 of Ch. 32 also contains the following:
“The billing provider must include in the beneficiary's medical record the following information:
trial name, sponsor, and sponsor-assigned protocol number.
This information does not need to be submitted with the claim but must be provided if requested for medical review.” (emphasis added)
120

©2013 Aegis Compliance & Ethics Center, LLP
Add-on that applies to all: Identifying treatment of complications Note that in some studies, the sponsor will pay for unscheduled events and treatment of complications. A system needs to be devised to identify these Suggestion:
• Flag studies in database which pay for treatment of complications or unscheduled events
• Batch ED census and bump against subject database for the flagged studies
• Hold charges for any matched • Obtain information from PI/study coordinator
121
©2013 Aegis Compliance & Ethics Center, LLP
Useful for Effective CRB Claims Management Database of research studies Database of research subjects CAs/tool

4147 N Ravenswood Ave Ste. 200 Chicago, IL 60613 888.739.8194 w w w . a e g i s - c o m p l i a n c e . c o m
©2013 Aegis Compliance & Ethics Center, LLP
Questions?
123









![Xtend Call Billing System Xtend Call Billing User Manual ... · This user manual allows you to learn the basics to the advanced features of Xtend Call Billing [Voice Logger]. Refer](https://img.pdfslide.net/doc/110x75/5e768c5c2dc3ff42814286c8/xtend-call-billing-system-xtend-call-billing-user-manual-this-user-manual-allows.jpg)