Embed Size (px)
Citation preview
Clinical Trials for
Bloodstream Infection / Infective Endocarditis
G. Ralph Corey, MD
Vance Fowler, MD
Duke Clinical Research Institute
April 15, 2004
Issues With Bacteremia As an Indication
CAP
UTI
Bacteremia
Meningitis
EndocarditisComplicated
IABD
Osteomyelitis
1998 Anti-Infective Drugs Advisory Committee
I. Bloodstream infection (BSI) of known tissue origin
*Cure of origin leads to cure of bacteremia
UTI
Pneumonia
Intra-abdominal abscess
1998 Anti-Infective Drugs Advisory Committee (cont’d)
II. Bloodstream infection of known catheter origin
Removal of catheter and 1-2 of weeks of antibiotic leads to cure
S. aureus
Enterococcus spp.
Candida
Coagulase Negative Staphylococci
1998 Anti-Infective Drugs Advisory Committee (cont’d)
Committee conclusions became guidelines for trials of anti-infective agents in patients with documented
catheter-associated BSI
Problems With This Approach
• Requires proof of catheter infection
• Assumes that origin of BSI defines complication potential
• Combines virulent and less virulent organisms
• Allows approval for more benign diseases without subsequent requirement for trials in life-threatening disease
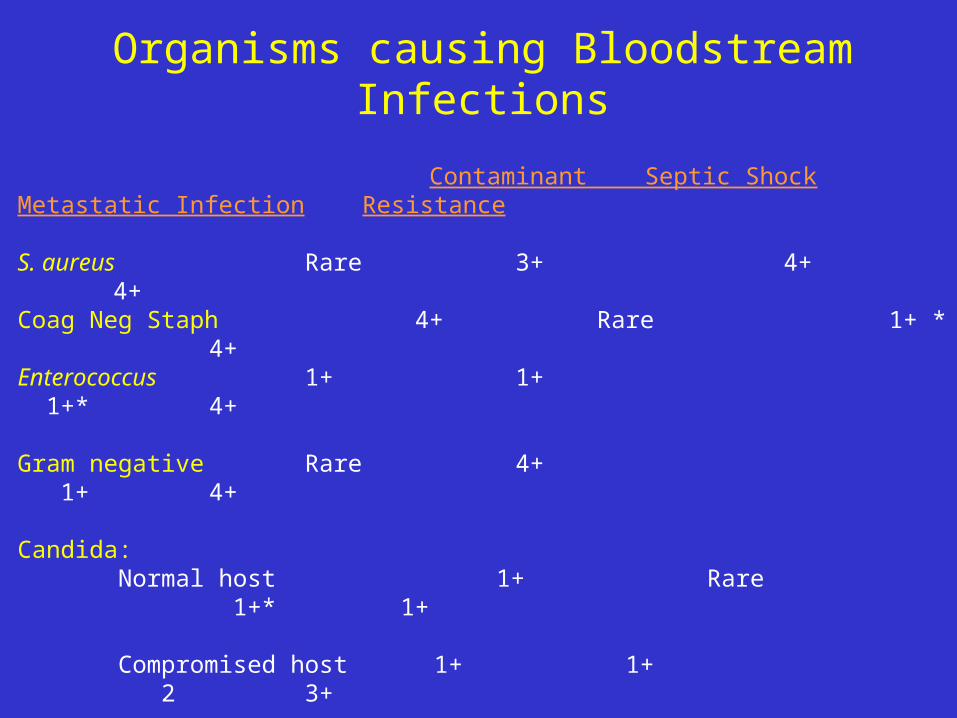
Contaminant Septic Shock Metastatic Infection Resistance
S. aureus Rare 3+ 4+ 4+
Coag Neg Staph 4+ Rare 1+ * 4+
Enterococcus 1+ 1+ 1+* 4+
Gram negative Rare 4+ 1+ 4+
Candida: Normal host 1+ Rare 1+* 1+ Compromised host 1+ 1+ 2 3+
* Primarily with intravascular foreign bodies
Organisms causing Bloodstream Infections
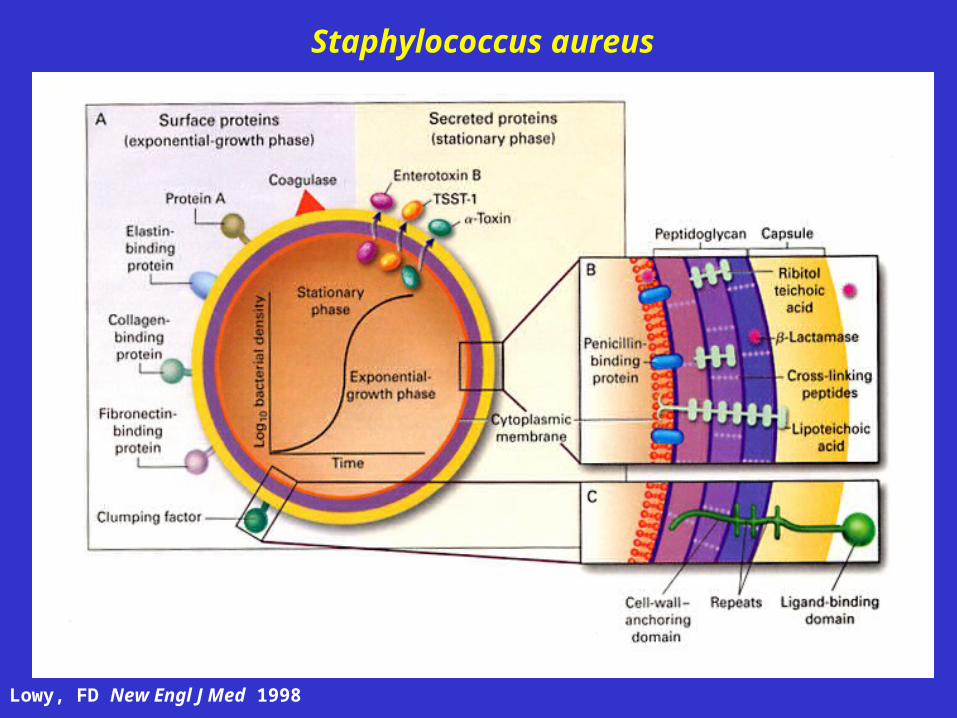
Staphylococcus aureus
Lowy, FD New Engl J Med 1998
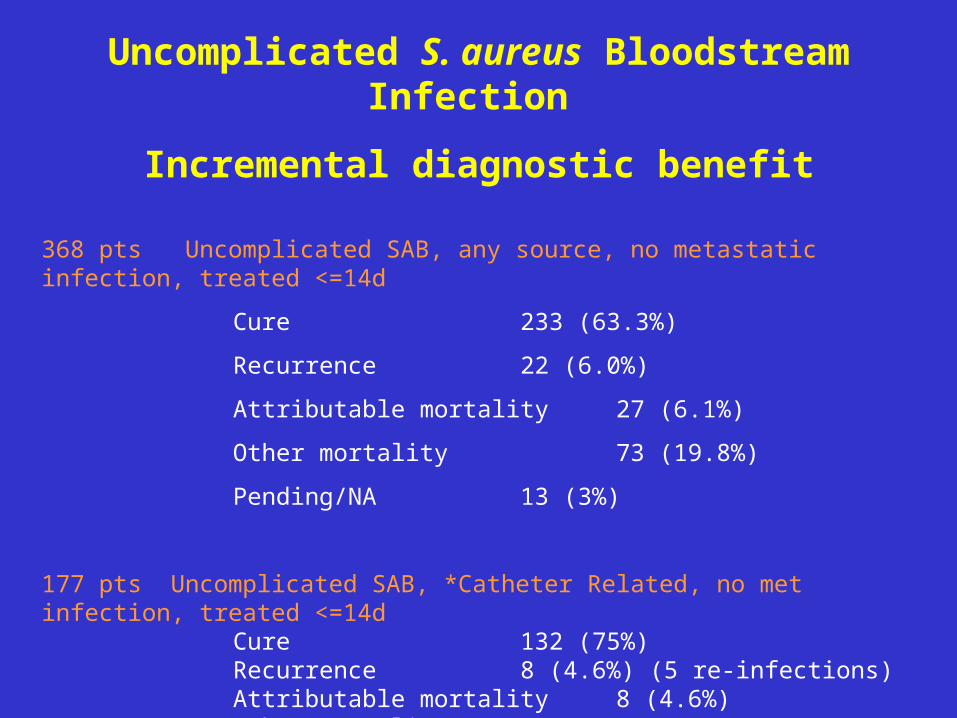
Uncomplicated S. aureus Bloodstream Infection
Incremental diagnostic benefit
368 pts Uncomplicated SAB, any source, no metastatic infection, treated <=14d
Cure 233 (63.3%)
Recurrence 22 (6.0%)
Attributable mortality 27 (6.1%)
Other mortality 73 (19.8%)
Pending/NA 13 (3%)
177 pts Uncomplicated SAB, *Catheter Related, no met infection, treated <=14dCure 132 (75%)Recurrence 8 (4.6%) (5 re-infections)Attributable mortality 8 (4.6%)Other mortality 26 (14.7%)Pending/NA 3 (1.7%)
*Presumed
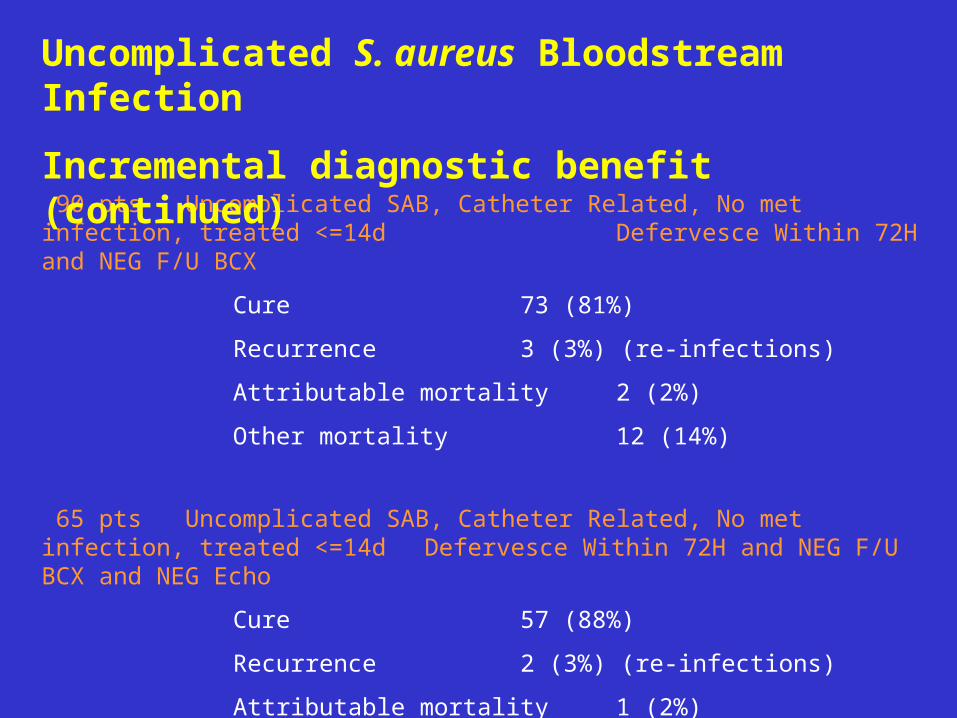
90 pts Uncomplicated SAB, Catheter Related, No met infection, treated <=14d Defervesce Within 72H and NEG F/U BCX
Cure 73 (81%)
Recurrence 3 (3%) (re-infections)
Attributable mortality 2 (2%)
Other mortality 12 (14%)
65 pts Uncomplicated SAB, Catheter Related, No met infection, treated <=14d Defervesce Within 72H and NEG F/U BCX and NEG Echo
Cure 57 (88%)
Recurrence 2 (3%) (re-infections)
Attributable mortality 1 (2%)
Other mortality 5 (7%)
Uncomplicated S. aureus Bloodstream Infection
Incremental diagnostic benefit (continued)
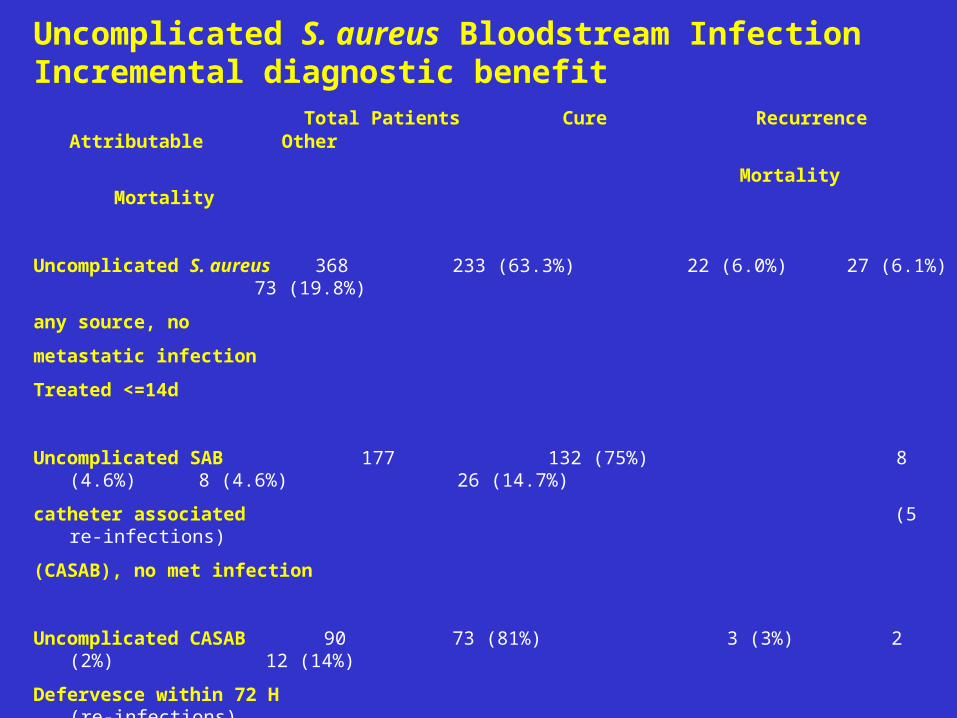
Total Patients Cure Recurrence Attributable Other
Mortality Mortality
Uncomplicated S. aureus 368 233 (63.3%) 22 (6.0%) 27 (6.1%) 73 (19.8%)
any source, no
metastatic infection
Treated <=14d
Uncomplicated SAB 177 132 (75%) 8 (4.6%) 8 (4.6%) 26 (14.7%)
catheter associated (5 re-infections)
(CASAB), no met infection
Uncomplicated CASAB 90 73 (81%) 3 (3%) 2 (2%) 12 (14%)
Defervesce within 72 H (re-infections)
and NEG F/U BCX
Uncomplicated CASAB 65 57 (88%) 2 (3%) 1 (2%) 5 (7%)
NEG echo
Uncomplicated S. aureus Bloodstream Infection Incremental diagnostic benefit
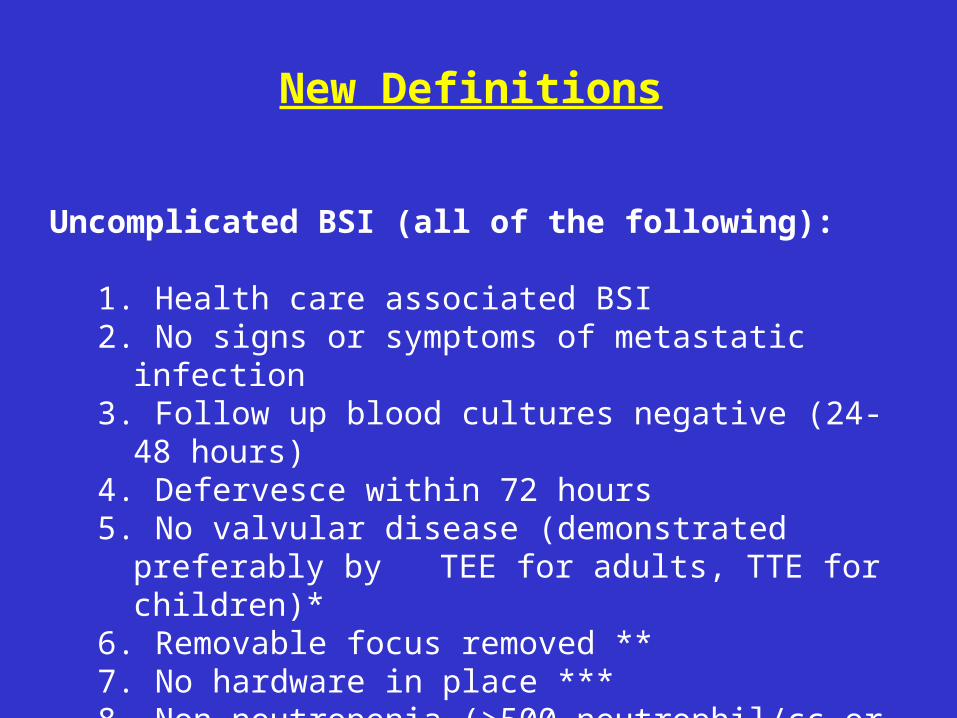
New Definitions
Uncomplicated BSI (all of the following):
1. Health care associated BSI2. No signs or symptoms of metastatic infection3. Follow up blood cultures negative (24-48 hours)4. Defervesce within 72 hours5. No valvular disease (demonstrated preferably by
TEE for adults, TTE for children)*6. Removable focus removed **7. No hardware in place ***8. Non-neutropenia (>500 neutrophil/cc or if known
HIV patient CD4>200 cell/mm3)
Complicated BSI: A. For study purposes
1. Follow up blood culture positive despite removal of all intravascular devices after initial blood culture
2. No signs and symptoms of metastatic disease upon enrollment (exception-uncomplicated IE)
3. No hardware***
Note: Length of fever may be either less or greater than 72 hours Echo not necessary before enrollment
Inappropriate for studies:
1. S or S of metastatic disease on presentation
2. Removable focus not removed
3. Hardware in place***
4. Neutropenia
*Significant valvular heart disease is defined (by TTE or TEE) as:
1. More than trivial insufficiency and/or more than mild stenosis
2. Congenital heart disease (not including mitral valve prolapse unless meeting above criteria)
** Primarily intravenous catheters
*** Non-removable hardware is defined as:
1. Joint prostheses, plaques, screws, and rods
2. Intravascular valves, vein filters, and stents/grafts placed within 6 weeks of BSI
Present Guidance
1. Phase 2: randomized double blind study of cSSSi2. Phase 2: 2 randomized double blind studies of
uncomplicated BSI (preferably superiority)
3. Phase 3: randomized double blind study of complicated BSI
Assumption I: Step 1 predicts success / failure in step 2Step 2 predicts success / failure in step 3
Assumption II: Completion of step 1 leads to step 2 and step 2
leads to step 3
Proposal
1. Change Definitions
a. Uncomplicated BSI
b. Complicated BSI
c. Others
2. Change Trial Design
Proposal
Fast Track
1. Phase 2: randomized double blind study of cSSSi
2. 50 patient open label consecutive series with new anti-infective in uncomplicated bloodstream
infections a. Cure > 85% then proceed to large randomized,
double blind, Phase 3 trial in patients with both complicated and uncomplicated disease
b. Cure < 85% then proceed to randomized, double blind Phase 2 trial in patients with uncomplicated
bacteremia only. After showing non-inferiority proceed to Phase 3 trial with both uncomplicated and complicated BSIs.
Middle of the Road
1. Phase 2: randomized double blind study of cSSSi
2. Phase 2/3: large open label randomized study of all patients with SAB with adjudication
every 5 cases
Mimic Cardiology
1. Test the drug in the disease of interest
2. Start with both uncomplicated and complicated BSI with case by case adjudication
3. Prevents having the drugs “tested” in the sickest patient with off label, unsupervised use by practicing physicians





























