Embed Size (px)
Citation preview

CLINICAL SUPPORT SERVICESMANAGING IABP THERAPY - CS300™ IABP

CS300 IABP COLOR DISPLAY AND kEYPAD CONTROLS

1 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
MANAGING INTRA-AORTIC BALLOON THERAPY
Course Description:
This six hour program is designed for the experienced
healthcare professional directly involved with the care of
the patient requiring intra-aortic balloon pump therapy.
Participants should have experience with hemodynamic
monitoring and 6 months critical care experience.
Previous experience with intra-aortic balloon pump
therapy is preferred.
This program is comprised of 3 modules consisting
of theoretical, technical, and clinical considerations
for a patient requiring IABP therapy. The theoretical
module will briefly review cardiac physiology and the
theory of intra-aortic balloon pumping. The technical
module will discuss percutaneous insertion and removal
of the intra-aortic-balloon catheter followed by a
detailed explanation of the MAQUET IABP, highlighting
troubleshooting in the clinical setting. Case studies
will be utilized to further reinforce troubleshooting
techniques. The clinical module provides a discussion
of clinical considerations for patients requiring IABP
therapy. A skills workshop utilizing the system trainer
and Abbreviated Operator’s Guide will be provided.
Behavioral Objectives:
At the conclusion of this program, the participants will
be able to:n Define the two physiological effects achieved by
the mechanics of inflation and deflation of the IAB
as it relates to the cardiac cycle illustrated by an
augmented arterial pressure waveform.n Identify four indications and three contraindications
for IABP therapy.n Identify the potential complications associated with
IABP therapy.n Demonstrate the set up, operation, and
troubleshooting of the MAQUET IABP utilizing the
system trainer for practice and the abbreviated
operators guide for reference.

| 2 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
COURSE SCHEDULE
8:00-8:10
Introduction
Review Program
8:10-9:30
MODULE I - Theoretical Aspects
Review Cardiac Mechanics
Measurement of Cardiac Performance
Left Ventricular Failure
Theory of IABP
Factors Affecting Diastolic Augmentation/Timing Errors
Indications/Contraindications
9:30-9:40
Break
9:45-10:45
MODULE II IAB -
Catheter and Technical Introduction to IABP
IAB Catheter Insertion
Technical Features of the IABP
10:45 – 11:00
Break
11:00 -12:00
Troubleshooting Alarm and Advisory Messages
Hands On
12:00 – 12:30
Lunch
12:30 – 1:15
Additional Hands on
1:15 – 1:45
MODULE III - Clinical Considerations
Side Effects/Potential Complications
Care Management/Case Studies
1:45 – 2:00
Open Discussion
Program Evaluation

3 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
| 3 | | CLINICAL SUPPORT SERVICES | MANAgINg INTRA-AORTIC BALLOON PUMP ThERAPy - CS300
MODULE I THEORETICAL ASPECTS Of IABP

| 4 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
ATRIALSYSTOLE
VENTRICULARFILLING
ISOVOLUMETRICRELAXATION
ISOVOLUMETRICCONTRACTION
VENTRICULAREJECTION PHASE
I. REVIEw PHYSIOLOGY Of CARDIAC MECHANICS
A. CARDIAC CYCLE
1. Atrial Systole
2. Isovolumetric Contraction
3. Ventricular Ejection
a. Slow Ejection
b. Rapid Ejection
c. Slow Ejection
4. Isovolumetric Relaxation
5. Ventricular Filling
a. Rapid Filling
b. Slow Filling

5 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
ATRIALSYSTOLE
SEMI-LUNARVALVE OPENS100
120
80
60
40
10
0
ATRIALSYSTOLE
VENTRICULARSYSTOLE
DIASTOLE
AV VALVECLOSES
AV VALVEOPENS
SEMI-LUNARVALVE CLOSES
VENTRICULARPRESSURE
APPX. TIME (sec.) 0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8
ELECTROCARDIOGRAM
PR
ES
SU
RE
(m
mH
g)
ARTERIALPRESSURE
VENTRICULAREJECTION PHASE
VENTRICULARFILLING
ISOVOLUMETRICCONTRACTION
ISOVOLUMETRICRELAXATION
P
R
T
Q S
B. PRESSURE wAVES
1. Ventricular Waveform
a. Pressure
b. Volume
2. Arterial
a. Radial/Brachial
b. Aortic

| 6 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
B. PRESSURE wAVES (continued)
NORMAL ARTERIAL wAVEfORM
SYSTOLIC PRESSURE
RAPID VENTRICULAREJECTION PHASE(75% SV Ejected)
NORMAL ARTERIAL WAVEFORM
AORTIC VALVE OPENS AORTIC END DIASTOLIC PRESSURE
DICROTIC NOTCH ■ Aortic Valve Closes ■ Diastole Begins
RUN-OFF PHASE(25% SV Ejected)
I. REVIEw PHYSIOLOGY Of CARDIAC MECHANICS (continued)

7 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
160
100 200 300 400
120
ST
RO
KE
VO
LU
ME
– m
l
END – DIASTOLIC VOLUME
CARDIACFAILURE
CARDIACRESERVE
80
40
C. MYOCARDIAL OXYGEN SUPPLY AND DEMAND
SUPPLY
1. Coronary artery anatomy
2. Diastolic pressure
3. Diastolic time
4. O2 extraction
a. Hemglobin
b. PaO2
D. fRANk-STARLING LAw Of HEART
Ventricular function curve. As the end-diastolic volume increases, so does the force of ventricular contraction. Thus the stroke volume becomes greater up to a critical point after which stroke volume decreases. [Cardiac failure]
DEMAND
1. Heart Rate
2. Afterload
3. Preload
4. Contractility
MVO2

| 8 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
LV fAILURE
Pumping Efficiency
Baroreceptors Activate
Activation of Renin-Angiotensin-Aldosterone-ADH
Pulmonary Edema
AnaerobicMetabolism
Lactic AcidProduction
Tissue Acidosis
Tissue Anoxia
DEATH
LV Volume & Pressure
HR
Release of Catecholamines
Afterload (SVR)
Na+ & H2O Reabsorption
O2 Demand
Preload (LVEDP)
Preload (LVEDP) Afterload (SVR)
Pulmonary Artery Pressure
HR
C.O.
C.O.
O2 Supply
Contractility
O2 Demand
Glomerular Filtration Pressure
Oxygenation
BP
C.O.
VASOCONSTRICTION
HYPERVOLEMIA
TISSUE HYPOXIA
Supply
Demand
Supply
Demand
MVO2
MVO2
Supply
Demand
MVO2
I. REVIEw PHYSIOLOGY Of CARDIAC MECHANICS (continued)

9 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
II. THEORY Of IABP THERAPY
A. COUNTERPULSATION
1. Balloon Structure and Position
2. Increased Coronary Perfusion
a. Inflation
b. Augmentation of Diastolic Pressure
3. Decreased Left Ventricular Workload
a. Deflation
b. Afterload Reduction
4. Physiological Pressure Wave Changes
a. Dicrotic Notch
b. Diastole: Augmentation
c. Decreased End-Diastolic Pressure
d. Systole: Decreased Assisted Systolic Pressure
Inflate Deflate
| 10 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
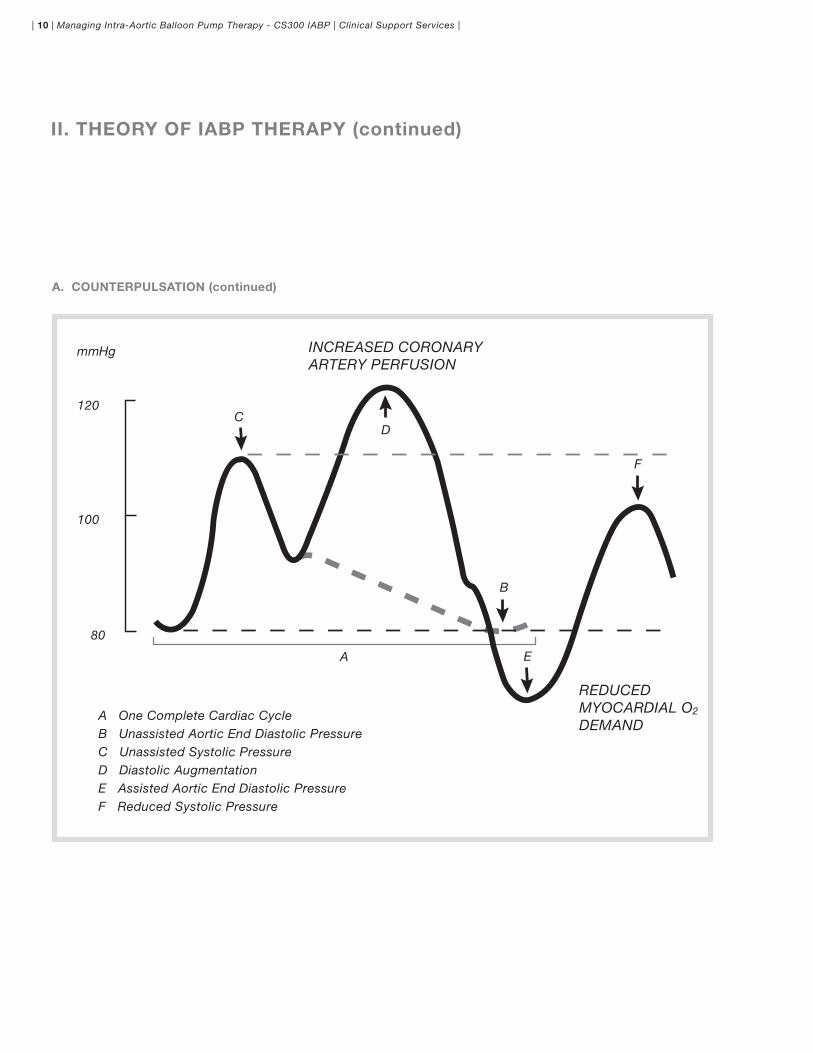
A. COUNTERPULSATION (continued)
mmHg
120
100
CD
A
A One Complete Cardiac CycleB Unassisted Aortic End Diastolic PressureC Unassisted Systolic PressureD Diastolic AugmentationE Assisted Aortic End Diastolic PressureF Reduced Systolic Pressure
B
E
F
80
REDUCEDMYOCARDIAL O2
DEMAND
INCREASED CORONARYARTERY PERFUSION
II. THEORY Of IABP THERAPY (continued)

11 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
ARTERIAL wAVEfORM VARIATIONS DURING IABP THERAPY
1:1 IABP fREQUENCY
1:2 IABP fREQUENCY
1:3 IABP fREQUENCY
DIASTOLIC AUGMENTATION
ASSISTED AORTIC ENDDIASTOLIC PRESSURE
ASSISTED SYSTOLEASSISTED SYSTOLE
mmHg
120
140
100
80
DIASTOLIC AUGMENTATION
ASSISTED AORTIC ENDDIASTOLIC PRESSURE
ASSISTED SYSTOLE
UNASSISTED SYSTOLE
mmHg
120
140
100
80 UNASSISTED AORTIC ENDDIASTOLIC PRESSURE
DIASTOLIC AUGMENTATION
UNASSISTED AORTIC END DIASTOLIC PRESSURE
ASSISTED AORTIC END DIASTOLIC PRESSURE
ASSISTED SYSTOLE
UNASSISTED SYSTOLE
mmHg
100
120
60
80
UNASSISTED SYSTOLE

| 12 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
II. THEORY Of IABP THERAPY (continued)
B. EffECTS Of IABP
1. Primary
a. Supply
b. Demand
2. Secondary
a. CO/CI
b. HR
c. PAD-PCWP
d. SVR
e. B/P-SYSTOLIC
DIASTOLIC
MAP
DIASTOLIC AUGMENTATION
3. Systemic
a. Neuro
b. Renal
c. Vascular
d. Respiratory

13 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
C. fACTORS AffECTING DIASTOLIC AUGMENTATION
1. Patient Hemodynamics
a. Heart Rate
b. Stroke Volume
c. Mean Arterial Pressure
d. System Vascular Resistance
2. Intra-Aortic Balloon
a. IAB in Sheath
b. IAB Not Unfolded
c. IAB Position
d. Kink in IAB Catheter
e. IAB Leak
f. Low Helium Concentration
3. IABP
a. Timing
b. Position of IAB Augmentation Control

| 14 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
II. THEORY Of IABP THERAPY (continued)
D. TIMING ERRORS
1. Early Inflation
Inflation of the IAB prior to aortic valve closure
waveform Characteristics:
n Inflation of IAB prior to dicrotic notch
n Diastolic augmentation encroaches onto
systole (may be unable to distinguish)
Physiologic Effects:
n Potential premature closure of aortic valve
n Potential increase in LVEDV and LVEDP or
PCWP
n Increased left ventricular wall stress or afterload
n Aortic Regurgitation
n Increased MVO2 demand
2. Late Inflation
Inflation of the IAB markedly after closure
of the aortic valve
waveform Characteristics:
n Inflation of the IAB after the dicrotic notch
n Absence of sharp V
n Sub-optimal diastolic augmentation
Physiologic Effects:
n Sub-optimal coronary artery perfusion
UNASSISTEDSYSTOLE
DIASTOLICAUGMENTATION
ASSISTEDSYSTOLE
ASSISTED AORTICEND DIASTOLIC
PRESSURE
UNASSISTEDSYSTOLE DIASTOLIC
AUGMENTATIONASSISTEDSYSTOLE
DICROTICNOTCH
ASSISTED AORTICEND DIASTOLIC
PRESSURE
EARLY INfLATION
LATE INfLATION
15 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
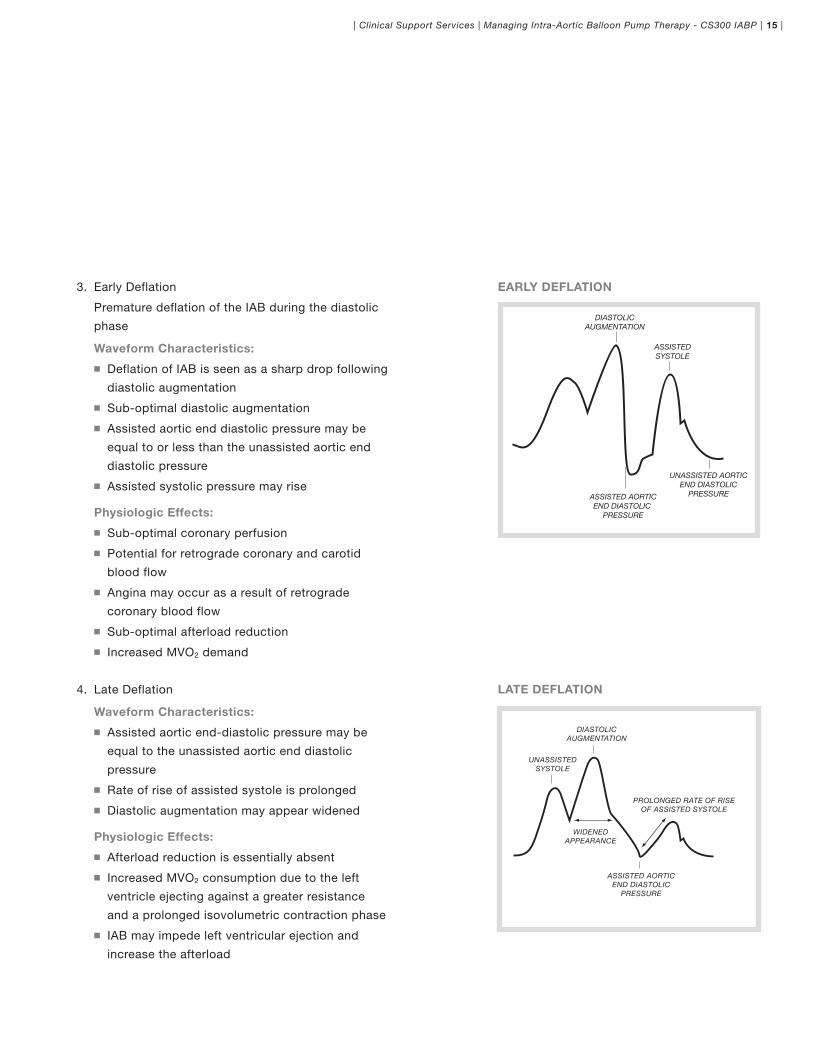
EARLY DEfLATION
LATE DEfLATION
3. Early Deflation
Premature deflation of the IAB during the diastolic
phase
waveform Characteristics:
n Deflation of IAB is seen as a sharp drop following
diastolic augmentation
n Sub-optimal diastolic augmentation
n Assisted aortic end diastolic pressure may be
equal to or less than the unassisted aortic end
diastolic pressure
n Assisted systolic pressure may rise
Physiologic Effects:
n Sub-optimal coronary perfusion
n Potential for retrograde coronary and carotid
blood flow
n Angina may occur as a result of retrograde
coronary blood flow
n Sub-optimal afterload reduction
n Increased MVO2 demand
4. Late Deflation
waveform Characteristics:
n Assisted aortic end-diastolic pressure may be
equal to the unassisted aortic end diastolic
pressure
n Rate of rise of assisted systole is prolonged
n Diastolic augmentation may appear widened
Physiologic Effects:
n Afterload reduction is essentially absent
n Increased MVO2 consumption due to the left
ventricle ejecting against a greater resistance
and a prolonged isovolumetric contraction phase
n IAB may impede left ventricular ejection and
increase the afterload
DIASTOLICAUGMENTATION
ASSISTEDSYSTOLE
ASSISTED AORTICEND DIASTOLIC
PRESSURE
UNASSISTED AORTICEND DIASTOLIC
PRESSURE
PROLONGED RATE OF RISEOF ASSISTED SYSTOLE
DIASTOLICAUGMENTATION
UNASSISTEDSYSTOLE
WIDENEDAPPEARANCE
ASSISTED AORTICEND DIASTOLIC
PRESSURE

| 16 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
II. THEORY Of IABP THERAPY (continued)
E. INDICATIONS
1. Refractory Unstable Angina
2. Impending Infarction
3. Acute MI
4. Refractory Ventricular Failure
5. Complications of Acute MI [i.e. acute MR or
VSD, or papillary muscle rupture]
6. Cardiogenic Shock
7. Support for diagnostic, percutaneous
revascularization, and interventional procedures
8. Ischemia related intractable ventricular
arrhythmias
9. Septic Shock
10. Intraoperative pulsatile flow generation
11. Weaning from bypass
12. Cardiac support for non-cardiac surgery
13. Prophylactic support in preparation for
cardiac surgery
14. Post surgical myocardial dysfunction/low
cardiac output syndrome
15. Myocardial contusion
16. Mechanical bridge to other assist devices
17. Cardiac support following correction of
anatomical defects
f. CONTRAINDICATIONS
1. Severe aortic insufficiency
2. Abdominal or aortic aneurysm
3. Severe calcific aorta-iliac disease or
peripheral vascular disease
4. Sheathless insertion with severe obesity,
scarring of the groin, or other
contraindications to percutaneous insertion
Please Refer to the Instructions for Use Prior to Insertion of the IAB

MODULE II TECHNICAL ASPECTS

| 18 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
I. INTRA-AORTIC BALLOON CATHETER
A. DESIGNED fOR SHEATHLESS OR SHEATHED INSERTION
Fiberoptic IAB Catheter
Conventional IAB Catheter

19 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
Infusion Bag 500ml Sterile IV Solution Maintained at300 mmHg
Arterial Recipient Set
To Arterial Pressure Input on IAB Pump
Continuous FlushingDevice
Three-Way Stopcock
Maximum 8ft(2.5 Meters)Pressure Tubing
To Luer Connection on Catheter Extender
Stopcock
Transducer
PRESSURE MONITORING THROUGH IAB CATHETER
PRECAUTIONSn Use a standard flushing apparatus for arterial
pressure monitoring with the inner lumen. Careful
technique should be used in the set up and flushing
of the arterial pressure monitoring apparatus to
minimize the risk of an embolus entering the aorta
where it could potentially enter the carotid or
coronary arteries.n Aspirate and discard a 3cc volume of blood from the
inner lumen prior to attaching a flushing apparatus to
the female luer hub.n Ensure that all air bubbles are removed from the
inner lumen and flushing apparatus. In addition, tap
the Y-fitting to remove all air bubbles.n Prior to fast flushing, stop IAB pumping to reduce
the risk of an embolus entering the aortic arch should
an embolus be ejected from the inner lumen.n For optimal signal quality the inner lumen should not
be used for blood sampling.n Always aspirate 3cc initially if the inner lumen aortic
pressure signal becomes damped. If you meet
resistance during aspiration, consider the inner
lumen to be occluded. Discontinue the use of the
inner lumen by placing a luer cap on the female luer
hub.n The use of in-line filters or other devices can
potentially alter the appearance of the arterial
pressure waveform.n Do not over-tighten connections.
B. CLINICAL CONSIDERATIONS fOR CENTRAL
AORTIC PRESSURE MONITORING
PRECAUTION n For optimal signal quality, use no more than 8 feet
(2.5 meters) maximum of pressure tubing between
the transducer and female luer hub of the Y-fitting.
When monitoring pressure through the inner lumen,
use a standard arterial pressure monitoring apparatus
connected to a three-way stopcock. Connect the
three-way stopcock to the female luer hub of the
inner lumen. A 3cc/hour continuous flow through the
inner lumen is recommended. The anticoagulation
dosage should be in accordance with standard
hospital practice for arterial pressure lines and may
be modified, on physician discretion, for patients
receiving anticoagulation therapy. Per hospital policy,
a fast forward flush may be performed hourly to help
maintain patency of the inner lumen.

| 20 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
RECOMMENDATIONS fOR ACHIEVING OPTIMAL
PRESSURE SIGNAL QUALITY
1. Use no more than 8ft (2.5m) of a low compliance
pressure tubing such as that supplied by MAQUET
in the IAB Insertion Kit between the transducer
and Y-fitting of the catheter.
2. Once the catheter is in place, aspirate and
discard 3cc of blood from the inner lumen and
then immediately perform a manual flush using
a syringe filled with 3cc to 5cc of flush solution.
This will minimize the chances of stagnant blood
clotting in the inner lumen.
3. Apply only gentle force to the syringe when
aspirating the inner lumen.
4. Do not use a R.O.S.E. (Resonance Over Shoot
Eliminator) or other damping device.
5. Remove air from flush bag prior to pressurizing.
6. Prime the pressure set-up using gravity flush.
7. Maintain 300 mmHg of pressure on the flush
solution and elevate it above the transducer.
8. Whenever the inner lumen of the IAB becomes
filled with blood (such as after aspiration), the
flush valve should be activated for a minimum of
15 seconds in addition to the time it takes to clear
the pressure tubing of blood.
9. Ensure that all air bubbles are removed from the
inner lumen and flushing apparatus.
10. Use room temperature flush solution.
B. CLINICAL CONSIDERATIONS fOR CENTRAL
AORTIC PRESSURE MONITORING (continued)

21 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
II. TECHNICAL COMPONENTS Of THE CS300 IABP

| 22 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
A. REAR PANEL
1. Fiberoptic Module
a. IAB Sensor Input
b. Vent Key
c. To bedside monitor
2. Safety Disk/Condensate Removal System
a. DC Input
b. IAB Fill Port
c. Drain Port
3. Helium Supply
a. Pressure Gauge
b. Manual Fill Port
4. Patient Connections
a. ECG
b. Pressure
c. Monitor Input
n ECG
n Pressure
d. ECG/Pressure Output
5. Data Communications Outputs
a. RS-232
b. Phone Line
c. Diagnostic Output
6. Power Cord/Mains
7. System Timer
II. TECHNICAL COMPONENTS Of THE CS300 IABP (continued)

23 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
1. Alarm and Advisory Messages
2. ECG
a. Lead
b. Gain
3. Pressure Source
4. IAB Fill Mode
5. Slow Gas Alarm Status
6. Operation Mode
7. IAB Status Indicator
8. Trigger
9. Heart Rate Display
10. Pressure Display
11. Augmentation Alarm
12. Battery Indicator
13. Helium Indicator
B. MONITOR CS300
| 24 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
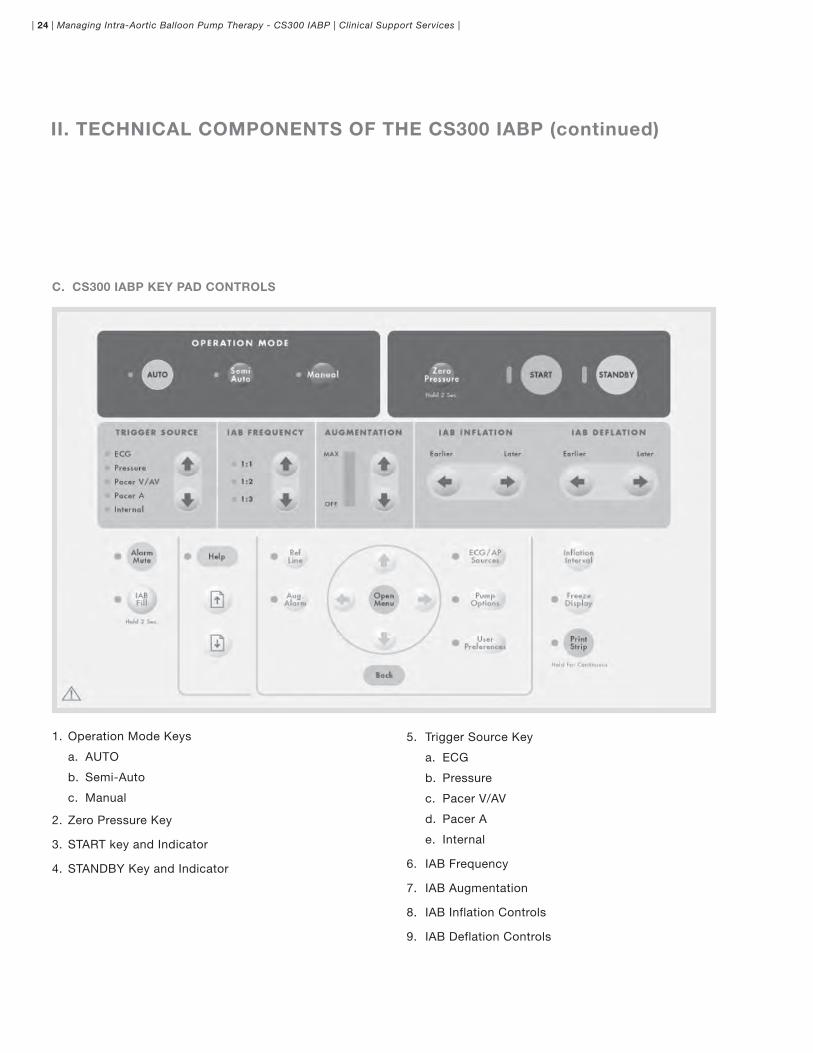
C. CS300 IABP kEY PAD CONTROLS
5. Trigger Source Key
a. ECG
b. Pressure
c. Pacer V/AV
d. Pacer A
e. Internal
6. IAB Frequency
7. IAB Augmentation
8. IAB Inflation Controls
9. IAB Deflation Controls
1. Operation Mode Keys
a. AUTO
b. Semi-Auto
c. Manual
2. Zero Pressure Key
3. START key and Indicator
4. STANDBY Key and Indicator
II. TECHNICAL COMPONENTS Of THE CS300 IABP (continued)

25 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
1. Alarm Mute Key
2. IAB Fill Key
3. Help Key Indicator
4. Menu Guide
a. Ref Line
b. Aug. Alarm
c. ECG/AP Sources
d. Pump Options
e. User Preferences
5. Inflation Interval Key
6. Freeze Display Key
7. Print Strip Key
D. CS300 kEY PAD CONTROL PANEL

| 26 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
1. ECG
E. RECORDER
2. Pressure
3. Balloon Pressure Waveform
II. TECHNICAL COMPONENTS Of THE CS300 IABP (continued)

27 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
f. SYSTEM BATTERY
1. Charge Status
2. Portable Operation
G. DOPPLER STORAGE

| 28 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
The inflation marker shows the period of inflation. Vertical timing marks located
below the arterial waveform are also available to aid with initial timing.
INfLATION MARkERS
A unique automatic timing algorithm allows effective balloon pumping even during atrial fibrillation.
Press the Inflation Interval key to observe the period of inflation while pumping. Vertical markers
located below the arterial waveform and the highlighted portion indicate the period of balloon inflation.
II. TECHNICAL COMPONENTS Of THE CS300 IABP (continued)

29 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
III. TROUBLESHOOTING
A. HIGH PRIORITY ALARMS
All Modes
Augmentation Below Limit Set*
No Trigger
IAB Disconnected
Check IAB Catheter
Leak in IAB Circuit
Rapid Gas Loss
Blood Detected
Autofill Failure
Autofill Failure – No Helium
High Pressure Drive
Low Vacuum
AUTO Operation Mode
Poor Signals Persist
Semi Auto or Manual Mode
ECG Detected*
No Pressure Trigger
Trigger Interference
Check Pacer Timing
Autofill Required
Other:
Safety Disk Test Fails
B. MEDIUM PRIORITY ALARMS
All Modes
IAB Optical Sensor Failure
Low Battery
Low Battery
AUTO Operation Mode
Poor Signal Quality
No Pressure Source Available
C. LOw PRIORITY ALARM
AUTO Operation Mode
Unable to Update Timing
D. TECHNICAL ALARMS
Electrical Test Fails Code #
System Failure
No Patient Status Available
E. INfORMATIONAL MESSAGES
All Modes
A.P. Optical Sensing Module Failure
Unable to Calibrate IAB Optical Sensor
IAB Optical Sensor Calibration Expired
No Trigger
Prolonged Time In Standby
Autofilling
Auto Zeroing
Autofilling and Zeroing
Function Not Available
Low Helium
Battery in Use [EXT]
Battery In Use
System Test OK
System Trainer
Maintenance Required Code #
Slow Gas Loss Alarm is OFF
Leak In IAB Circuit – Overridden
Blood Detected – Overridden
AUTO Operation Mode
Function Unavailable in Auto Operation Mode
* Pumping NOT suspended

| 30 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
E. INfORMATIONAL MESSAGES (continued)
AUTO or SemiAuto Operation Mode
Auto R-Wave Deflate
R-Wave Deflate
SemiAuto
Irregular Pressure Trigger
SemiAuto or Manual:
Verify Proper Timing
IAB Not Filled
Manual Fill IAB
Auto Operation Mode is Disabled
Gas Loss and Catheter Alarms Disabled
Manual Mode
Manual Timing Selected – See Help
Other
Install Safety Disk
Unplug Disk Outlet
Plug Disk Outlet
Leak Testing Safety Disk
f. PATIENT CONDITIONS
1. Atrial Fibrillation
2. Ectopics
3. Cardiac Arrest
4. Cardioversion/Defibrillation
G. CHANGING HELIUM TANk
H. SAfETY DISk LEAk TEST
I. MANUAL fILL
J. MANUAL TIMING
III. TROUBLESHOOTING (continued)

31 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
IV. NORMAL BALLOON PRESSURE wAVEfORM
PEAK INFLATION(POSITIVE OVERSHOOT)
PLATEAU (FULL INFLATION OF IAB)
IABDEFLATION
IABINFLATION
ZERO BASELINE RETURN TO ZERO BASELINE
PEAK DEFLATION(NEGATIVE OVERSHOOT)

| 32 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
VARIATIONS IN BALLOON PRESSURE wAVEfORMS
1. HEART RATE
BRADYCARDIAIncreased duration of plateau due to longer diastolic phase
TACHYCARDIADecreased duration of plateau due to shortened diastolic phase
2. RHYTHM
Varying R-R intervals result in irregular plateau durations
3. BLOOD PRESSURE
HYPERTENSIONIncreased height or amplitude of the waveform
HYPOTENSIONDecreased height oramplitude of the waveform

33 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
4. GAS LOSS
Leak in the closed system causing the balloon pressure waveform to fall below zero baseline. This may be due to a loose connection, a leak in the IAB catheter, H2O condensation in the external tubing, or a patient who is tachycardiac and febrile which causes increased gas diffusion through the IAB membrane.
5. CATHETER kINk
Rounded balloon pressure waveform, loss of plateau resulting from a kink or obstruction of shuttle gas. This may be caused by a kink in the catheter tubing, improper IAB catheter position, sheath not being pulled back to allow inflation of the IAB, the IAB is too large for the aorta, the IAB is not fully unwrapped, or H2O condensation in the external tubing.
6. SUSTAINED INfLATION
Theoretical possibility if the IAB remains inflated longer than 2 seconds. The intra-aortic balloon pump will activate the System Failure alarm and deflate the IAB.


MAQUET IABP PERfORMANCE CHECkLIST – CS300
Name: Date:
Hospital Policy and Procedure Review: Date: Initials:
Basic Intra-Aortic Balloon Pump Course: Date: Initials:
Technical Seminar/Advanced Troubleshooting: Date(s): / Initials:
Challenge Exam (if applicable): Date: Score: (P/f)
DIRECTIONS fOR INSTRUCTORPlace your initials next to the skills the participant is able to perform. Leave blank the skills requiring repeat performance. Clarify learning needs if necessary in the comment section. The “Clinical Setting” column is an optional checklist for use by a preceptor or resource person for reinforcement of skills acquired on system trainer.
SkILLS SYSTEM TRAINER CLINICAL SETTING
INITIAL SET UP
Establish Power: Main power switch & IABP On/Off switch ON
Open helium tank and verify helium pressure
Establish ECG and Pressure connections
If Using a Sensor IAB:n Ensure the IAB Sensor Cable is connected to the sensor module and clipped to helium extender tubing
If Using a Conventional IAB/Transducer:n Open transducer to airn Press zero pressure key for 2 secondsn Close transducer
CONfIRM OPERATION MODE – AUTO
INITIATE PUMPING
Attach IAB catheter & appropriate extender to safety disk
Press the Start key
If Using a Sensor IAB:n Observe the “Autofilling & Zeroing” messagen Verify optimal diastolic augmentation
If Using a Conventional IAB/Transducer:n Observe the “Autofilling” messagen Verify optimal diastolic augmentation
VERIfY AUG. ALARM
Verify Aug. Alarm setting is approximately 10mmHg less than the patient’s augmented diastolic pressure
Adjust, if necessary by pressing Aug. Alarm key and using the up and down arrow keys, in the navigation circle, to change value displayed on the screen
ASSESS HEMODYNAMIC BENEfITS
Ensure optimal augmentation
Ensure optimal afterload reduction
If desired, IAB deflation can be fine tuned using the IAB deflation control
RECORD PRESSURES: ASSISTED & UNASSISTED
Press Print Strip key to record waveforms
Use Printer Menu in User Preferences to change printer settings
AUTO OPERATION MODE
Describe ECG and pressure source selection
Describe Trigger source selection
Describe automatic timing and Cardiosync 2 with R-Trac
SEMI-AUTO OPERATION MODE
Describe ECG and pressure source selection
Describe Trigger source selection
Describe automatic timing and Cardiosync 2 with R-Trac
PRESSURE SOURCE - Describes understanding of how pressure source is originated and calibrated
Fiberoptics
Conventional IAB/Transducer

TROUBLESHOOTING SYSTEM TRAINER CLINICAL SETTING
DEMONSTRATES ABILITY TO IDENTIfY VARIABLE TRIGGER SELECTION CRITERIA & APPROPRIATE USE Of EACH TRIGGER
Atrial Fibrillation
Demand Ventricular Pacemaker, Rate 60
AV sequential pacemaker, demand mode
Unobtainable ECG signal, regular rhythm, BP 100/50
Cardiac arrest with good chest compressions
Sinus Tachycardia
Sinus Rhythm with frequent PVC’S
Fixed rate AV sequential pacemaker
Atrial pacemaker - 100% paced
EVALUATES SITUATIONS THAT MAY CAUSE AN IAB CATHETER ALARM & DESCRIBES APPROPRIATE INTERVENTION
Kink in the catheter or tubing
Patient sitting straight up in bed
IAB has not exited the sheath
IDENTIfIES & RECOMMENDS APPROPRIATE ACTION fOR POTENTIAL LOSS Of HELIUM (“GAS LOSS”)
Blood in the IAB catheter shuttle gas tubing
IAB catheter disconnected from the console
DISCUSSES THE fOLLOwING ALARM & INfORMATIONAL MESSAGES
Poor Signal Quality
Poor Signals Persist
No Pressure Source Available
Unable to Update Timing
IAB Optical Sensor Failure
AP Optical Sensing Module Failure
Unable to Calibrate IAB Optical Sensor
IAB Optical Sensor Calibration Expired
SkILLS SYSTEM TRAINER CLINICAL SETTING
DISCUSSES THE HEMODYNAMIC RELATIONSHIP BETwEEN THE PATIENT & IABP THERAPY IN REGARD TO DIASTOLIC AUGMENTATION
Increased heart rate
Decrease in patient stroke volume
Ectopy
Increase in patient BP
Decreased SVR
DEMONSTRATES APPROPRIATE INTERVENTION fOR THE fOLLOwING ERRORS IN TIMING & VERBALIZES POTENTIAL CLINICAL IMPLICATIONS
Early inflation
Late inflation
Early deflation
Late deflation
PORTABLE OPERATION
Initiates and terminates portable operation
Identifies location of battery charge light
INTERfACE CABLES (If APPLICABLE)
Identifies location and use of ECG and/or pressure interface cables
Describes proper use of ECG interface cable in the presence of pacemakers
LOw LEVEL OUTPUT CABLE (If APPLICABLE)
Identifies location and use of low level output cable
Instructor Signature Instructor Initials
Instructor Signature Instructor Initials
Comments

MODULE IIICLINICAL CONSIDERATIONS

| 38 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
I. SIDE EffECTS AND COMPLICATIONS
ASSESSMENT PREVENTION TREATMENT OPTIONS
1. Limb Ischemia n Check distal pulses, color, temp. and capillary filling Q30 min. x 2 hrs, then Q2 hrs.
n Monitor differential toe temperatures.
n Use smallest sheath/catheter sizes indicated.
n Risk factors: female, diabetics, peripheral vascular diseases.
n Select limb with best pulse.
n Remove sheath and observe for bleeding.
n Subcutaneous Xylocaine injection for arterial spasm.
n Change insertion site to opposite limb.n Bypass graft femoral artery.
2. Excessive bleeding from insertion site
n Observation - anteriorly and posteriorly for blood or hematoma.
n Careful insertion technique.n Monitor anticoagulation
therapy.n Prevent catheter movement at
insertion site.
n Apply pressure. Assure distal flow.n Surgical repair.
3. Thrombocytopenia n Daily platelet count. n Avoid excessive heparin. n Replace platelets as needed.
4. Immobility of balloon catheter.
n The IAB should not remain inactive (i.e. not inflating and deflating) for more than 30 min. because of potential for thrombus formation.
n Observation of IAB status indicator movement.
n Observation of augmentation.
n Maintain adequate trigger.n Observe movement of IAB
Status indicator.n If unable to inflate the IAB with
the IABP, inflate and deflate the IAB by hand, using a syringe and stopcock once every 3-5 min.
n Notify the physician if the IAB is immobile for > 30 min.
5. Balloon leak n Observe tubing for blood with or without the presence of a blood detect, low augmentation, and/or gas loss or IAB catheter alarm.
n Do not remove the IAB from its tray until it is ready to be inserted.
n If blood is observed in the pneumatic tubing, disconnect the balloon from the IABP and notify the physician immediately.
6. Infection n Observation of insertion site.n Blood cultures for symptoms of
infection.
n Sterile technique during insertion and dressing changes as per infection control policy.
n Antibiotics.
7. Aortic Dissection n Assess for pain between shoulder blades.
n Daily hematocrit.n If suspected, aortogram may be
indicated.
n Insertion of IAB over guide wire with fluoroscopic control.
n Balloon removal.n Surgical repair.
8. Compartment syndrome may develop after IAB removed.
n Observation of limb for swelling and/or hardness.
n Measure calf girth.n Monitor interstitial pressure.
n Use the smallest catheter/ sheath appropriate.
n Maintain adequate colloid osmotic pressure.
n Fasciotomy if necessary.

39 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
II. wEANING AND REMOVAL
A. fREQUENCY
B. BALLOON AUGMENTATION

UN
IT N
UM
BE
R:
BE
DS
PA
CE
: N
AM
E:
DX
: P
HY
SIC
IAN
:
IAB
P:
Ref
ill I
AB
Q2
H/P
RN
Mai
nta
in o
pti
mal
au
gm
enta
tio
n a
nd
af
terl
oad
red
uct
ion
by
adju
stin
g t
imin
g P
RN
Zer
o t
ran
sdu
cer
PR
NN
ote
pla
cem
ent
IAB
on
ch
est
X-r
ayC
han
ge
Hel
ium
tan
k P
RN
Vit
al S
ign
s:M
on
ito
r Q
15
"- Q
30
" u
nti
l sta
ble
Incl
ud
ing
hem
od
ynam
ic p
aram
eter
sH
eart
Rat
eM
ean
Art
eria
l Pre
ssu
reC
VP
Pu
lmo
nar
y A
rter
y P
ress
ure
Pu
lmo
nar
y C
apill
ary
Wed
ge
Pre
ssu
reN
ote
an
d r
eco
rd:
Car
dia
c O
utp
ut/
Car
dia
c In
dex
S
yste
m V
ascu
lar
Res
ista
nce
No
tify
ph
ysic
ian
if:
Acc
epte
d h
emo
dyn
amic
par
amet
ers
dev
iate
Sig
nifi
can
t ch
ang
e A
BG
stu
die
s o
r ch
est
film
Lo
w u
rin
e o
utp
ut
< 3
0cc
/hr
Sig
ns
of
limb
isch
emia
IAB
P n
on
-fu
nct
ion
ing
> 1
5"
Ch
ang
e H
eliu
m t
ank
PR
N
Sp
ec
ial T
rea
tme
nt
Ne
ed
s:N
ote
an
d r
eco
rd q
ual
ity
of
ped
al p
uls
es Q
30
" af
ter
inse
rtio
n x
2H
, th
en Q
2H
Ch
ang
e IA
BP
dre
ssin
g -
PR
N w
ith
ste
rile
te
chn
iqu
eU
tiliz
e ai
r m
attr
ess/
hee
l pro
tect
ors
PR
NM
ain
tain
an
ti-c
oag
ula
nt
pro
toco
lO
bse
rve
for
sid
e ef
fect
s/co
mp
licat
ion
s o
f IA
BP
Ro
uti
ne
care
ass
oci
ated
wit
h:
Res
pir
ato
ry a
nd
O2 t
her
apy
N-G
tu
be
Hem
od
ynam
ic m
on
ito
rin
g li
nes
Ch
est
tub
eIV
’sF
ole
y ca
thet
er
Inta
ke
/Ou
tpu
t:Q
1H
(S
tric
t)U
rin
e S
pec
ific
Gra
vity
- Q
8H
Su
gar
/Ace
ton
e P
RN
Ac
tivi
ty:
Bed
rest
wit
h lo
g r
olli
ng
Do
no
t el
evat
e H
OB
> 3
0°-
45
°D
o n
ot
flex
bal
loo
n le
g a
t g
roin
or
knee
Uti
lize
frac
ture
bed
pan
RO
M Q
8H
to
un
invo
lved
ext
rem
ity
Do
rsifl
exio
n o
f in
volv
ed f
oo
t
Die
t:N
PO
- c
lear
liq
uid
- s
oft
as
tole
rate
dS
up
ple
men
tal n
utr
itio
nal
su
pp
ort
Tub
e fe
edin
gs
- h
yper
alim
enta
tio
n
Re
spir
ato
ry T
he
rap
y:E
valu
ate
bre
ath
so
un
ds
Q4
H &
PR
NR
ou
tin
e re
spir
ato
ry c
are
of
pat
ien
t w
ith
en
do
tu
be/
trac
hS
teri
le s
uct
ion
tec
hn
iqu
eM
od
ified
res
pir
ato
ry t
her
apy
Co
ug
hin
g a
nd
dee
p b
reat
hin
g,
ince
nti
ve s
pir
om
etry
an
d
nas
otr
ach
ial s
uct
ion
ing
may
be
uti
lized
Da
ily L
ab
wo
rk/P
RN
Blo
od
wo
rk:
SM
A -
18
QD
Mo
nit
or
K+
, B
UN
, cr
eati
nin
e cl
ose
ly P
RN
Car
dia
c en
zym
es C
PK
, is
oen
zym
es Q
DC
BC
wit
h D
iff.
QD
/PR
NP
late
lets
, P
T, P
TT,
clo
ttin
g t
imes
QD
/PR
NA
BG
- m
on
ito
r cl
ose
ly Q
D/P
RN
Ch
est
X-r
ay Q
DU
rin
e an
d s
eru
m o
smo
lari
ty -
QD
EK
G Q
D -
rh
yth
m s
trip
s P
RN
Blo
od
, u
rin
e an
d s
pu
tum
cu
ltu
res
for
tem
per
atu
re 1
02
°
III.
NU
RS
ING
CA
RE
kA
RD
EX

41 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
SYSTEM POTENTIAL PROBLEMS NURSING INTERVENTIONS
Cardiac Left Ventricular Failure Monitor Vital Signs q15-30" until stableBlood Pressure MAP, Syst, DA, AOEDPHeart RatePAPPCWP/LAPCardiac Output/Cardiac IndexCVPSVR (Systemic Vascular Resistance)Maintain Optimal Diastolic Augmentation and Afterload ReductionMaintain Clarity of ECG Pattern Serving as TriggerRhythm Strips PRN12 Lead ECGs QD and PRNCardiac EnzymesCheck Pacer Function
CAUTION n In the event of Asystole, assure balloon movement by placing Trigger on ECG, Arterial Pres-
sure or Internal (bear in mind a Mean Arterial Pressure of about 50 mmHg is required to visualize augmentation).
Respiratory Pulmonary EdemaPulmonary EmboliAtelectasisPneumoniaPleural Effusions
Monitor ABGs closely PRNObserve Chest X-ray QDn Lung fieldsn Balloon positionProvide appropriate ventilatory supportStandard respiratory care on intubated patient with sterile suctioning techniquePost-extubation, modified respiratory therapy is utilizedDeep breathing, coughing, chest physiotherapy and naso-tracheal suctioning may be usedElevate HOB 30°Turning (if hemodynamically stable) cautiously
NeurologicalPsychiatric
Altered Level of ConsciousnessPsychosisOver SedationCerebral Embolization
Neurological assessment q2h/PRN(Pupils, LOC, motor function)Appropriate sedationNormalization of environment (TV and radio, if appropriate)Uninterrupted rest periods are essential to these patientsEmotional support regarding fears and anxieties should be provided to patient and family
Renal Prerenal FailureAcute Renal FailureUrinary Tract InfectionOcclusion of Renal Artery
Observe urine output q1hNotify physician if < 30cc or > 200 cc/hr. In absence of diuretics or fluid challengeStrict Intake and OutputObserve patient’s fluid volume status - Intake and OutputDaily Serum K+, BUN, Creatinine or Blood chemistries qd/PRNDaily weightUrine Specific Gravity q8hUrine Electrolytes and Osmolarity qdNote appearance of urineWatch for sings of urinary tract infectionCheck position of IAB catheter on chest film
IV. NURSING CARE Of THE PATIENT ON AN IABP

| 42 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
IV. NURSING CARE Of THE PATIENT ON AN IABP (continued)
SYSTEM POTENTIAL PROBLEMS NURSING INTERVENTIONS
Vascular Peripheral IschemiaThrombocytopeniaPeripheral EmbolismBleeding from Anticoagulation
Check peripheral pulse (q15" x 1 hr, then q2h post-insertionPedal, Posterior Tibial, PoplitealObserve color and temperature of involved leg q2hMaintain anticoagulation protocol:HeparinAspirinRheomacrodexObserve coagulation studies: PT, PTT, Platelets, Hgb and HctObserve for side effects of anticoagulation therapy: petechiae, ecchymosis, excessive bleeding from catheter insertion sitesAvoid flexing the patient’s hip and knee of involved leg due to IAB catheterApply anti-embolism stockings to non-involved leg
Immunologic Wound InfectionSystemic Sepsis
Monitor temperatureObserve WBCMaintain antibioticsChange IAB dressing qd - strict sterile techniqueMaintain “Best Practice” for all hemodynamic lines and observe for drainageCulture appropriate sites including blood, urine and sputum if specific signs and sym-ptoms of infection process are present.
Gastro-intestinal NutritionalStress UlcerationParalytic Ileus
May have diet as tolerated (clear liquid/soft)Hyperalimentation or tube feedings may be necessary with prolonged intubationMeasure abdominal girth q8hAssess bowel sounds q8hObserve for abdominal distention. Use stool softeners and fracture bedpan as appropriatePortable KUB X-ray may be required without interrupting IABPNaso-Gastric tube if appropriateNaso-Gastric drainage q8h for occult bloodProvide appropriate antacid regimen
Musculoskeletal ThrombosisDecubitus UlcerFoot Drop
ROM - Active and Passive to uninvolved legDorsiflexion of foot on involved legTurn (log roll) q1-2h – cautiously if hemodynamically stableApply air mattress and utilize heel and elbow protectorsUse footboard or high top tennis shoes to prevent foot drop
Patient and Family Teaching
Family anxietyLate Distal EmboliLate Aortic Dissection
Reinforce simple explanation to patient and familyDischarge planning – communication of progress to nursing floorObserve for and instruct in manifestations of late peripheral ischemia or emboli
Cardiac Assist Device
Mechanical Function of IABP Note and record settings according to hospital policyObtain optimal diastolic augmentation and optimal afterload reduction PRNNotify physician of difficultyPrevent inflation of IABP during Ventricular EjectionMaintain adequate ECG and arterial traceChange Helium tank PRNNote IAB autofill q2h/refill PRNWatch for signs of balloon leak: frequent loss of augmentation, blood in extender tubingIf IAB catheter is immobile for greater than 30 minutes, notify physician for appropriate intervention

43 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
V. CRITICAL PATHwAY Of THE IABP PATIENT
INSERTION PUMPING wEANING REMOVAL
Blood Work H&H, pt, ptt Platelet count, WBC Prior to removal, obtain: H&H, pt, ptt, platelet count
Diagnostic Procedures
FluoroscopyPortable CXR
Routine CXR qd, radiopaque tip at 2nd to 3rd ICS
Treatments Shave and prep both potential insertion sites.
Monitor insertion site frequently.Arterial line care per policy.Dressing change per policy.
Pressure applied and site dressed per policy.
Activity Maintain bed rest:Do not raise HOB > 45°.Do not flex or bend the leg in which the IAB was inserted.Assist the patient with log rolling and positioning.
Bed rest per policy.OOB as tolerated.
Nutrition Will depend on the patient’s condition and the indication for IAB insertion.
Nursing Interventions
Assess patient and monitor hemodynamic alterations per ICU routine.Administer IV fluids, vasodilator and/or inotropic agents per orders.Assess patient for pain or discomfort and medicate per physician order.Assess vascular status (color, sensation and movement) as well as pulse quality (pedal, posterior tibial, popliteal, femoral, and radial bilaterally).
NOTE: diminished left radial pulse may indicate IAB migration.Maintain anticoagulation protocol per physician order and observe for side effects.Encourage deep breathing.Assist the patient with turning and positioning at least q2h.Observe for urine output.
NOTE: urine output < 30cc/hr may be an indication that the IAB is occluding the renal arteries.Assure IAB movement, verify IABP controls in accordance with hospital policies.
NOTE: IAB should not remain immobile for > 30 minutes in situ.
NOTE: change of pedal pulses in affected leg could be a sign of limb ischemia.
Patient Teaching
Educate the patient and family members on IABP therapy utilizing the patient education brochure.Explain each phase of the IABP process. Instruct patient to:n Apply pressure to insertion site if they should cough or sneezen Report any chest pain or heavinessn Report any pain, numbness or tingling in their arms or legs
Expected Outcomes
Patient and family will have adequate knowledge base of IABP therapy.Relief of patient and family anxiety.The patient will experience clinical improvement from the IAB by:n Increasing the supply of myocardial oxygenn Decreasing the demand for myocardial oxygenThis will be evidenced by:n Increased cardiac outputn Increased MAPn Decreased PAP/PCWPn Decreased chest painSmooth progression through IABP therapy.Patient hemodynamically stable.
The foregoing is intended to serve as a guideline for the development of a critical pathway. It is not a recommendation
from MAQUET.

| 44 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
INSERTION PUMPING wEANING REMOVAL
Description of Phases A balloon is positioned in your aorta after being introduced through an artery.
The IABP shuttles gas from the console to the balloon and is timed with your heart beat.
Decreasing the amount of assistance your heart needs from the IABP.
Removing the balloon from your artery.
Teaching Most insertions of the IAB can be completed in approx. 15 minutes. The insertion site will be numbed prior to insertion. During the insertion, you may feel some pressure at the insertion site.
The IABP is helping your heart but not beating for it. Pumping will stop every 2 hours for a short period of time. This is normal.
The amount of time it takes to wean varies for each patient.
Removal is typically done at the bedside and only takes a few minutes to complete.
Activity Bed Restn To ensure that the IAB remains in the proper position, you should not sit up or
attempt to get out of bed.n The leg in which the IAB is inserted should not be bent or flexed.
Your nurse will assist you with turning and changing your position.Take deep breaths frequently.
Once the IAB is removed, you will remain in bed for a specific length of time depending on what your physician has ordered. This is usually 6-8 hours.
Nursing Interventions Your condition will be monitored according to ICU routine.The nurse will assess your vital signs, which include:n Heart rate and rhythm, blood pressure, respirations, pulse checks and other
measurements as your condition warrants.The insertion site will be checked frequently by your nurse.The dressing will be changed on a regular basis.Your nurse will give you pain medication. Please report any of the following:n Chest pain or heaviness, pain, numbness or tingling in your arms or legs.
Report any wetness at the insertion site.
Diagnostic Procedures Fluoroscopy (X-ray guidance) may be utilized during insertion. Chest X ray will be done to verify placement of the IAB.
Routine chest X-rays will be obtained during IABP therapy.
Nutrition Your diet will depend on your condition and the reason the IAB was inserted.
Lab Tests Blood tests will be obtained prior to the insertion.
Blood tests will be obtained as your condition warrants it.
The foregoing is intended to serve as a guideline for developing a clinical progression for IABP Therapy. It is not a
recommendation from MAQUET.
The clinical progression is an outline of what to expect for patients and families who require Intra-Aortic Balloon
Pump Therapy. The process will vary for each patient.
VI. CLINICAL PROGRESSION - IABP THERAPY

45 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
VII. CONSIDERATIONS fOR TRANSPORT
A. PURPOSE Of TRANSPORT PROGRAM
B. PLANNING THE TRANSPORT PROGRAM
1. Retrieval vs. Referral
2. Coordinator of Transport Team
C. TRANSPORT TEAM
1. Physician
2. Nurse, IABP Technician
D. TRANSPORT PROGRAM CONSIDERATIONS
1. Team Leader
2. Liabilities
3. Communication and Response Procedure
4. Consent Form and Patient Chart
5. Family Education
6. Patient Management During Transport
E. VEHICLE USED fOR TRANSPORT
1. Ambulance
a. power supply
b. equipment on board
c. ramp
d. response time
2. Aircraft
a. power supply
b. equipment on board
f. EQUIPMENT CONSIDERATIONS
1. IABP Supplies
2. Drugs
3. Infusion Pumps
4. Respiratory Care
G. POST TRANSPORT CONSIDERATIONS
1. Equipment Check
2. Follow-up

| 46 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
CITATIONS
REfERENCE LIST
Barron HV, Bowlby LJ, Breen T, et al. Use of reperfusion therapy for acute myocardial infarction in the United States - data from the National Registry of Myocardial Infarction 2. Circulation 1998;97(12):11.
Barron HV, Every NR, Parsons LS, et al. The use of intra-aortic balloon counterpulsation in patients with cardiogenic shock complicating acute myocardial infarction: Data from the National Registry of Myocardial Infarction 2. American Heart Journal 2001;141:933–9.
Benchmark Counterpulsation Outcomes Registry 2005.
Christenson JT, Licker M, Kalangos A. The role of intra-aortic counterpulsation in high-risk OPCAB surgery: a prospective randomized study. Journal of Cardiovascular Surgery 2003 Jul-Aug;18(4):286-94.
Christenson JT, Cohen M, Ferguson JJ III, et al. Trends in intra-aortic balloon counterpulsation complications and outcomes in cardiac surgery. Annals of Thoracic Surgery 2002 Oct;74(4):1086-91.
Christenson JT, Simonet F, Schmuziger M. Economic impact of preoperative intra-aortic balloon pump therapy in high-risk coronary patients. Annals of Thoracic Surgery 2000 Aug;70:510-5.
Christenson JT, Simonet F, Badel P, Schmuziger M. Optimal timing of preoperative intra-aortic balloon pump support in high-risk coronary patients. Annals of Thoracic Surgery 1999 Sep;68(3):934-9.
Christenson JT, Schmuziger M. Preoperative intra-aortic balloon pump therapy in high-risk coronary patients - impact on postoperative inotropic drug use. Today's Therapeutic Trends 1999;17(3):217-225.
Christenson JT, Simonet F, Badel P, Schmuziger M. Evaluation of preoperative intra-aortic balloon pump support in high risk coronary patients. European Journal of Cardiothoracic Surgery 1997 Jun;11(6):1097-1103; discussion 1104.
Christenson JT, Simonet F, Schmuziger M. The effect of preoperative intra-aortic balloon pump support in high risk patients requiring myocardial revascularization. Journal of Cardiovascular Surgery 1997 Aug;38(34):397-402.
Claflin, N, guest editor. AACN Clinical Issues in Critical Care Nursing - Standards and Quality Assurance. Vol. 2, No. 1 J.B. Lippincott Company Philadelphia February 1991.
Craver JM, Murrah CP. Elective intra-aortic balloon counterpulsation for high-risk off-pump coronary artery bypass operations. Annals of Thoracic Surgery 2001 Apr;71(4):1220-3.
Gould KA. Mechanical assist for the failing heart. Critical Care Nursing Clinics of North America WB Saunders Company Philadelphia 1989.
Guyton AC. Textbook of Medical Physiology. Seventh Edition; WB Saunders Company Philadelphia 1986.
Hasdai D, Califf RM, Thompson TD, et al. Predictors of cardiogenic shock after thrombolytic therapy for acute myocardial infarction. Journal of the American College of Cardiology 2000 Jan; 35(1):136-43.
Hasdai D, Holmes DR Jr, Califf RM, et al. Cardiogenic shock complicating acute myocardial infarction: predictors of death. American Heart Journal 1999 Jul;138(1 Pt 1):21-31.
Hochman JS. Cardiogenic shock complicating acute myocardial infarction. Expanding the paradigm. Circulation 2003;107:2998–3002.
Hochman JS, Sleeper LA, Godfrey E, et al. Should we emergently revascularize Occluded Coronaries for cardiogenic shock: an international randomized trial of emergency PTCA/CABg-trial design. American Heart Journal 1999 Feb;127(2):313-21.
Hollenberg SM, Kavinsky CJ, Parrillo JE. Cardiogenic shock. Annals of Internal Medicine 1999 Jul 6;131(1):47-59.
Hudson MP, Granger CB, Stebbins AL, et al. Cardiogenic shock survival and use of intra-aortic balloon counterpulsation: results from the gUSTO I and III trials - Abstract #1942. Circulation 1999 Nov;100 Suppl(18):I370.
Kahn JK. Intra-Aortic Balloon Pumping/Theory and Clinical Applications in the 21st Century. A Monograph for the Clinician. Datascope Corp. December 2004.
Kim KB, Lim C, Ahn H, Yang JK. Intra-aortic balloon pump therapy facilitates posterior vessel off-pump coronary artery bypass grafting in high-risk patients. Annals of Thoracic Surgery 2001 Jun;71(6):1964-8.
Kinney MR, Dear CB, Packa DR, Voorman DN. AACN’s Clinical Reference for Critical Care Nursing. Fourth Edition McGraw Hill Book Company 2001.

47 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
REfERENCE LIST (continued)
Kovack PJ, Rasak MA, Bates ER, et al. Thrombolysis plus aortic counterpulsation: Improved survival in patients who present to community hospitals with cardiogenic shock. Journal of the American College of Cardiology 1997 Jun;29(7):1454-8.
Millar S, Sampson LK, Soukup M. AACN Procedure Manual for Critical Care. WB Saunders Company Philadelphia 1985.
Mishra S, Chu WW, Torguson R, et al. Role of prophylactic intra-aortic balloon pump in high-risk patients undergoing percutaneous coronary intervention. American Journal of Cardiology 2006 Sep 1;98(5):608-12. Epub 2006 Jun 30.
Ohman EM. Counterpulsation and thrombolysis together improve survival after cardiogenic shock – the TACTICS results. Presented at the 22nd Congress of European Society of Cardiology on August 27, 2000 in Amsterdam, the Netherlands.
Quaal SJ. Comprehensive Intra-aortic Balloon Pumping. CV Mosby Company St. Louis 2nd Edition 1993.
Quaal SJ, guest editor. AACN Clinical Issues in Critical Care Nursing. Cardiac Assist Devices Vol 2, No. 3, JB Lippincott Company Philadelphia August 1991.
Ryan EW, Foster E. Images in cardiovascular medicine. Augmentation of coronary blood flow with intra-aortic balloon pump counter-pulsation. Circulation 2000 Jul 18;102(3):364-5.
Sanborn TA, Sleeper LA, Bates ER, et al. Impact of thrombolysis, intra-aortic balloon pump counterpulsation, and their combination in cardiogenic shock complicating acute myocardial infarction: a report from the ShOCK Trial Registry. Should we emergently revascularize Occluded Coronaries for cardiogenic shock? Journal of the American College of Cardiology 2000 Sep;36(3 Suppl A):1123-9.
Stone GW, Ohman EM, Miller MF, et al. Contemporary utilization and outcomes of intra-aortic balloon counterpulsation in acute myocardial infarction. Journal of the American College of Cardiology 2003 Jun 4;41(11):1940-45. Comment in: Journal of the American College of Cardiology 2003 Jun 4;41(11):1946-7.
Suzuki T, Okabe M, Handa M, et al. Usefulness of preoperative intra-aortic balloon pump therapy during off-pump coronary artery bypass grafting in high-risk patients. Annals of Thoracic Surgery 2004 Jun;77(6):2056-9; discussion 2059-60.
Underhill Sl, Wood SL, Sivarajan ES, Halpenny CJ. Cardiac Nursing. Second Edition. JB Lippincott Philadelphia 1989.
Vazquez M, Engman Lazear S, Larson EL. Critical Care Nursing. Second Edition WB Saunders Company Philadelphia 1992.
Vender JS, guest ed. Intensive care monitoring. Critical Care Clinics WB Saunders Company Philadelphia 1989.
Wolvek S. The evolution of the intra-aortic balloon: The Datascope contribution. Journal of Biomaterials Applications 1989 April; 3:527 542
BIBLIOGRAPHY
Theory
Bolooki H. Clinical Application of Intra-aortic Balloon Pump. Third Edition. Futura Publishing Company Inc, 1998.
Cadwell CA, Quaal SJ. Intra-aortic balloon counterpulsation timing. American Journal of Critical Care. July 1996; 5(4):254-261.
Donelli A, Jansen JRC, Hoeksel B, et al. Performance of a real-time dicrotic notch detection and prediction algorithm in arrhythmic human aortic pressure signals. Journal of Clinical Monitoring and Computing 2002;17:181–5.
Joseph D, Bates S. Intra-aortic balloon pumping - how to stay on course. American Journal of Nursing 1990 Sep; 90(9):42 47.
Maccioli GA, Ed. Intra-aortic balloon pump therapy. Baltimore Williams & Wilkins 1997.
Maccioli GA, Lucas WJ, Norfleet EA. The intra-aortic balloon pump: A review. Journal of Cardiothoracic Anesthesia 1988;2:365 373.
Mahaffey KW, Kruse KR, Ohman EM. Perspectives on the use of intra-aortic balloon counterpulsation in the 1990s. In: Topol EJ, ed. Textbook of Interventional Cardiology St. Louis WB Saunders 1996:303-321.
Quaal SJ, guest ed. Critical Care Nursing Clinics of North America. Philadelphia WB Saunders December 1996;8(4).
Shinn AE, Joseph D. Concepts of intra-aortic balloon counterpulsation. Journal of Cardiovascular Nursing 1994; 8(2):45 60.
Takeuchi M, Nohtomi Y, Yoshitani H, et al. Enhanced coronary flow velocity during intra-aortic balloon pumping assessed by transthoracic Doppler echocardiography. Journal of the American College of Cardiology. 2004;43:368–76.
Whitman G. Intra-aortic balloon pumping and cardiac mechanics: A programmed lesson. Heart and Lung 1978; 7(6):1034 1050.

| 48 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
Indications
Anwar A, Mooney MR, Stertzer SH. Intra-aortic balloon counterpulsation support for elective coronary angioplasty in the setting of poor left ventricular function: A two center experience. The Journal of Invasive Cardiology 1990 July/August;1(4):175 180.
Arafa OE, Geiran OR, Anderson K, et al. Intra-aortic balloon pumping after predominantly right ventricular failure after heart transplantation. Annals of Thoracic Surgery 2000;70:1587–93.
Baskett RJF, Ghali WA, Maitland A, Hirsch GM. The intra-aortic balloon pump in cardiac surgery. Annals of Thoracic Surgery 2002;74:1276–87.
Baskett RJF, O’Connor GT, Hirsch GM, et al. A multicenter comparison of intra-aortic balloon pump utilization in isolated coronary artery bypass graft surgery. Annals of Thoracic Surgery 2003;76:1988–92.
Bates ER, Stomel RJ, Hochman JS, Ohman EM. The use of intra-aortic balloon counterpulsation as an adjunct to reperfusion therapy in cardiogenic shock. International Journal of Cardiology 1998;65(Suppl 1):S37–42.
Bolooki H. Emergency cardiac procedures in patients in cardiogenic shock due to complications in coronary artery disease. Circulation 1989 June;79(6)(Suppl I):I 137 I 147.
Briguori C, Sarais C, Pagnotta P, et al. Elective versus provisional intra-aortic balloon pumping in high-risk percutaneous transluminal coronary angioplasty. American Heart Journal 2003;145:700–707.
Califf, R.M.; Ohman, E.M., Reocclusion after thrombolytic therapy and percutaneous transluminal coronary angioplasty. Cardiac Assists 1990 March; 5(2).
David JS, Gueugniaud PY, Hepp A, et al. Severe heart failure secondary to 5-fluorouracil and low doses of folinic acid: Usefulness of an intra-aortic balloon pump. Critical Care Medicine 2000;28:3358–60.
Demas C, Flancbaum L, Scott G. The intra-aortic balloon pump as an adjunctive therapy for severe myocardial contusion. American Journal of Emergency Medicine 1987;5:499–502.
Dietl CA, Berkheimer MD, Woods EL, et al. Efficacy and cost effectiveness of preoperative IABP in patients with ejection fraction of 0.25 or less. Annals of Thoracic Surgery 1996;62:401-409.
Emmerman CL, Pinchak AC, Hagen JF. hemodynamic effects of the intra-aortic balloon pump during experimental cardiac arrest. American Journal of Emergency Medicine 1989 July;7:373 383.
Emery RW, Eales F, Joyce LD. Mechanical circulatory assistance after heart transplantation. Annals of Thoracic Surgery 1991; 51:43 7.
Ferguson JJ, Cohen M, Freedman RJ Jr, et al. The current practice of intra-aortic balloon counterpulsation: Results from the Benchmark Registry. Journal of the American College of Cardiology 2001;38:1456–1462.
Freedman RJ Jr. Myoconservation in cardiogenic shock The use of intra-aortic balloon pumping and other treatment modalities. Cardiac Assists 1992 January;6(2).
Freedman RJ Jr. The intra-aortic balloon pump system: Current roles and future directions. Journal of Applied Cardiology 1991;6:313 318.
George BS. Thrombolysis and intra-aortic balloon pumping following acute myocardial infarction Experience in four TAMI studies. Cardiac Assists 1988 October;4(3).
Georgen RF, Dietrick JA, Pifarre R. Placement of intra-aortic balloon pump allows definitive biliary surgery in patients with severe cardiac disease. Surgery 1989 September;106(4):808 814.
Goodwin M, Hartman J, McKeever L, et al. Safety of intra-aortic balloon counterpulsation in patients with acute myocardial infarction receiving streptokinase intravenously. The American Journal of Cardiology 1989; 64:937 938.
Grotz RL, Yeston NS. Intra-aortic balloon counterpulsation in high risk cardiac patients undergoing non cardiac surgery. Surgery 1989 July;106(1):1 5.
Gunnar RM, Bourdillon PDV, Dixon DW. guidelines for the early management of patients with acute myocardial infarction. American College of Cardiology 1990 August;16(2):249 292.
Gurbel PA, Anderson RD, MacCord CS, et al. Arterial diastolic pressure augmentation by intra-aortic balloon counterpulsation enhances the onset of coronary artery reperfusion by thrombolytic therapy, Circulation 1994; 89(1):361 365.
Gutfinger DE, Ott RA, Miller M, et al. Aggressive preoperative use of intra-aortic balloon pump in elderly patients undergoing coronary artery bypass grafting. Annals of Thoracic Surgery 1999;67:610–613.
Hochman JS, Buller CE, Sleeper LA, et al. Cardiogenic shock complicating acute myocardial infarction-etiologies, management and outcome: a report from the ShOCK

49 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
Indications (continued)
Trial Registry. Should we emergently revascularize Occluded Coronaries for cardiogenic shock? Journal of the American College of Cardiology 2000 Sep;36(3 Suppl A):1063-70.
Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. New England Journal of Medicine 1999 Aug; 341(9):625-34.
Hochman JS, Boland J, Sleeper LA, et al. Current spectrum of cardiogenic shock and effect of early revascularization on mortality. Results of an international registry. Circulation 1995 Feb 1;91(3):873-881. Comment in: Circulation. 1995 Sep 1;92(5):1349-50.
Ishihara M, Sato H, Tateishi H, et al. Intra-aortic balloon pumping as the postangioplasty strategy in acute myocardial infarction. American Heart Journal August 1991;122(2):385 389.
Kahn JK, Rutherford BD, McConahay DR. Supported “high risk” coronary angioplasty using intraaortic balloon pump counterpulsation. Journal of the American College of Cardiology 1990 April;15:1151 5.
Kern MJ, Aguirre F, Bach R, et al. Augmentation of coronary blood flow by intra-aortic balloon pumping in patients after coronary angioplasty. Circulation 1993 Feb;87(2):500 511.
Kern MJ, Aguirre FV, Tatineni S, et al. Enhanced coronary blood flow velocity during intra-aortic balloon counterpulsation in critically ill patients. Journal of the American College of Cardiology 1993 Feb;21(2):359 368.
Kern MJ. Intra-aortic balloon pumping post angioplasty - Documentation of increased coronary blood flow. Cardiac Assists 1992 June;6:1 5.
Kern MJ. Intra-aortic balloon counterpulsation. Coronary Artery Disease August 1991;2(6):649 660.
Lane AS, Woodward AC, Goldman MR. Massive propranolol overdose poorly responsive to pharmacologic therapy: Use of the intra-aortic balloon pump. Annals of Emergency Medicine 1987 Dec;16(12):1381 1383.
Lazar HL, Yang XM, Rivers S, et al. Role of percutaneous bypass in reducing infarct size after revascularization for acute coronary insufficiency. Circulation 1991;84(Suppl III):III 416 III 421.
Mangano DT, Browner WS, Hollenberg M. Association of perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. The New England Journal of Medicine 1990 Dec 27; 323(26):1781 8.
Marra C, de Santo LS, Amarelli C, et al. Coronary bypass grafting in patients with severe left ventricular dysfunction: A prospective randomized study in timing of perioperative intra-aortic balloon pump support. International Journal of Artificial Organs 2002;25:141–6.
Masaki E, Takinami M, Kurata Y, et al. Anesthetic management of high-risk cardiac patients undergoing noncardiac surgery under the support of intra-aortic balloon pump. Journal of Clinical Anesthesia 1999;11:342–5.
McNamara NS, Wharton WP, La Rochelle T, Deboard D. Use of intra-aortic counterpulsation in patients with acute myocardial infarction who present to community hospitals. Critical Pathways in Cardiology 2002;1:159–179.
Mercer D, Doris P, Salerno TA. Intra-aortic balloon counterpulsation in septic shock. The Canadian Journal of Surgery 1981 Nov;24(6):643 645.
Ohman EM, George BS, White CJ, et al. Use of aortic counterpulsation to improve sustained coronary artery patency during acute myocardial infarction. Results of a randomized trial. Circulation 1994 Aug;90(2):792 799.
Ohman EM, Califf RM, George BS, et al. The use of intra-aortic balloon pumping as an adjunct to reperfusion therapy in acute myocardial infarction. American Heart Journal 1991 Mar;121(3):895-901.
Reiss N, el-Banayosy A, Posival H, et al. Transport of hemodynamically unstable patients by a mobile mechanical circulatory support team. Artificial Organs 1996;20:959–63.
Ryan TJ, Antman EM, Brooks N, et al. 1999 Update: ACC/AhA guidelines for the management of patients with acute myocardial infarction: Executive summary and recommendations: A report of the American College of Cardiology/American heart Association Task Force on Practice guidelines (Committee on Management of Acute Myocardial Infarction). Circulation 1999;100:1016–1030.
Schreiber TL, Kodali UR, O’Neill WW, et al. Comparison of acute results of prophylactic intra-aortic balloon pumping with cardiopulmonary support for percutaneous transluminal coronary angioplasty (PTCA). Catheterization and Cardiovascular Diagnosis 1998;45:115–119.
Schreiber TL, Miller DH, Zola B. Management of myocardial infarction shock: Current status. American Heart Journal 1989 Feb;117(2):435 443.

| 50 | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP | Clinical Support Services |
Indications (continued)
Siu SC, Kowalchuk GJ, Welty FK, et al. Intra-aortic counterpulsation support in the high risk cardiac patient undergoing urgent noncardiac surgery. Chest 1991 Jun;99(6):1342 1345.
Stomel RJ, Rasak M, Bates ER. Treatment strategies for acute myocardial infarction complicated by cardiogenic shock in a community hospital. Chest 1994;105(4):997 1002.
Complications
Arceo A, Urban P, Dorsaz PA, et al. In-hospital complications of percutaneous intra-aortic balloon counterpulsation. Angiology 2003;54:577–85.
Barnett MG, Swartz MT, Peterson GJ, et al. Vascular complications from intra-aortic balloons: Risk analysis. Journal of Vascular Surgery 1994 Jan;19(1):81 89.
Brodell GK, Tuzcu EM, Weiss SJ. Intra-aortic balloon pump rupture and entrapment. Cleveland Clinic Journal of Medicine 1989 Oct;56(7):740 742.
Cohen M, Ferguson JJ, Freedman RJ Jr, et al. Comparison of outcomes after 8 vs. 9.5 French size intra-aortic balloon counterpulsation catheters based on 9,332 patients in the prospective Benchmark Registry. Catheterization and Cardiovascular Interventions 2002;56(2):200–206.
Eltchaninoff H, Dimas AP, Whitlow PL. Complications associated with percutaneous placement and use of intra-aortic balloon counterpulsation. American Journal of Cardiology 1993 Feb;71:328 332.
Funk M, Gleason J, Foell D. Lower limb ischemia related to use of the intra-aortic balloon pump. Heart and Lung 1989;18:542 552.
Goran SF. Vascular complications of the patient undergoing intra-aortic balloon pumping. Critical Care Nursing Clinics of North America 1989 Sep;1(3):459 467.
Gottlieb SO, Brinker JA, Borken AM, et al. Identification of patients at high risk for complications of intra-aortic balloon counterpulsation: A multivariate risk factor analysis. American Journal of Cardiology 1984; 53:1135 1139.
Kantrowitz A, Wasfie T, Freed PS, et al. Intra-aortic balloon pumping 1967 through 1982: Analysis of complications in 733 patients. American Journal of Cardiology 1986;57(11):976 983.
Kvilekval KH, Mason RA, Newton GB, et al. Complications of percutaneous intra-aortic balloon pump. Use in patients with peripheral vascular disease. Archives of Surgery 1991 May;126:621 623.
Lazar JM, Ziady GM, Dummer SJ, et al. Outcome and complications of prolonged intra-aortic balloon counterpulsation in cardiac patients. American Journal of Cardiology 1992,Apr;69:955 958.
Robicsek F, Holleman JH, Roush TS, et al. Peri-operative intra-aortic balloon assist, decreasing complications to the minimum. Thoracic and Cardiovascular Surgeon 2003;51:115–125.
Schecter D, Murali S, Uretsky BF. Vascular entrapment of intra-aortic balloon after short term balloon counterpulsation. Catheterization and Cardiovascular Diagnosis 1991;22:174 176.
Stahl KD, Tortolani AJ, Nelson RL, et al, Intra-aortic balloon rupture. ASAIO Journal 1988;XXXIV:496 499.
Velez CA, Kahn JK. Compartment syndrome from balloon pump. Catheterization and Cardiovascular Interventions 2000;51:217–219.
Insertion
Gorton ME, Soltanzadeh H. Easy removal of surgically placed intra-aortic balloon pump catheter. Annals of Thoracic Surgery 1991;51:325 6.
Heebler RF. Simplified technique for open placement and removal of intra-aortic balloon. Annals of Thoracic Surgery 1989;48:134 6.
Nash IS, Lorell BH, Fishman RF, et al. A new technique for sheathless percutaneous intra-aortic balloon catheter insertion. Catheterization and Cardiovascular Interventions 1991 May;23(1):57 60.
Phillips SJ, Tannenbaum M, Zeff RH, et al. Sheathless insertion of the percutaneous intra-aortic balloon pump: An alternate method. Annals of Thoracic Surgery 1992; 53:162.
Shahian DM, Jewell ER. Intra-aortic balloon pump placement through dacron aortofemoral grafts. Journal of Vascular Surgery 1988 Jun;7:795 7.
Pediatrics
Anella J, McCloskey A, Vieweg C. Nursing dynamics of pediatric intra-aortic balloon pumping. Critical Care Nurse 1990 Apr;10(4):24 28.
del Nido PJ, Benson LN, Bohn D, et al. Successful use of intra-aortic balloon pumping in a 2 kilogram infant. Annals of Thoracic Surgery 1988 Nov;46:574 576.

51 | | Clinical Support Services | Managing Intra-Aortic Balloon Pump Therapy - CS300 IABP |
Pediatrics (continued)
Dunn JM. The use of intra-aortic balloon pumping in pediatric patients. Cardiac Assists 1989 June; 5(1).
Nawa S, Sugawara E, Murakami T, et al. Efficacy of intra-aortic balloon pumping for failing fontan circulation. Chest 1988 Mar;93(3):599 603.
Pinkney KA, Minich LL, Tani LY, et al. Current results with intra-aortic balloon pumping in infants and children. Annals of Thoracic Surgery 2002;73:887–91.
Veasy LG, Blalock RC, Orth J. Intra-aortic balloon pumping in infants and children. Circulation 1983;68(5):1095 1100.
Webster H, Veasy LG. Intra-aortic balloon pumping in children. Heart and Lung 1985;14(6):548-555.
Transport
Bellinger RL, Califf RM, Mark DB. helicopter transport of patients during acute myocardial infarction. American Journal of Cardiology 1988 Apr;61:718 722.
Gottlieb SO, Chew PH, Chandra N. Portable intra-aortic balloon counterpulsation: Clinical experience and guidelines for use. Catheterization and Cardiovascular Diagnosis 1986;12:18 22.
Kramer RP Jr. helicopter transported intra-aortic balloon pumping: advanced technology made airborne. Cardiac Assists 1988 Jun;4(2).
Mertlich G, Quaal SJ. Air transport of the patient requiring intra-aortic balloon pumping. Critical Care Nursing Clinics of North America 1989 Sep;1(3):443 458.
Nursing Care
Bavin TK, Self MA. Weaning from intra-aortic balloon pump support. American Journal of Nursing 1991 Oct;91(10): 54 59.
Patacky MG, Garvin BJ, Schwirian PM. Intra-aortic balloon pumping and stress in the coronary care unit. Heart and Lung 1985 Mar;14(2):142-8.
Quaal SJ, guest ed. Critical Care Clinics of North America. Philadelphia WB Saunders 1996 Dec;8(4).
Shoulders O. Managing the challenge of IABP therapy. Critical Care Nurse 1991 Feb;11(2):60 76.
Weinberg LA. Buying time with an intra-aortic balloon pump. Nursing 1988 Sep;18(9):44 49.


PROGRAM AND SPEAkER EVALUATION
Managing IABP Therapy Date:Program Code 05:
Please rate the program and speaker items by placing a mark in the appropriate column.
PROGRAM EVALUATION1
POOR2
fAIR3
GOOD4
VERY GOOD5
EXCELLENT
Program met the stated objectives
Content covered topic adequately
Overall quality of this program
Overall quality of speaker(s)
Quality of the program objectives
Program met my personal objectives
I can incorporate program content into my practice
Speaker Name:
SPEAkER EVALUATION1
POOR2
fAIR3
GOOD4
VERY GOOD5
EXCELLENT
Objectives- Stated obectives met
Audiovisual- Contributed to presentation
Content- Relevance of content to objectives
Presentation- Speaker qualified and held interest
Effectiveness- Speaker was organized and effective
Practice- Validated and/or changed practice
Comments:
Participant Name:


GETINGE GROUP is a leading global provider of products andsystems that contribute to quality enhancement and costefficiency within healthcare and life sciences. We operate under the three brands of ArjoHuntleigh, GETINGE and MAQUET. ArjoHuntleigh focuses on patient mobility and wound management solutions. GETINGE provides solutions for infection control withinhealthcare and contamination prevention within life sciences.MAQUET specializes in solutions, therapies and products for surgical interventions, interventional cardiology and intensive care.
PN
: 000
2-08
-087
3 R
3 · (
U.S
.) M
CV
0001
2628
RE
VA ·
(Intl.
) MC
V-LP
-800
0060
9-E
N-0
1 · M
AQ
UE
T is
a t
rad
emar
k of
MA
QU
ET
gm
bh
· C
S30
0 is
a t
rad
emar
k of
Dat
asco
pe
Trad
emar
k C
orp
., b
ut r
egis
tere
d s
tatu
s ha
s no
t ye
t b
een
rece
ived
. · C
opyr
ight
201
2 D
atas
cop
e C
orp
. or
its a
ffili
ates
. All
right
s re
serv
ed. 0
9/12
· C
autio
n: U
.S. F
eder
al L
aw r
estr
icts
thi
s d
evic
e to
sal
e b
y or
on
the
ord
er o
f a
phy
sici
an.
R
efer
to
Inst
ruct
ions
fo
r U
se f
or c
urre
nt in
dic
atio
ns, w
arni
ngs,
con
trai
ndic
atio
ns, a
nd p
reca
utio
ns.
MAQUET1300 MacArthur Blvd.Mahwah, NJ 07430, USAPhone: +1 201 995 8700
MAQUET Medical Systems USA45 Barbour Pond DriveWayne, NJ 07470, USAPhone: 1 888 880 2874
http://ca.maquet.comwww.maquet.com





























