-
Sungha Park M.D
Division of Cardiology
Yonsei Cardiovascular Center
Yonsei University College of Medicine
Clinical utility of Novel
biomarkers
-
Agenda
• Identifying high risk patients(Primary
prevention)
• Accurate diagnosis of coronary artery disease in
the ER
• Prognostic factor for future cardiovascular
events(Secondary prevention)
-
Biomarkers in ACS patients: vascular inflammation to
plaque rupture to ischemia to cell death to myocardial
dysfunction
Clinical Chemistry 2005;51:5 810–824
-
Prerequisite requirement
for useful biomarker
• Standardized assay
• Very specific for cardiovascular system
• Established reference value
• Strongly correlates with CVD while showing poor correlation
with traditional risk factors
• Ability to improve prediction beyond traditional risk
factors
• Acceptable cost
-
Prevalence of Risk Factors in Patients with Coronary Heart
Disease
Khot, et al. JAMA 2003;290:898-904
0
5
10
15
20
25
30
35
40
45P
erc
en
t
0 1 2 3 4Risk Factors
Women
Men
-
Does CRP provide predictive
information beyond existing
global predictors?
-
CRP and Risk of MI: Rotterdam Study
van der Meer, et al Arch Intern Med 2003;164:1323-8
Rotterdam Study: Prospective trial of 7093
apparently healthy men and women, age > 55,
in which 157 with myocardial infarction were
compared with 500 selected controls were
compared in nested case control analysis based
on baseline CRP levels.
CRP compared with Framingham Risk Score (FRS):
Receiver operating characteristic curve was not
improved when hs-CRP was added FRS:
•AUC FRS: 0.745
•AUC FRS + CRP = 0.748
P Trend = 0.50
00.5
11.5
22.5
33.5
44.5
5
Od
ds R
ati
o f
or
Myo
card
ial
Infa
rcti
on
1 2 3 4
CRP Quartile
-
Folsom AR et al Arch Intern Med 2006;166:1368-1373Folsom AR et
al Arch Intern Med 2006;166:1368-1373
-
CRP and Framingham Risk Score
Ridker PM et al NEJM 2002;347:1557-1565
27939 subjects in the Women’s Health Study
-
Variability of CRP
according to ethnicity
Arnand SS et al ATVB 2004;24:1509-1515
-
AHA/CDC Consensus Panel
Class I: None
Class IIa:
• In primary prevention, CRP measurement may be
useful in those at intermediate risk (10-20% 10-year
CHD risk), to help direct further evaluation and
treatment.
• In patients with stable CAD or ACS, CRP may be
useful as an independent marker of recurrent events,
including death, MI and restenosis following PCI.
Circulation 2003;107:499-511
Hs-CRP Recommendations
-
Agenda
• Identifying high risk patients(Primary prevention)
• Accurate diagnosis of coronary artery
disease in the ER
• Prognostic factor for future cardiovascular
events(Secondary prevention)
-
Clinical dilemma in diagnosing
troponin negative
acute coronary syndrome
• Absence of biomarkers that are specific for the heart except
troponin
• Absence of biomarkers that has the ability to improve
prediction beyond traditional risk factors
-
Sensitivity of IMA for diagnosis of ACS
Sinha MK et al.Emerg Med J 2004;21:29–34
IMA for diagnosis of CAD
-
Change of IMA during exercise40 consecutive pts with known
CAD
Sbarouni E et al J Am Coll Cardiol 2006;48:2482-2484
-
Ischemia modified albumin in the
clinical practice
• Period: from Nov.2005 to Aug. 2007
• Patients: 500 patients with chest pain who arrived at the
emergency department or outpatient clinic
• Method:
Blood sampling for IMA at the time of the hospital arrival.
Echocardiography, coronary angiography, TMT,or MIBI
-
Comparison of IMA levels between patients with
atypical chest pain and ischemic heart disease
Atypical
chest pain(N=236)IHD (N=264) p
Age 57.8 +/- 15.8 66.3 +/- 45.6 0.007
Sex, M/F 55.9/44.1 70.1/29.9 0.001
Diabetes 12.70% 24.20% 0.001
Hypertension 33.10% 52.70%
-
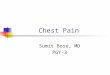
sensitivity specificitypositive
predictivenegative predictive
IMA>90 84.1 14.4 52.4 44.7
IMA>95 67.8 34.3 53.6 48.8
IMA>98 51.9 42.8 50.4 44.3
IMA>105 30.7 64.4 49.1 45.4
IMA>110 23.1 78.8 55 47.8
ROC curve comparing sensitivity
and specificity of IMA levels
YUMC data
AUC=0.52
-
Agenda
• Identifying high risk patients(Primary prevention)
• Accurate diagnosis of coronary artery disease in
the ER
• Prognostic factor for future cardiovascular
events(Secondary prevention)
-
Early Risk Stratification - cTn
In patients with a clinical syndrome consistent with ACS, a
maximal (peak) concentration exceeding the 99th percentile of
values for a reference control group should be considered
indicative of increased risk of death and recurrent ischemic
events
Class I, Level of Evidence A
-
Antman EM et al. JAMA. 2000;284:835-42.n = 1957 ACS patients
Risk factors
(n)
0
45
35
25
15
5
0/1 2 3 4 5 6/7
Death/MI/
severe ischemia
at 14 days
(%)
4.7
8.3
13.2
19.9
26.2
40.9
TIMI risk score in UA/NSTEMI
-
Risk of death in patients with NSTEAC syndrome stratified by
quartile of
concentration of NT-proBNP (Elecsys 2010, Roche Diagnostics) at
baseline
James SK et al. Circiculation 2003;108:275-81.
-
Westerhout CM et al. J Am Coll Cardiol 2006;48:939-947
-
1. Screening of the population as a whole is NOT recommended
2. Application of secondary prevention measures should not
depend upon hs-CRP results
3. Application of management guidelines for acute coronary
syndromes should not be dependent upon hs-CRP level
4. Serial CRP levels should not be used to monitor effects of
treatment
Circulation 2003;107:499-511
AHA/CDC Consensus PanelHs-CRP Recommendations
-
Comparison of novel biomarkers
Standardized Specific Established
Reference
Independent
from traditional
risk factors
Improve prediction
beyond traditional
risk factors
hsCRP Yes No Yes No Weak
CD40L No No No Yes NA
PAPPA No No No No NA
IMA No No Yes Yes NA
Myeloperoxidase No No No No NA
Non of the biomarkers have proven to be
better than hsCRP: Why use it?
-
Yonsei Cardiovascular Hospital
Yonsei University College of Medicine
-
Class IIa:
• Measurement should be done twice (two weeks apart)
and results averaged.
• If level > 10 mg/L, test should be repeated and patient
examined for sources of infection or inflammation
• Classify risk as follows:
Low < 1 mg/L
Average 1.0 – 3.0 mg/L
High: > 3.0 mg/L
Circulation 2003;107:499-511
AHA/CDC Consensus Panel
Hs-CRP Recommendations
-
CRP Limitations
• Most studies limited to North American and
European population -- limited ability to
extrapolate to Native American, African and
South Asian
• Not good indicator of extent of disease burden
• Most studies have not adjusted for body-mass-
index
• Strength of association lessoned in some
studies when adjusting for other risk factors
-
C-reactive Protein
• Circulating acute phase reactant
• Many-fold increase with injury & infection
• Synthesized in liver, induced primarily by
interleukin-6 (IL-6)
• Stable levels in circulation, not affected by
meals, no circadian levels
• Level – within normal range – predicts
CVD risk
-
*Family history of CAD, hypertension, elevated
cholesterol, diabetes, current smoker†Creatine-kinase MB and/or
cardiac troponins Antman EM et al. JAMA. 2000;284:835-42.
TIMI risk score for UA/NSTEMI
• Age ≥65 years
• ≥3 CAD risk factors*
• Significant coronary stenosis
• ST-segment deviation
• Severe angina (≥2 anginal events in last 24
hours)
• Daily use of aspirin in prior 7 days
• Elevated serum cardiac markers†
-
CRP and Cardiovascular Risk
• MI
• Stroke
• Peripheral arterial disease
• Sudden cardiac death
• Recurrent ischemia and death in:
• Unstable Angina
• Myocardial Infarction
• Percutaneous intervention
CRP will Predict:
-
Early Risk Stratification
hsCRP and BNP/NTproBNP
… may be useful, in addition to a cardiac
troponin…
The benefits of therapy based on this strategy
remain uncertain!
Class IIa, Level of Evidence A
-
Ischemia-Modified Albumin
• The amino terminal end (N-terminal) of the albumin molecule is
a binding site for transitional metals such as cobalt, copper and
nickel.
• Possibly as the result of hypoxia, acidosis, free-radical
injury and energy dependent membrane disruption, the N-terminal
undergoes a decrease in binding capacity in the presence of
ischemia.
This alteration can be measured: a set amount of cobalt is added
to the patient’s serum, after which a colorimetric assay, the
albumin–cobalt binding assay, is used to determine the amount of
cobalt that remains unbound.
Bar-Or D et al. Am Heart J 2001;141:985-91.
-
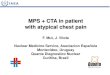
OPUS-TIMI 16
Sabatine MS et al. Circulation. 2002;105:1760-3.
TACTICS-TIMI 18
1
1.8
3.5
6
12.1
5.7
13
1 2 301 2 30
14
10
6
2
BNP = B-type natriuretic peptide
CRP = C-reactive protein
6
4
2
0
30-day
mortality
relative
risk
Elevated cardiac biomarkers (n) Elevated cardiac biomarkers
(n)
P = 0.014 P < 0.001
67 150 155 78 504 717 324 90
0
Multimarker strategy: Identifying high-risk
patients by troponin I, CRP, and BNP
n =