Embed Size (px)
Citation preview

Clinical Trials
Horizon 2020 'Health, demographic change and
wellbeing'
Open Info Day -Horizon 2020'Health, demographic change and wellbeing'
Brussels, 22 Nov 2013
Disclaimer
Pending formal adoption by the EU of the Horizon 2020 legal texts, the content of these slides is not definitive and so should not be taken as such, nor used or referred to as such in any way or for any purpose
Agenda
• Essential information on clinical trials/studies/ investigations (CT) to be provided in the (2nd stage!) proposal
• Financial and contractual aspects•Subcontracting – CROs
•Involvement of patient recruitment sites
•Unit costs per patient
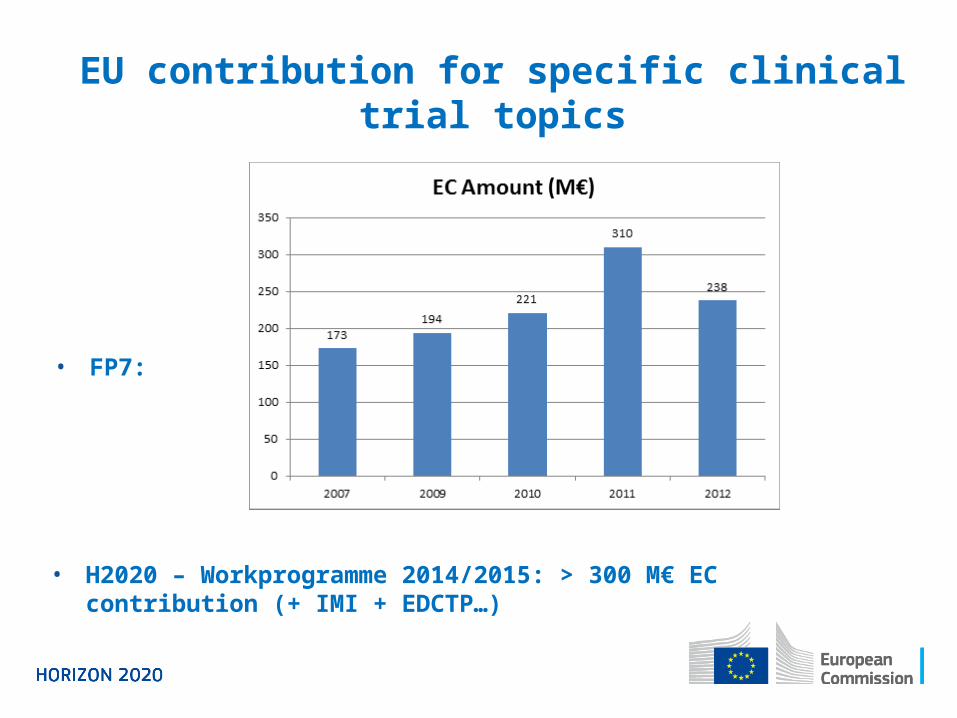
• H2020 – Workprogramme 2014/2015: > 300 M€ EC contribution (+ IMI + EDCTP…)
EU contribution for specific clinical trial topics
• FP7:
Each section shall be shortly and concisely described.
In case one or more issues do not apply to a particular study, please explain/justify.
When information is currently not available (e.g. a clinical trial is planned for a later stage of the project and will be based on data of previous studies) the source of required data shall be provided and / or the selection of the applied methodology clearly described.
Format for this information to be decided (possibly specific template in submission system)
Essential information aboutClinical trials / studies / investigations (stage 2)
1.1 IdentifierTitle, short title of unique identifier.
1.2 Study design and endpointsDescription of selected study design and primary and secondary objectives (endpoints/outcome measures).
1.3 Scientific advice / protocol assistanceIf scientific advice / protocol assistance from a competent/regulatory authority has been requested, please provide the full text answer of the authority or a comprehensive summary. If the answer is not available provide explanation of current status.
1.4 Subjects/population(s)Definition of study population(s) by inclusion and exclusion criteria. Definition of sub-populations if subgroup analysis is intended.
1.5 Sample sizeDefinition and justification (power calculation) of sample size.
Essential information aboutClinical trials / studies / investigations (stage 2)
1.6 Statistical methodsDefinition of statistical methods and planning of statistical analysis.
1.7 ConductDescription of planned strategy for study management, monitoring, data management and planned schedule for study conduct (including provisions and timelines for ethics and further administrative approvals). If a study medication is required, please provide information on whether manufacturing and/or labelling of the study medication is required and which plans are in place for this.
1.8 Orphan designationIf orphan designation has been granted provide the reference of the Commission Decision. If orphan designation has been requested but not granted provide an update on the current status.
Essential information aboutClinical trials / studies / investigations (stage 2)
1.9 Calculation of ‘unit costs per patient’ for Clinical studies
See below
Essential information aboutClinical trials / studies / investigations (stage 2)
Financial and Contractual Aspects - Basics
• Clinical trials (CT) subject to the same legal provisions and guidance notes as other H2020 projects. No special 'derogations' (with the possible exception of special 'unit costs')
• BUT: Specific features of CT require consistent application of existing rules
Subcontracting – Clinical/Contract Research Organisations (CROs)
• Only limited part of the action can be subcontracted, i.e. core CT expertise needs to be available in consortium
• BUT: specialised services (pharmacokinetics, regulatory etc.) from CROs might be indispensable for CT
• 'Academic CROs' exist (e.g. ECRIN network) – might be willing to become beneficiary!
• But: CROs usually 'for profit' → Commission will consider accepting subcontracting
Subcontracting - CROs
'Rule of thumb' for amount of subcontracting:
• If CT is the main activity of the project:
Clinical trial cannot be subcontracted entirely, but certain parts
(GMP manufacturing, audit, monitoring etc.) might be
subcontracted as long as the design, overall planning,
oversight and intellectual input into the trial is clearly with
beneficiaries (budget share not essential criterion!)
• If CT is just a small part of the project, i.e. most of the project is preclinical activity:
CT might be subcontracted in its entirety
Involvement of patient recruitment sites
Centres whose contribution is limited to patient recruitment and inclusion may have status of: • Full beneficiary – always preferred, never discouraged!
But: if obstacles for centres to become beneficiary, two other options remain:
• Use of in-kind contributions provided by 'third parties against payment' (ex-FP7: Third party 'making available its resources')
• Subcontractor
Use of in-kind contributions provided by third parties against payment
• Third parties must be identified in Annex I
• no profit, reimbursement of actual costs (!)
• requires prior agreement with beneficiary – prior to start of work, not necessarily prior to signature of GA
• agreement might be 'ad-hoc'/specific to project
• No indirect costs for beneficiary! But in case of 100% reimbursement rate of direct costs, no more 'shortfall' for linked beneficiary
Involvement of patient recruitment sites (2)
Subcontractor
• task (!) must be identified in Annex I
• agreed 'price per patient', profit possible
• best price/quality ratio, transparency equal treatment
• public bodies: internal rules and applicable legislation related to public procurement
• No indirect costs for beneficiary! But in case of 100% reimbursement rate of direct costs, no more "shortfall" for linked beneficiary
Involvement of patient recruitment sites (3)
Decision pending
'Unit costs' per patient
• Unit costs (UC) foreseen by RfP (Art. 19.2 + 30.1) and FR (Art. 124)
• Specific unit costs to be defined in Commission Decision – currently pending for unit costs per patient for clinical studies
• Planned as optional for each beneficiary (alternative: real costs!)
• If applied – to be applied to all patients for this beneficiary!
Decision pending• Based on actual costs recorded in last closed accounts of
beneficiary
• Beneficiary estimates resources needed per patient
• Estimations (per patient, per trial, per beneficiary) would be included in 2nd stage (!) proposal and will be assessed by evaluators
• Ex-post audits would check only
• number of units/patients and
• compliance of estimations with correct accounts
'Unit costs' per patient (2)
Decision pending• Advantage:
• Much simplified way of claiming all directly patient-related costs (no need for time sheets or detailed documentation for each patient!)
• BUT:
• Effort in describing resources and costs at (stage 2) proposal level
• Correct determination of value of a given resource remains subject to verification.
'Unit costs' per patient (3)






























