Embed Size (px)
Citation preview

N D T A N E T W O R K • M A R C H / A P R I L 2 0 0 5 • N D T W O R L D W I D E • 2 5
any orthopedic surgical procedures are
designed to enhance the walking ability
of children and adults. Congenital deformities,
developmental abnormalities, acquired
problems such as amputation or trauma, and
degenerative changes all contribute to dimin-
ished gait efficiency. Locomotion is an extremely
complex endeavor with an
interaction between bony
alignment, joint range of
motion, neuromuscular
activity, and the laws of
physics. An understanding
of gait analysis enables the
treating physician to
understand the nature of
the gait problem, gain
insight into the etiology,
and predict possible treatment options. It is
certainly the only way that the technical
outcome of a procedure that is designed to
improve gait can be objectively assessed.
Gait analysis can range from simply observing
a patient’s walk to a fully computerized three-
dimensional motion analysis with energy meas-
urements.
OBSERVATIONAL GAIT ANALYSIS
A complete physical examination with measured
range of motion should be performed on all
Management ofthe Web SpaceTREATMENT ANDSPLINTING INTERVENTION
By Bonnie Boenig, M. Ed, OTR/L
he impact of neurological insult
on the upper extremity often
includes an increase in muscle tightness
distally, particularly in the hand. The
tightness in the hand can be related to
centrally generated tone, posturing dis-
tally in response to demands on postur-
al reactions, or anticipatory response to
task demands. Fisting of the hands may
be characteristically seen, and the degree
of fisting often increases with demands
on posture and active movement. In
treatment, generally speaking, once the
tone-related tension in the hand is
reduced, there is notable weakness and
inactivity in palmar intrinsic muscula-
ture, shortened range of motion in long
finger flexors, and limitations in the
ranges of movement of the thumb
which are reflective of shortened tissue
in the web space.
The posturing that is generally
expressed throughout the whole upper
extremity includes pronation of the
forearm, extremes of flexor or extensor
activity around the elbow, and humer-
al internal rotation. In the hand, there
is a reflection of
Walking Through the Gait LabGAIT ANALYSIS AND DEVELOPMENTAL DISABILITIESBy Hank Chambers, MD
(Excerpted in part from Chambers, HG and Sutherland DH: A Practical Guide to Gait Analysis. Journal of
the American Academy of Orthopedic Surgeons, 10:222-231, 2002).
3
patients who have gait problems. The presence
of muscle and joint contractures, spasticity,
extrapyramidal signs (such as dystonia and
tremor), weakness, motor control problems,
and pain should be determined and charted
in a systematic way. Any abnormal neurological
signs should also be documented as these can
contribute to the gait
abnormalit ies . Radi-
ographic abnormalities
should be documented
inc luding rotat ional
malalignment.
In order to evaluate the
gait of a patient with a
walking problem, one
must sys temat ica l ly
observe the gait. Obser-
vation of the patient walking toward and away
from the observer will enable an understanding
of coronal (or frontal) plane abnormalities
such as trunk sway, pelvic obliquity, hip
adduction/abduction, and possibly rotation.
Each segment (trunk, thigh, leg, and foot)
should be observed coming to and going away
from the evaluator. Abnormalities should then
be charted. The patient will then walk back
and forth with the observer sitting 90 degrees
from the patient. This enables sagittal plane
evaluation such as pelvic (continued on page 18)(continued on page 10)
T H E N E U R O - D E V E L O P M E N T A L T R E A T M E N T A S S O C I A T I O N • M AY / J U N E 2 0 0 5 • VO L U M E 1 2 , I S S U E 3
C L I N I C A L T O O L S
3 President’s Message | 4 NDT Clinician’s Corner | 7 NDT in Australia | 15 Patient Perspective
I N S I D E T H E N E T W O R K :
M
Three-dimensional
motion analysis helps
eliminate some of
the ambiguity
of visual analysis.
T

2 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
REGION 1WA, OR, ID, MT (West Canada)Nancy Garcia, PT130 W. 34th, Spokane,WA 99203509-624-2407 (H)509-623-0400 (W)[email protected]
REGION 2NB, NF, NS, ON, PE, PQ (East Canada)Karen Guha, PT506 Mayflower St.Waterloo, Ontario, Canada(519) [email protected]
REGION 3Southern CA, Northern CA, NVMichelle G. Prettyman, PT5460 White Oak Ave. K301Encino, CA [email protected]
Carrie H.Taguma-Nakamura, OT1235 South Ogden DriveLos Angeles, CA 90019(323) [email protected]
REGION 4WY, CO, UT, NM,AZTori J. Rosenthal, PT, MS3718 Pioneer Ave.Cheyenne,WY 82001307-635-2900 (H)307-421-5554 (W) [email protected]
Marybeth Aretz, PT3627 Osceola StreetDenver CO [email protected]
REGION 5TX, LACarol S. Nuñez-Parker, OTR andTeresa De La Isla, MS, OTRNTS, Inc.4423 ShadowdaleHouston,TX 77041Work: (713) 466-6872 Ext 221Fax: (713) [email protected]
REGION 6KS, MO, OK,ARMyles Quiben, DPT, PT, GCSUniversity of Central ArkansasDepartment of Physical Therapy201 Donaghey Ave. PT Center, Ste300Conway, AR 72032smylesaway1@ aol.com501-450-5557 fax: 501-450-5822
REGION 7ND, SD, MN,WI, NE, IA, IL,Middle CanadaStacy Reichmuth, OTR/L7819 South 97th CircleLa Vista, NE 68128(402) [email protected]@yahoo.com
REGION 8MI, IN, OHKristie Swoverland, PT10911 Old Oak Ct.Ft.Wayne, IN 46845206-373-9761 (W)[email protected]
Kris Waffle, PT827 Upland Ridge DriveFt.Wayne, IN 46825260-489-8329 (H) • 260-446-0100 (W)[email protected] (H)[email protected] (W)
REGION 9KY,VA,TN, NC,Al, MS,GA, SC, FL, PRJeannette A. Beach, PT220 Hemphill Ave.Chattanooga,TN 37411(423) [email protected]
REGION 10ME, NH,VT, NY, MA.CT, RI, PA, DE,NJ, MD,WV, DCLaura Z. Gras PT, DSc ,GCSThe Sage Colleges45 Ferry StreetTroy, NY 12180(518) 244-2066 • Fax: (518) 244-4524
Debra Berube PT1270 Belmont AveSchenectady, NY 12308(518) [email protected]
REGION 11AKDee Berline, OT1000 Fairwood DriveAnchorage,AK 99518907-338-1871 (H)907-550-3004 (W)907-227-5434 (C)[email protected] (W) [email protected] (W)
Cara Leckwold1716 Morningtide Ct.Anchorage,AK [email protected]
REGION 12HISandra Kong, OT99-033 Kaupili PlaceAiea, HI 96701(808) [email protected]
Jan A. Miyashiro1251 Ulupuni StreetKailua, HI 96734(808) 262-1057
PRESIDENTWendy Drake-Kline, OTNeurodevelopmental Therapy Associates1314 Timber Ridge Ct.Waynesville, OH 45068(937) [email protected]
PAST PRESIDENT (appointed)Debbie Evans-Rogers838 Maplewood Falls CourtHouston,TX 77062(281) [email protected]
SECRETARY/TREASURER Linda Markstein, PTMiami Valley Hospital1 Wyoming St., Dayton OH45409(937) [email protected]
IG EXECUTIVE COMMITTEE CHAIRCathy Hazzard, PT916 31 Avenue, NW Calgary, AlbertaCanada T2K 0A5 (403) 289-8249 [email protected]
IG REPRESENTATIVE
Therese McDermott, MHS, CCC-SLP1416 W. Thome Ave.Chicago, IL 60660(773) [email protected]
DIRECTOR OF REGIONS
Pam Moore, MOT, OTR3215 S. Oswego Ave.Tulsa, OK 74135(918) [email protected]
IG REPRESENTATIVEPamela Mullens, Ph.D., PT5623 57th Ave. NESeattle,WA 98105206/[email protected]
MEMBER-AT-LARGEWendi McKenna, DPT7110 Caminito ZabalaSan Diego, CA 92122(858) [email protected]
MEMBER-AT-LARGEKim Westhoff, OTR/LKim’s Kids Pediatric Occupational Therapy15900 S. Hawkins RoadAshland, MO 65010 USA(573) 657-0171 [email protected]
MEMBER-AT-LARGE/FINANCEDenise Koonce1910 VikingHouston,TX 77018 USA(713) [email protected]
CHAIR-ELECT IGEXECUTIVE COMMITTEEGay GirolamiPathways Center2591 Compass RoadGlenview, IL 60025(847) [email protected]
R E G I O N A L C H A I R P E R S O N S
N D T A B O A R D O F D I R E C T O R S
Views expressed in the NDTA Network are those of the authors and are not attributed to the NDTA, the Director of Publications or the Editor, unless expressly stated.The NDTA does not endorse any instructors, courses, educational opportunities, employment classifieds, products or services mentioned in the NDTA Network. Copyright 2001 by the Neuro-Developmental Treatment Association. Materials may not be reproduced without written permission from the Editor.
IG EXECUTIVE COMMITTEEChair: Cathy Hazzard Chair Elect: Gay GirolamiVice Chair:Teddy ParkinsonTreasurer: Sherry W.Arndt Secretary:Teresa GutierrezPeds Subcommittee Chair: Kacy HertzAH Subcommittee Chair: Cathy RunyanCI Working Group Chair: Karen BruntonOT Working Group Chair: Lezlie AdlerPT Working Group Chair:
Susan Breznak-HoneychurchSLP Working Group Chair: Gay Lloyd PinderCI Representative: Judi BiermanOT Representative: Mechthild RastPT Representative: Monica DiamondSLP Representative: Rona AlexanderNominating Committee Chair: Mona Miley, OT
IG STANDING COMMITTEESBonnie Boenig, Grievance Committee ChairTom Diamond, Peer Review Committee ChairJudith C. Bierman and Lois L. Bly,Theoretical
Base Committee Co-ChairsLinda Kliebhan, Curriculum Committee Chair
L E A D E R S H I P D I R E C T O R Y
INSTRUCTORS GROUP
NDTA OFFICE1540 S. Coast Hwy, Ste. 203Laguna Beach, CA 92651
800/869-9295 • 949/376-3456 Fax [email protected] • www.ndta.org

N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 3
A subscription to the Network, which is publishedsix times annually to more than 3,000 members,is included in every NDTA membership.Additional subscriptions and copies of archivedarticles are available for a small fee.
EDITORIAL INFORMATIONWe invite members and non-members to submit articles, ideas and comments to the editor. Editorialassistance and guidelines are available for writers.Look below for upcoming deadlines and themes.
ADVERTISING INFORMATIONTo reach health care professionals who practiceNDT, advertise your products, services, employ-ment classifieds, educational opportunities andNDTA-approved courses in the Network. All adsare placed on a first-come, first-served basis.Payment is required prior to insertion.
DISPLAY AD RATESAdvertise your products and services in multiplethemed issues to maximize your investment. Formore information or to place your ad, contactthe NDTA Office at 800/869-9295 ext. 266.
Space Per issue 4 or more issuesFull page . . . . . . $800 . . . . . . $600 per issueHalf page. . . . . . $500 . . . . . . $400 per issueQuarter page . . $350 . . . . . . $250 per issue
EMPLOYMENT CLASSIFIEDSHave an open position? Find your next employeehere. Members can place employment classifiedads for $100 for the first 50 words, plus $1 foreach additional word. Non-members may placeclassifieds at an additional fee. Placement is for oneissue of the Network and 60 days on the NDTAWeb site. Longer placement is available for anadditional fee. For more information or to placeyour ad, contact contact the NDTA Office at800/869-9295, ext. 266.
EDUCATIONAL OPPORTUNITIESOrganizing a workshop? Your educational oppor-tunity can be placed in one issue of Network andfor 60 days on the NDTA Web site for $200.Longer placement is available for an additional fee.For more information or to place your ad, contactthe NDTA Office at 800/869-9295, ext. 266.
NDTA-APPROVED COURSESEducational courses that are approved by NDTAcan be placed in one issue of Network for $100.Formore information or to place your ad, contact theNDTA Office at 800/869-9295, ext. 266.
ARTICLE & ADVERTISING DEADLINESCopy received after the dates specified will beconsidered for the following issue.
2005 ISSUES THEME DEADLINESept/Oct . . . Pharmacology . . . . . . . . . . . . . . . . June 1Nov/Dec. . . Predicting Lifelong Outcomes. . August 1
K.T. Anders, Editor, NDTA NetworkP.O. Box 521, Upperville,VA 20185540/592-7002 • 540/592-7032 [email protected]
Marcia Stamer, Chair, Publications Committee3752 Seasons DriveAntioch,TN 37013615/367-3604 • [email protected]
Pamela Mullens, Ph.D., PT, Network Liaison5623 57th Ave. NESeattle,WA 98105206/524-1743 • [email protected]
A B O U T T H E N D T A N E T W O R K M E S S A G E F R O M T H E P R E S I D E N T
he web taping and gait analysis articles in
this issue are examples of clinically sophis-
ticated tools for improving the care we give our
clients. They put me in mind of one tool we may
sometimes forget: the ability to communicate
with our clients.
Communication. Sounds so simple. Webster
defines communication as “sharing information,
a sense of mutual understanding and sympathy,
conveying feelings, and being connected to
another person.” I am beginning to understand
more fully how truly complicated the commu-
nication process is and the important responsi-
bility that we all face as we meet the challenges
involved in communicating with our clients.
Therapy sessions involve ongoing communi-
cation between the therapist, the client, and
family member/caregiver and all involve time,
effort, diligence, and a commitment from all
parties in order to be effective.
As therapists, we use whatever it takes to
convey our message—explaining directions and
information in detail, as simply as possible, and
if necessary, providing sensory/motor cues.
Successful rehabilitation depends upon clients
understanding the information we share and
being able to follow through with the functional
activities and exercises that we determine are
appropriate and necessary for recovery. Their
keen awareness of the personal relevance and
importance of these tasks is critical. Our clients
must believe that we care about them as indi-
viduals as much as they believe that we have the
knowledge and skill to aid their recovery. They
need to know that we are truly interested in them
and value their feelings and the feedback that
they share with us.
But although we have endless tools available
to assist us in our communications with others,
such as face-to-face
conversation, telephone,
written word, type,
gesture, facial expressions,
and body language, many
of our clients are not so
fortunate. For them, the
skills we take for granted are often significantly
delayed or absent.Yet from the beginning of their
rehabilitation and recovery process, we bombard
them with new and unfamiliar information that
they are immediately expected to grasp, assim-
ilate, and attempt to utilize for improving their
functional and independent performance. Never
mind that they are also dealing with weakness,
balance issues, spasticity, etc.
Their caregivers, too, are overwhelmed with a
myriad of responsibilities, worries, and fears
related to the care of a loved one. No wonder we
have to repeat the same things over and over
again for them to understand and integrate the
information! It can be frustrating for us as ther-
apists to do so. On the other hand, in trying to
survive one day at a time, our clients and their
caregivers can only absorb so much information
at one time.
I plan to spend a bit more time listening to
my clients and working on mutual understanding
and empathy. Perhaps that will be a form of
communication that they really can “hear.” Might
be good for all of us.
Wendy Drake-Kline
NDTA President
Wendy Drake-Kline
T
The Commitment to Communication

any clinicians seem to have little desire
to study treatment theory, preferring
to use their time learning hands-on tech-
niques. But techniques are only tools; under-
standing theory can provide possible expla-
nations for the expected impact of therapy
and can offer suggestions for the selection of
therapy tools and handling strategies.
The following is a clinician’s interpretation
of treatment theories based upon infor-
mation in Janet Howle’s book Neuro-Devel-
opmental Treatment Approach: Theoretical
Foundations and Principles of Clinical Practice
(2002). These synopses are intended to
provide a brief working knowledge of the
basic theories and are followed by a treatment
model. The practice of NDT is currently
based on an Interactive Systems Model,
which accepts that each system is dependent
upon the integrity of another. The Dynamic
System Theory and the Neuronal Group
Selection Theory, discussed below, are the
basis for this model.
SYSTEMS THEORY/DYNAMIC SYSTEMS APPROACH
Names to know: Nicoli Bernstein, physiol-
ogist (1967) applied the principles of
dynamic systems to the understanding of
human behavior. A number of theorists have
expanded the systems theory, including:
Darrah & Bartlett, Heriza, Kelso, Kugler,
Kelso & Turvey, Perry, Thelen.
Definitions of Key Terms:
Degrees of freedom: Elements of movement
are assembled into functional patterns.
Coordinative Structure: Two or more inde-
pendent parts (muscles or joints ) combine
to perform as one functional unit or synergy.
Functional linkages between groups of
muscles simplifies motor control.
Self organization: Interacting systems,
through repetition and practice, can organize
themselves and create motor patterns out
of this continual activity as discussed in
“Clinical implications of a dynamical
systems theory,” Neurology Report, 22,4-10
by S.B. Perry, 1998).
Rate-limiting factors: Each subsystem
develops at its own rate, but is constrained
(or supported) by physical and environ-
mental factors.
Transitions: Motor behavior is made up of a
series of states of stability, instability,and
phase shifts. During development, motor
behaviors can either become more stable or
destabilize.
Most change can occur during periods of
de-stabilization.
Theory basics:
• Biological systems, like other physical
systems, are complex, multidimensional,
cooperative systems in which no one
subsystem has priority for organizing
the behavior of the subsystem (Howle
2002, pg. 17).
• As a new movement sequence is learned,
the learner attempts to limit the number
of muscles and joints to an excessive
degree, providing mechanical stability.
As learning takes place, the mechanical
constraints are less used, and there is a
freer use of a combination of neural and
musculo-skeletal constraints that allow
for greater motion,variability, and a
higher level of success.
• Movement and changes in movement
patterns generated by various systems
are organized by the interactions of
multiple components of cooperating
systems, such as body weight, muscle
strength, joint configuration, postural
support, mood, attention, specific envi-
ronmental conditions (such as inertia
and gravity), and patterns of neural
firing (Howle 2002, pg. 20).
Clinical Application: Because the impair-
ments underlying functional limitations are
considered rate-limiting factors, treatment
designed to reduce the impact of these factors
will improve function.A clinician’s definition
of constraints to movement can include bony
restrictions, limited flexibility in soft tissue
and fascia, and constraints created by faulty
timing and lack of coordinative firing of
muscles attempting to work cooperatively
together. According to this theory, as new
skills are integrated and become more auto-
matic and less cognitively driven, we should
expect to see more ease of movement and
ability to refine skill. Within the context of
developmental sequence, or when learning
motor behaviors under the conditions of
neuromotor deficit or insult, certain periods
of time are more supportive of having new
skills emerge. Our therapeutic intervention
can actually create periods of “chaos” by
inhibiting compensatory or habitual patterns
of movement; during these opportune times,
the client is more likely to make a shift in
motor behavior.
NEURONAL GROUP SELECTIONTHEORY (NGST)
Names to know: Edelman (1987) and Sporns
(1994) have offered a balance between matu-
ration and interactive physical systems.
Theory Basics:
• Neuronal groups are arranged in neural
Theory Basics Refine Clinical PracticeBy Bonnie Boenig, M.Ed, OTR/L
4 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
C L I N I C I A N ’ S C O R N E R
M

N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 5
maps in segregated areas of the brain;
however long-reaching reciprocal connec-
tions between groups integrate activities
of multiple sensory and motor areas of
the brain.
• Each person has individualized neural maps
as a result of unique motor experiences.
• The development or recovery from brain
damage is aided during activities that occur
in functionally or developmentally appro-
priate environmental contexts and the
individual generates movement to meet
the demands of the task.
Clinical Application: This theory supports the
necessity for including functional tasks during
treatment and using environmental set-up and
handling strategies to assist in providing
effective, precise feedback information.
Clinical judgment is the clinician’s ability
to analyze movement and decipher clues
based upon an understanding of the human
body and accepted theories of motor
behavior, and then to choose the appropriate
combinations of strategies. The best outcomes
in therapy result from having a toolbox of
strategies and techniques, a strong working
knowledge of the structure and systems of
the human body, and an understanding of
the scientific bases of human movement. A
sound theoretical foundation is a beacon to
the appropriate choice of therapeutic
approach, a guide for making shifts in the
therapy plan, and the cornerstone to
achieving optimal functional outcomes. ■
Bonnie Boenig is an NDTA occupational
therapy instructor and a clinical specialist for
Lifeworks of Southwest General Health Center
in Middleburg Heights, Ohio. Bonnie’s private
practice includes short term intensive therapy,
teaching short courses, and providing
customized staff and parent-training programs
for facilities that specialize in pediatric therapy.
She can be reached at [email protected].
MAY 20-22Neurophysical Principles and NDTA
Location: NTS Therapy (Houston)3250 WilliamsburgMissouri City, TX 77049Instructor: Judi Bierman, PT_______________________________________
JUNE 17-19, 2005Functional Activities in Standing and Gait: AnNDT Perspective for Adults with Hemiplegia
Location: Miami Valley HospitalOne Wyoming St., Dayton, OH 45409Instructor: Marie Simeo, PT_______________________________________
JULY 15-17, 2005Practical Applications for Treating Children withNeuromotor Impairments–An NDT/BobathPerspective
Location: KIDSCenter982 Eastern Parkway, Louisville, KY 40217Instructor: Wendy Drake-Kline, OT_______________________________________
JULY 29-31, 2005Problem Solving for Function: An NDT/BobathPediatric Handling Intensive Course
Location: American International College1000 State St., Springfield, MA 01109Instructor: Barb Hodge, PT_______________________________________
AUGUST 27-28 (TWO DAYS ONLY)Topic To Be Announced
Location: Parkview Health System2200 Randallia Dr., Ft. Wayne, IN 46805Instructor: To be announced
SEPT. 23-25, 2005Creative Routes to Outcomes
Location: Erie County Medical Center462 Grider St., Buffalo NY 14215Instructor: Kay Folmar, PT_______________________________________
OCTOBER 14-16, 2005Moving Into NDT/Bobath for SLP’s: AnIntroduction to Neurodevelopmental Treatment
Location: Erie County Medical Center462 Grider St., Buffalo NY 14215Instructor: Therese McDermott, SLP_______________________________________
OCTOBER 21-23, 2005Creative Routes to Outcomes
Location: Genesys Regional Medical CenterOne Genesys Parkway, Grand Blanc, MI 48439Instructor: Kay Folmar, PT_______________________________________
OCTOBER 28-30, 2005Managing Adults with Hemiplegia:An NDT/Bobath Perspective
Location: Estes Park Conference Ctr.101 S. St. Vrain Ave.,Estes Park, CO 80517Instructor: Kay Folmar, PT_______________________________________
NOVEMBER 11-13, 2005Treatment of Children & NeurologicalDisorders: An NDT/Bobath Perspective
Location: Aberdeen Hospital835 East River Rd., New GlasgowNS B2H 5C8 CanadaInstructor: Marcia Stamer, PT
Full refund of the course registration fee, less $50 administrative fee, will be granted upon receipt of a
written request postmarked on or before 30 days before the first day of the course.
Register on the web at www.ndta.org or fax your form into theNational NDTA office at 949/376-3456
NDTA is a nonprofit professional organization of Physical Therapists, Occupational Therapists & Speech LanguagePathologists dedicated to promoting the theory and principles of the Neuro-Developmental Treatment approach.

2. COMPLETE THE ABSTRACT IDENTIFICATION INFORMATION:TITLE OF ABSTRACT. Use all CAPITAL Letters
AUTHOR(S). Underline submitting author
SITE/AGENCY. Indicate where the research study was done
3. SUBMIT APPLICATION INFORMATION:For ABSTRACT submission, please provide ALL of the requestedinformation. For DISPLAY submission, please include:1) Objective, 2) Description, 3) Conclusions/Ramifications.
PURPOSE: Study hypothesis/questions
SUBJECTS: Number and characteristics
METHODS: Techniques/materials used
DATA ANALYSIS: Statistical tests used
RESULTS: What did data analysis reveal?
CONCLUSIONS: Do results support the researchhypothesis?
RELEVANCE: Significance of the study relative to healthcare
ACKNOWLEDGEMENTS: Site/Agency funding/supporting the study
4. SUBMIT BY JULY 31, 2005NDTA 2004 Research Exhibit, C/O Evangeline Yoder13057 Warwick Blvd., Newport News,VA 23602E-mail: [email protected]: (757) 249-2258 • Fax: (757) 881-9709
Evangeline Yoder, Research Reviewer, will acknowledge acceptance of your submission and send Poster DisplayInstructions.All poster presenters will be required to register for the Conference.
The NDTA Conference Committee invites you to participate in the Poster Display being held in the Exhibit Hall duringthe 2005 Conference in Houston,Texas. Posters will be on display beginning on Friday, September 30th through Saturday,October 1st. The Staffed Poster Session will take place on Friday, September 30th from 6:00 – 8:00 P.M.All poster pre-senters will be acknowledged and abstracts will be printed in the Conference Program Book.
ABSTRACTS: We encourage you to submit an ABSTRACT of your clinical research. Each submitting Author may entera maximum of three Abstracts. Please follow the instructions listed below when offering your research for consideration.
DEMONSTRATION POSTERS: You may wish to create a DISPLAY featuring Clinical Applications of NDT/Bobathphilosophy and treatment and/or areas of interest to clinicians working with individuals with neurological impairment.The purpose of a demonstration poster is to report a clinical observation, present colleagues with a new idea ordescribe your unique clinical service.
Guidelines for Poster Presentation Submission:
1. COMPLETE THE SUBMITTING AUTHOR INFORMATION:
Name: __________________________________________________________________________________________
Address: ________________________________________________________________________________________
City, State, Zip Code, Country: ______________________________________________________________________
Telephone: __________________________ Fax:: ________________________ E-mail: __________________________
Title of Research _________________________________________________________________________________
Call for Research Posters
THE RELATIONSHIP OF HAMSTRING SPASTICITY & CONTRACTURE TO GAIT IMPAIRMENT IN CHILDRENWITH SPASTIC DIPLEGIA. Glock E., Yoloho E., Physical Therapy Program, Young University, Pungo VA.
PURPOSES: The purposes of this research were to determine the: 1) reliability of hamstring spasticity meas-urements; 2) reliability of popliteal angle measurements; 3) relationship of hamstring spasticity to step length,stride length & gait velocity; 4) relationship of hamstring contracture to step length, stride length & gaitvelocity. SUBJECTS: Eleven children (8M/3F) with spastic diplegia (ages 3-15 yrs) were studied. Allwalked independently with or without appliances. METHODS: Two raters twice graded hamstring spas-ticity in both legs of subjects using the modified Ashworth scale while subjects simulated the Terminal Swing(TSw) Phase position in standing. Raters twice goniometrically measured subjects popliteal angles in thesupine position. Each subject walked 20í with inked shoe pads to determine stride & step length distances.Gait velocity was determined using a stopwatch. DATA ANALYSIS: Intraclass correlation coefficients (ICC)and percent of agreement (0-100%) were used to determine the reliability of intrarater & interater meas-urements of spasticity and popliteal angles. Speanean rank correlation coefficient was used to assess therelationship between spasticity & gait, and between hamstring contracture & gait. RESULTS: Intratesterreliability for hamstring spasticity measurement was fair (.487) to good (.941); intertester reliability waspoor (.242) to fair (.613); the percent of agreement ranged from 0% - 10%. The reliability of poplitealangle measurements was good (.884) to high (.962). Negative correlation between hamstring spasticity& gait measurements was poor (.305) to fair (.431) on the right side, and moderate (.564) to good (.877)on the left side. The Pearson product moment correlation coefficients between hamstrings range (poplitealangle) & gait were moderate (.685) to good (.840). Correlation of hamstring range with Terminal SwingPhase gait was significant at the .05 level. CONCLUSIONS: The reliability of spasticity measurements wasvariable, and the relationship of spasticity to gait was equivocal with respect to the right and left sides. Mea-surements of hamstring range were reliable, and there was a significant relationship between hamstringrange of motion and swing-phase gait. RELEVANCE: Reliable examination procedures are required to as-sess patient impairments and their impact on functional movement. Assessment of the efficacy of treat-ment on patient functional outcomes requires the heath care provider to analyze the relationship betweenmeasured impairments and measured functional performance. ACKNOWLEDGEMENT: This researchwas supported by Grant No 652 awarded by Young University, Pungo, VA.
S A M P L E A B S T R A C T
SAMPLE
SUBMISSION DEADLINE:JULY 31, 2005
C A L L F O R P O S T E R S
6 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S

‘m pleased to be able to share with
Network readers the Neuro-develop-
mental Treatment (NDT)–based therapy
we provide in our KIDS+ program, which
we run through our therapy practice,
Children’s Therapy Services, in Geelong,
southern Australia.
My initial ideas for KIDS+ resulted from
observations and learning at the various
facilities I attended in the United States
while training to become an NDTA OT
Instructor. I worked with a number of
extraordinary therapists and my obser-
vation of the power of NDT was reinforced
through the remarkable results achieved
by my mentor and friend, Regi Boehme, in
her sessions with children both in the U.S.
and as she travelled and taught in Australia.
I was inspired, to say the least, and worked
towards the creation of the KIDS+ program
together with my physiotherapist practice
partner and later our associate speech
pathologist. This article is based upon a
publicity document written for pediatri-
cians in our region.
The KIDS+ program provides specialized
therapy programs for children (0-18 yrs
old) with neuro-developmental disabilities,
including children with cerebral palsy, brain
injury, and stroke. The overall objective is
to increase the participation of these
children in daily life, including their roles in
family and societal settings such as
preschool and school (ICF 2001).
We started KIDS+ at Children’s Therapy
Services in 1997. It incorporates PT, OT, and
SLP. The program was initiated in response
to parents’ wish for a more intensive, regular
therapy service, due to the diminishing
frequency of pediatric therapy available for
these children in our region.
The program is essentially a number of
‘mini’ intensive group-therapy sessions. Each
of three children has a therapist – PT, OT,
or SLP (or co-treatment by two therapists)—
for each session. They therefore receive the
individual goal-based therapy they require,
while also receiving some of the positive
attributes of a group setting, such as simi-
larly aged children joining in for play and
socialization and parent-to-parent contact
and support available within each session.
PROGRAM STRUCTURE
Currently 27 children attend sessions. The
program is held over a day and a half per
week and runs for an eight to nine weeks
block, four terms per year. Children are
chosen for each treatment block according to
certain selection criteria, which includes
parents’ preferred duration of involvement.
In each 11/4 hour session we have the time to:
• Review parents’ comments about progress
• Address parents’ session goal choice (of the
current 2-4 goals each child has)
• Utilize Neuro-Developmental Treatment
(NDT) strategies towards goal achievement
• Address ‘carryover’ ideas as requested by
parents
• Document the outcome of each session and
plan for the next
• Offer support and advice on new issues
which may have arisen
• Review goals and outcomes for the
treatment block at the last session and
begin to plan for future goals with parents
SETTING FUNCTIONAL MEASURABLE GOALS
These may be related to communication;
postural control/mobility; leisure skills; self-
care, including eating/drinking; and hand
skills for play/classroom tasks.
Examples:
• An eight year old boy stepping up one
step to be able to use the toilet himself.
• A baby learning to hold and drink from
a bottle
• A six-year-old girl moving from a seated
position to a standing position to walk 10
steps with a walker as needed in a
classroom setting
• A teenager working on speech clarity
and volume to read out project material
to a class
• A two-year-old learning to move his
hand to activate a toy switch
• A seven-year-old utilizing a communi-
cation device to communicate
Children attending KIDS+ may have appar-
ently “mild” functional limitations, such as
difficulty with manipulation skills; oral motor
control issues, such as saliva control; or higher
level balance skills, such as required in team
ball games. Severity of disability progresses to
children who have no independent mobility,
verbal communication, or grasp.
TREATMENT
The underlying treatment approach used in
the KIDS+ program is Neuro-Developmental
Treatment, which was initially developed by
Dr. and Mrs. Bobath in the U.K. It is an
advanced therapeutic approach practiced by
experienced occupational therapists, physical
therapists, and speech-language patholo-
gists. This “hands-on” approach is used in
working with children who have central
KIDS+A PEDIATRIC NDT PROGRAM IN AUSTRALIA
By Kate Bain, OT
N D T W O R L D W I D E
N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 7
I

nervous system (CNS) insults which have
resulted in difficulties with posture and
movement (NDTA Web site ’03).
Therapists using NDT treatment have
completed advanced training in Bobath/NDT.
As the PT and OT in the KIDS+ program,
we are also the Australian Bobath/NDT
Instructors qualified respectively in the U.K.
and U.S. We also attended the NDTA
Advanced Baby Course, taught by Suzanne
Davis in Melbourne in 2001.
We work closely with children, helping
them to become as independent as possible;
we also work collaboratively with family,
caregivers, and physicians in the ongoing
development of this comprehensive
treatment program.
Our focus is firstly on the strengths and
abilities of each child related to the specific
goal/skill identified. The impairments that
a child may have in relation to that goal or
skill are then assessed, using task analysis to
identify the system impairments impeding
that child from achieving his or her func-
tional goal. Formal assessment tools, such
as the PEDI (Haley et al 1992), GMFM
(Russell et al 2002), and The Melbourne
Assessment of Unilateral Upper Limb
Function (Randall et al 1999) are also used
to measure changes in function over time.
Examples of systems impairments related
to tasks:
• Insufficient length in muscles, such as hip
adductors/ internal rotators for climbing on
playground equipment
• Reduced range of active reach—for
example, arms above head to comb hair,
or reach forward to a tap
• Low tone/weakness in jaw musculature for
chewing
• Inability to adequately coordinate head and
eye movements to watch a film at the theatre.
• Distal neuromuscular/biomechanical
dysfunction—e.g., pre-shaping of hand for
picking up a spoon, or coordination of a
dynamic tripod grasp for writing
• Inability to vocalise during parallel play
at childcare
• Insufficient strength, for example, to lift
foot to hand to put on shoes for PE
• Inability to weight shift the trunk/pelvis
within the task to free another part of the
body for mobile function, for example, to
wipe bottom
• Insufficient endurance to pedal a bike
around the preschool path
This analysis and treatment approach
follows a “top down” processing model that
always proceeds from the child’s current
performance in the task/goal.
NDT treatment is guided by a number
of theoretical models for motor control,
including:
• Neuronal Group Selection Theory:
addressing the selection and fine tuning
of functional CNS neuronal groups
• Dynamic Systems Theory: addressing
the functional linkages between systems
in task performance, e.g., between the
neuromuscular, biomechanical, and
sensory systems in a given task, such as
visually guided reach and grasp (Bern-
stein 1967 cited in Howle 2002). The
treatment strategies used within a KIDS+
session address impairments through the
relevant systems.
Examples of treatment strategies related
to system impairments:
• Elongation of muscle groups/soft tissue for
joint alignment, such as hamstrings, or
the latissimus musculature, to increase
range of movement for dynamic control of
the pelvis in floor sitting
• Facilitation of weight shifting, which may
combine with these approaches, as required,
for example, in transitional movements
required to get up from the floor
• Treatment strategies to improve lip closure
for saliva control and swallowing, such as
resistive activities utilizing musical
blowing toys
• Systematic desensitization of tactile hyper-
sensitivity in hands; for example, using hand
sized toys which also develop dynamic
palmar control. Both treatment strategies
support manipulation with hands.
• Strengthening of hip and knee extensors
for stepping
• Dynamic weight bearing through upper
extremities in play in prone to increase
coactivation in shoulder girdle muscu-
lature, and in turn, for improved control
in targeting and timing during wide range
reaching
• Traction and vibration through the ribcage
to increase respiratory volume for breath
control and phonation
• Stimulation techniques to improve head
raising and vision for “looking play”; for
example, using linear vestibular movement
and/or light intermittent compression to
the head, aligned in midline.
Playfulness and “child lead” involvement
in an enriched treatment environment is
integral to every NDT session to maximize
motivation, self esteem, and encourage
learning to occur.
Other theoretical underpinnings to NDT
include knowledge from motor development
and motor-learning theories, sensory inte-
gration theory, biomechanics, neurophysi-
ology, and pathophysiology. An example of
applied motor-learning theory is the
necessity of independent practice by children
in order to consolidate and generalize goals
in their natural environments. Contextual
factors related to these environments are
taken into account, and practice opportu-
nities are given within each session to
strengthen the child’s skill within the task.
Fellow team members, such as childcare and
pre/school integration aides, are invited into
8 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
N D T W O R L D W I D E

N D T W O R L D W I D E
N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 9
sessions. Therapists visit these settings out
of the program, when possible.
Treatments are also planned within a
framework of family-centred practice (King
2002). Parents are always asked in KIDS +
sessions about aspects they wish to learn to
practice or carryover into home settings.
Examples of further practice through
home programs which are considered
compatible with family-centred practice:
• Playful lengthening/“massaging” interactions
at care times, such as nappy change time
• Rough-and-tumble strengthening play
• Books and songs
• Riding a scooter or bike
• Undressing at bath time
• Use of vertical surfaces–blackboard,
fridge–sibling involvement
• Swimming
• Eating – finger foods/using cutlery, drinking
from a cup
EVIDENCE BASED PRACTICE
Research by Knox and Lloyd-Evans in 2002
showed significant improvements occurred
in the self-care domain, as rated on the PEDI,
by a group of children who had undergone
Bobath Therapy. Examples of improvements
among the children were increased inde-
pendence in self dressing and personal
hygiene, such as grooming, and bathing. In
addition there was a significant decrease in
caregiver assistance required for transitional
movements, locomotion indoors and
outdoors, and in managing stairs.
Adjunct therapies such as the use of spe-
cialized equipment,post-botox programming,
orthotics, and constraint induced (CI) thera-
py may also be used in conjunction with KIDS+
sessions to maximize function.
Other treatment frameworks, such as
cognitive behavioral approaches, are often
incorporated with NDT as necessary.
A few further comments about KIDS +:
• With parents’ permission regarding confi-
dentiality, we are happy to work closely
together with other agencies and thera-
pists. This includes sharing goals and
outcome reports and including other
therapists in our sessions.
• Case management can be arranged with
families.
• Parent evaluations guide us in program
development.
KIDS+ also incorporates a separate resi-
dential Farm Treatment Program. This is an
intensive therapy program which we have
held on a number of occasions, for 2 – 3
days with families who live in the country
and are unable to attend weekly therapy. It
is based on a program I attended which was
run by Regi Boehme for families at “The
Center” in Montana. In place of the beautiful
deer which ran through the mountains on
the Boehme’s ranch, the children here in
Australia see kangaroos in the bushland and
help to feed farm animals as their families
combine a holiday with therapy. This
program currently awaits funding, as below,
and will then continue.
This year, another long-held wish came
to fruition: funding of families for the weekly
KIDS+ program. This was driven by parents
and resulted in the formation of the KIDS
Plus Foundation, which has deductible gift
recipient and income tax exempt charitable
status (www.kidsplus.org.au). It is run by
an energetic and enterprising co-ordinator
and Board of Directors, who continue to
oversee the smooth running of the program.
It fully funds 27 families, both current and
future, to receive the therapy they are seeking
for their children. ■
Kate Bain OT, is an OT NDT Instructor
(U.S.A) and partner in Children’s Therapy
Services in Geelong, Australia. She can be
reached at [email protected].
REFERENCES:
Erhardt, Rhoda P. (ed.). (1999) Parent Articles
about NDT. Therapy Skill Builders: Tucson,
Arizona.
Haley S M, Coster W J, Ludlow L H, Halti-
wanger J T, and Andrellos P J. (1992). Pedi-
atric Evaluation of Disability Inventory:
Development, Standardization, and Admin-
istration Manual, Version 1.0. Boston, MA:
Trustees of Boston University, Center for
Rehabilitation Effectiveness.
Howle J. in collaboration with the NDTA
Theory Committee. (2002) Neuro-Develop-
mental Treatment Approach Theoretical Foun-
dations and Principles of Clinical Practice NDTA.
ICF (2001) Disability–International
Classification of Functioning,Disability and Health
www.aihw.gov.au/disability/icf/index.html. World
Health Organization.
King G. (2002) Family-Centred Service:
Concepts, Measurement, and Implications
AusACPDM Sydney, Sept.
Knox V and Lloyd–Evans A. (2002) Evalu-
ation of the Functional Effects of a Course
of Bobath Therapy in Children with Cerebral
Palsy: A Preliminary Study. Dev. Med. &
Child Neurology, 44: 447-460.
NDTA Web site Neuro-Developmental
Treatment Association (NDTA–USA).
www.ndta.org
Randall MJ, Carlin J, Reddihough DS,
Chondros P, Randall MJ, Johnson LM,
Reddihough DS. (1999) The Melbourne
Assessment of Unilateral Upper Limb Function
Test Administration Manual. RCH
(Melbourne).
Russell D, Rosenbaum P, Avery L, and Lane
M. (2002). The Gross Motor Function
Measure (GMFM-66 & GMFM-88) User’s
Manual Clinics. Developmental Medicine No.
159. Published through Mac Keith Press in
the U.K. and distributed through Cambridge
University Press.

the internal rotation and pronation attitude, with the thumb fol-
lowing along in the pattern by flexing, adducting and pronating
in towards the palm. The adducted thumb position consequently
leads to tightness in the soft tissue connecting the thenar at the
palm at the carpal transverse arch, and narrowing of the palm.
There is an impact on the web space where the lack of soft tissue
flexibility limits active expansion and results in a loss of range of
motion in the thumb. In addition, the tightly adducted thenar
eminence precipitates hyper-extension at the CMC joint during
attempted use, and the thumb is unable to move towards antepo-
sition, which is the movement that makes it functional in opposi-
tion of the fingers. The neurological impact may also lead to dif-
ficulty with accessing selective motor control and differentiation
of movement of the thumb away from the hand and in function-
al ranges opposing the fingers.
Clinically, treatment and orthotic management of thumb is
critical to the ability to functionally use the hand and is key to the
reduction of the impact of tone throughout the upper extremity.
Thumb alignment and function is an ongoing challenge and con-
cern for all therapy disciplines. The thumb position effects the
overall efficiency of hand use in activities of weight bearing, gross
grasps (as needed for transitions on the floor and use of mobility
devices), selective use of other fingers of the hand (such as point-
ing the index finger for augmentative communication), and
development or use of a variety of refined grasps and complex
manipulation strategies (as are needed for all activities of daily
living and writing skills). To best understand treatment strategies
and the types of splints that are effective, it is first important to
understand the structural design, muscular components, and
active movements of the thumb.
THE THUMB AND WEB SPACE
Skeletal/Structural Considerations
The thumb emerges from the palm wedge as a narrow triangular
block supported from underneath by the fleshy curved thenar
eminence. The first web space is created by a triangular connec-
tion of soft tissue on the ulnar aspect of the thumb and the radi-
al aspect of the index finger. The web space between the thumb
and the index finger is designed by the long bone of the thumb
between the carpalmetacarpal joint (CMC) and the metacarpal-
phalangeal joints.
Thumb movement is much greater than that of the fingers
because of the attachment of the first metacarpal to the trapezi-
um bone by a capsular ligament only, which allows much wider
excursions in movement than the other four. The saddle-shaped
trapezium bone of the carpal (wrist) bones articulates with the
first metacarpal of the thumb. The saddle-shaped joint is signifi-
cant in that it allows good range of motion in many directions
and movement in two planes, sagittal and frontal. The
metacarpalphalangeal I (the thumb) also differs from II through
V in these other ways: more massive, capsule not as taut laterally,
and there is available axial rotation. Two small bones known as
the sesmoid bones are imbedded into the palmar fascia of the
thumb and serve for tendon attachment—again allowing for
much more range of motion.
Muscle Attachments/ Kinesiological Components
The muscles that move the various articulations of the thumb ray
increase in number in proportion to the planes of movement of the
joints they mobilize (Tubiana 1984).
The muscles responsible for movement of the thumb include:
Extrinsic: The long muscles of the thumb. Anterior: tendon of
long flexor. Posterior: tendons of the long abductor, the short
extensor, and the long extensor
Intrinsic: The thenar muscles: the adductor and the first dorsal
interosseous muscle. The thenar muscles also act together with
the flexor pollicis longus to flex the proximal phalanx.
The muscles responsible for the opening up of the first web
space are:
• Extrinsic: long abductor and short extensor
• Intrinsic: short abductor and opponens
The thenar muscles form a cone whose summit is the base of
W E B T A P I N G
1 0 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
(Management of Web Space continued from page 1)
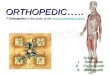
Above: External Thenar Muscles: (1) Abductor pollicis brevis (2) opponenspollicis (3) flexor pollicis brevis. Internal thenar muscles: (4) oblique head ofadductor (5) transverse head of adductor. (Adapted from Tubiana, Raoul.)
INTRINSIC MUSCULATURE OF THE THUMB

W E B T A P I N G
N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 1 1
the proximal phalanx (Tubiana 1984). These muscles can be
divided into two groups to differentiate their contributions to
functional components of grasp.
1. External thenar muscles: abductor pollicis brevis, opponens,
and flexor pollicis brevis
• Innervated by median nerve, and attach to sesamoid
bones
• Functional contribution is circumduction
• They are pronators
2. Internal thenar muscles: oblique and transverse heads of the
adductor, first palmar interosseous muscle
• Innervated by ulnar nerve
• Functional contribution is to bring thumb metacarpal toward
index metacarpal at end of opposition, and to reinforce
• They are supinators
Movements of the Thumb
Terminology used to describe the movements of the thumb is
complex and may vary between authors, researchers, and clini-
cians. In the thumb, the multifaceted nature of the angles of
alignment afforded by the saddle joint and loosely strung tendon
structure provide the basis for movement into more than one
plane of movement at a time. In describing movements, we need
to designate a point of reference. There are actions associated
with the accepted physical planes of movement, namely: flexion
and extension in the sagittal plane, abduction and adduction in
the frontal plane, and rotation in the coronal plane.
Describing movements becomes tricky because the point of
reference, or starting point for opposition of the thumb to the
palm and to each finger involves an angle of circumduction (or
the angle of spatial rotation) formed by the intersection of two
planes (Tubiana 1984).
In clinical practice, it is not often important for us to measure
precise angles of separation, but it is important to have terminol-
ogy to describe consistently the movements that we observe and
effect through our intervention. The terminology which best pro-
vides the clinician with descriptions of movement of the thumb
metacarpal as it applies to function includes in the frontal plane
adduction (or flexion-adduction), and abduction (or extension-
abduction). Positions of the thumb in the sagittal plan are best
described as anteposition and retroposition. The movement car-
rying the thumb ray into anteposition is accompanied by internal
rotation (pronation) of the thumb. The movement of the thumb
ray into retroposition is accompanied by external rotation
(supination). This has been described as automatic longitudinal
rotation (Kapanji 1972).
Opposition is a combined movement which involves all three
segments of the thumb. The metacarpal segment moves into
anteposition, and then in adduction, a movement that is accom-
panied by automatic longitudinal rotation into pronation. The
proximal phalanx flexes, pronates, and radially deviates. The dis-
tal phalanx flexes to variable degree and this is accompanied by
some degree of pronation relative to the demands of the grip.
There is not one opposition, but a whole range of oppositions
which allows for a wide variety in grips (Tubiana 1984).
Treatment of the Thumb/ Web Space
Treatment of the thumb and web-space begins with recognizing
the relationship of the hand to wrist position and ranges of move-
ment, forearm position and its available mobility into ranges of
pronation and supination, elbow range and graded control into
ranges of flexion and extension, and shoulder girdle stability. The
range and control of reach is related to the integrity and selective
movement control of proximal joints. The orientation of the
hand in space is most naturally and smoothly led by the move-
ment of the thumb, which facilitates the rotation through the
forearm into ranges of pronation and supination. In the follow-
ing focus on treatment and orthotic management of the web
space and thumb, the influence of the upper extremity is also
assumed and acknowledged.
Treatment of the hand for improved web space mobility and
soft tissue extensibility begins with addressing the palmar intrin-
sics with strategies to get width across the palm and into the lon-
gitudinal arches. The carpal transverse arch at the base of the
palm creates the connection horizontally between the thenar and
hypo-thenar. The characteristic flexion-adduction position of
the thumb assumed in tight and fisted hands limits expansion
and width within the palm across this arch. The oblique arches
are important to address as well: they often lack any presence in
Above: (1) Oblique adductor pollicis (2) Transverse adductor pollicis (3)First dorsal interroseous. (Adapted from Tubiana, Raoul.)
LATERAL VIEW OF THE THUMB WITH THE THUMB
IN ANTEPOSITION

a tight hand, especially in situations where the neurological dam-
age is from birth as opposed to being acquired. The oblique arch-
es are used in opposition of the thumb to each finger. Clinically
we know that slow, deep input can be inhibitory and relaxing. In
approaching the arches of the hand in treatment, it is beneficial-
ly to use a constant, deep input and move into an expanded arch
formation during lengthening strategies (Boehme 1988).
One suggested strategy specific to the web space, following gen-
eralized opening of the hand through expansion across the trans-
verse arches, is for the clinician to
encircle the long bone of the thumb
with her hand and to move it into
abduction and extension while using
the thumb and index finger of her
other hand to sink deep into the apex
of the triangle of the web space. Deep
input and gentle oscillations help to
relax the tension and to effect actual
change in the length of the tissue.
Following this strategy up with
widening of the hand through the
oblique arches, and gradually moving
the thumb into ante-position pre-
pares the alignment and extensibility
of the web space and affords the pos-
sibility of moving the thumb into
positions of opposition in relation-
ship to palm and fingers.
In addition to addressing align-
ment and elongation of tissue, treat-
ment strategies should include weight
bearing over a contoured surface (or
different sized contours) and presen-
tation of functional activities to facil-
itate active use of thumb to palm and
fingers. It is at this point the clinician
is wise to begin thinking about use of
a splint or taping techniques to main-
tain the benefits achieved by the active
hands on strategies.
THUMB/WEB SPACE MANAGEMENT THROUGHSPLINTING AND TAPING
Static Splints
In some instances in the progression of treatment, choosing to
immobilize the thumb by using a static orthosis or splint is an
appropriate choice. The immobilization of joints in positions of
newly achieved range of motion is important if the individual is not
able to immediately call into functional all use of the available range.
In this instance, the static splint may be put on with a variable wear
schedule and removed for practice and exercise. Another reason to
choose immobilization is to assure maintenance of full available
range for an individual whose limitations in accessing muscle con-
trol—secondary to severity of neurological damage—are so great
that there is little or no potential for them to do so.
Static splinting does not always
mean full immobilization, however.
The use of static splinting to immo-
bilize one or more joints encourages
more efficient practice of distal joint
function upon a base of good align-
ment and can facilitate the emer-
gence of grasp patterns. Some exam-
ples of customized static splints that
immobilize the CMC joint of the
thumb and support width in the web
space are: 1) Thumb MP
Immobilization Splint, 2) CMC
Immobilization Splint, 3) Thumb
CMC Immobilization Splint, and 4)
Thumb Abduction Immobilization
Splint (Jacobs & Austin 2003). These
splints are named for the joints that
are incorporated into the splint and
will take on a slightly unique form
each time they are customized to an
individual, depending on the choic-
es of splinting materials and strap-
ping methods.
Pictured here are customized splints
designed by this author, each for a
unique purpose. The Palmar Web
Splint, Figure 1, is helpful in maintain-
ing the web space as well as encourag-
ing the support of the width of the
palm in wide transverse arches.
The CMC/MP Web Splint in Figure
2 & 3 immobilizes the CMC and MP of the thumb while maintain-
ing a wide web space. The special functional feature of this particu-
lar splint is that it is designed to position the pad of the thumb in
opposition of the pads of the index and third finger. The CMC/MP
Web Splint is great for providing stability to the base of the thumb
W E B T A P I N G
1 2 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
F I G U R E 1
F I G U R E 2
F I G U R E 3
Palmar Web Splint
CMC/MP Web Splint
CMC/MP Web Splint

W E B T A P I N G
N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 1 3
and web space, and encouraging prac-
tice of functional digital grasps.
A variety of commercially available
splints provide wrist and thumb sup-
port. Some of the name brands
include Comfort Cool, Liberty,
Thermo-Form, and Otto-Bock, and
Benik. These options are available in
catalogs such as North Coast Medical
and Sammons Preston Rolyan, or
directly from the company named.
Semidynamic Splints
Semidynamic splints position and
support the hand and/or wrist for
optimal function, but do not neces-
sarily immobilize any particular joint.
Clinicians generally use material such
as Neoprene or “Fabri-foam” to
design these splints. Many of the soft
splints that are commercially avail-
able can be classified under this cate-
gory. Examples of such splints include
a variety of splints from a number of
different companies, most of which
are available through professional
rehabilitation catalogs or from the
companies that created them. The
Benik Company makes splints out of
neoprene material, some of which are
designed to support the thumb web space, and there are modifi-
cations that take the support across the wrist as well. Benik offers
a pediatric sizing kit for purchase to help with ordering the cor-
rect size to fit. Neoprene, on its own, at times is not enough to
hold the web space of a tight hand; therefore, using a low-temp
plastic to customize reinforcement is usually a good idea.
The Joe Cool Splint is another web space/thumb support
option, also made out of neoprene. This company sells a splint
that is called a thumb splint, and one that is called a glove which
supports the long bone of the thumb, as well as providing some
input to the webspace. A variety of other splints in this category
are commercially available through the catalogs noted above, or
directly from the company that holds the trademark for the
design, such as the McKie Splint.
The splint in Figure 4, designed by this author, is named The
Peanut. This splint is very versatile
and can be secured with strapping or
used in combination with a neoprene-
type splint. The benefit of The Peanut
is that it supports the width of the web
space while not interfering with opti-
mal mobility of the thumb joints. The
strapping options are numerous, and
depending upon the direction of pull,
can include support for the carpal
transverse arch or oblique arches.
Taping for support and to prevent
collapse of the web space is another
option that offers lots of possibilities
for dynamic support and does not
interfere with functional use of the
hand. Taping can facilitate function, as
well. Tape can be applied directly at
the webspace on the hand to encour-
age maintained width and efficient
thumb alignment, and also can be
used to facilitate the use of thumb
and/or wrist extensors by following
the muscle groups into the forearm.
Figures 5 and 6 show one way tape can
be applied to support web space width
and carpal arch formation.
The different types of tape available
each offer different properties. The
choice of which tape to use and when
is generally left up to clinical judgement. Courses are available for
continuing education credits that provide clinicians with guide-
lines for use of tape, contraindications, and precautions. Some of
the brand names of tape typically used therapeutically are:
Coban, Kinesiotape, and Leukotape.
Understanding the unique structural aspects of the thumb joint
and all the movement that it affords is essential in treating the
thumb and the web space through splinting. Inhibition of tight-
ness includes addressing soft tissue extensibility, joint range of
motion, and achieving maximal alignment through use of
orthotics or taping. Improved hand skill can be achieved by focus-
ing on the alignment of the thumb towards abduction-extension,
with maximum function obtained through approximating func-
tional ranges in anteposition, which is necessary for the use of
thumb opposition. ■
F I G U R E 4
F I G U R E 5
F I G U R E 6
The Peanut
Tape
Tape

W E B T A P I N G
1 4 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
Bonnie Boenig, M.Ed, OTR/L, is an NDTA occupational therapy
instructor. She is in private practice and also a clinical specialist for
Lifeworks of Southwest General Health Center in Middleburg Heights,
Ohio. Easy-to-use kits of the customized splints featured above are
available for on-line purchase through boenigwork@ aol.com.
REFERENCES:
Alexander, R, Boehme, R, Cupps, B. (1993). Normal Development of
Functional Motor Skills. San Antonio, TX.: Therapy Skill Builders.
Boehme, R. (1988). Improving Upper Body Control. Tuscon, AZ:
Therapy Skill Builders.
Calis-Germain, B. (1993). Anatomy Of Movement. Seattle, WA :
Eastland Press.
Case-Smith, J. and Pehoski, C. (1992). Development of Hand Skills
in the Child. Rockville MD.:AOTA, Inc.
Cech, D. and Martin, S. (1995). Functional Movement Development
across the Life Span. Philadelphia, PA., W.B. Saunders Company.
Erhardt, R. (1982). Developmental Hand Dysfunction. Laurel, MD:
RAMSCO Publishing.
Gowitzke, B, and Milner, M. (1980). Understanding the Scientific
Bases of Human Movement, 2nd Edition. Baltimore, MD: Williams
and Wilkins.
Henderson/Pehoski. (1995). Hand Function in the Child. St. Louis,
MO: Mosby Publishers
Hogan, Laura and Uditsky, Tracey (1998). Pediatric Splinting
Selection, Fabrication, and Clinical Application of Upper Extremity
Splints. San Antonio, Texas. Therapy Skill Builders.
Hogarth, B. (1988). Drawing Dynamic Hands. New York, NY.
Watson-Guptill Publications.
Howle, J. (2002). Neurodevelopmental Treatment Approach
Theoretical Foundations and Principles of Clinical Practice.
California: NDTA Association.
Jacobs, MaryLynn and Austin, Noelle (2003). Splinting the Hand
and Upper Extremity. Baltimore, MD: Lippincott Williams and
Wilkins.
Jenkins, D. (1998). Hollinshead’s Functional Anatomy of the Limbs and
Back, Seventh Edition. Philadelphia, PA: W.B. Saunders Company.
Kapanji, I. (1982). Upper Limb. In The Physiology of the Joints, Vol
1. New York: Churchill Livingstone.
Kase, K, Hashimoto T, and Okane T. (1998). Kinesio Taping Perfect
Manual. Kinesio Taping Association: Universal Printing and
Publishing, Inc.
Kendall, F, McCreary, E, and Provance, P. (1993). Muscles Testing
and Function, 4th Edition. Baltimore, MD: Williams & Wilkins.
Netter, F. (1995). Interactive Atlas of Human Anatomy. Summit, NJ:
Ciba-Geigy Corporation.
Ryerson, S. and Levit, K. (1997). Functional Movement Reeducation.
Philadelphia, PA: Churchill Livingstone.
Tubiana, R.(1984). Examination of the Hand & Upper Limb.
Philadelphia, PA:W.B. Saunders Co.
1. Benik Corporation 11871 Silverdale Way NW, #107 Silverdale,WA
800/442-8910 • www.benik.com
2. Boenig Workshops and Consultants, Inc.P.O. Box 87, Berea, Ohio [email protected]
3. Joe Cool Company9448 Dove Lane South Jordan, Utah
Phone: 800/233-3556 • www.joecool.com
4. McKie SplintsP.O. Box 16046, Deluth, MN 55816Phone: 888/4SPLINT (477-5468)
www.mckiesplints.com
5. North Coast Medical Hand Therapy Catalog
Phone: 877/213-9300 • www.ncmedical.com
6. Sammons Preston RolyanPO Box 5071
Bolingbrook, IL 60440Phone: 800/323-5547
www.sammonsprestonrolyan.com
SPLINTING MATERIALS RESOURCES:

N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 1 5
y name is Terri Lynn Hinson and I am 22 years old. I am
a senior at McGavock High School in Nashville, Tennessee.
I was born with cerebral palsy on November 13, 1982 and was
on life support for three months. They didn’t think that I would
live (I weighed just 2 lbs., 9 oz.). I was adopted by my grand-
parents, Ellen and Billy Hinson. I am so thankful that they took
me in as their own child.
I started school when I was 13 months old. When I was three
years old I started using a communication device with a head stick
called a Light Talker [manufactured by Prentke Romich]. I was
very excited about using a communication
device because I like to carry on conversa-
tions with people.
When I was five I was the Clinic Bowl
Child to raise money for Vanderbilt
University. They had a dinner for the Junior
Chamber of Commerce to introduce me to
them. I said the Pledge of Allegiance on my
Light Talker. When I was six, I was on
Channel 4. They had a story about children
using speaking devices.
I used a head stick for a long time. My speech pathologists,
Cathy Lackey and Colleen Hatcher at Vanderbilt University,
worked with me weekly for many years. When I was in the second
grade I had hip surgery. I was in a body cast and couldn’t use my
head pointer. Mom and I worked for six weeks to learn to use
my hands on the Light Talker.
The Light Talker didn’t have as many sentences on it as I wanted,
and I couldn’t store sentences in it. I was 11 years old when I got
my Liberator communication device [made by the Prentke Romich
Company], which has a large vocabulary. It was easier for me to
communicate because I could make up my own sentences. My
Liberator also has a printer on it.
When I was 11 years old I was a cheerleader for the Donelson
Warriors. We went to a compe-
tition at DuPont High School.
Leslie Gregg was our cheerleading
coach, and we worked out a
routine around me using my
Liberator. The dance was called
“Rock Around the Clock”. I was in the middle and they cheered
around me. We came in second place. Cheerleading was a wonderful
experience because I felt like I had really achieved something in
my life and I made friends.
Also when I was younger, our class at
school was asked to be special guides at the
Hermitage (Andrew Jackson’s home). We
had to dress in old dresses. We programmed
a greeting to the visitors and I sat beside a
portrait and had to say something about
the picture
When Al Gore was running for Pres-
ident I got to go to the Opryland Hotel to
meet him.
In my Life Skills class at school, and at nursery schools and nursing
homes when we go to work, I have used my Liberator and Pathfinder,
which has picture words in it for things like,“It’s nice to meet you,”
and “What’s up?” The children would go home and tell their parents
that they met a girl who talks with a box! They said that she sings
Christmas carols and nursery rhymes with it.
I started making greeting cards this year with my Pathfinder and the
computer. I have a special mouse. The Pathfinder is my keyboard.
I have lots of friends and I go to church. One friend is Whitney.
She uses a Delta Talker and a power chair like I do. I have another
friend who has cerebral palsy. He is 17 years old. ■
Terri Hinson is a senior at McGavock High School in Nashville, TN.
She can be reached at 615-889-9182.
Finding My VoiceADVENTURES WITH MY COMMUNICATION DEVICES
By Terri Lynn Hinson
PAT I E N T A N D FA M I LY P E R S P E C T I V E
M
I was very excitedabout using a
communication devicebecause I like to
carry on conversationswith people.

N D T N E W S
1 6 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
2005
This exceptional two-and-a half-day conference has been
designed especially for you, the NDT practicing clinician. Mary
Ann Sharkey, PhD., PT will set the conference theme in the opening
general session as she addresses the question: “How Can We
Measure the Effectiveness of NDT in the Clinic?” Fifteen hands-on
facilitation labs based on case-presentations will be presented
by an eminent faculty of NDT Instructors. Other conference
highlights include an Exhibitor Showcase, Panel Presentation,
Roundtable Discussion Session, Networking Reception, Luncheon,
and more…
For more detailed information and to register for the NDTA ANNUAL CONFERENCE,
please visit the Conference Page at www.ndta.org
Lezlie Adler, OTSteve Anderson, PT
Kim Barthel, OTLauren Beeler, PT-CI
Judith Bierman, PT-CILois Bly, PT-CI
Kristine Brandel, PTSuzanne Davis, PT-CI
Monica Diamond, PT-CIKay Folmar, PT-CI
Cathy Hazzard, PT-CIAnn Heavey, SLPKacy Hertz, PT-CI
Therese McDermott, SLPMadonna Nash, OT
Teddy Parkinson, PT-CIMechthild Rast, PhD, OT
Mary Ann Sharkey, PhD, PTBeth Tarduno, OTR
NDTA™ is pleased to announcethe 2005 Conference Faculty:

N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 1 7
FRIDAY, SEPTEMBER 30, 20057:30am – 8:30am . . . . . Continental Breakfast
8:30am – 10:00am . . . . Opening General Session:» Being a Clinical Detective: Clues for Success • Mary Ann Sharkey, PT, PhD
10:00am – 10:30am . . . Break
10:30am – 11:30am . . . Concurrent Sessions:» It’s About Being A Kid • Lauren Beeler, PT, PCS, CI, Kim Barthel, OTR
and Therese McDermott, MHS, CCC-SLP» Adult Case Video Presentations • Monica Diamond, PT, CI and Cathy Hazzard, PT, CI
11:30am – 12:30pm . . . Lunch On Own
12:30pm – 2:30pm . . . . CONCURRENT LABS (PEDIATRIC):» What Goes Up Must Come Down • Lauren Beeler, PT, PCS, CI» Reach For The Stars • Kim Barthel, OTR» That’s What I Was Talking About • Therese McDermott, MHS, CCC-SLP
CONCURRENT LABS (ADULT)» Straighten Up and Fly Right • Cathy Hazzard, PT, CI, MBA and Teddy Parkinson, PT, CI» Alignment & Activation • Monica Diamond, PT, CI and Beth Tarduno, OTR
2:30pm – 3:30pm . . . . . Exhibitor Showcase & Afternoon Break3:30pm – 5:30pm . . . . . Concurrent Labs Repeat6:00pm – 8:00pm . . . . . Exhibitor Showcase & Reception • Staffed Poster Session • Silent Auction
SATURDAY, OCTOBER 1, 20057:30am – 8:30am . . . . . Exhibitor Showcase & Continental Breakfast
8:30am – 10:15am . . . . CONCURRENT LABS (PEDIATRIC)» In Sync: Baby Lab • Lois Bly, MA, PT,CI & Madonna Nash, OTR/L» More To Talk About • Therese McDermott, MHS, CCC-SLP and Kacy Hertz, PT, CI» So Close…Yet So Far Away: The Mildly Involved Child • Lezlie Adler, MA, OTR, FMOT
and Suzanne Davis, PT-CI
CONCURRENT LABS (ADULT)» Problem Solving for Functional Gains with Low Level Adult Hemiplegia •
Steve Anderson, PT and Beth Tarduno, OTR» He’s Walking…Now What? • Kay Folmar, PT, CI and Kristine Brandel, PT
10:15am – 11:15am . . . Exhibitor Showcase & Morning Break11:15am – 1:00pm . . . . Concurrent Labs Repeat1:00pm – 2:30pm . . . . . Networking Luncheon – ‘Meet Your NDTA’
2:30pm – 4:30pm . . . . . CONCURRENT GENERAL LABS» Extreme Make-Over: Clinic Edition • Kay Folmar, PT, CI» Play In The Context Of NDT • Mechthild Rast, PhD, OTR/L» Getting In Touch With Technology • Ann Heavey, MS, CCC-SLP (Moderator)» A Leg To Stand On: Better Stance Makes Things Swing • Teddy Parkinson, PT, CI
and Lauren Beeler, PT, PCS, CI» Let’s Get On The Ball With NDT • Judith Bierman, PT-CI
5:00pm – 10:00pm . . . . Optional Off-Site Event: Carl’s Back Porch
SUNDAY, OCTOBER 2, 2005
8:00am – 9:45am . . . . . Breakfast Roundtable Discussion Session • Mary Ann Sharkey, PT, PhD (Moderator)9:45am – 10:15am . . . . Break10:15am – 12:00pm . . . Panel Discussion • Lezlie Adler, MA, OTR, FMOT (Moderator)
SCHEDULE AT A GLANCESCHEDULE AT A GLANCE

G A I T A N A L Y S I S
tilt, hip, knee, and ankle flexion and extension. Axial or rotational
abnormalities are difficult to quantify by simply watching the patient
walk.Videos taken from the front and the side will aid in this process,
as the video can be slowed or stopped to help with the analysis.
MOTION ANALYSIS LABORATORY
Observational gait analysis is limited in its ability to determine the
biomechanical causes of a patient’s gait abnormality. Although one
can infer causation, without measurements of muscular activity
(dynamic EMG) or kinetics, one can rarely be sure of the etiology
of a problem. For example, a child might have an equinovarus foot.
With observational gait analysis and a good physical examination,
one might determine that there is swing phase varus and
recommend a certain procedure such as a split posterior tendon
transfer. However, the same pattern can be present from other
etiologies, such as tibialis anterior spasticity with a normal tibialis
posterior pattern. The gait lab can provide much more information
(electromyography, force plate, foot pressure, and kinetic data)
which may clarify the picture. It is often difficult in a short clinical
examination to determine the amount of extrapyramidal activity
a patient has (for example athetosis or ataxia). The variability
present in the gait of patients with athetosis, ataxia or dystonia is
much easier to determine with the motion analysis laboratory than
with simple observation.
Kinematics: Kinematics is the portion of the gait study in which
the dynamic range of motion of a joint (or segment) is measured.
When one observes a person walking, rotational abnormalities in
the transverse plane may be confused with sagittal or coronal prob-
lems. For example, a child with severe femoral anteversion may ap-
pear to have increased adduction or knee valgus when viewed from
the front. Three-dimensional motion analysis helps eliminate some
of the ambiguity of visual analysis.
Standardized reflecting skin markers or markers mounted on
wands are captured by CCD (charge-coupled device) cameras while
the patient walks down a walkway in the Gait Lab. [Figure 1] These
cameras are positioned so that three-dimensional analysis of the
data can be performed. The images are processed by a computer to
derive the graphs of the kinematic plots. The same joint range of
motion which one observes on visual inspection is now displayed
with actual numbers and a plotted curve. These can be compared
to age specific norms and different conditions of walking (barefoot,
brace, shoes, etc.) and they can easily be compared to previous gait
studies such as the pre-operative condition. The three-dimension-
ality permits the assessment of dynamic rotational problems which
cannot be observed in a routine manner. Stride-to-stride differ-
ences can be assessed and plotted to determine the variability of
the gait. A patient with an athetoid or ataxic problem will have
marked variability which may be missed in the clinical setting.
Kinetics: Kinetics describe the forces acting upon a moving body.
The resultant joint moments and forces are derived from force plate
measurements and the kinematic data. Also required is anthropo-
metric data (e.g. leg length, foot length, etc.). As the patient walks
through the Gait Lab, her foot strikes one or more force plates. The
transducers are set up such that vertical force, fore-aft shear, medi-
al-lateral shear, and torque can be measured and compared with
norms. When these data are combined with the kinematic and an-
thropometric data, a representation of the force at each joint (joint
moment) can be determined.
Kinetics can be reported as internal moments in which the force
at a joint is assumed to be secondary to muscle activity. Ligament
stretch, joint morphology, contractures, etc. may also contribute to
the moment. Kinetics can also be described as external moments in
which the force acting upon a joint is thought to be a response to
the ground reaction force. Besides the conceptual underpinnings,
the only difference between the two is a positive or negative sign.
1 8 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
(Walking Through the Gait Lab continued from page 1)
F I G U R E 1 Child with markers in motion analysis lab.

G A I T A N A L Y S I S
MUSCLE ACTIVITY IN GAIT
Although the action of the muscles can be inferred from watching
a patient walk, it is often difficult to determine which muscle is
active or inactive during a particular motion. This knowledge may
or may not be very important in determining which therapeutic
intervention will correct the problem. It is critical in helping to
determine which muscles should be used as a “motor” in a muscle
transfer. For example, one may feel that if a patient has an equino-
varus foot deformity, then a split posterior tibial tendon transfer
should be performed to correct it. However, there are many instances
in which there is little or no activity of the posterior tibialis muscle
during the gait cycle in a patient with equinovarus. Other causes
of equinovarus could include an overactive anterior tibialis muscle
or a combination of anterior tibialis and posterior tibialis muscle
overactivity. Fixed hindfoot varus could also be present. In these
patients who have not had dynamic electromyography, the wrong
procedure would have been performed.
Surface or fine-wire electromyograph (EMG) measures the muscle
impulses. When one is interested in group muscle activity, such as
the gastrocsoleus or adductors, then surface electrodes suffice. There
is a problem with “cross-talk” from adjacent muscles, but these
usually do not alter clinical decisions. In deep,
buried muscles (for example, tibialis posterior
or flexor digitorum profundus) fine-wire elec-
trodes must be placed to get any meaningful
information. One must weigh the information
gained from fine-wire EMG data with the
minimal discomfort the patient experiences in
its placement. Young children often are not
able to cooperate with this somewhat techni-
cally demanding procedure.
FOOT PRESSURE
The measurement of pressures of the foot is
helpful in patients who have subtle varus or
valgus foot deformities or in those with
increased pressure at certain points such as a
diabetic or Charcot foot. Not only can this be
utilized to define the problem, this can also
determine if the proposed solution (e.g.
orthotic, shoe modification, or surgery) has
improved the pressure concentration.
Case Example: A four year and five month
old boy with spastic diplegic cerebral palsy
presents with bilateral toewalking and internal rotation of the
limbs. He wears bilateral ankle-foot orthoses but falls up to twen-
ty times per day. He is able to ride a tricycle, can climb stairs and
has an endurance of about one half mile. The experienced referring
orthopedic surgeon thought that he should have bilateral heel cord
lengthenings.
The physical examination demonstrates mild hip flexion con-
tractures and an increase in femoral internal rotation of 70
degrees bilaterally. He has a popliteal angle of 150 degrees (30
degrees) and plantar flexion contractures at the ankle of 15
degrees. He has hyperreflexia and has a positive Ely-Duncan test
suggestive of rectus femoris spasticity.
The kinematic data demonstrated, in the sagittal plane:
increased anterior pelvic tilt, minimal increased flexion of the hip,
diminished and delayed peak knee flexion in swing and a marked
increase in ankle plantar flexion throughout the gait cycle.
Frontal or coronal plane abnormalities included: increase pelvic
obliquity in stance phase and increased adduction throughout the
cycle. Transverse plane abnormalities included: increased femoral
rotation, tibial rotation which followed the femoral rotation and
an internal foot progression angle.
N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 1 9
F I G U R E 2 Preoperative Kinematics.

G A I T A N A L Y S I S
The electromyography data showed full cycle activity of the rectus
femoris but most importantly, increased activity in swing phase;
full cycle activity of the vastus lateralis; minimal but out of phase
activity of the adductors; mostly stance phase activity of the gastroc-
soleus; and full cycle activity of the tibialis anterior.
Based on his physical examination, review of the videotape and
integration of the gait data, the following procedures were recom-
mended: bilateral varus derotational osteotomies of the femurs,
psoas lengthening at the pelvic brim, adductor longus recession,
distal medial hamstring lengthening, rectus to semitendinosus
transfer and Strayer gastrocnemius recession. Although some of
these procedures could have been predicted by a meticulous exam-
ination of the child, not all of them would necessarily be suggested,
such as the rectus transfer based on the kinematic and elec-
tromyographic data.
One year after the surgery, the child was no longer falling, was
playing soccer and learning to roller blade. The kinematic plots
show that the parameters have all returned to near normal.
Practical Uses of the Gait Lab: The most common use for
clinical gait laboratories in the United States is for the evaluation
of children with developmental disabilities, particularly cerebral
palsy and myelomeningocele. These children have very complex
gait problems combined with the underlying neurological insult.
It is often very difficult to completely evaluate these patients in a clin-
ical setting and gait analysis has been very helpful in formulating
treatment plans. DeLuca et al reviewed 91 patients who had rec-
ommendations for surgery from experienced physicians and then
compared the recommendations based on gait analysis. They found
that the addition of gait analysis data resulted in changes in surgi-
cal recommendations in 52% of the patients with an associated re-
duction in cost of surgery, not to mention the impact on the patient
for performing the inappropriate procedure. Kay et al performed
a similar study in 97 patients with an even higher number (89%)
of treatment plan alterations.
The development of new surgical techniques and orthotics have
benefited from research performed in motion analysis laboratories.
There is often a clinical question as to the need for an orthotic and then
to determine the appropriate orthotic. Several studies have evaluated
the efficacy of various orthotics in the management of children with
developmental disabilities. These all have practical applications for
patient management.
SUMMARY
Motion analysis is a diagnostic and outcome research tool which
should be viewed as similar to modern radio-
logic imaging techniques of the musculoskeletal
system. While many and possibly most gait
problems can be evaluated with a systematic
visual inspection and complete clinical evalu-
ation, some problems require some or all of the
components of the modern motion analysis
laboratory. Human gait, with its neurological
control, muscular response, and bone and joint
motion is far too complex for any clinician to
appreciate all of the intricacies with simple
observation. Although an overall idea about the
gait can be obtained in this manner, subtleties
and fine nuances of gait cannot. Gait analysis
provides an objective record of a patient’s gait
before and after therapeutic intervention and
should be considered a vital part of the clin-
ician’s decision making. ■
Hank Chambers, MD, is chief of staff at San Diego
Children’s Hospital and Health Center, University
of California at San Diego. He can be reached at
2 0 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
F I G U R E 3 Postoperative Data.

N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 2 1
CITY KIDS COURSES 20055669 N. Northwest Hwy Chicago, IL 60646 • (773) 467-5669 • www.Citykidsinc.com • E-mail: [email protected]
May 23-27, 2005 • Five Days $700
NDT for SLPs–An Intro Pediatric Course For Non-NDT-Trained Therapists
June 17-18, 2005 • Two Days $300
Two Days in the Mouth-Building Blocks for Oral TreatmentInstructor: Therese McDermott, MA-CCC-SLP
July 17-18, 2005 • Two Days $300
Into The Mouth of Babes-Feeding for BabiesInstructor: Therese McDermott, MA-CCC-SLP
July 22-24, 2005 • Two and a half days $375
Taping For Improved Alignment and Neuromuscular Re-Education–Kinesiotaping Certification CounselInstructor: Trish Martin, PT, Audrey Yasukawa, MOT,OTR/L, CKTI
August 6-7, 2005 • Two Days For $400
Serial Casting and Splinting Techniques: Part II (Practicum)Instructor: Beverly Cusick, MS, PT
August 12-13, 2005 • Two Days For $350
Neuromuscular Electrical Stimulation For ChildrenInstructor: Gad Alon, Ph.D., PT
September 16-17. 2005 • Two Days $300
SI for STInstructors: Madonna Nash OTR/L & Lisa Mesecar MA, OTR/L
September 18-19, 2005 • Two Days For $300
Why Kids Won’t EatInstructors: Therese McDermott, MA-CCC-SLP, and
Madonna Nash OTR/L
October 24-Nov. 11, 2005
$2500/NDT members • $2700/non-members
NDT Approved Three Week Baby CourseInstructors: Lois Bly, PT, Madonna Nash, OTR/L, Kacy Hertz, PT and
Therese McDermott, MA-CCC-SLP
For further information please call Sheila de Armas at 773/467-5669 x150 or fax 773/314-0079.
All 3 courses for
$1200
Bothcourses for
$550

E D U C A T I O N A L O P P O R T U N I T I E S
2 2 • N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S
Upcoming NDTA Inc. Approved Courses
NDT/BOBATH CERTIFICATECOURSE IN THE TREATMENT AND MANAGEMENT OF ADULTS WITH HEMIPLEGIA
Course #: 05A101Dates: 7/21/2005–7/24/2005
8/18/2005–8/21/20059/15/2005–9/18/200510/13/2005–10/16/2005
Location: Asheville, NCInstructors: Kay Folmar, PT, CICathy Hazzard, PT, CIContact: Ron HoechstetterCarePartners: Staff Development Dept.68 Sweeten Creek Rd.,Asheville, NC 28803828-274-9567 [email protected]_______________________________________
Course #: 05A105Dates: 9/21/2005–9/24/2005
9/27/2005–10/1/200511/09/2005–11/12/200511/14/2005–11/16/2005
Location: Columbus, OHInstructors: Marie Simeo, CI, PTPatricia Bonner, OTContact: David Rupp, Ohio Health6200 Cleveland Ave., Columbus, OH 43231614-566-0562 • Fax [email protected]_______________________________________
Course #: 05A108Dates: 8/3/2005–8/14/2005
11/30/2005–12/5/2005Location: San Jose, CAInstructors: Cathy Runyan CI, OTPeggy Miller, PTContact: Recovering Function408-268-3691 • [email protected]_______________________________________
Course #: 05A109Dates: 10/31/2005–11/18/2005Location: Sunrise (Fort Lauderdale), FLContact: Monica Diamond5403 Middleton Dr., Greendale,WI 53129414-421-8427 • Fax 414-421-8429 [email protected]
Course #: 05A110Dates: 10/17/2005–10/28/2005
11/28/2005–12/3/2005Location: Little Rock,ArkansasInstructors: Nicky Schmidt, PT, CI,Pat Bonner, OTContact: Jeana KelleyBaptist Health Rehab. Institute9601 Interstate 630, Little Rock, AR 72205501-202-7598 • Fax 501-202-7141
NDT/BOBATH CERTIFICATECOURSE IN THE TREATMENT ANDMANAGEMENT OF INDIVIDUALSWITH CEREBRAL PALSY
Course #: 05B102Dates: 6/13/2005–6/17/2005
6/20/2005–6/24/20057/8/2005–7/10/20057/22/2005–7/24/20058/5/2005–8/7/20058/26/2005–8/28/20059/9/2005–9/11/20059/23/2005–9/25/200510/17/2005–10/21/2005
Location: Orlando, FLInstructors: Suzanne Davis, RPT ,Lezlie Adler, OTRMonica Wojcik, SLP, Nancy Marin, OTContact: Kris Fought or Irma Rosa–NDT Course CoordinatorsUCP Child Development Centers3305 S. Orange Ave, Orlando, FL 32806321-281-7129 or [email protected] [email protected]_______________________________________
Course #: 05B103Dates: 4/29/2005–5/2/2005
6/3/2005–6/6/20056/20/2005–6/24/20056/27/2005–7/1/20058/5/2005–8/8/20059/16/2005–9/19/200510/21/2005–10/24/2005
Location: Monticello, NYInstructors: Margo Prim Haynes, PT, CI,
Jane Styer-Acevedo, PT, CI,Loren Arnaboldi, SLP, Kate Bain, OTR/LContact: Denita Newsome JohnsP.O. Box 5316, Philadelphia, PA 19142215-815-4880 • [email protected]_______________________________________
Course #: 05B105Dates: 9/15/2005–9/18/2005
10/6/2005–10/9/200512/1/2005–12/9/20051/26/2006–1/29/20062/22/2006–2/26/20063/15/2006–3/19/2006
Location: Cleveland, OHInstructors: Susan Breznak-Honeychurch,PT, CI, Bonnie Boenig, M Ed, OTR,Rona Alexander, PhD, CCC-SLPContact: New Directions @ 710 Associates710 Central Avenue, Dunkirk, NY 14048716-366-2944 • Fax [email protected]_______________________________________
Course #: 05B107Dates: 7/25/2005 - 8/19/2005
10/17/2005 - 11/11/2005Location: New Castle, Galway, IrelandInstructors: Susan Breznak Honeychurch,CI, PT, Christine Cayo, OT, Rona Alexander, SPContact: Clare Lenehah, Director of ServicesEnable Ireland Children’s Centre GalwaySeamus Quirke Road, New Castle, Galway+353.91.526321 • Fax [email protected]_______________________________________
Course #: 05B108Dates: 7/8/2005–7/13/2005
8/5/2005–8/7/20059/16/2005–9/18/200510/14/2005–10/16/200511/4/2005–11/6/20051/13/2006–1/15/20062/10/2006–2/12/20063/10/20006–/12/20064/21/2006–4/23/2006
Location: Austin (Cedar Park),TXInstructors: Judith Bierman, CI, PT,Gail Ritchie, OTR, Ann Heavey, SLPContact: Susan Alabaugh

N D T A N E T W O R K • M A Y / J U N E 2 0 0 5 • C L I N I C A L T O O L S • 2 3
Welcome to the 21st century! And what a
century it is destined to be. Globalization.
Consolidation. Instant access. These are all
terms for the new millennium. It is hard to
imagine what the future holds. However one
thing is certain. The more advances we make,
the greater our need for quality leaders.
Leadership must come from the heart.
Leaders must be driven by a passion to facil-
itate and manage change. When I think of
leadership, these are the characteristics that
come to mind.
Throughout my journey with the Neuro-
Developmental Treatment Association
(NDTA), the spirit of volunteerism has been
a prevailing force. Recently, I read an article
by William C. Richardson, President and
Chief Executive Officer of the W.K. Kellogg
Foundation, titled “Leadership Reconsidered:
Engaging Higher Education in Social
Change.” This article made some strong
points, which I would like to share with you.
Richardson wrote, “The capacity to lead is
rooted in virtually any individual and in every
community.” Further, he said a leader can be
anyone, regardless of formal position, who
serves as an effective agent of change.
The point is simple. The potential to be a
leader and a “change agent” is in all of us.
There are many people in this organization
with a passion and drive for change. These
individuals take it upon themselves to get
involved and help motivate others in the
right direction. Leadership is responsible for
communicating (through words and action)
the mission, vision and priorities of an organ-
ization. In October, a number of individuals
made a commitment to embark on a lead-
ership journey. The NDTA Board of
Directors welcomed incoming Secretary
Barry Chapman, Director of Regions Pamela
Moore and Instructor Group (IG) Executive
Committee Chair Kay Folmar. Director of
Public Relations Carol Nunez-Parker and
Director of Research Clare Giuffrida have
returned to their respective positions. Brenda
Pratt, our outgoing President, will lend her
leadership, kanowledge and expertise as Vice
President/President Elect. Our outgoing
Secretary Carrie Mori, Director of Regions
Debbie Evans-Rogers and IG Executive
Committee Chair Nicky Schmidt have been
deeply involved and committed in helping
move our association forward. On behalf of
NDTA, I would like to thank all of these indi-
viduals for their dedication, enthusiasm and
leadership.
In this and upcoming issues of the NDTA
N e t w o r k ,
members will see
the collaborative
work of the
E d i t o r i a l
A d v i s o r y
C o m m i t t e e .
Better than ever,
the publication
continues to
communicate
the direction of
our professions
and NDTA. Its
articles may help
you reshape your
current prac-
tices. They may
cause you to
reflect on the
direction our
association and,
most impor-
tantly, what it all
means to you as
a member. This
issue of the
Network is dedi-
cated to
exploring forced
use/constraint-induced intervention. Make
sure to read Susan Woll’s and Jan Utley’s
article on the close relationship between the
theme and NDT.
Our association is not successful without
the contributions, input and hard work from
our members. I would encourage you to
actively participate in the leadership of NDTA
through committee involvement at a regional
or board level, research development or
educational events. The opportunities to lead
are endless.
Never hesitate to step forward and take on
a leadership role.Your involvement can help
All Members Are LeadersNDTA IS STRONGER WHEN EACH OF US CONTRIBUTES.
BY DEBRA J . PAUL. OTR
Upcoming NDTA Inc. Approved Courses
Administrative Assistant/Continuing Education,Neuro-Developmental Treatment Programs, Inc.817 Crawford,Augusta, GA 30904706-736-1255 • Fax 706-736-1258 • [email protected]_________________________________________________________
Course #: 05B109Dates: 11/7/2005–11/12/2005
12/9/2005–12/11/20051/20/2006–1/22/20062/17/2006–2/20/20063/31/2006–4/2/20064/28/2006–4/30/20066/23/2006–6/25/20067/21/2006–7/23/20068/18/2006–8/20/2006
Location: Salem, NHInstructors: Linda Kleibhan, PT, CI, Barbara Hodge, PT, CI,Rona Alexander, CCC, SLP, PhD, Gail Ritchie, OTR
Contact: Kristen Tortora, Jon Greenwood, PT
Northeast Rehabilitation Hospital
70 Butler St., Salem, NH 03079
603-893-2900 Ext. 766 • [email protected]
NDT/BOBATH APPROVED ADVANCED COURSES REQUIRING THE SUCCESSFUL COMPLETION
OF AN NDT BASIC COURSE
Course #: 05U101Course Title: NDTA Approved Advanced Course in theTreatment of Adults: Upper Extremity CourseDates: 1/18/2006–1/22/2006Location: Sunrise (Fort Lauderdale), FLInstructor: Monica Diamond, CI, MS, PTContact: Monica Diamond, CI, MS, PT414-421-8427 • Fax [email protected]________________________________________________________
Course #: 06Y101Course Title: Advanced Baby CourseLocation: Allentown, PADates: 3/27/2006–4/7/2006Instructor: Lois Bly, CI, MA, PT, Mechthild Rast, PhD, OTR/L,Lisa Glasner, SLPContact: Cindy Miles, PT, MeD, PCS, Cindy Miles and Assoc.3721 Crescent Ct. W,Whitehall, PA 18052610-820-7667 • Fax 610-820-7671 • E-mail: [email protected]
E D U C A T I O N A L O P P O R T U N I T I E S
PEDIATRIC SPEECH THERAPIST:Innovative Outpatient, Private Practice in Whitehall,
Pennsylvania (Near Allentown)
Center & Home Based Services Early Intervention, Preschool & School age
Full Time/Part Time/Per DiemFlexible Hours
Experience a MustLicensed & CCC’s
Contact: Cindy MilesPhone: 610-820-7667
Fax: 610-820-7671www.cindymiles.com
E M P L O Y M E N TO P P O R T U N I T Y

Neuro-Developmental Treatment Association1540 S. Coast Hwy, Suite 203Laguna Beach, CA 92651
Prsrt StdU.S. Postage
PAIDDocumation
T H E N E U R O - D E V E L O P M E N T A L T R E A T M E N T A S S O C I A T I O N • M A Y / J U N E 2 0 0 5 • V O L U M E 1 2 , I S S U E 3
Confused about the Initials NDT?The letters “NDT” are used by many entities (Non-Destructive Testing comes to mind). But in the therapy world since atleast 1983, NDT has stood for Neuro-Developmental Treatment and is associated with the treatment approach originally developed by Karel and Berta Bobath in 1943.
Neuro-Developmental Treatment is:
• An evolving, holistic approach, developed by the Bobaths, in which “everything done in treatment should serve as adirect preparation for specific functional use.” (B. Bobath, 1977, p. 312).
• The most widely used treatment in North America for children and adults with cerebral palsy and for adults withhemiplegia following stroke in North America (as discussed by Cherry & Knutson, 1993; Hayes, McEwen, Lovett, Sheldon &Smith, 1999; Sweeny, Heriza & Markowitz, 1994.
• The therapy approach sanctioned by the Neuro-Developmental Treatment Association (NDTA), whichhas been in existence since the mid-1970s and was registered in 1977 as an association of physical, occupational, andspeech-language therapists who practice Neuro-Developmental Treatment.
• Definitively explained in the 2002 theory book, Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Practice by Janet Howle in collaboration with the NDTA Theory Committee (published by NDTA, Inc.) The book has been reviewed by a number of national journalists and has been recommended as“the best resource on the current status of the NDT approach....”
If you are planning to take an NDT course or study NDT theory, don’t be confused by initials. Make sure it is a Neuro-DevelopmentalTreatment course, sanctioned or sponsored by NDTA, Inc., with Instructors and Coordinator Instructors that are trained and active with NDTA, Inc.
C O N S U M E R A L E R Ty