Embed Size (px)
Citation preview

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 1/14
Clinical Significance of Changes in the BoneMarrow and Intra-Articular Soft Tissues of theTemporomandibular Joint
Tore Arne Larheim, Tsukasa Sano, and Yoritaka Yotsui
Patients with facial pain and jaw function problems constitute a large andheterogeneous group. Disk displacement and osteoarthritis are the most com-mon intra-articular abnormalities observed at imaging. As disk displacement isseen rather frequently in asymptomatic volunteers, it is a challenge to explainwhy disk displacement sometimes is symptomatic and sometimes is not. Thepresent review focuses on abnormalities in the condylar bone marrow and theintra-articular soft tissues accompanying the disk displacement. The findings oftemporomandibular joint in asymptomatic volunteers and in temporomandib-
ular disorder (TMD) patients are reviewed. Both bone marrow edema andmarrow necrosis are documented at histology and at magnetic resonance
imaging (MRI) in TMD patients. Intra-articular soft tissue changes, such assynovitis, are additionally documented at arthroscopy. However, there is acontroversy concerning which diagnostic imaging information is essential.Although there is no doubt that disk displacement and osteoarthritis may beaccompanied by inflammatory alterations in the bone marrow and the intra-articular soft tissues, it has been difficult to consistently relate a specific imag-ing manifestation (bone edema, joint effusion, and synovitis) to joint pain.
Longitudinal studies are needed to evaluate the importance of MRI abnormal-ities in the management of TMD patients. (Semin Orthod 2012;18:30-43.) Crown
Copyright © 2012 Published by Elsevier Inc. All rights reserved.
P atients with facial pain and jaw functionproblems constitute a large and heteroge-
neous group with the umbrella diagnosis tem-poromandibular disorder (TMD).1,2 There isconsensus that myofascial pain disorder of themasticatory muscle system is the most commonof all TMDs. Disk derangement disorders andosteoarthritis are the most common intra-articu-
lar disorders. Rheumatoid arthritis is less com-mon, but is the most frequent of the arthritidesthat may involve the temporomandibular joint (TMJ). In this article, we will focus on disk de-rangement disorders and osteoarthritis.
In patients with pain and impaired jaw func-tion referred for diagnostic magnetic resonanceimaging (MRI), disk displacement with or with-out osteoarthritis is the most common intra-ar-ticular abnormality observed. However, disk dis-placement is seen rather frequently also inasymptomatic volunteers. Therefore, it has beenand still is a challenge to explain why disk dis-placement sometimes is symptomatic and some-times is not. A number of joint abnormalitiesaccompanying disk displacement have been in- vestigated.
Knowledge of TMJ findings in asymptomatic volunteers is mandatory to rule out joint mani-festations that may be responsible for patient
Department of Maxillofacial Radiology, Faculty of Dentistry,
Institute of Clinical Dentistry, University of Oslo, Oslo, Norway; Department of Oral and Maxillofacial Radiology, Tokyo Dental College, Mihama-ku, Chiba, Japan; Department of Oral Radiology,Osaka Dental University, Chuo-ku, Osaka, Japan.
Address correspondence to Tore Arne Larheim, DDS, PhD, De- partment of Maxillofacial Radiology, Institute of Clinical Dentistry, Faculty of Dentistry, University of Oslo, PO Box 1109, Blindern 0317, Oslo, Norway. E-mail: [email protected]
Crown Copyright © 2012 Published by Elsevier Inc. All rights reserved.
1073-8746/12/1801-0$30.00/0 doi:10.1053/j.sodo.2011.10.006
30 Seminars in Orthodontics, Vol 18, No 1 (March), 2012: pp 30-43

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 2/14
symptomatology. Therefore, TMJ findings inhealthy individuals will be reviewed first. Then, joint abnormalities reported as possible causesof facial pain in TMD patients will be discussed.
TMJ Findings in Asymptomatic HealthyVolunteers
Disk position and function in asymptomatic volun-teers has been thoroughly investigated. Larheimet al3 found disk displacement in about one-third of the volunteers, significantly less fre-quently than in the patients referred for MRI,and this is in accordance with a number of ear-lier studies.4-6 This study also showed that diskdisplacement in the volunteers was predomi-nantly unilateral, in contrast with the bilateral
displacement that was frequently seen in the
patients.3 Further, the disk displacement wasfound to be less severe in the volunteers; the disk was commonly (90%) displaced in one portionof the joint and normally located in another(Fig. 1). In joints with such partial disk displace-
ment, the displacement was mostly found in thelateral part of the joint, supporting an investiga-tion on the variability of disk position f rom thelateral to the medial portion of the joint.7 Partialdisk displacement has previously been con-firmed by surgery,8 and has also been observedin autopsy studies.6,9,10 Most interestingly, par-tial disk displacement occurred with similar fre-quency percentages (about 22%) in the volun-teers and the patients. In both groups, the vast majority showed reducing disk displacement.3 A higher frequency of part ial disk displacement
has also been observed.
7
Almost all displaced
Figure 1. Partial disk displacement. MRI (A, B, C) of TMJ in asymptomatic volunteer and autopsy specimen of TMJ (D, E). (A) Lateral image. (B) Centromedial image. Anterior disk displacement in lateral part and normaldisk position in centromedial part of the joint with closed mouth. (C) Open mouth image. Normal disk positionand normal bone. ([A-C] Reprinted with permission from Larheim et al, 3 © Radiological Society of North
America.) (D) Lateral section. (E) Medial section. Anterior disk displacement in lateral part and normal diskposition in medial part of the joint. ([D-E] Reprinted with permission from Larheim et al,21 © S. Karger AG,Basel, Switzerland.) (Color version of figure is available online.)
31Changes in the Bone Marrow and Soft Tissues of TMJ

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 3/14
disks in asymptomatic volunteers reported in theliterature have been found to normalize onmouth opening.3-6
Complete disk displacement, that is, disk dis-placement in all sections throughout the joint,
occurred very seldom in the volunteers, but ratheroften in the patients.3 Almost all joints with nonre-ducing disk displacement belonged to this sub-group.
Retrodiskal tissues (posterior disk attachment,bilaminar zone) in asymptomatic volunteershave a brighter signal than the disk that is uni-formly dark, with no increased signal intensity on T1- or T2-weighted magnetic resonance(MR) images.11
Contrast enhancement of intra-articular soft tis-sues on T1-weighted MR images after i.v. injec-
tion of contrast medium in asymptomatic volun-teers is very slight or is not seen. This was first demonstrated by Smith et al12 and later con-firmed by others.13,14
Joint fluid , dots or lines of bright T2 signalalong articular surfaces,15 was demonstrated inmore than half of 62 asymptomatic volunteers.16
In about one-fifth, even more fluid was ob-served, consistently related to disk displacement in that portion of the joint (Fig. 2).
Cortical bone alterations have been reportedto occur in 0 to 3% of TMJs in asymptomatic volunteers.6,17,18 The osseous changes have
consisted of condylar flattening and small os-teophyte formation found unilaterally, but oth-erwise with smooth cortical outline.18 Minimalflattening of the condyle and/or the articulareminence has been found in about one-third of
asymptomatic volunteers.17
Such an osseouschange should generally not be interpreted asosteoarthritis because the bony changes most likely represent remodeling, that is, a functionaladaptation of the joint with an intact surfacelayer.
Bone marrow of the mandibular condyle hasbeen reported as normal in all joints of allasymptomatic volunteers examined with MRI,although very few series focusing on TMJ bonemarrow in healthy individuals are available.16,17
Normal bone marrow findings at histology and
MRI are described in Tables 1 and 2,
19
andillustrated in Fig. 3.
TMJ Findings in Patients
Disk displacement is by far the most frequent intra-articular abnormality in patients with TMJdisorders. It is commonly referred to as internal derangement , defined as a mechanical fault that interferes with the smooth action of the joint.20
Joint abnormalities that may accompany internalderangement will be discussed in the following
Figure 2. Normal joint fluid. MRI of TMJ in asymptomatic volunteer. (A) Proton-density image. (B) Corre-sponding T2-weighted image. Increased T2 signal consistent with fluid in superior joint compartment of theanterolateral recess. (The disk is displaced in this part of the joint.) Maximum amount of fluid seen inasymptomatic volunteers. (Reprinted with permission from Larheim et al.16)
32 Larheim, Sano, and Yotsui

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 4/14
sections, with focus on changes in the bone mar-row and intra-articular soft tissues.21,22
Bone Marrow Abnormalities
In a series of 50 TMJs in 44 patients in whomMRI and surgery were performed for painfulinternal derangements, a core biopsy specimen was obtained from the marrow of the mandibu-lar condyles at the time of surgery.19 The biopsy
was obtained whether or not abnormal MRI sig-nals were seen from the condyle marrow. Thishighly selected material from surgically treatedpatients showed histologically abnormal bonemarrow in more than one-third (36%) of the joints. Half of these joints showed marrow edema without osteonecrosis (Fig. 4) and theother half showed osteonecrosis (Fig. 5) with or without marrow edema. Table 2 shows the MRIclassification of the bone marrow, and Table 3
shows the correlation of MRI and histologic eval-uation of the core biopsy specimens. More thanhalf of the joints with marrow edema were nor-mal on MRI, probably because the edemas werefocal, occupying only small areas of the condyle
marrow (Fig. 4). Thus, MRI seemed to be fairly insensitive for the detection of focal marrow edemas, as also experienced in an experimentalstudy of the femoral head.23
The detection of osteonecrosis in the mandib-ular condyle with MRI showed a sensitivity of 78% (Table 3).19 The most reliable MRI featureof osteonecrosis in the bone marrow was foundto be a combination of edema pattern and scle-rosis pattern (Fig. 6). Marrow sclerosis patternon MRI could either be osteonecrosis (Fig. 7) oradvanced osteoarthritis without osteonecrosis,
histologically (Fig. 8), giving a positive predictive value of only 54%. Thus, an overestimation of osteonecrosis was found when the imaging diag-nosis was based on the MR signal pattern of marrow sclerosis (Table 3). The combination of decreased and increased MR signal recognizedin osteonecrotic TMJs is rather similar to the“double line sign” seen on T2-weighted imagesof hip or knee osteonecrosis.24,25 The focal sub-chondral signal intensity in those joints isthought to represent sclerosis and hyper vasculargranulation tissue w ith devitalized bone.25,26
Larheim et al19 found that 39% (7 of 18
cases) with histologically documented marrow edema and/or osteonecrosis showed MRI signsof joint effusion (Fig. 7), in both early and late
Table 2. MRI Classification of Bone Marrow of Mandibular Condyles
MRI Classification Signal Intensity Patterns
I. Normal Homogeneous bright signal onT1-weighted (protondensity) images andhomogenous intermediatesignal on T2-weightedimages.
II. Edema Decreased signal on T1- weighted (proton density)images and increased signalon T2-weighted images;edema pattern.
III. Osteonecrosis a. Decreased signal on T1- weighted (proton density)images and on T2-weightedimages; sclerosis pattern.
b. Combination of edema (II)and sclerosis (IIIa) pattern.
Reprinted with permission from Larheim et al.19
Table 1. Histologic Classification of Core Biopsiesof Mandibular Condyles
Histologic Classification Description of Microscopic Features
I. Normal a. Without reactive bone formation:
Normal marrow architecture,preservation of thehematopoietic marrow, normaltrabecular and cortical bonearchitecture.
b. With reactive bone formation:Normal marrow architecture,preservation of thehematopoietic marrow, evidenceof increased bone cell activity,increased bone remodeling andreactive bone formation.
II. Edema a. Early: Edema fluid with serumprotein exudate within marrow interstitium, preservation of hematopoietic marrow elements,
no evidence of reticulin fibrosis.b. Late: Edema fluid with serumprotein exudate within marrow interstitium, preservation of hematopoietic marrow elements,focal evidence of disruption of marrow interstitium and reticulinfibrosis.
III. Osteonecrosis a. Early: Loss of hematopoieticmarrow elements, loss of normalmarrow stroma and marrow fat,no evidence of reticulin fibrosis.
b. Late: Loss of hematopoieticmarrow elements, loss of normalmarrow stroma and marrow fat,evidence of reticulin fibrosis.
Reprinted with permission from Larheim et al.19
33Changes in the Bone Marrow and Soft Tissues of TMJ

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 5/14
osteonecrosis. This is in accordance with MRIobservations in the various stages of osteonecro-sis of the hip.27 In a consecutive series of patients with internal TMJ derangements and evident joint effusion, abnormal bone marrow wasfound in 31%.28 In both these studies,19,28 joint effusion was defined as a larger amount of TMJfluid t han was seen in any asymptomatic volun-
teer.16
The association between abnormal bone
marrow and effusion in the TMJ has been alsoobserved previously in clinical MRI studies.29-31
Almost half (4 of 9) of the patients with his-tologically documented marrow edema (without evidence of necrosis) and 2 patients with histo-logic evidence of osteonecrosis showed normalcortical bone on MRI.19 The observation of ab-normal bone marrow in joints with intact corti-
cal outline has been substantiated in clinicalMRI studies28,32,33 (Fig. 9), suggesting that mar-
Figure 3. Normal bone marrow. MRI (A, B) of TMJ and bone marrow biopsy of mandibular condyle (C) in TMDpatient. (A) Proton-density image. (B) Corresponding T2-weighted image. Normal homogeneous signal fromthe bone marrow (and slightly displaced disk and small condylar osteophyte). (C) Histologic section showsnormal hematopoietic elements interspersed with marrow fat and intact trabecular bone (Hematoxylin eosin;original magnification 50). (Reprinted with permission from Larheim et al.19) (Color version of figure isavailable online.)
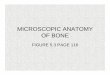
Figure 4. Bone marrow edema. Bone marrow biopsy of mandibular condyle in TMD patient. Histologicsection shows early marrow edema, a patchy focus
with serum proteins within marrow interstitium sur-rounded by areas of normal hematopoietic marrow (Hematoxylin eosin; original magnification 50).(Reprinted with permission from Larheim et al.19)(Color version of figure is available online.)
Figure 5. Bone marrow necrosis. Bone marrow bi-opsy of mandibular condyle in TMD patient. Histo-logic section shows osteonecrosis, complete loss of hematopoietic marrow and evidence of inflammatory cell infiltrate (Hematoxylin eosin; original magnifica-tion 50). (Reprinted with permission from Larheimet al.19) (Color version of figure is available online.)
34 Larheim, Sano, and Yotsui

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 6/14
row edema and osteonecrosis may occur as sep-arate entities from osteoarthritis of the TMJ.This is well known from the hip where osteoar-thritis develops secondary to osteonecrosis after
weakening of the subarticular bone with collapseand subarticular fracture.34
The pathogenesis of osteonecrosis is, in gen-eral, poorly understood, but it is well known that marrow edema in the hip may be a precursor toosteonecrosis, and that a marrow edema condi-tion may be transient.23,35 In the hip, the predis-posing factors for osteonecrosis include sicklecell disease, long-term steroid therapy, and alco-
holism. Nontraumatic cases are frequently bilat-eral; how ev er, trauma can cause unilateral osteo-necrosis.36 No such systemic factors were present in the patient group studied with histology of the TMJ, and all cases were unilateral, including
the 2 patients with bilateral histologic observa-tions.19 Therefore, the pathogenesis may be dif-ferent in the TMJ than in other joints. As most patients with histologic evidence of osteonecro-sis showed MRI signs of osteoarthritis and allpatients had internal derangement, the etiology in the TMJ may be possibly related to local mi-crotrauma from internal derangement ratherthan vascular compromise. However, bone mar-row abnormalities seem to occur in both joints with and without int ernal TMJ derangement.Recently, Orhan et al37 demonstrated marrow
alterations of the TMJs in patients with chronicanemia, showing no cases with internal TMJ de-rangement and using healthy individuals as con-trols. This is the first study reporting bone mar-row alterations in the TMJs of patients withsystemic diseases.
The relationship between bone marrow alter-ations and osteoarthritis is not fully understood,not in the TMJ,19 or in other joints. It was re-
Table 3. Correlation of MRI Interpretation andHistologic Evaluation of Core Biopsy Specimensfrom 50 Mandibular Condyles
MRI
Histology Normal
Marrow
Edema Osteonecrosis Total
Normal 27 2 3 32Marrow edema 5 1 3 9Osteonecrosis 2 0 7 9Total 34 3 13 50
MRI, magnetic resonance imaging.Reprinted with permission from Larheim et al.19
Figure 6. Disk displacement, osteoarthritis, and bone marrow necrosis. MRI (A, B) of TMJ and bone marrow biopsy (C, D) of mandibular condyle in TMD patient. (A) Proton-density image with open mouth. (B)Corresponding T2-weighted image. Anterior disk displacement without reduction, osteoarthritis, and marrow edema pattern combined with marrow sclerosis pattern within the condylar head. Marrow edema pattern;decreased signal on proton-density image (A) and increased signal on T2-weighted image (B). Marrow sclerosispattern; decreased signal on proton-density image (A) and on T2-weighted image (B). (C) Histologic sectionshows osteonecrosis, complete loss of hematopoietic marrow and evidence of inflammatory cell infiltrate.(Hematoxylin eosin; original magnification 50.) (D) Histologic section shows marked increase of reticulinfiber deposition. (Reticulin fiberstain; original magnification 50.) (Reprinted with permission from Larheimet al.19) (Color version of figure is available online.)
35Changes in the Bone Marrow and Soft Tissues of TMJ

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 7/14
cently stated that bone marrow edema may play a central role in the evolution of knee osteoar-thritis and needs to be further explored.38 More-over, the distinction between primary osteone-
crosis and necrosis secondary to osteoarthritismay be impossible based on core biopsy speci-mens. In advanced cases of osteoarthritis, micro-scopic foci of necrosis are frequently foundimmediately adjacent to the joint surface. Occa-sionally, small infarcts can occur, but again they are found at the joint surface and only in joints with advanced osteoarthritis.39 The end-stages of both of these pathologic processes are likely tobe indistinguishable.
Bone marrow edema is generally demonstratedas a nonspecific finding on MRI in relation to a
number of conditions, including osteoarthritis.40
When it occurs in isolation not triggered by any obvious bone pathology in a clinical setting of joint pain, it constitutes the “bone marrow edema syn-drome.” Radiology–histology correlation studieshave, however, shown variably interstitial marrow edema, necrosis, fibrosis, and trabecular bone ab-normalities. In studies that have attempted to elu-cidate the underlying histopathology, conflictingevidence has thus been generated with regards to
the contribution of the various morphologic ele-ments yielding the bone marrow edema patternon MRI.40 Further research in this field is needed.
Intra-Articular Soft Tissue Changes
Changes in the retrodiskal tissues that are not seenin asymptomatic volunteers have been demon-strated in patients with TMJ disorders. Sano and Westesson41 demonstrated a correlation be-tween increased T2 signal in this area and TMJpain. More recently, this observation was con-firmed by Chiba et al,42 who found that 22% of 283 TMJs showed an increased T2 signal andthat 77% of those reported pain compared with44% of those with low signal intensity. They also
showed that the high signal intensity was closely related to the severity of internal derangement,occurring in 8.5% of joints with reducing diskdisplacement, in 21.8% of joints with nonreduc-ing disk displacement, and in 32.4% of joints with nonreducing disk displacement and osteo-arthritis.
Chiba et al42 applied T2-weighted fat-sup-pressed MR images of TMJs to confirm the pres-ence of increased water content, consistent with
Figure 7. Disk displacement, osteoarthritis, and bone marrow necrosis with joint effusion. MRI of TMJ in TMDpatient. (A) Proton-density image. (B) Corresponding T2-weighted image. Disk displacement, osteoarthritis,
joint effusion in superior joint component, and marrow sclerosis pattern (see Fig. 6) in major part of themandibular condyle. Histology (not shown) demonstrated osteonecrosis. (Reprinted with permission fromLarheim et al.19)
36 Larheim, Sano, and Yotsui

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 8/14
inflammatory changes in the posterior disk at-tachment. However, it should be noted that themajority of the joints showed reduced signalintensity in the posterior disk attachment. Inprevious studies on internal TMJ derangement,such reduced signal has been associated withfibrosis,43,44 probably a result of altered function
and loading in this area.Contrast enhancement of intra-articular soft tissues
after i.v. contrast-medium injection has beenshown in several studies.13,14,45,46 One of thesestudies focused on contrast enhancement of theposterior disk attachment,13 whereas the othersdemonstrated contrast enhancement in the in-ferior or the superior joint compartment (Fig.10). In all studies, contrast-enhanced TMJs wereassociated with internal derangement and joint pain. In one of these studies, the thickness of thesoft tissue surrounding the condyle was mea-
sured to a mean of 4.58 mm in the painful TMJgroup, compared with 1.03 mm in the painlessTMJ group and 0.71 mm in the control group,demonstrating a significant difference betweenthe painful TMJ group and the other 2 groups.14
It is unclear what kind of tissue is enhancingin these TMJ studies because no histologic doc-umentation is available. However, in one study of knee joints with osteoarthritis or rheumatoidarthritis, MR assessment of contrast enhance-
ment and joint effusion was compared with his-tologically diagnosed biopsies.47 The amount of contrast enhancement correlated with the over-all histologic assessment of inflammation andreflected the mass of cell-infiltrated vascularizedsubsynovial tissue, and to lesser extent the cu-mulative synovial proliferative activity.
Arthroscopic TMJ studies have frequently shownsynovitis and osteoarthritis.48-51 Synovitis hasbeen defined as hypervascularity (hyperemia) orsynovial hyperplasia, and osteoarthritis has beendefined as fissured articular eminence or disk,subchondral bone exposure, or disk perfora-tion.51 In one of these studies, 90% of 114 highly symptomatic TMJs showed synovitis when basedon the degree of vascularity alone.50 Osteoarthri-tis was found in 62% of the joints, of which the vast majority (92%) had an associated synovitis.Osteoarthritis was based on the appearance of
fissure or erosion of the cartilage lining at thearticular eminence as well as fissure or perfora-tion of the disk. The majority of the jointsshowed synovitis and osteoarthritis or only syno- vitis; only osteoarthritis rarely occurred.50 Theseobservations substantiate those of previous ar-throscopic studies,48,49 although placing evenmore emphasis on the prevalence of synovitis.
Joint effusion was found to reflect TMJ synovitis inone arthroscopic study of internal derangements.52
Figure 8. Disk displacement, osteoarthritis but no bone marrow necrosis. MRI (A, B) of TMJ and bone marrow
biopsy (C) of mandibular condyle in TMD patient. (A) Proton-density image. (B) Corresponding T2-weightedimage. Anterior disk displacement and osteoarthritis, marrow sclerosis pattern (see Fig. 6) in major part of thecondyle. (C) Histologic section shows replacement of marrow space by dense sclerotic bone and fibrous tissue,suggesting a reparative process and not osteonecrosis (Hematoxylin eosin; original magnification 50).(Reprinted with permission from Larheim et al.19) (Color version of figure is available online.)
37Changes in the Bone Marrow and Soft Tissues of TMJ

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 9/14
This seems to be the first study that has comparedthe amount of joint fluid and the degree of synovitis.It should be noted that joint effusion was defined asmore fluid than just lines of increased T2 signalintensity in the joint compartments.
Histologic evidence of inflammatory changes in
symptomatic TMJs based on biopsies obtainedduring open TMJ surgery procedures has beendemonstrated in several studies. In particular, analtered vascularity has been consistently ob-served, being increased53-56 or decreased.57-59
Furthermore, synovial proliferation has beendemonstrated.55,60,61
What Diagnostic Imaging Information Is Essential?
There seems to be no doubt that internal derange-ment and osteoarthritis are frequent TMJ abnor-
malities in patients with TMJ disorders. It is alsoclear that these manifestations may be accompa-nied by inflammatory alterations in the bone mar-row and the soft tissues. However, it has beendifficult to consistently relate a specific imagingmanifestation to the joint pain. Also, longitudinalstudies on the outcome of treatment have givenconflicting results. This is not specific for theTMJ. Chronic or recurrent pain in the knee is acentral feature of osteoarthritis, but consistent cor-
relations have not been found between pain andimaging findings of osteoarthritis.38
Another aspect of the TMJ literature becameobvious in a systematic literature review on theefficacy of MRI in the diagnosis of degenerativeand inflammatory TMDs.62 The authors con-
cluded that in
5% of the articles reviewed, theconclusions were based on moderate or low levelsof evidence.
Bone Marrow Abnormalities
In one TMJ study, patients with abnormal bonemarrow on MRI had a greater degree of painthan those with normal bone marrow.33 That study also indicated that those with bone mar-row edema pattern had more severe pain thanthose with bone marrow sclerosis pattern, al-
though this difference was not significant. In alater study, Sano et al63 found such significanceand reported that patients with a marrow edemapattern had a higher degree of pain. Further, ina study of different imaging manifestations re-corded before and after the performance of ar-throcentesis of the TMJ, it was shown that thisprocedure was clinically successful (resolvingpain) and associated with a significant decreasein the prevalence of TMJ bone marrow edema.64
Figure 9. Disk displacement, normal cortical bone, and bone marrow edema. MRI of TMJ in TMD patient. (A)Proton-density image. (B) Corresponding T2-weighted image. Anterior disk displacement, normal cortical bone,and marrow edema pattern (see Fig. 6) in entire condyle. (Reprinted with permission from Larheim et al.28)
38 Larheim, Sano, and Yotsui

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 10/14
The findings were contradicted by Chiba et al65
in a longitudinal study, demonstrating persis-tence of bone marrow edema in 70% of the joints with a clinically successful arthrocentesis.
In one study, Yajima et al66 demonstrated that a symptomatic osteoarthritic TMJ can accom-pany increased signal of the condylar bone mar-row on proton density-weighted MR images.
Associations between bone marrow edemaand joint pain in other joints, such as the
knee38,67,68 and the hip,69-71 are reported. How-ever, there are also reports showing no signifi-cant correlations between joint pain and MR findings of the bone marrow.72,73
Joint Effusion
Even more conflicting results have been demon-strated for TMJ effusion, which has been foundto be associated with pain in several cross-sec-tional studies but not in others. In a longitudinalMRI study, TMJ pain was alleviated or resolved
in all joints in which the amount of fluid de-creased.74 It was also stated by Emshoff and Ru-disch75 that presence or absence of effusion may prove to be an important diagnostic determi-nant in successful arthrocentesis. Previously, thesame authors suggested that pain was not reli-able for predicting the presence of effusion in aconsecutive series of patients with TMJ pain.76
Similarly, changes in the amount of joint effu-sion was not related to the patients’ clinical con-
dition, when MRI before and after TMJ ar-throscopic lysis and lavage was compared.77
The definition of joint effusion has varied sub-stantially, and the fact that TMJ fluid is rathercommon in asymptomatic volunteers and that theamount of fluid may be evident 16 should be paidmore attention. This was also recently empha-sized.78 Knowledge about the amount of joint fluidseen in healthy volunteers is of great importance alsoin the diagnostic assessment of knee79 and ankle
joints.80 The latter study demonstrated no significant differences between the amount of fluid in patientsand asymptomatic volunteers. In the knee study, theauthors reported the normal range of variation inasymptomatic volunteers, including the rare cases of more evident fluid. They concluded that joint effu-sion should be expected when the amount of fluidexceeded t he maximum amount observed in healthy volunteers.79 In a TMJ study where a similar defini-tion was applied, 15% of 500 patients had in-creased amounts of fluid.28 Of the 70 patients with joint effusion, 30% had bone marrow abnormali-
ties, and most of these had complete disk displace-ment without reduction.28
Synovitis
A more recent study demonstrated that the se- verity of synovitis significantly improved afterarthroscopic surgery with visually guided TMJirrigation.51 However, this improvement did not seem to be associated with the clinical outcome.
Figure 10. Disk displacement, osteoarthritis, and contrast enhancement. MRI of TMJ in TMD patient (who alsohad rheumatoid arthritis). (A) T1-weighted precontrast image. (B) T1-weighted postcontrast image. Anteriordisk displacement, osteoarthritis, and enhancement of intra-articular soft tissue around the disk and in theposterior attachment. (Reprinted with permission from Larheim et al.,21 © S. Karger AG, Basel, Switzerland.)
39Changes in the Bone Marrow and Soft Tissues of TMJ

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 11/14
In one study comparing i.v. contrast enhance-ment at MRI before and after nonsurgical treat-ment, decreased contrast enhancement of theposterior disk attachment was observed in 7 of 10 joints and was associated with the resolution
or reduction of joint pain.81
The authors statedthat this association “was much stronger thanthe association between the clinical findings andthe anatomy of the disk.”
Disk Position, Morphology, andMobility
In one MRI study of disk position, disk morphol-ogy, and disk mobility before and after 4 differ-ent treatments for closed lock, Ohnuki et al82
found that neither disk position nor morphol-
ogy did improve despite the clinically successfultreatment. The improved mobility of the disk was the only investigated variable that could berelated to clinical success; stuck disk indicatedunsuccessful clinical outcome. The same conclu-sion was made by Kurita et al83 in a long-termfollow-up study of TMD patients: “Patients whoappeared symptomatic at a younger age or whohad a fixed disk were the most likely to haverecurrent or persistent clinical signs/symptomsof TMJ disorder after 8 years.”
Impaired TMJ function with lack of normaldisk mobility seems to be an important cause of
pain. This is also in accordance with one of theconclusions in a recent systematic literature re- view.84 The calculated odds ratio for the rela-tionship between pain and disk displacement without reduction was rather high, but the oddsratios for pain were generally low in relation toother MRI findings. This is not unexpected be-cause nonreducing disk displacements occur al-most exclusively in patients, whereas less severeforms of disk displacements also occur in asymp-tomatic volunteers as discussed earlier in ourreview article.
The systematic literature review revealed a vast heterogeneity in study design, clinical exam-ination methods, and diagnostic criteria. Theconclusions concerning the relationship be-tween pain and various MRI findings were con-tradictory, although significant relationships were reported for some studies concerning joint effusion and bone marrow edema.84
There is probably no unique factor that canexplain the joint pain in patients with TMJ
problems.85 Moreover, the subgroup of pa-tients showing joint abnormalities additionalto the internal derangement (disk displace-ment) and osteoarthritis constitutes only a mi-nor portion of TMD pat ients referred for di-
agnostic TMJ imaging.21
Conclusions
Future studies must use standardized and well-described imaging criteria for TMJ diagnosis. It is mandatory to have knowledge about MR find-ings in asymptomatic healthy volunteers. As im-aging signs of inflammation fluctuate over time,longitudinal studies are needed to evaluate theimportance of MRI in the management of TMD
patients.
References
1. Laskin DM, Greene CS, Hylander WL: Temporomandib-
ular disorders: An evidence-based approach to diagnosisand treatment. Chicago, Quintessence, 2006
2. Scrivani SJ, Keith DA, Kaban LB: Temporomandibular
disorders. N Engl J Med 359:2693-2705, 2008
3. Larheim TA, Westesson P-L, Sano T: Temporomandib-ular joint disk displacement: Comparison in asymptom-
atic volunteers and patients. Radiology 218:428-432,
2001
4. Kircos LT, Ortendahl DA, Mark AS, et al: Magneticresonance imaging of the TMJ disc in asymptomatic
volunteers. J Oral Maxillofac Surg 45:852-854, 1987
5. Katzberg RW, Westesson PL, Tallents RH, et al: Ana-
tomic disorders of the temporomandibular joint disc inasymptomatic subjects. J Oral Maxillofac Surg 54:147-
153, 1996
6. Tasaki MM, Westesson PL, Isberg AM, et al: Classifica-
tion and prevalence of temporomandibular joint diskdisplacement in patients and symptom-free volunteers.
Am J Orthod Dentofacial Orthop 109:249-262, 1996
7. Rammelsberg P, Pospiech PR, Jäger L, et al: Variability of
disk position in asymptomatic volunteers and patients with internal derangements of the TMJ. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 83:393-399, 1997
8. Kerstens HC, Golding RP, Valk J, et al: Magnetic reso-
nance imaging of partial temporomandibular joint discdisplacement. J Oral Maxillofac Surg 47:25-29, 1989
9. Katzberg RW, Westesson PL, Tallents RH, et al: Tem-
poromandibular joint: MR assessment of rotational and
sideways disk displacements. Radiology 169:741-748,1988
10. Dijkgraaf LC, de Bont LG, Otten E, et al: Three-dimen-
sional visualization of the temporomandibular joint: A
computerized multisectional autopsy study of disc positionand configuration. J Oral Maxillofac Surg 50:2-10, 1992
40 Larheim, Sano, and Yotsui

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 12/14
11. Katzberg RW, Tallents RH: Normal and abnormal tem-poromandibular joint disc and posterior attachment as
depicted by magnetic resonance imaging in symptom-
atic and asymptomatic subjects. J Oral Maxillofac Surg63:1155-1161, 2005
12. Smith HJ, Larheim TA, Aspestrand F: Rheumatic and
nonrheumatic disease in the temporomandibular joint:Gadolinium-enhanced MR imaging. Radiology 185:229-
234, 1992
13. Suenaga S, Hamamoto S, Kawano K, et al: Dynamic MR imaging of the temporomandibular joint in patients with
arthrosis: Relationship between contrast enhancement of the posterior disk attachment and joint pain. AJR
Am J Roentgenol 166:1475-1481, 1996
14. Farina D, Bodin C, Gandolfi S, et al: TMJ disorders andpain: Assessment by contrast-enhanced MRI. Eur J Ra-
diol 70:25-30, 2009
15. Westesson PL, Brooks SL: Temporomandibular joint:Relationship between MR evidence of effusion and the
presence of pain and disk displacement. AJR Am JRoentgenol 159:559-563, 1992
16. Larheim TA, Katzberg RW, Westesson PL, et al: MR
evidence of temporomandibular joint fluid and condylemarrow alterations: Occurrence in asymptomatic volun-
teers and symptomatic patients. Int J Oral Maxillofac
Surg 30:113-117, 200117. Brooks SL, Westesson PL, Eriksson L, et al: Prevalence of
osseous changes in the temporomandibular joint of asymptomatic persons without internal derangement.
Oral Surg Oral Med Oral Pathol 73:118-122, 1992
18. Ribeiro RF, Tallents RH, Katzberg RW, et al: The prev-alence of disc displacement in symptomatic and asymp-
tomatic volunteers aged 6 to 25 years. J Orofac Pain
11:37-47, 199719. Larheim TA, Westesson PL, Hicks DG, et al: Osteone-
crosis of the temporomandibular joint: Correlation of magnetic resonance imaging and histology. J Oral Max-
illofac Surg 57:888-898, 1999
20. Adams JC: Outline of Orthopaedics. Edinburgh, ChurchillLivingstone, 2001
21. Larheim TA: Role of magnetic resonance imaging in the
clinical diagnosis of the temporomandibular joint. CellsTissues Organs 180:6-21, 2005
22. Larheim TA, Westesson P-L: TMJ Imaging in Laskin DM,Greene CS, Hylander WL (eds): Temporomandibular Dis-
orders: An Evidence-Based Approach to Diagnosis and
Treatment. Chicago, Quintessence, 2006, pp 149-17923. Nakamura T, Matsumoto T, Nishino M, et al: Early
magnetic resonance imaging and histologic findings in a
model of femoral head necrosis. Clin Orthop Relat Res334:68-72, 1997
24. Gil HC, Levine SM, Zoga AC: MRI Findings in the sub-chondral bone marrow: a discussion of conditions in-
cluding transient osteoporosis, transient bone marrow edema syndrome, SONK, and shifting bone marrow
edema of the knee. Semin Musculoskelet Radiol 10:177-186, 2006
25. Hayes CW, Conway WF, Daniel WW: MR imaging of
bone marrow edema pattern: Transient osteoporosis,transient bone marrow edema syndrome, or osteonecro-
sis. Radiographics 13:1001-1011, 1993
26. Mitchell DG, Rao VM, Dalinka MK, et al: Femoral headavascular necrosis: Correlation of MR imaging, radio-graphic staging, radionuclide imaging, and clinical find-ings. Radiology 162:709-715, 1987
27. Mitchell DG, Steinberg ME, Dalinka MK, et al: Magneticresonance imaging of the ischemic hip. Alterations
within the osteonecrotic, viable, and reactive zones. ClinOrthop Relat Res 244:60-77, 1989
28. Larheim TA, Westesson PL, Sano T: MR grading of temporomandibular joint fluid: Association with diskdisplacement categories, condyle marrow abnormalitiesand pain. Int J Oral Maxillofac Surg 30:104-112, 2001
29. Schellhas KP, Wilkes CH: Temporomandibular joint in-flammation: Comparison of MR fast scanning with T1-and T2-weighted imaging techniques. AJR Am J Roent-genol 153:93-98, 1989
30. Schellhas KP, Wilkes CH, Fritts HM, et al: MR of osteo-chondritis dissecans and avascular necrosis of the man-dibular condyle. AJR Am J Roentgenol 152:551-560,1989
31. Schellhas KP, Piper MA, Omlie MR: Facial skeleton re-
modeling due to temporomandibular joint degenera-tion: An imaging study of 100 patients. AJR Am J Roent-genol 155:373-383, 1990
32. Sano T, Westesson PL, Larheim TA, et al: Osteoarthritisand abnormal bone marrow of the mandibular condyle.Oral Surg Oral Med Oral Pathol Oral Radiol Endod87:243-252, 1999
33. Sano T, Westesson PL, Larheim TA, et al: The associa-tion of temporomandibular joint pain with abnormalbone marrow in the mandibular condyle. J Oral Maxil-lofac Surg 58:254-257, 2000
34. Sweet D, Madewell J: Pathogenesis of osteonecrosis, inResnick D, Niwayama G (eds): Diagnosis of Bone and Joint Disorders. Philadelphia, WB Saunders, 1988, pp3188-3237
35. Plenk H Jr, Hofmann S, Eschberger J, et al: Histomor-phology and bone morphometry of the bone marrow edema syndrome of the hip. Clin Orthop Relat Res1997:73-84
36. Hauzeur JP, Pasteels JL, Orloff S: Bilateral non-traumaticaseptic osteonecrosis in the femoral head. An experi-mental study of incidence. J Bone Joint Surg Am 69:1221-1225, 1987
37. Orhan K, Delilbasi C, Paksoy C: Magnetic resonance imagingevaluation of mandibular condyle bone marrow and tem-poromandibular joint disc signal intensity in anaemia pa-tients. Dentomaxillofac Radiol 38:247-254, 2009
38. Link TM: Correlations between joint morphology andpain and between magnetic resonance imaging, histol-
ogy, and micro-computed tomography. J Bone Joint Surg Am 91:30-32, 200939. Milgram JW: Radiologic and histologic pathology of
nontumorous diseases of bones and joints. Northbrook,IL, Northbrook Pub, Co, 1990
40. Thiryayi WA, Thiryayi SA, Freemont AJ: Histopatholog-ical perspective on bone marrow oedema, reactive bonechange and haemorrhage. Eur J Radiol 67:62-67, 2008
41. Sano T, Westesson PL: Magnetic resonance imaging of the temporomandibular joint. Increased T2 signal in theretrodiskal tissue of painful joints. Oral Surg Oral MedOral Pathol Oral Radiol Endod 79:511-516, 1995
41Changes in the Bone Marrow and Soft Tissues of TMJ

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 13/14
42. Chiba M, Kumagai M, Echigo S: Association betweenhigh signal intensity in the posterior disc attachment
seen on T2 weighted fat-suppressed images and tem-
poromandibular joint pain. Dentomaxillofac Radiol 36:187-191, 2007
43. Westesson PL, Paesani D: MR imaging of the TMJ. De-
creased signal from the retrodiskal tissue. Oral Surg OralMed Oral Pathol 76:631-635, 1993
44. Manzione JV, Tallents RH: “Pseudomeniscus” sign: Po-
tential indicator of repair or remodeling in temporo-mandibular joints with internal derangements. Pre-
sented to the Radiologic Society of North America.Radiology185(suppl):175, 1992
45. Ogasawara T, Kitagawa Y, Ogawa T, et al: Inflammatory
change in the upper joint space in temporomandibular joint with internal derangement on gadolinium-enhanced MR im-
aging. Int J Oral Maxillofac Surg 31:252-256, 2002
46. Matsumura Y, Nomura J, Murata T, et al: Magnetic res-onance imaging of synovial proliferation in temporo-
mandibular disorders with pain. J Comput Assist To-mogr 28:73-79, 2004
47. Østergaard M, Stoltenberg M, Løvgreen-Nielsen P, et al:
Magnetic resonance imaging-determined synovial mem-brane and joint effusion volumes in rheumatoid arthritis
and osteoarthritis: Comparison with the macroscopic
and microscopic appearance of the synovium. ArthritisRheum 40:1856-1867, 1997
48. Holmlund A, Hellsing G: Arthroscopy of the temporo-mandibular joint: Occurrence and location of osteoar-
throsis and synovitis in a patient material. Int J Oral
Maxillofac Surg 17:36-40, 198849. Holmlund A, Hellsing G, Axelsson S: The temporoman-
dibular joint: A comparison of clinical and arthroscopic
findings. J Prosthet Dent 62:61-65, 198950. Israel HA, Diamond BE, Saed-Nejad F, et al: Correlation
between arthroscopic diagnosis of osteoarthritis and sy-novitis of the human temporomandibular joint and
keratan sulfate levels in the synovial fluid. J Oral Maxil-
lofac Surg 55:210-217, 199751. Hamada Y, Holmlund AB, Kondoh T, et al: Severity of
arthroscopically observed pathology and levels of inflam-
matory cytokines in the synovial fluid before and after visually guided temporomandibular joint irrigation cor-
related with the clinical outcome in patients withchronic closed lock. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 106:343-349, 2008
52. Segami N, Nishimura M, Kaneyama K, et al: Does joint effusion on T2 magnetic resonance images reflect syno-
vitis? Comparison of arthroscopic findings in internal
derangements of the temporomandibular joint. OralSurg Oral Med Oral Pathol Oral Radiol Endod 92:341-
345, 200153. Scapino RP: Histopathology associated with malposition
of the human temporomandibular joint disc. Oral SurgOral Med Oral Pathol 55:382-397, 1983
54. Kurita K, Westesson PL, Sternby NH, et al: Histologicfeatures of the temporomandibular joint disk and pos-
terior disk attachment: Comparison of symptom-free
persons with normally positioned disks and patients withinternal derangement. Oral Surg Oral Med Oral Pathol
67:635-643, 1989
55. Holmlund AB, Gynther GW, Reinholt FP: Disk derange-ment and inflammatory changes in the posterior disk at-tachment of the temporomandibular joint. A histologicstudy. Oral Surg Oral Med Oral Pathol 73:9-12, 1992
56. Paegle DI, Holmlund AB, Reinholt FP: Characterization of tissue components in the temporomandibular joint disc
and posterior disc attachment region: Internal derange-ment and control autopsy specimens compared by mor-phometry. J Oral Maxillofac Surg 60:1032-1037, 2002
57. Hall MB, Brown RW, Baughman RA: Histologic appear-ance of the bilaminar zone in internal derangement of the temporomandibular joint. Oral Surg Oral Med OralPathol 58:375-381, 1984
58. Isacsson G, Isberg A, Johansson AS, et al: Internal de-rangement of the temporomandibular joint: Radio-graphic and histologic changes associated with severepain. J Oral Maxillofac Surg 44:771-778, 1986
59. Isberg A, Isacsson G, Johansson AS, et al: Hyperplasticsoft-tissue formation in the temporomandibular joint associated with internal derangement. A radiographicand histologic study. Oral Surg Oral Med Oral Pathol
61:32-38, 198660. Bjørnland T, Refsum SB: Histopathologic changes of the
temporomandibular joint disk in patients with chronicarthritic disease. A comparison with internal derange-ment. Oral Surg Oral Med Oral Pathol 77:572-578, 1994
61. Takaku S, Toyoda T, Sano T, et al: Correlation of mag-netic resonance imaging and surgical findings in pa-tients with temporomandibular joint disorders. J OralMaxillofac Surg 53:1283-1288, 1995
62. Limchaichana N, Petersson A, Rohlin M: The efficacy of magnetic resonance imaging in the diagnosis of degen-erative and inflammatory temporomandibular joint dis-orders: A systematic literature review. Oral Surg OralMed Oral Pathol Oral Radiol Endod 102:521-536, 2006
63. Sano T, Westesson PL, Yamamoto M, et al: Differences
in temporomandibular joint pain and age distributionbetween marrow edema and osteonecrosis in the man-dibular condyle. Cranio 22:283-288, 2004
64. Emshoff R, Gerhard S, Ennemoser T, et al: Magneticresonance imaging findings of internal derangement, os-teoarthrosis, effusion, and bone marrow edema before andafter performance of arthrocentesis and hydraulic disten-sion of the temporomandibular joint. Oral Surg Oral MedOral Pathol Oral Radiol Endod 101:784-790, 2006
65. Chiba M, Kumagai M, Fukui N, et al: The relationship of bone marrow edema pattern in the mandibular condyle with joint pain in patients with temporomandibular joint disorders: Longitudinal study with MR imaging. Int J Oral Maxillofac Surg 35:55-59, 2006
66. Yajima A, Sano T, Otonari-Yamamoto M, et al: MR evi-dence of characteristics in symptomatic osteoarthritis of the temporomandibular joint: Increased signal intensity ratio on proton density-weighted images of bone marrow in the mandibular condyle. Cranio 25:250-256, 2007
67. Felson DT, Chaisson CE, Hill CL, et al: The associationof bone marrow lesions with pain in knee osteoarthritis. Ann Intern Med 134:541-549, 2001
68. Felson DT, Niu J, Guermazi A, et al: Correlation of thedevelopment of knee pain with enlarging bone marrow lesions on magnetic resonance imaging. ArthritisRheum 56:2986-2992, 2007
42 Larheim, Sano, and Yotsui

7/17/2019 Clinical Significance of Changes in the Bone.pdf
http://slidepdf.com/reader/full/clinical-significance-of-changes-in-the-bonepdf 14/14
69. Koo KH, Ahn IO, Kim R, et al: Bone marrow edema andassociated pain in early stage osteonecrosis of the femo-ral head: Prospective study with serial MR images. Radi-ology 213:715-722, 1999
70. Huang GS, Chan WP, Chang YC, et al: MR imaging of bone marrow edema and joint effusion in patients with
osteonecrosis of the femoral head: Relationship to pain. AJR Am J Roentgenol 181:545-549, 2003
71. Ito H, Matsuno T, Minami A: Relationship between bonemarrow edema and development of symptoms in pa-tients with osteonecrosis of the femoral head. AJR Am JRoentgenol 186:1761-1770, 2006
72. Kornaat PR, Bloem JL, Ceulemans RY, et al: Osteoarthri-tis of the knee: Association between clinical features andMR imaging findings. Radiology 239:811-817, 2006
73. Kornaat PR, Kloppenburg M, Sharma R, et al: Bonemarrow edema-like lesions change in volume in themajority of patients with osteoarthritis; associations withclinical features. Eur Radiol 17:3073-3078, 2007
74. Yano K, Sano T, Okano T: A longitudinal study of mag-netic resonance (MR) evidence of temporomandibular
joint (TMJ) fluid in patients with TMJ disorders. Cranio22:64-71, 2004
75. Emshoff R, Rudisch A: Temporomandibular joint inter-nal derangement and osteoarthrosis: Are effusion andbone marrow edema prognostic indicators for arthro-centesis and hydraulic distention? J Oral Maxillofac Surg65:66-73, 2007
76. Rudisch A, Innerhofer K, Bertram S, et al: Magneticresonance imaging findings of internal derangement and effusion in patients with unilateral temporomandib-ular joint pain. Oral Surg Oral Med Oral Pathol OralRadiol Endod 92:566-571, 2001
77. Sato J, Segami N, Kaneyama K, et al: Importance of thechanges in joint effusion shown by magnetic resonanceimaging before and after arthroscopic lysis and lavage of
the temporomandibular joint. Br J Oral Maxillofac Surg40:72-75, 2002
78. Manfredini D, Basso D, Arboretti R, et al: Association
between magnetic resonance signs of temporoman-
dibular joint effusion and disk displacement. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 107:
266-271, 2009
79. Ginalski JM, Landry M, Meuli RA: Normal range of
intraarticular fluid in the knee of healthy volunteers:Easy evaluation with MRI. Eur Radiol 3:135-137, 1993
80. Schweitzer ME, van Leersum M, Ehrlich SS, et al: Fluid
in normal and abnormal ankle joints: Amount and dis-
tribution as seen on MR images. AJR Am J Roentgenol
162:111-114, 1994
81. Suenaga S, Sonoda S, Oku T, et al: MRI of the temporo-
mandibular joint disk and posterior disk attachment
before and after nonsurgical treatment. J Comput Assist
Tomogr 21:892-896, 1997
82. Ohnuki T, Fukuda M, Nakata A, et al: Evaluation of the
position, mobility, and morphology of the disc by MRI
before and after four different treatments for temporo-
mandibular joint disorders. Dentomaxillofac Radiol 35:
103-109, 2006
83. Kurita H, Uehara S, Zhao C, et al: Baseline clinical and
radiographic features are associated with long-term (8
years) signs/symptoms for subjects with diseased tem-
poromandibular joint. Dentomaxillofac Radiol 36:155-
159, 2007
84. Koh KJ, List T, Petersson A, et al: Relationship between
clinical and magnetic resonance imaging diagnoses and
findings in degenerative and inflammatory temporo-
mandibular joint diseases: A systematic literature review.
J Orofac Pain 23:123-139, 2009
85. Emshoff R, Brandlmaier I, Bertram S, et al: Relative odds
of temporomandibular joint pain as a function of mag-
netic resonance imaging findings of internal derange-
ment, osteoarthrosis, effusion, and bone marrow edema.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod95:437-445, 2003
43Changes in the Bone Marrow and Soft Tissues of TMJ