Embed Size (px)
Citation preview
Clinical Stars Lead a Successful Professional Practice Program!
Deborah Devine, MS, RN, AOCN, CRNI Carolyn Dietrich MS, RN IV, CPAN
Amanda Nenaber MS, RN, CCNS, PCCN Michelle Rudolph BSN, RN III, CMSRN
INTERPROFESSIONAL GRAND ROUNDSFebruary 11, 2013
Session Objectives
1. Describe the elements that create a winning clinical nurse led professional practice program.
2. Review longitudinal data used to constantly improve program components and outcomes.
• Academic Medical Center• Not-for-profit• 407 licensed beds• 1,500 clinical RNs• 3 X recognized ANCC
Magnet® Hospital• ANCC Magnet Prize® for
Innovation in EBP• ANCC Magnet Nurse of the
Year: Neurosurgical APN • Ranked #1 Hospital in Denver• Ranked #1 in Quality by UHC
University of Colorado Hospital
Profile: UCH Nursing
• Certified nurses = 44%• BSN or higher degree clinical nurses =
84.5%• Inpatient nursing workforce key
demographic:– 50% of inpatient nursing workforce are
graduates of our UHC/AACN Post-Baccalaureate Nurse Residency program
• Average age of our clinical RNs = 41 years
• Succession Planning: 53 % of educators, CNS, managers & directors advanced to Levels III or IV in our UEXCEL Professional Practice Program prior to becoming nurse leaders
RN Practice Program Literature
• Significant body of literature on practice programs since 1972, when Zimmer first published on clinical ladders. Highlights of recent literature include:– Winslow, et al (2011): revitalized their long-
standing program using their shared governance structure to drive changes
– Murphy et al (2011): linked professional practice program to performance expectations to strengthen professionalism
– Pierson, et al (2010): described a 20 year clinical ladder program’s evolution related to recruitment, retention
– Watts, M. (2010): described program emphasizing certification to enhance professionalism
Professional Practice Model
Background: UEXCELProfessional Practice Program
• Initiated 22 years ago in 1990 after 2 years of planning.
• Goal: to establish a professional practice program for all registered clinical nurses at UCH providing direct patient care– Credentials nurses to practice, provides
program standards of practice to unify RNs across the hospital services, serves as the criteria for performance appraisals, and provides an opportunity for advancement.
• Standards based on ANA Standards for Clinical Nurse Practice
– Evidence-based practice and research are the foundation for professional nurse practice at UCH
UEXCEL Professional Practice Program
• Framework: Benner’s Novice to Expert (1984), based on Dreyfus theory of skill acquisition.
• Four Levels: – Level I: BSN prepared graduate nurse resident– Level II: competent professional nurse– Level III: advanced proficient nurse– Level IV: Expert professional RN
• Four categories of standards: Exemplary Professional Practice, Transformational Leadership, Structural Empowerment, New Knowledge and Innovation.
• Human Resources: Each level represents a distinct and separate job description, salary range and new classification.
UEXCEL Clinical Nurse Practice Roles• LEVEL I
– Entry level Advanced Beginner: graduated from an accredited baccalaureate or Masters entry into practice program. All newly licensed RNs participate in the UHC/AANC Nurse Residency Program; hired into Inpatient, Peri-Operative & Emergency Services.
• LEVEL II– Experienced clinician who is Competent to care for complex
patients. Works collaboratively on healthcare team, incorporates research and life long learning into practice, participates in quality initiatives.
• LEVEL III– Advanced, Proficient nurse clinician, recognized as leader in
clinical area. Takes active role to improve patient outcomes, education, management. Promotes safety and professional development; participates in professional activities; certified in specialty.
• LEVEL IV– Demonstrates Expert clinical skills. Regarded as clinical
authority & resource within the unit/service and hospital. Significant degree of responsibility & leadership; acts as mentor, resource. Active in professional organization; certified in specialty.
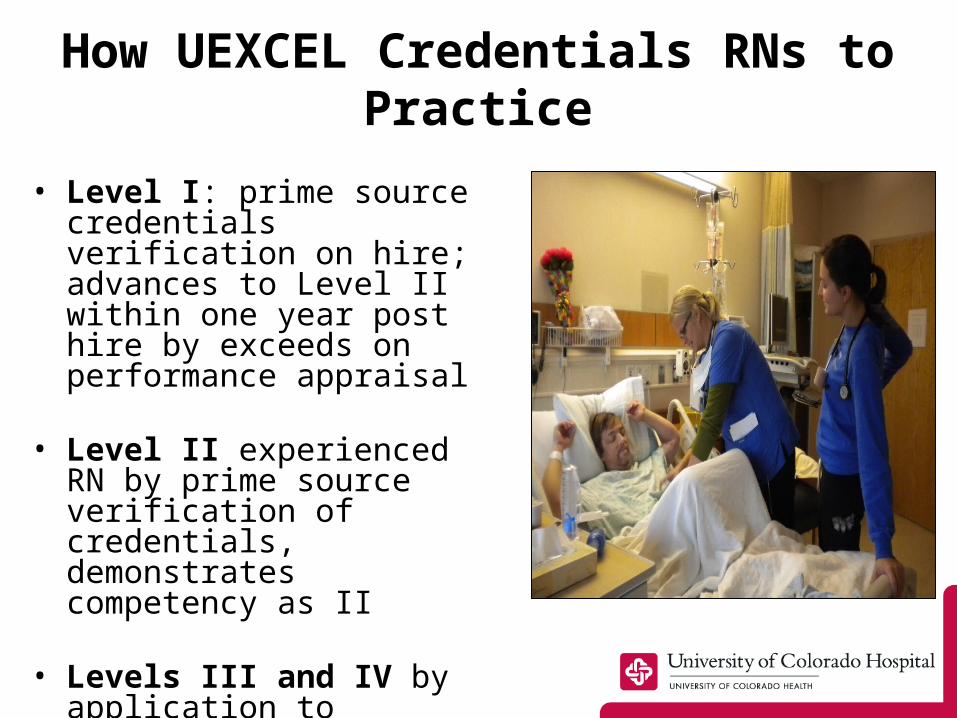
How UEXCEL Credentials RNs to Practice
• Level I: prime source credentials verification on hire; advances to Level II within one year post hire by exceeds on performance appraisal
• Level II experienced RN by prime source verification of credentials, demonstrates competency as II
• Levels III and IV by application to advance; Board review & approval of paper or digital portfolio
What Does it Mean To Advance?
• Advancement demonstrates personal achievement as a professional nurse; raises the bar for practice!
• Provides professional growth opportunities; EBP and Research projects add value to service, hospital
• Provides fiscal rewards
• Strengthens professional practice through peer review
12
UEXCEL BOARD
• The UEXCEL Board is the governing body for the practice program.
• Chair: clinical RN; co-chair is a nursing director • Composition of Board: 33 clinical nurses representing
hospital clinical areas; other members by related entities: HR, Educator, Nurse Manager, CNO/VP
• Structure: Meetings held monthly; clinical nurses commit to 3 year term of service
UEXCEL Board Roles• Reviews, approves credentials of clinical registered nurses
for the four levels of nursing practice.• Supports the philosophy, vision, goals of professional
nursing by maintaining oversight of nursing practice standards across hospital services.
• Provides path for career promotion through mentoring & development., including education, guidance to nurses interested in advancing, advisor course for mentors.
• Provides professional structure for evaluating registered nurse performance within the UCH Human Resources Performance Management program.
• Maintains, updates bylaws defining the UEXCEL structure, program functions.
• Sponsors longitudinal evaluation of clinical nurse satisfaction with the UEXCEL Practice Program.
• Supports special nursing groups within the Practice Program: example is Level IV Nurse Council.
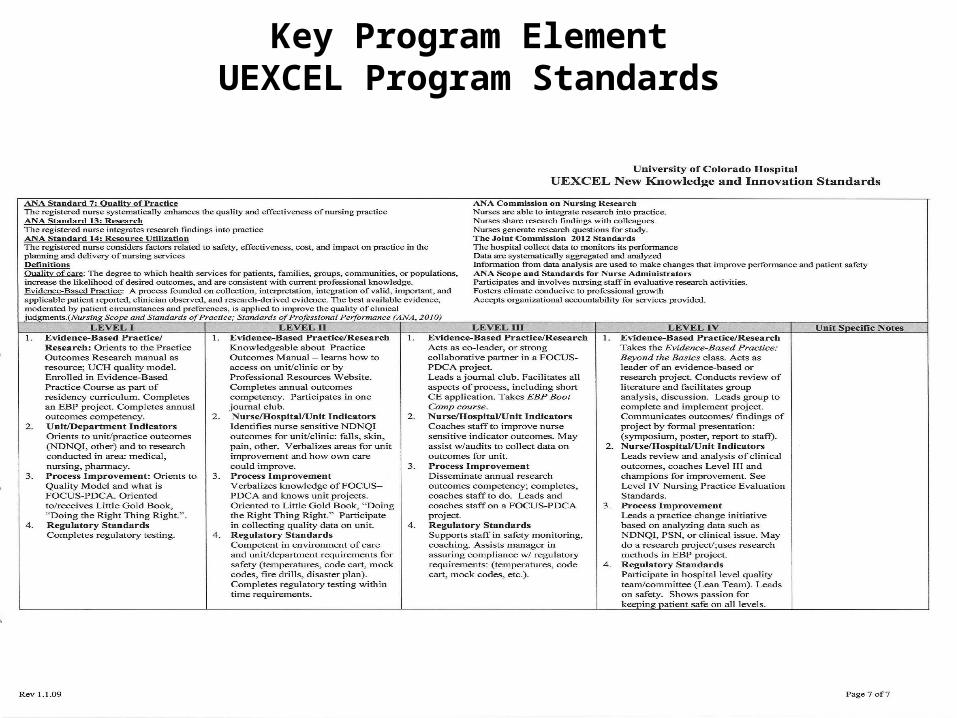
Key Program ElementUEXCEL Program Standards
Key Program Element: Clinical Narratives
• UCH values reflective practice to support development of nursing practice and critical thinking
• Reflective practice is emphasized at all levels of practice– Level I: complete narratives during one year
residency – Level II: informally give narrative account or
written account of practice in their self evaluation for performance appraisal process if desiring a role model (exceeds) rating
– Level III and Level IV: complete a formal narrative as part of portfolio for advancement
(Johns, 2004)
Clinical Narrative
16
Key Program Element: Peer Review Process
• Peer review is a hallmark of a professional practice program, essential to our shared leadership framework
• A professional practice model with a peer review process reinforces high standards of practice
• The UEXCEL peer review methods maintain standards, evaluate performance and provide credibility.
Cummings et al (2010)Kramer, Maguire & Brewer (2011)
17
Key Element: UEXCEL Mentorship
• All levels of clinical nurse practice receive mentoring: – nurse residents in first year of
practice– Level II RNs by mentoring to set
annual goals, defining career plans for education, advancement to Level III
– Level III continued development, advance to Level IV
• Nurses advancing must select a mentor advisor for the credentialing process: – Mentors take Advisor Certification
Course – Receive standardized language and
direction– Encourage ongoing career
development & leadership growth beyond achieving advancement
Brooks et al, (1995)Luzinski (2011)
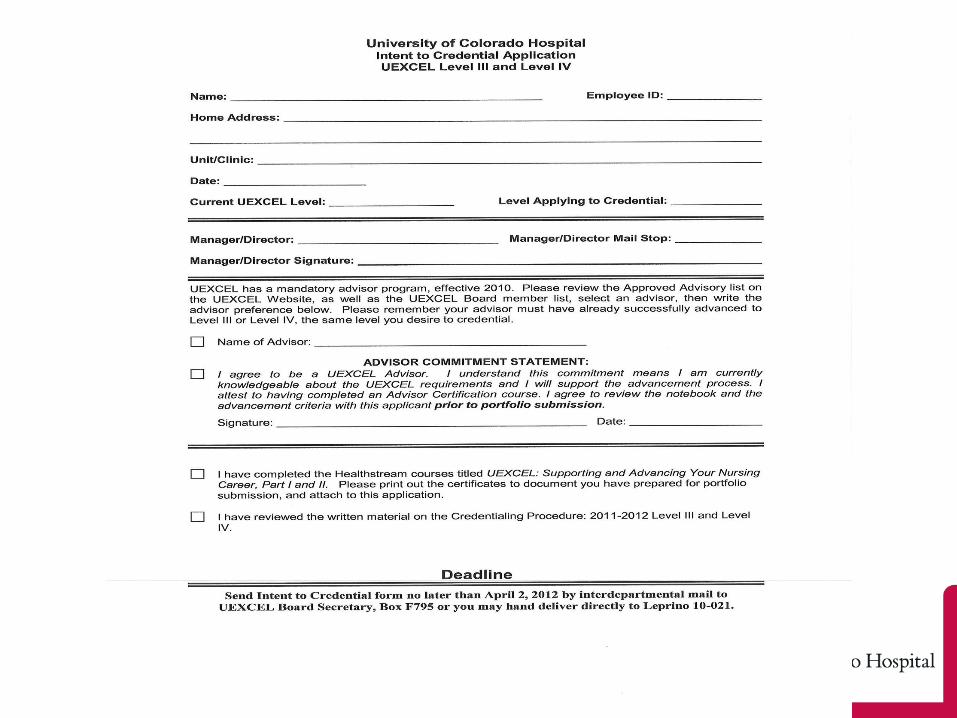
Level III and IV Advancement Requirements
• Role Model status on current performance appraisal
• Currently enrolled in BSN (level III), or holds BSN (level IV)
• Certified advisor who advanced to level nurse applicant aspires to reach
• Follows steps outlined in credentialing procedure
• Takes on-line learning center course on advancement process
• Portfolio submitted on time, with all sections completed per requirements
Portfolio Section IExemplary Professional
Practice• Two Letters of Recommendation
– RN Manager or RN Director (Ambulatory)– RN Peer
• Performance Appraisal– Copy of most recent performance appraisal– Role Model rating
• Clinical Narrative– Your nursing voice– Philosophy/values; how you practice these values– Provide current clinical example showing how your practice
has advanced/ changed to reflect level III or IV• Resume in professional format• Copy of BSN degree, or proof of active enrollment for
Level III RN
Portfolio Section IITransformational Leadership
– Unit or Institutional Project (s)• Additional work, not just day to day role• Adds value to unit/hospital
– Policy and Procedure, Standards, Guidelines
• Contributes to improving care, applying evidence-based practice; includes literature review, abstracts, or citations
• Follows institutional procedures for approval eg. Professional Practice Council, internal approval per unit, Pt. Education Committee review, other
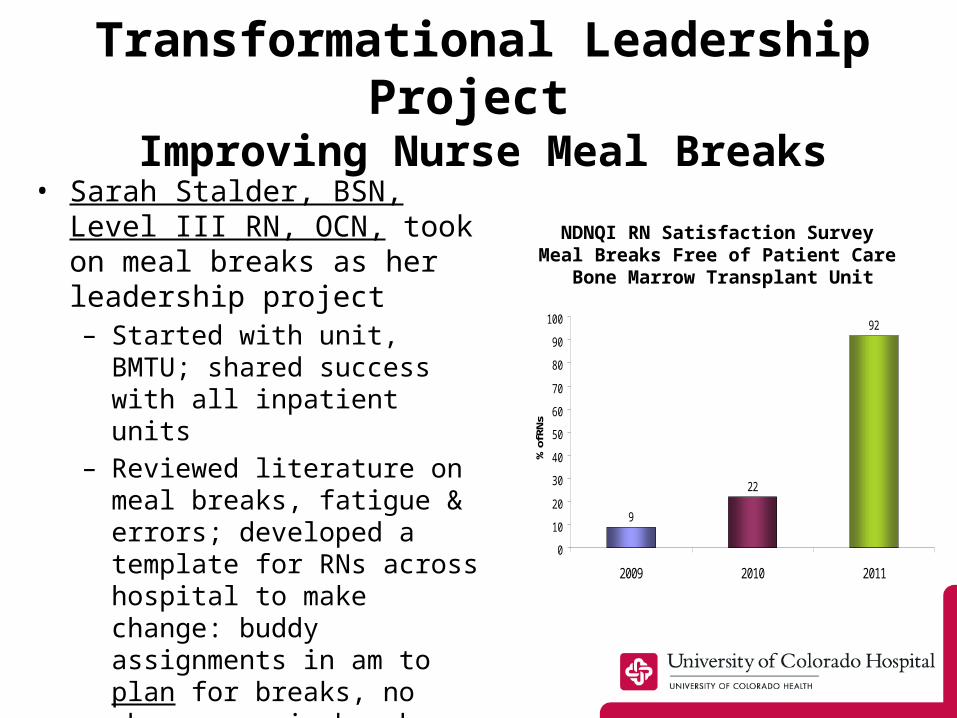
Transformational Leadership Project
Improving Nurse Meal Breaks• Sarah Stalder, BSN, Level
III RN, OCN, took on meal breaks as her leadership project– Started with unit, BMTU;
shared success with all inpatient units
– Reviewed literature on meal breaks, fatigue & errors; developed a template for RNs across hospital to make change: buddy assignments in am to plan for breaks, no phone zone in break rooms, peer teams to reinforce break time culture change
9
22
92
0
10
20
30
40
50
60
70
80
90
100
2009 2010 2011
% o
f RNs
NDNQI RN Satisfaction Survey Meal Breaks Free of Patient Care
Bone Marrow Transplant Unit
Portfolio Section IIIStructural Empowerment
Peer to Peer Teaching/ Structural Changes Based On Standards– Teaching Activities
• Preceptor– Include certificate and evaluation form samples
• Conducting an in-service, skills lab, or teaching a CNE class, or leading a Clinical Review Session or Journal Club
– Include copies of CE application, attendance record, evaluations
– Projects Incorporating National, Other Standards
H.U.S.H Project
• Noise Reduction Project based on EPA, AHRQ Data, and JC Environment of Care Standards
• Initiated in the PACU by team & lead Rachel Romero, Level IV, MSN, RN, CPAN, CAPA and Monica Brock, Level IV, MSN, RN, CPAN
• Literature review; reports from similar projects in other hospitals
• Implemented 4 interventions: signs, device to measure noise, noise cancelling devices, professional education
Clinical Narrative
• Pre-H.U.S.H– Average reported noise =
4.16– Noise level most frequent
= 5– % patients reporting noise
level 4 or higher = 83%
• Post –H.U.S.H– Average reported noise
= 2.90– Noise level most
frequent = 3– % patients reporting
noise level of 4 or higher = 25%
• Also conducted surveys of RNs, Users of noise cancelling devices
Section IVNew Knowledge, Innovations & Improvements
– Role leading a Quality, EBP or Research Project
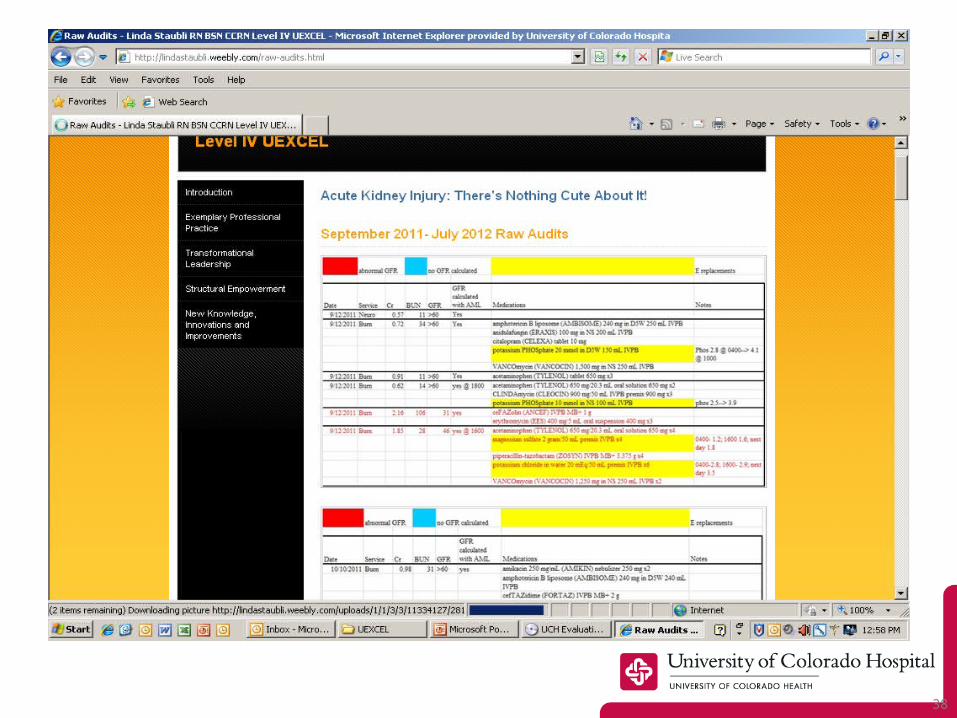
• Studies, collects and analyzes data on a unit/hospital quality issues, FOCUS-PDCA
– Include audit forms and graphs when appropriate– Must document outcomes in any outcomes project
– Serves on a champion of change team– What did RN do to actively improve outcomes or make a
change on unit/service?
– Facilitates a Journal Club or Clinical Review Session
– Include article, critique, and attendance record– How did this impact/change practice on your unit?
Outcomes required
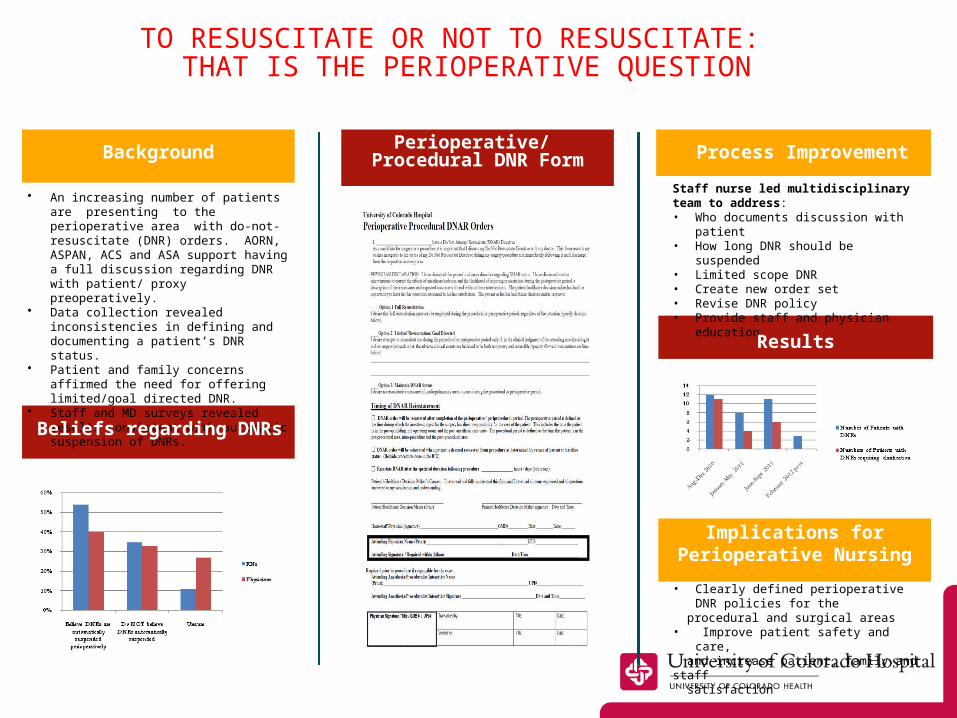
Nicole Babu BSN, RN, CPAN, Michelle Ballou BSN, RN, CPAN and Barbara Krumbach MSN, RN, CNS, CPAN, CCRN
• An increasing number of patients are presenting to the perioperative area with do-not-resuscitate (DNR) orders. AORN, ASPAN, ACS and ASA support having a full discussion regarding DNR with patient/ proxy preoperatively.
• Data collection revealed inconsistencies in defining and documenting a patient’s DNR status.
• Patient and family concerns affirmed the need for offering limited/goal directed DNR.
• Staff and MD surveys revealed results consistent with automatic suspension of DNRs.
Background Process Improvement
Staff nurse led multidisciplinary team to address:• Who documents discussion with patient• How long DNR should be suspended• Limited scope DNR• Create new order set• Revise DNR policy• Provide staff and physician education
Beliefs regarding DNRs
Results
Perioperative/ Procedural DNR Form
TO RESUSCITATE OR NOT TO RESUSCITATE: THAT IS THE PERIOPERATIVE QUESTION
Implications for Perioperative Nursing
• Clearly defined perioperative DNR policies for the
procedural and surgical areas• Improve patient safety and care, and increase patient, family and staff satisfaction
27
Paper versus Digital Portfolio?
28
Selected Review of Digital Portfolio Literature
Lewis & Baker (2007) conclusions and student reflections of E-Portfolio:– Changed their technology comfort level & acquired new
skills and abilities– “easy to update…much more user friendly…”– Encourages creative, lively media that displays
professional’s best work– Creative and efficient way to organize, summarize and
share information– Promotes learning of new technology
Pincombe, McKellar, Weise, Grinter and Beresford (2010) evaluation of ePortfolio to paper-based portfolio:– Paper-based: Confusing at first, Cumbersome, Created
Anxiety– ePorfolio: Simple, Streamline, Safe– “The way of the future”
29
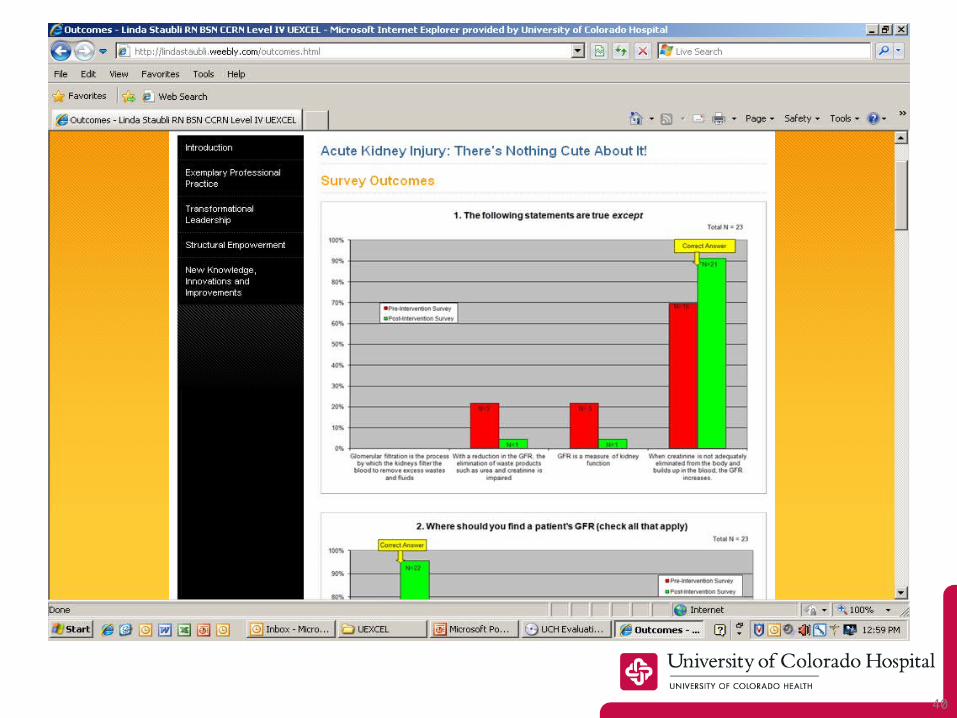
Our Digital Portfolio Platform
• Web product, accessible to general public
• Multiple media features • Allows the individual to
• access drag & drop website editor• Password protect• Increased size uploaded files• Embed documents• Have Fast online support
• Example of digital portfolio

30

31
32
33
34
35
36
37
38
39
40
Introduced Digital Portfolios to Level III & Level IV Applicants
• Demonstrated this type of portfolio submission to UEXCEL Board– Board member trialed it
• Held workshops on this new option for Level III & Level IV applicants
• Surveyed attendees to gain feedback on this new innovation
Digital Workshop Survey Results
• 5 digital portfolio sessions held– 10 RNs attended
• 11 RNs credentialed using a digital portfolio
• 100% of respondents– Found workshop helpful– Would recommend digital
portfolio– 80% found digital platform
easy to use• Additional comments from
participants – “love it!”– “Very happy that someone
helped bring this idea to UCH”
4343
PODCAST: PORTFOLIO REVIEW
44
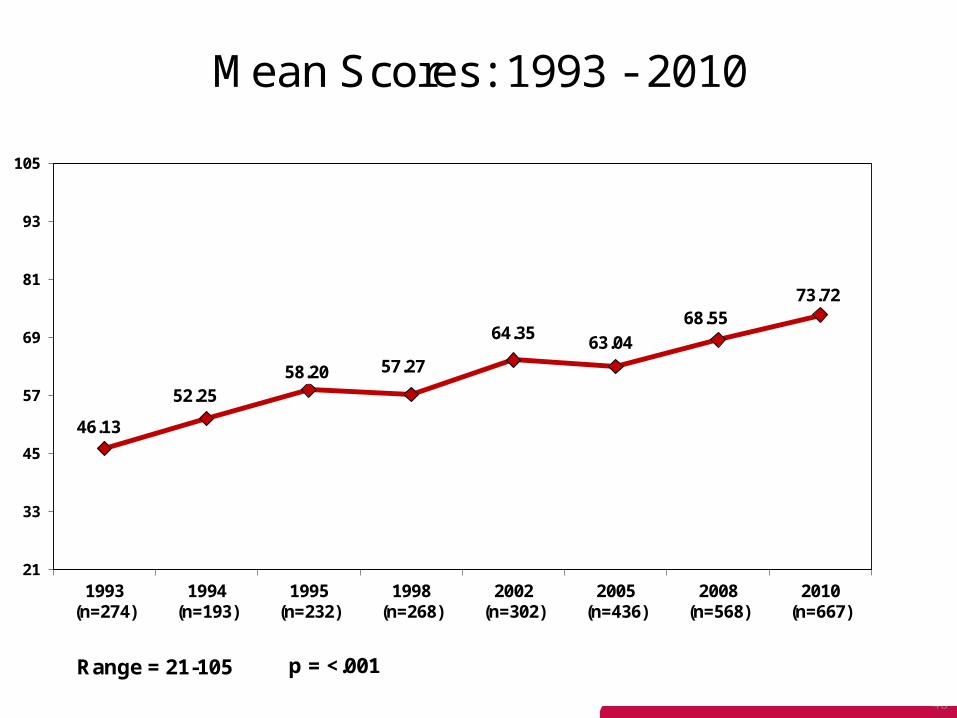
UEXCEL Longitudinal Evaluation
45
Background• Survey of RN UEXCEL practice program
1993 to 2010; next survey 2013• Each 2-3 year evaluation cycle results in
changes based on Clinical RN UEXCEL member feedback– Modification from 5 levels to 4– Deleting out of date survey questions over time– Updating practice standards with each cycle– Improved Board representation, visibility, based
on RN qualitative feedback – Developed mentoring program, structured prep
courses
46
Survey Tool Characteristics
• Valid and reliable survey instrument over time– Alpha coefficient = .96 /1.00
• Instrument originally from an unpublished 1980’s dissertation; questions significantly changed, 1-5 rating scale format adopted
• 21 item scale with 2 open ended qualitative questions
• All items analyzed at a .05 level of significance

47
Demographic Overview
• Total RN respondents over 17 year period = 3,101
• Comparing demographics between 1993 and 2010, RN respondents are now like ‘bookends’– Significant ↑ of RNs working 5 years or less
(58%), compared to RNs working > than 15 years (31%)
– Increase of 25% male RNs since 1993– Increase of graduate nurses from 23 hired in
1993 to 89 hired in 2011-2012– UEXCEL RN level numbers:
• Level I = 89 Level II = 1,200 Level III = 215 Level IV = 31
48
46.13
52.2558.20 57.27
64.3563.04
68.5573.72
21
33
45
57
69
81
93
105
1993 (n=274)
1994 (n=193)
1995 (n=232)
1998 (n=268)
2002 (n=302)
2005 (n=436)
2008 (n=568)
2010 (n=667)
Mean Scores: 1993 - 2010
Range = 21-105 p = <.001
Longitudinal Issues Improved to Increase RN Program Satisfaction• Perceived performance
appraisals not fair or equitable
• UEXCEL may not really recognize different levels of practice
• UEXCEL does not really recognize my nursing expertise
• UEXCEL standards are too global; don’t reflect my practice
• HR sessions for Permanent Charge RNs who assist managers w/ appraisals; managers meet w/ team to review process prior to appraisals
– Rating ↑ 3.00 to 3.48 (p=.003)
• UEXCEL Board members assumed ↑visibility & engagement re role as unit rep. Rating ↑ 2.93 to 3. 34 (p=<.001)
• UEXCEL advancement celebration publicized in Hospital newsletter/ Passport to Career
– Rating ↑ 2.99 to 3.41 (p=< .001)
• Small group work with ambulatory/Periop for guidance on customizing forms
– Rating ↑ 2.93 to 3.29 (p=<.001)
50
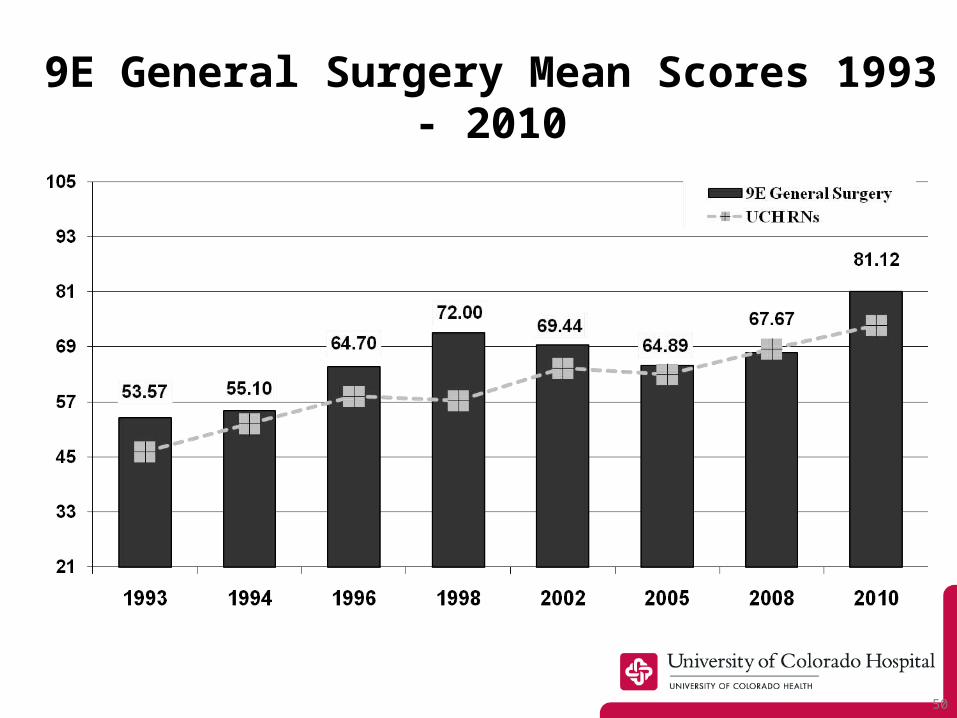
9E General Surgery Mean Scores 1993 - 2010

51
Neurosurgical ICU Mean Scores 2005 - 2010
Professional Practice Programs Empower and Engage Clinical RNs!
• UEXCEL reflects long standing commitment to shape the nursing professional workforce:– Change slow in first decade, accelerated with
new generation of clinical nurses: well-educated, career oriented, embrace the values of hospital, profession
• Program linked to performance, certification & rewards based on engagement, expertise, evidence-based practice & research
• Our commitment results in high nurse job satisfaction, exceptional productivity and an excellent retention rate
53
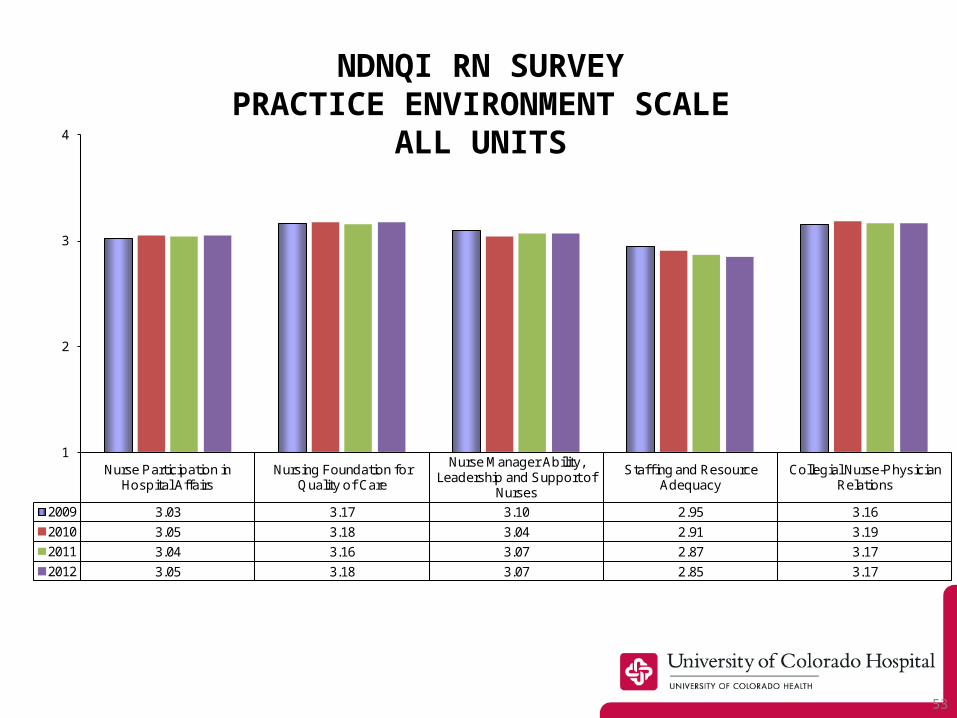
Nurse Participation in Hospital Affairs
Nursing Foundation for Quality of Care
Nurse Manager Ability, Leadership and Support of
Nurses
Staf f ing and Resource Adequacy
Collegial Nurse-Physician Relations
2009 3.03 3.17 3.10 2.95 3.16
2010 3.05 3.18 3.04 2.91 3.19
2011 3.04 3.16 3.07 2.87 3.17
2012 3.05 3.18 3.07 2.85 3.17
1
2
3
4
NDNQI RN SURVEYPRACTICE ENVIRONMENT
SCALEALL UNITS

54
55
REFERENCES
Cummings, G., MacGregor, T., Davey, M., Lee, H., Wong, C., Lo, E., Muise, M., Stafford, E. (2010). Leadership styles and outcome patterns for the nursing workforce and work environment: A systemic review. International Journal of Nursing Studies, 47(3), 363-385.Bogossian, F.E., and Kellett, S. E.M., (2010) Barriers to electronic portfolio access in the clinical setting. Nurse Education Today, 30, 768-772.Brooks B, Olsen S, Rieger-Kligys P, Mooney, L. (1995). Peer review: An approach to performance evaluation in a professional practice model. Critical Care Nursing Quarterly, 18(3), 36-47Driessen, E.W., Muijtjens, A.M.M., Tartwijk, J.V., & Van Der Bleuten, C.P.M., (2007) Web- or paper-based portfolios: is there a difference? Medical Education, Vol 41, 1067-1073.Johns, C. (2004). Becoming a reflective practitioner. Oxford, England: Blackwell Publishing.Kramer, M., Maguire, P., Brewer, B. (2011). Clinical nurses in Magnet hospitals confirm productive, healthy unit work environments. Journal of Nursing Management, 19(1), 1-5.Lammintakanen, J., Sarnto, K., Kivinen, T., & Kinnunen, J., (2002). The digital portfolio: a tool for human resource management in health care? Journal of Nursing Management, Vol 10, 321-
328.Luzinski, C. (2011). The Magnet model: An infrastructure for excellence. Journal of Nursing Administration; 41(11), 441-442.Lewis, K.O., and Baker, R.C., (2007). The Development of an Electronic Educational Portfolio: An Outline for Medical Education Professionals. Teaching and Learning in Medicine, 19(2), 139- 147.
REFERENCES
McKenzie, J.F., Cleary, M.J., McKenzie, B.L. & Stephen, C.E., (2002). E-Portfolios: Their Creation and Use by Pre-service Health Educator. The International Electronic Journal of Health Education, Vol 4, 79-83.Murphy, M., Hinch, B., Llewellyn, J., Dillon, P.J., & Carlson, E. (2011). Promoting professional nursing practice: Linking a professional practice model to performance expectations. Nurs Clin N Am. , 46: 67-79.Pierson MA, Liggett C, Moore KS. (2010). Twenty years of experience with a clinical ladder: A tool for professional growth, evidence-based practice, recruitment and retention. J Contin Edu Nurs, 41(1): 33-40.Pincombe, J., McKellar, L., Weise, M., Grinter, E., & Beresford, G., (2010). ePortfolio in Midwifery Practice: “The Way of the Future”. Women and Birth, 23, 94-102.Richards, J.A., (2001). Nursing in a Digital Age. Dermatology Nursing, Vol. 13, No. 5, 365-370.Watts M.D., (2010). Certification and clinical ladder as the impetus for professional development. Critical Care Nurse Q, 33(1):52-59.Winslow, S.,A., Fickley, S., Knight, D., Richards, K., Rosson, J., Rumbley, N., (2011). Journal for Nurses in Staff Development, 27(1): 13-17.
57
CONTACT INFORMATION
Carolyn Dietrich [email protected]
Mary Krugman [email protected]
Amanda Nenaber [email protected]
Michelle Rudolph [email protected]





























